Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 60-year-old man is evaluated in the ICU after a rollover motor vehicle accident 3 days ago. He has multiple upper and lower extremity trauma and was found unresponsive at the accident scene. Surgery is planned for the extremity trauma once the patient is medically stable. He remains intubated and the cervical spine is immobilized in a semi-rigid collar. Examination reveals mild erythema in the posterior occipital cervical region. Initial AP and lateral radiographs of the cervical spine have not revealed any obvious fracture. What is the most appropriate treatment option at this time?

Explanation
Ackland and associates demonstrated that the failure to achieve early spinal clearance in an unconscious blunt trauma patient predisposed the patient to increased morbidity secondary to the prolonged used of cervical immobilization. They demonstrated that the four significant predictors of collar-related ulcers were ICU admission, mechanical ventilation, the necessity for cervical MRI, and the time to cervical spine clearance and collar removal. The risk of pressure-related ulceration increased by 66% for every 1-day increase in Philadelphia collar time and this highlights the need for definitive C-spine clearance. Ackland HM, Cooper DJ, Malham GM, et al: Factors predicting cervical collar-related decubitus ulceration in major trauma patients. Spine 2007;32:423-428.
Question 2
High Yield
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?




Explanation
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Question 3
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
Neurologic injury after shoulder replacement is relatively uncommon, occurring in 4% of shoulders in one large series. The importance of identifying and protecting the musculocutaneous and axillary nerves cannot be overemphasized; it is especially critical during revision arthroplasty when the normal anatomic relationships have been distorted. The long deltopectoral approach leaving the deltoid attached to the clavicle was found to be significant in the development of postoperative neurologic complications. A correlation was found between surgical time and postoperative neurologic complications, with long surgical times being associated with more neurologic complications. The presumed mechanism of injury is traction on the plexus that occurs during the surgery. A neurologic injury after total shoulder arthroplasty usually does not interfere with the long-term outcome of the arthroplasty itself; it is best managed by protective measures with passive range of motion of the involved extremity. Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 4
High Yield
Lumbar instability may be surgically induced by
Explanation
In cadaveric studies, unilateral facetectomy, or excision of 50% or more of both facets, significantly decreases the biomechanic integrity of the motion segment and may increase the risk of iatrogenic instability. Sacrifice of the spinous process, interspinous ligaments, and ligamentum flavum weakens the motion segment but does not increase the risk for instability. Facetectomy, even unilateral, predisposes the patient toward lumbar instability.
Question 5
High Yield
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of

Explanation
Monteggia fractures in children must be recognized. Early appropriate treatment is much easier than delayed reconstruction for a missed radial head dislocation. In younger children, attempts should be made to reduce the ulna fracture and radial head dislocation with traction and manual manipulation. Anterior Monteggia fractures are the most common, and in this variety the radius is much better stabilized in elbow flexion. Posterior Monteggia fractures are less common and may be managed in elbow extension. Closed reduction is much more successful in younger children; ulnar fixation with a rod or plate may be needed in older patients with unstable fractures. Annular ligament repair is rarely needed in the acute fracture. Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554. Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
Question 6
High Yield
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?

Explanation
Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended. Herscovici D Jr, Widmaier J, Scaduto JM, et al: Operative treatment of calcaneal fractures in elderly patients. J Bone Joint Surg Am 2005;87:1260-1264. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 7
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the

Explanation
The radiographs show fractures of the coronoid and radial head. The medial collateral ligament has been avulsed from the ulnar insertion, and there is a valgus opening on the medial side. The lateral collateral ligament is always disrupted in elbow dislocations and fracture-dislocations that occur secondary to falls. This is known as the terrible triad injury (dislocation and fractures of the coronoid and radial head); it has a very poor prognosis because of its propensity for recurrent or persistent instability and late arthritis. The principle in treating this injury is to repair all of the injured parts or protect them with a hinged external fixator until they heal. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 8
The oblique radiograph of the foot and the CT scan shown in Figures 10a and 10b show a patient whose symptoms have failed to respond to rest and non-steroidal anti-inflammatory drugs. What is the best course of action?


Explanation
The radiograph and MRI scan show elongation and fragmentation of the os peroneum. Although casting, orthoses, and steroid injection may relieve symptoms, excision of the os peroneum and primary repair when necessary, with or without tenodesis of the peroneus longus to the peroneus brevis, have been shown to produce excellent results. Haddad SL: Disorders of tendons: Peroneal tendon dysfunction, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 812-817.
Question 9
High Yield
Which of the following is considered the best cementless acetabular reconstruction method when planning for total hip arthroplasty in a patient with developmental dysplasia of the hip (DDH)?

Explanation
Anatomic positioning of the acetabular component has been shown to be the optimal position for reconstruction of the acetabulum in total hip arthroplasty for DDH. The use of medialized component positioning has been shown to be successful at maximizing the host bone coverage and minimizing the use of bone graft to structurally support the acetabular component. A small acetabular component can be used successfully as long as the femoral head is also reduced in size to maintain the thickness of the acetabular polyethylene. High and lateral positioning for the acetabular reconstruction will result in an increase in the joint reaction forces. In addition, a high and lateral placement will not provide adequate bone to stabilize the reconstruction. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360. Dorr LD, Tawakkol S, Moorthy M, Long W, Wan Z: Medial protrusio technique for placement of a porous-coated, hemispherical acetabular component without cement in a total hip arthroplasty in patients who have acetabular dysplasia. J Bone Joint Surg Am 1999;81:83-92.
Question 10
When compared with the normal anterior cruciate ligament (ACL), placement of an anterior cruciate ligament graft in the over-the-top position on the femoral side has what effect on its function?
Explanation
The placement of ACL graft with respect to its femoral and tibial attachments has a significant effect on its function. Evidence has shown that if the graft is placed in the over-the-top position, the graft will become lax in flexion and more taut with extension. Conversely, if the graft is placed too anterior on the femoral side, it will tighten in flexion and become lax in extension. Azar FM: Revision anterior cruciate ligament reconstruction. Instr Course Lect 2002;51:335-342. Draganich LF, Hsieh YF, Sherwin SH, et al: Intra-articular anterior cruciate ligament graft placement on the average most isometric line on the femur: Does it reproducibly restore knee kinematics? Am J Sports Med 1999;27:329-334.
Question 11
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient's left knee. Abnormal findings include


