Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show


Explanation
The patient has a slipped capital femoral epiphysis (SCFE) at a younger than average age (average age 13.5 years for boys and 12.0 years for girls); therefore, an etiology that is not idiopathic must be considered. Hypothyroidism can result in a SCFE, but these children typically fall into the category of less than the 10th percentile for height. SCFE may develop in children with a growth hormone deficiency who have undergone hormonal replacement. Osteodystrophy caused by chronic renal failure may result in a SCFE, but the bone quality is markedly osteopenic on radiographs and the children are chronically ill with both low height and weight percentiles. An elevated estrogen level results in physeal closure and is protective to physeal slippage. Therefore, this child will most likely have normal laboratory values. Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Question 2
High Yield
An axillary nerve lesion may cause weakness in the deltoid and the
Detailed Explanation
While the most prominent functional deficit from axillary nerve lesions occurs from denervation of the deltoid, denervation of the teres minor also occurs.
Question 3
A young active patient with a complete isolated posterior cruciate ligament (PCL) tear undergoes a double bundle PCL reconstruction. The tensioning pattern of the anterolateral (AL) and posteromedial (PM) bundles most likely to reproduce the most normal knee kinematics would be to tension
Explanation
During flexion and extension of the normal knee, the AL bundle of the PCL is taut in flexion, and the PM bundle is taut when the knee is near extension. The AL bundle is approximately two times larger at its midsubstance, stiffer, and has a higher ultimate load than the PM bundle. In vitro testing has demonstrated that by tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 0 degrees of flexion, essentially normal knee kinematics are restored. Tensioning the AL bundle at 45 degrees of flexion and the PM bundle at 0 degrees of flexion would result in increased laxity with flexion at 90+ degrees. Tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 45 degrees of flexion would result in increased laxity near extension. Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin T, Woo SL: Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 2000;28:144-151.
Question 4
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and 49b, respectively. Which of the following best explains the 8-week postinjury clinical findings seen in Figure 49c?



Explanation
Patients older than age 40 years at the time of initial anterior dislocation have low rates of redislocation; however, 15% of these patients experience a rotator cuff tear. Moreover, there is a dramatic increase (up to 40%) in the incidence of rotator cuff tears in patients older than age 60 years. Axillary nerve injury may occur but is less common than rotator cuff tear. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 273-284.
Question 5
A 58-year-old woman who underwent a successful total hip replacement for degenerative arthritis 8 years ago reports groin pain for the past 6 months. A radiograph of the hip is shown in Figure 32. At revision, severe deficiency of the posterior column is noted. What reconstructive option would be most appropriate for the acetabulum?

Explanation
The radiograph shows medial migration of the cementless acetabular component, strongly suggesting acetabular discontinuity with a combined segmental and cavitary medial deficiency. The treatment of choice is a morcellized or structural graft, supported with a reconstructive cage bridging the pelvic discontinuity, and a cemented cup. Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Question 6
Figures 50a and 50b show the standing clinical photographs of a 12-year-old boy who has had increasing pain in the left foot for the past 9 months. He reports that the pain is activity related, aching in nature, and localized to the medial aspect of the midfoot and hindfoot. History reveals that he sustained a puncture wound located superior and posterior to the medial malleolus from a plate glass window 18 months ago. Examination reveals no restriction of ankle or subtalar motion, normal neurovascular status, no masses, and a well-healed 1.5-cm laceration posterior to the superior aspect of the medial malleolus. Inversion strength of the foot is decreased to grade 3/5. Radiographs of the foot show no bony abnormalities. Treatment should consist of


Explanation
The photographs show a planovalgus posture of the foot. The foot deformity and decreased inversion strength are secondary to laceration of the posterior tibial tendon 18 months ago. If the injury had been recognized acutely, optimal treatment would have consisted of repair of the tendon; however, contracture now precludes that possibility. Therefore, transfer of the flexor digitorum longus or flexor hallucis longus is the preferred treatment. In adults with posterior tibial dysfunction, the entire tendon is typically degenerated and the transfer must be anchored through a drill hole in the navicular. In this patient, the distal end of the posterior tibial tendon is a satisfactory insertion site. Lengthening osteotomy of the calcaneus could be combined with the tendon transfer if the patient had a fixed deformity of the foot. UCBL orthoses and an ankle-foot orthosis are not considered good long-term solutions for a 12-year-old patient. Mosca VS: Flexible flatfoot and skewfoot, in Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 355-376.
Question 7
High Yield
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
Peak embolization is observed during femoral stem insertion. Embolization is also observed during acetabular preparation and hip reduction. Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.
Question 8
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the

Explanation
The sciatic nerve is formed by the roots of the lumbosacral plexus. It exits the pelvis through the greater sciatic notch and appears in the buttock anterior to the piriformus. From that point, the sciatic nerve passes posteriorly over the superior gemellus, obturator internus, inferior gemellus, and quadratus femoris before it passes deep to the biceps femoris. The tendon of the obturator internus passes through the lesser sciatic notch. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 347. Anderson JE: Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-34, 4-36.
Question 9
In a patient with a soft-tissue sarcoma treated by wide excision and radiation therapy, the risk of subsequent fracture is probably most influenced by

Explanation
While most pathologic fractures are in the lower extremity in patients treated for soft-tissue sarcomas by wide excision and adjuvant radiation therapy, risk factors for such fractures are bone resection associated with excision of the tumor and soft-tissue sarcomas of the thigh that require periosteal stripping at the time of resection. Such fractures can occur late, often more than 6 months after surgery, are difficult to treat, and often result in nonunion. Bell RS, O'Sullivan B, Nguyen C, et al: Fractures following limb-salvage surgery and adjuvant irradation for soft-tissue sarcoma. Clin Orthop 1991;271:265-271.
Question 10
High Yield
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed

Explanation
Very large corrections of tibial deformity can be achieved at or just below the tibial tubercle. This level of osteotomy maintains the relationship between the tubercle and the rest of the joint, does not alter patellofemoral mechanics, and avoids complicating possible future conversion to total knee arthroplasty. High tibial osteotomy is contraindicated for large corrections because of excessive elevation of the tibial tubercle and overhang of the lateral plateau. Correction in the tibial diaphysis creates a zig zag pattern in the tibia by correcting below the deformity and risks nonunion in cortical bone. There is no evidence that the femur is deformed; therefore, femoral osteotomy is not indicated.
Question 11
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
Nonsurgical care for hallux rigidus involves limiting the motion of the first metatarsophalangeal joint during toe-off and ensuring that there is a deep enough toe box to accommodate dorsal osteophytes. A rigid shank or forefoot rocker both help to reduce the forces of extension during toe-off. Beskin JL: Hallux rigidus. Foot Ankle Clin 1999;4:335-353.
Question 12
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?


Explanation
The MRI scans reveal a large postoperative hematoma causing significant thecal compression. An epidural hematoma with neurologic deficit is a surgical emergency requiring immediate evacuation of the hematoma. Although the incidence of postoperative epidural hematomas is rare, the consequences of a missed diagnosis can be catastrophic. Early recognition and evacuation are essential in preserving or restoring neurologic function. Uribe and associates attributed delayed postoperative hematomas to previous multiple lumbar surgeries as a possible contributing factor. Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.
Question 13
A 20-year-old man reports painless snapping about the lateral aspect of the right hip. He denies any history of trauma. Examination reveals no limp or tenderness. Hip range of motion is full, and there is good strength. Radiographs are normal. What anatomic structure is most likely causing these symptoms?
Explanation
Coxa saltans (snapping hip syndrome) can occur in two forms: external/lateral or interior/medial/anterior. This patient has the external/lateral form. The external/lateral form involves the iliotibial band, tensor fascia, or gluteus medius, which snaps over the greater trochanter. The external form usually can be treated with physical therapy alone; however, several recent studies report satisfactory results with surgical treatment. Faraj and associates reported good results from surgical Z-plasty in a series of 10 patients. White and associates reported good results in a series of 16 patients with 17 hips who underwent surgical release of an external snapping hip. The interior/medial/anterior form can involve the iliopsoas tendon, acetabular labrum, subluxation of the hip, and loose bodies. White RA, Hughes MS, Burd T, et al: A new operative approach in the correction of external coxa saltans: The snapping hip. Am J Sports Med 2004;32:1504-1508. Faraj AA, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Question 14
A 19-year-old woman reports persistent neck pain for 2 years. Pain is relieved with aspirin. A bone scan shows intense uptake in the superior, posterior portion of the C3 vertebral body. A sagittal CT reconstruction is shown in Figure 5. Treatment should consist of

