Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
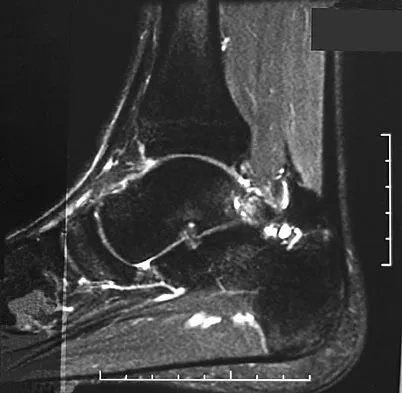
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of

Explanation
The imaging studies reveal findings typical of the os trigonum syndrome. This condition results from inflammation between the os trigonum and the adjacent talus. The symptoms of posterior ankle pain are exacerbated by plantar flexion, which stresses the fibrous union between these two bones. Definitive management of the high-level athlete involves excision of the os trigonum from a medial approach, although arthroscopic excision has also been described. The os trigonum is not an intra-articular structure; therefore, ankle arthroscopy is neither diagnostic nor therapeutic. Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057. Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Question 2
Which of the following factors has the greatest effect on the pull-out strength of a lumbar pedicle screw?
Explanation
All of the factors listed contribute to some extent to the pull-out strength of lumbar pedicle screws, but bone mineral density correlates most precisely. Wittenberg RH, Shea M, Swartz DE, et al: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Question 3
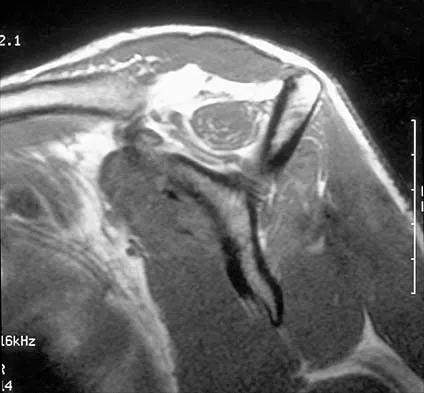
Examination of the shoulder seen in Figure 52 shows atrophy and tenderness of the infraspinous fossa and profound weakness in external rotation. The supraspinous fossa shows normal muscle bulk. What is the most likely cause of this condition?

Explanation
Compression of the suprascapular nerve by a ganglion cyst is a well-documented cause of pain and weakness in the shoulder. Isolated involvement of the infraspinatus indicates that the area of entrapment is at the spinoglenoid notch and not the suprascapular notch. The majority of ganglion cysts found in the shoulder are related to tears of the labrum. When such a compressive lesion is found, decompression can be accomplished through either an open or arthroscopic approach. Several authors have shown the value of arthroscopy in the treatment of this condition. It has been shown that it is technically possible to decompress a paralabral ganglion cyst using arthroscopy; this method is usually followed by repair of the torn labrum. Alternatively, arthroscopic repair of the labrum can be performed and the cyst may be aspirated at the time of surgery. Open cyst excision through a posterior approach is also an acceptable method of treatment. Schickendantz MS, Ho CP: Suprascapular nerve compression by a ganglion cyst: Diagnosis by magnetic resonance imaging. J Shoulder Elbow Surg 1993;2:110-114. Thompson RC, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187.
Question 4
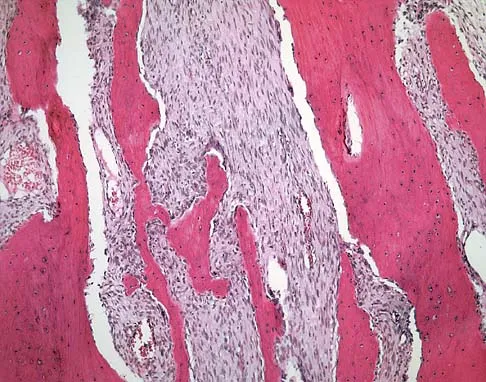
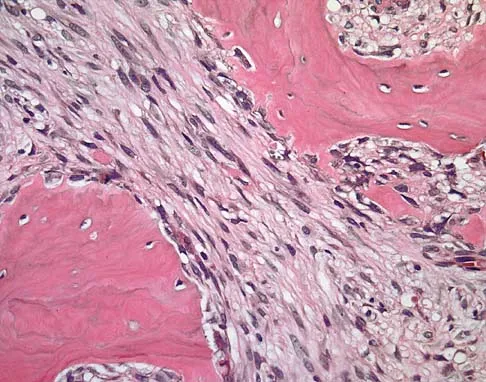
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?



Explanation
The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function. Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Question 5
High Yield
Injury to which of the following structures has been reported following iliac crest bone graft harvest?
Explanation
Injury to the lateral femoral cutaneous nerve and the ilioinguinal nerve have both been described with an anterior iliac crest bone graft harvest. The lateral femoral cutaneous nerve may be injured from retraction after elevating the iliacus muscle or from direct injury when the nerve actually courses over the crest. A posterior crest harvest can injure the superior gluteal artery if a surgical instrument violates the sciatic notch. Injury to the inferior gluteal artery has not been described; it leaves the pelvis below the piriformis muscle belly and should not be at risk even with a violation of the sciatic notch. Injury to the ilioinguinal nerve has been reported from vigorous retraction of the iliacus muscle after exposing the inner table of the anterior ilium. Cluneal nerve injury may occur with posterior crest harvest, particularly if the skin incision is horizontal or extends more than 8 cm superolateral from the posterior superior iliac spine. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 323-341.
Question 6
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?


Explanation
Crossover second toes are attributed to attenuation or rupture of the plantar plate and lateral collateral ligament and are associated with varying degrees of instability. Flexor-to-extensor transfer (Girdlestone/Taylor procedure) can provide intrinsic stability to the toe. Although plantar metatarsal head condylectomy can increase stability by resulting in scarring of the plantar plate, excision of the entire second metatarsal head carries a high risk of transfer metatarsalgia. Removal of the base of the proximal phalanx destabilizes the toe and should be reserved as a salvage procedure. Simple flexor tenotomy alone will not improve stability, and arthrodesis of the second metatarsophalangeal joint will limit motion and impair function. Coughlin MJ: Crossover second toe deformity. Foot Ankle 1987;8:29-39.
Question 7
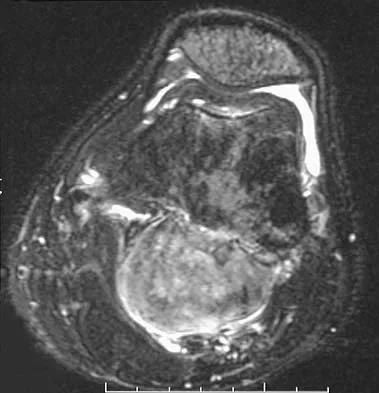
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of




Explanation
The diagnosis is synovial chondromatosis. While the plain radiograph fails to show any calcifications, the MRI scan shows an intra-articular mass that involves the capsule. Grossly multiple granular cartilage nodules are seen. Management should consist of removing all loose bodies along with the synovial membrane.
Question 8
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Explanation
The musculocutaneous nerve travels through the conjoined tendon approximately 8 cm distal to the tip of the acromion. The musculocutaneous nerve innervates the biceps muscle and the bracialis muscle, both of which are responsible for elbow flexion. Shoulder flexion is facilitated by the anterior fibers of the deltoid muscle (axillary nerve) and the supraspinatus muscle (suprascapular nerve). The subscapular muscle facilitates internal rotation of the shoulder (upper and lower subscapularis nerve). Shoulder abduction is performed by the deltoid muscle (axillary nerve), and forearm pronation is facilitated by the pronator teres (median nerve). Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 391-393.
Question 9
High Yield
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
Early postoperative wound infections after open reduction and internal fixation should be treated with aggressive debridement and maintenance of stability of the fracture. If infection persists following healing of the fracture, the hardware should be removed. Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Question 10
High Yield
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?

