Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
Surgical curettage or en bloc resection is the treatment of choice for osteoid osteoma. Night pain and relief of symptoms with nonsteroidal anti-inflammatory drugs are classic findings for osteoid osteoma. Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598. Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Question 2
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?

Explanation
There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high energy humeral shaft fractures. J Hand Surg 2004;29:144-147. Foster RJ, Swiontkowski MR, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 3
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?

Explanation
A compression or burst injury occurs with vertical loading of the spine, such as from a blow to the vertex with the neck flexed (eg, spear tackling in football). This leads to vertebral end plate fractures before disk injury. At higher forces, the entire vertebra and disk may explode into the spinal canal. Analysis has shown this to be the major mechanism of cervical fracture, dislocation, and quadriplegia. With the normal head-up posture, the cervical spine has a gentle lordotic curve, and forces transmitted to the head are largely dissipated in the cervical muscles. When the neck is flexed, the cervical spine becomes straight, with the vertebral bodies lined up under one another. This allows for minimal dissipation of the impact forces to be absorbed by the neck muscles. Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532. Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Question 4
High Yield
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes

Detailed Explanation
This Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction of the radial shaft and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. If not, either open or closed reduction with pinning is undertaken. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
Question 5
High Yield
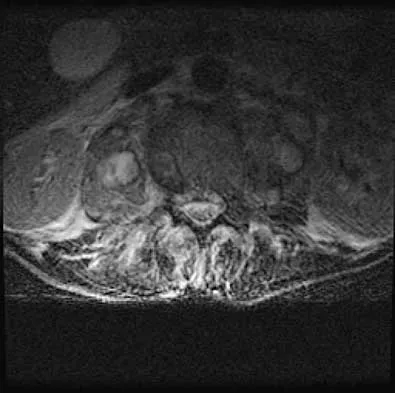
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be
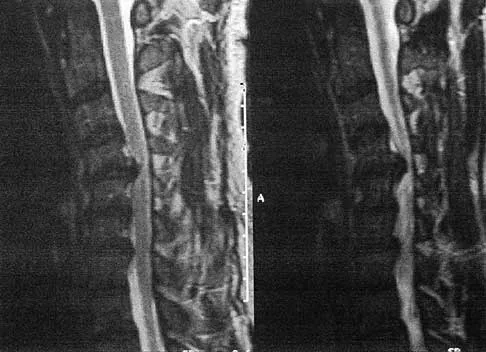
Explanation
Although the patient has a large herniated nucleus pulposus, the pain has decreased from 10/10 to 3/10 over a 4-week period and the patient is now free of any neurologic symptoms. It is quite likely that further nonsurgical management will continue to resolve his symptoms. In the absence of any neurologic deficits, there is no evidence that the patient is at significant risk for paralysis. Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
Question 6
Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
Explanation
Redislocation following acute dislocation occurs in approximately 3% of patients. This redislocation tends to occur in middle-aged and elderly patients. A higher incidence of redislocation occurs when there are accompanying fractures of the glenoid rim and the greater tuberosity. Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment. J Bone Joint Surg Am 2002;84:1552-1559.
Question 7
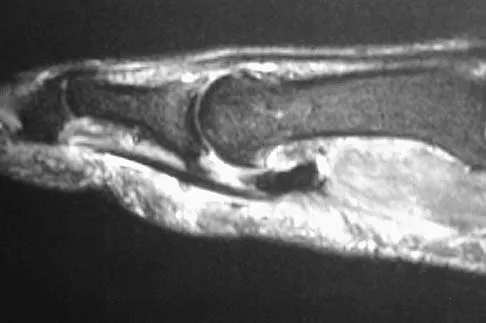
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?

Explanation
On T1-weighted images, the posterior cruciate ligament is a low-signal (black) structure that courses from the posterior aspect of the tibia to the medial femoral condyle. The posterior cruciate ligament can appear as arcuate, U-shaped, or kinked. The other structures have similar signal but different anatomic locations. Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Question 8
A 27-year-old woman has a bilateral C5-C6 facet dislocation and quadriparesis after being involved in a motor vehicle accident. Initial management consisted of reduction with traction, but she remains a Frankel A quadriplegic. To facilitate rehabilitation, surgical stabilization and fusion is planned. From a biomechanical point of view, which of the following techniques is the LEAST stable method of fixation?
Explanation
In two different biomechanical studies performed in both bovine and human cadaveric spines, all posterior techniques of stabilization were found to be superior to anterior plating in flexion-distraction injuries of the cervical spine. These injuries usually have an intact anterior longitudinal ligament that allows posterior fixation to function as a tension band. Anterior plating with grafting destroys this last remaining stabilizing structure and does not allow for a tension band effect because all of the posterior stabilizing structures have been destroyed with the injury. In clinical practice, however, anterior plating can be effective in the treatment of this injury with appropriate postoperative orthotic management. Sutterlin CE III, McAfee PC, Warden KE, et al: A biomechanical evaluation of cervical spine stabilization methods in a bovine model: Static and cyclical loading. Spine 1988;13:795-802.
Question 9
High Yield
Based on the findings shown in Figures 22a and 22b, corrective surgery to obtain maximal safe correction and optimal instrumentation fixation should be performed at which of the following locations?


Detailed Explanation
The clinical photograph and radiograph show an iatrogenic flatback deformity with loss of the normal lumbar lordosis. The safest correction for this malalignment typically is performed away from the spinal cord in the midlumbar spine, most commonly at L2 or L3. The more distal the correction is performed, the more sagittal plane translation of the C7 plumb line with respect to the posterior sacrum. Performing the osteotomy too distally, however, makes it difficult to obtain adequate distal fixation. Shufflebarger HL, Clark CE: Thoracolumbar osteotomy for postsurgical sagittal imbalance. Spine 1992;17:S287-S290.
Question 10
High Yield
A 20-year-old man sustains the injury shown in Figures 1a and 1b in a motorcycle accident. In addition to a prompt closed reduction, his outcome might be optimized by


Explanation
Lateral subtalar dislocations, which are less common than medial subtalar dislocations, are high-energy injuries that are frequently associated with small osteochondral fractures. It is generally recommended that large fragments be internally fixed, and small fragments entrapped within the joint be excised. Although arthrosis frequently occurs after this injury and is the most common long-term complication, primary subtalar arthrodesis is not indicated. A talar neck fracture is not evident on the radiographs, and lateral subtalar dislocation usually does not lead to instability.
Question 11
What complication is most likely to develop after right total hip arthroplasty in the patient shown in Figure 5?

Explanation
The patient has hypertrophic arthritis, which is a strong risk factor for heterotopic bone formation. The remaining complications are possible but do not have the same significant risks. Goel A, Sharp DJ: Heterotopic bone formation after hip replacement: The influence of the type of osteoarthritis. J Bone Joint Surg Br 1991;73:255-257.
Question 12
High Yield
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle?

Explanation
Compartment syndrome of the anterior and deep posterior compartments results in anterior tibialis and posterior tibialis tendon weakness, respectively. Furthermore, the long flexors to the hallux and lesser toes will be weak as well. The intact peroneus longus overpowers the weak anterior tibialis tendon, resulting in plantar flexion of the first metatarsal, cavus, and hindfoot varus. Therefore, transferring the peroneus longus to the dorsolateral midfoot reduces the first metatarsal plantar flexion torque, and possibly augments ankle dorsiflexion torque. Hansen ST: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott, Williams & Wilkins, 2000, pp 433-435.
Question 13
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?