Explanation
The CT scan shows an osteoblastic nidus pathognomic for an osteoid osteoma. Surgical treatment should include an en bloc excision of the lesion. Surgical treatment is not mandatory because the lesion often becomes asymptomatic over time. This lesion is not amenable to radiofrequency ablation due to its proximity to the spinal cord. A complete corpectomy is not necessary to adequately resect the lesion, as only the nidus needs to be removed. Radiation therapy and antibiotics are not appropriate treatments for an osteoid osteoma. Posterior C2-C3 fusion will not address the pathology. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
Question 15
High Yield
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
The patient has a pectoralis major rupture, an injury that occurs most commonly during weight lifting. Grade III injuries represent complete tears of either the musculotendinous junction or an avulsion of the tendon from the humerus, the most common injury site. Examination will most likely reveal ecchymoses and swelling in the proximal arm and axilla, and strength testing will show weakness with internal rotation and in adduction and forward flexion. Axillary webbing, caused by a more defined inferior margin of the anterior deltoid as the result of rupture of the pectoralis, can be seen as the swelling diminishes. Surgical repair is the treatment of choice for complete ruptures. Nonsurgical treatment is associated with significant losses in adduction, flexion, internal rotation, strength, and peak torque. The pectoralis major originates from the proximal clavicle and the border of the sternum, including ribs two through six. The pectoralis major inserts (rather than originates) on the humerus. The coracoid process is the insertion site for the pectoralis minor, as well as the origin for the conjoined tendon. The pectoralis major has no attachment or origin from the scapula. The anterior deltoid originates from the lateral one third of the clavicle and the anterior acromion. Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Question 16
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?


Explanation
The radiographs reveal osteonecrosis with collapse. The most reliable and durable treatment for osteonecrosis of the humeral head remains prosthetic shoulder arthroplasty. Osteonecrosis of the humeral head may be seen after the use of steroids, and there is an increasing demand for shoulder arthroplasty in young people because of the use of high-dose steroids in chemotherapy regimes for the treatment of malignant tumors. The indications for most shoulder arthrodeses today include posttraumatic brachial plexus injury, paralytic disorders in infancy, insufficiency of the deltoid muscle and rotator cuff, chronic infection, failed revision arthroplasty, severe refractory instability, and bone deficiency following resection of a tumor in the proximal aspect of the humerus. Clearly, the role of arthroscopy and related minimally invasive techniques in the treatment of humeral head osteonecrosis remains unknown. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298. Hattrup SJ: Indications, technique, and results of shoulder arthroplasty in osteonecrosis. Orthop Clin North Am 1998;29:445-451.
Question 17
High Yield
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Detailed Explanation
Because the patient has significant arthritis, arthrodesis is the treatment of choice. Adding a bone graft will prevent further shortening and add length to her toe, resulting in improved cosmesis. A cheilectomy will not alleviate her arthritis pain. The toe is too short for an effective Moberg phalangeal dorsiflexion osteotomy. A Waterman first metatarsal dorsal osteotomy will not address the degenerative joint disease or shortening. Silastic arthroplasty may help, but there is the risk of additional problems with foreign body reaction and a significant risk of failure known to occur with Silastic materials. Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306. Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Question 18
When posterior fusion with instrumentation to the sacrum is used to treat adult scoliosis, what instrumentation technique best increases the chance of a successful lumbosacral fusion?
Explanation
As the chance of success of lumbosacral fusion increases with the stiffness and rigidity of the construct, fixation and stiffness improve with fixation into both the upper sacrum and the ilium. In a review of individuals treated with long constructs to the pelvis for adult scoliosis, Islam and associates reported that the rate of pseudarthrosis was significantly lower with sacral and iliac fixation compared with sacral fixation alone or iliac fixation alone. Iliac screws provide significant fixation anterior to the instantaneous axis of rotation for flexion and extension, as well as provides resistance to lateral bending and rotational forces. Numerous biomechanical studies support the concept of increasing biomechanical stabilization with increased fixation from the sacrum to the ilium. Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173. O'Brien N, et al: Sacral pelvic fixation and spinal deformity, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 601-614.
Question 19
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?




Explanation
The "sunburst" radiographic appearance suggests an osteosarcoma, and the histologic findings confirm the diagnosis with malignant cells surrounded by pink osteoid. MRI scans are not particularly helpful in the diagnosis of osteosarcoma but are mandatory for surgical planning. Osteosarcomas are high-grade sarcomas that are best treated with chemotherapy and wide resection. Even though the peroneal nerve is involved, limb salvage is indicated. Survival after limb salvage is equivalent to amputation, with better function. Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637. Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Question 20
A 50-year-old woman has a painful hallux valgus and a painful callus beneath the second metatarsal head. A radiograph is shown in Figure 46. To correct these problems, treatment of the great toe deformity should consist of

Explanation
The patient has a significant hallux valgus and instability of the first ray, causing transfer metatarsalgia to the second metatarsal head. Therefore, the best procedure is fusion of the metatarsal cuneiform joint with soft-tissue realignment of the first metatarsophalangeal joint. This procedure provides the best chance of relieving symptoms under the second metatarsal head, as well as correcting the hallux valgus.
Question 21
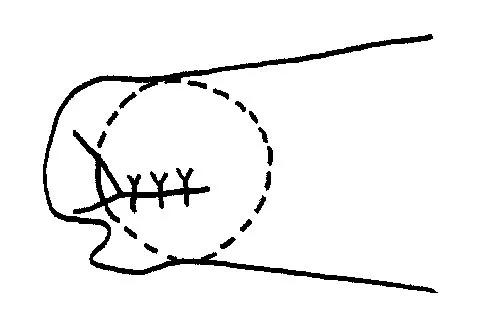
The photomicrograph in Figure 37 shows a repaired dural tear 4 days after surgery. The material interposed between the dural edges (D) is composed of

Explanation
During the initial healing phases of a dural tear, pia and arachnoid from adjacent nerve roots migrate, fill the dural defect, and create a pia-arachnoid plug. It is this initial plugging of the defect that is believed to prevent further egress of cerebrospinal fluid through the defect. The plug has been shown to develop by the second postoperative day. Fibroblastic proliferation occurs within the dura itself and accounts for the bulbous ends of the dura seen in the photomicrograph. The appearance of the material within the dural edges is inconsistent with the appearance of neural elements, and scar tissue formation occurs later in the healing process. Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Question 22
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
The beach chair position may cause sudden hypotension and bradycardia as a result of the Bezold-Jarisch reflex. This reflex occurs when venous pooling and increased sympathetic tone induce a low-volume, hypercontractile ventricle, resulting in activation of the parasympathetic nervous system and sympathetic withdrawal. The reported incidence of this phenomenon associated with the sitting position is between 13% to 24%. Left untreated, the result may be cardiac arrest. Pneumothorax or central nervous system toxicity after interscalene block is rare and has an incidence of less than 0.2%. Laryngeal nerve block associated with interscalene nerve block can occur but usually results in hoarseness secondary to ipsilateral vocal cord palsy. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Question 23
High Yield
Which of the following structures is the most important restraint to posterior subluxation of the glenohumeral joint when positioned in 90 degrees of flexion and internal rotation?
Explanation
The posterior band of the inferior glenohumeral ligament is the most important restraint to posterior subluxation of the glenohumeral ligament with the shoulder in 90 degrees of flexion and internal rotation. With the shoulder in external rotation, the subscapularis is an important stabilizer to posterior subluxation. When the shoulder is in neutral rotation, the coracohumeral ligament is the primary stabilizer. The middle glenohumeral ligament functions primarily to resist anterior translation of the shoulder in the midrange of abduction. The supraspinatus muscle and tendon have relatively little contribution to anterior and posterior translation of the glenohumeral joint. Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML: Posterior glenohumeral subluxation: Active and passive stabilization in a biomechanical model. J Bone Joint Surg Am 1997;79:433-440.
Question 24
High Yield
A 24-year-old man reports the development of a foot drop following a knee dislocation 1 year ago. The common peroneal nerve was found to be in continuity at the time of surgical reconstruction of the posterolateral corner of the knee joint. He would like to eliminate the need for an ankle-foot orthosis. What is the best option to achieve elimination of the orthosis?
Explanation
The ankle dorsiflexor muscles have been denervated for too long a period to expect reinnervation to be successful. Even if the extensor hallucis longus tendon was functional, it is unlikely to have sufficient strength to achieve dynamic ankle dorsiflexion. The tibialis posterior tendon transfer has been shown to predictably achieve these goals in a high percentage of patients. Successful ankle fusion is likely to fail with time due to the development of forefoot equinus. Pinzur MS, Kett N, Trilla M: Combined anteroposterior tibial tendon transfer in post-traumatic peroneal palsy. Foot Ankle 1988;8:27l-275.
Question 25
An 18-year-old girl with quadriplegic cerebral palsy underwent posterior spinal fusion from T2 to the pelvis 3 weeks ago. She now has a low-grade fever and mild midline erythema in a 1-cm area from which there is slight clear yellowish drainage. What is the next most appropriate step in management?

