Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
A positive jaw jerk reflex suggests that the problem is above the level of the pons. All of the other physical signs are exhibited in patients with cervical myelopathy. Although these signs also may be present in conditions affecting the brain, they do not help differentiate between a brain etiology and a cervical spine etiology. A jaw jerk reflex, however, is not present in patients with cervical myelopathy alone. Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493. Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
Question 2
High Yield
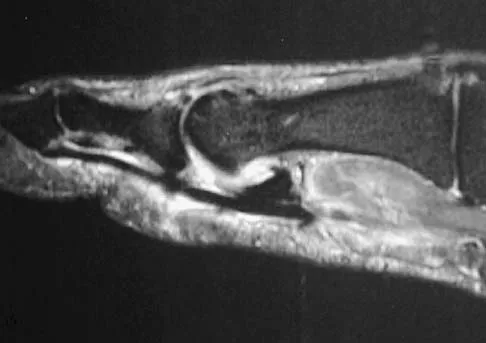
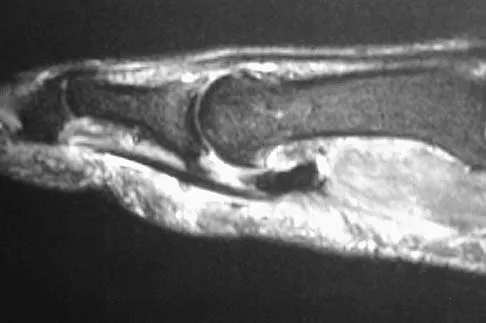
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T1- and T2-weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?


Explanation
The findings are most consistent with a rupture of the anterior tibial tendon. The damaged area of tendon should be resected, followed by tendon reconstruction or tenodesis. The histology is not consistent with giant cell tumor of the tendon sheath, gout, or synovial sarcoma. Fibromatosis is characterized by a large number of spindle cells within the collagen background. Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Question 3
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient?
Explanation
The patient has a burst fracture with probable unilateral entrapment of the cauda equina within the elements of the fractured lamina. A dural tear is likely in this scenario as well. It is recommended that this type of burst fracture be treated surgically with laminectomy, freeing of the entrapped nerve roots, and dural repair followed by stabilization of the fracture by either a posterior or combined approach. The degree of kyphosis and the extent of anterior canal compromise does not warrant corpectomy in this patient. Therefore, after completing the laminectomy and dural repair, posterior fusion and instrumentation should be sufficient to stabilize the fracture. Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 4
In patients who have undergone nonsurgical management for idiopathic adhesive capsulitis, long-term follow-up studies have shown which of the following results?
Explanation
Results have been satisfactory in many patients; however, at long-term follow-up, examination of the affected shoulder often shows some decrease in range of motion compared with the contralateral side. Although range of motion often improves over time, it does not return to normal in 60% of patients. Pain improves but is often increased compared with the contralateral side. Griggs SM, Ahn A, Green A: Idiopathic adhesive capsulitis: A prospective functional outcome study of nonoperative treatment. J Bone Joint Surg Am 2000;82:1398-1407.
Question 5
High Yield
What joint always remains uninvolved in all stages of scapholunate advanced collapse (SLAC) deformity of the wrist?
Explanation
The development of arthritis in SLAC wrist follows a consistent pattern. Beginning at the radial styloid to the scaphoid articulation, it progresses through the entire radioscaphoid joint and the midcarpal joint. In all stages, the radiolunate joint is spared, which is the basis for a scaphoid excision and four-corner fusion performed as a motion-sparing procedure for treatment of this condition. Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of arthritis. J Am Acad Orthop Surg 2003;11:277-281. Watson HK, Ballett FL: The SLAC wrist: Scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9:358-365.
Question 6
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling's test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis?

Explanation
The definition of brachial neuritis or Parsonage-Turner syndrome is a rare disorder of unknown etiology that causes pain or weakness of the shoulder and upper extremity. The loss of active motion excludes cervical C6-7 radiculopathy and impingement. A normal MRI scan and full passive motion exclude a rotator cuff tear and adhesive capsulitis, respectively. Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
Question 7
A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nonsteroidal anti-inflammatory drugs has failed to provide lasting relief. Examination reveals tenderness over the acromioclavicular (AC) joint and over the subacromial bursa. He has positive Neer and Hawkins impingement signs and AC joint pain with adduction of the shoulder. Radiographs are shown in Figures 36a and 36b. An MRI scan reveals an intact rotator cuff. Management should now consist of


Explanation
Because the patient has clinical and radiographic signs of AC arthritis and subacromial impingement, the treatment of choice is anterior acromioplasty and distal clavicle excision. Arthroscopic acromioplasty alone would not address the AC arthritis. The rotator cuff is intact; therefore, rotator cuff repair is not indicated. An open Mumford procedure would address the AC arthritis only and not the impingement symptoms. Immobilization might lead to stiffness of the shoulder and is not recommended for treating impingement.
Question 8
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70 degrees of the right knee. The active arc of motion is from 70 degrees to 90 degrees, and the opposite knee has a flexion contracture of 10 degrees. Both hips are dislocated with flexion contractures of 10 degrees, passive hip motion is from 10 degrees to 90 degrees of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
Most children with amyoplasia are ambulatory and when a decrease in function occurs because of a severe contracture, it must be addressed. A radical posterior soft-tissue release, including the posterior knee capsule and often the collateral ligaments and the posterior cruciate ligament, is needed to obtain extension. After the age of 1 year, aggressive physical therapy will do little to correct a contracture. Botulinum toxin A is indicated for spasticity and is contraindicated with severe contractures. Supracondylar femoral extension osteotomy works well, but will remodel at an average rate of 1 degree per month, which is not considered ideal in a young patient. Gradual correction with a circular ring external fixator is an option, but a soft-tissue release will also most likely be needed for a contracture of this severity. Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469. DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Question 9
High Yield
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?

Detailed Explanation
In the early 1990s, a transition was made from a two-incision ACL reconstruction to a single-incision ACL reconstruction, and there was concern over divergence of the femoral screws. It was shown radiographically that approximately 5% of the time, divergence of the screw was greater than 15 degrees from the bone plug. In a bovine model, there was significant loss of pull-out strength with an increase in divergence from 15 degrees to 30 degrees. Therefore, attempts should be made to minimize divergence to 15 degrees or less. Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Question 10
High Yield
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?

Explanation
Treatment of shoulder instability with thermal devices has lead to numerous complications including recurrent instability, chondrolysis, stiffness, and capsular necrosis. This patient's findings are consistent with a heat-induced axillary nerve injury. Normal radiographs exclude extensive chondrolysis. Levine WN, Bigliani LU, Ahmad CS: Thermal capsulorrhaphy. Orthopedics 2004;27:823-826.
Question 11
Management of a grade IV osteochondritis dissecans lesion of the capitellum should consist of
Explanation
Osteochondritis dissecans of the capitellum is seen most commonly in adolescent athletes. It should be distinguished from osteochondrosis of the capitellum (Panner's disease), a self-limiting condition seen in younger patients. Lesions are graded I through V based on radiographic and arthroscopic appearance. Grade I lesions show intact but soft cartilage. Grade II lesions show fissuring of the overlying cartilage. Grade III lesions show exposed bone or an attached osteoarticular flap that is not loose. Grade IV lesions show a loose but nondisplaced osteoarticular flap. Grade V lesions show a displaced fragment. Simple excision of the loose osteoarticular flap is the treatment of choice for grade IV and V lesions. More complex procedures such as drilling of the in situ lesion, bone grafting, or internal fixation are associated with significantly worse results. While some authors advocate abrasion chondroplasty, the long-term benefits of the procedure are yet to be proven. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Question 12
Which of the following best describes the course of the ulnar nerve in the midforearm?

