Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
While experts disagree whether the postpolio syndrome is caused by a reactivation of the dormant virus or by an attritional aging phenomena of muscles that have been overworked over a period of time, both groups recommend which of the following guidelines for optimizing function in this population?

Detailed Explanation
Most leaders in orthopaedic surgery support Jacqueline Perry's theory that the postpolio syndrome is an attritional degenerative process that is the result of overuse of muscles and joints that are unable to adequately tolerate overload, and have little functional reserve. For that reason, aerobic conditioning and exercise are important. Overload and exhaustion of involved muscles should be avoided.
Question 2
High Yield
Figures 15a through 15c show the radiographs of a 23-year-old football player who was injured when another player fell on his flexed and planted foot. He reports severe pain in the midfoot with a feeling of numbness on the dorsum of the foot, and he is unable to bear weight on the limb. Examination reveals mild swelling. Management should consist of



Explanation
Myerson and associates studied the outcomes of 19 patients with tarsometatarsal joint injuries during athletic activity. Injuries were classified as first- or second-degree sprains of the tarsometatarsal joint or a third-degree sprain with diastasis between the metatarsals or cuneiforms. Poor functional results were seen in those with a delay in diagnosis and with inadequate treatment. For patients with third-degree sprains, poor results were obtained with nonsurgical management. These patients required open reduction and internal fixation for optimal return to function. The anatomic reduction is critical to the outcome; therefore, open reduction is preferred. Baxter DE: The Foot and Ankle in Sport, ed 1. St Louis, MO, Mosby, 1995, pp 107-123. Curtis MJ, Myerson M, Szura B: Tarsometatarsal joint injuries in the athlete. Am J Sports Med 1993;21:497-502. Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 3
High Yield
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb "feels" different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?

Detailed Explanation
The patient initially has a distal third femoral fracture and a pulseless limb. The first step is to reduce the fracture and reassess the vascular status. Although the pulse returns, it feels different than the quality of the pulse in the contralateral uninjured extremity. There is a risk of a vascular injury with this fracture pattern due to tethering of the femoral vessels at the adductor hiatus; therefore, the vascular status needs further assessment since the pulses are not symmetrical. A physical examination is not very accurate in assessing whether a vascular injury is present; therefore, serial examinations are not appropriate. Angiography is very sensitive and specific but is time consuming and can cause complications secondary to the dye and the arterial puncture required to perform it. Duplex ultrasound is effective but is very operator-dependent and may not be available 24 hours a day. The ABI is easily performed and has been shown to be sensitive and specific. If the value is greater than 0.9, the negative predictive value is 99% and when the value is less than 0.9, it is 95% sensitive and 97% specific for a major arterial injury. It has been shown to be useful for blunt lower extremity injuries as well as knee dislocations. Levy BA, Zlowodzki MP, Graves M, et al: Screening for extremity arterial injury with the arterial pressure index. Am J Emerg Med 2005;23:689-695. Abou-Sayed H, Berger DL: Blunt lower-extremity trauma and politeal artery injuries: Revisiting the case for selective arteriography. Arch Surg 2002;137:585-589.
Question 4
High Yield
Injury to which of the following structures has been reported following iliac crest bone graft harvest?
Explanation
Injury to the lateral femoral cutaneous nerve and the ilioinguinal nerve have both been described with an anterior iliac crest bone graft harvest. The lateral femoral cutaneous nerve may be injured from retraction after elevating the iliacus muscle or from direct injury when the nerve actually courses over the crest. A posterior crest harvest can injure the superior gluteal artery if a surgical instrument violates the sciatic notch. Injury to the inferior gluteal artery has not been described; it leaves the pelvis below the piriformis muscle belly and should not be at risk even with a violation of the sciatic notch. Injury to the ilioinguinal nerve has been reported from vigorous retraction of the iliacus muscle after exposing the inner table of the anterior ilium. Cluneal nerve injury may occur with posterior crest harvest, particularly if the skin incision is horizontal or extends more than 8 cm superolateral from the posterior superior iliac spine. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 323-341.
Question 5
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?


Explanation
The area shown in the arthroscopic view and MRI scan is referred to as a Buford complex and represents a normal labral variant. It consists of a thickened, cord-like middle glenohumeral ligament, a superior labral attachment of the middle glenohumeral ligament just anterior to the biceps tendon, and absence of the anterosuperior labrum. This combination of findings can be confusing and may simulate labral pathology. Mistaken repair of the lesion back to the glenoid rim can result in significant loss of external rotation. A Bankart lesion would be located at the inferior anterior glenoid rim. The subscapularis is seen anterior to the labrum. Normal variations that occur in the anterosuperior labrum can simulate pathology. Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 6
A 39-year-old man has anterior shoulder pain after landing on his abducted left shoulder while playing softball. Examination reveals a stable glenohumeral joint, pain on passive external rotation of greater than 25 degrees, and pain and weakness on belly press (Napoleon's) test. An MRI scan is shown in Figure 32. To provide maximum pain relief and return of function, management should include

Explanation
The examination and MRI scan confirm a subscapularis rupture and dislocation of the long head of the biceps tendon. The greatest return of function will result from repair of the subscapularis and tenodesis of the biceps tendon. Physical therapy alone will result in inadequate healing of the subscapularis and will not address the biceps tendon. While biceps tenotomy is an option, it will not provide the same level of pain relief and return of function as a tenodesis in a young, active man. There is no evidence for a supraspinatus tear. Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 7
An 8-year-old boy sustains nondisplaced midshaft fractures of the tibia and fibula after being struck by a car while he was riding his bicycle. No other injuries are noted, but the patient reports pain with passive motion of his toes. His neurovascular examination is otherwise normal. What is the best course of action?

Explanation
Pain with passive motion of the toes is a recognized early sign of increased compartment pressures. At a minimum, a baseline evaluation of the leg compartment pressures should be obtained. While it is normal for the patient to have pain related to the associated muscle contusions, any significant concerns should be addressed immediately in light of the severe consequences likely when a compartment syndrome occurs. Mubarak SJ, Owen CA, Hargens AR, et al: Acute compartment syndromes: Diagnosis and treatment with the aid of the wick catheter. J Bone Joint Surg Am 1978;60:1091-1095.
Scientific References
-
:
Question 8
High Yield
When compared to patients with osteoarthritis, patients with ankylosing spondylitis undergoing total hip arthroplasty can expect a
Explanation
Joshi and associates reported a 96% incidence of pain relief in 181 total hip arthroplasties in patients with ankylosing spondylitis. Only 65% of patients had good to excellent functional results, primarily the result of associated systemic diseases and spinal deformity. The incidence of infection was slightly higher, and the incidence of heterotopic ossification was higher in this group of patients.
Question 9
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a "primed" immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered. Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.
Question 10
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?


Explanation
The floating elbow is best managed with early open reduction and internal fixation of the humeral and forearm fractures, followed by early range of motion. These fractures predispose the elbow to stiffness, and early range of motion is recommended. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 11
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of

Explanation
A supracondylar fracture of the femur that occurs after total knee replacement can be treated effectively by a number of methods. For this fracture, the use of a retrograde supracondylar nail has been found to be effective in several series. The treatment of these complex injuries needs to be individualized based on the stability of the implant, the quality of the bone, and the extent of comminution of the fracture. Revision with the use of an unstemmed implant will not result in effective stabilization of the knee or the fracture.
Question 12
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 13
What is the most common surgical cause of the foot deformity shown in Figure 9?

Explanation
The radiograph shows a hallux varus deformity. Iatrogenically acquired hallux varus is most often the result of excessive lateral soft-tissue release, sesamoidectomy, or both. It also can be caused by a medial tibial sesamoid subluxation in conjunction with excessive postoperative dressing application, overcorrection of the intermetatarsal angle, or excessive medial eminence resection. Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Question 14
High Yield
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?

