Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
The medial collateral ligament complex of the elbow consists of three portions: the anterior bundle, the posterior bundle, and a transverse component that has little biomechanic significance. The origin of the ligament is from the central two thirds of the anteroinferior undersurface of the medial epicondyle.
Question 2
High Yield
Figures 5a and 5b show the radiographs of a 45-year-old patient. What is the most likely diagnosis?


Detailed Explanation
Glenoid dysplasia is an uncommon anomaly that usually has a benign course but may result in shoulder pain, arthritis, or multidirectional instability. Shoulder pain and instability often improve with shoulder strengthening exercises. Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Question 3
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Question 4
High Yield
Examination of a 7-year-old boy reveals 20 degrees of valgus following a lawn mower injury to the lateral femoral epiphysis. Treatment consists of total distal femoral epiphyseodesis and varus osteotomy. Following surgery, he has a limb-length discrepancy of 3 cm and 5 degrees of genu valgum. Assuming that he undergoes no further treatment, the patient's predicted limb-length discrepancy at maturity would be how many centimeters?
Explanation
The distal femoral epiphysis grows approximately 1 cm per year and in boys, growth ceases at approximately age 16 years. Therefore, the patient's limb-length discrepancy at maturity would be 12 cm (9 cm plus the 3-cm discrepancy he has from the previous surgery). Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphyseodesis. J Pediatr Orthop 1996;16:173-179.
Question 5
What additional percentage of energy expenditure above baseline is required for ambulation after an above-the-knee amputation?
Explanation
Patients with an above-the-knee amputation have a 65% increase in energy expenditure. A patient with a transtibial amputation requires 25% more energy above baseline values; however, bilateral transtibial amputations are associated with a 40% increase in energy expenditure. Otis JC, Lane JM, Kroll MA: Energy cost during gait in osteosarcoma patients after resection and knee replacement and after above-the-knee amputation. J Bone Joint Surg Am 1985;67:606-611.
Question 6
High Yield
A 7-month-old girl has had a severe flatfoot deformity since birth. The talar head is prominent in the medial plantar arch of the foot. No other deformities of the spine or extremities are present. Motor and sensory examinations of the extremities are normal. Figures 37a through 37c show simulated weight-bearing AP and lateral radiographs and a planter flexion lateral view. What is the most likely diagnosis?



Explanation
Congenital vertical talus is a fixed dorsal dislocation of the talonavicular joint with equinus of the ankle joint. The AP radiograph shows valgus of the midfoot and an increased talocalcaneal angle; the lateral radiograph shows a vertically positioned talus and equinus of the ankle joint, and the plantar flexion lateral view shows that the talonavicular joint does not reduce. A line drawn through the long axis of the talus passes below the long axis of the first metatarsal. Initial management should consist of serial casting to stretch the dorsal soft-tissue structures; surgery eventually will be required to reduce the talonavicular joint. The differential diagnosis of congenital vertical talus includes pes calcaneovalgus, flexible pes planus, and peroneal spastic flatfoot. Pes calcaneovalgus, flexible pes planus, congenital short Achilles tendon, and peroneal spastic flatfoot would not show resistent dorsal dislocation of the navicular on the plantar flexion view. Kodros SA, Dias LS: Single-stage surgical correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Question 7
High Yield
A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?

Detailed Explanation
The patient has a scaphoid fracture involving the proximal pole. Surgical treatment is recommended for such fractures because of the prolonged period of cast immobilization necessary and the increased risk of delayed union, nonunion, and/or osteonecrosis with nonsurgical management. A cannulated compression screw, inserted in the central scaphoid via a dorsal approach, is biomechanically advantageous and provides greater stability for fracture healing than Kirschner wires. Recently, good outcomes have been reported with arthroscopic-assisted percutaneous fixation of nondisplaced or minimally displaced scaphoid fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210. Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79. Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.
Question 8
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of

Explanation
The arthroscopic image shows a tear through more than 50% of the biceps tendon; therefore, treatment should consist of tenodesis or tenotomy of the tendon. However, because this patient is relatively young and active, the treatment of choice is tenodesis of the biceps tendon. Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654. Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Question 9
A 42-year-old man has had left lower extremity pain in an L5 radicular pattern for the past 6 weeks. He denies significant axial low back pain. History reveals that he underwent an L4-5 diskectomy with successful relief of similar pain 5 years ago. Which of the following imaging studies would offer the greatest amount of information?
Explanation
MRI with gadolinium will best identify recurrent herniated nucleus pulposus or other root compression and distinguish scar from recurrent disk. CT is unable to distinguish scar from recurrent disk density, and the addition of myelogram dye can reveal compromise of the thecal sac but cannot distinguish the scar from recurrent disk as the source of compression. Although lateral flexion-extension radiographs may be important to rule out any instability, much of that information can be inferred from the associated disk and adjacent bony changes on MRI. Bone scan techniques may identify subtle stress fractures resulting from previous aggressive facet resection, but low back pain also would be expected. Mirowitz SA, Shady KL: Gadopentetate dimeglumine-enhanced MR imaging of the postoperative lumbar spine: Comparison of fat-suppressed and conventional T1-weighted images. Am J Roentgenol 1992;159:385-389.
Question 10
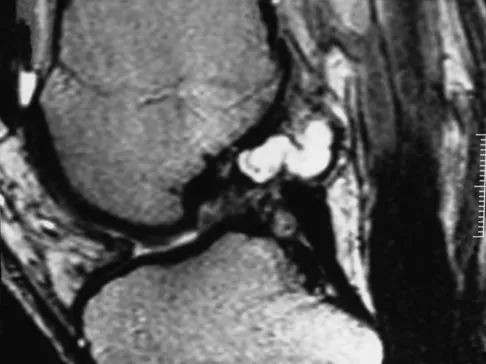
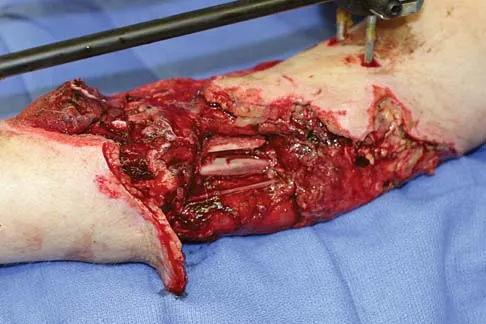
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of




Explanation
The diagnosis is synovial chondromatosis. While the plain radiograph fails to show any calcifications, the MRI scan shows an intra-articular mass that involves the capsule. Grossly multiple granular cartilage nodules are seen. Management should consist of removing all loose bodies along with the synovial membrane.
Question 11
High Yield
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 12
High Yield
A 35-year-old woman who is a recreational runner reports posterior knee pain and tightness in the knee with flexion during running. She denies any history of trauma. Examination reveals normal patellar glide and tilt and no patellar apprehension. Range of motion is 5 degrees to 120 degrees, and quadriceps function and knee ligamentous examination are normal. Radiographs are normal. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
Ganglia involving the cruciate ligaments have been recently reported as a cause of knee pain that interferes with knee flexion and extension. The symptoms are poorly localized in this patient and not along the medial joint line, making the diagnosis of a torn medial meniscus less likely. In addition, the MRI findings do not show a significant medial meniscal lesion. A Baker's cyst is usually posteromedial and extends posterior to the interval between the medial head of the gastrocnemius and semimembranosus. MRI scans show a fluid-filled lesion with an increased signal on T1- and T2-weighted images. A lipoma would be bright on the T1-weighted image only. Deutsch A, Veltri DM, Altchek DW, et al: Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy 1994;10:219-223.
Question 13
High Yield
Which of the following is considered a physiologic effect of anemia?
Explanation
The expected physiologic effects of anemia include an increased heart rate and increased cardiac output. The coronary blood flow requirement increases. There is a decrease in peripheral resistance and blood viscosity.
Question 14
High Yield
Design and manufacturing of a metal-on-metal articulation has an important influence on the tribology. Which of the following statements best characterizes the type of contact that is best for metal-on-metal articulations?
Detailed Explanation
It is important that the radii of a metal-on-metal head to cup articulation be such that there is polar contact. As the radii become closer to equal, conditions favor higher frictional torque and equatorial seizing. The "bedding in" of metal-on-metal surfaces and their stiffness are both components of the properties considered in the design of polar contact surfaces.
Question 15
Bioabsorbable polymers are used in a wide range of orthopaedic devices, including anchors, staples, pins, plates, and screws. What is the primary drawback for bioabsorbable implants?
Explanation
A number of bioabsorbable polymers are used in orthopaedic applications, and all have in common reports of foreign body reactions, which occur in more than 50% of patients in some series. In general, the high cost of these polymers is offset by the elimination of a second surgery to remove the implant. Bioabsorbable polymers are low strength in comparison to metallic alloys but of sufficient strength for many orthopaedic applications. The elastic modulus is not as high as many other orthopaedic biomaterials, making them suitable for applications where lower stiffness is an asset. Ambrose CG, Clanton TO: Bioabsorbable implants: Review of clinical experience in orthopedic surgery. Ann Biomed Eng 2004;32:171-177.
Question 16
When evaluating a patient with hallux rigidus, what is the most important clinical factor indicating the need for an arthrodesis as opposed to a cheilectomy?

