Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
A 28-year-old man has a painful nodule on the plantar aspect of his foot in the midarch. Use of a soft orthosis has failed to provide relief. Examination reveals that the mass is approximately 2 1/2 cm in diameter, firm, and tender to palpation. An MRI scan confirms the presence of a plantar fibroma. Management should now consist of

Explanation
Plantar fibromas have an extremely high recurrence rate (approximately 60%) with local excision only. Resection of the entire plantar fascia is effective at irradicating the lesion. There is no role for chemotherapy or amputation with plantar fibromatosis. Radiation therapy may be helpful in combination with resection of the plantar fascia. Kirby EJ, Shereff MJ, Lewis MM: Soft-tissue tumors and tumor-like lesions of the foot: An analysis of 83 cases. J Bone Joint Surg Am 1989;71:621-626.
Question 2
High Yield
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?



Detailed Explanation
The MRI scans clearly show an extruded L4-5 disk that is affecting the L5 nerve root on the left side. In addition, the L5 nerve root has a cutaneous distribution in the first dorsal web space. S1 affects the lateral foot. L4 affects the medial calf.
Question 3
The arrow in the axial T1-weighted MRI scan shown in Figure 18 is pointing to which of the following structures?

Explanation
The arrow is pointing to the ulnar nerve within Guyon's canal. Guyon's canal is approximately 4 cm long, beginning at the proximal extent of the transverse carpal ligament and ending at the aponeurotic arch of the hypothenar muscles. Many structures comprise the boundaries of Guyon's canal. The floor, for example, consists of the transverse carpal ligament, the pisohamate and pisometacarpal ligaments, and the opponens digiti minimi. Within Guyon's canal, the ulnar nerve bifurcates into the superficial and deep branches, with the deep branch of the ulnar nerve persisting distal to the canal. The ulnar artery is immediately adjacent and radial to the ulnar nerve. The median nerve is visualized within the carpal tunnel. The radial artery is on the radial side of the wrist. The hook of the hamate is clearly seen in the figure, orienting the observer to the ulnar side of the wrist. Goss MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop 1985;196:238-247.
Question 4
High Yield
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?


Detailed Explanation
The patient has no clinical or observed signs of sepsis. The skin just proximal to the gangrenous tissue appears somewhat hyperemic and is clearly viable. These wounds should be managed much like burn wounds. Moist dressings should be used until the tissue clearly demarcates. Much of the insult may simply be superficial and only require late debridement. McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective. Am J Orthop 1999;28:21-26.
Question 5
A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate (ESR) and leukocytosis. A plain radiograph and MRI scan are shown in Figures 1a and 1b. Biopsy specimens are shown in Figures 1c and 1d. What is the most likely diagnosis?




Explanation
Ewing's sarcoma typically can occur in the diaphysis of the long bones (50% to 55%). It is often accompanied by a large soft-tissue mass. Abnormal findings are common, including a low-grade fever, an elevated ESR, and leukocytosis. The histology is consistent with a small round blue cell tumor. The unique pathology and other findings exclude osteosarcoma. Giant cell tumor and chondrosarcoma have a different histologic appearance and typically are more metaphyseal in location. Chondrosarcoma typically is found in older age groups, has a different histologic pattern, and rarely occurs in the midshaft of the femur.
Question 6
High Yield
Osteonecrosis of the large joints may develop in patients with which of the following conditions?
Detailed Explanation
Osteonecrosis of major joints can occur in patients exposed to corticosteroids, alcohol, and antiseizure medications, as well as patients with hemaglobulinopathy, such as sickle cell anemia. In addition, patients with primary APS who had not taken corticosteroids were also found to be at high risk for osteonecrosis of the hip. In one study of 30 patients with primary APS, asymptomatic osteonecrosis was evident in 20%. A recent article has also found a high association between idiopathic osteonecrosis of the hip and collagen II mutation. None of the other conditions has been shown to be associated with a higher risk of osteonecrosis. Tektonidou MG, Malagari K, Vlachoyiannopoulos PG, et al: Asymptomatic avascular necrosis in patients with primary antiphospholipid syndrome in the absence of corticosteroid use: A prospective study by magnetic resonance imaging. Arthritis Rheum 2003;48:732-736.
Question 7
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?