Explanation
The presence of drainage 3 weeks after surgery is a sign of wound infection. This infection most likely involves deep tissues until proven otherwise. Oral or IV antibiotics, in the absence of debridement, are not sufficient. Removal of the hardware would lead to rapid progression of the scoliosis in a spine that has been surgically destabilized by removal of the facet joints. The appropriate treatment is debridement with wound culture, IV antibiotics, and retention of hardware. The wound should be closed over drains. Theiss SM, Lonstein JE, Winter RB: Wound infections in reconstructive spine surgery. Orthop Clin North Am 1996;27:105-110.
Question 26
A biopsy of the involved physis in a patient with slipped capital femoral epiphysis (SCFE) would most likely reveal
Explanation
Vascular invasion, histologically similar to granulation tissue, has been noted between the columns in the zone of hypertrophy, leading to the theory of microtrauma as an etiology. SCFE is also associated with conditions that increase the height of the zone of hypertrophy, including the adolescent growth spurt and endocrinopathies. The perichondral ring has been shown to decrease in thickness with age. Normal undulations in the growth plate also decrease during this time, possibly further destabilizing the physis. Abnormal accumulations of proteoglycan have been reported. Chung SM, Batterman SC, Brighton CT: Shear strength of the human femoral capital epiphyseal plate. J Bone Joint Surg Am 1976;58:94-103.
Question 27
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45-degree lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?

Explanation
There are several indications for extending adult scoliosis fusions to the sacrum, rather than stopping in the lower lumbar spine. These indications include posterior column deficiencies at L5-S1, such as spondylolysis and laminectomy, and deformities extending to the sacrum, such as fixed tilt of L5-S1 or sagittal imbalance. MRI signal changes in the L5-S1 disk do not preclude stopping the fusion at L5. Some surgeons use diskography or diagnostic facet blocks to evaluate the integrity of the L5-S1 level prior to stopping the fusion at L5. Long scoliosis fusions stopping at L5 have a significant risk of failure, highlighting the importance of careful selection of fusion levels. Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629. Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Question 28
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of

Explanation
The patient has an acute grade III posterior cruciate ligament injury. The majority of grade I and II injuries can be treated with protected weight bearing and quadriceps rehabilitation, and most patients can return to sports within 2 to 4 weeks. In contrast, grade III injuries require immobilization in full extension for 2 to 4 weeks to protect the posterior cruciate ligament and the other posterolateral structures presumed to be damaged. The mainstay of postinjury rehabilitation for all posterior cruciate ligament injuries is quadriceps strengthening exercises, which have been shown to counteract posterior tibial subluxation. Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Question 29
A 17-year-old football player continues to have discomfort after sustaining a blow to his midthigh during a game 8 weeks ago. A plain radiograph is shown in Figure 13. What is the most appropriate management?

Explanation
The patient has myositis ossificans. Rest of the involved area is important to help limit the continued irritation of the muscle, but range-of-motion exercises are important to limit stiffness. While immobilization for 1 or 2 days following a muscle contusion is appropriate, longer periods of immobilization result in muscle atrophy and fibrosis. Injections and irradiation have not been found to be of benefit for myositis ossificans. Excision is rarely required, and if performed, it should not be performed prior to maturation of the lesion, which is a minimum of 6 months. Lipscomb AB, Thomas ED, Johnston RK: Treatment of myositis ossificans traumatica in athletes. Am J Sports Med 1976;4:111-120. Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Question 30
The spread of malignant cells to the vertebrae is often through
Explanation
In 1940, Batson described a valveless plexus of veins that extend from the dural venous sinuses of the skull to the sacrum. This system permits retrograde blood flow and enables tumor cells to enter vertebral bodies at multiple levels. Increased intra-abdominal pressure will enhance this retrograde blood flow.
Question 31
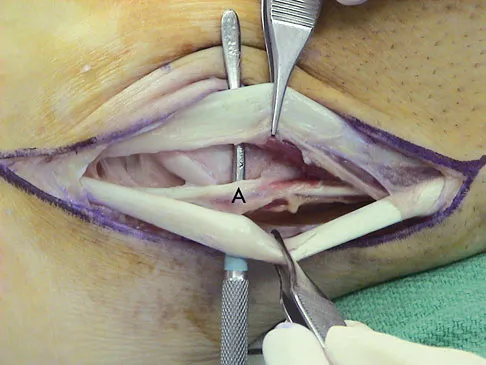
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 32
High Yield
Which of the following best describes the course of the median nerve at the elbow?
Explanation
The median nerve courses superficial to the ulnar artery, deep to the fibrous arch of the superficialis muscle, and deep to the superficial head of the pronator teres muscle. The median nerve lies within the interval between the flexor digitorum superficialis muscle and the flexor digitorium muscle as it progresses toward the wrist. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 33
High Yield
Figure 1 shows the radiograph of a 60-year-old woman who underwent a previous operation for great toe pain 20 years ago. She has had increasing pain over the past 5 years and now reports pain with any motion, swelling, and clicking. She also reports pain under the ball of foot. What is the most appropriate management to alleviate her metatarsalgia and great toe pain?

Explanation
The patient has a failed Silastic implant. Nonsurgical management will not work at this point. A Keller resection will only exacerbate her metatarsalgia. Implant removal with structural bone grafting and MTP fusion is the most appropriate choice because restoration of length is needed to alleviate the forefoot pain and bone grafting is required to fuse the MTP joint because there is an abundance of osteolysis. Total toe implants do not offer good long-term outcomes and are very difficult to fit into the large exploded-out cavity of the proximal phalanx. Hecht PJ, Gibbons MJ, Wapner KL, et al: Arthrodesis of the first metatarsophalangeal joint to salvage failed silicone implant arthroplasty. Foot Ankle Int 1997;18:383-390.
Question 34
High Yield
A 13-year-old girl is referred for a painful progressive valgus deformity of the right knee. Examination reveals an antalgic gait with an obvious valgus deformity. The right distal femur has a palpable, tender mass with erythema and warmth. Figures 4a and 4b show a clinical photograph and a radiograph. Management should consist of