Explanation
In the midforearm, the ulnar nerve travels deep to the flexor carpi ulnaris muscle and ulnar to the ulnar artery as it lies on the flexor digitorum profundus muscle. In this region, the ulnar nerve and artery lie side-by-side, whereas more proximal in the forearm, the ulnar artery originates from the brachial artery in the antecubital fossa, and the ulnar nerve lies within the cubital tunnel. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 13
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
The presence of a dorsal ulcer in the presence of weak or absent pulses strongly suggests the possibility of arterial insufficiency. The best initial noninvasive study to assess for ischemia is the Doppler arterial study. A determination of the vascular status is of a greater priority than an assessment for infection or neuropathy because of the location and presentation of the ulcer. If ankle pressures are less than 45 mm Hg, there is a high risk that these lesions will not heal without revascularization. Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Question 14
High Yield
What is the most appropriate orthosis for hallux rigidus?

Explanation
A Morton's extension limits excursion of the first metatarsophalangeal joint. It also functions as a ground reaction stabilizer during the toe-off phase of gait and thus reduces torque and joint reaction force at the first metatarsophalangeal joint. The metatarsal arch pad and full-length semi-rigid longitudinal arch support may help by dorsiflexing the first metatarsal relative to the phalanx and thus decompress the first metatarsophalangeal joint. However, they are not as biomechanically effective as the Morton's extension. Both medial hindfoot and lateral forefoot posting are contraindicated because they increase ground reaction at the first metatarsophalangeal joint. Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 611.
Question 15
An otherwise healthy 57-year-old woman has limited range of motion and moderate effusion after undergoing total knee arthroplasty 6 months ago. One of two cultures of joint aspirate reveals methicillin-resistant Staphylococcus epidermidis. Management should now consist of
Explanation
The rapidly increasing prevalence of infection from Staphylococcus epidermidis has made this the most frequently cultured organism. In most patients, the infection occurred intraoperatively, thereby resulting in a chronic infection if not detected within the first 6 weeks after surgery. Irrigation of the joint may be successful during this time in 60% of patients, but the most successful treatment is extirpation for 6 weeks, followed by delayed reimplantation. This approach may result in a salvage rate of as high as 90% in some patients. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993;24:751-759.
Question 16
What common cytologic abnormality is associated with Ewing's sarcoma?
Explanation
Cytogenetic abnormalities have been well characterized in a number of tumors. Translocation t (2, 13), (x, 18), (12, 16), and (12, 22) have been characterized in rhabdomyosarcoma, synovial cell sarcoma, myxoid liposarcoma, and clear cell sarcoma, respectively. Translocation t(11:22) can be identified in 95% of patients with Ewing's sarcoma. This was first described by Turc-Carel and associates in 1984. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, pp 105-118. Turc-Carel C, Philip I, Berger MP, Philip T, Lenoir GM: Chromosome study of Ewing's sarcoma (ES) cell lines: Consistency of a reciprocal translocation t(11;22) (q24;q12). Cancer Genet Cytogenet 1984;12:1-19.
Question 17
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction. Rockwood and Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Question 18
High Yield
A 14-year-old boy has had knee pain for the past 2 months. He also has a low-grade fever of 101.3 degrees F (38.5 degrees C). Laboratory studies show a WBC count of 12,100/mm3 and an erythrocyte sedimentation rate of 58/h. A biopsy specimen of a lesion in the distal femoral metaphysis is shown in Figure 38. What is the most appropriate treatment?

Detailed Explanation
The clinical presentation of this patient is consistent with both acute osteomyelitis and Ewing's sarcoma. Both entities can be noted in the distal femoral metaphysis although Ewing's sarcoma is classically noted in the diaphysis. The histology reveals a mixed inflammatory cell infiltrate with neutrophils, plasma cells, lymphocytes, and histiocytes. Ewing's sarcoma would be a uniform population of small round blue cells without an inflammatory component. Eosinophilic granuloma (EG) is characterized by Langerhans histiocytes and eosinophils. Treatment of EG often consists of an intralesional steroid injection. Treatment of acute osteomyelitis includes surgical debridement and antibiotics. McCarthy JJ, Dormans JP, Kozin SH, et al: Musculoskeletal infections in children: Basic treatment principles and recent advancements. Instr Course Lect 2005;54:515-528.
Question 19
Which of the following antibiotics is contraindicated in children?
Explanation
The tetracycline family of medications can stain teeth and bone in skeletally immature patients and as a result should be avoided in those patients. The remaining antibiotics have no known specific contraindication to use in children.
Question 20
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
Neurologic injury after shoulder replacement is relatively uncommon, occurring in 4% of shoulders in one large series. The importance of identifying and protecting the musculocutaneous and axillary nerves cannot be overemphasized; it is especially critical during revision arthroplasty when the normal anatomic relationships have been distorted. The long deltopectoral approach leaving the deltoid attached to the clavicle was found to be significant in the development of postoperative neurologic complications. A correlation was found between surgical time and postoperative neurologic complications, with long surgical times being associated with more neurologic complications. The presumed mechanism of injury is traction on the plexus that occurs during the surgery. A neurologic injury after total shoulder arthroplasty usually does not interfere with the long-term outcome of the arthroplasty itself; it is best managed by protective measures with passive range of motion of the involved extremity. Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 21
A superior labrum anterior and posterior (SLAP) lesion doubles the strain in which of the following stabilizing structures?
Explanation
A superior labrum, when intact, stabilizes the shoulder by increasing its ability to withstand excessive external rotational forces by an additional 32%. The presence of a SLAP lesion decreases this restraint and increases the strain in the superior band of the inferior glenohumeral ligament by over 100%. Rodosky MW, Harner CD, Fu FH: The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med 1994;22:121-130.
Question 22
High Yield
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Detailed Explanation
Weil osteotomies are useful in achieving shortening of a lesser metatarsal with preservation of the distal articular surface. The osteotomy is oriented from distal-dorsal to proximal-plantar; therefore, proximal displacement of the distal fragment is associated with plantar (not dorsal) displacement as well. Plantar displacement can result in the intrinsics acting dorsal to the center of the metatarsophalangeal joint and the development of an extended or "floating toe." Nonunion, osteonecrosis, and inadequate shortening are infrequent complications associated with the Weil lesser metatarsal osteotomy. Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Question 23
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
In the adolescent population, a lumbar herniated disk is characterized by a paucity of clinical findings, with a positive straight leg raising test the only consistently positive finding. This may result in a prolonged period of nonsurgical management that fails to provide relief. Activities that place a significant shear load on the lumbar spine, such as the dead lift, are associated with an increased risk of central disk herniation. An adolescent who lifts weights and has a history of back pain that fails to respond to a short period of active rest should undergo MRI evaluation for the diagnosis of a lumber herniated disk. Epstein JA, Epstein NE, Marc J, et al: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Question 24
High Yield
Turf toe typically involves injury to which of the following structures of the great toe?
Explanation
The term turf toe includes a range of injuries of the capsuloligamentous complex of the first metatarsophalangeal joint with or without osteochondral fracture of the first metatarsal head or one of the sesamoids. The mechanism of injury is hyperextension. Clanton TO, Butler JE, Eggert A: Injuries to the metatarsophalangeal joints in athletes. Foot Ankle 1986;7:162-176.
Question 25
What is the most frequent complication following primary total hip arthroplasty?
Explanation
Thromboembolic disease can occur in up to 58% of unprotected patients and up to 20% of protected patients depending on the type of prophylaxis used, even though most thrombi are small and have little clinical consequence. The primary goal of prophylaxis is to prevent symptomatic deep venous thrombosis and fatal pulmonary emboli. Dislocation has been reported in up to 10% of primary cases, but generally acceptable rates of less than 5% are the norm. Component loosening following primary total hip arthroplasty is rare prior to a 10-year follow-up, and 90% to 95% of patients should reach the 10-year follow-up without the need for revision for any reason. Metal hypersensitivity is unusual, and nickel found in cobalt-chromium alloys is the most common offending agent. Infection of primary total hip arthroplasty is less than 1%. Eftekhar N: Total Hip Arthroplasty. St Louis, MO, Mosby,1993, pp 1445-1676.
Question 26
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 27
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Explanation
Chondrocytes are obtained from cartilage harvested from non-weight-bearing areas of the knee. The extracellular matrix is digested, and the chondrocytes are expanded for later transplantation. Cells implanted into a defect are secured with a flap of periosteum. Cells are expanded to obtain 20 to 50 times the original number of cells to transplant at a cell density of 3x10-7 cells/mL. There is a direct relationship between cell number and biosynthetic activity. Osteochondral lesions of up to 8 mm may be treated with autologous transplant alone; larger depth lesions should be bone grafted at the time of harvest. Mesenchymal stem cells differentiate easily into fibrous tissue, bone, and fat; conversion of mesenchymal stem cells into cartilage in vitro currently is difficult to accomplish. Goldberg and Caplan, however, were able to obtain cartilage repair using mesenchymal stem cells transplanted into defects in rabbits in vivo. In animal studies, fluorescent-labeled cells persist for at least 14 weeks, integrate with the surrounding normal margins, and become part of the repaired tissue replete with sulfated proteoglycans and type II collagen. Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am 2003;85:109-115.
Question 28
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?