Explanation
The MRI scans show meniscal tissue extending across the entire lateral compartment, revealing a discoid lateral meniscus. The increased signal within the lateral meniscal tissue indicates a tear. Discoid lateral menisci are congenital variants that often present with mechanical symptoms in adolescents. The other structures in the knee are normal. Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Question 12
High Yield
When performing ankle arthroscopy through the anterolateral portal, what anatomic structure is at greatest risk?
Explanation
The superficial branch of the peroneal nerve travels subcutaneously anterior to the lateral malleolus at the ankle. It can be easily damaged by deep penetration of the knife blade when making this portal or when passing shavers in and out of the portal. Anesthesia or dysesthesia from laceration or neuroma formation can cause significant postoperative morbidity. The anterior tibialis tendon, anterior tibial artery, and the deep peroneal nerve are located much more anterior and central on the ankle. The sural nerve is posterior lateral to the ankle and is not at risk from this portal. Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Question 13
High Yield
Which of the following is associated with the use of bisphosphonates in the setting of metastatic breast cancer to the spine?
Explanation
The indications of bisphosphonate therapy in breast cancer patients range from the correction of hypercalcemia to the prevention of cancer treatment-induced bone loss. Bisphosphonates reduce metastatic bone pain in at least 50% of patients and can reduce the frequency of skeletal-related events by 30% to 40%. Osteonecrosis of the jaw could occur in up to 2.5% of breast cancer patients during long-term bisphosphonate therapy.
Question 14
High Yield
A 22-year-old college quarterback is tackled and sustains a reducible first carpometacarpal dislocation. What is the recommended treatment?
Explanation
When comparing closed reduction and pinning to ligament reconstruction, the reconstruction group had slightly better abduction and pinch strength. The volar oblique ligament usually tears off the first metacarpal in a subperiosteal fashion. In this young patient, motion-sparing procedures are preferred. Simonian PT, Trumble TE: Traumatic dislocation of the thumb carpometacarpal joint: Early ligamentous reconstruction versus closed reduction and pinning. J Hand Surg Am 1996;21;802-806.
Question 15
High Yield
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient's family reports that he is a Jehovah's Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient's blood pressure becomes unstable. What is the most appropriate action?
Explanation
Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah's Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah's Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open would is not recommended nor would there likely be enough from an open tibial fracture to salvage. The patient's family may be expressing their own beliefs rather than the patient's beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability. Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 16
High Yield
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of

Detailed Explanation
Fractures of the hook of the hamate frequently are not identified in the acute phase. Because the fracture can be difficult to see on plain radiographs, the lack of findings can lead to a painful nonunion. A carpal tunnel view may show the fracture, but a CT scan will best detect the injury. Immobilization is the treatment of choice and will result in union in most patients unless the diagnosis is delayed. However, excision of the fragment may be necessary for patients who have nonunion, persistent pain, or ulnar nerve palsy. Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Question 17
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?

Explanation
The radiograph reveals osteonecrosis of both femoral heads with reasonably maintained joint surfaces. There may be some slight flattening of the femoral heads. Hip arthrodesis is difficult to perform because of the necrotic bone. Its use in patients with osteonecrotic hips is limited because of the 80% bilaterality; therefore, it is not an acceptable alternative. All the other options are acceptable interventions. Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 18
High Yield
Which of the following is considered a major characteristic of hyaluronate?
Explanation
Hyaluronate is a naturally occurring compound that is the backbone of the central core of the proteoglycan aggregate. Cartilage is made of two principal tissue structures. The connective tissue component includes collagen, which forms the framework for structural strength and elasticity. The proteoglycan aggregate provides a unique property of water incorporation and friction reduction capabilities. Hyaluronate forms the base or central core of the aggregate on which a link protein binds a protein core. Chondroitin sulfate and keratin sulfate are then bound to this protein core, forming the terminal extension of the aggregate. Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 69-78. Felson DT: Osteoarthritis. Rheum Dis Clin North Am 1990;16:499-512.
Question 19
High Yield
Which of the following substances is least likely to affect the success of bone union after lumbar arthrodesis?

Detailed Explanation
Much attention has been given to the use of supplemental postoperative analgesia with nonsteroidal anti-inflammatory drugs (NSAIDs), and a significant reduction in narcotic use has been recorded. However, a high failure rate of arthrodesis has been associated with the use of postoperative NSAIDs. Glassman and associates reported 29 cases of pseudarthrosis in 167 patients when ketorolac was used as a postoperative analgesic, whereas only five fusion failures were noted in 121 patients not using ketorolac. Indomethacin and ibuprofen have been shown to adversely affect bone formation in clinical and animal trials. Nicotine has also been shown in a number of studies to decrease the fusion rate. Oxycodone hydrochloride is a synthetic morphine and does not affect the fusion process. Glassman SD, Rose SM, Dimar JR, Puno RM, Campbell MJ, Johnson JR: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838. Deguchi M, Rapoff AJ, Zdeblick TA: Posterolateral fusion for isthmic spondylolisthesis in adults: Analysis of fusion rate and clinical results. J Spinal Disord 1998;11:459-464.
Question 20
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 21
High Yield
A 6-month-old child is seen in the emergency department with a spiral fracture of the tibia. The parents are vague about the etiology of the injury. There is no family history of a bone disease. In addition to casting of the fracture, initial management should include
Explanation
Unwitnessed spiral fractures should raise the possibility of child abuse, especially prior to walking age. With nonaccidental trauma being considered in the differential diagnosis, a skeletal survey is indicated to determine if there are other fractures in various stages of healing. Kempe CH, Silverman FN, Steele BF, et al: The battered-child syndrome. JAMA 1962;181:17-24.
Question 22
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
Although technically challenging, the Ganz periacetabular osteotomy offers advantages over other rotational pelvic osteotomies. Posterior column integrity is maintained, as is the acetabular vascular supply. Free mobility of the fragment makes large corrections in the center edge angle possible. Because of the asymmetric cuts and the need to restore anterior coverage, there is a tendency to anterior displacement of the joint while flexing the acetabulum. The procedure is commonly performed through a Smith-Petersen incision. Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 23
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of

Explanation
The radiograph shows excessive thoracic kyphosis (normal 20 degrees to 50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann's kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann's kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees. Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248. Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Question 24
High Yield
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child's back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of

Explanation
Congenital anomalies of the spine, including failure of formation and failure of segmentation, are associated with other anomalies in other organ systems that develop at the same time. These include anomalies in the genitourinary system, cardiac anomalies, Sprengel's deformity, radial hypoplasia, and gastrointestinal anomalies including imperforate anus and trachealesophageal fistula. Spinal dysraphism is the most common associated abnormality. McMaster found an 18% incidence before the common use of MRI. Bradford and associates reported on 16 of 42 patients with congenital spinal anomalies and spinal dysraphism using MRI. Neural axis lesions may be associated with visible midline abnormalities such as a hairy patch or nevus. The child has already had a cardiac and renal work-up, and based on the findings of the hairy patch and congenital vertebral anomalies, MRI of the entire spine is prudent at this time. Spinal fusion is indicated for progressive congenital scoliosis or kyphosis. Physical therapy does not affect the natural history of congenital scoliosis. McMaster MJ: Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am 1984;66:588-601. Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 25
High Yield
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
Explanation
The annulus fibrosis has a multilayer lamellar architecture mode of type I collagen fibers. Each successive layer is oriented at 30 degrees to the horizontal in the opposite direction, leading to a "criss-cross" type pattern. This composition allows the annulus, which has the highest tensile modulus, to resist torsional, axial, and tensile loads.
Question 26
Osteonecrosis of the femoral head after intramedullary nailing in children is thought to be the result of injury to the

Explanation
All of these are possible explanations for the development of osteonecrosis following intramedullary nailing in children. However, the lateral ascending cervical artery, which supplies the epiphysis, is much more vulnerable to injury in children because it lies in the trochanteric fossa. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
Question 27
High Yield
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of

Detailed Explanation
Immediate spica casting is ideal for younger children with uncomplicated femoral fractures that are the result of relatively low-energy injury. Surgical stabilization of pediatric femoral fractures is most commonly performed in children who are older than age 6 years or in children with other factors associated with their femoral fracture, such as concomitant head injury, open fracture, floating knee, severe comminution, or vascular injury. Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659. Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365. Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Question 28
High Yield
A corset-type brace may help reduce symptoms during an episode of acute low back pain as the result of
Explanation
Although there is no significant alteration in motion with a corset, studies have shown a decrease in intradiskal pressure. Nachemson A, Morris JM: In vivo measurements of intradiscal pressure: Discometry, a method for determination of pressure in the low lumbar disc. J Bone Joint Surg Am 1964;46:1077-1092.
Question 29
A 40-year-old right hand-dominant construction worker has had a 6-month history of aching left shoulder pain that is worse after working a long day. Examination reveals limited range of motion and good strength when compared to his asymptomatic right arm. He has not had any orthopaedic intervention to date. Radiographs are shown in Figures 43a and 43b. What is the most appropriate treatment?