Explanation
The history and findings are consistent with a diagnosis of a sprain of the medial collateral ligament (MCL) of the elbow; therefore, contrast-enhanced MRI is considered the most sensitive and specific study for accurately showing this injury. Arthroscopic visualization of the MCL is limited to the most anterior portion of the anterior bundle only; complete inspection of the MCL using the arthroscope is not possible. CT without the addition of contrast is of no value in this situation. Use of a technetium Tc 99m bone scan is limited to aiding in the diagnosis of occult fracture, a highly unlikely injury in this patient. There are no clinical indications for electromyography. Timmerman LA, Andrews JR: Undersurface tear of the ulnar collateral ligament in baseball players: A newly recognized lesion. Am J Sports Med 1994;22:33-36. Timmerman LA, Schwartz ML, Andrews JR: Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation of 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-32.
Question 14
High Yield
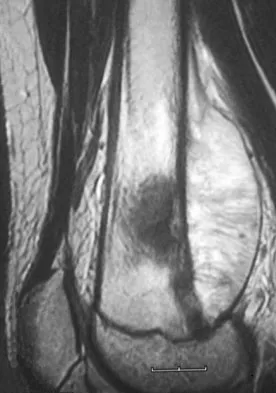
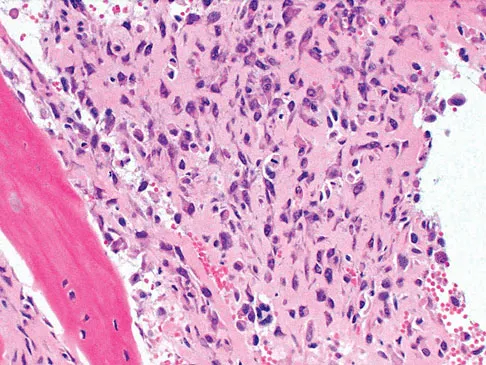
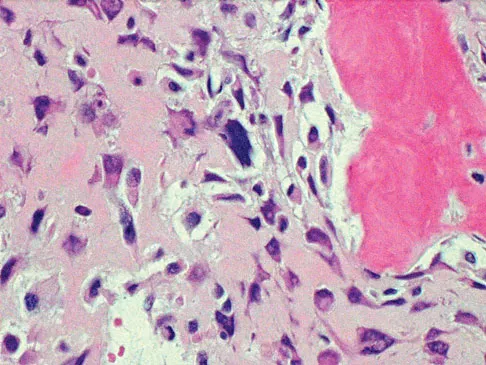
Figure 26 shows the radiograph of a 48-year-old woman who has right arm pain and hematuria. A bone scan reveals increased uptake in the left ribs and thoracic spine. A needle biopsy specimen shows that the lesion is highly keratin positive and composed primarily of clear cells. What is the best course of action?

Detailed Explanation
The lesion has the typical "blown out" lytic radiographic appearance that is most commonly found in thyroid or renal cell metastases. Given the history of hematuria and histology findings, the most likely diagnosis is metastatic renal cell carcinoma. This tumor is relatively resistant to chemotherapy. Radiation therapy is used as a postoperative adjuvant treatment with varying response rates. Surgery should be performed after preoperative embolization to decrease the risk of intraoperative bleeding, as no tourniquet can be used in this location. Patients with metastatic renal cell carcinomas may survive for years, resulting in a higher likelihood of local tumor progression with ineffective adjuvant therapy. Intramedullary fixation combined with curettage and cementation will provide the best chance of local control while maintaining the patient's native shoulder and elbow joints. A total humeral resection is an extensive surgery with considerable morbidity and is not indicated for this patient because less extensive surgery is likely to be effective. Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1054. Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Question 15
High Yield
A 34-year-old man has had a 13-month history of an equinovarus deformity of the foot and ankle after a motorcycle accident. His foot and ankle are flexible, but bracing has become uncomfortable. Active dorsiflexion and eversion are absent. What is the most appropriate treatment?

Detailed Explanation
Arthrodesis of any of the ankle or hindfoot joints should be reserved for fixed deformities or end-stage degenerative arthritis. Achilles tendon lengthening is necessary to correct the equinus and to improve dorsiflexion-plantar flexion balance. Similarly, transfer of the posterior tibialis tendon reduces both plantar flexion and inversion torque. Hansen ST: Function Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 442-447.
Question 16
A 77-year-old woman with osteoporosis who underwent cemented total hip arthroplasty 12 years ago fell down a flight of stairs. A radiograph is shown in Figure 15. What is the best option for treating this fracture?

Explanation
Type I fractures are trochanteric fractures usually secondary to osteolysis. Type II fractures are located around the stem. Type III fractures are distal to the stem. If the fracture and prosthesis are stable, the fracture can be treated nonsurgically. If the fracture is unstable, the stability of the prosthesis should be assessed. If the prosthesis is unstable (type IIB), treatment should consist of revision to a long stem prosthesis that bypasses the fracture by two cortical diameters. If, as in this patient, the prosthesis is not loose (type IIA), open reduction and internal fixation is the appropriate option. Proximal femoral allograft is appropriate for type IIIC fractures in which the proximal bone is significantly compromised and the femoral component is loose. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Question 17
High Yield
Which of the following statements best describes synovial fluid?
Detailed Explanation
Synovial tissue is composed of vascularized connective tissue that lacks a basement membrane. Two cell types (type A and type B) are present: type B cells produce synovial fluid. Synovial fluid is made of hyaluronic acid and lubricin, proteinases,and collagenases. It is an ultrafiltrate of blood plasma added to fluid produced by the synovial membrane. It does not contain erythrocytes, clotting factors, or hemoglobin. It lubricates articular cartilage and provides nourishment via diffusion. Synovial fluid exhibits non-Newtonian flow characteristics. The viscosity coefficient is not a constant, the fluid is not linearly viscous, and its viscosity increases as the shear rate decreases.
Question 18
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?


Explanation
The MRI scans reveal a large postoperative hematoma causing significant thecal compression. An epidural hematoma with neurologic deficit is a surgical emergency requiring immediate evacuation of the hematoma. Although the incidence of postoperative epidural hematomas is rare, the consequences of a missed diagnosis can be catastrophic. Early recognition and evacuation are essential in preserving or restoring neurologic function. Uribe and associates attributed delayed postoperative hematomas to previous multiple lumbar surgeries as a possible contributing factor. Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.
Question 19
High Yield
A 52-year-old woman slips in her bathroom and strikes her right hand on a cabinet. She notes swelling, ecchymosis, and pain with attempted motion. There are no open wounds. Radiographs are shown in Figures 5a through 5c. What is the most appropriate treatment?



Detailed Explanation
Nondisplaced transverse fractures of the phalanges are stable. Immobilization in the intrinsic plus position will prevent MCP joint stiffness. Displaced oblique fractures are more at risk for instability. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Question 20
High Yield
Which of the following is considered a risk factor for the development of low back pain?
Detailed Explanation
Risk factors associated with low back pain include poor physical fitness, smoking, a history of repetitive bending or stooping on the job, or whole body vibration exposure. Some radiographic factors such as stenosis, spondyloarthropathy, severe deformity, or instability are also associated with low back pain. Gender, weight, transitional anatomy, or facet trophism are not associated with low back pain.
Question 21
High Yield
In Figure 2, which of the following structures is the primary stabilizer in preventing valgus instability of the elbow?
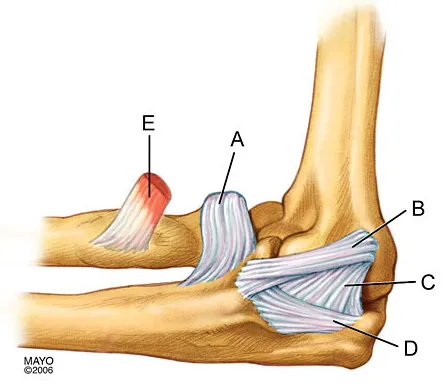
Explanation
The anterior bundle of the medial collateral ligament is the prime stabilizer of the medial aspect of the elbow and is indicated by "B" in the figure. When intact, this anterior bundle of the medial collateral ligament is a restraint to valgus instability of the elbow. The posterior bundle is regarded as a secondary stabilizer of the medial elbow (C). The transverse bundle (D), annular ligament (A), and biceps tendon (E) do not play a role in valgus stability of the elbow. Jobe F, Elattrache N: Diagnosis and treatment of ulnar collateral ligament injuries in athletes, in Morrey B (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1993, p 566.
Question 22
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Question 23
A right-handed 24-year-old woman underwent an arthroscopic Bankart repair for recurrent anterior dislocations 9 months ago. Despite extensive physical therapy for 8 months, the patient has very limited range of motion (elevation to 130 degrees and external rotation to 10 degrees with the arm at the side). Shoulder radiographs are normal. The next step in management should consist of