Explanation
Use of systemic steroids has been implicated in the development of nontraumatic osteonecrosis of the humeral head. Staging of the disease is most relevant to prognosis and treatment. Cruess has described a widely accepted staging system. Several authors have shown that patients who have a lower stage of disease (ie, stage I or II) have a much less likely chance of progression compared with those who are in the later stages (IV and V). Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39. Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Question 15
High Yield
Figures 35a and 35b show the radiographs of a patient who underwent debridement of a chronically infected, fully constrained knee prosthesis and now reports pain and instability despite bracing. History reveals that the patient has had no drainage since undergoing the last debridement 6 months ago. A C-reactive protein level and aspiration are negative for infection. Treatment should now consist of


Explanation
The radiographs show a significant loss of the proximal anterior tibial cortex, consistent with an extensively damaged or deficient extensor mechanism. Such a deficit precludes insertion of another knee arthroplasty. Arthrodesis is the treatment of choice for this patient and is indicated for loss of the extensor mechanism and knee instability. A recent report on arthrodesis following removal of an infected prosthesis showed a union rate of 91% using a short intramedullary nail. Insertion of an antibiotic-impregnated PMMA spacer is not indicated because the rationale for using a spacer is to maintain a space for reinsertion of another prosthesis. Reconstruction of the extensor mechanism would not address the loss of the joint. Amputation is the final treatment option if the arthrodesis fails. Rand JA: Alternatives to reimplantation for salvage of the total knee arthroplasty complicated by infection. J Bone Joint Surg Am 1993;75:282-289. Lai KA, Shen WJ, Yang CY: Arthrodesis with a short Huckstep nail as a salvage procedure for failed total knee arthroplasty. J Bone Joint Surg Am 1998;80:380-388.
Question 16
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections. Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 17
High Yield
Osteonecrosis of the large joints may develop in patients with which of the following conditions?
Detailed Explanation
Osteonecrosis of major joints can occur in patients exposed to corticosteroids, alcohol, and antiseizure medications, as well as patients with hemaglobulinopathy, such as sickle cell anemia. In addition, patients with primary APS who had not taken corticosteroids were also found to be at high risk for osteonecrosis of the hip. In one study of 30 patients with primary APS, asymptomatic osteonecrosis was evident in 20%. A recent article has also found a high association between idiopathic osteonecrosis of the hip and collagen II mutation. None of the other conditions has been shown to be associated with a higher risk of osteonecrosis. Tektonidou MG, Malagari K, Vlachoyiannopoulos PG, et al: Asymptomatic avascular necrosis in patients with primary antiphospholipid syndrome in the absence of corticosteroid use: A prospective study by magnetic resonance imaging. Arthritis Rheum 2003;48:732-736.
Question 18
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?

Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Question 19
High Yield
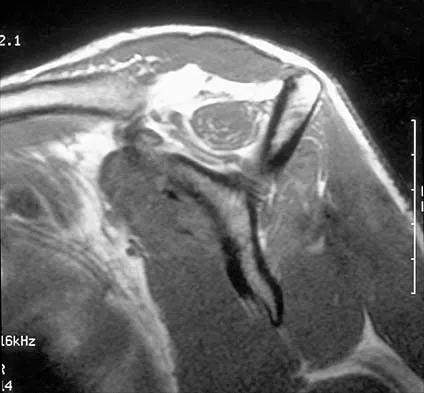
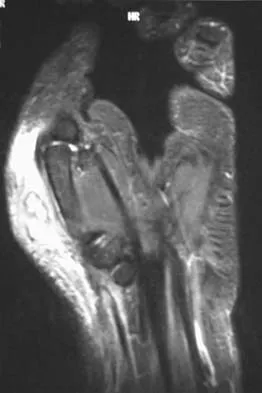
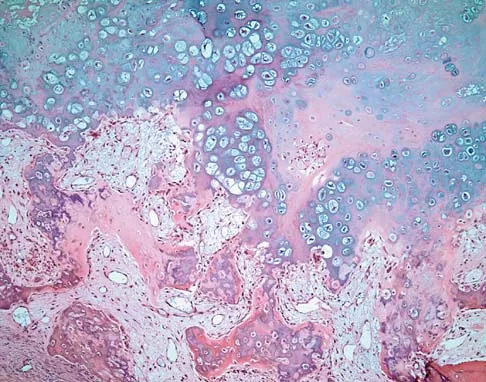
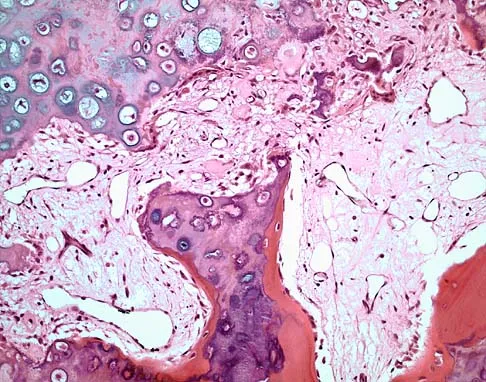
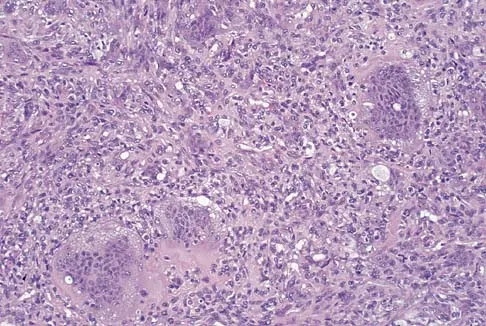
A 10-year-old girl reports activity-related bilateral arm pain. Examination reveals no soft-tissue masses in either arm, and she has full painless range of motion in both shoulders and elbows. The radiograph and bone scan are shown in Figures 20a and 20b, and biopsy specimens are shown in Figures 20c and 20d. What is the most likely diagnosis?




Detailed Explanation
Based on these findings, the most likely diagnosis is fibrous dysplasia. Twenty percent of patients with fibrous dysplasia have multifocal disease. The lesions show a typical ground glass appearance. Fibrous dysplasia frequently involves the diaphysis of the long bones. There is no associated soft-tissue mass and no periosteal reactions to these lesions, suggesting a benign lesion. The histology shows proliferating fibroblasts in a dense collagen matrix. Trabeculae are arranged in an irregular or "Chinese letter" appearance. Osteogenic sarcoma and Ewing's sarcoma have a much different radiographic appearance of malignant osteoid and small round blue cells. Periosteal chondroma does occur in the proximal humerus but is not typically multifocal. It appears as a surface lesion with saucerization of the underlying bone and a bony buttress adjacent to the lesion. Some patients with multifocal lesions have associated endocrine abnormalities (McCune-Albright syndrome). Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 118-119.
Question 20
In an acute closed boutonniere injury, what is the most appropriate splinting technique for the proximal interphalangeal joint?

Explanation
Rupture of the central slip of the extensor mechanism and a varying degree of lateral band volar migration are the pathologic entities in an acute boutonniere injury. Splinting the proximal interphalangeal joint in full extension allows reapproximation of the central slip to the base of the middle phalanx. Distal interphalangeal joint flexion is permitted to allow movement of the lateral bands distally and dorsally, preventing contracture. Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Question 21
Figure 21 shows the tomogram of a 26-year-old woman who sustained an axial load injury to her neck in a fall off a horse. What ligament is injured?

Explanation
Levine and Edwards, in their description of the classic C1 burst (Jefferson) fracture, noted that spread of the lateral masses of more than 7 mm is indicative of a transverse ligament rupture. Long-term C1-C2 instability, however, has not been described with this fracture pattern. Although long-term traction followed by halo vest immobilization has been described as the best technique for achieving an ideal result, treatment of this injury remains somewhat controversial. Levine AM, Edwards CC: Fractures of the atlas. J Bone Joint Surg Am 1991;73:680-691.
Question 22
High Yield
What changes in muscle physiology would be expected in an athlete who begins a rigorous aerobic program for an upcoming marathon?
Explanation
Muscle fibers can be categorized grossly into two types. Type I muscle, also known as slow-twitch muscle, is responsible for aerobic, oxidative muscle metabolism. It has a much lower strength and speed of contraction than fast-twitch type II muscle but is significantly more fatigue resistant. With training for endurance sports, the type I muscle undergoes adaptive changes to the increased stress. Increases in capillary density, oxidative capacity, mitochondrial density, and subsequent fatigue resistance are all observed changes. Hypertrophy of type IIb muscle is seen in strength training. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
Question 23
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
Explanation
An infection of the shoulder is considered a surgical emergency unless there are medical reasons that a patient cannot be taken to the operating room. If cultures of wound drainage are in question, then an aspiration should be done emergently, not several days later. The hallmark of infection in any major joint is increasing pain out of proportion to what is expected. Drainage occurring 1 to 2 days after an arthroscopic procedure is not normal, and it should be aggressively treated. Delay in diagnosis can result in sepsis and on a delayed basis, postinfectious arthritis. Both the glenohumeral joint and the subacromial space require debridement and irrigation, followed by antibiotics after both areas are cultured. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213. Settecerri JJ, Pitner MA, Rock MG, Hanssen AD, Cofield RH: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5. Ward WG, Eckardt JJ: Subacromial/subdeltoid bursa abscesses: An overlooked diagnosis. Clin Orthop 1993;288:189-194.
Question 24
Which of the following describes the correct proximal to distal progression of the annular and cruciform pulleys of the digits?
Explanation
The correct progression of the annular and cruciform pulley in the digits is A1, A2, C1, A3, C2, A4, C3. The two cruciform pulleys are collapsible elements adjacent to the more rigid annular pulleys of the flexor tendon sheath. This arrangement enables unrestricted flexion of the proximal interphalangeal joint. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186.
Question 25
High Yield
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of