Explanation
The radiograph shows a pathologic fracture through a destructive lesion of the distal femur metaphysis with osteolytic and osteoblastic features. The lateral cortex is destroyed, and there is periosteal new bone formation. These findings are consistent with malignancy, most likely an osteogenic sarcoma. Patients with suspected malignant tumors are best managed by surgeons with specific expertise in orthopaedic oncology. The biopsy of a malignant lesion should be deferred to the surgeon who is capable of definitive management of the patient. Enneking W: Principles of musculoskeletal oncologic surgery, in Evarts C (ed): Surgery of the Musculoskeletal System. New York, NY, Churchill Livingston, 1990.
Question 35
High Yield
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
Failure of the scalene block, necessitating general anesthesia or the immediate administration of narcotic medications, is the most common complication, occurring in 3% to 18% of patients. Cardiac arrest or cardiovascular collapse has been reported in anecdotal occurrences. Seizure that is the result of intravascular injection of local anesthetic is a rare complication, with an incidence reported of 0% to 6%. Neurologic complications, including laryngeal and phrenic nerve injuries, are rare although parathesias lasting up to 2 weeks have been reported in up to 3% of patients. Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Question 36
High Yield
A 10-year-old girl has a midshaft both bone forearm fracture. After attempted closed reduction, alignment consists of bayonet apposition, 10 degrees of malrotation, and 8 degrees of volar angulation. Management should now consist of

Detailed Explanation
Acceptable alignment in both bone forearm fractures is related to age and location. In children younger than age 9 years, angulations of 15 degrees and malrotation of 45 degrees are acceptable. In children older than age 9 years, acceptable alignment is 10 degrees of angulation and 30 degrees of malrotation. Bayonet apposition is acceptable provided that the angular and rotational reductions are held within these guidelines. A long arm cast provides better control of deforming forces than a short arm cast. Do TT, Strub WM, Foad SL, et al: Reduction versus remodeling in pediatric distal forearm fractures: A preliminary cost analysis. J Pediatr Orthop B 2003;12:109-115. Flynn JM: Pediatric forearm fractures: Decision making, surgical techniques, and complications. Instr Course Lect 2002;51:355-360. Ring D, Waters PM, Hotchkiss RN, et al: Pediatric floating elbow. J Pediatr Orthop 2001;21:456-459.
Question 37
High Yield
Which of the following is associated with the use of bisphosphonates in the setting of metastatic breast cancer to the spine?
Explanation
The indications of bisphosphonate therapy in breast cancer patients range from the correction of hypercalcemia to the prevention of cancer treatment-induced bone loss. Bisphosphonates reduce metastatic bone pain in at least 50% of patients and can reduce the frequency of skeletal-related events by 30% to 40%. Osteonecrosis of the jaw could occur in up to 2.5% of breast cancer patients during long-term bisphosphonate therapy.
Question 38
High Yield
Titanium and its alloys are unsuitable candidates for which of the following implant applications?

Detailed Explanation
Titanium alloy is highly biocompatible, has higher strength than stainless steel, and is highly resistant to corrosion. It is particularly suited for use in fracture plates, bone screws, and intramedullary nails because of its low modulus of elasticity (low stiffness), which can reduce stress shielding. It is also widely used for porous-ingrowth coatings. However, clinical experience has shown that titanium alloy bearing surfaces such as a femoral ball are highly susceptible to severe metallic wear, particularly in the presence of third-body abrasive particles (PMMA fragments, bone chips, metal debris, etc). McKellop HA, Sarmiento A, Schwinn CP, et al: In vivo wear of titanium-alloy hip prostheses. J Bone Joint Surg Am 1990;72:512-517. Salvati EA, Betts F, Doty SB: Particulate metallic debris in cemented total hip arthroplasty. Clin Orthop 1993;293:160-173.
Question 39
High Yield
A 42-year-old woman with a long-standing history of rheumatoid arthritis undergoes total shoulder arthroplasty for persistent pain that has failed to respond to nonsurgical management. Intraoperative radiographs reveal an oblique, minimally displaced fracture of the greater tuberosity. Based on these findings, what is the best course of action?

Explanation
The risk of intraoperative fracture in osteoporotic bone in patients with rheumatoid arthritis is significant. Fractures most often occur during humeral head dislocation and positioning for canal reaming. If the fracture occurs at the greater tuberosity, cerclage suture fixation of the tuberosity fracture with autogenous cancellous bone graft from the resected humeral head is the treatment of choice. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 215-225.
Question 40
High Yield
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of

Explanation
Based on the history, examination, and radiograph, the patient has typical degenerative arthritis of the elbow. This condition is found almost exclusively in men, and there is almost universally a history of repetitive heavy use or overuse of the elbow. Patients report pain at terminal extension and usually have a flexion contracture. Radiographs reveal osteophytes on the coronoid and olecranon and in the coronoid and olecranon fossae. The osteophytes are often associated with loose bodies that sometimes are attached to the soft tissues. Treatment should consist of removal of all loose bodies and impinging osteophytes using open technique or by arthroscopy. The capsular contractures should be released at the same time. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294. Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413. Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
Question 41
Pain associated with a proximal medial tibial osteochondroma in a 10-year-old patient is most commonly the result of
Explanation
Pain secondary to an osteochondroma is usually from soft-tissue irritation and bursal formation. This is particularly common for proximal medial tibia osteochondromas that irritate the pes anserine tendons. Malignant degeneration into a chondrosarcoma rarely occurs, is usually associated with multiple hereditary exostoses, and usually occurs after skeletal maturity. Borges AM, Huvos AG, Smith J: Bursa formation and synovial chondrometaplasia associated with osteochondromas. Am J Clin Pathol 1981;75:648-653.
Question 42
High Yield
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
The steel shank is a flat 1-inch steel strip placed between layers of the shoe to extend the foot lever and prevent deformity at the toe break seen following a partial first ray amputation. A rocker sole may be added as well to facilitate transition from foot flat to the toe-off phase of gait. Proper shoe fit is important, but "snug" fitting shoes in a patient with peripheral neuropathy and likely fluctuations in volume from intermittent swelling are to be avoided. A custom shoe is an unnecessary expense. The patient has at least 10 degrees of dorsiflexion at the ankle with an intact anterior tibialis muscle; therefore, catching the sole on carpeting should not be a problem. Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Question 43
A 25-year-old woman who fell on her outstretched hand reports chronic pain over the hypothenar eminence region and some dorsal ulnar wrist pain. She also notes difficulty playing golf and tennis. Plain radiographs of the hand and wrist are unremarkable. A CT scan is shown in Figure 36. What is the next most appropriate step in management?

Explanation
The CT scan reveals a hook of the hamate nonunion with irregular resorption at the fracture site, which is at the base of the hamate. Symptomatic relief of the pain and discomfort has been well documented after excision of the hook of the hamate. Ultrasound therapy will not provide long-term symptomatic relief or induce nonunion healing. MRI for further soft-tissue evaluation is inappropriate because this is a bony problem; the bony architecture of the wrist is best visualized by CT. Open reduction and internal fixation of the hook of the hamate does not provide the symptomatic relief that is found with excision of the hook of the hamate. In addition, the technical difficulties and relative risk of persistent nonunion after open reduction and internal fixation are not merited when hamate excision can be effected easily and causes no long-term untoward effects. Electrodiagnostic evaluation is inappropriate because there is no history of the persistent numbness and tingling that is found in peripheral compression neuropathies. Stark HH, Chao EK, Zemel NP, Rickard TA, Ashworth CR: Fracture of the hook of the hamate. J Bone Joint Surg Am 1989;71:1206-1207. Failla JM: Hook of hamate vascularity: Vulnerability to osteonecrosis and nonunion. J Hand Surg Am 1993;18:1075-1079. Carter PR, Easton RG, Littler JW: Ununited fracture of the hook of the hamate. J Bone Joint Surg Am 1977;59:583-588.
Question 44
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?

Explanation
One possible reason for improved efficacy of LMWHs is the relative improved bioavailability compared with that of unfractionated heparin. This is, in part, the result of a more predictable dose response and a longer half-life. There is no alteration of venous flow, and the rate of bleeding complications is the same or slightly higher than that of other prophylactic agents. Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14. Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Question 45
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?