Explanation
Cheilectomy has been shown to provide satisfactory pain relief and improved function in long-term studies. It is important to select patients appropriately when choosing a cheilectomy versus an arthrodesis. Pain at the midrange of motion and loss of more than 50% of the metatarsal head cartilage are predictors of a poor outcome following cheilectomy, and these patients should receive an arthrodesis. Coughlin MJ, Shurnas PS: Hallux rigidus: Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003;85:2072-2088.
Question 17
High Yield
What is the most common pediatric soft-tissue sarcoma?

Explanation
Soft-tissue sarcomas are the sixth most common cancer in children. Rhabdomyosarcoma is the most common type of pediatric soft-tissue sarcoma. Nearly 50% of rhabdomyosarcomas are diagnosed in children who are age 5 years or younger. Unfortunately, there has not been a significant increase in survival in children with metastatic rhabdomyosarcoma despite aggressive therapy including multiple-drug chemotherapy regimens.
Question 18
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?


Explanation
The history, examination, and radiographs are pathognomonic for Little League shoulder, a stress syndrome of the proximal humeral physis caused by overuse. Complete fracture rarely occurs, and recovery usually occurs with rest. Night pain is always a serious concern and further work-up is needed if the patient does not respond to activity modification. Occult instability is not a real concern in this patient, although it should be included in the differential diagnosis. Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Question 19
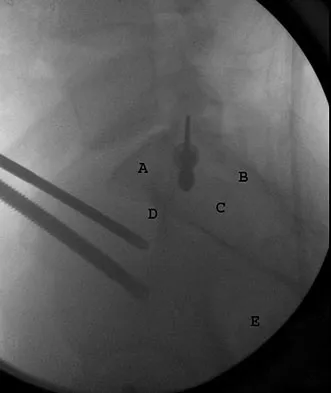
Figure 30 shows an axial cross section of extensor tendon anatomy in zone 7 of the wrist. What letter best depicts the location of the posterior interosseous nerve?

Explanation
The posterior interosseous nerve in contained in the floor of the fourth dorsal compartment of the wrist, which is labelled C in this diagram. Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 224.
Question 20
High Yield
Osteopenia is defined by the World Health Organization (WHO) as a bone mineral density (BMD) that is
Detailed Explanation
Osteopenia, decreased bone mass without fracture risk as defined by the WHO criteria for diagnosis of osteoporosis, is when a woman's T-score is within -1 to -2.5 SD. The T-score represents a comparison to young normals or optimum peak density. The Z-score represents a comparison of BMD to age-matched normals. Measurements of bone mineral density (BMD) at various skeletal sites help in predicting fracture risk. Hip BMD best predicts fracture of the hip, as well as fractures at other sites.
Question 21
High Yield
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?
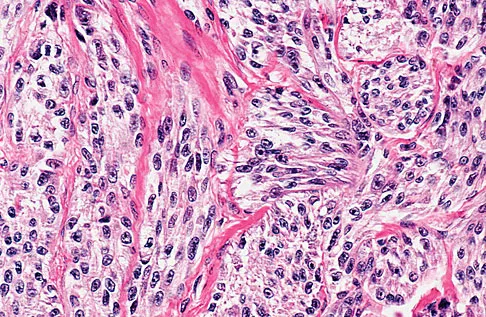
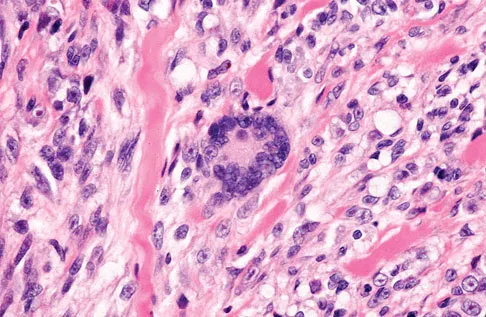
Explanation
The histologic appearance of the soft-tissue lesion reveals compact nests of cells with a clear cytoplasm surrounded by a delicate border of fibrocollagenous tissue. There can be scattered multinucleated giant cells. This is consistent with a clear cell sarcoma, also called malignant melanoma of soft parts. This tumor is usually positive for S-100 and HMB45 (a melanoma-associated antigen). These tumors are frequently found around the foot and ankle. Similar to epithelioid sarcoma, it is usually intimately bound to tendons or tendon sheaths. Often the tumors are present for many years. The classic histologic appearance of this lesion differentiates it from the other choices. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Question 22
High Yield
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include

Explanation
In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
Question 23
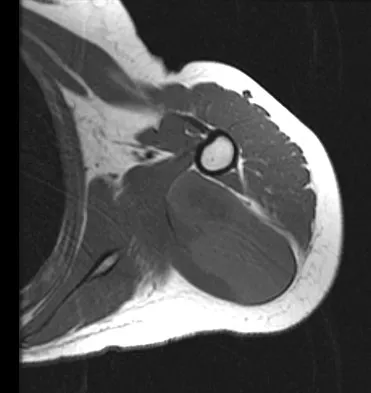
Figure 14 shows an intra-articular gadolinium-enhanced MRI scan of a 52-year-old woman who has stopped playing tennis because of pain in her left shoulder while serving. What is the most likely diagnosis?

Explanation
The MRI scan shows increased signal intensity along the deep fibers of the supraspinatus near its insertion. This is typical of tendinosis and a probable partial-thickness rotator cuff tear. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Question 24
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?


Explanation
The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 25
High Yield
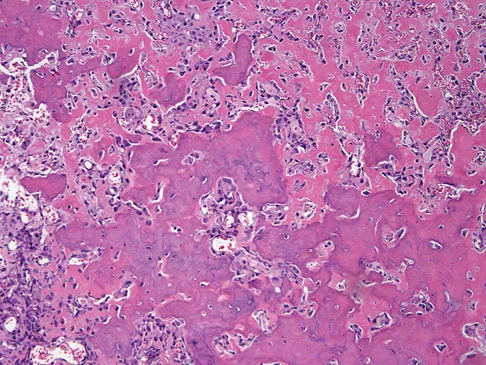
The biopsy specimens seen in Figures 55a and 55b are from a lytic lesion in the sacrum of a 58-year-old man. What is the most likely diagnosis?