Explanation
Arthroscopic capsular release is an effective means of treating stiffness that is the result of capsular contractures, such as in the case of a tight Bankart repair. Open release allows lengthening of a surgically shortened subscapularis, such as after a tight Putti-Platt repair. Additional physical therapy is unlikely to be effective because 8 months of treatment has failed to result in improvement. Accepting this degree of asymptomatic limited motion is not advisable because of the functional limitations for the patient and the increased risk of postoperative degenerative arthritis. Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Question 24
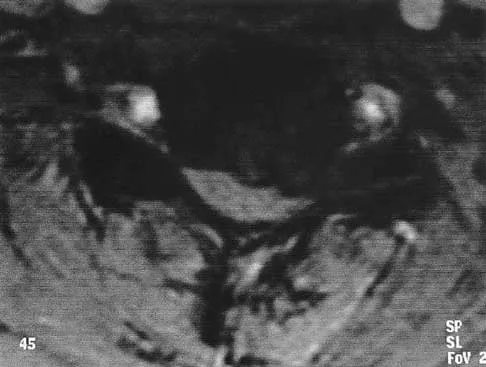
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of



Explanation
An intramuscular lipoma is a benign soft-tissue lesion that can grow and has a small risk of progressing to a liposarcoma. Radiographs usually show a globular radiolucent mass adjacent to higher-density muscle tissue shadows. When the patient has symptoms and reports an increase in size of the mass, the treatment of choice after appropriate radiographic analysis is complete excision of the mass with marginal resection. Sampling error is a problem with fatty lesions and core or incisional biopsies are frequently unnecessary, especially if an MRI scan of the lesion shows signal intensity that matches subcutaneous fat on all sequences. Damron TA: What to do with deep lipomatous tumors. Instr Course Lect 2004;53:651-655. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Question 25
High Yield
A 26-year-old woman sustained a nondisplaced femoral neck fracture and treatment consisted of use of percutaneous cannulated screws. At her 3-month follow-up visit, she reports hip pain and is unable to ambulate. A radiograph is shown in Figure 1. What is the next most appropriate treatment?

Detailed Explanation
Femoral neck fracture nonunion is a challenging problem for orthopaedic surgeons. Vertical fractures are more prone to nonunion due to shear stress rather than compressive forces across the fracture site. Several authors have suggested these fractures are more common in young adults due to injury type and bone composition. It is widely regarded that an effort should be made to salvage the femoral head if vascularity remains. The most common method to treat this complication is valgus intertrochanteric osteotomy of the femur. This functionally makes a vertical fracture more horizontal, converting shear into compressive forces. It also helps correct the varus position of the fracture nonunion. Hartford JM, Patel A, Powell J: Intertrochanteric osteotomy using a dynamic hip screw for femoral neck nonunion. J Orthop Trauma 2005;19:329-333.
Question 26
A patient who sustained a knife wound to the axilla 4 months ago now has profound interosseous wasting and generalized hand weakness. A brachial plexus injury is likely at which of the following locations in Figure 29?

Explanation
Penetrating sharp wounds in proximity to major nerve or vascular structures should always be acutely explored. Because this patient did not seek treatment for a potentially treatable injury, interosseous wasting implies injury to the C8 and T1 nerve roots that contribute to ulnar nerve function. The most likely location for the brachial plexus injury is the location marked L or the inferior trunk. A wrist drop that is the result of radial nerve dysfunction would be expected with an injury at K or O. An upper brachial plexus palsy with loss of elbow flexion and shoulder abduction would be expected with an injury at B. A loss of elbow flexion alone would be expected following an injury at C. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29. Wolock B, Millesi H: Brachial plexus-applied anatomy and operative exposure, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1255-1272.
Question 27
High Yield
An 18-year-old gymnast has had a 1-year history of foot pain. Examination reveals medial midfoot tenderness without swelling. Non-weight-bearing in a cast for 6 weeks has failed to provide relief. An axial CT scan of the midfoot is shown in Figure 20. What is the optimal treatment for this condition?

Detailed Explanation
Stress fractures of the navicular are often seen in running and jumping sports. Whereas most individuals heal with nonsurgical management consisting of 6 weeks of casting, this gymnast has had pain for 1 year and nonsurgical management has failed. Open reduction with bone grafting is the preferred treatment. Quirk RM: Stress fractures of the navicular. Foot Ankle Int 1998;19:494-496.
Question 28
A 21-year-old basketball player inverts his foot during practice. Examination reveals obvious deformity of the hindfoot with a prominence of the talar head dorsolaterally and medial displacement of the forefoot. A radiograph is shown in Figure 17. What is the most likely obstacle to closed reduction?

Explanation
The patient has a medial subtalar dislocation. These injuries should be reduced as soon as possible to minimize risk to the skin. Most often, this can be done easily, and further radiographic evaluation then can be performed as necessary. On rare occasions, closed reduction is not possible because of fractures of the articular surface of the talus, navicular, interposed extensor digitorum brevis, or transverse fibers of the cruciate crural ligament. The posterior tibial tendon is the most common obstruction to closed reduction in lateral subtalar dislocations, which are less common than medial dislocations. The majority of both injuries can be managed by closed reduction and immobilization. Mulroy RD: The tibialis posterior tendon as an obstacle to reduction of a lateral anterior subtalar dislocation. J Bone Joint Surg Am 1953;37:859-863. Heckman JD: Fractures and dislocations of the foot, in Rockwood CA, Green DP, Bucholz RW (eds): Fractures in Adults. Philadelphia, PA, JB Lippincott, 1991, pp 2093-2100.
Question 29
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?

Explanation
The patient has nonunions of the metatarsal fractures and a hallux valgus deformity with arthritic changes. To address all of the findings, management should consist of open treatment of the metatarsal nonunions and hallux metatarsophalangeal arthrodesis. Cast immobilization and a bone stimulator are unlikely to be beneficial at this time. Isolated correction of the hallux valgus deformity will not address the metatarsal nonunions or the arthritis at the hallux metatarsophalangeal joint. Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214. McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Question 30
A 9-year-old boy has a painless enlarged mass on the dorsum of his hand. Figures 14a through 14d show the clinical photograph, radiographs, and biopsy specimen. What is the most likely diagnosis?




Explanation
Multiple hereditary exostosis and enchondroma commonly present as multiple lesions in the hand. Multiple hereditary exostosis consists of cartilage capped bony exostoses arising from the metaphyseal end of rapidly growing bones. Osteosarcoma and chondrosarcoma rarely appear as multiple lesions. Fracture callus can exhibit enchondral ossification that is usually circumferential, but the radiographic findings are not consistent with fracture. Porter DE, Emerton ME, Villanueva-Lopez F, Simpson AH: Clinical and radiographic analysis of osteochondromas and growth disturbance in hereditary multiple exostoses. J Pediatr Orthop 2000;20:246-250.
Question 31
High Yield
The recurrent motor branch of the median nerve innervates which of the following muscles?
Explanation
The recurrent motor branch of the median nerve supplies the thenar muscles (abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis) that are primarily responsible for thumb opposition. The nerve can be injured in carpal tunnel release. A branch of the nerve also supplies the first lumbrical. The adductor pollicis and the interossei are supplied by the ulnar nerve. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Question 32
High Yield
What is the most likely long-term sequela of the injury shown in Figures 47a and 47b?