Explanation
A 30% to 50% loss of cervical range of motion is reported postoperatively in most patients following cervical laminoplasty. Inadvertent closure of the laminoplasty does occur but is rare. Laminoplasty is advocated in lieu of laminectomy to prevent progressive kyphosis and can effectively decompress the spinal cord. C5 nerve root palsies are a poorly understood but rare complication of surgical decompression for cervical spondylotic myelopathy. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 46
A 65-year-old man has a painful right hip mass that has been growing for several years. A radiograph, CT scan, and photomicrograph are shown in Figures 56a through 56c. What is the most appropriate treatment?



Explanation
This is a conventional chondrosarcoma. The radiograph and the CT scan show a lesion arising from the inferior pubic ramus with a large soft-tissue mass. Abundant punctate, stippled, or "popcorn-like" calcification is present. The photomicrograph demonstrates hypercellular cartilage. Surgical resection is the only effective treatment. Whereas chemotherapy might play a role in the treatment of a dedifferentiated chondrosarcoma, it has no role in the treatment of a conventional chondrosarcoma. Chondrosarcomas are relatively radioresistant. Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530. Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Question 47
High Yield
A 20-year-old football player has repeated episodes of heat cramps during summer training sessions. A deficiency of what electrolyte is most responsible for heat cramps?
Detailed Explanation
Sodium deficiency is the cause of heat cramps. It is the principle electrolyte of sweat and is readily lost during training, especially in warmer temperatures. The condition can be avoided by adding extra table salt to food and maintaining good hydration before and after sports activities. Salt tablets are to be avoided when a patient has heat cramps because the high soluble load will cause gastric irritation. Bergeron MF, Armstrong LE, Maresh CM: Fluid and electrolyte losses during tennis in the heat. Clin Sports Med 1995;14:23-32.
Question 48
A 42-year-old woman has a history of nontraumatic ankle swelling with tenderness over the Achilles tendon and plantar fascia. She reports that while vacationing in Connecticut 2 months ago she noted the presence of a "red bull's eye" rash. Management should consist of
Explanation
The most likely diagnosis is Lyme disease because of the patient's recent vacation in an area with a high risk of exposure. The most effective treatment is doxycycline. Neu HC: A perspective on therapy of Lyme infection. Ann NY Acad Sci 1988;539:314-316.
Question 49
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?

Explanation
Discoid menisci are rare causes of lateral knee pain in children. Various etiologies have been proposed, including failure of central absorption of the developing meniscus and hereditary transmission. Patients with discoid menisci have pain, clicking, and locking with a loss of active extension on range-of-motion testing. Classification of discoid menisci according to the Watanabe classification include complete, incomplete, and Wrisberg ligament type. The Wrisberg variant contains an abnormal posterior meniscal attachment. MRI is the diagnostic tool of choice, revealing a thick, flat meniscus generally seen in three consecutive MRI images. Symptomatic knees are often associated with a meniscal tear or degeneration and are managed with arthroscopic partial excision to a more normal shape (saucerization). Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Question 50
Patients with patellar clunk syndrome are best managed by which of the following methods?

Explanation
Patellar clunk syndrome is usually the result of a fibrous nodule that forms on the undersurface of the distal quadriceps tendon. It may get entrapped in the intercondylar notch of the femoral component during flexion, and lead to a sudden snap as the nodule is pulled out of the notch during active extension. Nonsurgical management is rarely successful. Surgical debridement is usually curative, with only rare recurrence. More aggressive procedures such as realignment, revision, or patellectomy are usually not necessary, and are reserved for cases resistant to soft-tissue debridement. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 329. Diduch DR, Scuderi GR, Scott WN, et al: The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166-171.
Question 51
A 62-year-old patient with rheumatoid arthritis has had pain and instability of the elbow following total elbow replacement 2 years ago. A complete work-up, including aspiration and cultures, is negative. Figures 9a and 9b show the AP and lateral radiographs. Treatment should consist of


Explanation
The patient has aseptic loosening of the original semiconstrained prosthesis and significant proximal ulnar bone destruction; therefore, the treatment of choice is revision arthroplasty using a semiconstrained design. Although orthotic stabilization could be used, it will not provide long-term pain relief. Resection arthroplasty after removal of the components may lead to painful instability. Elbow arthrodesis would be difficult with the bone stock loss and is not considered the best option. Two main contraindications to the use of an unconstrained prosthesis are significant bone loss and previous use of a hinged or semiconstrained prosthesis. An ulnar allograft could be combined with the use of a semiconstrained long-stemmed ulnar prosthesis as a treatment modification. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 52
High Yield
An otherwise healthy 54-year-old man who underwent a successful multilevel lumbar decompression and fusion 4 years ago now reports increasingly severe bilateral thigh claudication with paresthesia and severe back pain for the past 12 months. Physical therapy, bracing, and epidural steroids have failed to provide relief. A radiograph and MRI scans are shown in Figures 15a through 15c. He is afebrile, and laboratory studies show an erythrocyte sedimentation rate of 5 mm/h and a normal WBC count. What is the best course of action?



Detailed Explanation
The patient has degeneration of an adjacent segment with resultant kyphosis and stenosis. Because he is healthy, has responded well to previous surgery, and has a potentially correctable lesion, he is not a good candidate for an end-stage failed back procedure such as a morphine pump. The stenosis is exacerbated by the deformity; therefore, a simple decompression will contribute to instability. Because of the kyphosis and the patient's relatively young age, the treatment of choice is restoration of sagittal alignment and posterior decompression.
Question 53
A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm3. What is the most common organism in this scenario?

Explanation
The most common bacterial etiologic agent following varicella is group A beta-hemolytic streptococcus. The other organisms are much less common. Staphylococcus aureus is the most common bone infection organism. Staphylococcus epidermidis is increasingly a bone infection organism. Group B streptococcus occurs more commonly in newborns. Kingella kingae is a common joint pathogen but is not as common following varicella. Schreck P, Schreck P, Bradley J, et al: Musculoskeletal complications of varicella. J Bone Joint Surg Am 1996;78:1713-1719.
Question 54
High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 55
High Yield
Which of the following best describes heat stroke?
Detailed Explanation
Heat stroke consists of hyperthermia (greater than 105.8 degrees F [41 degrees C]), central nervous system dysfunction, and cessation of sweating with hot, dry skin. It is a medical emergency that results from failure of the thermoregulatory mechanisms of the body. It has a high death rate and requires rapid reduction in body core temperature. Heat syncope is characterized by a transient loss of consciousness with peripheral vasodilation and decreased cardiac output with normal body temperature. Heat cramps involve painful contractions of large muscle groups because of decreased hydration and a decrease of serum sodium and chloride. Heat exhaustion is distinguished by a core temperature of less than 102.2 degrees F (39 degrees C) and an absence of central nervous system dysfunction. Hypernatremic heat exhaustion results from inadequate water replacement. Knochel JP: Environmental heat illness: An eclectic review. Arch Intern Med 1974;133:841-864. Hubbard RW, Gaffin SL, Squire DL: Heat related illness, in Wilderness Medicine, ed 3. St Louis, MO, Mosby, 1995, p 167.
Question 56
High Yield
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
Explanation
The pisotriquetral joint is best seen on a lateral view in 30 degrees of supination. The carpal tunnel view provides visualization of the joint but to a lesser extent. The other views do not provide clear and accurate visualization. Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Question 57
High Yield
What neurovascular structure is most at risk when performing an inside-out repair of the posterior horn of the medial meniscus?
Explanation
The saphenous nerve is located on the posterior medial aspect of the knee and must be protected when performing an inside-out repair of the medial meniscus. The peroneal nerve is most at risk with lateral meniscal repairs. The other structures usually are not at risk with meniscal repair. Cannon WD Jr, Morgan CD: Meniscal repair: Arthroscopic repair techniques. Instr Course Lect 1994;43:77-96.
Question 58
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Explanation
A knee dislocation carries the potential for an arterial injury and has always brought up the question of need for arteriography to rule out this limb-threatening injury. However, arteriography has an inherent complication rate that may compromise the general care of the patient. In over 240 published cases with documented knee dislocations that were evaluated for vascular injury by physical examination (without imaging studies), not a single missed injury was reported, for a 100% negative predictive value (0% false-negative rate). This degree of accuracy at excluding major vascular injury is unsurpassed by the results obtained with arteriography but with no risk involved and a marked savings in time, equipment, and costs. Therefore, the most appropriate first step to rule out vascular injury is examination of the pedal pulses. If there is any doubt about an arterial injury, another option is the ankle-brachial index (ABI). If the ABI is greater than 0.9, the chance of arterial injury is again nonexistent. However, a positive physical examination or an ABI of less than 0.9 is not 100% predictive of an arterial injury; therefore, arteriography is recommended. Miranda FE, Dennis JW, Veldenz HC, et al: Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: A prospective study. J Trauma 2002;52:247-252.
Question 59
High Yield
Which of the following is a recognized consequence of hip fusion?