Explanation
C-reactive protein declines rapidly as the clinical picture improves. Failure of the C-reactive protein to decline after 48 to 72 hours of treatment should indicate that treatment may need to be altered. Blood culture is positive only 50% of the time and will be negative soon after antibiotics are administered, even if treatment is not progressing satisfactorily. WBC count is highly variable and poorly correlated with treatment. The ESR rises rapidly but declines too slowly to guide treatment. Radiographic findings may not change but can take up to 2 weeks to show changes.
Question 11
High Yield
Which of the following is not a reported mode of failure for a constrained acetabular component?
Explanation
There is no evidence of increased polyethylene wear in constrained acetabular components. The rates of wear appear to be the same using standard or constrained liners. Lachiewicz PF, Kelley SS: Constrained components in total hip arthroplasty. J Am Acad Orthop Surg 2002;10:233-238. Anderson MJ, Murray WR, Skinner HB: Constrained acetabular components. J Arthroplasty 1994;9:17-23.
Question 12
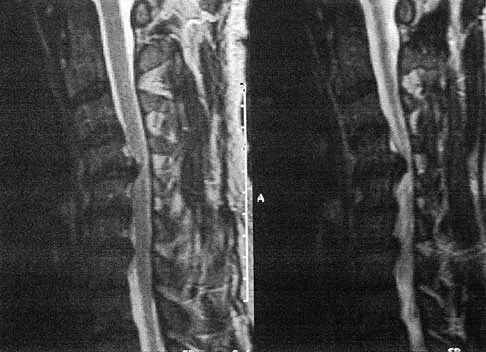
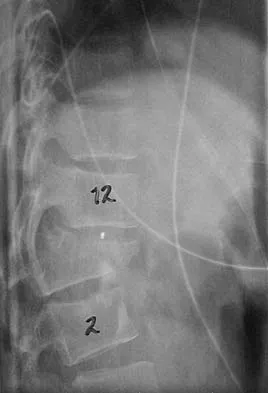
A 21-year-old man has had posterior neck discomfort for the past 6 months. Radiographs, an MRI scan, and a photomicrograph of the biopsy specimen are shown in Figures 17a through 17d. What is the most likely diagnosis?




Explanation
Forty percent of osteoblastomas occur in the spine, and they can become large and locally aggressive lesions. They generally occur in the posterior elements but can occur in the ribs and transverse processes. Microscopic analysis of the lesion will reveal hyperchromatic osteoblasts separated by incompletely mineralized bars of bone. Recommended treatment is en bloc excision. Fibrous dysplasia, giant cell tumor, and hemangioma can have similar radiographic appearances; therefore, biopsy may be required to differentiate them from more aggressive lesions. Osteochondromas are characterized by an osteocartilaginous growth arising from the cortex. Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1143-1174.
Question 13
Figure 13 shows the radiographs of a 20-year-old intercollegiate basketball player who was injured 6 weeks prior to the start of the season. What is the most appropriate treatment?

Explanation
A Jones fracture occurs at the metaphyseal-diaphyseal junction of the fifth metatarsal. It is often an acute fracture in conjunction with a chronic stress-related injury. It requires either a short leg cast with strict non-weight-bearing or surgical fixation. In the high performance athlete, the need for rapid return to sport activity usually requires surgical intervention, most commonly with an intramedullary screw. Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, vol 2, pp 2391-2409.
Question 14
Figure 29 shows the radiograph of a 55-year-old patient who has recurrent total hip dislocation. Dislocation is most likely to occur in this patient when the hip is in which of the following positions?

Explanation
The patient has an acetabular component that is placed in excessive anteversion; this is confirmed by the shoot-through radiograph. The most common reasons for dislocation of a total hip replacement include inappropriate positioning of the components, inadequate abductor tension, or impingement. Implants placed without adequate total anteversion tend to dislocate posteriorly, and implants with excessive anteversion tend to dislocate anteriorly. Superior dislocations can occur if the acetabular component is placed in a severely vertical position with inadequate lateral coverage.
Question 15
High Yield
An axillary nerve lesion may cause weakness in the deltoid and the
Detailed Explanation
While the most prominent functional deficit from axillary nerve lesions occurs from denervation of the deltoid, denervation of the teres minor also occurs.
Question 16
High Yield
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?

Explanation
Use of systemic steroids has been implicated in the development of nontraumatic osteonecrosis of the humeral head. Staging of the disease is most relevant to prognosis and treatment. Cruess has described a widely accepted staging system. Several authors have shown that patients who have a lower stage of disease (ie, stage I or II) have a much less likely chance of progression compared with those who are in the later stages (IV and V). Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39. Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Question 17
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?

Explanation
The patient has end-stage rotator cuff tear arthropathy. The radiograph shows complete proximal humeral migration (acromiohumeral interval of 0 mm), severe glenohumeral arthritis, and acetabularization of the acromion. In addition, she has "pseudoparalysis" with active elevation of only 30 degrees. Reverse shoulder arthroplasty affords her the best opportunity for pain relief and functional improvement. The other procedures have mixed results but typically are better for pain relief than they are for functional gains. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Question 18
High Yield
A 19-year-old football player who sustained three traumatic anterior shoulder dislocations underwent surgery to repair a Bankart lesion. Nine months after surgery, examination reveals stability, elevation to 150 degrees, external rotation to 0 degrees with the elbow at his side and to 50 degrees at 90 degrees of abduction, and internal rotation to T12. If his range of motion does not improve, he is at most risk for
Detailed Explanation
Loss of external rotation can lead to degenerative joint disease following an anterior stabilization procedure. A tight anterior capsule will prevent internal impingement. Risk of thoracic outlet syndrome should not be increased. Subscapularis detachment is a risk following open anterior repair; however, a gain in external rotation would be noted. In time, this patient's shoulder may show increased posterior glenohumeral wear but should not have symptoms of recurrent subluxation unless multidirectional instability is present. Hawkins RJ, Angelo RL: Glenohumeral osteoarthrosis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 19
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
A large annular defect at the site of a lumbar disk herniation is associated with persistent radicular pain postoperatively. Large sequestered herniations and a positive SLR preoperatively correlate with good outcomes after diskectomy. Neither symptoms of more than 3 months' duration nor preoperative epidural steroid injections correlate with postoperative results after diskectomy. Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Question 20
A 45-year-old man has had left thigh pain for the past 4 months. An AP radiograph, bone scan, MRI scans, and biopsy specimens are shown in Figures 6a through 6f. What is the most appropriate treatment?






Explanation
The radiograph demonstrates thickened trabeculae and thickened cortices in the left proximal femur compared to the right, and the bone scan shows increased uptake in this area. The MRI scans show thickened trabeculae with normal marrow signal. These findings are diagnostic of Paget's disease. Medical treatment, including bisphosphonates and calcitonin, is indicated for painful bone lesions. Hadjipavlou AG, Gaitanis IN, Kontakis GM: Paget's disease of the bone and its management. J Bone Joint Surg Br 2002;84:160-169.
Question 21
Figures 48a and 48b show the radiographs of a 26-year-old woman who fell down two steps and twisted her foot and ankle. What is the most appropriate treatment for this injury?


Explanation
The patient has a zone 1 base of the fifth metatarsal fracture (Pseudojones) that represents a less serious injury compared to zone 2 and 3 fractures with regard to healing potential. Treatment is symptomatic and casting is not necessary. These fractures are well treated with a hard-soled shoe for comfort and weight bearing as tolerated. Surgical intervention is not warranted. Vorlat P, Achtergael W, Haentjens P: Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop 2007;31:5-10. Wiener BD, Linder JF, Giattini JF: Treatment of fractures of the fifth metatarsal: A prospective study. Foot Ankle Int 1997;18:267-269.
Question 22
A 45-year-old woman has had radiating pain in the medial ankle for the past 3 months. Examination reveals a small mass in the retromedial ankle region and a positive Tinel's sign. An intraoperative photograph and a hematoxylin/eosin biopsy specimen are shown in Figures 24a and 24b. Treatment should consist of


Explanation
Neurilemoma is a benign tumor of nerve sheath origin, and peak incidence is in the third through sixth decades. The tumor is well encapsulated on the surface of a peripheral nerve. MRI findings may be significant for a "string sign." A positive Tinel's sign in the distribution of the nerve affected may be present. Grossly, the lesion is well encapsulated in a nerve sheath. Microscopically, there are structures referred to as Antoni A (a pattern of spindle cells arranged in intersecting bundles) and Antoni B (areas with less cellularity with loosely arranged cells). These lesions are benign, and treatment should consist of marginal excision. Nerve function may be preserved by careful dissection, excising the lesion parallel to the nerve fascicles so the lesion may be extruded. Recurrence is rare. Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Question 23
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
Cigarette smoking has been directly linked to pseudarthrosis in spinal fusions. The direct mechanism of action is diminished revascularization of cancellous bone graft. Additionally, a smaller area of revascularization is seen in these grafts, as well as an increased area of necrosis. Increased activity of osteoblasts would result in more bone production. Increased activity of osteocytes would not affect the fusion because osteocytes are mature bone cells.
Question 24
A patient undergoes the procedure shown in Figure 19. An important part of this procedure is preservation of what wrist ligament?