Explanation
The radiograph shows developmental dysplasia of the hip with the hip reduced and congruent. The treatment of choice is a periacetabular osteotomy because it can improve hip biomechanics and prolong the function of the hip joint. This procedure should be performed prior to the development of severe degenerative changes. Observation will not alter the patient's natural history or the biomechanics of the hip. A total hip arthroplasty should be delayed until severe degenerative changes are present. A Chiari osteotomy is a salvage osteotomy used for a noncongruent subluxated hip. A Pemberton osteotomy requires an open triradiate cartilage; therefore, it is not an option in an adult. Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Question 26
High Yield
A 12-year-old Little League pitcher reports lateral elbow pain and "catching." Examination reveals painful pronation and supination and tenderness over the lateral elbow. Radiographs are shown in Figures 22a and 22b. Initial management should consist of


Explanation
Osteochondritis of the capitellum is a common problem in young throwing athletes and gymnasts. The mechanism of injury involves lateral compression and axial loading of the capitellum. Repetitive trauma causes ischemia with resultant osteochondral necrosis and sometimes eventual separation. Initial management includes rest for a minimum of 6 weeks; occasionally bracing is used. At long-term follow-up, there is typically an observed radiographic abnormality indicating incomplete healing even in asymptomatic patients. Arthroscopy with in situ drilling is reserved for symptomatic lesions that have an intact articular surface. Lesions with partial separation often require fixation. Lateral column osteotomy is a new investigational procedure designed to relieve lateral compression forces and may be used in salvage cases. Kobayashi K, Burton KJ, Rodner C, et al: Lateral compression injuries in the pediatric elbow: Panner's disease and osteochondritis dissecans of the capitellum. J Am Acad Orthop Surg 2004;12:246-254.
Question 27
High Yield
A patient with a cobalt-chromium alloy (Co-Cr) femoral stem has a periprosthetic fracture that is to be fixed with a cable-plate device. The surgeon should make sure that the plate, screws, and cable, respectively, are made of
Explanation
Contact between metals in a biologic environment leads to galvanic corrosion. Reduction potentials of Co-Cr and stainless steel produce the worst combination of metals in commonly used implants. Because the fixation implants are not intended to contact the existing implant, it is not as great a consideration as the plate and the screws and cables that will directly contact each other. Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 119-144.
Question 28
A 35-year-old patient sustained a bimalleolar ankle fracture. What is the most reliable method of predicting a tear of the interosseous membrane?

Explanation
The Weber and Lauge-Hansen fracture classifications suggest that the interosseous membrane (IOM) is torn with certain fracture patterns. In a recent study that evaluated ankle fractures with MRI, Nielson and associates identified 30 patients with IOM tears. Ten of the tears did not correspond with the level of the fibular fracture. The authors concluded that stability of the syndesmosis should not be based on the level of the fibular fracture alone but should also include an intraoperative stress test. Transsyndesmotic fixation should be considered for those fractures where the intraoperative stress test demonstrates instability. A widened medial clear space may occur with a deltoid injury and distal fibular fracture in the absence of a significant tear of the interosseous membrane.
Question 29
High Yield
Which of the following radiographic images is best for detecting anterior acetabular deficiency in the dysplastic hip?

Explanation
The false profile view of Lequesne and de Seze is obtained with the patient standing with the affected hip on the cassette, the ipsilateral foot parallel to the cassette, and the pelvis rotated 65 degrees from the plane of the cassette. This view best assesses anterior coverage of the femoral head. Garbuz DS, Masri BA, Haddad F, et al: Clinical and radiographic assessment the young adult with symptomatic dysplasia. Clin Orthop Relat Res 2004;418:18-22.
Question 30
High Yield
An 18-month-old child with obstetrical palsy has a maximum external rotation as shown in Figure 34. The parents should be advised that without surgical treatment the likelihood that glenoid dysplasia will develop is approximately what percent?

Explanation
Based on the available literature, the probability of development of glenoid dysplasia in the setting of a significant limitation of external rotation is close to 70%. Humeral dysplasia is also likely and can be managed surgically. Efforts are being made to identify procedures that will prevent glenoid dysplasia and help maintain function. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667. Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 31
Which of the following muscles attaches to the coracoid process of the scapula?
Explanation
The insertion of the pectoralis minor is on the base of the coracoid process. The coracoid helps define the interval between the subscapularis and supraspinatus muscles but neither attaches to it. The coracobrachialis and short head of biceps attach to the tip of the coracoid but are not listed as options. The long head of the biceps attaches to the supraglenoid tubercle. The serratus arises from the vertebral border of the scapula. Jobe CM: Anatomy and surgical approaches, in Jobe FW (ed): Operative Techniques in Upper Extremity Sports Injuries. St Louis, MO, Mosby, 1996, pp 140-142.
Question 32
High Yield
Figure 9 shows a cross-sectional view of the spinal cord at the lower cervical level. Injury to the structure indicated by the black arrow will lead to what neurologic deficit?
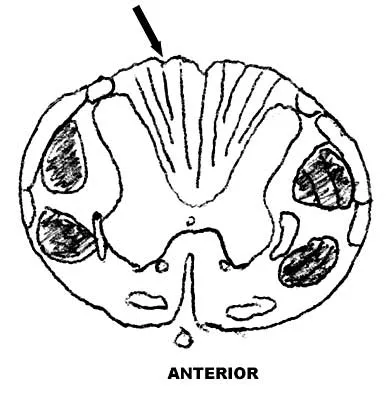
Explanation
The arrow is pointing to the posterior columns of the spinal cord that transmit position sense, vibratory sense, and proprioception. There are no motor tracts in the posterior columns. Bohlman H, Ducker T, Levine A: Spine trauma in adults, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 911.
Question 33
High Yield
What is the primary mechanism of injury for the fracture shown in Figures 33a and 33b?


Detailed Explanation
The radiographs show a triplane fracture of the ankle. In adolescence, closure of the distal tibial physis starts peripherally at the anteromedial aspect of the medial malleolus and extends posteriorly and laterally. The anterolateral quadrant of the physis is the last to close, making this region the most susceptible to separation. When the foot is twisted into external rotation, the anterolateral portion of the epiphysis is avulsed by the pull of the anterior tibiofibular ligament. When this fragment alone is avulsed, the result is a juvenile Tillaux fracture. When the fracture extends to involve the remainder of the physis and posterior metaphysis, as in this patient, the result is a triplane fracture. Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 267-272. Dias LS, Giegerich CR: Fractures of the distal tibial epiphysis in adolescence. J Bone Joint Surg Am 1983;65:438-444.
Question 34
High Yield
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
The acromial branch of the thoracoacromial artery courses along the medial aspect of the coracoacromial ligament and may be encountered when performing an open or arthroscopic subacromial decompression. Bleeding can be controlled by ligation of its branch from the thoracoacromial artery. The other arteries may be injured in other surgical exposures of the shoulder. Esch JC, Baker CL: The shoulder and elbow, in Whipple TL (ed): Arthroscopic Surgery. Philadelphia, PA, JB Lippincott, 1993, pp 65-66.
Question 35
High Yield
Which of the following structures is the most important restraint to posterior subluxation of the glenohumeral joint when positioned in 90 degrees of flexion and internal rotation?
Explanation
The posterior band of the inferior glenohumeral ligament is the most important restraint to posterior subluxation of the glenohumeral ligament with the shoulder in 90 degrees of flexion and internal rotation. With the shoulder in external rotation, the subscapularis is an important stabilizer to posterior subluxation. When the shoulder is in neutral rotation, the coracohumeral ligament is the primary stabilizer. The middle glenohumeral ligament functions primarily to resist anterior translation of the shoulder in the midrange of abduction. The supraspinatus muscle and tendon have relatively little contribution to anterior and posterior translation of the glenohumeral joint. Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML: Posterior glenohumeral subluxation: Active and passive stabilization in a biomechanical model. J Bone Joint Surg Am 1997;79:433-440.
Question 36
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
The patient has an acute peroneal tendon dislocation. The evaluation for syndesmotic injury and lateral ankle instability is negative. The cortical avulsion off the distal tip of the lateral malleolus, a rim fracture, is characteristic of peroneal tendon dislocations. The sensation of apprehension or frank subluxation of the peroneal tendons with active dorsiflexion of the foot while the foot is held in plantar flexion confirms the diagnosis. Based on these findings, initial management should consist of cast immobilization and protected weight bearing. If a recurrent or chronic condition develops, surgery is the most reliable treatment option. Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Question 37
What is the main function of collagen found within articular cartilage?