Explanation
The patient is a young laborer with osteoarthritis. Initial treatment should begin with nonsurgical management that may include anti-inflammatory drugs, cortisone injections, and physical therapy to diminish pain and improve motion. The other choices may eventually be necessary but should only follow a course of nonsurgical management. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Question 30
High Yield
The acceleration of an object under the influence of a force depends directly on the mass of the object. The angular acceleration of an object under the influence of a moment depends directly on the
Explanation
Similar to the action of a force, a moment tends to angularly accelerate an object in a manner proportional to a quantity related to the mass of the object. The concept of a more massive object requiring a larger force to cause the same straight line acceleration is straightforward. The concept for changing angular velocity is similar but not identical. The proportional constant between the moment and the resulting angular acceleration is the mass moment of inertia, which depends not only on the mass of the object, but also its distribution. The unit of mass moment of inertia is obtained by multiplying the mass of the object by the square of the distance between an equivalent location of the center of rotation of the object and an equivalent location of the center of mass. Orthopaedic surgeons can change both the amount of mass carried by a limb and the way that the mass is distributed. For example, in applying a cast to the leg, the physician can affect the mass of the cast by the choice of casting material and by the size of the cast. As the mass moment of inertia of the limb increases (eg, by applying the cast farther down on the leg or using a heavier casting material), the patient will need to exert larger moments to angularly accelerate the leg during gait. Andriacchi T, Natarajan RN, Hurwitz DE: Musculoskeletal dynamics, locomotion, and clinical applications, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 43-47.
Question 31
Figures 21a and 21b show the clinical photograph and radiograph of a 15-year-old girl who has a deformity of her feet. Her parents are concerned because there is a family history of Charcot-Marie-Tooth disease. The patient reports some mild instability of the ankle and has noticed mild early callosities; however, she is not having any significant pain. Coleman block testing reveals a forefoot valgus and supple hindfoot. She has weakness to eversion and dorsiflexion. Initial management should consist of


Explanation
Initial management of a young patient with a cavovarus deformity of the foot and a family history of Charcot-Marie-Tooth disease should focus on mobilization and strengthening of the weakening muscular units and an accommodative insert. Surgical intervention should be delayed until progression of the deformity begins to cause symptoms and/or weakness of the muscular units, resulting in contractures of the antagonistic muscle units. Pinzur MS: Charcot's foot. Foot Ankle Clin 2000;5:897-912. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 32
High Yield
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel's sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
The examination findings reveal that there is specific involvement of the medial plantar nerve by the distribution of the pain medially. The symptoms exclude the possibility of plantar fasciitis and anterior tibial tendinitis. Sinus tarsi syndrome would produce anterolateral symptoms rather than medial symptoms. Rask MR: Medial plantar neurapraxia (jogger's foot): Report of three cases. Clin Orthop 1978;134:193-195. Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Question 33
High Yield
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
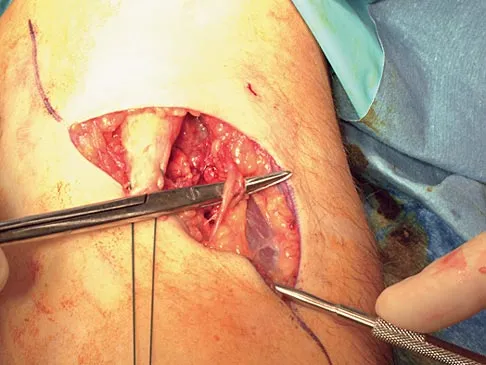
Explanation
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach. Kelly EW, Morrey BF, O'Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Question 34
High Yield
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T1- and T2-weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?
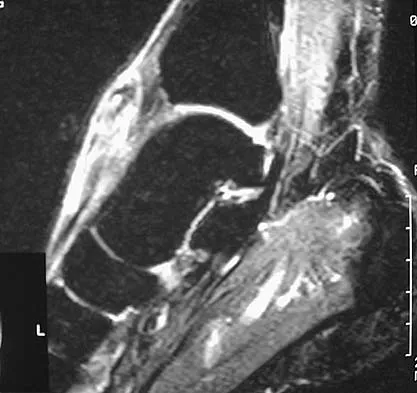


Explanation
The findings are most consistent with a rupture of the anterior tibial tendon. The damaged area of tendon should be resected, followed by tendon reconstruction or tenodesis. The histology is not consistent with giant cell tumor of the tendon sheath, gout, or synovial sarcoma. Fibromatosis is characterized by a large number of spindle cells within the collagen background. Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Question 35
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 36
A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness?
Explanation
Chronic subscapularis tendon ruptures preclude primary repair. In such instances, subcoracoid pectoralis major tendon transfers may improve function and diminish pain. The subcoracoid position of the transfer allows redirection of the pectoralis major in a direction recreating the vector of the subscapularis tendon. Shoulder fusion is a salvage procedure, and corticosteroid injection may reduce pain but will not improve function. Jost B, Puskas GJ, Lustenberger A, et al: Outcome of pectoralis major transfer for the treatment of irreparable subscapularis tears. J Bone Joint Surg Am 2003;85:1944-1951.
Question 37
High Yield
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?


Explanation
The radiographs reveal nonunion of a talar neck fracture. There is no radiographic evidence of osteonecrosis or significant degenerative arthritis. The results of talectomy are suboptimal. Arthrodesis would be indicated for degenerative arthritis. Revision ORIF is feasible and preserves motion. A vascularized graft should be considered whenever osteonecrosis is present, but the talar body appears viable in this case. Calvert E, Younger A, Penner M: Post talus neck fracture reconstruction. Foot Ankle Clin 2007;12:137-151.
Question 38
A 28-year-old cowgirl was injured while herding cattle 1 week ago. A radiograph and CT scans are shown in Figures 13a through 13c. What is the most appropriate management for this injury?



Explanation
The patient has an AP I pelvic ring disruption with minimal symphyseal widening. The best treatment is nonsurgical management and weight bearing as tolerated. This will help close the anterior pelvic ring during the healing process. Pelvic binders are excellent for acute treatment of widely displaced pelvic fractures but are not recommended for long-term use. Open reduction and internal fixation is not indicated for this injury and furthermore, the posterior ring is not injured. Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96. Templeman DC, Schmidt AH, Sems SA, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Question 39
A 100-lb 9-year-old boy has a closed midshaft transverse femoral fracture. The oblique fracture is shortened by 3 cm with a 10-degree varus angulation. Surgical management consists of intramedullary, retrograde flexible titanium nailing. To optimize fracture stability, the surgeon should
Explanation
The technique of intramedullary nailing with titanium elastic nails is based on the concept of balanced forces across the fracture site with two equally sized nails. Implantation of the largest sized nails possible, with two equally sized nails, maximizes the stiffness at the fracture site, thereby optimizing fracture alignment and stability. Impacting the nails into the medullary canal can impact the fixation by minimizing distal purchase of the nail at the cortical insertion site. Closed reduction commonly permits bony reduction and passage of the nails; open reduction is reserved for inability to align the fracture. Luhmann SJ, Schootman M, Schoenecker PL, et al: Complications of titanium elastic nails for pediatric femur fractures. J Pediatr Orthop 2003;23:443-447. Lascombes P, Haumont T, Journeau P: Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop 2006;26:827-834.
Question 40
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and

Explanation
The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures. Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424.
Question 41
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Explanation
In bone defects where host bone support is less than 50%, the failure rate is 70% at 5.1 years. The presence or absence of columns or hip position is of relatively little importance if the supportive bone is not present in at least 50% of the surface area around the future acetabular implant.
Question 42
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?