Explanation
A Charcot flare in adjacent joints is not uncommon in patients with neuropathy who undergo surgery or other trauma. Venous thrombosis would present with swelling of the entire leg, while infection would present earlier in the postoperative period. The radiographs are pathognomonic of Charcot arthropathy, not an unrecognized fracture or gout. A compartment syndrome this late after injury is extremely rare, and there would be no bony distraction associated with compartment syndrome.
Question 8
High Yield
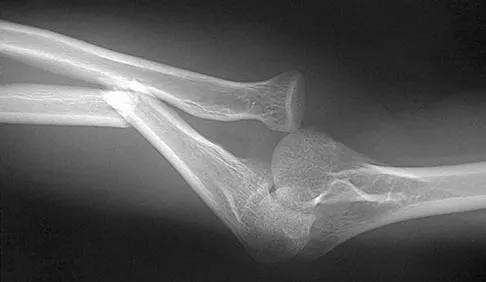
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in

Explanation
The elbow dislocates by a three-dimensional movement of supination and valgus during flexion. Additional trauma during reduction is minimized by recreating the deformity and reducing the elbow in supination. The actual maneuver includes full supination (actually hypersupination) of the elbow in a valgus position. This is followed by pushing the olecranon distally in line with the long axis of the ulna while swinging the elbow into varus, and then relaxing the supination torque. Postreduction stability is enhanced in pronation, except when the soft-tissue disruption is extensive. O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 414.
Question 9
High Yield
Radiographs of an 80-year-old woman with back pain reveal a compression fracture. Which of the following imaging studies best evaluates the acuity of the fracture?
Explanation
The best method of evaluating the acuity of osteoporotic compression fractures is to look for edema in the vertebral body. This is best accomplished with a STIR-weighted MRI scan. Bone scans can show increased uptake at the site of fracture for many months after the fracture. T1-weighted MRI scans show loss of normal marrow fat that may not necessarily correspond with acuity of the fracture. CT scans and radiographs show fracture deformity but cannot be used to judge acuity. Phillips FM: Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 2003;28:S45-S53.
Question 10
High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 11
High Yield
Chemotherapy is routinely included in the treatment of which of the following soft-tissue sarcomas?

Detailed Explanation
Most soft-tissue sarcomas are treated with a combination of radiation therapy and wide resection. Rhabdomyosarcomas are an exception, where chemotherapy is included in all treatment plans. Chemotherapy for other soft-tissue sarcomas is controversial. Enzinger FM, Weiss SW: Rhabdomyosarcoma, in Soft Tissue Tumors, ed 3. St Louis, MO, CV Mosby, 1995, p 539.
Question 12
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?

Explanation
Based on the MR arthrogram in which gadolinium (bright on T1-weighted images) was injected into the joint space prior to imaging, the study shows a tear of the anterior band of the ulnar collateral ligament (UCL). The disruption in the distal end of the UCL is outlined by contrast. A small collection of contrast extravasation into the flexor musculature further confirms the presence of a tear. The UCL has a broad-based attachment on the medial epicondyle and has a pointed or tapered attachment distally on the ulna. Most UCL tears occur distally at the ulnar (coronoid) attachment. MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps. Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Question 13
High Yield
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?


Explanation
The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation. Robinson CM, Aderinto J: Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Question 14
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
Most patients lose elbow range of motion after open reduction and internal fixation of a distal humeral fracture. Ulnar nerve dysfunction, nonunion, and infection all occur less commonly. Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
Question 15
High Yield
A 25-year-old woman has significant pain and swelling in her left ankle after falling off her bicycle. Examination reveals that she is neurovascularly intact. Radiographs are shown in Figures 33a through 33c. What is the next most appropriate step in management?



Explanation
The radiographs show a displaced ankle fracture with widening of the syndesmosis. Open reduction and internal fixation is indicated with fixation of the mortise with syndesmotic screws. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Question 16
High Yield
When performing ankle arthroscopy through the anterolateral portal, what anatomic structure is at greatest risk?
Explanation
The superficial branch of the peroneal nerve travels subcutaneously anterior to the lateral malleolus at the ankle. It can be easily damaged by deep penetration of the knife blade when making this portal or when passing shavers in and out of the portal. Anesthesia or dysesthesia from laceration or neuroma formation can cause significant postoperative morbidity. The anterior tibialis tendon, anterior tibial artery, and the deep peroneal nerve are located much more anterior and central on the ankle. The sural nerve is posterior lateral to the ankle and is not at risk from this portal. Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Question 17
High Yield
For the athlete performing heavy exercise, the magnitude of core temperature and heart rate increase is most proportional to

Explanation
Studies examining the impact of graded water debt have clearly shown that the magnitude of core temperature and heart rate increase accompanying work are proportional to the magnitude of water debt at the onset of exercise. Though added thermal burden from hot climates is a factor, it appears to be less significant. Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524. Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Question 18
High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 19
What is the most important stabilizing mechanism in the midrange of motion of the glenohumeral joint?
Explanation
Concavity compression is a stabilizing mechanism by which muscular compression of the humeral head into the glenoid fossa stabilizes the glenohumeral joint against shear forces. This is dependent on the depth of the concavity and the magnitude of the compressive force. Lee SB, Kim KJ, O'Driscoll SW, et al: Dynamic glenohumeral stability provided by the rotator cuff muscles in the mid-range and end-range of motion: A study in cadavera. J Bone Joint Surg Am 2000;82:849-857.
Question 20
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?