Explanation
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Question 38
Figure 18a shows the initial lateral radiograph of a 6-year-old girl who sustained a fracture in a motor vehicle accident and was treated in a cast 1 year ago. She now has the valgus deformity seen in Figure 18b. Treatment should consist of


Explanation
Proximal tibial metaphyseal fractures may result in late genu valgum as a result of asymmetric growth of the proximal tibia. These patients are best treated with observation because the deformity is likely to remodel. Osteotomy is not indicated and potentially will lead to recurrence. Stapling of the medial tibial physis is appropriate in patients who have a severe and progressive deformity. Cozen L: Knock-knee deformity in children: Congenital and acquired. Clin Orthop 1990;258:191-203. Jackson DW, Cozen L: Genu valgum as a complication of proximal tibial metaphyseal fractures in children. J Bone Joint Surg Am 1971;53:1571-1578. Brammar TJ, Rooker GD: Remodeling of valgus deformity secondary to proximal metaphyseal fracture of the tibia. Injury 1998;29:558-560. Ogden JA, Ogden DA, Pugh L, et al: Tibia valga after proximal metaphyseal fractures in childhood: A normal biologic response. J Pediatr Orthop 1995;15:489-494.
Question 39
High Yield
What vessel is marked with an asterisk in Figure 44?
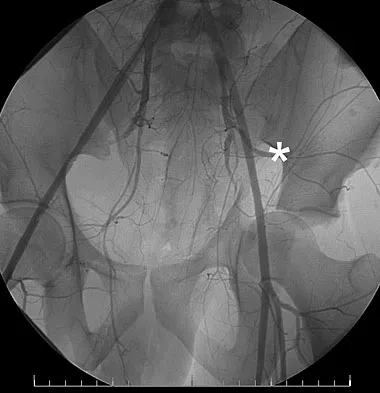
Explanation
The superior gluteal artery is a branch of the posterior division of the internal iliac artery and exits the pelvis through the greater sciatic notch. It can be injured as a result of a pelvic ring fracture or acetabular fracture that has a fracture of the posterior column. Agur AM, Dalley AF (eds): Grant's Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.
Question 40
High Yield
A 62-year-old man has cervical myelopathy with no evidence of cervical radiculopathy. MRI reveals stenosis at C4-5 and C5-6 with severe cord compression. Examination will most likely reveal which of the following findings?

Explanation
Cervical myelopathy involves compression of the spinal cord and presents as an upper motor neuron disorder. Patients commonly have extremity spasticity and problems with ambulation and balance. Hoffman's sign is often present and is elicited by suddenly extending the distal interphalangeal joint of the middle finger; reflexive finger flexion represents a positive finding. The extremities are usually hyperreflexic with myelopathy. With cervical radiculopathy (lower motor neuron disorder), reflexes are hyporeflexic, and patients report pain along a dermatomal distribution. A hyperactive jaw jerk reflex indicates pathology above the foramen magnum or in some cases, systemic disease. Flaccid paraparesis suggests a lower motor neuron problem. Sachs BL: Differential diagnosis of neck pain, arm pain and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 741-742.
Question 41
Which of the following best characterizes bone mineralization?
Explanation
Mineralization occurs at the site of hole zones between the collagen fibrils. Crystals begin from the necessary ions of the lattice that come together with the correct orientation to form the first stable crystal. Formation of this critical nucleus is the most energy-demanding step of crystallization. Enzymes within the extracellular matrix vesicles degrade inhibitors such as adenosine triphosphate, pyrophosphate, and proteoglycans found in the surrounding extracellular matrix. Bone mineral consists of numerous impurities (carbonate, magnesium) that are more soluble, allowing the bone to act as a reservoir for calcium, phosphate, and magnesium ions. Crystals may form by addition of ions or ion clusters to the critical nucleus in many directions, with 'kink' sites forming to branch and exponentially proliferate the crystals. Macromolecules facilitate formation of the critical nucleus and increasing local concentrations of necessary ions. Once the crystals are formed and proliferating, macromolecules bind to the surface and block the growth of the crystal, regulating size, shape, and number of crystals. Lian JB, Stein GS, Canalis E, et al: Bone formation: Osteoblast lineage cells, growth factors, matrix proteins, and the mineralization process, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 14-29.
Question 42
High Yield
A 30-year-old man caught his dominant little finger on the straps of his windsurfing board 10 days ago. He reports swelling about the distal phalanx and has difficulty completely extending the distal interphalangeal joint. A radiograph is shown in Figure 47. What is the most appropriate treatment for this injury?

Detailed Explanation
The radiograph reveals a "bony mallet injury." As the distal phalanx is not volarly subluxated, extension splinting, similar to a classic mallet injury without bony involvement, is appropriate. If there is volar subluxation associated with a large bony fragment, surgical intervention is appropriate. Baratz ME, Schmidt CC, Hughes TB: Extensor tendon injuries, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 192.
Question 43
The strongest biomechanical construct for open reduction and internal fixation of a talar neck fracture uses what interval and entry point?
Explanation
The strongest biomechanical construct is posterior to anterior fixation with the entry point being at the level of the posterolateral tubercle of the talus. This uses the interval between the peroneus brevis and the flexor hallucis longus. The interval between the flexor digitorum longus and the flexor hallucis longus with entry at the posteromedial tubercle of the talus is not an accepted approach for fixation of talar neck fractures. All of the other options use screw placements from anterior to posterior. Swanson TV, Bray TJ, Homes GB Jr: Fractures of the talar neck: A mechanical study of fixation. J Bone Joint Surg Am 1992;74:544-551.
Question 44
High Yield
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique. Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170. Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Question 45
As a baseball player dives to catch a line drive in the outfield, the ball strikes the tip of the player's finger when extended, causing forcible flexion to avulse the extensor tendon from the distal phalanx. Following evaluation and normal radiographic findings, initial management should include
Explanation
Avulsion of the terminal extensor tendon from the distal phalanx (mallet or baseball finger) may or may not be associated with a bony avulsion. The injury is caused by forcible flexion of the DIP joint while catching a ball or hitting an object with the finger extended. Most authorities recommend continuous extension splinting to the DIP joint for 6 weeks, followed by nighttime splinting for an additional 6 weeks. It must be emphasized to the patient that at no time during the initial 6 weeks of treatment should the DIP joint be allowed to fall into flexion or an additional 6 weeks of continuous splinting is required. Miller MD, Cooper DE, Warner JP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 255. Rettig AC: Closed tendon injuries of the hand and wrist in the athlete. Clin Sports Med 1992;11:77-99.
Question 46
A 54-year-old woman sustained an elbow injury 3 months ago that was treated with open reduction and internal fixation. She now reports pain and limited elbow motion. Radiographs are shown in Figures 10a and 10b. Treatment should now consist of


Explanation
Radiographs reveal malunion of a Monteggia fracture-dislocation. Dislocation of the posterior radial head is caused by the malunited ulnar fracture. The deformity includes shortening with an apex posterior angulation. In the acute setting, open reduction of the radial head rarely is necessary; however, in chronic dislocations, open reduction is required. Without ulnar osteotomy, recurrent radial head dislocation is likely.
Question 47
High Yield
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?