Explanation
The histologic appearance of the soft-tissue lesion reveals compact nests of cells with a clear cytoplasm surrounded by a delicate border of fibrocollagenous tissue. There can be scattered multinucleated giant cells. This is consistent with a clear cell sarcoma, also called malignant melanoma of soft parts. This tumor is usually positive for S-100 and HMB45 (a melanoma-associated antigen). These tumors are frequently found around the foot and ankle. Similar to epithelioid sarcoma, it is usually intimately bound to tendons or tendon sheaths. Often the tumors are present for many years. The classic histologic appearance of this lesion differentiates it from the other choices. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Question 43
A 10-year-old girl has a right elbow deformity that is the result of trauma 5 years ago. She has no pain despite the arm deformity. The radiographs in Figures 42a and 42b show complete healing. This radiographic appearance demonstrates what complication?


Explanation
Cubitus varus is a common complication of displaced supracondylar humeral fractures that are treated with closed reduction and cast immobilization. Treatment with closed reduction and percutaneous pinning decreases the incidence of this complication. Cubitus varus also can occur in minimally displaced fractures when unrecognized collapse of the medial column of the distal humerus is not corrected with manipulation. This can be detected on physical examination of the carrying angle or on radiographs measuring Baumann's angle, both in comparison to the opposite side. Cubitus varus may result in unacceptable cosmesis and may predispose the patient to fractures of the lateral condyle. The lateral radiograph demonstrates the crescent sign from overlap of the distal humerus with the olecranon seen in patients with cubitus varus. Patients with growth arrest to the medial trochlear physis would have atrophy of the trochlea on radiographs. Flynn JM, Sarwark JF, Waters PM, et al: The surgical management of pediatric fractures of the upper extremity. Instr Course Lect 2003;52:635-45. Papandrea R, Waters PM: Posttraumatic reconstruction of the elbow in the pediatric patient. Clin Orthop 2000;370:115-126.
Question 44
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?

Explanation
Tillaux and triplane fractures occur in adolescents as the result of an external rotation injury of the ankle. As seen on the CT scan, the growth plate starts to close during adolescence; therefore, growth arrest resulting in limb-length discrepancy or angulation is less of a concern in this age group than achieving joint congruity. The joint should be surgically reduced if displacement is greater than 2 mm to minimize the chances of late arthrosis. Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-278. Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Question 45
High Yield
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of


Detailed Explanation
The patient has grade IV heterotopic ossification with the limb in an abnormal nonfunctional position. Treatment should consist of excision of the bone to restore hip motion and prophylaxis to prevent recurrent formation. The best time to excise the bone is controversial, with no conclusive evidence supporting early or late excision. Pellegrini VD Jr, Koniski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 46
What is the most important factor regarding the risk of recurrent instability in a patient with an acute anterior dislocation of the shoulder?

Explanation
The recurrence rate of anterior dislocation of the shoulder after the first episode in athletes younger than age 20 years is thought to be as high as 90%, making surgery after the initial episode a consideration. The rate drops from 50% to 75% in the 20- to 25-year age group and down to 15% in patients older than age 40 years. An excellent prospective study of 257 patients in Sweden showed that there was no difference in those who did or did not complete 3 weeks of immobilization. The study also showed variability among different age groups in the importance of athletic participation; athletes in the 12- to 22-year age group had a higher recurrence rate, whereas the more sedentary patients in the 23- to 29-year age group had a higher rate. Hovelius L: The natural history of primary anterior dislocation of the shoulder in the young. J Orthop Sci 1999;4:307-317.
Question 47
High Yield
What clinical parameter will most likely decrease the need for blood transfusion after total joint arthroplasty?
Detailed Explanation
Bilateral joint replacement, chronic disease, and preoperative autologous donation all increase the risk of needing blood. Young patients and a high hemoglobin level (greater than 15 g/dL) are considered clinical parameters that decrease the risk for requiring allogenic blood. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 48
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
Although pseudarthrosis can be found anywhere within the spine that has been fused using long multisegmental fixation to the sacrum, it most commonly occurs at the lumbosacral junction. The thoracolumbar junction is another common site of potential pseudarthrosis. In this location, the anatomy changes from lumbar transverse processes to thoracic through the transition zone, and overlying instrumentation often makes it difficult to obtain enough sound bone on decorticated bone to achieve a successful fusion. Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653. Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine 1983;8:489-500.
Question 49
A 43-year-old woman has an enlarging mass in the left groin. A radiograph, CT scan, and a biopsy specimen are shown in Figures 42a through 42c. Treatment should consist of



Explanation
The patient has a pelvic chondrosarcoma. The radiograph shows a lytic bone lesion emanating from the left inferior pubic ramus and extending into the soft tissues. Punctate calcifications are revealed on the radiograph and CT scan. The histology is consistent with a malignant cartilage lesion. Appropriate treatment for a pelvic chondrosarcoma is wide resection. In this location, wide resection of the ischiopelvic region (type 3 internal hemipelvectomy) is the treatment of choice. A type 2 internal hemipelvectomy involves resection of the periacetabular region. A type 1 internal hemipelvectomy involves resection of the ilium. No reconstruction is required for a type 3 resection. A classic hemipelvectomy is not necessary because the tumor can be removed with an adequate margin while maintaining the neurovascular structures and hip joint. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642. Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 50
During a posterior cruciate ligament-sacrificing total knee arthroplasty with anterior referencing, 8 mm of distal femur is resected. It is noted that the flexion gap is tight and the extension gap appears stable. What is the next most appropriate step in management?
Explanation
If the flexion gap is tight and the extension gap is correct, it is preferable to change only the flexion gap and leave the extension gap unchanged; therefore, the treatment of choice is to decrease the size of the femoral component. The smaller component will be smaller in both medial-lateral as well as anterior-posterior dimensions. A smaller anterior-posterior size will allow more space for the flexion gap without significantly affecting the extension gap. Decreasing the size of the tibial polyethylene insert thickness or cutting more proximal tibia will affect both the flexion and extension gaps. Cutting more distal femur will increase the extension gap and not change the flexion gap, making the described situation worse. Cutting both the proximal tibia and distal femur will increase both the flexion and extension gaps.
Question 51
High Yield
What type of nerve palsy is most common following elbow arthroscopy?

Explanation
Transient ulnar nerve palsy is the most common palsy following elbow arthroscopy. The ulnar nerve is most frequently affected, followed by the radial nerve. Injury to the other nerves has been reported but less frequently. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
Question 52
High Yield
Osteoporotic vertebral compression fractures are associated with

Explanation
Osteoporotic vertebral compression fractures are associated with neurologic complications in less than 1% of patients. After the initial fracture however, patients have a 20% risk of further fractures. The mortality rate of patients with vertebral fractures exceeds that of patients with hip fractures when they are followed beyond 6 months. Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11. Lindsay R, Silverman SL, Cooper C, et al: Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285:320-323.
Question 53
A 28-year-old professional football player reports painless loss of ankle motion after sustaining a "severe" ankle sprain 12 months ago. A mortise radiograph is shown in Figure 1. Surgical treatment should be reserved for which of the following conditions?