Detailed Explanation
The lesion is a chordoma and the other listed choices can be eliminated based on the histology. Many tumors can occur in the sacrum including chordoma, multiple myeloma, giant cell tumor, aneurysmal bone cyst, and metastatic disease. The histology in this patient shows a lobulated lesion on low power with fibrous septae separating the lobules. At higher magnification, the cells have eosinophilic vacuolated cytoplasm and are called physaliferous cells. Chordoma is a low-grade neoplasm that most commonly occurs in the sacrum and rarely in the base of the skull. The diagnosis is often delayed. Chordoma is thought to originate from notochordal remnants. Chordoma typically occurs in the midline and has an associated soft-tissue mass. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 372. Fuchs B, Dickey ID, Yaszemski MJ, et al: Operative management of sacral chordoma. J Bone Joint Surg Am 2005;87:2211-2216.
Question 26
High Yield
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
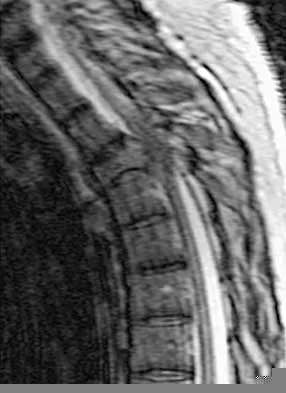
Explanation
Surgical decompression and stabilization have been shown to be the most effective means of improving neurologic function. Decompression is most reliably done from the side of the compression, which is anterior in this patient. Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Question 27
A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The preferred initial course of action should consist of
Explanation
Surgical decompression is unnecessary in a patient with no neurologic deficit and canal compromise of less than 50%. A compression deformity of less than 50% and kyphosis of less than 30 degrees may be successfully treated with a TLSO extension brace. Deformity in this range will reliably heal with minimal risk for late deformity or residual pain. Although some studies suggest 6 weeks of bed rest as treatment, early mobilization and bracing is preferred. Hartman MB, Chrin AM, Rechtine GR: Nonoperative treatment of thoracolumbar fractures. Paraplegia 1995;33:73-76. Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Question 28
High Yield
A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
Explanation
The patient likely has a significant Achilles contracture that causes her to always bear more weight on her forefoot. A gastrocnemius recession takes the ankle out of plantar flexion and she will be able to return to a normal gait and reduce the pressures on her forefoot. A forefoot amputation is a salvage option. The other choices are appropriate; however, the patient has had this problem for 2 years and she has already had multiple attempts at shoe wear modification. Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.
Question 29
High Yield
An otherwise healthy 35-year-old woman reports dorsal wrist pain and has trouble extending her thumb after sustaining a minimally displaced fracture of the distal radius 3 months ago. What is the next most appropriate step in management?
Explanation
Extensor pollicis longus tendon rupture can occur after a fracture of the distal radius, even a minimally displaced one. Poor vascularity of the tendon within the third dorsal compartment is the suspected etiology, not the displaced fracture fragments. Tendon transfer will suitably restore active extension of the thumb interphalangeal joint. Christophe K: Rupture of the extensor pollicis longus tendon following Colles fracture. J Bone Joint Surg Am 1953;35:1003-1005.
Question 30
High Yield
In the preoperative planning of revision acetabular reconstruction, the surgeon should identify significant posterior column deficiency by noting which of the following radiographic features?
Explanation
Proximal and medial migration of the femoral head usually indicates deficiencies of the dome or anterior column. Wear of the polyethylene may result in osteolysis and impingement, which are not indicative of any major bone deficiency. A significant osteolytic lesion in the ischium may represent a major posterior column deficiency that can create a technical challenge during the reconstruction. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 31
High Yield
The specificity of intraoperative frozen sections obtained for the evaluation of infected total hip arthroplasty may be improved by
Detailed Explanation
Lonner and associates conducted a prospective study to determine the reliability of analysis of intraoperative frozen sections for the identification of infection during 175 consecutive revision total joint arthroplasties (142 hips and 33 knees). The mean interval between the primary arthroplasty and the revision arthroplasty was 7.3 years (range, 3 months to 23 years). Of the 175 patients, 23 had at least 5 polymorphonuclear leukocytes per high-powered field on analysis of the frozen sections and were considered to have an infection. Of these 23 patients, five had 5 to 9 polymorphonuclear leukocytes per high-powered field and 18 had at least 10 polymorphonuclear leukocytes per high-powered field. The frozen sections for the remaining 152 patients were considered negative. On the basis of cultures of specimens obtained at the time of the revision surgery, 19 of the 175 patients were considered to have an infection. Of the 152 patients who had negative frozen sections, three were considered to have an infection on the basis of the results of the final cultures. Of the 23 patients who had positive frozen sections, 16 were considered to have an infection on the basis of the results of the final cultures; all 16 had frozen sections that showed at least 10 polymorphonuclear leukocytes per high-powered field. The sensitivity and specificity of the frozen sections were similar regardless of whether an index of 5 or 10 polymorphonuclear leukocytes per high-powered field was used. Analysis of the frozen sections had a sensitivity of 84% for both indices, whereas the specificity was 96% when the index was 5 polymorphonuclear leukocytes and 99% when it was 10 polymorphonuclear leukocytes. However, the positive predictive value of the frozen sections increased significantly (P < 0.05), from 70% to 89%, when the index increased from 5 to 10 polymorphonuclear leukocytes per high-powered field. The negative predictive value of the frozen sections was 98% for both indices. At least 10 polymorphonuclear leukocytes per high-powered field was predictive of infection, while 5 to 9 polymorphonuclear leukocytes per high-powered field was not necessarily consistent with infection. Less than 5 polymorphonuclear leukocytes per high-powered field reliably indicated the absence of infection. Feldman DS, Lonner JH, Desai P, Zuckerman JD: The role of intraoperative frozen sections in revision total joint arthroplasty. J Bone Joint Surg Am 1995;77:1807-1813. Lonner JH, Desai P, Dicesare PE, Steiner G, Zuckerman JD: The reliability of analysis of intraoperative frozen sections for identifying active infection during revision hip or knee arthroplasty. J Bone Joint Surg Am 1996;78:1553-1558. Spangehl MJ, Younger AS, Masri BA, Duncan CP: Diagnosis of infection following total hip arthroplasty, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 285-295.
Question 32
High Yield
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?

Detailed Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Question 33
Figure 6 shows the lateral radiograph of a 22-year-old woman who has painful Scheuermanns's kyphosis in the middle and lower thoracic spine. When planning surgical correction using instrumentation, the distal aspect of the instrumentation should ideally extend to the

Explanation
Posterior constructs for Scheuermann's kyphosis ideally should extend from the most superior to the most inferior aspect of the Cobb angulation. However, the most distal fusion level must be in a stable or lordotic position to avoid the development of junctional kyphosis. Lowe reported that failure to incorporate the first lordotic segment of the lumbar spine is associated with a higher risk of junctional kyphosis. The first lordotic segment of the lumbar spine is typically at least one level below the distal aspect of the curve as measured by the Cobb technique and most commonly is in the upper part of the lumbar spine. Lowe TG: Scheuermann's disease. Orthop Clin North Am 1999;30:475-487.
Question 34
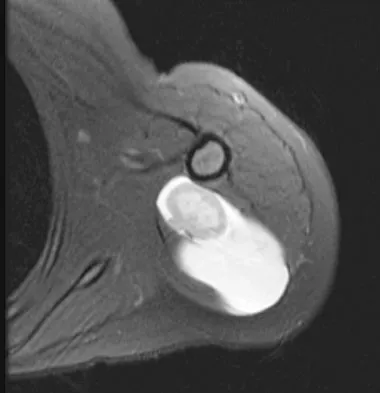
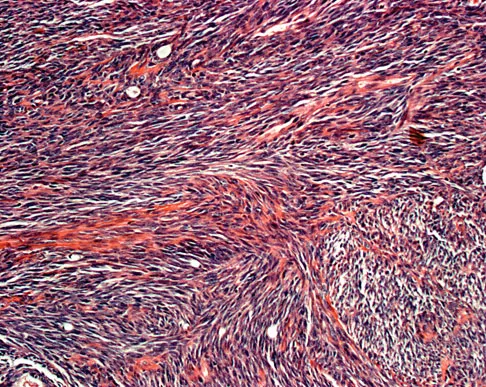
A 37-year-old man pulled his hamstring playing softball 3 weeks ago. The patient had not noted any mass prior to his injury. MRI scans of the posterior thigh are shown in Figures 4a and 4b. Figure 4c shows the biopsy specimen from a needle biopsy. What is the most likely diagnosis?