Explanation
Low back pain is an expected long-term complication of fusion; ipsilateral knee laxity is frequently encountered, as is degeneration of the contralateral hip. Hip fusion is equally valuable for both men and women, with both genders reporting satisfactory sexual function. Female patients often deliver by elective Cesarean section, although vaginal deliveries are reported. Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Question 60
High Yield
A corset-type brace may help reduce symptoms during an episode of acute low back pain as the result of
Explanation
Although there is no significant alteration in motion with a corset, studies have shown a decrease in intradiskal pressure. Nachemson A, Morris JM: In vivo measurements of intradiscal pressure: Discometry, a method for determination of pressure in the low lumbar disc. J Bone Joint Surg Am 1964;46:1077-1092.
Question 61
High Yield
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause

Detailed Explanation
If the Buford complex is mistakenly reattached to the neck of the glenoid, severe painful restriction of external rotation will occur. Williams MM, Snyder SJ, Buford D Jr: The Buford complex - the "cord-like" middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 62
When performing an arthroscopic subacromial decompression, bleeding can be encountered when dividing the coracoacromial ligament because of injury to what artery?
Explanation
The acromial branch of the thoracoacromial trunk courses along the coracoacromial ligament. This artery enters the ligament approximately 5 mm below the acromial edge. Division of the ligament at its insertion on the acromion minimizes the risk of bleeding. Esch JC, Baker CL: Arthroscopic anatomy and normal variations, in Whipple TL (ed): Surgical Arthroscopy: The Shoulder and Elbow. Philadelphia, PA, JB Lippincott, 1993, pp 63-76.
Question 63
High Yield
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Detailed Explanation
Shufflebarger and others have reported that the placement of anterior interbody structural support at the lumbosacral junction increases the overall construct stiffness and reduces the strain on posterior instrumentation, thereby reducing the risk of screw pull-out or fracture. The stiffness of the posterior instrumentation actually increases, whereas the actual strength of the instrumentation remains the same. Actual strain measured at an adjacent intervertebral disk to a fusion construct is expected to increase. Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393. Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Question 64
High Yield
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?


Explanation
An increased density of the talar body compared to the distal tibia following fracture of the talar neck is highly suggestive of vascular compromise of the talar body. Subchondral osteopenia of the talus at 6 to 8 weeks (Hawkins sign) is a favorable sign but does not eliminate the possibility of osteonecrosis. Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Question 65
A 60-year-old woman has a mass in the right scapula. Figures 25a and 25b show a CT scan and a biopsy specimen. The cells are lymphocyte common antigen positive, Ewing's specific antigen (CD99) negative, and keratin negative. What is the next step in management?


Explanation
The clinical history, CT scan, and histology are most consistent with a lymphoma of bone. An important part of the staging is bone marrow aspiration and biopsy. The other studies listed are not indicated. Lymphoma of bone, when localized, is usually treated with chemotherapy and radiation therapy and has excellent survival rates. Widespread lymphoma has a worse prognosis. Finiewicz K, van Biesen K: Non-Hodgkins lymphoma, in Golomb H, Vokes E (eds): Oncologic Therapies, ed 2. Berlin, Germany, Springer, 2003, pp 295-318.
Question 66
Figure 30 shows an axial cross section of extensor tendon anatomy in zone 7 of the wrist. What letter best depicts the location of the posterior interosseous nerve?

Explanation
The posterior interosseous nerve in contained in the floor of the fourth dorsal compartment of the wrist, which is labelled C in this diagram. Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 224.
Question 67
High Yield
What is the most common complication following interscalene nerve block for shoulder surgery?
Explanation
All of these complications have been documented after interscalene nerve block. Other serious complications such as cardiac arrest and respiratory distress have also been noted. However, the most common complication after interscalene nerve block appears to be temporary paresthesia to the hand that can occur in up to 2.3% of the patients. Bishop JY, Sprague M, Gelber J, et al: Interscalene regional anesthesia for shoulder surgery. J Bone Joint Surg Am 2005;87:974-979.
Question 68
High Yield
A 22-year-old college basketball player who was hit from behind while going up for a rebound is rendered immediately quadraparetic for approximately 10 minutes, followed by complete resolution of motor loss and return of full sensation. The radiograph and MRI scan of the cervical spine shown in Figures 2a and 2b reveal a canal diameter of 13 mm, loss of cerebrospinal fluid space about the spinal cord, and no signal change within the cord. What is the best course of action?


Detailed Explanation
The correct decision on return to sports participation after episodes of transient quadraparesis is controversial. Cantu and Mueller feel strongly that the loss of cerebrospinal fluid space about the spinal cord signifies an unacceptable risk for future spinal cord injury if the athlete returns to sports. However, Watkins and Torg and Lasgow have reported no evidence of increased spinal cord injury in athletes with narrow spinal canals, even in football. These authors suggest judgment be used in advising return to contact or high-energy sports and that the physician's responsibility is to give accurate and relevant information, allowing the athlete to make his or her own choice regarding return to sports participation. Cantu R, Mueller FO: Catastrophic spine injuries in football (1977-1989). J Spinal Disord 1990;3:227-231. Watkins RG: Neck injuries in football players. Clin Sports Med 1986;5:215-246. Torg JS, Lasgow SG: Criteria for return to contact activities following cervical spine injury. Clin Sports Med 1991;1:12-26.
Question 69
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of

Explanation
Displaced clavicular fractures lateral to the coracoid process (Neer type II and III) are best managed nonsurgically with sling immobilization and physical therapy, starting with pendulum exercises and progressing to active-assisted exercises when comfortable. Supervised therapy should be performed for 3 months or until full painless motion is achieved. In one study by Robinson and Cairns, this form of treatment provided patients with a 86% chance of avoiding a secondary reconstructive procedure. Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Question 70
When performing the exposure for an anterior approach to the cervical spine, the surgical dissection should not enter the plane between the trachea and the esophagus and excessive retraction should be avoided to prevent injury to the
Explanation
The recurrent laryngeal nerve lies between the trachea and the esophagus. The vagus nerve lies in the carotid sheath. The sympathetic trunk lies anterior to the longus colli muscles. The hypoglossal and superior laryngeal nerves are both at risk during the exposure but are not located between the trachea and the esophagus. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 71
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of



Explanation
Although the MRI findings could be misinterpreted as an aggressive soft-tissue process, the periosteal-based ossification on the radiograph in an athlete most likely suggests myositis ossificans. The radiograph should be repeated to see further maturation of the ossification with a typical "zoning" pattern. The zoning pattern is one of peripheral ossification. This is often best seen on a CT scan. King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
Question 72
An 82-year-old woman reports right buttock pain after a car trip. Laboratory studies show an erythrocyte sedimentation rate of 30 mm/h and WBC of 4,600/mm3. Figure 34a shows a plain AP radiograph of the pelvis, and Figure 34b shows a delayed technetium Tc 99m bone scan. Management should consist of


Explanation
The radiograph shows bilateral cemented total hip arthroplasties. The acetabular components are loose bilaterally, but there has been no acute change. Therefore, it is unlikely that the acetabular loosening is contributing to the patient's pain. The bone scan is consistent with a sacral insufficiency fracture. This is best treated with bed rest and pain medication. Activity can be increased as the pain allows. Revision will not address the pain. Newhouse KE, el-Khoury GY, Buckwalter JA: Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am 1992;74:1472-1477.
Question 73
High Yield
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
Detailed Explanation
Absence of the rotator cuff results in superior migration of the humeral head because of unopposed deltoid function. This proximal migration results in eccentric loading of glenoid components with early loosening. Hemiarthroplasty yields good pain relief with limited goals of active elevation of 90 degrees. The coracoacromial arch should be preserved. Achieving satisfactory subscapularis tension is preferred to the use of an oversized humeral component. Zeman CA, Arcand MA, Cantrell JS, Skedros JG, Burkhead WZ Jr: The rotator cuff-deficient arthritic shoulder: Diagnosis and surgical management. J Am Acad Orthop Surg 1998;6:337-348. Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491. Williams GR Jr, Rockwood CA Jr: Hemiarthroplasty in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 1996;5:362-367.
Question 74
High Yield
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?