Explanation
The radiograph shows posttraumatic tibiofibular synostosis. This condition typically follows an eversion (high) ankle sprain that results in disruption of the interosseous membrane. Ossification usually develops within 6 to 12 months after the injury. Return to sports is possible despite the lack of normal ankle dorsiflexion and mobility between the tibia and fibula. Surgical excision is reserved for persistent pain that fails to respond to nonsurgical management once the ossification is "cold" on bone scintigraphy. Whiteside LA, Reynolds FC, Ellsasser JC: Tibiofibular synostosis and recurrent ankle sprains in high performance athletes. Am J Sports Med 1978;6:204-208. Henry JH, Andersen AJ, Cothren CC: Tibiofibular synostosis in professional basketball players. Am J Sports Med 1993;21:619-622.
Question 54
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?

Explanation
A compression or burst injury occurs with vertical loading of the spine, such as from a blow to the vertex with the neck flexed (eg, spear tackling in football). This leads to vertebral end plate fractures before disk injury. At higher forces, the entire vertebra and disk may explode into the spinal canal. Analysis has shown this to be the major mechanism of cervical fracture, dislocation, and quadriplegia. With the normal head-up posture, the cervical spine has a gentle lordotic curve, and forces transmitted to the head are largely dissipated in the cervical muscles. When the neck is flexed, the cervical spine becomes straight, with the vertebral bodies lined up under one another. This allows for minimal dissipation of the impact forces to be absorbed by the neck muscles. Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532. Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Question 55
High Yield
A 33-year-old man had his foot run over by a forklift 1 hour ago. Examination reveals that the head of the fifth metatarsal is extruded through the plantar aspect of the foot. The foot is severely swollen and pale, there is no sensation in the toes, and the pulses are not palpable. Radiographs are shown in Figures 42a and 42b. Emergent management should consist of


Explanation
Following a severe crush injury, the patient has an acute compartment syndrome. Even though there is an open fracture, this is not sufficient to decompress the compartment syndrome. Therefore, splinting and observation are not appropriate. The surgical treatment of choice is fasciotomy with fixation of the multiple fractures. A primary amputation is not indicated because there is potential for salvage of this devastating injury. Fakhouri AJ, Manoli A II: Acute foot compartment syndromes. J Orthop Trauma 1992;6:223-228. Myerson MS: Management of compartment syndromes of the foot. Clin Orthop 1991;271:239-248.
Question 56
High Yield
The relocation test is most reliable for diagnosing anterior subluxation of the glenohumeral joint when

Detailed Explanation
The relocation test is most accurate when true apprehension is produced with the arm in combined abduction and external rotation and then relieved when posterior pressure is placed on the humeral head. Pain with this test is a less specific response and may occur with other shoulder disorders such as impingement.
Question 57
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?

Explanation
The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a "double PCL sign." This is due to the flipped portion of the meniscus in the notch. Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Question 58
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of

Explanation
Radiographic abnormalities such as coxa magna, coxa breva secondary to growth arrest, and coxa plana and acetabular deformities are associated with healed Legg-Calve-Perthes disease. Femoral heads that were flat yet congruent with the acetabulum are at risk for disabling arthritis in the sixth decade of life in 50% of these untreated patients. As the normal ball-and-socket joint deforms to a flattened cylinder, the hip loses abduction and rotation capability, while retaining flexion and extension potential. If the femoral head is flat and is not concentric with the acetabulum, early severe arthritis occurs. Hinge abduction and anterior impingement are known sequelae of a flat, incongruent femoral head.
Question 59
Oxidation of polyethylene after sterilization occurs most rapidly when the implant undergoes
Explanation
The use of gamma radiation to sterilize polyethylene will result in the formation of free radicals in the material that increase the susceptibility of the material to oxidation and wear. The packaging can also have an impact. If the polyethylene is packaged in air, the oxygen in the packaging can significantly oxidize the material on the shelf prior to clinical use. Gas plasma and ethylene oxide sterilization do not appear to increase oxidation of polyethylene. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Wright TM: Ultra-high molecular weight polyethylene, in Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 37-46.
Question 60
Following reconstruction of the anterior cruciate ligament (ACL), which of the following rehabilitation exercises has the greatest potential to harm the graft?
Explanation
Isometric quadriceps contraction between 15 and 30 degrees of flexion creates significant strain in the ACL and potential damage to the reconstructed graft. Isolated quadriceps contraction with knee flexion of greater than 60 degrees, hamstring contraction at any angle of knee flexion, and active knee motion between 35 and 90 degrees of flexion create substantially less strain in the properly implanted ACL graft. Beynnon BD, Gleming BC, Johnson RL, Nichols CE, Renstrom PA, Pope MH: Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am J Sports Med 1995;23:24-34.
Question 61
A 10-year-old boy has activity-related knee pain that is poorly localized. He denies locking, swelling, or giving way. Examination shows mild tenderness at the medial femoral condyle and painless full range of motion without ligamentous instability. Radiographs are shown in Figures 2a through 2c. What is the best course of action?



Explanation
The radiographs show an osteochondritis dissecans (OCD) lesion in the medial femoral condyle of a skeletally immature patient. The lesion is not displaced from its bed. Nonsurgical management of a stable OCD lesion in a patient with open physes consists of a period of activity limitation and occasional immobilization. Unstable lesions, loose bodies, and patients with closed physes require more aggressive treatment. Most of the surgical procedures can be done arthroscopically. Because the radiographic appearance is typical, biopsy is unnecessary. The radiographs do not show an osteocartilaginous loose body, and the patient reports no catching or locking; therefore, removal of the loose body is not indicated. Linden B: Osteochondritis dissecans of the femoral condyles: A long term follow-up study. J Bone Joint Surg Am 1977;59:769-776. Cahill BR: Osteochondritis dissecans of the knee: Treatment of juvenile and adult forms. J Am Acad Orthop Surg 1995;3:237-247.
Question 62
High Yield
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Explanation
Although any of these structures can be injured by pressure from the medial blade of a self-retaining retractor, the recurrent laryngeal nerve runs cephalad in the interval between the esophagus and trachea and is vulnerable to pressure if caught between the retractor and an inflated endotracheal tube balloon. Ebraheim NA, Lu J, Skie M, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine. Spine 1997;22:2664-2667.
Question 63
High Yield
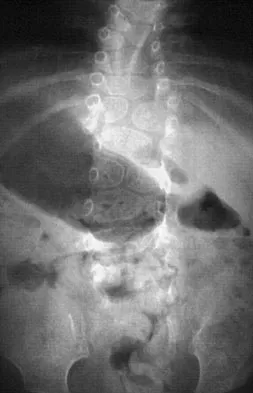
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches


Detailed Explanation
Mortality following trauma that requires surgical intervention for head, chest, and abdominal injury exceeds 90%. The type of pelvic fracture is a predictor of associated injury, blood requirements, and overall mortality. AP III pelvic fractures require the most blood, and are associated with significant abdominal trauma and shock. Lateral compression pelvic fractures are more associated with head, chest, and occasionally abdominal trauma, and mortality often occurs from associated injuries. Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000. Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.
Question 64
High Yield
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient's neurologic recovery can be best determined by
Explanation
The patient has spinal shock. Steroid administration and MRI are appropriate therapeutic and diagnostic procedures. Myelography with CT is of little value unless there is an unusual skeletal variant. Spinal cord-evoked potentials have no value. The best method to determine the patient's neurologic recovery is repeated physical examinations over the first 48 to 72 hours. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Question 65
High Yield
A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and recently had an intramedullary nail placed for the skeletal injury. Vacuum-assisted closure (VAC) has been used to cover the defect since the injury. The risk of infection developing in the tibia is
Detailed Explanation
The risk of infection in a 3B open tibia fracture is most directly related to the timing of the soft-tissue coverage and less related to the size or location of the wound. The wound VAC does not lower or raise the risk of infection in open fractures. It does appear to increase the window of time to obtain coverage without increasing the risk of infection. Additionally, the wound VAC may decrease the probability of needing free tissue coverage. Intramedullary nailing has not been shown to lower the risk of infection in 3B fractures. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292. Dedmond BT, Kortesis B, Punger K, et al: The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibia shaft fractures. J Orthop Trauma 2007;21:11-17.
Question 66
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of

Explanation
Because the radiograph shows that the femoral stem is loose within the femoral canal and there is a fracture in the distal cement mantle, the stem should be revised. The Ogden-type plate and the allograft bone plates will reconstruct the femur but will not restore stability to the stem. Similarly, traction may allow the femur to heal but will not restore stability to the femoral stem within the femur. Resection arthroplasty is considered a salvage option following failure of the other procedures. Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Question 67
High Yield
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Explanation
The history is most consistent with a plantar fibroma. The nodules typically are located within the substance of the plantar aponeurosis. The clinical appearance is usually diagnostic without the need for advanced imaging studies. While the lesion may be prominent and painful to direct palpation, the anatomic location is usually off of the weight-bearing surface. Observation with or without an accommodative orthotic is the treatment of choice. Recurrence is common following attempted excision. Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 68
High Yield
Which of the following statements best describes the location of the nerve that is at risk in a direct posterior approach to the Achilles tendon?
Explanation
The sural nerve lies lateral to the Achilles tendon at the level of the foot but follows an oblique course proximally to lie directly over the tendon as it heads to the popliteal fossa. It is at risk with any proximal dissection from a direct posterior approach and in particular with procedures done at the musculotendinous junction. The nerve crosses over the lateral border of the Achilles tendon at an average of 9.8 cm above its insertion. Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Question 69
High Yield
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?


Detailed Explanation
The radiographs show nonunion of both the greater and lesser tuberosities. Tuberosity pull-off and nonunion remain among the most common causes of failed humeral head arthroplasty for fracture. Strict attention to securing the tuberosities to each other and to the shaft, and autogenous bone grafting from the excised humeral head will decrease the incidence of pull-off and improve healing rates. Active-assisted range-of-motion and strengthening exercises should be delayed until tuberosity healing is noted radiographically, usually at 6 to 8 weeks postoperatively. Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475. Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation. Phys Ther 1975;55:850-858.
Question 70
High Yield
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
Nonsurgical care for hallux rigidus involves limiting the motion of the first metatarsophalangeal joint during toe-off and ensuring that there is a deep enough toe box to accommodate dorsal osteophytes. A rigid shank or forefoot rocker both help to reduce the forces of extension during toe-off. Beskin JL: Hallux rigidus. Foot Ankle Clin 1999;4:335-353.
Question 71
High Yield
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
While transtibial amputees can be fitted with a prosthesis with a residual limb as short as 5 cm, or with retention of the insertion of the patellar tendon, this patient has an unstable gait because of the limited ability of the prosthetic socket to maintain a snug and stable fit. While cumbersome and bulky, double metal uprights and a corset is the only predictable method of gaining stability. The other methods attempt to add an element of stability; however, they are unlikely to be successful. Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Question 72
High Yield
Which of the following is not a reported mode of failure for a constrained acetabular component?
Explanation
There is no evidence of increased polyethylene wear in constrained acetabular components. The rates of wear appear to be the same using standard or constrained liners. Lachiewicz PF, Kelley SS: Constrained components in total hip arthroplasty. J Am Acad Orthop Surg 2002;10:233-238. Anderson MJ, Murray WR, Skinner HB: Constrained acetabular components. J Arthroplasty 1994;9:17-23.
Question 73
An axial T1-weighted MRI scan of the pelvis is shown in Figure 35. Which of the following structures is enclosed by the circle?

Explanation
The obturator vessels and nerve pass along the lateral pelvic wall along the true pelvic brim (nerve lies anterior to the vessels and lies on the obturator internus muscle) and descend into the obturator groove at the upper portion of the obturator foramen. Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, et al (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Question 74
High Yield
A 63-year-old woman who sustained a distal radial fracture 2 months ago now reports that she is unable to achieve active extension of the thumb at the interphalangeal joint. What type of trauma may lead to this clinical finding?
Explanation
Nondisplaced distal radial fractures have a higher rate of spontaneous rupture of the extensor pollicis longus tendon. The extensor mechanism is felt to impinge on the tendon following a nondisplaced fracture and causes either a mechanical attrition of the tendon or a local area of ischemia in the tendon. Helal B, Chen SC, Iwegbu G: Rupture of the extensor pollicis longus tendon in undisplaced Colles' type of fracture. Hand 1982;14:41-47.
Question 75
What is the peak period of onset in children with pauciarticular juvenile rheumatoid arthritis?

Explanation
Approximately one half of patients with juvenile rheumatoid arthritis (JRA) have the pauciarticular form, which by definition includes only patients with fewer than five joints involved. The peak period of onset is between the ages of 2 and 4 years, with half of the affected children coming to medical attention before age 4 years. The knee is most often affected, with the ankle-subtalar and elbow joints next in frequency. The average duration of the disease is 2 years and 9 months, with half the cases lasting less than 2 years. Arthritis, in Herring JA (ed): Tachdjian's Pediatric Orthopaedics, ed 3. St Louis, MO, WB Saunders, 2002, pp 1811-1839.
Question 76
High Yield
A 19-year-old man has had intermittent progressive knee pain with ambulation and pain at night following a rodeo accident 4 weeks ago. Figures 4a through 4e show the radiographs, a bone scan, CT scan, and T2-weighted MRI scan. What is the most likely diagnosis?





Detailed Explanation
The imaging studies reveal a predominantly blastic lesion in the distal femur with posterolateral periosteal changes. The bone scan shows increased uptake in the distal femur, beyond that expected with radiography. Cross-sectional imaging confirms the presence of a soft-tissue mass extending from the lateral aspect of the femur, with diffuse intramedullary signal changes. This aggressive presentation, particularly in this location and in a patient of this age, is most consistent with osteosarcoma. The mineralization in the soft tissue strongly suggests neoplasm, not the reactive bony changes seen in an infectious process. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 77
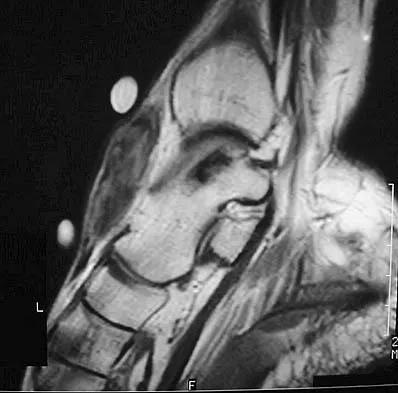
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of

Explanation
The MRI scan shows a massive tear of the supraspinatus tendon with medial retraction to the level of the glenoid. This is most likely an attritional tear with a high risk of failure of the repair. The preferred treatment is nonsurgical management for pain and stiffness. Acromioplasty and coracoacromial ligament release in this setting are controversial, as they can result in the devastating complication of anterosuperior subluxation of the humerus. Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr: Debridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-866.
Question 78
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of

Explanation
Humeral arthroplasty is indicated for chronic posterior dislocations when the impression defect in the humeral head is greater than 45% to 50%. If the condition remains undiagnosed for more than 9 to 12 months, secondary degenerative changes on the glenoid may occur, necessitating total shoulder arthroplasty. Open reduction and transfer of the subscapularis and lesser tuberosity are used for impression defects that consist of 20% to 40% of the humeral articular surface. Closed reduction and immobilization with the arm in slight extension and external rotation is useful when the posterior dislocation is diagnosed within the first 6 weeks and the articular defect is less than 20%. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 79
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show

Explanation
The radiograph shows the correct tibial tunnel and anterior femoral tunnel; therefore, range of motion will most likely show loss of flexion. Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin Sports Med 1999;18:109-171.
Question 80
A well-developed college football player reports swelling and a heaviness in the arm after lifting weights. Examination reveals that distal pulses are normal and equal in both arms. A venogram is shown in Figure 13. What is the most likely cause of this condition?