Explanation
Malignant fibrous histiocytoma (MFH) is the most common soft-tissue sarcoma. MFH typically presents as a large mass, deep to the fascia with heterogeneous signal on MRI. The MRI scans show a heterogeneous lesion in the posterior thigh. There is significant high signal uptake on the T2-weighted image. The histology shows malignant histiocytic cells with marked atypia and pleomorphism. Histology of a hematoma would show only old hemorrhage and some granulation tissue. Lipoma and liposarcoma are both seen as a fat-containing lesion on histology. No significant fat tissue is seen in this histologic specimen. Histology of myositis ossificans would show bone formation. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 35
High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 36
High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 37
High Yield
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to


Detailed Explanation
The radiograph shows a fracture distal to the prosthesis in a stable, apparently well-fixed prosthetic stem. The well-fixed prosthesis-bone composite is stiff, creating a modulus mismatch between the proximal and distal femur. Therefore, the risk of fracture, particularly in osteoporotic bone, is increased at this level. Revision of the stem to a longer construct is unnecessary, and standard plate and screw fixation has been shown to yield union rates of greater than 90%. Nonsurgical treatment of fractures distal to the tip of the prosthesis results in high nonunion rates, reported to be from 25% to 42%. Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 38
High Yield
A 3-year-old child has bilateral genu varum and short stature. Radiographs show physeal widening and generalized osteopenia. The femora and tibiae show anterolateral bowing. Laboratory studies show low normal serum calcium values, significantly decreased serum phosphate levels, and normal parathyroid hormone (PTH), alkaline phosphatase, and vitamin-D levels. These findings are consistent with
Detailed Explanation
Children with vitamin D-resistant rickets are short in stature and have genu varum, physeal widening, and generalized osteopenia. The abnormality in inherited vitamin D-resistant rickets is the renal tubule's inability to resorb phosphate leading to hypophosphatemia. Laboratory findings in the condition are normal or near normal serum calcium values, significantly decreased serum phosphate levels, elevated alkaline phosphatase levels, and normal PTH and vitamin-D levels. The most common form is inherited as an X-linked dominant trait. Nutritional rickets has a normal or low serum phosphate levels, normal or low serum calcium values, and decreased levels of 25(OH) vitamin D and 1,25-dihydroxyvitamin D. Hypophosphatasia is a rare condition characterized by a deficiency of alkaline phosphatase in the serum and tissues, leading to generalized abnormal mineralization of bone. Primary hyperparathyroidism usually is caused by a parathyroid adenoma, and the child generally has abdominal problems and hypercalcemic crisis. Laboratory findings include elevated serum calcium values, alkaline phosphatase levels, and PTH levels, and decreased serum phosphate levels. Children with renal osteodystrophy tend to have genu valgum, and laboratory findings include elevated serum phosphate, alkaline phosphatase, and PTH levels, and low serum calcium values. Findings of renal disease include elevated BUN and creatinine. Herring JA: Metabolic and endocrine bone diseases, in Herring JA (ed): Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, pp 1686-1710.
Question 39
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?

Explanation
An isolated tear of the subscapularis tendon has been noted as early as 1835 by Smith. In Gerber and associates' 1991 report of 16 men with an average age of 51 years, isolated subscapularis tendon rupture was often caused by a violent hyperextension injury. All patients reported pain anteriorly along with night pain. They also noted pain and weakness of the arm. The lift-off test is performed by having the patient lift the palm of the hand away from the small of the back. The patient must have sufficient internal rotation to allow this test to be performed. A subscapularis rupture is likely if the patient cannot perform the lift-off test. Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394. Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 40
A 17-year-old high school track athlete has had progressive midfoot pain for the past 3 weeks that prevents him from running. Examination reveals pain over the tarsal navicular. Radiographs are normal, but a CT scan reveals a nondisplaced sagittally oriented fracture line. Management should consist of
Explanation
The patient has a nondisplaced stress fracture of the tarsal navicular. Weight bearing is associated with a high rate of nonunion; therefore, management should consist of immobilization and no weight bearing for 8 weeks. Delayed union or nonunion is treated by excision of sclerotic fracture margins and bone grafting, with or without internal fixation. Generally, CT should be repeated to document healing before permitting a return to sports. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Question 41
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?



Explanation
The MRI scans show disruption of the fibers of the PCL. Patients sustaining an isolated acute PCL injury can present with only minimal discomfort and have full range of motion. When examination reveals a contusion over the tibial tubercle and discomfort with the posterior drawer examination, with or without instability, a possible injury to the PCL should be considered. In acute injuries, the reported accuracy of MRI imaging for diagnosing PCL tears ranges from 96% to 100%. Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 42
High Yield
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?



Explanation
The radiographs show a bone-producing lesion in the distal femoral metaphysis in this case of classic osteosarcoma presenting in the most common location, the distal femur. The coronal MRI scan reveals a marrow-occupying lesion with extension into the soft tissues. The histology shows osteoid production by pleomorphic cells consistent with an osteosarcoma. Ewing's sarcoma is a bone tumor characterized by uniform small blue cells on histology. Rhabdomyosarcoma is the most common childhood soft-tissue sarcoma. Osteomyelitis has an inflammatory appearance on histology. Malignant fibrous histiocytoma of bone has a lytic radiographic appearance and a pleomorphic storiform pattern without osteoid on histology. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
Question 43
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include "onion bulb" formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?

Explanation
The patient has HMSN-III or Dejerine-Sottas syndrome. This form of HMSN progresses very rapidly and frequently results in severe foot deformity in early childhood. The changes are progressive and are the result of muscle imbalance during growth. Balancing of the foot musculature is essential, particularly during the phases of rapid growth of the foot. However, this cannot be accomplished using the anterior tibial muscle because it is already weak and the transfer will further weaken it. Bony procedures also may be required, and tendon transfers cannot be depended on to correct bony deformity. However, these procedures can be deferred until the foot is closer to adult size. Surgeries that lead to joint arthrodesis, such as triple arthrodesis and some midfoot osteotomies, are contraindicated because the feet may lose protective sensation as the disease progresses. Fusions in insensate feet are less successful than realignment procedures that maintain mobility. Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Question 44
High Yield
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?

Explanation
During transaxillary resection of the first rib, the long thoracic nerve is at risk as it passes either through or posterior to the middle scalene muscle. Injury to this nerve may occur as the result of overly aggressive retraction of the middle scalene during the procedure. Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Question 45
What is the most common malignancy involving the hand?

Explanation
Skin cancers far outnumber primary musculoskeletal malignancies of the hand and the most common of these is squamous cell carcinoma. Metatastic lung carcinoma, while classic for the carcinoma that metastasizes to the hand, does so at an extremely low rate. Fink JA, Akelman E: Nonmelanotic malignant skin tumors of the hand. Hand Clin 1995;11:255-264.
Question 46
High Yield
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of



Detailed Explanation
Open reduction and subscapularis and lesser tuberosity transfer into the defect is the treatment of choice in young individuals who have defects that involve between 20% to 45% of the head. Disimpaction and bone grafting is an option in injuries that are less than 3 weeks old. Closed reduction 2 to 3 months after injury usually is unsuccessful and increases the risk of fracture or neurovascular injury. Total shoulder arthroplasty is reserved for defects of greater than 50% or with associated glenoid surface damage. Hemiarthroplasty should be avoided in young individuals unless 50% or more of the head is involved. Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Question 47
High Yield
A 17-year-old boy has had a mass in his right thigh for the past 6 months. He denies any history of trauma. Examination reveals that the mass is painless and firm. A radiograph and axial MRI scan are shown in Figures 49a and 49b. What is the most likely diagnosis?


Detailed Explanation
Osteochondroma typically occurs as a bony projection or a sessile growth on the bone, and there can be flaring of the metaphysis. The radiograph shows continuity from the adjacent cancellous bone into the lesion itself. There is no soft-tissue mass or bone destruction to suggest osteosarcoma or Ewing's sarcoma. Periosteal chondroma has a scalloped out radiographic appearance. Chondroblastoma typically is an epiphyseal-based lesion.
Question 48
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?