Detailed Explanation
The imaging studies show a comminuted lateral talar process fracture. This injury is often missed on plain radiographs; therefore, CT provides the best method of diagnostic evaluation. The most likely long-term sequela of this injury is subtalar joint arthrosis. Although this injury involves the fibular gutter region, progression to true ankle arthritis is unlikely. There does not appear to be any association with this injury and chronic mechanical instability of the ankle or disruption of the superior peroneal retinaculum and subsequent peroneal tendon instability. Entrapment of the flexor hallucis longus tendon may occur with fractures of the sustentaculum tali but not with injuries of the lateral talar process. Surgical management includes open reduction and internal fixation versus excision; the goal is preservation of the large articular surface fragments. In this patient, there is significant comminution and early fragment excision may be the best option for acute treatment. Tucker DJ, Feder JM, Boylan JP: Fractures of the lateral process of the talus: Two case reports and a comprehensive literature review. Foot Ankle Int 1998;19:641-646.
Question 33
High Yield
A 15-year-old female field hockey player sustains a blow to the mouth from a hockey stick. Three front teeth are knocked out and shown in Figure 4. In addition to calling a dentist immediately, what is the next best step in management?

Detailed Explanation
Tooth avulsions can occur in contact or collision sports. An avulsed tooth is a medical emergency. The likelihood of survival of the tooth depends on the length of time that the tooth is out of the socket and the degree to which the periodontal ligament is damaged. The tooth should be handled only by the crown end and not the root end. It can be rinsed of debris with water or normal saline solution. The tooth should not be brushed or cleaned otherwise. During transport, the tooth must be kept moist. An avulsed tooth can be transported in whole milk, saliva, sterile saline solution, or commercially available kits with physiologic buffer solutions. The tooth and the athlete should be transported to the dentist for reinsertion as soon as possible and preferably within an hour. Krasner P: Management of sports-related tooth displacements and avulsions. Dent Clin North Am 2000;44:111-135. Sullivan JA, Anderson SJ (eds): Care of the Young Athlete. Rosemont IL, American Academy of Orthopaedic Surgeons, Elk Grove Village, IL, American Academy of Pediatrics, 2000, p 190.
Question 34
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?

Explanation
The standard approach to the volar aspect of the distal radius is the Henry approach. Following incision of the skin and subcutaneous tissues, the forearm fascia is incised. The radial artery and venae comitantes lie in the interval between the tendons of the flexor carpi radialis muscle and the brachioradialis muscle. This interval is developed, and the radial artery and veins are retracted in a radial direction. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 35
High Yield
Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?

Explanation
Stiffness following total knee arthroplasty can be a disabling condition. There are many reasons for loss of knee motion following total knee arthroplasty. Technical errors, such as overstuffing of the patella, malpositioning of the components, and ligamentous imbalance, are all known to result in stiffness following total knee arthroplasty. In some patients with a possible genetic predisposition, aggressive arthrofibrosis may develop and result in loss of knee motion. In any patient who has deteriorating knee motion, particularly after revision arthroplasty, deep infection should be ruled out. Although on occasion surgical intervention may be required to address knee stiffness, the outcome of revision surgery is poor if no reason for stiffness can be determined. Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.
Question 36
High Yield
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?

Explanation
Arthroscopic versus open distal clavicle excision has the advantage of allowing evaluation of the glenohumeral joint arthroscopically prior to moving into the subclavicular and subacromial space to perform the distal clavicle excision. This can be of value in both confirming the diagnosis as well as avoiding diagnostic errors. Berg and Ciullo showed that in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament. Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Question 37
What is the most likely type of pathology seen in Figure 16?

Explanation
The figure shows the missing pedicle or "winking owl" sign that is characteristic of tumor involvement of the cortical bone of the pedicle. None of the other pathologic processes commonly gives this radiographic picture. Thinned, but not missing pedicles, have been described as a normal variant. McLain R, Weinstein J: Tumors of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1173.
Question 38
High Yield
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of

Explanation
The dislocation is between the medial and middle cuneiform. Although the first and second tarsometatarsal joints are aligned, there is a gap between the cuneiforms. The radiograph shows a Lisfranc dislocation variant. In a healthy active individual, open reduction and internal fixation yields the best results. The reestablishment of the normal arch and medial column support with anatomic reduction is critical to obtaining the best possible outcome from these injuries. Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int 2002;23:922-926.
Question 39
Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good motion and stability. What is the most likely diagnosis?


Explanation
The radiographs show narrowing of the medial joint space, which indicates polyethylene wear and progressive varus alignment. Wear particles incite osteolytic lesions like the one seen on the lateral radiograph. O'Rourke MR, Callaghan JJ, Goetz DG, et al: Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design. J Bone Joint Surg Am 2002;84:1362-1371.
Question 40
For halo traction, what is the preferred site for anterior pin placement?
Explanation
The safe zone for anterior halo pin insertion is marked laterally by the anterior border of the temporalis muscle (to avoid penetration of this muscle and relative thin cortex of the skull). Medially, the pin should be placed 4.5 cm lateral to the midline to avoid injury to the supraorbital nerve or the frontal sinus. The safe area is marked superiorly by the head equator to avoid cephalad migration of the pin and inferiorly by the supraorbital ridge to prevent displacement or penetration into the orbit.
Question 41
Pacinian corpuscles are lamellated nerve endings that are responsible for providing the perception of

Explanation
Pacinian corpuscles are nerve endings that provide the perception of pressure.
Question 42
Radiographs of an 80-year-old woman with back pain reveal a compression fracture. Which of the following imaging studies best evaluates the acuity of the fracture?
Explanation
The best method of evaluating the acuity of osteoporotic compression fractures is to look for edema in the vertebral body. This is best accomplished with a STIR-weighted MRI scan. Bone scans can show increased uptake at the site of fracture for many months after the fracture. T1-weighted MRI scans show loss of normal marrow fat that may not necessarily correspond with acuity of the fracture. CT scans and radiographs show fracture deformity but cannot be used to judge acuity. Phillips FM: Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 2003;28:S45-S53.
Question 43
High Yield
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended?

Detailed Explanation
The patient needs restrictions on his external rotation to allow healing of the subscapularis tendon repair. Limitation to 60 degrees is common if the tendon repair is robust and shows no evidence of tension on range-of-motion testing during the surgery. Restriction from external rotation stretching for even 3 weeks would compromise his ultimate functional recovery. Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Question 44
High Yield
A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?

Explanation
The lateral cord terminates as the musculocutaneous nerve and also contributes sensory fibers to the median nerve. Involvement of the C6 root or upper trunk could potentially cause weakness of the infraspinatus and the brachioradialis. The middle trunk and the posterior cord do not contribute motor fibers to the thumb or sensory fibers to the thumb.
Question 45
High Yield
A 13-year-old boy has knee pain after sustaining a mild twisting injury while playing basketball 4 weeks ago. Radiographs and MRI scans are shown in Figures 24a through 24d, and biopsy specimens are shown in Figures 24e and 24f. Treatment should consist of



Explanation
The imaging studies and histology are consistent with high-grade osteosarcoma. The standard treatment for osteosarcoma is neoadjuvant chemotherapy combined with wide surgical resection that can be performed with amputation or limb salvage depending on characteristics unique to each tumor and each patient. In most patients, limb salvage surgery can be performed with reconstruction using allografts and/or megaprostheses. Osteosarcoma is poorly responsive to radiation therapy. Chemotherapy alone, in the absence of appropriate surgery, has not proven effective. Simon MA, Springfield DS: Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274.
Question 46
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of

Explanation
The patient has a displaced fracture of the apophysis of the olecranon for which most authorities recommend surgical treatment. In older children, stability of the reduction may be achieved by the use of two parallel medullary Kirschner wires and a figure-of-8 tension band loop of either stainless steel wire or absorbable suture. The use of an absorbable suture does not require removal of the implant. Absorbable suture alone is best used in very young patients who have this type of injury. An intramedullary screw would pose an unnecessary risk of future growth disturbance. A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma. Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033. Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Question 47
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?