Explanation
The clinical findings indicate venous obstruction without arterial compression, and the venogram reveals occlusion of the subclavian vein, which is most likely the result of thoracic outlet compression. In the developed athlete, scalene muscle hypertrophy (Paget-Schroetter syndrome) causes compression of the subclavian vein. Treatment should consist of thrombolysis followed by decompressive surgery. Angle N, Gelabert HA, Farooq MM, et al: Safety and efficacy of early surgical decompression of the thoracic outlet for Paget-Schroetter syndrome. Ann Vasc Surg 2001;15:37-42.
Question 81
An 18-year-old man has acute respiratory distress after sustaining injuries in a motorcycle accident. He has a blood pressure of 80/60 mm Hg and a pulse rate of 110/min. Examination reveals chest tympany to percussion, distended neck veins, and deviation of the trachea away from his right hemithorax where the breath sounds are diminished. Heart sounds are regular and normal on auscultation. Initial management should consist of

Explanation
Tension pneumothorax occurs when air trapped in the pleural space between the lung and chest wall achieves sufficient pressure to compress the lungs and shift the mediastinum. Urgent needle decompression of the pleural space air followed by definitive chest tube placement is the treatment of choice.
Question 82
High Yield
In a patient who has rheumatoid arthritis with acetabular protrusion, what is the best biomechanical position for the cup with respect to the preoperative center of rotation?

Explanation
Acetabular protrusion in patients with rheumatoid arthritis moves the center of hip rotation medially and posteriorly. Positioning of the acetabular component in a patient with protrusion is best accomplished in the normal (anterior and inferior) position and not in a protruded position. This has been shown both clinically and in a finite-element analysis. Any medial positioning will produce impingement of the prosthesis neck on the rim, and superior placement produces improper hip mechanics. Crowninshield RD, Brand RA, Pedersen DR: A stress analysis of acetabular reconstruction in protrusio acetabuli. J Bone Joint Surg Am 1983;65:495-499.
Question 83
High Yield
A 5-year-old boy sustained an elbow injury. Examination in the emergency department reveals that he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. The radial pulse is palpable at the wrist, and sensation is normal throughout the hand. Radiographs are shown in Figures 6a and 6b. In addition to reduction and pinning of the fracture, initial treatment should include


Explanation
The findings are consistent with a neurapraxia of the anterior interosseous branch of the median nerve. This is the most common nerve palsy seen with supracondylar humerus fractures, followed closely by radial nerve palsy. Nearly all cases of neurapraxia following supracondylar humerus fractures resolve spontaneously, and therefore, further diagnostic studies and surgery are not indicated. Cramer KE, Green NE, Devito DP: Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-505.
Question 84
A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?

Explanation
When managing a complex intra-articular fracture, it is imperative that there is adequate visualization of the joint; this usually means an extensile approach. At the elbow, this is usually through a transolecranon osteotomy. The recent addition of a muscle-sparing approach as described by Bryan and Morrey has gained popularity, but it is difficult to maintain soft-tissue viability and it may put the ulnar nerve at risk. A triceps-splitting approach, which can be used for simple single articular splits into the joint where extra-articular reduction is available, is possible and good results have been reported. To date, there is minimal data on these alternative approaches for comminuted intra-articular distal humeral fractures. McKee MD, Mehne DK, Jupiter JP: Fractures of the distal humerus: Part II, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1483-1522 McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707. Patterson SD, Bain GI, Mehta JA: Surgical approaches to the elbow. Clin Orthop 2000;370:19-33.
Question 85
High Yield
The space available for the cord is an important determinant in neurologic recovery. Recent analysis suggests that the most reliable radiographic predictor for neurologic recovery after surgery in patients with rheumatoid arthritis and paralysis is a preoperative

Detailed Explanation
Boden and associates' recent article presents significant evidence that patients with rheumatoid arthritis, neurologic deterioration, and C1-2 instability are more likely to improve after surgery if the posterior alanto-odontoid interval is greater than 10 mm preoperatively. The accepted safe range for the posterior atlanto-odontoid interval is 14 mm. This measurement is believed to better represent the space available for the cord than the anterior alanto-odontoid interval. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 273-279. Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 86
An olecranon fracture-dislocation of the elbow in which the fracture line exits distal to the coronoid process is best managed by open reduction and
Explanation
Fracture-dislocations of the elbow present difficult management problems. Standard olecranon fractures normally are not associated with a dislocation; however, the surgeon needs to recognize that some fractures that have a dislocation, in particular a posterior dislocation, represent a Monteggia equivalent. These injuries are not ulnar shaft fractures because they are fractured at or just distal to the coronoid; however, because of the unstable fracture-dislocation, the forces across this reduction are high. Two Kirschner wires and a tension band wire provide inadequate fixation. Therefore, the preferred method of fixation is plate osteosynthesis with a 3.5-mm low-contact dynamic compression plate or reconstruction plate. Jupiter JP, Kellam JF: Fractures of the forearm, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 421-454. Quintero J: Fracture of the forearm, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 323-337.
Question 87
High Yield
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
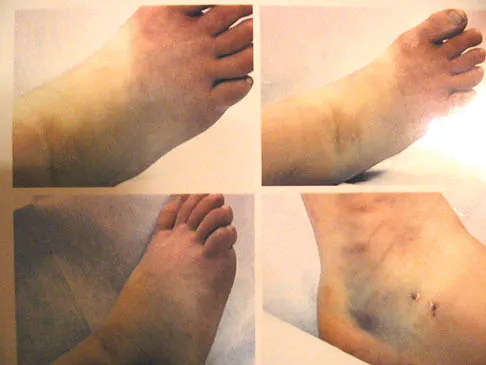
Explanation
The patient has a classic history and examination for an acute compartment syndrome of the foot. CT, MRI, or stress radiographs are not necessary prior to emergent fasciotomies of the foot. These studies can be performed after the initial fasciotomies to determine the best long-term management of the fractures. There are nine compartments in the foot. These are decompressed through three incisions (two on the dorsal foot and one medially). A short leg cast does not address the compartment syndrome and could be limb threatening with excessive swelling in a circumferential cast. It is preferable to splint severe crush injuries rather than apply a cast. Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Question 88
High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 89
Figures 28a through 28c show the MRI scans of a 30-year-old woman who weighs 290 lb and has low back and left leg pain. She also reports frequent urinary dribbling, which her gynecologist has advised her may be related to obesity. Examination will most likely reveal