Explanation
The vertebral artery is contained within the vertebral foramen and thus tethered alongside the vertebral body, making it vulnerable to injury if a drill penetrates the lateral wall. The C5 root passes over the C5 pedicle and is not in the vicinity. The C6 root passes under the C5 pedicle but is posterior to the vertebral artery and is only vulnerable at the very posterior-inferior corner. The carotid artery and the vagus nerve are both within the carotid sheath and well anterior. Pfeifer BA, Freidberg SR, Jewell ER: Repair of injured vertebral artery in anterior cervical procedures. Spine 1994;19:1471-1474.
Question 49
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of

Explanation
In a subgroup of patients with monoarticular JRA and a limb-length discrepancy that developed before the age of 9 years, Simon and associates showed that a subsequent growth deceleration on the affected side may correct a large part of the difference in length. This possibility would make surgery unnecessary and should prompt further observation. Simon S, Whiffen J, Shapiro F: Leg-length discrepancies in monoarticular and pauciarticular juvenile rheumatoid arthritis. J Bone Joint Surg Am 1981;63:209-215.
Question 50
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in

Explanation
The elbow dislocates by a three-dimensional movement of supination and valgus during flexion. Additional trauma during reduction is minimized by recreating the deformity and reducing the elbow in supination. The actual maneuver includes full supination (actually hypersupination) of the elbow in a valgus position. This is followed by pushing the olecranon distally in line with the long axis of the ulna while swinging the elbow into varus, and then relaxing the supination torque. Postreduction stability is enhanced in pronation, except when the soft-tissue disruption is extensive. O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 414.
Question 51
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
The first extensor compartment of the wrist typically contains a single extensor pollicis brevis tendon and the abductor pollicis longus tendon that nearly always has multiple tendon slips. The extensor pollicis brevis tendon is frequently found to be separated from the slips of the abductor pollicis longus tendon by an intracompartmental septum. During surgery, this septum must be divided to complete the release of the compartment. Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM: Anatomical variations in the first extensor compartment of the wrist: A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-926.
Question 52
High Yield
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of

Explanation
The radiographs are classic for a Bennett's fracture, which involves a fracture of the palmar ulnar aspect of the proximal phalanx. This fracture fragment is still attached to the anterior oblique ligament. The deforming forces that cause subluxation of the base of the proximal phalanx include the pull of the abductor pollicis longus as well as the adductor pollicis. Adequate reduction can be achieved by closed reduction, percutaneous pin fixation, and casting. The fragment is too small for secure internal fixation. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Question 53
High Yield
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?

Detailed Explanation
Tillaux and triplane fractures occur in adolescents as the result of an external rotation injury of the ankle. As seen on the CT scan, the growth plate starts to close during adolescence; therefore, growth arrest resulting in limb-length discrepancy or angulation is less of a concern in this age group than achieving joint congruity. The joint should be surgically reduced if displacement is greater than 2 mm to minimize the chances of late arthrosis. Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-278. Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Question 54
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of



Explanation
The MRI scans show an os acromiale of the mesoacromion type. This represents an unfused acromial apophysis. Pain is thought to be caused by either motion at the site or downward displacement of the anterior aspect of the acromion onto the rotator cuff, causing impingement. Most patients can be treated nonsurgically as they are usually asymptomatic. In those patients with persistent symptoms of pain and tenderness over the acromion, surgery consisting of rigid internal fixation and bone grafting has yielded satisfactory results. Excision may be a viable treatment option for the preacromion type. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20. Warner JP, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 55
What is the 5-year overall survival rate for adults with high-grade soft-tissue sarcomas?
Explanation
The 5-year overall survival rate for deep, high-grade soft-tissue sarcomas is around 50%. The overall survival and disease-free survival rates chiefly depend on the tumor stage, but for all stages combined, most cancer treatment centers report a 5-year overall survival rate of around 70% and a disease-free survival rate of 65%. Fleming ID, et al: Manual for Staging of Cancer/American Joint Committee on Cancer, ed 5. Philadelphia, PA, Lippincott Raven, 1997, pp 149-156.
Question 56
A 20-year-old man sustained a closed tibial fracture and is treated with a reamed intramedullary nail. What is the most common complication associated with this treatment?

Explanation
The most common complication is anterior knee pain (57%). The knee pain is activity related (92%) and exacerbated by kneeling (83%). Although knee pain is the most common complication, most patients rate it as mild to moderate and only 10% are unable to return to previous employment. Some authors report less knee pain with a peritendinous approach when compared to a tendon-splitting approach. In one study, nail removal resolved pain in 27%, improved it in 70%, and made it worse in 3%. The incidence of the other complications was: infection 0% to 3%, nonunion 0% to 6%, and malunion 2% to 13%. Compartment syndrome is rare after nailing. Court-Brown CM: Reamed intramedullary tibial nailing: An overview and analysis of 1106 cases. J Orthop Trauma 2004;18:96-101. McQueen MM, Gaston P, Court-Brown CM: Acute compartment syndrome: Who is at risk? J Bone Joint Surg Br 2000;82:200-203.
Question 57
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
An inversion ankle injury typically involves ligamentous damage to the lateral ligaments of the ankle to include the anterior talofibular ligament and calcaneofibular ligament. Acute and particularly chronic ankle sprains also can have associated injuries. The inversion mechanism has been implicated in osteochondral and transchondral talar dome lesions, producing splits in the peroneus tendons, and in the development of meniscoid and soft-tissue impingement lesions in the anterolateral ankle. An inversion mechanism can also stretch the superficial peroneal nerve, leading to pain and paresthesias along its distribution. A fracture of the anterior colliculus is typically the result of an eversion mechanism resulting in a bony avulsion of the deltoid ligament from the anterior colliculus of the medial malleolus. Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Question 58
A 25-year-old man has ankle instability and a lateral foot callosity. Radiographs are shown in Figures 49a through 49c. Management options are best determined by the



Explanation
The patient has a cavovarus deformity that has resulted in lateral foot overload and stressing of the lateral ligaments. Further treatment depends on the ability to correct the deformity. The Coleman block test indicates whether a deformity is fixed or supple. A supple deformity will respond to orthotic management or soft-tissue procedures, while a fixed deformity requires corrective osteotomy or fusion. Physical therapy, casting, and injection will not address the underlying pathophysiology. There is no indication that this is a neuropathic problem.
Question 59
Duchenne's muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?

Explanation
Patients with Duchenne's muscular dystrophy show progressive muscular weakness because of the absence of dystrophin and have the clinical picture of progressive muscle weakness. The condition is an X-linked genetic disease. Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Question 60
High Yield
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
Hypophosphatemia is a rare genetic disease usually inherited as an X-linked dominant trait. The fact that the woman has no skeletal manifestations would indicate that the husband has the X-linked mutation. The disease is more severe in boys than it is in girls. The husband will not transmit the disease to his sons. However, all of their daughters will be affected either with the disease or as carriers. If the woman has the disease or the trait, there is a 50% chance that her sons will inherit the disease and a 50% chance that her daughters will be carriers or have a milder form of the disease. Parents should be advised to have genetic counseling so they can be informed when deciding whether to have children. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743. Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Question 61
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?




Explanation
The "sunburst" radiographic appearance suggests an osteosarcoma, and the histologic findings confirm the diagnosis with malignant cells surrounded by pink osteoid. MRI scans are not particularly helpful in the diagnosis of osteosarcoma but are mandatory for surgical planning. Osteosarcomas are high-grade sarcomas that are best treated with chemotherapy and wide resection. Even though the peroneal nerve is involved, limb salvage is indicated. Survival after limb salvage is equivalent to amputation, with better function. Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637. Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Question 62
The third plantar intrinsic muscle layer of the foot consists of which of the following structures?
Explanation
The plantar intrinsic muscles are divided into four layers with respect to depth from the plantar fascia. They are (from superficial to deep): 1) abductor hallucis, flexor digitorum brevis, abductor digiti minimi; 2) quadratus plantae, lumbricals; 3) flexor digiti minimi, flexor hallucis brevis, adductor hallucis brevis; and 4) dorsal and plantar interosseous muscles. The flexor hallucis brevis and adductor hallucis brevis originate from the midtarsal bones, encompass the sesamoids, and insert into the base of the proximal phalanx. The adductor hallucis brevis consists of two muscle bellies forming a conjoined tendon and inserting into the lateral portion of the proximal phalanx and the lateral sesamoid. The adductor hallucis brevis is stronger than the abductor hallucis brevis, which may contribute to hallux valgus. The flexor digitorum minimi travels under the fifth metatarsal, arising at the base and inserting into the lateral base of the fifth proximal phalanx.
Question 63
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of

Explanation
Monteggia fractures in children must be recognized. Early appropriate treatment is much easier than delayed reconstruction for a missed radial head dislocation. In younger children, attempts should be made to reduce the ulna fracture and radial head dislocation with traction and manual manipulation. Anterior Monteggia fractures are the most common, and in this variety the radius is much better stabilized in elbow flexion. Posterior Monteggia fractures are less common and may be managed in elbow extension. Closed reduction is much more successful in younger children; ulnar fixation with a rod or plate may be needed in older patients with unstable fractures. Annular ligament repair is rarely needed in the acute fracture. Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554. Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
Question 64
High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Question 65
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?