Explanation
Proximal row carpectomy is a salvage wrist procedure that yields a surprisingly stable construct. This has been attributed to two factors: 1) the congruency of the head of the capitate in the lunate fossa (this articulation is less congruent than the native lunate/lunate fossa relationship, but surprisingly stable), and 2) preservation of the radioscaphocapitate ligament, the most radial of the palmar extrinsic ligaments, which prevents ulnar subluxation after proximal row carpectomy.
Question 25
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed

Explanation
Very large corrections of tibial deformity can be achieved at or just below the tibial tubercle. This level of osteotomy maintains the relationship between the tubercle and the rest of the joint, does not alter patellofemoral mechanics, and avoids complicating possible future conversion to total knee arthroplasty. High tibial osteotomy is contraindicated for large corrections because of excessive elevation of the tibial tubercle and overhang of the lateral plateau. Correction in the tibial diaphysis creates a zig zag pattern in the tibia by correcting below the deformity and risks nonunion in cortical bone. There is no evidence that the femur is deformed; therefore, femoral osteotomy is not indicated.
Question 26
High Yield
Which of the following is considered the most predictive factor in determining whether a patient will need a blood transfusion after total knee arthroplasty?
Explanation
Multiple studies have shown that the preoperative hemoglobin level is the most predictive factor in determining whether a transfusion will be necessary after total hip or total knee arthroplasty. Studies have not shown any correlation with the other options. Salido JA, Marin LA, Gomez LA, Zorrilla P, Martinez C: Preoperative hemoglobin levels and the need for transfusion after prosthetic hip and knee surgery: Analysis of predictive factors. J Bone Joint Surg Am 2002;84:216-220. Sculco TP, Gallina J: Blood management experience: Relationship between autologous blood donation and transfusion in orthopedic surgery. Orthopedics 1999;22:S129-S134.
Question 27
Figures 20a and 20b show the radiographs of a 14-year-old boy who sustained a twisting injury to his ankle. If attempted closed reduction is unsuccessful, what is the primary reason to proceed with surgical treatment?


Explanation
Triplane fractures generally occur in children who are near skeletal maturity. The injury is generally caused by a supination external rotation mechanism. The number of fracture fragments present (two or three) depends on what part of the physes is closed at the time of injury. Articular congruity is the major concern in the management of these injuries since the patient has almost reached skeletal maturity. The goal is to restore articular congruity to minimize the development of posttraumatic arthritis. Vaccaro A (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765. Kling TF Jr, Bright RW, Hensinger RN: Distal tibial physeal fractures in children that may require open reduction. J Bone Joint Surg Am 1984;66:647-657.
Question 28
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 29
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
Iliosacral screws have gained popularity for posterior stabilization of pelvic ring disruptions, but complications attributed to incorrect placement are a clinical problem. The L5 nerve root is at greatest risk and is in closest proximity to a malpositioned screw (exiting the sacrum). The L4 root is more anterior at this level. The S1 root is still intraosseous at this level and is at risk but not from the screw exiting anteriorly at this level. The arteries are at risk but are more anterior and are at less risk than the L5 nerve root.
Question 30
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
Nonsurgical care for hallux rigidus involves limiting the motion of the first metatarsophalangeal joint during toe-off and ensuring that there is a deep enough toe box to accommodate dorsal osteophytes. A rigid shank or forefoot rocker both help to reduce the forces of extension during toe-off. Beskin JL: Hallux rigidus. Foot Ankle Clin 1999;4:335-353.
Question 31
High Yield
Which of the following statements regarding conus medullaris syndrome is most accurate?
Explanation
Conus medullaris syndrome most frequently occurs as a result of trauma or with a disk herniation at L1, resulting in a lower motor neuron syndrome but with a poor prognosis for recovery of bowel and bladder dysfunction. The conus region, as the termination of the spinal cord, contains the motor cell bodies of the sacral roots. The syndrome is usually a sacral level neural injury; therefore, lower extremity weakness is uncommon. Haher TR, Felmly WT, O'Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Question 32
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?



Explanation
The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function. Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Question 33
The quadrilateral space in the shoulder contains which of the following structures?

Explanation
The quadrilateral or quadrangular space of the shoulder is formed laterally by the humerus, proximally by the subscapularis (and teres minor viewed from posterior), distally by the teres major, and medially by the long head of triceps. The posterior humeral circumflex artery and axillary nerve pass through it. The axillary artery is more proximal. The radial nerve and profunda brachii pass through a triangular space more inferior. The circumflex scapular artery passes through a triangular space more medial. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, pp 205-206.
Question 34
What is the correct order of the elastic modulus of the following materials from greatest to least?

Explanation
In Young's modulus of elasticity, E is a measure of the stiffness of a material and its ability to resist deformation. In the elastic region of the stress-stain curve, E = stress/strain. The moduli of elasticity for these materials are alumina ceramic = 380 Gigapascals (GPa), cobalt-chromium = 210 GPa, stainless steel = 190 GPa, titanium = 116 GPa, and PMMA = 1.1 to 4.1 GPa. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 182-215.
Question 35
High Yield
A 25-year-old woman with a healed proximal tibiofibular fracture treated with an intramedullary nail 2 years ago is currently wearing an ankle-foot orthosis (AFO) and reports a persistent foot drop. She is unhappy with the AFO and has not seen any functional improvement despite months of physical therapy. Serial electromyograms (EMG) show no recent change over the past year. Examination and EMG findings are consistent with a tibialis anterior 1/5, extensor hallucis longus 2/5, extensor digitorum longus 2/5, posterior tibial tendon (PTT) 5/5, peroneals 3/5, flexor hallucis longus 5/5, and gastrocsoleus 5/5. No discrete nerve lesion was identified. The patient has a flexible equinovarus contracture. What is the most appropriate management?

Explanation
This pattern of injury is consistent with an unrecognized compartment syndrome of the anterior and lateral compartments. Transfer of the PTT through a long incision in the interosseous membrane corrects the foot drop deformity, and allows adequate dorsiflexion provided that the tendon to be transferred has a strength of 5/5. Muscles/tendons typically lose one grade of strength after transfer. Transfer into the tendons at the level of the ankle prevents overtensioning or pullout of a PTT tendon that is not long enough. Debridement of the scarred muscle in the anterior compartment decreases the risk of scarring down to the tendon transfer. Transfer of the peroneus longus is not preferred given its relative lack of strength and line of pull. Continued therapy and bracing are unlikely to lead to further improvement at 2 years after injury. An ankle fusion would correct the foot drop but would not address the tendon imbalances between the tibialis anterior and the peroneus longus, and the PTT and the peroneus brevis. Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 192. Atesalp AS, Yildiz C, Komurcu M, et al: Posterior tibial tendon transfer and tendo-Achilles lengthening for equinovarus foot deformity due to severe crush injury. Foot Ankle Int 2002;23:1103-1106. Scott AC, Scarborough N: The use of dynamic EMG in predicting the outcome of split posterior tibial tendon transfers in spastic hemiplegia. J Pediatr Orthop 2006;26:777-780.
Question 36
A 52-year-old woman with diabetes mellitus has had a plantar foot ulcer under the second metatarsal head for the past week. The patient had a similar ulcer 2 months ago, and total contact casting resulted in healing. Examination reveals no signs of infection. What procedure will best prevent recurrence of the ulcer?
Explanation
The contracted Achilles tendon leads to increased forefoot pressure, thus increasing the risk for ulceration in neuropathic patients. Several studies have shown the benefit of Achilles tendon lengthening to heal and prevent forefoot ulceration in these patients. The flexor hallucis longus transfer is used for chronically torn/deficient Achilles tendons, not a contracted Achilles tendon. The Jones procedure works well for the first ray but does not help to alleviate pressure under the second ray. Peripheral bypass surgery is unnecessary because the ulcer healed during the initial treatment, indicating that the patient has adequate circulation. The posterior tibial tendon transfer is used for foot drop or other neuromuscular conditions to correct deformity and increase function. It is not used for forefoot ulcers in patients with diabetes mellitus. Armstrong DG, Stacpoole-Shea S, Nguyen H, et al: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 37
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?