Explanation
The primary change that takes place in the aging spine is degeneration of the lumbar disks and loss of the overall lumbar lordosis. This also may be associated with osteopenic-related compression fractures. With these changes, the sagittal vertical line moves anteriorly relative to the sacrum; cervical scoliosis is uncommon and not part of the normal aging process. Overall kyphosis in the thoracic spine gradually increases, but the coronal balance remains essentially the same unless scoliosis develops. Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Question 48
A 67-year-old man is requesting revision surgery because of continued pain in the knee after undergoing a total knee replacement 2 years ago. Examination reveals that the knee is not warm, the incision is well-healed, and the skin has normal coloration and hair formation. No varus or valgus instability is noted, and knee range of motion is 5 degrees to 100 degrees. Laboratory studies show an erythrocyte sedimentation rate of 15 mm/h and a WBC of 5,000/mm3. Aspiration of the knee reveals clear fluid that shows no growth on culture. Radiographs reveal an appropriately positioned cruciate-retaining cemented total knee arthroplasty that is well-fixed. What is the probability that the patient's pain will be improved with revision surgery?

Explanation
The patient has a well-fixed and aligned painful total knee replacement. The success rate of revision knee replacement for pain when no mechanical problem can be identified is approximately 40%. The critical step is to rule out the presence of infection with appropriate laboratory studies and aspiration. If no infection is detected, revision should be avoided. Rand JA: Planning for revision total knee arthroplasty, in Zuckerman JD (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 161-166.
Question 49
A 3-year-old boy with severe cerebral palsy is unable to sit independently and does not crawl. Examination reveals a 40-degree hip flexion contracture by the Thomas test and 25 degrees of passive abduction. A radiograph of the pelvis shows subluxation of both hips, with a migration index of 30%. Management should consist of
Explanation
Progressive hip subluxation occurs in up to 50% of children with spastic quadriparesis. The subluxation is the result of chronic muscle hypertonicity, especially in the adductor muscle group. In time, the constant muscle tension will lead to dislocation, dysplastic changes in the acetabulum, and erosive changes in the cartilage of the femoral head. Many of these children will experience pain. Two recent studies have shown that early soft-tissue releases can successfully prevent progressive subluxation in children who are younger than age 4 years and who have a Reimers index (migration index) of less than 40%. Botulinum toxin A injections may reduce tone in the adductors for 4 to 6 months, but it is difficult to inject into the iliopsoas. Additionally, there are no long-term studies documenting the efficacy of botulinum toxin A to treat progressive hip subluxation in patients who have spastic quadriparesis. In general, proximal femoral osteotomy, combined with soft-tissue release as necessary, is indicated in older children (older than age 4 years) with progressive subluxation. Although selective dorsal rhizotomy has been used in nonambulatory patients, outcomes are less well documented than in ambulatory patients. There are no studies documenting the effect of selective dorsal rhizotomy on progressive hip subluxation in nonambulatory children. Miller F, Cardoso Dias R, Dabney KW, et al: Soft-tissue release for spastic hip subluxation in cerebral palsy. J Pediatr Orthop 1997;17:571-584.
Question 50
High Yield
A 36-year-old woman has neck pain in the upper cervical region and occipital discomfort after being involved in a motor vehicle accident. Examination reveals no forehead or scalp lacerations. The neurologic examination is normal. A CT scan shows no evidence of bony injury. Figures 39a and 39b show a lateral radiograph and an MRI scan. Management should consist of


Explanation
The lateral radiograph shows 8 mm of atlantoaxial translation. In the absence of a bony injury, this represents rupture of the transverse atlantal ligament. The MRI scan reveals soft-tissue swelling posterior to the odontoid and a high intensity zone in the atlanto-dens interval consistent with acute injury. These injuries require arthrodesis because nonsurgical measures will not provide stability. Techniques for C1-2 fusion include Gallie, Brooks, or triple wiring. Transarticular screw fixation across the C1-2 articulation provides the most rigid means of fixation and the highest arthrodesis rates but is technically demanding. Anterior C2-3 arthrodesis will not address the level of instability. The normal atlanto-dens interval is 3 mm in an adult and 4 mm in a child. Kurz LT: Transverse atlantal ligament insufficiency, in Clark CR (ed): The Cervical Spine. Philadelphia, PA, Lippincott-Raven, 1998, pp 401-407.
Question 51
Analysis of primary total hip arthroplasty using press-fit acetabular components without supplementary screw fixation reveals that screw fixation
Explanation
Using mechanical failure of fixation as the end point, Udomkiat and associates demonstrated a 12-year survivorship of 99.1% for titanium press-fit acetabular components without supplementary screw fixation. This study suggests that it is unlikely that the use of supplementary screws would lead to improved results. In addition, polyethylene wear debris tends to migrate through screw holes and along the course of screws. Screw holes also decrease the available surface for bone ingrowth. Screws that back up may be a source of backside polyethylene wear. This suggests that screw holes and the use of screws should be avoided when they are unnecessary for cup fixation.
Question 52
High Yield
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
Explanation
The MRI scans show a complete disruption of the sesamoid complex with proximal retraction of the medial sesamoid and high signal originating from the site normally occupied by the plantar plate (metatarsophalangeal ligament). This injury is the result of a hyperextension injury and is a severe variant of a turf toe. Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Question 53
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?


Explanation
The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.
Question 54
High Yield
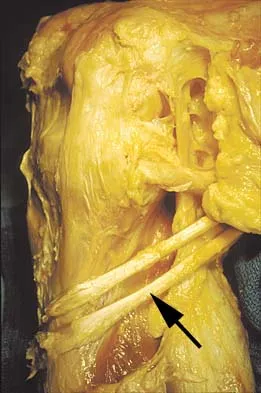
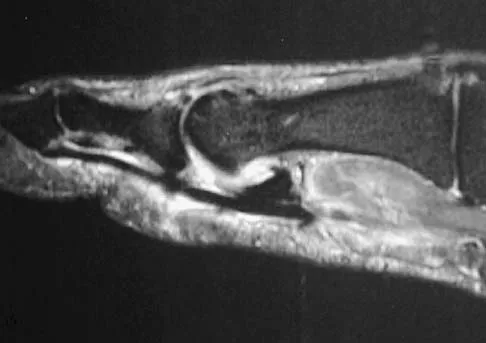
The arrow in the axial T1-weighted MRI scan shown in Figure 18 is pointing to which of the following structures?

Explanation
The arrow is pointing to the ulnar nerve within Guyon's canal. Guyon's canal is approximately 4 cm long, beginning at the proximal extent of the transverse carpal ligament and ending at the aponeurotic arch of the hypothenar muscles. Many structures comprise the boundaries of Guyon's canal. The floor, for example, consists of the transverse carpal ligament, the pisohamate and pisometacarpal ligaments, and the opponens digiti minimi. Within Guyon's canal, the ulnar nerve bifurcates into the superficial and deep branches, with the deep branch of the ulnar nerve persisting distal to the canal. The ulnar artery is immediately adjacent and radial to the ulnar nerve. The median nerve is visualized within the carpal tunnel. The radial artery is on the radial side of the wrist. The hook of the hamate is clearly seen in the figure, orienting the observer to the ulnar side of the wrist. Goss MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop 1985;196:238-247.
Question 55
A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?


Explanation
In a relatively young patient who is an avid tennis player, the treatment of choice is a joint preserving procedure. The radiographs reveal varus alignment with loading of the medial compartment. After all nonsurgical management options have been used, the best treatment option is a medial opening wedge osteotomy. A lateral closing wedge osteotomy of the proximal tibia is also a reasonable option, but it is not one of the choices. A unicompartmental arthroplasty or a total knee arthroplasty would place significant restrictions in this patient. A unispacer may be a temporizing procedure but is controversial and without substantial data in the literature. The knee arthroscopy will not address the medial compartment osteoarthritis. Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358. Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Question 56
High Yield
A 70-year-old man underwent primary total knee arthroplasty 3 months ago. Figures 7a and 7b show the radiograph and clinical photograph following incision and drainage of the wound 1 week ago. Aspiration of the joint reveals methicillin-sensitive Staphylococcus aureus. What is the next most appropriate step in management?