Explanation
It is common for patients with ankylosing spondylitis to sustain extension-type fractures, typically near the cervicothoracic junction. These fractures can be minimally displaced, making them difficult to diagnose. In addition, the vertebral bodies are vascular and their canals are relatively enclosed, making them vulnerable to epidural bleeding. The MRI scan shows an epidural hematoma posteriorly compressing the cord. Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142. Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 66
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
In a cadaver ligament sectioning study, the posterior capsular ligament was considered the most important structure for anterior-posterior stability of the sternoclavicular joint. The anterior capsular ligament also helps prevent anterior displacement but not to the same degree as the posterior ligament. The interclavicular ligament provides little support for anteroposterior translation. Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 67
High Yield
A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management?
Explanation
Displaced supracondylar humerus fractures in children may have associated vascular compromise. Decreased blood flow may be due to vessel injury, entrapment within the fracture site, kinking from fracture displacement, or from vessel spasm. Optimal initial treatment in the emergency department includes gentle realignment of the limb and vascular assessment. Angiography is not required in isolated injuries as the level of the vessel compromise is always at the site of the fracture. When blood flow is not restored, the next best step in treatment is to proceed urgently to the operating room. A formal closed reduction and pinning is performed, and then the vascular status is reassessed. Exploration and vascular repair is required if the hand is cool, white, and without pulses. Ay S, Akinci M, Kamiloglu S, et al: Open reduction of displaced pediatric supracondylar humeral fractures through the anterior cubital approach. J Pediatr Orthop 2005;25:149-153. Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 68
What is the most common complication following surgical fixation of a distal humeral fracture?

Explanation
In most series, elbow stiffness is the most common complication and can be overcome by achieving stable fixation and initiating early motion after surgery. All of the other complications are seen but to a lesser degree than elbow stiffness. Sanders RA, Raney EM, Pipkin S: Operative treatment of bicondylar intra-articular fractures of the distal humerus. Orthopedics 1992;15:159-163.
Question 69
Up to what time frame are the risks minimized in anterior revision disk replacement surgery?

Explanation
Revision anterior exposure within 2 weeks of total disk replacement incurs relatively little additional morbidity because adhesion formation is minimal. Surgeons should have a low threshold for revising implants that are clearly dangerously malpositioned or show early migration within this 2-week window. Beyond this time period, a revision strategy must be individualized to the particular clinical situation. A posterior fusion with instrumentation with or without a laminectomy is currently the most effective salvage procedure.
Question 70
High Yield
A 32-year-old woman has an isolated left posterior wall acetabular fracture in which about 25% of the wall surface is involved. Which of the following criteria would indicate the need for surgical reduction and fixation?
Explanation
Fractures with a posterior wall fragment that makes up less than one third of the surface generally are stable. Conversely, fractures with a fragment making up more than 50% of the surface are unstable. Patients with an intermediate fracture fragment should undergo a fluoroscopic examination under sedation or anesthesia to determine if the fragment is truly stable. If so, the patient can be treated nonoperatively and safely mobilized. Tornetta P III: Non-operative management of acetabular fractures: The use of dynamic stress views. J Bone Joint Surg Br 1999;81:67-70.
Question 71
High Yield
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Detailed Explanation
The failure load of an evenly tensioned four-stranded hamstring tendon autograft has been reported to be 4,500 Newtons. The failure load of a 10-mm patellar tendon autograft has been estimated at 2,600 Newtons. The intact anterior cruciate ligament failure load has been calculated at 1,725 Newtons. Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454. Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Question 72
A 2-year-old child is brought in by his parents for evaluation of intoeing. The child has a normal neuromuscular examination, but the heel bisector line is in the fourth web space, indicating a severe flexible metatarsus adductus deformity. The remainder of the lower extremity examination is unremarkable. What is the most appropriate treatment?

Explanation
Weinstein reported on 31 patients (45 feet) with congenital metatarsus adductus followed for an average of 33 years. Twenty-nine feet had moderate to severe deformities treated with manipulation and casting with a 90% success rate. In a young child, surgery is not indicated until nonsurgical management has failed. In patients 2 to 4 years of age, tarsometatarsal capsulotomies are indicated, whereas multiple metatarsal osteotomies are reserved for recalcitrant deformities in children older than 4 years of age. Mild or moderate metatarsus adductus that is passively correctable will resolve without treatment. Beaty J: Congenital anomalies of the lower extremity, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. Philadelphia PA, Mosby, 2003, pp 983-988. Katz K, David R, Soudry M: Below-knee plaster cast for the treatment of metatarsus adductus. J Pediatr Orthop 1999;19:49-50.
Question 73
High Yield
When performing ankle arthroscopy through the anterolateral portal, what anatomic structure is at greatest risk?
Explanation
The superficial branch of the peroneal nerve travels subcutaneously anterior to the lateral malleolus at the ankle. It can be easily damaged by deep penetration of the knife blade when making this portal or when passing shavers in and out of the portal. Anesthesia or dysesthesia from laceration or neuroma formation can cause significant postoperative morbidity. The anterior tibialis tendon, anterior tibial artery, and the deep peroneal nerve are located much more anterior and central on the ankle. The sural nerve is posterior lateral to the ankle and is not at risk from this portal. Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Question 74
High Yield
A 16-year-old girl has had painless swelling in her posterior left arm for the past 4 months. A radiograph, MRI scans, and an incisional biopsy specimen are shown in Figures 43a through 43d. What is the cytogenetic translocation most commonly associated with this tumor?

Explanation
This is a case of synovial sarcoma. The radiograph shows some soft-tissue swelling in the upper arm. The MRI scans show a lesion that has increased signal on T2-weighted images and low signal on T1-weighted images. There is a suggestion of a large cystic component to this lesion. The pathology shows a biphasic population of cells, a spindle cell component, and an epithelioid component. Up to 20% of synovial cell sarcomas have areas of cyst formation. The most common cytogenetic translocation with synovial cell sarcoma is X; 18. The 11; 22 translocation is most commonly associated with Ewing's sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Kawai A, Woodruff J, Healey JH, et al: SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. New Engl J Med 1998;338:153-160.
Question 75
An 18-year-old man sustains an injury to his lateral ankle after being kicked while playing soccer. He reports persistent pain on the lateral ankle as well as a popping sensation with attempted ankle dorsiflexion and eversion. Which of the following structures anatomically restrains the retracted structure shown in Figure 12?

Explanation
The peroneus brevis and peroneus longus muscles are the main evertors of the hindfoot. As they descend along the posterior fibula, they pass through the retromalleolar sulcus, formed by the concavity of the retromalleolar fibula. This sulcus is deepened by a fibrocartilaginous rim. The superior peroneal retinaculum covers the fibular groove and stabilizes the peroneal tendons within the retromalleolar sulcus. It originates from the posterolateral ridge of the fibula and inserts onto the lateral calcaneus. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 81-89.
Question 76
Figure 50 shows the AP radiograph of an asymptomatic 82-year-old woman who underwent total hip arthroplasty 16 years ago. What is the most likely diagnosis?

Explanation
Pelvic osteolysis in the presence of a well-fixed porous-coated socket is a recognized complication in total hip arthroplasty. The radiograph shows large lytic lesions superiorly adjacent to an acetabular screw and inferiorly extending into the ischium. It also reveals eccentricity of the femoral head with respect to the acetabular component, consistent with polyethylene wear. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 440.
Question 77
What is the most important factor regarding the risk of recurrent instability in a patient with an acute anterior dislocation of the shoulder?