Explanation
Burks and Schaffer described an approach to the tibial insertion of the posterior cruciate ligament that uses the interval between the semimembranosus and the medial gastrocnemius. The medial gastrocnemius muscle is retracted laterally and protects the neurovascular bundle. This approach is used to repair an avulsion of the posterior cruciate ligament tibial attachment or for performing a posterior cruciate ligament tibial inlay reconstruction. Berg EE: Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy 1995;8:95-99.
Question 29
High Yield
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?
Explanation
The standard approach to the volar aspect of the distal radius is the Henry approach. Following incision of the skin and subcutaneous tissues, the forearm fascia is incised. The radial artery and venae comitantes lie in the interval between the tendons of the flexor carpi radialis muscle and the brachioradialis muscle. This interval is developed, and the radial artery and veins are retracted in a radial direction. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 30
A 12-year-old boy sustained a both bone forearm fracture 10 weeks ago and underwent closed reduction and casting. Examination now reveals that the injury is healed, but he is unable to extend his little and ring fingers of the injured hand with his wrist extended. Full extension is possible with the wrist flexed. A radiograph and clinical photograph are shown in Figures 15a and 15b. The remainder of his hand and wrist examination and neurologic evaluation in the hand are normal. What is the most likely diagnosis?


Explanation
In this patient, examination reveals an inability to extend the fingers with the wrist extended, but full extension is possible with wrist flexion. These findings demonstrate isolated tenodesis of the flexor digitorum to the ring and little fingers. These findings are not consistent with compartment syndrome or nerve injury. Scarring or entrapment of tendons in forearm fractures can occur. Watson PA, Blair W: Entrapment of the index flexor digitorum profundus tendon after fracture of both forearm bones in a child. Iowa Orthop J 1999;19:127-128. Shaw BA, Murphy KM: Flexor tendon entrapment in ulnar shaft fractures. Clin Orthop 1996;330:181-184. Kolkman KA, van Niekerk JL, Rieu PN, et al: A complicated forearm greenstick fracture: Case report. J Trauma 1992;32:116-117.
Question 31
High Yield
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Detailed Explanation
A knee dislocation carries the potential for an arterial injury and has always brought up the question of need for arteriography to rule out this limb-threatening injury. However, arteriography has an inherent complication rate that may compromise the general care of the patient. In over 240 published cases with documented knee dislocations that were evaluated for vascular injury by physical examination (without imaging studies), not a single missed injury was reported, for a 100% negative predictive value (0% false-negative rate). This degree of accuracy at excluding major vascular injury is unsurpassed by the results obtained with arteriography but with no risk involved and a marked savings in time, equipment, and costs. Therefore, the most appropriate first step to rule out vascular injury is examination of the pedal pulses. If there is any doubt about an arterial injury, another option is the ankle-brachial index (ABI). If the ABI is greater than 0.9, the chance of arterial injury is again nonexistent. However, a positive physical examination or an ABI of less than 0.9 is not 100% predictive of an arterial injury; therefore, arteriography is recommended. Miranda FE, Dennis JW, Veldenz HC, et al: Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: A prospective study. J Trauma 2002;52:247-252.
Question 32
High Yield
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Explanation
The patient has snapping hip syndrome of the internal type, which is more common in ballet dancers. It is caused by the iliopsoas tendon gliding over the iliopectineal line or the femoral head. The diagnosis usually can be made by the history and physical examination. Snapping is reproduced by hip flexion and extension or flexion with external rotation and abduction. Conventional and dynamic ultrasonography will confirm the snapping structure. Radiographs occasionally show calcifications near the lesser trochanter. MRI can be used to rule out other diagnoses that can simulate snapping hip. Gruen GS, Scioscia TN, Lowenstein JE: The surgical treatment of internal snapping hip. Am J Sports Med 2002;30:607-613.
Question 33
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of


Explanation
The underlying diagnosis is multiple myeloma. Because the patient has a large lucent lesion in the peritrochanteric region of the left proximal femur, the risk of pathologic fracture is high. Consideration should be given to prophylactic internal fixation with a locked intramedullary rod. The lesion does not appear to be a sarcoma requiring wide resection and endoprosthetic reconstruction. Neither chemotherapy nor radiation therapy alone is likely to result in long-term stabilization of the proximal femur. Postoperative treatment with bisphosphonates and radiation therapy is indicated to decrease the risk of future pathologic fractures. The patient should also be referred to a medical oncologist for medical management. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Question 34
High Yield
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in

Explanation
The surface hardness of titanium is low compared with that of cobalt-chromium alloys. Titanium articulations are easily scratched, resulting in a significantly increased rate of wear and debris production. The wear and resulting lysis can also result in an increased rate of loosening. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Question 35
What is the most prevalent adverse event associated with allogeneic blood transfusion?

Explanation
Clerical error leading to acute hemolysis and even death occurs in 1:12,000 to 1:50,000 transfusions. Bacterial contamination leading to sepsis/shock occurs in 1:1 million transfusions. HIV transmission is approximately 1:500,000 transfusions and hepatitis C is 1:103,000 transfusions. Anaphylactic reactions occur in 1:150,000 transfusions. Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Question 36
A 24-year-old dancer reports posterior ankle pain when in the "en pointe" position. Examination reveals posteromedial tenderness, no pain reproduction with passive forced planter flexion, and pain with motion of the hallux. What is the most likely diagnosis?
Explanation
Flexor hallucis longus tendinitis is a common cause of posterior ankle pain in dancers. It tends to be more posteromedial and is characterized by a clicking or catching sensation posteromedially with motion of the great toe. A painful os trigonum typically causes more posterolateral ankle pain and may occur after an ankle sprain or plantar flexion injury where there may be a fracture of the os trigonum. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 249-261.
Question 37
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?

Explanation
The tibia has grown into valgus secondary to the proximal fracture. This occurs in about one half of these injuries, and maximal deformity occurs at 18 months postinjury. The deformity gradually improves over several years, with minimal residual deformity. Therefore, treatment at this age is unnecessary as there is a high rate of recurrence and complications regardless of technique. The valgus deformity is not a result of physeal injury or growth arrest. Medial proximal tibial hemiepiphysiodesis is an excellent method of correcting the residual deformity but is best reserved until close to the end of growth. Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482. McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 38
When performing a long fusion to the sacrum in an osteopenic patient in whom optimal sagittal balance is restored, which of the following is a benefit of extending the distal fixation to the pelvis, rather than the sacrum alone?