Explanation
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Question 38
Medial dislocation of the long head of the biceps tendon in the shoulder is most commonly caused by a
Explanation
Medial dislocation of the biceps tendon in the shoulder is commonly associated with subscapularis tendon tears. Although type II SLAP tears can result in bicipital instability, type I SLAP lesions do not. Congenitally shallow grooves and tears of the transverse ligaments usually do not lead to dislocation of the biceps tendon. Supraspinatus tendon tears are associated with long head of the biceps tendon ruptures but do not cause biceps tendon dislocations. Werner A, Mueller T, Boehm D, et al: The stabilizing sling for the long head of the biceps tendon in the rotator cuff interval: A histoanatomic study. Am J Sports Med 2000;28:28-31.
Question 39
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of


Explanation
Brodsky and associates reviewed 34 cases of cervical pseudarthrosis after anterior fusion. Seventeen were treated with revision anterior fusion and 17 with posterior foraminotomy and fusion. Good results were seen in 75% of patients who underwent revision anterior surgery, but better results (94%) were seen with posterior surgery, including foraminotomy and stabilization. Tribus and associates reported treatment of 16 patients with pseudarthrosis using revision anterior debridement of the fibrous tissue and fusion with autograft and plates. There was improvement of the neck in 75% of the patients, nonunion in 19%, continued weakness in 28%, and dysphagia in 5%. Farey and associates reported on 19 patients treated with posterior foraminotomy, stabilization, and fusion with a fusion rate of 100%, resolution of arm pain in 94%, resolution of weakness in 100%, and resolution of neck pain in 75%. It would appear that posterior foraminotomy is more effective for relieving arm pain and neurologic deficits associated with pseudarthrosis. Posterior fusion has the most reliable rate of arthrodesis in this setting. Dysphagia is reported in some patients undergoing more extensive anterior dissections required for applying plates. A neck brace is unlikely to aid in healing of pseudarthrosis in a patient who underwent surgery 8 months ago. A neck brace would be most effective within the first 3 months if a delayed union is identified. Brodsky AE, Khalil MA, Sassard WR, Neuman BP: Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair. Spine 1992;17:1137-1143. Tribus CB, Corteen DP, Zdeblick TA: The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine. Spine 1999;24:860-864.
Question 40
A 13-year-old girl has had increasing left hip pain for the past 4 months. A radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 1a through 1d. Which of the following immunohistochemistry results would confirm the most likely diagnosis?




Explanation
The imaging studies show a permeative lesion of the left hemipelvis with a large soft-tissue mass. The photomicrograph demonstrates a small blue cell tumor with pseudorosettes. The most likely diagnosis is primitive neuroectodermal tumor (Ewing's sarcoma family of tumors). MIC-2 is a highly sensitive and specific marker for this family of tumors. Cytokeratin is an epithelial marker. Vimentin is a mesenchymal marker. Thus, Ewing's sarcomas are cytokeratin negative and vimentin positive. Before discovery of the MIC-2 antigen, PAS and reticulin stains were commonly used to help differentiate Ewing's sarcoma from lymphoma. In contrast to lymphoma, Ewing's sarcomas are typically PAS positive and reticulin negative. Halliday BE, Slagel DD, Elsheikh TE, et al: Diagnostic utility of MIC-2 immunocytochemical staining in the differential diagnosis of small blue cell tumors. Diagn Cytopathol 1998;19:410-416.
Question 41
High Yield
What is the most appropriate indication for replantation in an otherwise healthy 35-year-old man?

Explanation
Vascular anastamoses are exceedingly difficult with amputations distal to the nail fold as the digital vessels bifurcate or trifurcate at this level, and little functional benefit is gained compared to other means of soft-tissue coverage. Single digit amputations, other than the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time of less than 6 hours. Urbaniak JR: Replantation, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1085.
Question 42
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Explanation
When attempting a revision anterior cervical approach from the side opposite the original approach, it is important to evaluate the function of the vocal cords. If this evaluation reveals dysfunction of the vocal cord on the side of the original approach, then an approach on the contralateral side should not be attempted. Injury to the stellate ganglion, which causes a Horner's syndrome, should not preclude an approach on the contralateral side. While the side of the symptomatology can influence the surgeon's choice as to the side of an anterior approach, it does not preclude a certain approach. When approaching the lower cervical spine from the right side, the recurrent laryngeal nerve can cross the surgical field and should be preserved. Excessive intraoperative pressure on the esophagus can increase the incidence of dysphagia, but its incidence is no different with either approach. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.
Question 43
A 10-year-old boy with severe hemophilia A (factor VIII) sustained an injury to his right forearm 2 hours ago when a classmate fell on his arm during a scuffle. Examination reveals moderate swelling in the forearm, decreased sensation in the distribution of the median and ulnar nerves, and pain on passive extension of the fingers. What is the most appropriate sequence of treatment?
Explanation
The patient has severe hemophilia with a volar forearm hemorrhage and an emerging compartment syndrome. Therefore, it is critical to normalize the clotting deficiency as the first step in treatment. In a patient who has a factor VIII level of less than 1% and no inhibitors to factor VIII, transfusion with 4 unit/kg will typically raise the factor VIII level to 100%. Continuous transfusion can then be used to maintain this level. Compartment pressures can be safely measured after infusion of factor VIII. Because the hemorrhage is of limited duration and any surgery is considered serious in a patient with hemophilia, the compartment pressure should be measured before making a decision regarding a fasciotomy. However, it is important to note that the use of factor VIII concentrates allows both emergency and elective surgery provided that adequate hematology backup is available. Splinting the elbow and wrist in flexion reduces the pressure in the volar compartments, protects the forearm from further trauma, and makes the patient more comfortable. Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell & Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 345-391. Greene WB, McMillan CW: Nonsurgical management of hemophilic arthropathy, in Barr JS (ed): Instructional Course Lectures 38. Park Ridge, Ill, American Academy of Orthopaedic Surgeons, 1989, pp 367-381.
Question 44
Which of the following describes the correct proximal to distal progression of the annular and cruciform pulleys of the digits?
Explanation
The correct progression of the annular and cruciform pulley in the digits is A1, A2, C1, A3, C2, A4, C3. The two cruciform pulleys are collapsible elements adjacent to the more rigid annular pulleys of the flexor tendon sheath. This arrangement enables unrestricted flexion of the proximal interphalangeal joint. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186.
Question 45
A 13-year-old boy has knee pain after sustaining a mild twisting injury while playing basketball 4 weeks ago. Radiographs and MRI scans are shown in Figures 24a through 24d, and biopsy specimens are shown in Figures 24e and 24f. Treatment should consist of






Explanation
The imaging studies and histology are consistent with high-grade osteosarcoma. The standard treatment for osteosarcoma is neoadjuvant chemotherapy combined with wide surgical resection that can be performed with amputation or limb salvage depending on characteristics unique to each tumor and each patient. In most patients, limb salvage surgery can be performed with reconstruction using allografts and/or megaprostheses. Osteosarcoma is poorly responsive to radiation therapy. Chemotherapy alone, in the absence of appropriate surgery, has not proven effective. Simon MA, Springfield DS: Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274.
Question 46
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?

Explanation
Tillaux and triplane fractures occur in adolescents as the result of an external rotation injury of the ankle. As seen on the CT scan, the growth plate starts to close during adolescence; therefore, growth arrest resulting in limb-length discrepancy or angulation is less of a concern in this age group than achieving joint congruity. The joint should be surgically reduced if displacement is greater than 2 mm to minimize the chances of late arthrosis. Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-278. Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Question 47
The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?

Explanation
Half pins placed in the AIIS are an alternative to pins placed in the iliac crest. A strong pillar of bone runs from the AIIS to the posterior iliac crest and less soft tissue is typically present in this area. The starting point is best seen on an obturator outlet view. The obturator outlet view is a combination of the pelvic outlet view and the obturator view of Judet and Letournel. The beam is rotated "over the top" of the patient since the iliac wing is externally rotated as well as cephalad to best visualize this column of bone running from the AIIS to the posterior iliac spine. This corridor of bone will appear as a teardrop. Once the correct view is obtained, the pin should be started at least 2 cm proximal to the hip joint to avoid placing a pin within the hip capsule. Blunt dissection and a guide sleeve should be used to prevent damage to the lateral femoral cutaneous nerve. An iliac oblique view is used after the pin has been partially inserted to make sure the pin is passing superior to the superior gluteal notch, and an obturator inlet view can be used at the completion of the procedure to make sure the pin is contained within the bone for its entire length. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 48
High Yield
Which of the following bearing materials is most resistant to scratching from third-body debris?
Detailed Explanation
Alumina is the hardest of all the materials listed. Clinical retrieval demonstrates resistance to scratching from third-body debris.
Question 49
In the radiograph shown in Figure 42, the fracture pattern around this well-fixed stem is classified as Vancouver type

Explanation
The Vancouver classifications describes periprosthetic hip fractures in the following way. Type A fractures are in the trochanteric region. Type B1 fractures occur around the stem or at the tip in the face of a well-fixed stem. These are usually treated with open reduction and internal fixation, usually including struts, cable, and/or cable plates. Type B2 fractures occur in the same region with a loose stem. Type B3 fractures occur with a loose stem where the proximal bone is of poor quality and/or severely comminuted. Type C fractures occur well below the stem. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 149-154. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 50
High Yield
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of

Explanation
Because the radiograph shows that the femoral stem is loose within the femoral canal and there is a fracture in the distal cement mantle, the stem should be revised. The Ogden-type plate and the allograft bone plates will reconstruct the femur but will not restore stability to the stem. Similarly, traction may allow the femur to heal but will not restore stability to the femoral stem within the femur. Resection arthroplasty is considered a salvage option following failure of the other procedures. Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Question 51
High Yield
The brachialis muscle is innervated by what two nerves?