Explanation
The recurrence rate of anterior dislocation of the shoulder after the first episode in athletes younger than age 20 years is thought to be as high as 90%, making surgery after the initial episode a consideration. The rate drops from 50% to 75% in the 20- to 25-year age group and down to 15% in patients older than age 40 years. An excellent prospective study of 257 patients in Sweden showed that there was no difference in those who did or did not complete 3 weeks of immobilization. The study also showed variability among different age groups in the importance of athletic participation; athletes in the 12- to 22-year age group had a higher recurrence rate, whereas the more sedentary patients in the 23- to 29-year age group had a higher rate. Hovelius L: The natural history of primary anterior dislocation of the shoulder in the young. J Orthop Sci 1999;4:307-317.
Question 78
High Yield
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?

Explanation
Pitchers tend to have a decrease in internal rotation and an increase in external rotation. The increase in external rotation is felt to be multifactorial. An increase in humeral retroversion occurs from repeated throwing. This results in increased soft-tissue stretching and results in a posterior capsular contracture. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Question 79
A 51-year-old woman has had progressively increasing right knee pain for the past 6 months. She has a history of metastatic renal cell carcinoma to the lung and the skeletal system. Radiographs are seen in Figures 18a and 18b. The next step in management of the right distal femur lesion should consist of


Explanation
In a patient with known metastatic disease, the surgeon must rule out additional lesions throughout the femur prior to surgical management. Lesions located in the diaphysis or in the peritrochanteric region may influence the surgical procedure. Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 80
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?


Explanation
The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 81
High Yield
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?

Explanation
The radiograph reveals osteonecrosis of both femoral heads with reasonably maintained joint surfaces. There may be some slight flattening of the femoral heads. Hip arthrodesis is difficult to perform because of the necrotic bone. Its use in patients with osteonecrotic hips is limited because of the 80% bilaterality; therefore, it is not an acceptable alternative. All the other options are acceptable interventions. Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 82
A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm3. What is the most common organism in this scenario?

Explanation
The most common bacterial etiologic agent following varicella is group A beta-hemolytic streptococcus. The other organisms are much less common. Staphylococcus aureus is the most common bone infection organism. Staphylococcus epidermidis is increasingly a bone infection organism. Group B streptococcus occurs more commonly in newborns. Kingella kingae is a common joint pathogen but is not as common following varicella. Schreck P, Schreck P, Bradley J, et al: Musculoskeletal complications of varicella. J Bone Joint Surg Am 1996;78:1713-1719.
Question 83
On MRI, a nonsanguinous effusion has what appearance?

Explanation
Nonbloody effusions that are greater than 1 mL are readily detected by MRI. They appear black on T1-weighted images and white on T2-weighted images. A sanguinous effusion is seen as white on T1-weighted images and black on T2-weighted images. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Question 84
High Yield
The anterolateral (Watson-Jones) approach to the hip exploits the intermuscular interval between the

Detailed Explanation
The Watson-Jones approach to the hip uses the intermuscular interval between the gluteus medius and the tensor fascia lata. This is not a true internervous plane, as both muscles are supplied by the superior gluteal nerve. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 316-332.
Question 85
The preferred surgical approach to the elbow of a child with an irreducible type III supracondylar distal humerus fracture and pulseless extremity is through which of the following muscle intervals?
Explanation
In a type III supracondylar distal humerus fracture of the elbow, the brachial artery can become incarcerated, yielding a pulseless extremity. In this situation, closed reduction may not be effective; therefore, open management is often necessary. The preferred surgical approach to the brachial artery and to this fracture is the anterior approach to the cubital fossa. The lacertus fibrosis is incised, and the dissection is carried out between the brachialis (musculocutaneous nerve) and the pronator teres (median nerve), mobilizing the brachial artery. Once the brachial artery is mobilized, the anterior elbow joint capsule may be exposed. The interval between the brachialis and the biceps describes the anterolateral approach to the elbow more commonly used for exposure of the proximal aspect of the posterior interosseous nerve. The dissection interval between the brachioradialis and the pronator teres describes the proximal extent of the anterior approach to the radius. Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 115.
Question 86
An 18-year-old collegiate basketball player has had a 3-month history of activity-related back pain. She describes isolated low back pain without radiation that increases with training and playing basketball. Her pain resolves with rest. Physical therapy for 6 weeks has failed to provide relief. An axial CT scan is shown in Figure 17a, and Figures 17b and 17c show sagittal CT reconstructions through the right and left lumbar facets, respectively. Further management should consist of which of the following?



Explanation
The sagittal and axial CT scans show a bilateral spondylolysis at L5. The defect is in the pars interarticularis on the right side but at the base of the pedicle on the left. Having failed a trial of physical therapy with only a 3-month history of pain, the next most appropriate step in management should consist of activity modification and bracing in an antilordotic lumbosacral orthosis. Surgical intervention is reserved for patients who have failed to respond to a trial of bracing and activity restriction. Debnath UK, Freeman BJ, Grevitt MP, et al: Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 2007;32:995-1000.
Question 87
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?

Explanation
The tibia has grown into valgus secondary to the proximal fracture. This occurs in about one half of these injuries, and maximal deformity occurs at 18 months postinjury. The deformity gradually improves over several years, with minimal residual deformity. Therefore, treatment at this age is unnecessary as there is a high rate of recurrence and complications regardless of technique. The valgus deformity is not a result of physeal injury or growth arrest. Medial proximal tibial hemiepiphysiodesis is an excellent method of correcting the residual deformity but is best reserved until close to the end of growth. Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482. McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 88
High Yield
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result?

Explanation
The radiographs show a fracture of the distal radius and ulna physis. The most likely complication is growth arrest of the distal ulna. In contradistinction to physis fractures of the radius (growth arrest incidence of less than 5%), the incidence of growth arrest in the ulna is between 30% and 40%. Entrapment of the EPL tendon and cross union between the two bones is extremely rare. Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120. Cannata G, De Maio F, Mancini F, et al: Physeal fractures of the distal radius and ulna: Long-term prognosis. J Orthop Trauma 2003;17:172-179. Ray TD, Tessler RH, Dell PC: Traumatic ulnar physeal arrest after distal forearm fractures in children. J Pediatr Orthop 1996;16:195-200.
Question 89
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause

Explanation
If the Buford complex is mistakenly reattached to the neck of the glenoid, severe painful restriction of external rotation will occur. Williams MM, Snyder SJ, Buford D Jr: The Buford complex - the "cord-like" middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 90
Which of the following structures is most commonly involved in lateral epicondylitis?
Explanation
The most common specific site of involvement is the origin of the extensor carpi radialis brevis. It is usually caused by overuse activities, such as the eccentric overload exhibited during a backhand in tennis. In most patients, the characteristic friable, grayish tissue described as angiofibroblastic hyperplasia or hyaline degeneration is seen at the extensor carpi radialis brevis origin. Nirschl RP: Elbow tendinosis/tennis elbow. Clin Sports Med 1992;11:851-870.
Question 91
High Yield
Following a vertebroplasty of L2, cement is noted to protrude directly anterior to the L2 vertebral body. The cement is closest to which of the following structures?
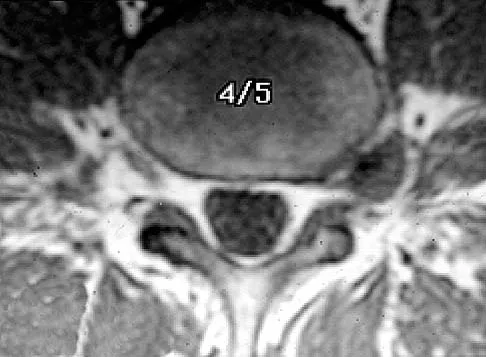
Explanation
At the level of L2, the liver and the vena cava lie to the right. The pancreas and duodenum are anterior to the aorta. The aorta lies in the midline just in front of the vertebral body. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 331.
Question 92
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of

Explanation
The CT scan shows a stress fracture of the olecranon. This injury is the result of repetitive abutment of the olecranon into the olecranon fossa, traction from triceps activity during the deceleration phase of the throwing motion, and impaction of the medial olecranon onto the olecranon fossa from valgus forces. Fractures may be either transverse or oblique in orientation. Initial treatment consists of rest and temporary splinting. Electrical bone stimulation may also be considered. Open fixation with a large compression screw is recommended when nonsurgical management has failed to provide relief. Ahmad CS, ElAttrache NS: Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med 2004;23:665-676.
Question 93
A newborn with bilateral talipes equinovarus undergoes serial manipulation and casting. What is the primary goal of manipulation?