Explanation
In osteopenic individuals, even those with excellent obtained or maintained balance, long instrumented fusions to the sacrum impart a high degree of strain, and the sacrum may fail in a transverse fracture or fracture-dislocation pattern. The risk of proximal functional kyphosis is unrelated to distal fixation as are coronal plane correction and rod contouring. Pubic ramus fractures have been shown to be associated with both fixation to the sacrum alone as well as to the ilium.
Question 39
Which of the following is considered the most useful screening method for the evaluation of protective foot sensation in a patient with diabetes mellitus?
Explanation
Patients with diabetes mellitus should be screened for the presence of protective foot sensation. In the absence of protective foot sensation, patients are at increased risk for the development of neuropathic ulcerations and neuropathic arthropathy. The most reliable screening tool for the presence of protective sensation is the ability to feel the 5.07 Semmes-Weinstein monofilament. Pinzur MS, Shields N, Trepman E, Dawson P, Evans A: Current practice patterns in the treatment of Charcot foot. Foot Ankle Int 2000;21:916-920.
Question 40
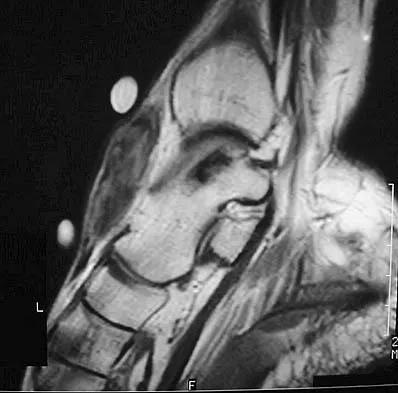
High Yield
Which of the following structures runs through the site indicated by the arrow in Figure 11?

Explanation
The vertebral artery traverses through the arcuate foramen after exiting the lateral aspect of C1 and before entering the skull. The foramen usually is not fully formed, but a complete foramen such as this one has been reported in up to 18% of patients. Stubbs DM: The arcuate foramen: Variability in distribution related to race and sex. Spine 1992;17:1502-1504.
Question 41
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?


Explanation
The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
Question 42
A 31-year-old woman has increasing pain and tightness in her right knee, with occasional stiffness and recurrent hemorrhagic effusions. MRI scans are shown in Figures 2a and 2b. What is the most likely diagnosis?


Explanation
PVNS is a rare inflammatory granulomatous condition of unknown etiology, and causes proliferation of the synovium of joints, tendon sheaths, or bursa. The disorder occurs most commonly in the third and fourth decades but can occur at any age. MRI provides excellent delineation of the synovial disease. Characteristic features of PVNS on MRI include the presence of intra-articular nodular masses of low signal intensity on T1- and T2-weighted images and proton density-weighted images. Synovial biopsy should be performed if there is any doubt of the diagnosis. Total synovectomy (open or arthroscopic) is required for the diffuse form, although recurrence is common. Rheumatoid arthritis and synovial chondromatosis are not typically associated with hemorrhagic effusions. De Ponti A, Sansone V, Malchere M: Result of arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 2003;19:602-607. Chin KR, Barr SJ, Winalski C, et al: Treatment of advanced primary and recurrent diffuse pigmented villonodular synovitis of the knee. J Bone Joint Surg Am 2002;84:2192-2202.
Question 43
High Yield
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of
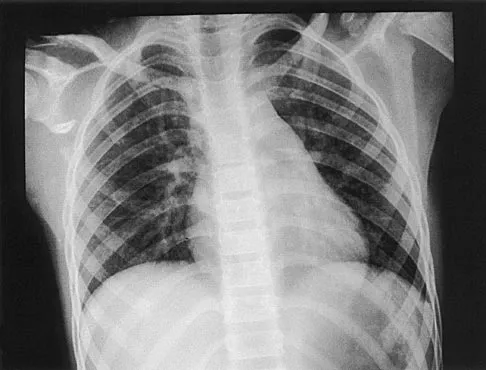


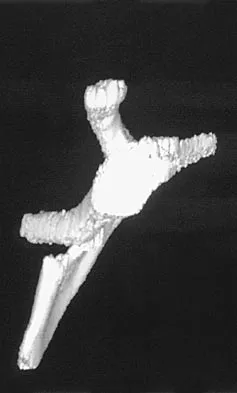
Explanation
Scapular body fractures in children are rare and are often associated with other injuries of the chest and thorax. Management is generally nonsurgical, unless the injury is open, and usually consists of support with a sling and gentle range-of-motion exercises to minimize shoulder stiffness. Green N, Swiontkowski M: Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 3, pp 319-341.
Question 44
High Yield
Which of the following factors can contribute to patellar subluxation following routine total knee arthroplasty?

Explanation
Excessive resection of the lateral facet of the patella can lead to subluxation. Rotational alignment of the components can have a significant impact on patellar tracking. Internal rotation of the femoral component leads to more lateral alignment of the patella within the trochlear groove. Internal rotation and medial placement of the tibial component results in lateralization of the tibial tubercle with an increase in the Q angle. Excessive valgus alignment of the mechanical axis, or insufficient correction of preoperative valgus, has a similar effect on the Q angle, and both can result in a higher rate of tracking problems.
Question 45
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
The patient's neurologic examination is consistent with a C7 radiculopathy on the right side. In a patient with this symptom complex in the absence of trauma, a cervical disk herniation is the most common etiology for a C7 radiculopathy. There are eight cervical nerve roots and the C7 nerve exits at the C6-7 disk space and is most frequently impinged by a disk herniation at this level. Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Question 46
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of

Explanation
Near complete correction and rebalancing of the spine can be achieved by hemivertebral resection that may be done as either a simultaneous or a staged procedure in the young patient. This eliminates the problem of future progression and possible development of compensatory curves. Nonsurgical management is not indicated in congenital scoliosis. Convex hemiepiphyseodesis is best suited for patients younger than age 5 years who have a short curve caused by fully segmented hemivertebrae that correct to less than 40 degrees with the patient supine. Hemiepiphyseodesis and isolated posterior fusion are not indicated. Bradford DS, Boachie-Adjei O: One-stage anterior and posterior hemivertibral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am 1990;72:536-540.
Question 47
High Yield
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
Convex hemiarthrodesis and hemiepiphysiodesis are procedures designed to gradually reduce curve magnitude in congenital scoliosis because of hemivertebrae. They are used to surgically create an anterior and posterior bar to arrest growth on the convexity of the existing deformity. Success of the technique is predicated on continued growth on the concave side of the deformity. Prerequisites for this procedure include curves of limited length (less than or equal to five vertebrae), curves of reasonable magnitude (less than 70 degrees), absence of kyphosis, concave growth potential, and appropriate age (younger than age 5 years).
Question 48
When performing a Weil osteotomy of a lesser metatarsal, the desired angle of the saw cut should be approximately
Explanation
Appropriate orientation of the saw cut when performing a Weil osteotomy is approximately parallel with the plantar surface of the foot. This is done in an effort to minimize plantar displacement of the capital fragment. The removal of additional bone from the osteotomy site either by removing a separate wafer of bone or using a thicker saw blade has also been described to minimize plantar displacement of the distal fragment. Trnka H, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Question 49
Examination of a hand with compartment syndrome is most likely to reveal which of the following?