Detailed Explanation
The overriding factor determining treatment in this case is the appearance of the surgical wound. Based on MacPhearson's work, this "C" wound is best managed with two-stage exchange. The functional outcome is markedly diminished following a knee arthrodesis compared to revision knee arthroplasty. Harwin SF: The diagnosis and management of infected total knee replacement. Seminars Arthroplasty 2002;13:9-22. Goldmann RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Question 57
During primary total knee arthroplasty, the trial components are in place. The extensor space is tight, but the flexion space is normal. What is the best gap balancing solution?

Explanation
The first rule of total knee arthroplasty is to restore the joint line to its original location. This will ensure optimal patellofemoral biomechanics and will facilitate ligament balancing. Changes on the tibial side affect both the flexion and extension gaps equally. Changes in femoral component sizing or position affect the flexion gap only. Tibial changes affect both the flexion and extension gaps. To convert a tight extension gap to a normal flexion gap, more distal femur needs to be resected. Vince KG: Revision knee arthroplasty technique. Instr Course Lect 1993;42:325-339.
Question 58
Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?


Explanation
Bayonet apposition of the radius and ulnar shafts is quite acceptable, as long as the angulation is less than 10 degrees. The rotation must be acceptable as well. This patient went on to full healing, with full supination and pronation of the forearm and no cosmetic deformity. Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Question 59
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of


Explanation
The patient has grade IV heterotopic ossification with the limb in an abnormal nonfunctional position. Treatment should consist of excision of the bone to restore hip motion and prophylaxis to prevent recurrent formation. The best time to excise the bone is controversial, with no conclusive evidence supporting early or late excision. Pellegrini VD Jr, Koniski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 60
A 36-year-old skier sustains a grade III posterior cruciate ligament (PCL) tear. Where will increased contact pressures develop over time?
Explanation
Complete rupture of the PCL leads to increased contact pressures in the patellofemoral and medial compartments of the knee. However, whether degenerative arthritis will develop and in which compartments still remains controversial.
Question 61
High Yield
What root is most commonly involved with a segmental root level palsy after laminoplasty?

Detailed Explanation
The postoperative incidence of C5 root palsy after laminoplasty ranges from 5% to 12%. Other roots also may be affected. The palsies tend to be motor dominant, although sensory dysfunction and radicular pain are also possible. The palsy may arise during the immediate postoperative period or up to 20 days later. C5 may be preferentially involved because it is at the apex of the cervical lordosis. Recovery usually occurs over weeks to months. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-249.
Question 62
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel's sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
Painful incisional neuromas after bunion surgery frequently involve the dorsomedial cutaneous branch of the superficial peroneal nerve. This is the medial branch of the superficial peroneal nerve that terminates as the dorsomedial cutaneous nerve to the hallux. Branches of the deep peroneal nerve to this area are rare, and no branches to this area exist from the sural nerve. The saphenous nerve branches are generally more proximal, and the medial plantar nerve lies plantarly. Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Question 63
High Yield
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
Alternative bearing surfaces in THA have received much attention in recent years as more and more hip arthroplasties are being performed on younger patients with hip arthritis. The two most popular nonmetal-on-polyethylene bearing surfaces are metal-on-metal and ceramic-on-ceramic. There are arguments supporting the use of either, but ceramic bearings have been shown to have a theoretic increased risk of fracture compared with cobalt-chromium. This has been shown to be clinically relevant with zirconium ceramics. Newer alumina ceramics are being produced with lower porosity and grain size and with higher density and purity, resulting in lower fracture risk but still greater than that of cobalt-chromium. Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
Question 64
A superior labrum anterior and posterior (SLAP) lesion doubles the strain in which of the following stabilizing structures?
Explanation
A superior labrum, when intact, stabilizes the shoulder by increasing its ability to withstand excessive external rotational forces by an additional 32%. The presence of a SLAP lesion decreases this restraint and increases the strain in the superior band of the inferior glenohumeral ligament by over 100%. Rodosky MW, Harner CD, Fu FH: The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med 1994;22:121-130.
Question 65
High Yield
A previously asymptomatic 14-year-old girl sustained a twisting injury to her ankle. Radiographs are shown in Figures 2a and 2b. Management should consist of


Explanation
The radiographs show a well-defined, irregular, eccentric lesion in the distal tibia metaphysis with a thin sclerotic margin. The radiographs are diagnostic of nonossifying fibroma, a common entity in this age group and in this location. No further work-up is indicated. The patient was asymptomatic prior to the injury and the lesion is small and thus not worrisome for an impending pathologic fracture; therefore, no treatment is indicated beyond observation. The natural history of these lesions is to gradually ossify as the patient reaches skeletal maturity. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 66
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
The beach chair position may cause sudden hypotension and bradycardia as a result of the Bezold-Jarisch reflex. This reflex occurs when venous pooling and increased sympathetic tone induce a low-volume, hypercontractile ventricle, resulting in activation of the parasympathetic nervous system and sympathetic withdrawal. The reported incidence of this phenomenon associated with the sitting position is between 13% to 24%. Left untreated, the result may be cardiac arrest. Pneumothorax or central nervous system toxicity after interscalene block is rare and has an incidence of less than 0.2%. Laryngeal nerve block associated with interscalene nerve block can occur but usually results in hoarseness secondary to ipsilateral vocal cord palsy. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Question 67
A 58-year-old woman sustained a ruptured Achilles tendon 1 year ago, and management consisted of an ankle-foot orthosis. She now reports increasing difficulty with ambulation and increasing pain. An MRI scan shows a 6-cm defect in the right Achilles tendon. Management should now consist of
Explanation
With a gap of less than 4 cm, a V-Y repair would be appropriate without a tendon transfer. For gaps greater than 5 cm, a lengthening with augmentation is the most appropriate treatment. Therefore, the treatment of choice is an Achilles tendon turndown with flexor hallucis longus tendon transfer. The plantaris tendon is not a strong enough repair, and direct repair is not possible given the large defect in the Achilles tendon. Continued use of the ankle-foot orthosis will not provide adequate relief for this patient.
Question 68
High Yield
In the spine, osteoblastomas usually originate in the

Detailed Explanation
Osteoblastomas are benign lesions that represent less than 5% of benign bone tumors. Most lesions are located in the spine, followed by the femur, tibia, and skull. Patients with spinal lesions usually have pain that may be associated with scoliosis. The most common location in the spine is within the posterior elements.
Question 69
A 12-year-old girl with juvenile rheumatoid arthritis (JRA) has had chronic pain and synovitis about the knee that is now well-controlled medically. Examination reveals 20 degrees of valgus at the knee. Knee range of motion shows 10 degrees to 90 degrees of flexion. Treatment should consist of
Explanation
Children with JRA frequently have valgus in association with hypervascularity because of chronic inflammation. This is normally caused by overgrowth of the medial femoral epiphysis. Staple hemiepiphyseodesis, if done early, can reverse the deformity. Osteotomy is usually unnecessary at this age, and there is a risk of stiffness of the knee following the procedure. Synovectomy may be helpful but will not prevent or correct a deformity.
Question 70
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?

Explanation
The MRI arthrogram reveals dye extravasation into the labrum, consistent with a labral tear. The MRI findings are not typical of osteonecrosis, stress fracture, or transient osteoporosis. There is no increase in bone marrow edema in the neck or femoral head. Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.
Question 71
High Yield
What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?
Explanation
Parvizi and associates studied the 30-day mortality rate after more than 22,000 total knee arthroplasties and found that the rate after bilateral total knee arthroplasty was significantly higher than after unilateral total knee arthroplasty. Aseptic loosening, bleeding, and range of motion have not been shown to be statistically different between patients who had unilateral and simultaneous bilateral total knee arthroplasty.
Question 72
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
The steel shank is a flat 1-inch steel strip placed between layers of the shoe to extend the foot lever and prevent deformity at the toe break seen following a partial first ray amputation. A rocker sole may be added as well to facilitate transition from foot flat to the toe-off phase of gait. Proper shoe fit is important, but "snug" fitting shoes in a patient with peripheral neuropathy and likely fluctuations in volume from intermittent swelling are to be avoided. A custom shoe is an unnecessary expense. The patient has at least 10 degrees of dorsiflexion at the ankle with an intact anterior tibialis muscle; therefore, catching the sole on carpeting should not be a problem. Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Question 73
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?