Detailed Explanation
The brachialis is innervated by two nerves: medially, the musculocutaneous nerve; laterally, the radial nerve. The muscle is split longitudinally to approach the humerus anteriorly. Henry AK: The distal part of the humerus and front of the forearm, in Henry AK (ed): Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 90-115.
Question 52
Following a fall from a height of 5 feet, a patient reports pain along the lateral border of the foot. The CT scan shown in Figure 54 indicates what pathology?

Explanation
The CT scan reveals an avulsion of the dorsal beak of the anterior process of the calcaneus. This common fracture is an avulsion of the origin of the bifurcate ligament, which runs from the anterior calcaneal process to both the cuboid and the lateral aspect of the navicular. An inversion mechanism is common, and the fracture is often missed in evaluation for a suspected ankle sprain. MRI may be useful in the diagnosis of these occult injuries, and suspicion should be present when tenderness exists over the superior portion of the anterior process of the calcaneus.
Question 53
High Yield
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?

Explanation
The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 54
High Yield
What pharmacologic agents are preferred for the treatment of symptomatic active Paget's disease?

Explanation
Recent medical literature supports the use of bisphosphonates as the treatment of choice for active Paget's disease.
Question 55
High Yield
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of



Detailed Explanation
Open reduction and subscapularis and lesser tuberosity transfer into the defect is the treatment of choice in young individuals who have defects that involve between 20% to 45% of the head. Disimpaction and bone grafting is an option in injuries that are less than 3 weeks old. Closed reduction 2 to 3 months after injury usually is unsuccessful and increases the risk of fracture or neurovascular injury. Total shoulder arthroplasty is reserved for defects of greater than 50% or with associated glenoid surface damage. Hemiarthroplasty should be avoided in young individuals unless 50% or more of the head is involved. Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Question 56
Figures 28a and 28b show AP and lateral radiographs of the knee. Based on these findings, which of the following structures has most likely been injured?


Explanation
The radiographs show a posterior knee dislocation. Knee dislocations almost always involve rupture of both the anterior and posterior cruciate ligaments. Collateral ligament injuries also are common. Arterial, nerve, and tendon injuries each occur in less than half of knee dislocations. Schenck RC Jr, Hunter RE, Ostrum RF, et al: Knee dislocations. Instr Course Lect 1999;48:515-522.
Question 57
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?



Explanation
The MRI scans show disruption of the fibers of the PCL. Patients sustaining an isolated acute PCL injury can present with only minimal discomfort and have full range of motion. When examination reveals a contusion over the tibial tubercle and discomfort with the posterior drawer examination, with or without instability, a possible injury to the PCL should be considered. In acute injuries, the reported accuracy of MRI imaging for diagnosing PCL tears ranges from 96% to 100%. Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 58
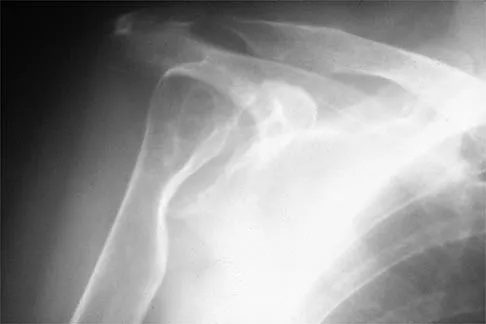
Figure 5 shows the radiograph of a 10-year-old girl who reports chronic shoulder pain after her gymnastics classes. Examination reveals pain on internal and external rotation but no instability. What is the most likely diagnosis?

Explanation
The patient has a very wide humeral growth plate, indicating the presence of a proximal humeral stress fracture, an uncommon diagnosis in gymnasts. Gymnasts are prone to stress fractures of the scaphoid, distal radius, elbow, and clavicle. Proximal humeral stress fractures are more commonly seen in those participating in racket or throwing sports. Stress fractures can lead to growth arrest or inhibition, particularly in the distal radius. The radiograph shows normal findings for the acromion, acromioclavicular joint, scapula, and triceps origin. Fallon KE, Fricker PA: Stress fracture of the clavicle in a young female gymnast. Br J Sports Med 2001;35:448-449. Sinha AK, Kaeding CC, Wadley GM: Upper extremity stress fractures in athletes: Clinical features of 44 cases. Clin J Sports Med 1999;9:199-202. Caine D, Howe W, Ross W, Bergman G: Does repetitive physical loading inhibit radial growth in female gymnasts? Clin J Sports Med 1997;7:302-308.
Question 59
A 68-year-old woman with a history of rheumatoid arthritis has had neck pain and weakness in all four extremities that has become worse in the past 6 months. She has gone from a community to a household ambulator and uses a wheelchair outside of the home. Examination of the extremities reveals poor coordination, diffuse weakness, hyperactive reflexes, and bilateral sustained clonus. She has a broad-based and unsteady gait. The posterior atlanto-dens interval is 12 mm. Based on these findings and the radiograph and MRI scan shown in Figures 13a and 13b, the treatment of choice is surgical decompression and stabilization. However, the patient inquires about the prognosis with surgery compared to nonsurgical management. Assuming there are no complications from surgery, the patient should be informed that, with surgery, she will most likely


Explanation
The patient has a cervical myelopathy with more than 10 mm of space available for the cord; therefore, she has a reasonable chance of improved neurologic function following surgery. If not treated with surgery, however, her neurologic condition likely will worsen and she will die earlier than if she had surgery. Matsunaga S, Sakou T, Onishi T, et al: Prognosis of patients with upper cervical lesions caused by rheumatoid arthritis: Comparison of occipitocervical fusion between C1 laminectomy and nonsurgical management. Spine 2003;28:1581-1587.
Question 60
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?

Explanation
Varus position of the stem is most commonly associated with failure of the cemented femoral component because of association with an inadequate cement mantle in the proximal medial and distal lateral zones. An inadequate cement mantle and obesity have been associated with increased loosening but not as frequently as a varus deformity. The influences of gender and osteoporotic bone on the outcome of cemented femoral components have not been established. Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Question 61
High Yield
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
The acromial branch of the thoracoacromial artery courses along the medial aspect of the coracoacromial ligament and may be encountered when performing an open or arthroscopic subacromial decompression. Bleeding can be controlled by ligation of its branch from the thoracoacromial artery. The other arteries may be injured in other surgical exposures of the shoulder. Esch JC, Baker CL: The shoulder and elbow, in Whipple TL (ed): Arthroscopic Surgery. Philadelphia, PA, JB Lippincott, 1993, pp 65-66.
Question 62
Which of the following best describes the course of the median nerve at the elbow?

Explanation
The median nerve courses superficial to the ulnar artery, deep to the fibrous arch of the superficialis muscle, and deep to the superficial head of the pronator teres muscle. The median nerve lies within the interval between the flexor digitorum superficialis muscle and the flexor digitorium muscle as it progresses toward the wrist. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 63
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
Explanation
Shock can be defined as inadequate tissue perfusion. Resuscitation or the resolution of shock is defined as when oxygen debt has been repaid, tissue acidosis is eliminated, and aerobic metabolism has been restored in all tissue beds. The end points for resuscitation are not clearly defined, but occult shock can still be present in the setting of normal vital signs and normal urine output due to selective perfusion of organ systems. Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: End point of resuscitation. J Trauma 2004;57:898-912. Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury, a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Question 64
A 12-year-old Little League pitcher reports lateral elbow pain and "catching." Examination reveals painful pronation and supination and tenderness over the lateral elbow. Radiographs are shown in Figures 22a and 22b. Initial management should consist of