Explanation
In a study of 19 patients with compartment syndrome of the hand, all had tense swollen hands with elevated compartment pressures. Most patients were neurologically compromised so pain with passive stretch may be difficult to illicit. Arterial inflow is present in the arch and thus pallor is not present. The typical posture of the hand is not clenched, rather it is an intrinsic minus posture of metacarpophalangeal joint extension and flexion of the proximal and distal interphalangeal joints. Oullette EA, Kelly R: Compartment syndromes of the hand. J Bone Joint Surg Am 1996;78:1515-1522.
Question 50
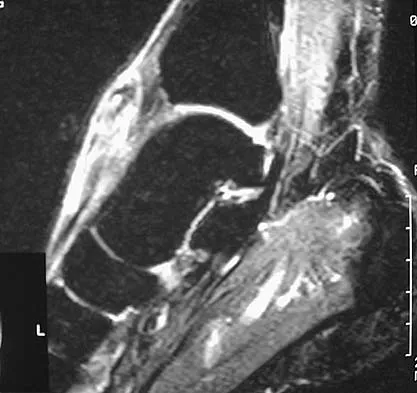
High Yield
Figure 35 shows the radiograph of a 44-year-old woman with rheumatoid arthritis who reports neck pain. Below what threshold number is surgical stabilization warranted for the interval shown by the arrow?

Detailed Explanation
The posterior atlanto-dens interval represents the space available for the spinal cord and a distance of less than 14 mm is predictive of neurologic progression, thus warranting consideration for fusion, even in the absence of symptoms.
Question 51
High Yield
A 13-year-old girl who is 2 years postmenarche has been referred for management of scoliosis. She denies any history of back pain. Radiographs show a right thoracic curve of 35 degrees. She has a Risser sign of 4 and a bone age of 15.5 years. Management should consist of
Detailed Explanation
Because the patient is skeletally mature with a curve of less than 40 degrees, there is no benefit to bracing and surgery is not indicated. Management should consist of observation and follow-up radiographs in 6 months. Lonstein JE, Carlson JM: The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am 1984;66:1061-1071.
Question 52
High Yield
A 45-year-old man sustains a low-velocity gunshot wound to the base of the right thumb. The open wound is allowed to heal by secondary intention, resulting in a contracture of the first web space. Clinical photographs are shown in Figures 49a through 49c. Treatment should now consist of



Explanation
The contracture is too large for a Z-plasty, which allows a 75% increase in length. Excision of the scar with placement of a skin graft is prone to contracture. A posterior interosseous fasciocutaneous flap will provide enough well-vascularized tissue and is well suited to reach the first dorsal web space. Buchler U, Frey HP: Retrograde posterior interosseous flap. J Hand Surg Am 1991;16:283-292.
Question 53
A 52-year-old man has had groin and deep buttock pain for the past 2 months. Examination reveals that hip range of motion is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 28. Management should consist of

Explanation
The MRI findings show highly increased signal through the entire femoral head and neck that is diagnostic of transient osteoporosis of the femoral head. This recently described entity is often seen in middle-aged men and should be treated nonsurgically with protected weight bearing and anti-inflammatory drugs. The natural history is that of self-resolution. Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Question 54
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis?

Explanation
The MRI scan shows an ALPSA lesion. This is also known as a medialized Bankart with medial displacement of the torn anterior labrum. During surgical stabilization, the labrum and periosteal sleeve must be mobilized and repaired laterally to reduce recurrent instability. A Perthes lesion is a nondisplaced labral tear. A GLAD lesion represents a nondisplaced anterior labral tear with an associated articular cartilage injury. Neviaser TJ: The anterior labroligamentous periosteal sleeve avulsion lesion: A cause of anterior instability of the shoulder. Arthroscopy 1993;9:17-21.
Question 55
High Yield
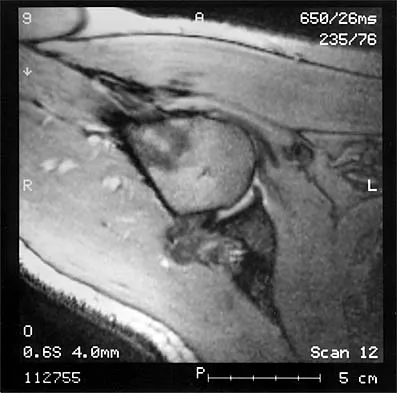
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of



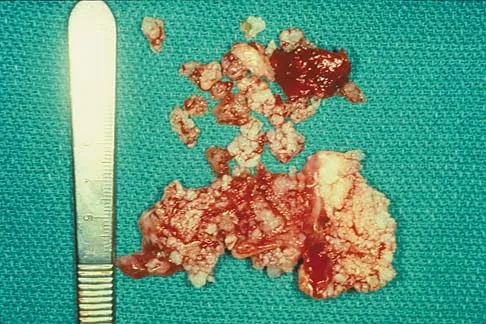
Explanation
The diagnosis is synovial chondromatosis. While the plain radiograph fails to show any calcifications, the MRI scan shows an intra-articular mass that involves the capsule. Grossly multiple granular cartilage nodules are seen. Management should consist of removing all loose bodies along with the synovial membrane.
Question 56
High Yield
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result?

Explanation
The radiographs show a fracture of the distal radius and ulna physis. The most likely complication is growth arrest of the distal ulna. In contradistinction to physis fractures of the radius (growth arrest incidence of less than 5%), the incidence of growth arrest in the ulna is between 30% and 40%. Entrapment of the EPL tendon and cross union between the two bones is extremely rare. Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120. Cannata G, De Maio F, Mancini F, et al: Physeal fractures of the distal radius and ulna: Long-term prognosis. J Orthop Trauma 2003;17:172-179. Ray TD, Tessler RH, Dell PC: Traumatic ulnar physeal arrest after distal forearm fractures in children. J Pediatr Orthop 1996;16:195-200.
Question 57
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?

Explanation
The radiograph reveals densities within the articular cartilage of the knee commonly referred to as chondrocalcinosis. The term chondrocalcinosis refers to the presence of calcium-containing crystals detected as radiodensities in cartilage. Calcium-containing crystals other than calcium pyrophosphate dihydrate may also deposit in articular cartilage and menisci, producing both radiographically detectable densities in cartilage and joint inflammation or degeneration. Hemochromatosis, alkaptonuria (ochronosis), and Wilson's disease are characterized by cellular deposition of iron, calcium, and copper ions, respectively, into various tissues including articular cartilage and can give this appearance. Septic arthritis does not usually cause chondrocalcinosis. Klippel JH (ed): Primer on the Rheumatic Diseases, ed 11. Atlanta, GA, Arthritis Foundation, 1997, pp 226-229 and 328-331.
Question 58
High Yield
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?
Explanation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity. Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower's shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49. Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 59
High Yield
What pharmacologic agents are preferred for the treatment of symptomatic active Paget's disease?

Explanation
Recent medical literature supports the use of bisphosphonates as the treatment of choice for active Paget's disease.
Question 60
A 47-year-old patient has had persistent pain and weakness after undergoing a reamed intramedullary nailing for a midshaft humerus fracture 8 months ago. There is no evidence of infection. Radiographs are shown in Figures 19a and 19b. Management should consist of


Explanation
Compression plating remains the treatment of choice for most established humeral nonunions. Autograft is felt to be superior to allograft. Electrical stimulation has not been found to improve healing rates in patients with nonunion after intramedullary nailing. Retrograde nailing with flexible nails gives inadequate rotational control to promote healing in this patient. Adding cancellous graft alone will not stabilize the nonunion site. Dynamic locking has been successful only in the lower extremity because the bone can be loaded axially. McKee MD, Miranda MA, Riemer BL, et al: Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-499.
Question 61
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?

Explanation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity. Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower's shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49. Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 62
Removal of both hallucal sesamoids should be reserved as a salvage procedure because of the high incidence of which of the following postoperative complications?