Explanation
There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high energy humeral shaft fractures. J Hand Surg 2004;29:144-147. Foster RJ, Swiontkowski MR, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 75
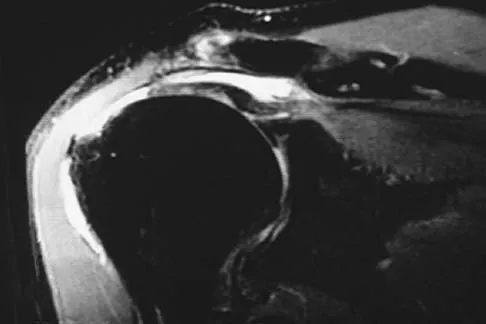
Figures 49a and 49b show MRI scans of the shoulder. What is the most likely diagnosis?


Explanation
The supraspinatus tendon shows clear detachment and retraction from its greater tuberosity attachment by the absence of the normal dark subacromial signal extending to the attachment on the greater tuberosity. There is no anterior inferior glenoid labral detachment that usually is seen in a Bankart lesion. The acromioclavicular joint shows no evidence of separation. The humeral head is migrated cranially, indicating a chronic rotator cuff tear. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29. Seeger LL, Gold RH, Bassett LW, Ellman H: Shoulder impingement syndrome: MR findings in 53 shoulders. Am J Roentgenol 1988;150:343-347.
Question 76
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?



Explanation
Anterior dislocation is the most common type of sternoclavicular dislocation. The medial end of the clavicle is displaced anterior or anterosuperior to the anterior margin of the sternum. In a study by Omer, 31% of athletic injuries have been known to cause a dislocation of the sternoclavicular joint. The serendipity view can show this dislocation, as will CT of the chest. This view requires the x-ray beam to be aimed at the manubrium with 40 degrees of cephalic tilt. An anterior sternoclavicular joint dislocation will appear superiorly displaced, while a posterior sternoclavicular joint dislocation is inferiorly displaced on the serendipity view. Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Question 77
High Yield
A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
Explanation
The patient likely has a significant Achilles contracture that causes her to always bear more weight on her forefoot. A gastrocnemius recession takes the ankle out of plantar flexion and she will be able to return to a normal gait and reduce the pressures on her forefoot. A forefoot amputation is a salvage option. The other choices are appropriate; however, the patient has had this problem for 2 years and she has already had multiple attempts at shoe wear modification. Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.
Question 78
The nerve to the abductor digiti quinti, implicated in some patients who have chronic heel pain, is most commonly a branch of what larger nerve?
Explanation
The nerve to the abductor digiti quinti is the first branch of the lateral plantar nerve. It branches off while the nerve is still on the medial side of the foot and also innervates a portion of the plantar fascia. It can become entrapped beneath the deep fascia of the abductor hallucis muscle and has been associated with some forms of chronic heel pain. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop 1992;279:229-236.
Question 79
A 30-year-old woman injures her knee while skiing. Based on the MRI scan shown in Figure 5, treatment should consist of

Explanation
The MRI scan demonstrates a grade III MCL tear. Basic science and clinical studies have shown that nonsurgical management is preferred for MCL tears. Functional rehabilitation and early motion have led to consistently better results than has surgical repair.
Question 80
High Yield
Figures 27a and 27b show the radiographs of a 32-year-old woman who was involved in a high-speed motor vehicle accident. She is neurologically intact. After stabilization and assessment, treatment should consist of
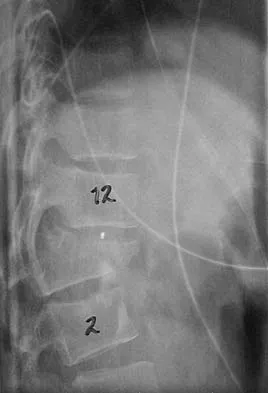

Explanation
The radiographs show a fracture-dislocation with translation in both the coronal and sagittal planes, evidence of significant instability requiring surgical stabilization. Anterior instrumentation is not as effective as posterior instrumentation in restoring stability, and because there is little bony destruction, the anterior column can be successfully reconstructed with simple realignment. The treatment of choice is multisegment posterior fusion with instrumentation. Lewandrowski KU, McLain RF: Thoracolumbar fractures: Evaluation, classification, and treatment, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 817-843.
Question 81
A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 20. Treatment should consist of

Explanation
The MRI findings show highly increased signal through the entire femoral head and neck on STIR imaging, diagnostic of transient osteoporosis of the femoral head. This disease entity can be seen in middle-aged men, and should be treated nonsurgically. The natural history is that of self-resolution. Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Question 82
High Yield
The radiograph shown in Figure 27 shows measurement of what angle?

Detailed Explanation
The relationship between the distal articular surface of the first metatarsal head and the long axis of the first metatarsal is called the distal metatarsal articular angle. This angle has been validated by Richardson and associates to measure and determine the congruence of the first metatarsophalangeal joint. This angle is critical in determining the appropriate surgical procedure to perform on a patient with a bunion deformity because a congruent joint requires a procedure to maintain congruence of the articular surfaces following osteotomy. Therefore, a chevron becomes a biplanar chevron, and a Lapidus procedure adds a second osteotomy of the distal metatarsal to tilt the metatarsal head into a congruent location. Coughlin MJ: Juvenile hallux valgus: Etiology and treatment. Foot Ankle Int 1995;16:682-697. Steel MW III, Johnson KA, DeWitz MA, et al: Radiographic measurements of the normal foot. Foot Ankle 1980;1:151-158.
Question 83
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of


Explanation
The patient has the findings of classic subacromial impingement. Initial management should consist of stretching exercises directed at the posterior capsule and a program of rotator cuff and deltoid strengthening exercises performed below the horizontal in a "safe" plane. The judicious use of subacromial cortisone injections (one or two) may be helpful. Anterior acromioplasty is reserved for patients who have failed to respond to nonsurgical management. Morrison DS, Frogameni AD, Woodworth P: Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:732-737. Neer CS: Impingement lesions. Clin Orthop 1983;173:70-77.
Question 84
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T1-weighted, sagittal T2-weighted, axial T1-weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?




Explanation
The MRI scans show multiple low-signal intensity lesions scattered throughout the knee, extending posteriorly inferior to the tibial plateau. The low-signal intensity on both the T1- and T2-weighted images, the modest vascularity noted on the gadolinium image, and the "blooming" noted on the gradient echo image (ferrous-laden tissue) are all strongly suggestive of diffuse PVNS. Whereas synovial chondromatosis can present as diffuse masses in the knee, they present as nodule masses that have low T1- and high T2-weighted signal characteristics. Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4241-4252.
Question 85
High Yield
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?

Explanation
The findings are characteristic of hemangioma. When the hemangioma is large enough, vertical striations may be visible on plain radiographs. Axial CT scans commonly reveal a speckled appearance. Metastatic lesions are typically hypointense on T1-weighted images because they replace the fatty marrow. Bony islands, like cortical bone, are dark on T1- and T2-weighted images. Intravertebral disk herniation would have characteristics similar to the disk and be in continuity with the disk. Osteoporosis is more diffuse. Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
Question 86
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?