Explanation
Osteochondritis of the capitellum is a common problem in young throwing athletes and gymnasts. The mechanism of injury involves lateral compression and axial loading of the capitellum. Repetitive trauma causes ischemia with resultant osteochondral necrosis and sometimes eventual separation. Initial management includes rest for a minimum of 6 weeks; occasionally bracing is used. At long-term follow-up, there is typically an observed radiographic abnormality indicating incomplete healing even in asymptomatic patients. Arthroscopy with in situ drilling is reserved for symptomatic lesions that have an intact articular surface. Lesions with partial separation often require fixation. Lateral column osteotomy is a new investigational procedure designed to relieve lateral compression forces and may be used in salvage cases. Kobayashi K, Burton KJ, Rodner C, et al: Lateral compression injuries in the pediatric elbow: Panner's disease and osteochondritis dissecans of the capitellum. J Am Acad Orthop Surg 2004;12:246-254.
Question 65
A 12-year-old girl has progressive development of cavus feet. Examination reveals slightly diminished vibratory sensation on the bottom of the foot. Reflexes are 1+ at the knees and ankles. Motor examination shows that all muscles are 5/5 in the foot, except the peroneal and anterior tibial muscles are rated as 4+/5. Which of the following studies is considered most diagnostic?
Explanation
The patient most likely has a form of Charcot-Marie-Tooth disease, or hereditary motor sensory neuropathy (HMSN). The most common varieties can now be diagnosed by DNA testing. Mutations have been detected in the peripheral myelin protein-22 (PMP-22) gene in HMSN type IA and in the connexin gene in the x-linked HMSN. Specific DNA diagnosis is useful in genetic counseling. Routine chromosomal testing most likely would not detect these mutations. Nerve conduction velocity study results are normal in some types of HMSN, and delayed nerve conduction, when found, indicates a peripheral neuropathy but does not specify the type or inheritance pattern. Biopsy of the sural nerve or of the quadriceps can be informative in some patients, but is not as specific as DNA testing. These procedures are most often reserved for patients with negative DNA test results. Chance PF: Molecular genetics of hereditary neuropathies. J Child Neurol 1999;14:43-52.
Question 66
A characteristic genetic translocation has been noted in which of the following tumors?

Explanation
There have been no characteristic gene translocations or rearrangements noted in osteosarcoma, chondrosarcoma, neurofibrosarcoma, or epithelioid sarcoma. In contrast, Ewing's sarcoma has been noted to have a consistent genetic translocation t(11:22). Brockstein BE, Peabody TD, Simon MA: Soft tissue sarcomas, in Vokes EE Golomb HM (eds): Oncologic Therapies. New York, NY, Springer-Verlag, 1999, pp 925-952.
Question 67
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be


Explanation
Although the patient has a large herniated nucleus pulposus, the pain has decreased from 10/10 to 3/10 over a 4-week period and the patient is now free of any neurologic symptoms. It is quite likely that further nonsurgical management will continue to resolve his symptoms. In the absence of any neurologic deficits, there is no evidence that the patient is at significant risk for paralysis. Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
Question 68
High Yield
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
Explanation
Because the patient has end-stage rheumatoid arthritis with glenoid and rotator cuff deficiency, humeral arthroplasty is the treatment of choice. When a patient has an intact rotator cuff and there is sufficient glenoid bone stock to implant a glenoid component, total shoulder arthroplasty is the preferred method because it appears to provide more predictable pain relief. Glenohumeral arthrodesis is generally avoided when there is a functional deltoid or rotator cuff. Open synovectomy is appropriate in early rheumatoid disease before articular changes are present. Anterior acromioplasty with coracoacromial ligament resection is avoided in patients with rheumatoid arthritis because this procedure compromises the coracoacromial arch and may result in anterosuperior instability. Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337. Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271. Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Question 69
Figures 51a and 51b show subluxation of the


Explanation
The extensor carpi ulnaris tendon is shown subluxated from its tunnel at the ulnar head; this requires disruption of the tendon's subsheath. Rowland SA: Acute traumatic subluxation of the extensor carpi ulnaris tendon at the wrist. J Hand Surg Am 1986;11:809-811.
Question 70
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of

Explanation
Following a CVA and with the resumption of upright posture, downward subluxation of the glenohumeral joint may occur. Although usually painless, some patients may report pain secondary to stretching of the brachial plexus. This is the result of flaccid paralysis of the deltoid muscle, and it will persist until some motor tone or spasticity returns to the shoulder girdle musculature. Early sling support and range-of-motion exercises to prevent contracture will provide the best relief. Surgical procedures are not indicated. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 71
A patient who underwent open reduction and internal fixation of an olecranon fracture 2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?


Explanation
The radiographs do not show an articular malunion. Treatment is directed at the soft-tissue contracture and should begin with formal physical therapy and static progressive splinting. Radiation therapy is effective in the perioperative period and is indicated when ectopic bone formation is a concern. Morrey BF: The posttraumatic stiff elbow. Clin Orthop Relat Res 2005;431:26-35.
Question 72
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical managment has failed to provide relief. What is the treatment of choice?

Explanation
The radiograph reveals the classic "bump" that is seen in patients with femoroacetabular impingement (FAI). Ganz and associates described two types of FAI. This patient has cam impingement, which describes a nonspherical femoral head being forced into the acetabulum during hip motion and resulting in labral and chondral injury. Hip arthroscopy and labral debridement is unlikely to control the symptoms because the underlying anatomic abnormality is often difficult to address with arthroscopy. The treatment involves surgical dislocation of the hip with preservation of the blood supply to the femoral head, removal of the asphericity on the femoral side (femoral osteoplasty), and removal of the acetabular rim (acetabular osteoplasty) if the latter is found to contribute to impingement. Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124. Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Question 73
High Yield
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?


Explanation
The patient has parosteal osteosarcoma. The posterior aspect of the distal femur is the typical location for this variant of osteogenic sarcoma. The imaging studies indicate a surface lesion with no involvement of the adjacent intramedullary canal. The histologic appearance is that of a low-grade fibroblastic osteosarcoma, consisting of relatively mature bone and a bland fibroblastic stroma lacking cytologic atypia and mitotic activity. A cartilaginous component is also frequently seen. Classic osteosarcoma typically has a more aggressive radiologic and histologic appearance. Sessile osteochondromas, while common behind the knee, have a presence of hematopoietic marrow and fat. The cartilage found in the associated cartilaginous cap is oriented. Chondrosarcomas are more typical in an older age group and have a histologic pattern consisting of malignant chondroid. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
Question 74
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
Two recent studies by Pollak and associates and Marsh and associates have focused on function after high-energy tibial plafond fractures. Findings are unfavorable even when anatomic reduction is performed in the best centers and patients are provided excellent rehabilitation. Function improves up to 2 years after injury, but even basic walking skills remain adversely affected. Virtually all patients have long-term adverse general health effects compared to their gender and age-matched peers. Posttraumatic degenerative arthritis is present in most ankles. Patients should be told early about the long-term prognosis, and early vocational/psychological counseling should be given. Despite these adverse outcomes, only a minority of patients require fusion or arthroplasty. Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 75
Which of the following statements best describes why the ulnar nerve is most prone to neuropathy at the elbow?

Explanation
The ulnar nerve is more prone to neuropathy than the radial or median nerves for many reasons. It has the greatest longitudinal excursion required to accommodate elbow range of motion, subjecting it to potential traction forces. The dimensions of the entrance of the cubital tunnel change with elbow motion, potentially causing compression in flexion. For these two reasons, the ulnar nerve is subjected to both compression and traction during elbow motion. Although it passes between two muscle heads as it enters the forearm, so do the median and radial nerves. Finally, the vascular supply is adequate because of the anastamoses between the superior ulnar collateral artery, the posterior ulnar recurrent artery, and the inferior ulnar collateral artery. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 369-378. Prevel CD, Matloub HS, Ye Z, Sanger JR, Yousif NJ: The extrinsic blood supply of the ulnar nerve at the elbow: An anatomic study. J Hand Surg Am 1993;18:433-438.
Question 76
High Yield
Figures 27a and 27b show the radiographs of a 32-year-old woman who was involved in a high-speed motor vehicle accident. She is neurologically intact. After stabilization and assessment, treatment should consist of