Explanation
Symphyseal widening of greater than 2.5 cm and less than 5 cm denotes an AP II injury and a rotationally unstable pelvis. An AP II pelvic ring injury is best treated with anterior open reduction and internal fixation. Nonsurgical management is reserved for AP I injuries. Pelvic binders are used only acutely and should not be used for definitive management. Iliosacral screws usually are not necessary in the acute management of AP II injuries. Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96. Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Question 48
Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
Explanation
Ankle arthrodesis for posttraumatic ankle arthrosis provides reliable pain relief. However, the long-term sequela of joint arthrodesis is the development of arthrosis in the surrounding joints. Over time, following ankle arthrodesis, the ipsilateral hindfoot and midfoot joints show signs of joint space wear, and this may be symptomatic. With a stable ankle arthrodesis, progressive limb-length discrepancy or talar osteonecrosis is not expected. Ankle arthrodesis has not been definitively linked to ipsilateral knee arthritis or contralateral ankle arthritis. Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Question 49
High Yield
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause

Detailed Explanation
If the Buford complex is mistakenly reattached to the neck of the glenoid, severe painful restriction of external rotation will occur. Williams MM, Snyder SJ, Buford D Jr: The Buford complex - the "cord-like" middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 50
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of

Explanation
For the patient with an anterior sternoclavicular dislocation, the most appropriate initial treatment should be symptomatic. Surgical options are usually contraindicated because the incidence of intraoperative and postoperative complications is high. A deformity from an anterior sternoclavicular dislocation is usually well tolerated. Return to play is allowed when symptoms resolve. Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 477-525.
Question 51
High Yield
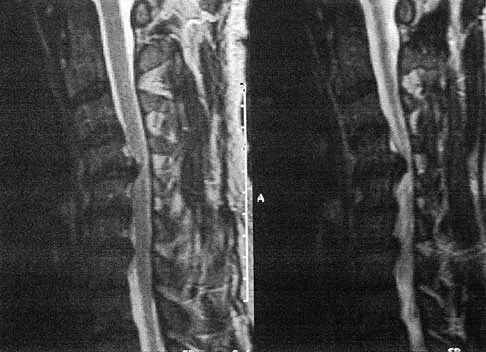
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?


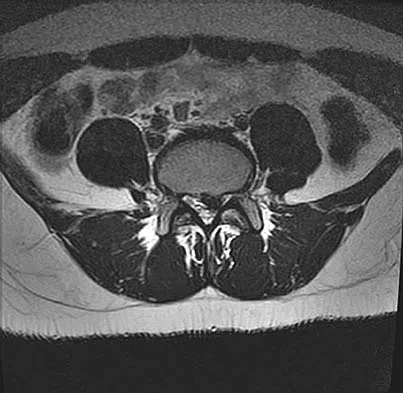
Explanation
The MRI scans clearly show an extruded L4-5 disk that is affecting the L5 nerve root on the left side. In addition, the L5 nerve root has a cutaneous distribution in the first dorsal web space. S1 affects the lateral foot. L4 affects the medial calf.
Question 52
High Yield
A 20-year-old man reports painless snapping about the lateral aspect of the right hip. He denies any history of trauma. Examination reveals no limp or tenderness. Hip range of motion is full, and there is good strength. Radiographs are normal. What anatomic structure is most likely causing these symptoms?
Explanation
Coxa saltans (snapping hip syndrome) can occur in two forms: external/lateral or interior/medial/anterior. This patient has the external/lateral form. The external/lateral form involves the iliotibial band, tensor fascia, or gluteus medius, which snaps over the greater trochanter. The external form usually can be treated with physical therapy alone; however, several recent studies report satisfactory results with surgical treatment. Faraj and associates reported good results from surgical Z-plasty in a series of 10 patients. White and associates reported good results in a series of 16 patients with 17 hips who underwent surgical release of an external snapping hip. The interior/medial/anterior form can involve the iliopsoas tendon, acetabular labrum, subluxation of the hip, and loose bodies. White RA, Hughes MS, Burd T, et al: A new operative approach in the correction of external coxa saltans: The snapping hip. Am J Sports Med 2004;32:1504-1508. Faraj AA, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Question 53
High Yield
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the

Explanation
The area indicated by the arrow represents gadolinium contrast extending into a separation between the lateral labrum and its acetabular attachment. This can be a traumatic detachment, but occasionally a cleft may be present as a normal variant of the labral morphology. The capsular attachment of the iliofemoral ligament is peripheral to the labrum. The pulvinar is the common name applied to the fat and overlying synovium contained within the acetabular fossa above the ligamentum teres. The zona orbicularis is a circumferential thickening of the capsule around the femoral neck, and the retinacular vessels travel within the capsular synovium up the femoral neck to supply the femoral head. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235. Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Question 54
High Yield
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?

Explanation
The axillary nerve lies within millimeters of the anterior inferior capsule. The inferior capsule is of varying thickness, and thermal energy used in shortening the ligament can cause damage to the sensory fibers of the axillary nerve. Clinically, this is manifested as a burnt skin sensation in the axillary nerve distribution area. The motor branch of the axillary nerve is usually spared. The suprascapular nerve and the radial nerve are far from the shrinkage zone. The musculocutaneous nerve, frequently at risk with open procedures, lies well anterior. Fanton GS: Arthroscopic electrothermal surgery of the shoulder. Op Tech Sports Med 1998;6:157-160.
Question 55
The spread of malignant cells to the vertebrae is often through
Explanation
In 1940, Batson described a valveless plexus of veins that extend from the dural venous sinuses of the skull to the sacrum. This system permits retrograde blood flow and enables tumor cells to enter vertebral bodies at multiple levels. Increased intra-abdominal pressure will enhance this retrograde blood flow.
Question 56
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in

Explanation
The elbow dislocates by a three-dimensional movement of supination and valgus during flexion. Additional trauma during reduction is minimized by recreating the deformity and reducing the elbow in supination. The actual maneuver includes full supination (actually hypersupination) of the elbow in a valgus position. This is followed by pushing the olecranon distally in line with the long axis of the ulna while swinging the elbow into varus, and then relaxing the supination torque. Postreduction stability is enhanced in pronation, except when the soft-tissue disruption is extensive. O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 414.
Question 57
A 65-year-old man has a painful mass of the middle finger. A clinical photograph, lateral radiograph, coronal MRI scan, and biopsy specimen are seen in Figures 20a through 20d. What is the most likely diagnosis?




Explanation
Although the degeneration of an isolated benign cartilaginous lesion into a chondrosarcoma is rare, it occurs in roughly 10% of patients with Ollier's disease. Pain is the most common symptom of chondrosarcoma. The treatment of low-grade chondrosarcoma ranges from intralesional excision to wide amputation. The intent of the surgery is to remove all the disease to decrease the chance of local recurrence. Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Question 58
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?

Explanation
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Question 59
High Yield
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
Several studies have identified a complete proximal avulsion of the hamstring muscles as an injury that leads to significant long-term disability, with a high percentage of athletes who must permanently restrict their activities following nonsurgical management. Early surgical repair and prolonged rehabilitation have yielded consistently better results than nonsurgical management. Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Question 60
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Explanation
Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.
Question 61
A 12-year-old boy sustained a grade III open tibial fracture 1 week ago and underwent multiple debridements and fracture fixation. He now has a soft-tissue defect that measures 6 cm x 6 cm, with an area of exposed bone and muscle on the distal medial leg that is a few centimeters proximal to the ankle. Management of the soft-tissue defect should now consist of

Explanation
The soft-tissue defect is in a very difficult position - the distal tibia. The defect is too distal for a gastrocnemius flap, and the exposed bone precludes an immediate skin graft. A free flap and skin graft would be required for closure. VAC is very effective in soft-tissue defects such as this one. Healthy granulation tissues form quickly. VAC can be the definitive treatment, or it can be used before skin grafting. Wet-to-dry dressings could promote granulation, but the process is hastened substantially by VAC. Amputation is not a consideration because there are no signs of infection or fracture healing problems at this time. Mooney JF III, Argenta LC, Marks MW, et al: Treatment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Orthop 2000;376:26-31.
Question 62
An 20-year-old elite college football player has ecchymosis, swelling, and pain on the lateral side of his foot after a game. Radiographs are shown in Figures 31a through 31c. Management should consist of