Explanation
Varus position of the stem is most commonly associated with failure of the cemented femoral component because of association with an inadequate cement mantle in the proximal medial and distal lateral zones. An inadequate cement mantle and obesity have been associated with increased loosening but not as frequently as a varus deformity. The influences of gender and osteoporotic bone on the outcome of cemented femoral components have not been established. Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Question 87
Pacinian corpuscles are lamellated nerve endings that are responsible for providing the perception of

Explanation
Pacinian corpuscles are nerve endings that provide the perception of pressure.
Question 88
High Yield
An 83-year-old woman with a long history of her foot slowly and progressively "turning out" now reports significant ankle pain. History reveals that she has significant cardiac disease and exercise-induced angina. Examination reveals a deficiency in the posterior tibial tendon; however, the hindfoot remains moderately supple. Radiographs reveal a valgus tilt of the tibiotalar joint and early arthrosis. What is the most appropriate orthotic management?
Explanation
The patient will continue to have pain secondary to the ankle arthrosis with both the UCBL and the molded articulated ankle-foot orthosis. The total contact orthotic does not provide enough hindfoot control to support the progressive collapse of the ankle into valgus positioning. A molded leather gauntlet will not only control tibiotalar motion but also control hindfoot motion and allow support of the longitudinal arch.
Question 89
Based on the findings seen in the posteroanterior radiograph of the wrist shown in Figure 17, which of the following structures is torn?

Explanation
The radiograph shows widening between the scaphoid and lunate. The normal variance is up to 5 mm. Although several ligaments may be torn, the scapholunate interosseous ligament must be torn for this widening to occur. Cooney WP, Linscheid RL, Dobyns JH: The Wrist: Diagnosis and Operative Treatment. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 503-506.
Question 90
High Yield
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Detailed Explanation
In the initial assessment of acute low back pain in adults, no diagnostic testing is indicated during the first 4 weeks in the absence of "red flags" for a serious underlying condition. The purpose of the initial assessment of acute low back pain in adults is to rule out serious underlying conditions presenting as low back pain. The Agency for Healthcare Policy and Research, in its 1994 clinical practice guideline, identified four serious conditions that may present with low back pain, including fracture, tumor, infection, and cauda equina syndrome. This patient has five "red flags" for a spinal tumor as a possible etiology of his low back pain, including age of older than 50 years, constitutional symptoms (recent weight loss), pain worse when supine, severe nighttime pain, and a history of cancer. Of these, his history of cancer is most significant, as greater than 90% of spinal tumors are metastatic. In order of frequency, breast, prostate, lung, and kidney make up approximately 80% of all secondary spread to the spine. In the presence of "red flags" for tumor or infection, it is recommended that the clinician obtain a CBC count, ESR, and a urinalysis. If these are within normal limits and suspicions still remain, consider consultation or seek further evidence with a bone scan, radiographs, or additional laboratory studies. Negative radiographs alone are insufficient to rule out disease. If radiographs are positive, the anatomy can be better defined with MRI. Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.
Question 91
Which of the following muscles has dual innervation?

Explanation
The brachialis muscle typically receives dual innervation. The major portion is innervated by the musculocutaneous nerve. Its inferolateral portion is innervated by the radial nerve. The others listed have single innervation. The anterior approach to the humerus, which requires splitting of the brachialis, capitalizes on this dual innervation.
Question 92
High Yield
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?


Detailed Explanation
It is often tempting to assign a diagnosis of plantar fasciitis in patients with hindfoot pain. In this patient, the radiographs confirm a diagnosis of a calcaneal insufficiency fracture. The dense condensation of bone on the lateral view confirms the diagnosis. There is no radiographic evidence of a heel spur, osteochondral lesions, or chondrocalinosis. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 2591. Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Question 93
In the treatment of all magnitudes of bunionette deformities, what is the most common complication associated with lateral condylectomy of the fifth metatarsal head?
Explanation
When a lateral condylectomy alone is performed for all bunionette deformities, a high recurrence rate is expected. Lateral condylectomy should be used alone when the primary deformity is an enlarged lateral condyle of the fifth metatarsal head. In cases with significant divergence of the fifth metatarsal shaft in relationship to the fourth metatarsal shaft or with lateral bowing of the distal fifth metatarsal shaft, the lateral fifth metatarsal prominence will not be effectively reduced and recurrent symptoms and deformity are expected. Transfer metatarsalgia and/or dislocation of the metatarsophalangeal joint can infrequently occur with excessive metatarsal head excision. Arthrosis of the metatarsophalangeal joint has not been frequently reported. Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465. Kelikian H: Deformities of the lesser toe, in Kelikian H (ed): Hallux Valgus, Allied Deformities of the Forefoot and Metatarsalgia. Philadelphia, PA, WB Saunders, 1965, pp 327-330.
Question 94
High Yield
A patient undergoes hip arthroscopy, and the pathology is seen in Figure 18. What is the most likely diagnosis?

Explanation
The motorized shaver is adjacent to the acetabular labrum, which is torn. The femoral head and acetabulum are normal in appearance. Neither the fat pad nor a loose body is identified.
Question 95
High Yield
With a full-thickness articular cartilage injury, the body's healing response produces cartilage mainly composed of what type of collagen?
Detailed Explanation
With a full-thickness articular cartilage injury, a healing response is initiated with hematoma, stem cell migration, and vascular ingrowth. This response produces type I collagen and resultant fibrous cartilage rather than desired hyaline cartilage as produced by chondrocytes. This repair cartilage has diminished resiliency, stiffness, poor wear characteristics, and the predilection for arthritis. Type I collagen is also found in the annulus of intervertebral disks, tendon, bone, meniscus, and skin. Type II is found in articular cartilage and nucleus pulposus of intervertebral disks. Type III is found in skin and blood vessels, type IV is found in basement membranes, and type X is found in the calcified layer of cartilage. Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 19-28.
Question 96
A 20-year-old man sustained a closed tibial fracture and is treated with a reamed intramedullary nail. What is the most common complication associated with this treatment?

Explanation
The most common complication is anterior knee pain (57%). The knee pain is activity related (92%) and exacerbated by kneeling (83%). Although knee pain is the most common complication, most patients rate it as mild to moderate and only 10% are unable to return to previous employment. Some authors report less knee pain with a peritendinous approach when compared to a tendon-splitting approach. In one study, nail removal resolved pain in 27%, improved it in 70%, and made it worse in 3%. The incidence of the other complications was: infection 0% to 3%, nonunion 0% to 6%, and malunion 2% to 13%. Compartment syndrome is rare after nailing. Court-Brown CM: Reamed intramedullary tibial nailing: An overview and analysis of 1106 cases. J Orthop Trauma 2004;18:96-101. McQueen MM, Gaston P, Court-Brown CM: Acute compartment syndrome: Who is at risk? J Bone Joint Surg Br 2000;82:200-203.
Question 97
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 98
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of

Explanation
The patient has a type IIIB patellar fracture (inferior pole fracture with an intact patellar tendon). Nonsurgical management is the treatment of choice if there is little displacement and the extensor mechanism is intact. Brown TE, Diduch DR: Fractures of the patella, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1290-1312.
Question 99
In the preoperative planning of revision acetabular reconstruction, the surgeon should identify significant posterior column deficiency by noting which of the following radiographic features?
Explanation
Proximal and medial migration of the femoral head usually indicates deficiencies of the dome or anterior column. Wear of the polyethylene may result in osteolysis and impingement, which are not indicative of any major bone deficiency. A significant osteolytic lesion in the ischium may represent a major posterior column deficiency that can create a technical challenge during the reconstruction. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 100
High Yield
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?



Explanation
The patient has an acute fracture of the proximal pole. A 100% healing rate has been reported for open reduction and internal fixation of proximal pole fractures via a dorsal approach. This allows for direct viewing of the fracture line, facilitates reduction, and bone grafting can be done through the same incision if necessary. A vascularized or corticocancellous graft is reserved for nonunions. Proximal fractures are very slow to heal with a cast, if they heal at all. As a small fragment, percutaneous fixation is very difficult and has been reported for waist fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