Explanation
The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 74
High Yield
A 33-year-old man had his foot run over by a forklift 1 hour ago. Examination reveals that the head of the fifth metatarsal is extruded through the plantar aspect of the foot. The foot is severely swollen and pale, there is no sensation in the toes, and the pulses are not palpable. Radiographs are shown in Figures 42a and 42b. Emergent management should consist of


Explanation
Following a severe crush injury, the patient has an acute compartment syndrome. Even though there is an open fracture, this is not sufficient to decompress the compartment syndrome. Therefore, splinting and observation are not appropriate. The surgical treatment of choice is fasciotomy with fixation of the multiple fractures. A primary amputation is not indicated because there is potential for salvage of this devastating injury. Fakhouri AJ, Manoli A II: Acute foot compartment syndromes. J Orthop Trauma 1992;6:223-228. Myerson MS: Management of compartment syndromes of the foot. Clin Orthop 1991;271:239-248.
Question 75
Figure 48 shows the initial AP chest radiograph of a 21-year-old motorcycle rider who sustained multiple injuries after striking a telephone pole at high speed. What is the most significant radiographic finding leading to a diagnosis?

Explanation
Scapulothoracic dissociation is a rare, violent traumatic injury in which the scapula is torn away from the chest wall but the skin remains intact. Massive swelling and ecchymosis are common. Neurovascular injury is the rule with possible subclavian or axillary artery disruption and severe partial or complete brachial plexus paralysis. The diagnosis is made on a nonrotated chest radiograph that shows significant lateral displacement of the medial scapular border from the sternal notch. A right midshaft clavicular fracture is present but is not considered the most significant finding. Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432. Ebraheim NA, Pearlstein SR, Savolaine ER, et al: Scapulothoracic dissociation. J Orthop Trauma 1987;1:18-23. Sampson LN, Britton JC, Eldrup-Jorgensen J, et al: The neurovascular outcome of scapulothoracic dissociation. J Vasc Surg 1993;17:1083-1088.
Question 76
High Yield
When performing an arthroscopic subacromial decompression, bleeding can be encountered when dividing the coracoacromial ligament because of injury to what artery?
Detailed Explanation
The acromial branch of the thoracoacromial trunk courses along the coracoacromial ligament. This artery enters the ligament approximately 5 mm below the acromial edge. Division of the ligament at its insertion on the acromion minimizes the risk of bleeding. Esch JC, Baker CL: Arthroscopic anatomy and normal variations, in Whipple TL (ed): Surgical Arthroscopy: The Shoulder and Elbow. Philadelphia, PA, JB Lippincott, 1993, pp 63-76.
Question 77
High Yield
A 32-year-old man notes increasing back pain and progressive paraparesis over the past few weeks. He is febrile, and laboratory studies show a WBC of 12,500/mm3. MRI scans are shown in Figures 6a and 6b. Management should consist of

Explanation
Indications for surgery in spinal infections include progressive destruction despite antibiotic treatment, an abscess requiring drainage, neurologic deficit, need for diagnosis, and/or instability. This patient has a progressive neurologic deficit. Debridement performed at the site of the abscess should effect canal decompression. Once the debridement is complete back to viable bone, the defect can be reconstructed with a strut graft. Additional posterior stabilization is used as deemed necessary by the degree of anterior destruction. CT-guided needle aspiration, while occasionally useful in the earliest phases of an infection, produces frequent false-negative results and would provide little useful information in the management of this patient. Emery SE, Chan DP, Woodward HR: Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine 1989;14:284-291. Lifeso RM: Pyogenic spinal sepsis in adults. Spine 1990;15:1265-1271.
Question 78
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?

Explanation
Varus position of the stem is most commonly associated with failure of the cemented femoral component because of association with an inadequate cement mantle in the proximal medial and distal lateral zones. An inadequate cement mantle and obesity have been associated with increased loosening but not as frequently as a varus deformity. The influences of gender and osteoporotic bone on the outcome of cemented femoral components have not been established. Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Question 79
An otherwise healthy 65-year-old man reports thigh pain of insidious onset. He states that the pain is increased with weight bearing and also occurs at night. He denies any history of cancer. Radiographs are shown in Figures 22a and 22b. A bone scan shows an isolated lesion. CT scans of the chest and abdominal are negative for any other lesions. Initial management should consist of


Explanation
The patient has a solitary lesion that is at high risk for fracture. While metastatic lesions are most common in this age group, a stabilization procedure is contraindicated until results of a biopsy confirm the presence of a metastasis. Because of the lytic lesion and the associated calcification shown on the radiograph, the most likely diagnosis is a chondrosarcoma. Therefore, any type of stabilization procedure with a rod or plate would compromise a wide surgical excision to remove the entire proximal femur. Radiation therapy and chemotherapy are also contraindicated until biopsy results are obtained. Because of these factors, obtaining a frozen section biopsy specimen is considered the next most appropriate step in management. If a metastatic lesion is confirmed on the frozen section, a stabilization procedure could then be performed under the same anesthetic. Therefore, it is important to have a pathologist available at the time of a biopsy. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 80
High Yield
In a retroperitoneal approach to the lumbar spine, what nerve is commonly found on the psoas muscle?
Explanation
The genitofemoral nerve and the sympathetic plexus consistently lie on the ventral surface of the psoas muscle. The ilioinguinal and iliohypogastric nerves are the most superior branches of the lumbar plexus and emerge along the upper lateral border of the psoas muscle traveling toward the quadratus lumborum. Both the obturator and femoral nerves are deep and lateral to the psoas muscle. Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107. Johnson R, Murphy M, Southwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Question 81
High Yield
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?


Explanation
Osteolysis in the trochanteric bed can result in weakening of the bone and fracture. Nonsurgical management will provide reasonable clinical and radiographic results in patients with limited fracture displacement. Claus MC, Hopper RH, Engh CA: Fractures of the greater trochanter induced by osteolysis with the anatomic medullary locking prosthesis. J Arthroplasty 2002;17:706-712.
Question 82
High Yield
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?




Explanation
A Charcot flare in adjacent joints is not uncommon in patients with neuropathy who undergo surgery or other trauma. Venous thrombosis would present with swelling of the entire leg, while infection would present earlier in the postoperative period. The radiographs are pathognomonic of Charcot arthropathy, not an unrecognized fracture or gout. A compartment syndrome this late after injury is extremely rare, and there would be no bony distraction associated with compartment syndrome.
Question 83
High Yield
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?



Explanation
The patient has an acute fracture of the proximal pole. A 100% healing rate has been reported for open reduction and internal fixation of proximal pole fractures via a dorsal approach. This allows for direct viewing of the fracture line, facilitates reduction, and bone grafting can be done through the same incision if necessary. A vascularized or corticocancellous graft is reserved for nonunions. Proximal fractures are very slow to heal with a cast, if they heal at all. As a small fragment, percutaneous fixation is very difficult and has been reported for waist fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Question 84
High Yield
Figures 25a and 25b show the radiographs of a 66-year-old man who has had a long history of bilateral painful flatfoot deformities. Examination reveals that his foot is partially correctable passively, albeit with discomfort, and he has an Achilles tendon contracture. An ankle-foot orthosis has failed to provide relief. Treatment should now consist of


Explanation
The patient has a pronounced deformity with pain and degenerative arthritis; therefore, triple arthrodesis is the treatment of choice. Gastrocnemius or Achilles tendon lengthening may be a necessary adjunct to the triple arthrodesis, but alone is inadequate to allow for correction. Because the ankle-foot orthosis has failed to provide relief, a UCBL is not likely to help. Osteotomy procedures are designed for lesser deformities and well-preserved joints. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 115-120.
Question 85
The photomicrograph in Figure 37 shows a repaired dural tear 4 days after surgery. The material interposed between the dural edges (D) is composed of

Explanation
During the initial healing phases of a dural tear, pia and arachnoid from adjacent nerve roots migrate, fill the dural defect, and create a pia-arachnoid plug. It is this initial plugging of the defect that is believed to prevent further egress of cerebrospinal fluid through the defect. The plug has been shown to develop by the second postoperative day. Fibroblastic proliferation occurs within the dura itself and accounts for the bulbous ends of the dura seen in the photomicrograph. The appearance of the material within the dural edges is inconsistent with the appearance of neural elements, and scar tissue formation occurs later in the healing process. Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Question 86
What structure is marked Q in the diagram of the brachial plexus shown in Figure 22?