Explanation
Metaphyseal-diaphyseal junction fractures of the fifth metatarsal require careful evaluation. In athletes, early intervention with a 4.5-mm intramedullary screw correlates with an earlier return to activity. One study examining the failure of surgically managed Jones fractures revealed that use of anything other than a 4.5-mm malleolar screw for internal fixation correlated with failure. Glasgow MT, Naranja RJ Jr, Glasgow SG, et al: Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: The Jones fracture. Foot Ankle Int 1996;17:449-457.
Question 63
High Yield
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of
Detailed Explanation
Mild scoliosis is not a painful condition, but it usually presents during adolescence. Intermittent back pain is reported by 25% to 30% of adolescents whether or not scoliosis is present. Such pain is often attributed to muscle strain from tight muscles, poor posture, or heavy school backpacks. The clinician must distinguish typical pain (mild, intermittent, nonlimiting) from atypical pain. The latter requires more careful examination and imaging studies (bone scan or MRI) to determine the source of pain. The patient's age and right thoracic curve pattern are typical for idiopathic scoliosis; therefore, imaging of the neuroaxis is not necessary to look for cord syrinx, tethering, or tumor. Brace treatment is not required for this small curve unless future progression is demonstrated. Ramirez N, Johnston CE, Browne RH: The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am 1997;79:364-368. Hollingworth P: Back pain in children. Br J Rheum 1996;35:1022-1028.
Question 64
High Yield
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
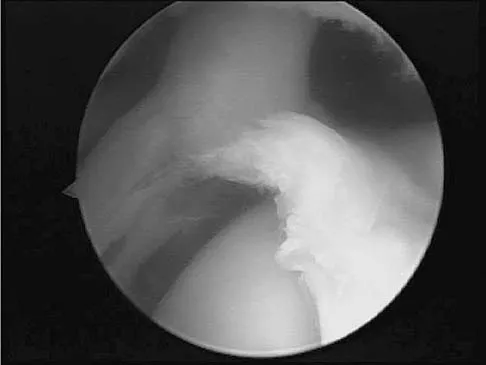
Explanation
According to Morgan and associates, a type II SLAP lesion can create or is associated with a superior instability pattern. They suggest that this can exist without a co-existing anteroinferior instability pattern. They reported that repair of the SLAP lesion alone resulted in satisfactory outcomes in 90% of patients and a return to throwing in more than 90% of pitchers. The arthroscopic findings in this patient do not support a diagnosis of anteroinferior laxity or instability; therefore, thermal capsular shift or capsular placation is not necessary. Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565. Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Question 65
A 3-year-old boy with severe cerebral palsy is unable to sit independently and does not crawl. Examination reveals a 40-degree hip flexion contracture by the Thomas test and 25 degrees of passive abduction. A radiograph of the pelvis shows subluxation of both hips, with a migration index of 30%. Management should consist of
Explanation
Progressive hip subluxation occurs in up to 50% of children with spastic quadriparesis. The subluxation is the result of chronic muscle hypertonicity, especially in the adductor muscle group. In time, the constant muscle tension will lead to dislocation, dysplastic changes in the acetabulum, and erosive changes in the cartilage of the femoral head. Many of these children will experience pain. Two recent studies have shown that early soft-tissue releases can successfully prevent progressive subluxation in children who are younger than age 4 years and who have a Reimers index (migration index) of less than 40%. Botulinum toxin A injections may reduce tone in the adductors for 4 to 6 months, but it is difficult to inject into the iliopsoas. Additionally, there are no long-term studies documenting the efficacy of botulinum toxin A to treat progressive hip subluxation in patients who have spastic quadriparesis. In general, proximal femoral osteotomy, combined with soft-tissue release as necessary, is indicated in older children (older than age 4 years) with progressive subluxation. Although selective dorsal rhizotomy has been used in nonambulatory patients, outcomes are less well documented than in ambulatory patients. There are no studies documenting the effect of selective dorsal rhizotomy on progressive hip subluxation in nonambulatory children. Miller F, Cardoso Dias R, Dabney KW, et al: Soft-tissue release for spastic hip subluxation in cerebral palsy. J Pediatr Orthop 1997;17:571-584.
Question 66
High Yield
What region of the spine is most susceptible to changes in the vascular supply to the spinal cord during an anterior approach?
Explanation
The thoracic spinal cord is characterized by a variable and, at times, complicated blood supply. The artery of Adamkiewicz, also known as the great anterior medullary artery, most typically arises off the left side of the aorta between T8 and T12. It represents the sole medullary blood supply to the thoracic spine. When this artery is divided or injured, the blood supply to the thoracic cord may be interrupted. It is important to avoid electocautery of blood vessels within or near the thoracic foramen because this is a site of important, albeit limited, collateral circulation. Sharma M, Anderson FC: Spinal vascular lesions, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 301-306.
Question 67
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
The PCL is a nonisometric structure with nonuniform tension during knee motion, with maximum tension at 90 degrees of flexion. While the posteromedial PCL fibers have been found to be the most isometric, the anterolateral fibers represent the bulk of the ligament. Studies have suggested that anterior placement of the femoral tunnel is superior to placement in an isometric position. The anterolateral bundle tightens as the knee flexes; therefore, it is optimal to tension the graft at 90 degrees of flexion. Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Question 68
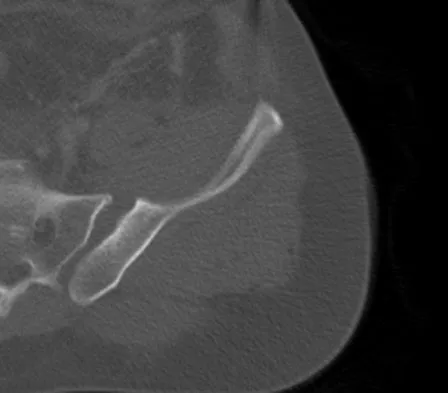
A 14-year-old boy sustained a femoral neck fracture in a fall from a tree and underwent open reduction and internal fixation 6 months ago. Follow-up examination now reveals an antalgic Trendelenburg gait and painful range of motion. A radiograph is shown in Figure 23, and a CT scan shows a nonunion. Treatment should consist of

Explanation
The coxa vara deformity and fracture nonunion should be treated simultaneously; therefore, the treatment of choice is curettage of the nonunion, intertrochanteric valgus osteotomy, and revision internal fixation. In addition, valgus osteotomy will convert the shear forces across the nonunion to compression, aiding in healing of the nonunion. None of the other procedures addresses both issues, and hip fusion is inappropriate under these conditions. Lam SF: Fractures of the neck of the femur in children. J Bone Joint Surg Am 1971;53:1165-1179.
Question 69
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 70
High Yield
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?

Explanation
The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 71
High Yield
An 18-year-old man has had an enlarging mass in his hand for the past 3 months. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 54a through 54d. What is the most likely diagnosis?

Explanation
Also known as Nora's lesion, BPOP is a benign osteocartilaginous tumor that almost always occurs in the hands and feet; one occurrence each in the femur and tibia has been reported. Although local recurrence is common after excision, metastases have not been reported. Abramovici L, Steiner GC: Bizarre parosteal osteochondromatous proliferation (Nora's lesion): A retrospective study of 12 cases, 2 arising in long bones. Hum Pathol 2002;33:1205-1210.
Question 72
The arrows in the axial T1-weighted MRI scan shown in Figure 25 show which of the following structures?

Explanation
The arrows in the figure show the deep branch of the ulnar nerve (more radial) and the superficial branch of the ulnar nerve within Guyon's canal. Guyon's canal is approximately 4 cm long beginning at the proximal extent of the transverse carpal ligament and ends at the aponeurotic arch of the hypothenar muscles. Many structures comprise the boundaries of Guyon's canal. The floor, for example, consists of the transverse carpal ligament, the pisohamate and pisometacarpal ligaments, and the opponens digiti minimi. Within Guyon's canal, the ulnar nerve bifurcates into the superficial and deep branches. The ulnar artery is immediately adjacent and radial to the ulnar nerve. The median nerve is visualized within the carpal tunnel, and the palmar cutaneous branch is more radial to Guyon's canal and volar to the carpal tunnel. The radial and ulnar digital nerves to the little finger are branches off of the superficial branch of the ulnar nerve distal to its emergence from Guyon's canal. The ulnar artery is the round structure located radial to the branches of the ulnar nerve within Guyon's canal. Adjacent to the ulnar artery are two small veins. The dorsal cutaneous branch of the ulnar nerve branches from the ulnar nerve in the distal forearm, well proximal to Guyon's canal. The common digital artery to the fourth web branches from the superficial palmar arch distal to Guyon's canal. The hook of the hamate is clearly seen in the figure, orienting the observer to the ulnar side of the wrist. Gross MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop Relat Res 1985;196:238-247.
Question 73
High Yield
Passive glycation of articular cartilage results in
Detailed Explanation
Passive glycation of articular cartilage occurs over decades. One of the consequences of this glycation appears to be the stiffening of collagen. This phenomenon appears to be associated with an increased collagen degradation and development of osteoarthrosis. Passive glycation also results in a relatively yellow appearance. Passive glycation does not directly influence chondrocyte proliferation. DeGroot J, Verzijl N, Wenting-van Wijk MJ, et al: Accumulation of advanced glycation end products as a molecular mechanism for aging as a risk factor in osteoarthritis. Arthritis Rheum 2004;50:1207-1215.
Question 74
Figures 4a through 4c show the clinical photographs and radiographs of a 12-month-old boy who has progressive difficulty wearing shoes because of the length of the second toe, as well as width of the forefoot. Management should consist of



Explanation
The patient has macrodactyly involving the second ray, with significant enlargement of the width and height of the foot. The radiographs show widening of the interval between the first and second metatarsal and between the second and third metatarsal. With this degree of involvement, amputation of the second ray with excision of the overgrowth of affected soft tissue provides the most consistent desired reduction in foot size. A threaded Steinmann pin should be inserted across the remaining metatarsals until healing has occurred. Patients with macrodactyly should be examined to exclude neurofibromatosis type 1 and Klippel-Trenaunay-Weber syndrome.
Question 75
High Yield
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?