Explanation
Removal of both sesamoids is associated with a high incidence of postoperative hallux valgus and cock-up deformity of the great toe because of weakening of the flexor hallucis brevis tendon. The sesamoids lie within these tendons and require meticulous repair following excision. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 17-25.
Question 63
High Yield
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mm3 and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of
Detailed Explanation
The patient has diskitis. Administration of IV antibiotics speeds resolution and minimizes recurrence. Bed rest and cast immobilization have been successfully used to treat this disorder but can be associated with prolonged recovery and frequent recurrence, even when oral antibiotics are administered. A perivertebral abscess seen in association with this condition usually resolves without surgery. Ring D, Johnston CE II, Wenger DR: Pyogenic infectious spondylitis in children: The convergence of discitis and vertebral osteomyelitis. J Pediatr Orthop 1995;15:652-660.
Question 64
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
Hypophosphatemia is a rare genetic disease usually inherited as an X-linked dominant trait. The fact that the woman has no skeletal manifestations would indicate that the husband has the X-linked mutation. The disease is more severe in boys than it is in girls. The husband will not transmit the disease to his sons. However, all of their daughters will be affected either with the disease or as carriers. If the woman has the disease or the trait, there is a 50% chance that her sons will inherit the disease and a 50% chance that her daughters will be carriers or have a milder form of the disease. Parents should be advised to have genetic counseling so they can be informed when deciding whether to have children. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743. Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Question 65
High Yield
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with



Explanation
The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 66
High Yield
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?



Explanation
The patient has an acute fracture of the proximal pole. A 100% healing rate has been reported for open reduction and internal fixation of proximal pole fractures via a dorsal approach. This allows for direct viewing of the fracture line, facilitates reduction, and bone grafting can be done through the same incision if necessary. A vascularized or corticocancellous graft is reserved for nonunions. Proximal fractures are very slow to heal with a cast, if they heal at all. As a small fragment, percutaneous fixation is very difficult and has been reported for waist fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Question 67
High Yield
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?

Detailed Explanation
Burks and Schaffer described an approach to the tibial insertion of the posterior cruciate ligament that uses the interval between the semimembranosus and the medial gastrocnemius. The medial gastrocnemius muscle is retracted laterally and protects the neurovascular bundle. This approach is used to repair an avulsion of the posterior cruciate ligament tibial attachment or for performing a posterior cruciate ligament tibial inlay reconstruction. Berg EE: Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy 1995;8:95-99.
Question 68
High Yield
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the

Explanation
The patient has primary scapular-trapezius winging. This condition can be caused by blunt trauma to the relatively superficial spinal accessory nerve that is located in the floor of the posterior cervical triangle in the subcutaneous tissue. Other causes of injury include penetrating trauma, traction, or surgical injury. With trapezius winging, the shoulder appears depressed and laterally translated because of an unopposed serratus anterior. This contrasts with primary serratus anterior winging, which is caused by injury to the long thoracic nerve. In this condition, the scapula assumes a position of superior elevation and medial translation, and the inferior angle is rotated medially. The thoracodorsal nerve supplies the latissimus dorsi and is not involved in primary scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 69
High Yield
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most influenced by

Explanation
While many factors play a role in the outcome of osteochondritis dissecans, ample evidence has shown that the prognosis is most influenced by the growth status of the plates. If the growth plates are open, the chance of a successful outcome is significantly greater than if they are closed. Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Question 70
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of

Explanation
A supracondylar fracture of the femur that occurs after total knee replacement can be treated effectively by a number of methods. For this fracture, the use of a retrograde supracondylar nail has been found to be effective in several series. The treatment of these complex injuries needs to be individualized based on the stability of the implant, the quality of the bone, and the extent of comminution of the fracture. Revision with the use of an unstemmed implant will not result in effective stabilization of the knee or the fracture.
Question 71
Stiffness relates the amount of load applied to a structure like a long bone or an intramedullary nail to the amount of resulting deformation that occurs in the structure. What is the most important material property affecting the axial and bending stiffness of a structure?
Explanation
The amount of deformation resulting in response to an applied load depends on the stress distribution that the load creates in the structure and the stress versus strain behavior of the material that makes up the structure. Axial and bending loads create stress distributions that involve normal stresses and normal strains. Although all five responses are indeed material properties, only one, elastic modulus, relates normal stresses to normal strains. In fact, axial and bending stiffness are directly proportional to modulus, so that a nail made from stainless steel will have nearly twice the stiffness of a nail made from titanium alloy (because their respective elastic moduli differ by about a factor of two). Hayes WC, Bouxsein ML: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 74-82. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 159-165.
Question 72
High Yield
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
Explanation
The pisotriquetral joint is best seen on a lateral view in 30 degrees of supination. The carpal tunnel view provides visualization of the joint but to a lesser extent. The other views do not provide clear and accurate visualization. Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Question 73
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following?
Explanation
The most predictable positive outcome from spinal surgery due to a cauda equina syndrome is early surgical intervention before any significant neurologic deficit develops. Meta-analysis studies demonstrate that surgical intervention more than 48 hours after the onset of cauda equina syndrome show an increased risk for poor outcomes. Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Question 74
High Yield
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
Explanation
The MRI scans show a complete disruption of the sesamoid complex with proximal retraction of the medial sesamoid and high signal originating from the site normally occupied by the plantar plate (metatarsophalangeal ligament). This injury is the result of a hyperextension injury and is a severe variant of a turf toe. Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Question 75
A 50-year-old man with metastatic renal cell carcinoma has right hip pain. A radiograph and CT scan are shown in Figures 48a and 48b. The first step in management should consist of


Explanation
These lesions are extremely vascular and can cause uncontrolled intraoperative bleeding; therefore embolization is the appropriate first treatment. Because the radiograph and CT scan show a lytic lesion in the supra-acetabular region that affects the weight-bearing dome and medial wall, the next step in treatment would most likely be a total hip arthroplasty and acetabular reconstruction. Treatment with bisphosphonates and radiation therapy will not prevent an acetabular fracture. Cementoplasty is an emerging technique in which cement is injected percutaneously into a lesion, but no long-term results have been reported. Radiofrequency ablation of bone metastases is also an emerging technique that provides palliative pain control. Layalle I, Flandroy P, Trotteur G, Dondelinger RF: Arterial embolization of bone metastases: Is it worthwhile? J Belge Radiol 1998;81:223-225.
Question 76
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 77
What is the primary limiting membrane and mechanical support for the periphery of the physis?

Explanation
The perichondrial fibrous ring of La Croix acts as a limiting membrane that provides mechanical support for the bone-cartilage junction of the growth plate. It is continuous with the ossification groove of Ranvier, which contributes chondrocytes for the increase in width of the growth plate. The zone of provisional calcification lies at the bottom of the hypertrophic zone and is the site of initial calcification of the matrix. It is quite weak and usually is the cleavage plane for fractures; therefore, it does not qualify as mechanical support. The last intact transverse septum separates the zone of provisional calcification from the primary spongiosa and provides no real support to the physis. The primary spongiosa is the part of the metaphysis nearest the physis. Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
Question 78
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?