Explanation
From proximal to distal, the brachial plexus is divided into roots, trunks, divisions, and cords before forming specific peripheral nerve branches. The structure marked Q is called the posterior cord because it lies posterior to the axially artery at the level of the cords. Its terminal branches are the upper subscapular (V), thoracodorsal (W), lower subscapular (X), axillary (F), and radial (G) nerves. Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams and Wilkins, 1978, pp 6-24.
Question 87
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20 degrees of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked "A," the resulting ligament reconstruction will excessively

Explanation
If the femoral tunnel is created using guide wire A, it will be too far anterior in the intercondylar notch. The distance between a central tibial insertion for the ACL and an anterior femoral tunnel will progressively increase as the knee is flexed. Therefore, if the graft is tensioned near extension, the ligament will excessively tighten as the knee flexes past 90 degrees. This will result in restricted knee flexion or failure of the graft as full flexion is gained. There will be little effect on the ligament as it extends from 20 degrees to 0 degrees of flexion. If the graft is tensioned in significant flexion (greater than 60 degrees), it will be excessively loose as the knee fully extends. Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Question 88
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction. Rockwood and Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Question 89
Figures 34a and 34b show the radiographs of a 28-year-old man who fell on his outstretched arm with significant force while mountain biking. The nerve deficit most likely to occur would result in weakness of


Explanation
The patient has a Monteggia fracture-dislocation (proximal ulnar fracture and radial head dislocation). The posterior interosseous nerve branch of the radial nerve is the most likely to be injured and could result in weakness of thumb extension and finger metacarpal extension. Considerably less likely are injuries to the more proximal radial nerve branches supplying the extensor carpi radialis longus and brevis, resulting in weak wrist extension; the ulnar nerve supplying the digital intrinsics, resulting in weak finger abduction; the anterior interosseous branch of the median nerve, resulting in weakness of the flexor pollicis longus; and the distal median nerve, resulting in weakness of thumb opposition. Bado JL: The Monteggia lesion. Clin Orthop 1967;50:71-86.
Question 90
High Yield
Figures 32a and 32b show the radiographs of an active 13-year-old boy who has persistent left thigh pain and a limp despite a trial of protected weight bearing. Management should consist of


Explanation
The plain radiographs show an eccentric metaphyseal lesion involving a long bone in a skeletally immature patient. The lesion is longer than it is wide, with distinctly lobular outer edges that are sclerotic. These findings are characteristic of a nonossifying fibroma. Small asymptomatic lesions may be followed clinically. Larger lesions that occupy greater than two thirds of the width of the shaft and are located in areas of high mechanical stress such as the femur are more prone to fracture than smaller lesions. Pain is often a sign of impending fracture or the presence of a small fracture that may not be apparent on radiographs. The natural history of the lesion is to resolve over a period of years. The procedure that would allow the patient to return to contact sports is curettage and bone grafting. Intralesional steroid injection has been advocated in the treatment of unicameral bone cysts and eosinophilic granuloma but not nonossifying fibromas. En block resection is not indicated for a benign lesion. Low-dose radiation therapy has been used for eosinophilic granuloma but not for nonossifying fibromas. Walker RN, Green NE, Spindler KP: Stress fractures in skeletally immature patients. J Pediatr Orthop 1996;16:578-584.
Question 91
High Yield
Figures 46a through 46e show the radiographs of a 22-year-old man who injured his wrist in a motorcycle accident. He has no other injuries. What is the best course of action?





Detailed Explanation
The patient has a fracture-dislocation of the radiocarpal joint. Attached to the large radial styloid fragment are the extrinsic wrist ligaments to the carpus. This injury should be treated with open reduction and internal fixation of the styloid fracture. Radiolunate fusion or extrinsic ligament repair is suggested when the extrinsic ligaments are ruptured, resulting in ulnar translocation of the carpus. Dumontier C, Meyer ZU, Reckendorf G, et al: Radiocarpal dislocations: Classification and proposal for treatment: A review of twenty-seven cases. J Bone Joint Surg Am 2001;83:212.
Question 92
Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of

Explanation
This rare complication occurs after fracture-dislocation and has been seen after surgical stabilization in the adolescent. In most reported cases, prolonged observation has been shown to result in revascularization. Pateder DB, Park HB, Chronopoulos E, et al: Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent: A case report. J Bone Joint Surg Am 2004;86:2290-2293.
Question 93
High Yield
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?

Explanation
Excessive flexion gap tightness can be addressed with a variety of techniques; including: (a) recess and release the posterior cruciate ligament; (b) resect a posterior slope in the tibia; (c) avoid an oversized femoral component that moves the posterior condyles more distally; (d) resect more posterior femoral condyle and use a smaller femoral component placed more anteriorly; and (e) release the tight posterior capsule and balance the collateral ligaments.
Question 94
High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 95
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?


Explanation
A Weber type B ankle fracture occurs with a supination external rotation mechanism of injury. The fibula generally fails with a spiral fracture pattern. The lag screws provide compression, and the plate acts to neutralize rotational and angular bending forces. A buttress plate resists vertical shear forces. A tension band is used over areas that may fail in tension, such as an olecranon fracture. Compression is provided by the lag screws, and distraction is again resisted by the lag screws.
Question 96
Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?

Explanation
Ultrasound is best at imaging abrupt changes in the density of adjacent tissue and therefore is best at imaging wood in the soft tissues of the foot. Mizel MS, Steinmetz ND, Trepman E: Detection of wooden foreign bodies in muscle tissue: Experimental comparison of computed tomography, magnetic resonance imaging, and ultrasonography. Foot Ankle Int 1994;15:437-443.
Question 97
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?

Explanation
The first branch of the lateral calcaneal nerve innervates the abductor digiti minimi. It is reported to be trapped at the interval between the abductor hallucis and the quadratus plantae muscles.
Question 98
Ganglion cysts about the wrist most commonly arise from what structure?
Explanation
Ganglion cysts are the most common mass or mass-like lesions seen in the hand and wrist. They arise in a variety of locations, including synovial joints or tendon sheaths. The most common location is the dorsal/radial wrist arising from the dorsal scapholunate interosseous ligament.
Question 99
High Yield
Figure 2 shows the AP radiograph of an 18-year-old woman with progressive and severe right hip pain. Nonsteroidal anti-inflammatory drugs no longer control her pain. What is the next most appropriate step in management?

Explanation
A concentric hip with acetabular dysplasia in a symptomatic patient is best treated by periacetabular osteotomy. The Salter osteotomy is less optimal because the method has limited correction, is uniaxial, cannot be tailored to the deformity, and lateralizes the entire hip joint, thereby increasing the joint reactive forces. Because the hyaline cartilage of the joint is histologically normal, rotating the hyaline cartilage into an optimal position is preferable to augmenting the acetabulum with a shelf or by Chiari osteotomy. Varus intertrochanteric osteotomy has no significant role in the treatment of acetabular dysplasia. Total hip arthroplasty may be required in the future but should not be the first choice.
Question 100
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should

Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