Explanation
Eighty percent of giant cell tumors occur in patients older than age 20 years, with the peak incidence in the third decade of life. Most of these tumors are eccentrically located and epiphyseal in location. They are lytic in nature as in this patient. Although named for the hallmarked multinucleated giant cells seen in the lesion, the basic cell type is the spindle-shaped stromal cell. Chondroblastoma is highly cellular and contains large multinucleated giant cells with intercellular chondroid material, some of which is calcified. Chondromyxoid fibroma has chondroid tissue separated by strands of more cellular tissue with occasional multinucleated giant cells. Desmoplastic fibroma is characterized by poorly cellular fibrous tissue, and lymphoma is highly cellular with characteristic round cells. Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Question 76
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of

Explanation
The MRI scan reveals a partial patellar tendon rupture in conjunction with chronic patellar tendinitis. Mild and moderate patellar tendinitis may be treated nonsurgically with rest, stretching, strengthening, and anti-inflammatory drugs. Severe tendinopathy or extensor mechanism disruption is best treated surgically with tendon debridement and repair. Al-Duri ZA, Aichroth PM: Surgical aspects of patella tendonitis: Techniques and results. Am J Knee Surg 2001;14:43-50.
Question 77
High Yield
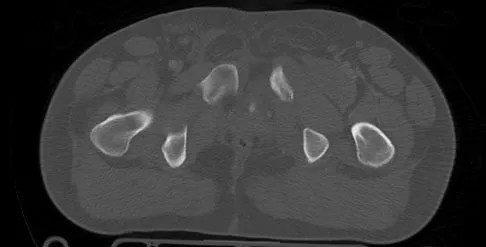
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include

Explanation
The patient has severe acetabular protrusio, a condition that is frequently associated with Marfan syndrome. An echocardiogram is necessary to rule out the most serious consequence of this syndrome, aortic root widening, which can lead to aortic valve dysfunction or fatal aortic rupture. An electromyogram may be indicated for Charcot-Marie-Tooth disease, which is associated with acetabular dysplasia, but not protrusio. The renal ultrasound, the MRI scan, and the biopsy would be of no value in this patient. Protrusio can also be seen in patients with osteogenesis imperfecta and juvenile rheumatoid arthritis. Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Question 78
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
Two recent studies by Pollak and associates and Marsh and associates have focused on function after high-energy tibial plafond fractures. Findings are unfavorable even when anatomic reduction is performed in the best centers and patients are provided excellent rehabilitation. Function improves up to 2 years after injury, but even basic walking skills remain adversely affected. Virtually all patients have long-term adverse general health effects compared to their gender and age-matched peers. Posttraumatic degenerative arthritis is present in most ankles. Patients should be told early about the long-term prognosis, and early vocational/psychological counseling should be given. Despite these adverse outcomes, only a minority of patients require fusion or arthroplasty. Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 79
Which of the following bearing materials is most resistant to scratching from third-body debris?
Explanation
Alumina is the hardest of all the materials listed. Clinical retrieval demonstrates resistance to scratching from third-body debris.
Question 80
A patient who underwent closed reduction of the hips as an infant now reports pain. An abduction internal rotation view shows an incongruous joint. Based on the findings shown in Figure 3, what is the most appropriate type of pelvic osteotomy for the right hip?

Explanation
Pelvic osteotomies that redirect hyaline cartilage over the femoral head offer the potential for long-term preservation of the hip; however, salvage procedures such as the Chiari osteotomy are indicated in patients without a concentrically reducible hip. Ito and associates reported that moderate dysplasia and moderate subluxation without complete obliteration of the joint space and a preoperative center-edge angle of at least minus 10 degrees are desirable selection criteria. Ohashi H, Hirohashi K, Yamano Y: Factors influencing the outcome of Chiari pelvic osteotomy: A long-term follow-up. J Bone Joint Surg Br 2000;82:517-525.
Question 81
High Yield
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 82
High Yield
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?

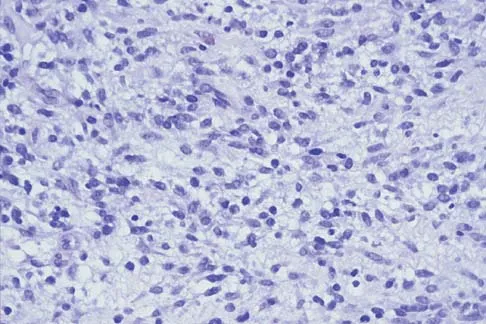
Explanation
The patient has infantile fibrosarcoma. For unresectable lesions, the treatment of choice is chemotherapy with vincristine, actinomycin-D, and cyclophosphamide, followed by excision if there is an adequate decrease in the size of the lesion.
Question 83
High Yield
The posterior horn of the medial meniscus receives its primary blood supply from what artery?
Explanation
The middle genicular artery supplies the posterior capsule and intracapsular structures (anterior cruciate ligament, posterior cruciate ligament, posterior horns of the meniscus). The medial and lateral inferior geniculates anastomose anteriorly to form a capillary network to supply the fat pad, synovial cavity, and patellar tendon. The lateral superior and inferior genicular arteries supply the lateral retinaculum. Insall J, Scott WN: Anatomy, in Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, pp 64-70.
Question 84
A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?
Explanation
Anteromedial displacement of the tibial tubercle unloads the distal and lateral facets of the patella and shifts the forces to the proximal and medial facets. Therefore, if findings indicate arthrosis predominately in the medial and proximal areas of the patella, this is considered a relative contraindication because it may accentuate arthritic symptoms. Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop 1983;177:176-181. Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a subluxation-type patellar malalignment. Am J Sports Med 1997;25:375-381.
Question 85
Figure 12 shows the radiograph of an 80-year-old woman who has had an 8-month history of back pain after a fall. What is the most likely diagnosis based on the radiographic findings at the fractured vertebrae?

Explanation
An intravertebral vacuum cleft suggests nonunion of the vertebral fracture with osteonecrosis and is not seen in routine healing fractures. MRI characteristically shows a high T2 signal in the cleft. The cleft is not indicative of an infectious or neoplastic lesion. A vacuum disk phenomenon is associated with end-stage degenerative disk disease, but those findings are not found in the vertebral body. Murakami H, Kawahara N, Gabata T, et al: Vertebral body osteonecrosis without vertebral collapse. Spine 2003;28:E323-E328.
Question 86
Figure 28 shows the postoperative radiograph of a 36-year-old patient. The cerclage cable was placed for a minimal medial calcar fracture seen during femoral preparation. In the immediate postoperative period, what is the highest level of activity that would be safely permitted?