Explanation
The patient will most likely exhibit ipsilateral weakness of the tibialis anterior. Gaenslen's test is designed to detect sacroiliac inflammation as a source of low back pain. Beevor's sign tests the innervation of the rectus abdominus and paraspinal musculature (L1 innervation). The extensor hallucis longus is predominantly innervated by L5. The peroneals are predominantly innervated by S1. Hoppenfeld S: Physical Examination of the Spine and Extremities. Appleton, WI, Century-Crofts, 1976.
Question 90
High Yield
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5 degrees of angulation. When the MCP joint is flexed 30 degrees, a radially directed stress produces 45 degrees of angulation. Radiographs are otherwise normal. Management should consist of
Detailed Explanation
Injuries to the ulnar collateral ligament of the MCP joint of the thumb commonly occur in recreational skiers. Historically, this injury has been referred to as "gamekeeper's thumb." The ligament consists of the proper collateral ligament and the more volar accessory collateral ligament. In extension, the accessory ligament is taut, and in flexion, the proper ligament is taut. For a complete tear of the ligament complex to occur, there must be laxity in full extension. Incomplete tears respond well to thumb spica splinting or casting for 2 to 3 weeks and gradual resumption of range of motion. Prolonged immobilization of incomplete injuries leads to higher rates of MCP joint stiffness. Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Question 91
High Yield
In the spine, osteoblastomas usually originate in the

Detailed Explanation
Osteoblastomas are benign lesions that represent less than 5% of benign bone tumors. Most lesions are located in the spine, followed by the femur, tibia, and skull. Patients with spinal lesions usually have pain that may be associated with scoliosis. The most common location in the spine is within the posterior elements.
Question 92
High Yield
What is the most common secondary malignancy arising in pagetic bone?

Explanation
The incidence of malignant transformation or the formation of a secondary malignancy in pagetic bone is estimated to be less than 1%. Osteosarcoma is the most common secondary malignancy, followed by fibrosarcoma and chondrosarcoma. Ewing's sarcoma arising in pagetic bone has not been reported. Grimer RJ, Carter SR, Tillman RM, et al: Osteosarcoma of the pelvis. J Bone Joint Surg Br 1999;81:796-802.
Question 93
High Yield
Which of the following radiographic views best depicts a Hill-Sachs defect?

Explanation
The Stryker notch view best shows this type of defect. An outlet view helps evaluate acromial shape, a true AP shows joint space narrowing, a serendipity view evaluates the sternoclavicular joint, and a Zanca view helps evaluate the acromioclavicular joint. An internal rotation AP may also depict a Hill-Sachs defect.
Question 94
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?

Explanation
Progressive weakness is a common sign with a large differential diagnosis. Nerve, muscle, and joint problems should be excluded when a patient has diffuse weakness and atrophy. Fascioscapulohumeral dystrophy is a rare disease characterized by facial muscle weakness and proximal shoulder muscle weakness. The weakness is usually bilateral, and scapular winging is common. If the scapular winging becomes pronounced, elevation of the shoulder can be affected. In severe cases, scapulothoracic fusion or pectoralis muscle transfer to the scapula may be indicated. Duchenne muscular dystrophy is typically severe and progressive. The other diagnoses are not compatible with the history or the physical findings. Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Question 95
A 25-year-old man injured his dominant shoulder after falling on his outstretched arm 4 months ago. Examination reveals that he cannot lift his arm above 90 degrees, and he has pronounced medial scapular winging. Management should consist of

Explanation
Serratus anterior palsy or long thoracic nerve palsy is usually caused by traction injury to the nerve, blunt injury, or iatrogenic injury. The palsy results in winging of the scapula and medial rotation of the inferior pole of the scapula. A patient with this injury will usually recover in 12 to 18 months. Initial treatment should include observation and shoulder strengthening exercises. Nerve exploration with repair has not proven beneficial in changing the outcome. Many orthopaedic surgeons favor using a split pectoralis major transfer for symptomatic patients. Electrodiagnostic studies are helpful in confirming the diagnosis. Post M: Pectoralis major transfer for winging of the scapula. J Shoulder Elbow Surg 1995;4:1-9.
Question 96
High Yield
The transverse diameter of the pedicle is most narrow at which of the following levels?

Detailed Explanation
Of the levels given, T5 has the most narrow pedicle in anatomic studies. One study in patients with scoliosis did note that T7 on the concave side was more narrow than T5, but T7 is not listed here as a possible answer. O'Brien MF, Lenke LG, Mardjetko S, et al: Pedicle morphology in thoracic adolescent idiopathic scoliosis: Is pedicle fixation an anatomically viable technique? Spine 2000;25:2285-2293.
Question 97
High Yield
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?
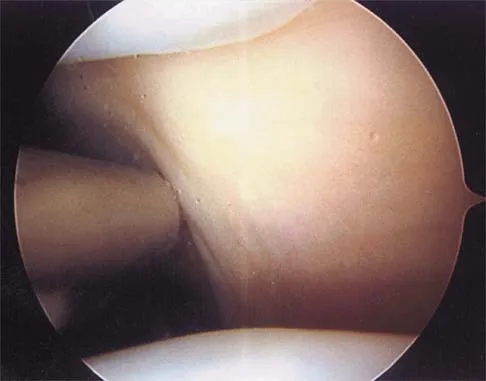
Explanation
While it is possible to damage any of these structures, unrecognized intraoperative laceration without adequate coagulation of the superior lateral geniculate artery is common. This can result in significant postoperative hemarthrosis and a return to surgery when bleeding cannot be controlled. Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Question 98
High Yield
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
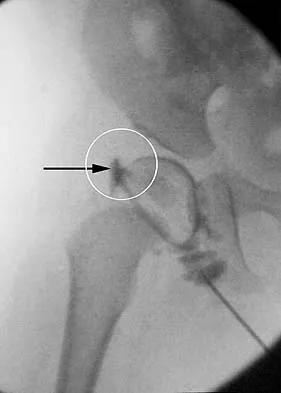
Explanation
The structure enclosed by the circle is the acetabular labrum. It is visible as the white point of tissue outlined by the darkly radiopaque contrast. The appearance of the contrast surrounding the sharp white point of a normal labrum is called the "rose thorn sign." The limbus is the term reserved for a rounded, infolded labrum seen with arthrography. The pulvinar is the fatty tissue seen in the empty acetabulum when the hip is dislocated. The ligamentum teres is seen as a white stripe outlined by contrast coursing from the central acetabulum to the dislocated femoral head. The transverse acetabular ligament courses across the inferior portion of the acetabulum and is not clearly seen with arthrography. Herring JA: Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 532-533.
Question 99
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
Convex hemiarthrodesis and hemiepiphysiodesis are procedures designed to gradually reduce curve magnitude in congenital scoliosis because of hemivertebrae. They are used to surgically create an anterior and posterior bar to arrest growth on the convexity of the existing deformity. Success of the technique is predicated on continued growth on the concave side of the deformity. Prerequisites for this procedure include curves of limited length (less than or equal to five vertebrae), curves of reasonable magnitude (less than 70 degrees), absence of kyphosis, concave growth potential, and appropriate age (younger than age 5 years).
Question 100
A 36-year-old skier sustains a grade III posterior cruciate ligament (PCL) tear. Where will increased contact pressures develop over time?
Explanation
Complete rupture of the PCL leads to increased contact pressures in the patellofemoral and medial compartments of the knee. However, whether degenerative arthritis will develop and in which compartments still remains controversial.