Explanation
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare. Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647. Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Question 79
High Yield
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of

Detailed Explanation
Displaced clavicular fractures lateral to the coracoid process (Neer type II and III) are best managed nonsurgically with sling immobilization and physical therapy, starting with pendulum exercises and progressing to active-assisted exercises when comfortable. Supervised therapy should be performed for 3 months or until full painless motion is achieved. In one study by Robinson and Cairns, this form of treatment provided patients with a 86% chance of avoiding a secondary reconstructive procedure. Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Question 80
What muscle is most often encountered during surgical approaches to C5-6?
Explanation
The omohyoid muscle crosses the surgical field from inferior lateral to anterior superior traveling from the scapula to the hyoid bone and may need to be transected. The posterior digastric crosses the field as well but higher near C3-4. The other muscles run longitudinally. Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-56.
Question 81
High Yield
The most favorable outcomes from release of the tarsal tunnel are in patients who have which of the following findings?
Explanation
Numerous causes of tarsal tunnel syndrome have been reported. The most favorable outcomes from release of the tarsal tunnel are in patients who have a space-occupying lesion (eg, ganglion, lipoma, or neurilemoma). While electrodiagnostic studies may be abnormal preoperatively, there is a low correlation between clinical outcome and electromyographic findings. Intrinsic weakness is a late finding in long-standing nerve dysfunction. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
Question 82
A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of


Explanation
The coracoid process is an essential component of the superior shoulder suspensory complex and must be maintained. Open reduction and internal fixation is recommended if the fragment is large and displaced more than 1 cm. Froimson AI: Fracture of the coracoid process of the scapula. J Bone Joint Surg Am 1978;60:710-711.
Question 83
High Yield
A 14-year-old patient with an L3 myelomeningocele underwent anterior and posterior spinal fusion for a curve of 50 degrees. Follow-up examination 1 week after the procedure now reveals persistent drainage from the posterior wound. Results of laboratory cultures show Streptococcus viridans, Staphylococcus aureus, and Enterococcus. In addition to IV antibiotics, surgical irrigation, and debridement, management should include
Explanation
The rate of wound infections has dramatically decreased with the routine use of prophylactic antibiotics. Factors known to increase the risk of infection include instrumentation, prolonged surgical time, excessive blood loss, poor perioperative nutritional status, a history of surgery, and a history of infection. The use of allograft does not result in an increased rate of infection. Adequate treatment requires early diagnosis and intervention. Temperature elevation and persistent wound drainage are highly suspicious for infection. An erythrocyte sedimentation rate and a WBC are not useful in diagnosis unless serial examinations show rising levels. Patients should be taken to the operating room where the entire wound can be reopened, irrigated, and debrided. Bone graft can be washed and replaced. Hardware should not be removed. The wound should be closed over suction drains. IV antibiotics should be given for a period of at least 10 days, followed by 6 weeks orally. Leaving the wound open to granulate with dressing changes results in prolonged hospitalization, inadequate treatment of the infection, and a poor cosmetic result. Lonstein JE: Complications of treatment, in Bradford DS, Lonstein JE, Moe JH, et al (eds): Moe's Textbook of Scoliosis and Other Spinal Deformities, ed 2. Philadelphia, Pa, WB Saunders, 1987, p 476.
Question 84
High Yield
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?

Detailed Explanation
There are four ways in which a plate acts: compression, tension bend, bridge or spanning, and buttress. Since there is no cortical contact with the large span of comminution, this plate is acting as a bridge plate. A bridge plate is defined as when the plate is used as an extramedullary splint attached to the two main fragments, leaving the comminution untouched.
Question 85
A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?


Explanation
Elbow dislocations in children are rare injuries and usually result from a fall on an outstretched arm. The incidence of these injuries increases as patients age and concurrently the incidence of supracondylar humerus fractures decreases. In adolescent patients, simple elbow dislocations are treated with splint immobilization and the initiation of physical therapy once comfortable. The practitioner must be aware of structures that may get caught in the joint on reduction. These include the median nerve as well as the medial epicondyle. In this patient, the radiographs reveal a medial epicondyle fracture. Postreduction radiographs show the joint to be incongruous secondary to intra-articular displacement. At this point, the most appropriate treatment is to perform an open reduction and repair of the medial epicondyle fragment. Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.
Question 86
Figure 36 shows the radiograph of a 14-year-old boy who has been treated in the past for Perthes' disease with an abduction brace. He now has hip pain that limits his activity, and nonsteroidal anti-inflammatory drugs have failed to provide relief. What is the most appropriate treatment?

Explanation
Several authors have reported good success in relieving pain with shelf acetabuloplasty. This patient's Perthes' disease is in the healed phase; therefore, proximal femoral varus and Salter innominate osteotomies aimed at improving containment are not indicated. The medial one half of the patient's femoral head is markedly deformed, and rotating it into a weight-bearing position with proximal femoral valgus osteotomy is unlikely to relieve pain. Hip arthrodesis can always be performed as a salvage procedure if the shelf acetabuloplasty fails. Daly K, Bruce C, Catterall A: Lateral shelf acetabuloplasty in Perthes' disease: A review of the end of growth. J Bone Joint Surg Br 1999;81:380-384.
Question 87
A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
Explanation
The patient has a stable fracture that can be initially treated with bed rest, followed by bracing and quick mobilization. The outcome is good and surgery is not required. These fractures can be treated nonsurgically if there is less than 50% compression, 15 degrees of angulation, and intact posterior structures. Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Question 88
High Yield
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T2-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T1-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient's symptoms?


Detailed Explanation
The MRI scans show Modic changes in the L4-L5 vertebral bodies due to spondylosis. There is no increased fluid signal or enhancement in the L4-L5 disk to suggest infection or any other pathologic process. Therefore, the patient's pain should be treated with a course of physical therapy and rehabilitation. There is no infection; therefore, IV antibiotics and debridement are not indicated. Similarly, a pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 319-329.
Question 89
High Yield
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?


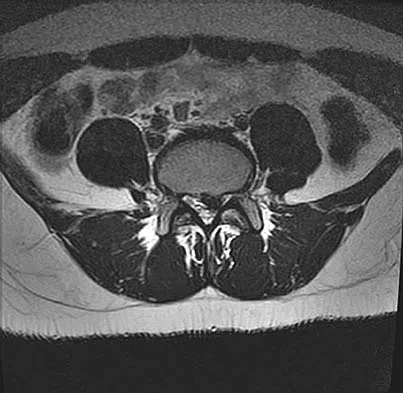
Explanation
The MRI scans clearly show an extruded L4-5 disk that is affecting the L5 nerve root on the left side. In addition, the L5 nerve root has a cutaneous distribution in the first dorsal web space. S1 affects the lateral foot. L4 affects the medial calf.
Question 90
High Yield
In Figure 2, which of the following structures is the primary stabilizer in preventing valgus instability of the elbow?
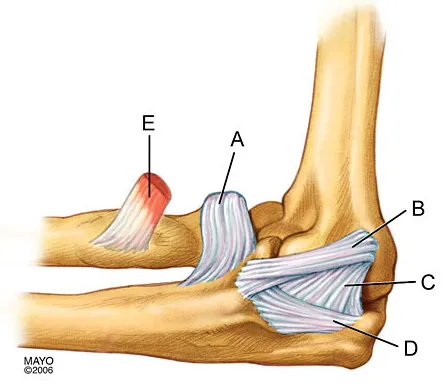
Explanation
The anterior bundle of the medial collateral ligament is the prime stabilizer of the medial aspect of the elbow and is indicated by "B" in the figure. When intact, this anterior bundle of the medial collateral ligament is a restraint to valgus instability of the elbow. The posterior bundle is regarded as a secondary stabilizer of the medial elbow (C). The transverse bundle (D), annular ligament (A), and biceps tendon (E) do not play a role in valgus stability of the elbow. Jobe F, Elattrache N: Diagnosis and treatment of ulnar collateral ligament injuries in athletes, in Morrey B (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1993, p 566.
Question 91
High Yield
An adult patient has an 8- x 4- x 10-cm soft-tissue mass located within the adductor compartment of the thigh. Staging studies should consist of

Detailed Explanation
The appropriate staging studies should consist of MRI and a radiograph of the primary lesion and CT of the chest. MRI is superior to CT for soft-tissue imaging. CT may be useful for evaluating the cortex of bone for invasion by tumor. Bone scans are not commonly used because soft-tissue sarcomas rarely metastasize to bone. CT of the abdomen and pelvis is not typically ordered except for possible liposarcoma. With liposarcoma, there may be a synchronous or metastatic retroperitoneal liposarcoma. Demetri GD, Pollock R, Baker L, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
Question 92
Figure 16 shows the radiograph of a 23-year-old man who has severe right shoulder pain after his motorcyle hit a bridge guardrail. He is neurologically intact. Nonsurgical management will most likely result in