Explanation
The incidence of femoral fracture in primary cementless total hip arthroplasty ranges from 1.5% to 27.8%. It is imperative that the implant and fracture are stable both intraoperatively and postoperatively. Cerclage wiring or cerclage cabling is the current recommended treatment for nondisplaced calcar fractures and minimally displaced proximal fractures. Berend and associates reviewed the results of 58 total hips in 55 patients with intraoperative calcar fracture managed with single or multiple cerclage wires or cables and immediate full weight bearing. Follow-up averaged 7.5 years, and there were no revisions of the femoral component. No patients had severe thigh pain. Berend KR, Lombardi AV Jr, Mallory TH, et al: Cerclage wires or cables for the management of intraoperative fracture associated with a cementless, tapered femoral prosthesis: Results at 2 to 16 years. J Arthroplasty 2004;19:17-21. Schmidt AH, Kyle RF: Periprosthetic fractures of the femur. Orthop Clin North Am 2002;33:143-152.
Question 87
High Yield
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of


Explanation
The patient has a displaced femoral neck fracture. Although the treatment remains controversial, most clinicians advocate either a closed or open reduction in younger active patients. Achieving an anatomic reduction is necessary to avoid loss of reduction, nonunion, or osteonecrosis. An acceptable reduction may have up to 15 degrees of valgus angulation and 10 degrees of posterior angulation. Parallel multiple screws or pins are the most common method of internal fixation. Prosthetic replacement is generally reserved for older and less active individuals. Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Question 88
High Yield
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of



Detailed Explanation
The patient has a chronic unrecognized volar lunate dislocation. Median nerve compression is the result of the lunate displaced into the carpal tunnel. The diagnosis can be made by radiographs; MRI is not necessary. A volar approach allows median nerve decompression with excision of the lunate, whereas a dorsal approach facilitates excision of the scaphoid and triquetrum. Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Question 89
A 36-year-old woman sustained a tarsometatarsal joint fracture-dislocation in a motor vehicle accident. The patient is treated with open reduction and internal fixation. What is the most common complication?

Explanation
The most common complication associated with tarsometatarsal joint injury is posttraumatic arthritis. In one series, symptomatic arthritis developed in 25% of the patients and half of those went on to fusion. In another series, 26% had painful arthritis. Initial treatment should consist of shoe modification, inserts, and anti-inflammatory drugs. Fusion is reserved for failure of nonsurgical management. Hardware failure may occur, but it is clinically unimportant. Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618. Arntz CT, Veith RG, Hansen ST Jr: Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am 1988;70:173-181.
Question 90
High Yield
A 10-year-old child reports acute leg pain after wrestling with his brother. AP and lateral radiographs are shown in Figures 21a and 21b. What is the best course of action?


Explanation
The radiographs show an eccentric metaphyseal lesion with a well-defined reactive rim of bone that is consistent with a nonossifying fibroma. Pathologic fractures through benign lesions should be treated as appropriate for the fracture, allowing the fracture to heal. Biopsy is not needed when the radiographic diagnosis is benign. MRI, in the presence of a fracture, is not particularly helpful because of the hematoma. If radiographic findings reveal that the lesion appears aggressive, a biopsy should be performed, obtaining tissue away from the fracture site. Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377.
Question 91
Which of the following nerves travels with the deep palmar arch?

Explanation
The ulnar nerve divides alongside the pisiform, and the deep branch supplies the three hypothenar muscles and crosses the palm with the deep palmar arch to supply the two ulnar lumbricals, all interossei, and finally the adductor pollicis. The superficial branch supplies the ulnar digital branches to the small and ring fingers. The median nerve branches are more superficial in the palm near the superficial palmar arch. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Question 92
High Yield
Which of the following anatomic structures is labeled 6 in Figure 27?
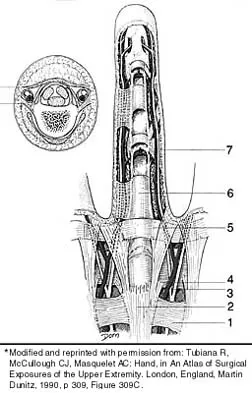
Explanation
The line labeled 6 points to the A2 pulley. This structure is the condensation of the digital flexor tendon sheath corresponding to the proximal aspect of the proximal phalanx. Grayson's ligament is volar to the digital nerve and artery. Cleland's ligament is dorsal to the digital nerve and artery. The sagittal band anchors the extensor tendons over the metacarpophalangeal joints. The triangular ligament connects the lateral bands just proximal to the terminal tendon inserting onto the base of the distal phalanx. Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, p 467.
Question 93
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
In Charcot-Marie-Tooth disease, the posterior tibialis and peroneus longus tendons remain strong, serving to invert the hindfoot and depress the first metatarsal head thus causing the cavovarus foot associated with this disease. In contrast, the tibialis anterior and peroneus brevis are less functional and therefore cannot dorsiflex the ankle, elevate the first metatarsal, or evert the foot, contributing to the deformity.
Question 94
Preservation or reconstruction of which of the following structures is essential to minimize the risk of hallux valgus developing after removal of part or all of the medial sesamoid?
Explanation
Complications of medial sesamoidectomy include stiffness, claw toe, and hallux valgus. Each sesamoid sits within its respective head of the flexor hallucis brevis tendon. Excision of one sesamoid can result in slack in its flexor hallucis brevis tendon; therefore, it is imperative to preserve or repair the flexor hallucis brevis tendon when removing the medial sesamoid. Dedmond BT, Cory JW, McBryde A Jr: The hallucal sesamoid complex. J Am Acad Orthop Surg 2006;14:745-753.
Question 95
Which of the following best describes the course of the ulnar nerve in the midforearm?

Explanation
In the midforearm, the ulnar nerve travels deep to the flexor carpi ulnaris muscle and ulnar to the ulnar artery as it lies on the flexor digitorum profundus muscle. In this region, the ulnar nerve and artery lie side-by-side, whereas more proximal in the forearm, the ulnar artery originates from the brachial artery in the antecubital fossa, and the ulnar nerve lies within the cubital tunnel. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 96
High Yield
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
Alternative bearing surfaces in THA have received much attention in recent years as more and more hip arthroplasties are being performed on younger patients with hip arthritis. The two most popular nonmetal-on-polyethylene bearing surfaces are metal-on-metal and ceramic-on-ceramic. There are arguments supporting the use of either, but ceramic bearings have been shown to have a theoretic increased risk of fracture compared with cobalt-chromium. This has been shown to be clinically relevant with zirconium ceramics. Newer alumina ceramics are being produced with lower porosity and grain size and with higher density and purity, resulting in lower fracture risk but still greater than that of cobalt-chromium. Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
Question 97
Which of the following clinical findings is commonly associated with symptomatic partial-thickness rotator cuff tears?
Explanation
In symptomatic partial-thickness rotator cuff tears, a painful arc with active range of motion is common, impingement signs are usually positive, and the lift-off test is normal. Active and passive range of motion measurements are often equal, although active range of motion can be painful. External rotation lag signs are often seen with larger full-thickness tears. Hertel R, Ballmer FT, Lambert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313. McConville OR, Iannotti JP: Partial thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 98
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?

Explanation
In an article in the Journal of Shoulder and Elbow, 431 total shoulder arthroplasties were performed with a cemented all-polyethylene glenoid component between 1990 and 2000. Follow-up averaged 4.2 years. In total, 53 surgical complications occurred in 53 patients (12%). Of these, 32 were major complications (7.4%), with 17 of these requiring reoperation. Index complications in order of frequency included rotator cuff tearing, postoperative glenohumeral instability, and periprosthetic humeral fracture. Notably, glenoid and humeral component loosening requiring reoperation occurred in only one shoulder. Data from the contemporary patient group suggest that there are fewer complications of shoulder arthroplasty and less need for reoperation. Especially striking is the near absence of component revision because of loosening or other mechanical factors. Complications involving the brachial plexus have been reported following total shoulder arthroplasty but are not as common of a cause for failure. Chin PY, Sperling JW, Cofield RH, et al: Complications of total shoulder arthroplasty: Are they fewer or different? J Shoulder Elbow Surg 2006;15:19-22.
Question 99
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?


Explanation
The MRI scans reveal a meso os acromiale with edema at the site in a skeletally mature patient. Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, p 23.
Question 100
A 7-year-old girl with spinal muscular atrophy (SMA) type II has popping of the left hip. Examination reveals painless subluxation of the joint in adduction with palpable reduction in abduction. Radiographs show coxa valga, subluxation of the left hip, and pelvic obliquity with elevation of the left hemipelvis. Treatment should consist of

Explanation
Observation is the treatment of choice. Hip subluxation and dislocation are not uncommon in patients with SMA type II who are unlikely to be ambulatory. Scoliosis occurs in these patients 100% of the time and frequently creates pelvic obliquity. However, in long-term follow-up, patients with SMA type II and hip dislocations had little associated pain or functional limitations because of hip instability. In addition, recurrent hip subluxation after surgical treatment has been documented. Given the rarity of symptoms from hip instability in long-term follow-up, and the possibility of recurrent dislocation, surgical intervention for hip instability may expose SMA type II patients to undue surgical risk for minimal if any functional gain. Sporer SM, Smith BG: Hip dislocation in patients with spinal muscular atrophy. J Pediatr Orthop 2003;23:10-14.