Explanation
Manipulative treatment and casting of talipes equinovarus has become popular because of disappointing surgical results and enthusiasm for the Ponseti method of manipulation. In this technique, the primary goal is to rotate the foot laterally around a talus that is held fixed by the manipulating surgeon's hands. While the navicular may be rotated anterolaterally with this technique, the primary focus is on the calcaneus. The calcaneus is rotated laterally and superiorly, not translated. Some dorsiflexion of the calcaneus can be obtained by manipulation, but the primary focus is on the rotational relationship of the talus and calcaneus, not the degree of calcaneal dorsiflexion. Ponseti IV: Common errors in the treatment of congenital clubfoot. Int Orthop 1997;21:137-141.
Question 94
High Yield
The acceleration of an object under the influence of a force depends directly on the mass of the object. The angular acceleration of an object under the influence of a moment depends directly on the
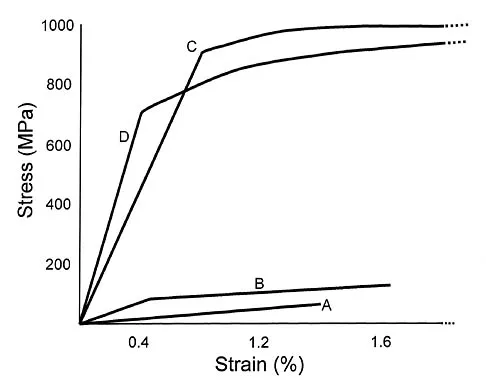
Explanation
Similar to the action of a force, a moment tends to angularly accelerate an object in a manner proportional to a quantity related to the mass of the object. The concept of a more massive object requiring a larger force to cause the same straight line acceleration is straightforward. The concept for changing angular velocity is similar but not identical. The proportional constant between the moment and the resulting angular acceleration is the mass moment of inertia, which depends not only on the mass of the object, but also its distribution. The unit of mass moment of inertia is obtained by multiplying the mass of the object by the square of the distance between an equivalent location of the center of rotation of the object and an equivalent location of the center of mass. Orthopaedic surgeons can change both the amount of mass carried by a limb and the way that the mass is distributed. For example, in applying a cast to the leg, the physician can affect the mass of the cast by the choice of casting material and by the size of the cast. As the mass moment of inertia of the limb increases (eg, by applying the cast farther down on the leg or using a heavier casting material), the patient will need to exert larger moments to angularly accelerate the leg during gait. Andriacchi T, Natarajan RN, Hurwitz DE: Musculoskeletal dynamics, locomotion, and clinical applications, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 43-47.
Question 95
A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
Explanation
The patient likely has a significant Achilles contracture that causes her to always bear more weight on her forefoot. A gastrocnemius recession takes the ankle out of plantar flexion and she will be able to return to a normal gait and reduce the pressures on her forefoot. A forefoot amputation is a salvage option. The other choices are appropriate; however, the patient has had this problem for 2 years and she has already had multiple attempts at shoe wear modification. Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.
Question 96
High Yield
A 29-year-old man reports severe knee instability and popliteal pain. History reveals that he had polio of the left lower extremity as a child and has been brace-free his entire life. Examination reveals that he walks with 40 degrees of knee hyperextension and has a fixed ankle equinus deformity of 30 degrees. He has no active motors about the knee or ankle. Which of the following methods will provide knee stability and pain relief?
Detailed Explanation
The ankle equinus allows the patient to keep his weight-bearing line anterior to the axis of the hyperextended knee joint. With time, pain has developed because of continued stretching and now incompetence of the posterior capsule of the knee joint. Several soft-tissue and bony procedures have been designed to provide knee stability in this situation; however, the results have been either short-lived or inconsistent. Tenodeses, capsular plications, and bony blocks have had limited success and generally fail over time. Current orthotic technology makes soft-tissue release and orthotic control the most predictable option. To decrease the hyperextension moment on the knee joint, the ankle deformity also must be corrected. The most predictable method of achieving stability and diminished pain during walking is with soft-tissue release of the ankle and a knee-ankle-foot orthosis with a locked ankle and drop-lock knee joint.
Question 97
High Yield
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a "lump" at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?

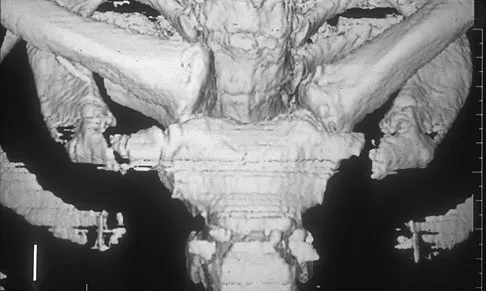
Explanation
Spontaneous subluxation of the sternoclavicular joint occurs without any significant trauma. It is usually accentuated by placing the extremity in an overhead position. Discomfort usually resolves within 4 to 6 weeks with nonsurgical management. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
Question 98
High Yield
A 53-year-old man has had a long history of multiple joint symptoms, and he notes that the worst pain is from his left shoulder. A radiograph and MRI scan are shown in Figures 13a and 13b. Prior to surgical treatment of the shoulder, what is the most appropriate work-up?

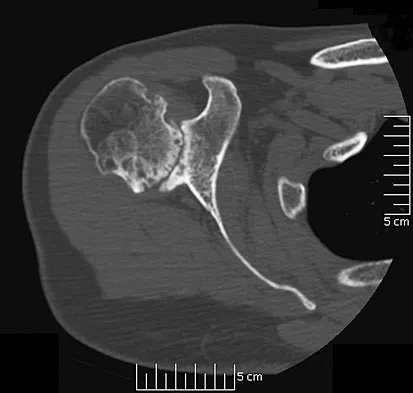
Explanation
Rheumatoid arthritis is sometimes associated with radiographic evidence of instability of the cervical spine. In a study by Grauer and associates, radiographs of the cervical spine of patients with rheumatoid arthritis who had undergone total joint arthroplasty over a 5-year period were retrospectively reviewed. Nearly one half of the patients had radiographic evidence of cervical instability on the basis of traditional measurements. While radiographic evidence of cervical instability was not infrequent in this population of patients who underwent total joint arthroplasty for rheumatoid arthritis, radiographic predictors of paralysis were much less common. MRI prior to surgery may also be a consideration if the radiographic appearance of the rotator cuff alters the consideration of surgical treatment. In a series of patients undergoing prosthetic arthroplasty for a variety of shoulder disorders, the presence of a rotator cuff tear has been shown to be associated with a less favorable outcome. Most often, the presence of a rotator cuff tear was associated with a diagnosis of rheumatoid or other inflammatory arthritis and the tears were large and generally irreparable. Some case series demonstrated a higher prevalence of loosening of the glenoid component in patients with a large rotator cuff tear associated with superior migration of the humeral head. However, obtaining an MRI scan of the shoulder is not considered the best response since failure to determine cervical instability may result in anesthetic death. Whereas MRI may be helpful in planning reconstruction, it would be a less important priority. Grauer JN, Tingstad EM, Rand N, et al: Predictors of paralysis in the rheumatoid cervical spine in patients undergoing total joint arthroplasty. J Bone Joint Surg Am 2004;86:1420-1424.
Question 99
High Yield
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic
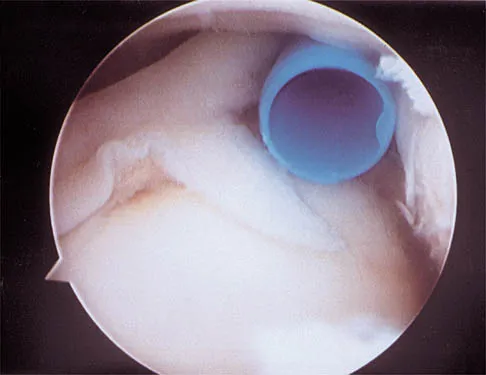
Explanation
The lesion is a variation of a type I superior labrum anterior and posterior lesion; therefore, appropriate treatment is simple debridement. Biceps tenodesis or release is not indicated because the biceps tendon and anchor are intact. There is no indication for labral repair or capsulorraphy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Question 100
High Yield
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Detailed Explanation
Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.