Explanation
The radiographs show a fracture-dislocation with translation in both the coronal and sagittal planes, evidence of significant instability requiring surgical stabilization. Anterior instrumentation is not as effective as posterior instrumentation in restoring stability, and because there is little bony destruction, the anterior column can be successfully reconstructed with simple realignment. The treatment of choice is multisegment posterior fusion with instrumentation. Lewandrowski KU, McLain RF: Thoracolumbar fractures: Evaluation, classification, and treatment, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 817-843.
Question 77
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
An inversion ankle injury typically involves ligamentous damage to the lateral ligaments of the ankle to include the anterior talofibular ligament and calcaneofibular ligament. Acute and particularly chronic ankle sprains also can have associated injuries. The inversion mechanism has been implicated in osteochondral and transchondral talar dome lesions, producing splits in the peroneus tendons, and in the development of meniscoid and soft-tissue impingement lesions in the anterolateral ankle. An inversion mechanism can also stretch the superficial peroneal nerve, leading to pain and paresthesias along its distribution. A fracture of the anterior colliculus is typically the result of an eversion mechanism resulting in a bony avulsion of the deltoid ligament from the anterior colliculus of the medial malleolus. Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Question 78
High Yield
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
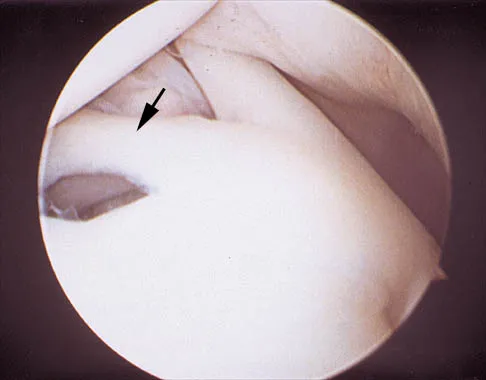
Explanation
The photograph shows a normal variant that is a sublabral hole beneath the anterosuperior labrum. In some instances, the labrum will become confluent with the middle glenohumeral ligament as a stout band. Because this variant is not abnormal, no treatment is necessary. Securing this portion of the labrum to the capsule may tighten the middle glenohumeral ligament complex and restrict external rotation of the arm. Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Question 79
High Yield
The first branch of the lateral plantar nerve innervates the
Explanation
The first branch of the lateral plantar nerve innervates the abductor digiti quinti, and more distal branches of the lateral plantar nerve supply the quadratus plantae and the interossei. The medial plantar nerve supplies the abductor hallucis brevis and the flexor digitorum brevis. Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Question 80
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?

Explanation
Hypertrophic cardiomyopathy (HCM) accounts for up to 50% of cases of sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH ("athlete's heart") from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm). Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete's heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436. Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Question 81
High Yield
A 13-year-old girl is diagnosed with a stage IIB osteosarcoma of the proximal tibia. Following neoadjuvant chemotherapy, local control should consist of
Explanation
Local control of osteosarcoma consists of wide resection and reconstruction. Radiation therapy is not recommended except in unresectable lesions or for palliation. Curettage and bone grafting result in intralesional resection with an unacceptable high rate of local recurrence. Chemotherapy alone is not adequate for local control. Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue. Philadelphia, PA, Lippincott Raven, 1998, p 274.
Question 82
A 22-year-old volleyball player reports the insidious onset of superior and posterior shoulder pain. Radiographs are normal. An MRI scan is shown in Figure 25. What is the most specific physical examination finding?

Explanation
Overhead athletes are prone to a number of problems involving the shoulder. Pitchers and volleyball players are susceptible to posterior superior labral tears and internal impingement. These patients will have posterior superior shoulder pain, a positive relocation sign, and a positive active compression test. Occasionally, these posterior superior labral tears are associated with a spinoglenoid cyst as seen in the MRI scan. These cysts cause compression of the suprascapular nerve which manifests primarily as weakness of the infraspinatus, resulting in weakness of external rotation. Romeo AA, Rotenberg DD, Bach BR Jr: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Question 83
High Yield
A 62-year-old man with diabetes mellitus has had a persistent 2-cm ulcer under the third metatarsal head for the past 4 months. He reports that he has had similar ulcers twice before, and both healed with nonsurgical management. He has used multiple types of commercial walking braces, shoes, and commercial dressings without resolution. He is insensate to the Semmes-Weinstein 5.07 monofilament. When the wound is probed with culture swab, there is no communication with the metatarsal head. Radiographs, bone scans, and laboratory studies reveal no evidence of osteomyelitis. What is the most predictable method of accomplishing wound healing without recurrence?
Explanation
The patient has a persistent diabetic foot ulcer without evidence of osteomyelitis. He has evidence of a sensory peripheral neuropathy and a concomitant motor neuropathy, leading to a dynamic motor imbalance. Use of a total contact cast would offer a high probability of healing the resistant ulcer but with a high potential for recurrence. Combining the total contact cast with Achilles tendon lengthening allows wound healing without a high risk for recurrence. Excision of the noninfected metatarsal head would make the patient vulnerable to the development of a transfer lesion under one of the remaining metatarsal heads. Robertson DD, Mueller MJ, Smith KE, et al: Structural changes in the forefoot of individuals with diabetes and a prior plantar ulcer. J Bone Joint Surg Am 2002;84:1395-1404.
Question 84
High Yield
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
Passive stretching is contraindicated during rehabilitation as it may potentiate the severity of the myositis ossificans. Electrical stimulation, iontophoresis, isometric exercise, and ice/heat contrast are not known to exacerbate this process. Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Question 85
The mother of a healthy 8-month-old boy reports that her son refuses to use his left arm. Examination reveals that the arm hangs limp at his side in an adducted and internally rotated position, and the affected shoulder subluxates posteriorly. Passive external rotation measures 15 degrees. Management should consist of

Explanation
Injury to the upper trunk of the brachial plexus during birth (Erb's palsy) occurs in approximately 1 in 3,000 births. In a complete lesion, paralysis of the deltoid, supraspinatus, infraspinatus, teres minor, biceps, and brachioradialis results in the findings described above. Spontaneous recovery may occur for up to 2 years. Passive exercises administered daily by the parents are the initial recommended treatment at this age. If significant contracture results in posterior dislocation, surgical correction may be considered. Neer CS: Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 452-454. Pearl ML: Arthroscopy release of shoulder contracture secondary to birth palsy: An early report on findings and surgical technique. Arthroscopy 2003;19:577-582.
Question 86
High Yield
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?

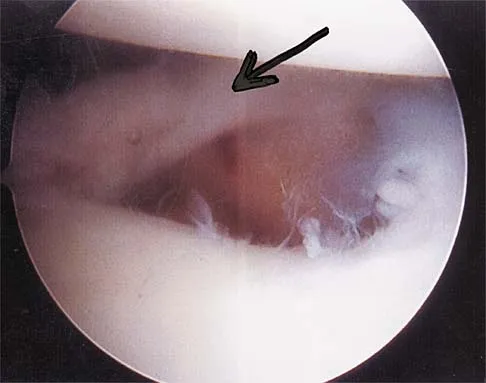
Explanation
The area shown in the arthroscopic view and MRI scan is referred to as a Buford complex and represents a normal labral variant. It consists of a thickened, cord-like middle glenohumeral ligament, a superior labral attachment of the middle glenohumeral ligament just anterior to the biceps tendon, and absence of the anterosuperior labrum. This combination of findings can be confusing and may simulate labral pathology. Mistaken repair of the lesion back to the glenoid rim can result in significant loss of external rotation. A Bankart lesion would be located at the inferior anterior glenoid rim. The subscapularis is seen anterior to the labrum. Normal variations that occur in the anterosuperior labrum can simulate pathology. Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 87
A 75-year-old woman has had severe shoulder pain for the past month. Her medical history includes hypertension and a total nephrectomy for renal cell carcinoma 7 years ago. Radiographs and sagittal MRI scans are shown in Figures 36a through 36d. A bone scan reveals this to be an isolated lesion. Biopsy findings are consistent with metastatic renal cell carcinoma. What is the most appropriate treatment for this patient?




Explanation
Resection and reconstruction of this very proximal lesion provides the best chance to avoid hardware complications that may be associated with stabilization procedures. Wide resection of isolated renal cell carcinoma metastasis, which presents distant to the nephrectomy, may improve long-term survival. Fuchs B, Trousdale RT, Rock MG: Solitary bony metastasis from renal cell carcinoma: Significance of surgical treatment. Clin Orthop Relat Res 2005;431:187-192.
Question 88
Which of the following patients is considered the most appropriate candidate for an isolated split posterior tendon transfer?