Explanation
Internal fixation of the clavicle, glenoid, or both has been recommended for fractures of the clavicle and glenoid neck (floating shoulders). Recently, the inherent instability of these dual fractures has been questioned in a biomechanical model without further disruption of the coracoclavicular or acromioclavicular ligamentous structures. Nonsurgical management of the majority of combined scapular/glenoid fractures in patients with less than 10 mm of displacement has resulted in excellent shoulder function and will most likely achieve an excellent result in this patient. Egol KA, Connor PM, Karunakar MA, Sims SH, Bosse MJ, Kellam JF: The floating shoulder: Clinical and functional results. J Bone Joint Surg Am 2001;83:1188-1194. Williams GR Jr, Naranja J, Klimkiewicz J, et al: The floating shoulder: A biomechanical basis for classification and management. J Bone Joint Surg Am 2001;83:1182-1187.
Question 93
High Yield
A 21-year-old woman sustained a minimally displaced traumatic spondylolisthesis of C2 (Hangman's fracture) after striking the windshield with her forehead during a motor vehicle accident. Management should consist of
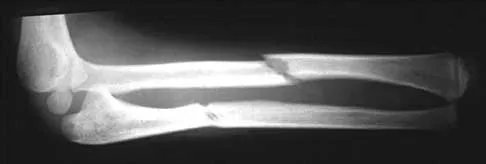
Explanation
According to the classification of Levine and Edwards, a type I Hangman's fracture is minimally displaced without angulation and represents a stable injury. Good clinical success has been achieved with nonsurgical management consisting of use of a rigid collar until the patient reports pain relief, followed by quick mobilization.
Question 94
High Yield
A 40-year-old unrestrained passenger reports chest wall pain after a motor vehicle accident. Which of the following structures is most important in preventing the injury shown in Figure 33?
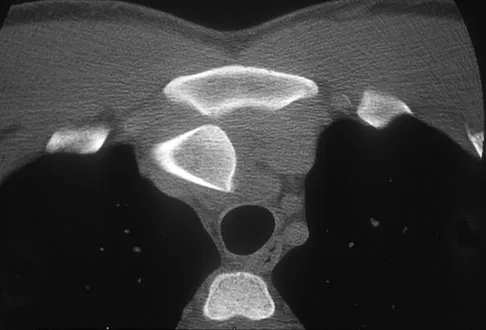
Explanation
Through cadaveric study, Spencer and associates measured anterior and posterior translation of the sternoclavicular joint. The study demonstrated that the posterior sternoclavicular joint capsule is the most important structure for preventing both anterior and posterior translation of the sternoclavicular joint. Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
Question 95
An 8-year-old boy with moderate factor VIII hemophilia played kickball earlier in the day and now reports progressively severe groin pain and is unable to walk. Examination reveals marked paresthesias over the medial aspect of the distal tibia. What is the most likely diagnosis?
Explanation
The iliacus muscle is a frequent site of hemorrhage in patients with severe or moderate hemophilia. In patients with moderate hemophilia, hemorrhage into the iliacus muscle often follows play or sporting events that include forceful contraction of the hip flexor muscles. An expanding iliacus hematoma compresses the adjacent femoral nerve, with one study reporting 60% complete femoral nerve palsy in hemophiliacs with an iliacus or iliopsoas hemorrhage. Femoral nerve compression typically includes paresthesias in the distribution of the terminal saphenous nerve branch. Hip joint hemarthrosis may occur, but this condition is not as frequent in hemophiliacs as muscle hemorrhage into the iliacus muscle. More importantly, a hip joint hemarthrosis is not associated with significant compression of the femoral nerve. Avulsion fractures of the anterior superior iliac spine typically occur during adolescence and are not associated with saphenous nerve paresthesias. Slipped capital femoral epiphysis does not have an increased association with hemophilia and usually occurs during the adolescent years. Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 379-426.
Question 96
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
SIS is a devastating but preventable complication of head injury. It occurs when return to activities is allowed prior to complete resolution of the symptoms of the first head injury. A second, sometimes trivial, head injury can lead to a devastating series of events that can result in sudden death. The symptoms tend to progress rapidly and often involve the brain stem. The prognosis is poor. Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44. Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Question 97
High Yield
A 54-year-old woman with idiopathic carpal tunnel syndrome undergoes open carpal tunnel release with a flexor tenosynovectomy. The pathology from the tenosynovium is likely to show
Detailed Explanation
The tenosynovium excised at the time of a carpal tunnel release for idiopathic carpal tunnel syndrome rarely shows signs of acute or chronic inflammation. Fibrosis, edema, and vascular sclerosis are the most common histologic findings. A tenosynovectomy with a carpal tunnel release usually is not necessary in the treatment of idiopathic carpal tunnel syndrome. Shum C, Parisien M, Strauch RJ, et al: The role of flexor tenosynovectomy in the operative treatment of carpal tunnel syndrome. J Bone Joint Surg Am 2002;84:221-225. Fuchs PC, Nathan PA, Myers LD: Synovial histology in carpal tunnel syndrome. J Hand Surg Am 1991;16:753-758.
Question 98
High Yield
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?



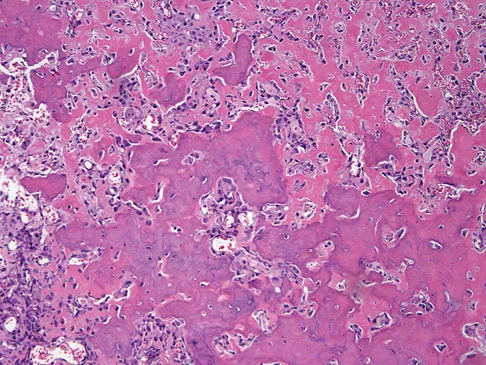
Explanation
The radiographs show a bone-producing lesion in the distal femoral metaphysis in this case of classic osteosarcoma presenting in the most common location, the distal femur. The coronal MRI scan reveals a marrow-occupying lesion with extension into the soft tissues. The histology shows osteoid production by pleomorphic cells consistent with an osteosarcoma. Ewing's sarcoma is a bone tumor characterized by uniform small blue cells on histology. Rhabdomyosarcoma is the most common childhood soft-tissue sarcoma. Osteomyelitis has an inflammatory appearance on histology. Malignant fibrous histiocytoma of bone has a lytic radiographic appearance and a pleomorphic storiform pattern without osteoid on histology. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
Question 99
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
Radiographic findings in patients with rheumatoid arthritis include symmetric joint space narrowing, periacetabular and femoral head erosions, and diffuse periarticular osteopenia. In advanced stages, protrusio acetabuli is a common finding. Ranawat and associates have shown a rate of superior femoral head migration of 4.5 mm per year and medial (axial) migration of 2.5 mm per year. Asymmetric joint space narrowing is a classic radiographic finding of degenerative arthrosis. Sacroiliac joint ankylosis commonly occurs in ankylosing spondylitis. Hip synovitis is a pathologic diagnosis, not a radiographic finding. Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Question 100
Figure 8 shows the radiograph of a 76-year-old man who has knee pain and swelling. History reveals that he underwent total knee arthroplasty 18 years ago. What is the most likely diagnosis?

Explanation
The radiograph reveals complete loss of joint space with particulate metal debris consistent with total polyethylene failure and metal-on-metal articulation. The components appear to be well fixed and minimal osteolysis is evident. Kilgus DJ, Moreland JR, Finerman GA, et al: Catastrophic wear of tibial polyethylene inserts. Clin Orthop Relat Res 1991;273:223-231.