Explanation
Isolated split posterior tendon transfer alone is best performed in a patient with cerebral palsy who is between the ages of 4 and 7 years and has a flexible equinovarus foot. Rigid deformities often must be managed with a combination of soft-tissue and bony procedures. Patients with out-of-phase activity may be best managed with a transfer of the posterior tibialis to the dorsum of the foot, while those with continuous activity are better candidates for an isolated split posterior tendon transfer. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 291-294. Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
Question 89
High Yield
Figures 47a through 47f show the AP radiograph, bone scan, CT scan, MRI scan, and biopsy specimens of a 30-year-old woman who has had vague left shoulder pain for 1 year. Management should consist of




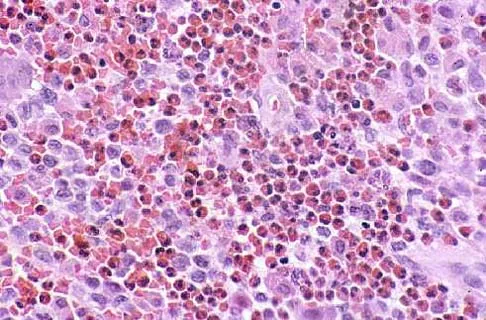
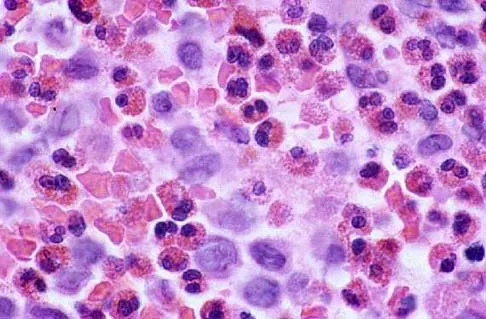
Explanation
The histology shows eosinophils with a background of larger cells (Langerhans' cells). This is consistent with eosinophilic granuloma. Localized sites are best treated with curettage, steroid injection, or observation. Chemotherapy is used only if there is systemic involvement. Mirra JM: Eosinophilic granuloma, in Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. London, England, Lea and Febiger, 1989, pp 1023-1060. Sessa S, Sommelet D, Lascombes P, Prevot J: Treatment of Langerhans-cell histiocytosis in children: Experience at the Children's Hospital of Nancy. J Bone Joint Surg Am 1994;76:1513-1525.
Question 90
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?


Explanation
The images demonstrate a L5 selective root block as it exits the L5-S1 foramen. This root block best helps relieve pain or paresthesias in the L5 distribution, which is the dorsal first web space and the great toe. The lateral foot is an S1 distribution and would need to be blocked through the posterior first sacral foramen. The anterior shin and thigh represent the L4 root which exits a level above this at the L4-5 foramen. A stocking distribution is nonanatomic and not indicative of a specific root. Magee D: Principles and concepts, in Orthopaedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Question 91
High Yield
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of
Detailed Explanation
Open reduction and subscapularis and lesser tuberosity transfer into the defect is the treatment of choice in young individuals who have defects that involve between 20% to 45% of the head. Disimpaction and bone grafting is an option in injuries that are less than 3 weeks old. Closed reduction 2 to 3 months after injury usually is unsuccessful and increases the risk of fracture or neurovascular injury. Total shoulder arthroplasty is reserved for defects of greater than 50% or with associated glenoid surface damage. Hemiarthroplasty should be avoided in young individuals unless 50% or more of the head is involved. Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Question 92
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?



Explanation
Anterior dislocation is the most common type of sternoclavicular dislocation. The medial end of the clavicle is displaced anterior or anterosuperior to the anterior margin of the sternum. In a study by Omer, 31% of athletic injuries have been known to cause a dislocation of the sternoclavicular joint. The serendipity view can show this dislocation, as will CT of the chest. This view requires the x-ray beam to be aimed at the manubrium with 40 degrees of cephalic tilt. An anterior sternoclavicular joint dislocation will appear superiorly displaced, while a posterior sternoclavicular joint dislocation is inferiorly displaced on the serendipity view. Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Question 93
High Yield
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?

Detailed Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Question 94
High Yield
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?

Explanation
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate. Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
Question 95
A 32-year-old man sustains multiple injuries in a motorcycle accident including ipsilateral open right femur and comminuted tibia fractures. He has acute abdominal distention and tenderness to palpation. The pelvis is stable to examination. He has a blood pressure of 70/40 mm Hg despite appropriate fluid resuscitation and a pulse rate of 120/min; the pulse is thready. Which of the following procedures is considered the highest priority in the management of this patient?

Explanation
The patient is in hemorrhagic shock, and timely hemostasis in the operating room should be the highest priority. Further imaging and insertion of central lines carry the risk of further delays in arresting the source of the patient's bleeding. Albumin (colloid) solutions have questionable indications, are expensive, and have been associated with increased mortality. Crystalloid solutions such as normal saline or lactated Ringer's solution are the initial resuscitative fluid of choice until blood becomes available. Pneumatic antishock garments have been associated with higher mortality rates, particularly in patients with cardiac and thoracic vascular injuries. Krettek C, Simon RG, Tscherne H: Management priorities in patients with polytrauma. Langenbecks Arch Surg 1998;383:220-227.
Question 96
A 49-year-old woman noted pain in her right axilla 1 day after moving heavy furniture. Two weeks later, she now reports persistent numbness and paresthesias along the inner aspect of her upper arm radiating into the ulnar digits. Examination reveals full shoulder motion, tenderness over the first rib, and a decreased radial pulse with the shoulder placed overhead. What is the most likely diagnosis?

Explanation
Thoracic outlet syndrome is thought to be caused by compression of the neurovascular supply to the upper limb in the supraclavicular and axillary regions of the shoulder. While typically progressive in onset, thoracic outlet syndrome may develop after acute injury. Injury or weakness of the scapular muscles, especially the trapezius, may result in descent of the scapula and cause compression of the thoracic outlet. In general, most symptoms are the result of neural compression. Typical symptoms include pain in the neck or shoulder and numbness or tingling that predominantly involves the ulnar side of the arm and hand. Exacerbation of these symptoms is typical when the arm is abducted. Initial management should consist of postural exercises aimed at restoring proper scapular stability. Severe recalcitrant symptoms may warrant surgical decompression. Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Question 97
High Yield
A 23-year-old woman reports right knee pain and fullness. The pain is worse with activity but also present at rest. Radiographs are shown in Figures 20a and 20b. What is the most likely diagnosis?


Explanation
The radiographs reveal a predominantly lytic, destructive lesion of the distal femur, although there is a hint of some blastic change as well. The lesion has violated the cortex, and there is mineralization outside the cortex laterally. The lateral radiograph suggests a soft-tissue density. These aggressive changes on radiographs in this age group are strongly suggestive of osteosarcoma. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 98
Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reveals a normal neurologic examination, and the patient reports no discomfort with the cast and crutches. Management should now include


Explanation
Stable fractures and minimally displaced fractures in children can and should be treated by closed methods. Because loss of reduction is common, alignment of tibia fractures must be monitored closely for the first 3 weeks after cast application. This is most easily handled in a cooperative patient by cast wedging. Some children require application of a second cast under general anesthesia 2 to 3 weeks after injury, particularly if the subsidence of swelling has caused the cast to loosen. Surgical indications include the presence of soft-tissue injuries, unstable fracture patterns, fractures associated with compartment syndrome, and the child with multiple injuries. Surgical options in children include percutaneous pins, external fixation, plates and screws, and intramedullary nails. Heinrich SD: Fractures of the shaft of the tibia and fibula, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1340-1346.
Question 99
High Yield
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45-degree lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
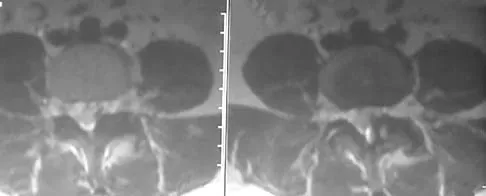
Explanation
There are several indications for extending adult scoliosis fusions to the sacrum, rather than stopping in the lower lumbar spine. These indications include posterior column deficiencies at L5-S1, such as spondylolysis and laminectomy, and deformities extending to the sacrum, such as fixed tilt of L5-S1 or sagittal imbalance. MRI signal changes in the L5-S1 disk do not preclude stopping the fusion at L5. Some surgeons use diskography or diagnostic facet blocks to evaluate the integrity of the L5-S1 level prior to stopping the fusion at L5. Long scoliosis fusions stopping at L5 have a significant risk of failure, highlighting the importance of careful selection of fusion levels. Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629. Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Question 100
High Yield
A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?


Explanation
In a relatively young patient who is an avid tennis player, the treatment of choice is a joint preserving procedure. The radiographs reveal varus alignment with loading of the medial compartment. After all nonsurgical management options have been used, the best treatment option is a medial opening wedge osteotomy. A lateral closing wedge osteotomy of the proximal tibia is also a reasonable option, but it is not one of the choices. A unicompartmental arthroplasty or a total knee arthroplasty would place significant restrictions in this patient. A unispacer may be a temporizing procedure but is controversial and without substantial data in the literature. The knee arthroscopy will not address the medial compartment osteoarthritis. Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358. Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