Explanation
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare. Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647. Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Question 21
High Yield
What procedure can eliminate a sulcus sign?
Explanation
A sulcus sign represents inferior subluxation of the shoulder. The elimination of this sign and correction of the inferior subluxation is best achieved through either an open or arthroscopic rotator interval closure. A SLAP repair stabilizes the biceps anchor but does not affect the sulcus sign. A Bankart repair, which corrects anterior-inferior laxity, is not sufficient to eliminate a sulcus sign. Subacromial decompression and supraspinatus repairs have no effect on inferior subluxation. Field LD, Warren RF, O'Brien SJ, et al: Isolated closure of rotator interval defects for shoulder instability. Am J Sports Med 1995;23:557-563.
Question 22
High Yield
In the treatment of acetabular dysplasia, what type of pelvic osteotomy leaves the "teardrop" in its original position and redirects the acetabulum?

Explanation
The dial or spherical osteotomy leaves the medial wall or teardrop in its original position and, as a result, is intra-articular. The other pelvic osteotomies (except Chiari) redirect the acetabulum, including the medial wall. The Chiari osteotomy improves coverage without redirecting the acetabulum within the pelvis, and it leaves the teardrop in the same place. Lack W, Windhager R, Kutschera HP, Engel A: Chiari pelvic osteotomy for osteoarthritis secondary to hip dysplasia: Indications and long-term results. J Bone Joint Surg Br 1991;73:229-234. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 23
High Yield
A 46-year-old woman who was involved in a motor vehicle accident reports a 4-month history of right-sided lower back pain and pain radiating into the right thigh. The patient underwent an extensive 3-month course of physical therapy and now is dependent on narcotic medication for pain control. Epidural injection therapy has failed to improve her symptoms. Examination is significant for weakness of hip flexion in the seated position and for decreased sensation to light touch in the medial anterior thigh region. Straight leg raise is negative, but the femoral stretch test reproduces anterior thigh pain. A CT myelogram image, at L3-L4, is shown in Figure 3. What is the most appropriate management at this time?
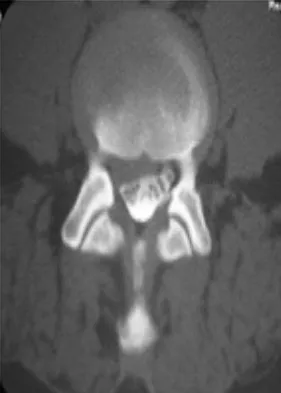
Explanation
The CT scan reveals a right-sided lateral disk protrusion at L3-4 that has been symptomatic for more than 4 months despite appropriate nonsurgical management. Relative surgical indications include persistent radiculopathy despite an adequate trial of nonsurgical management, recurrent episodes of sciatica, persistent motor deficit with tension signs and pain, and pseudoclaudication caused by underlying stenosis. Whereas studies have shown improvement in patients with sciatica from a lumbar disk herniation treated either nonsurgically or surgically, those undergoing surgical treatment had an overall greater improvement of symptoms. Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
Question 24
High Yield
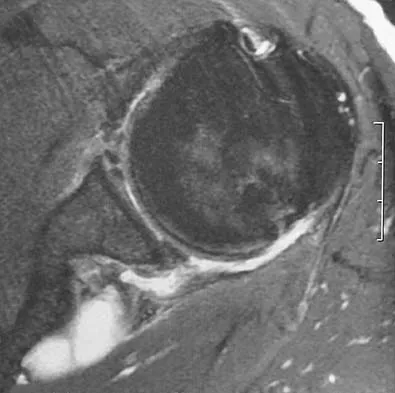
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T1-weighted, sagittal T2-weighted, axial T1-weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?
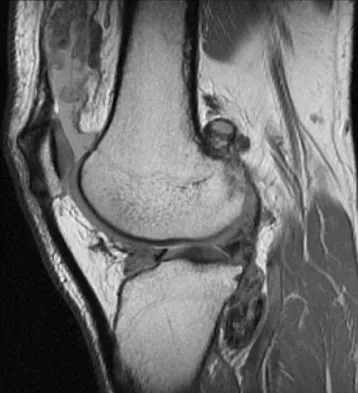
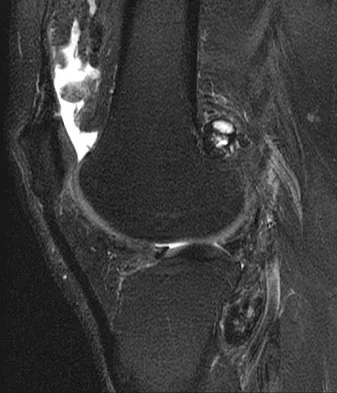
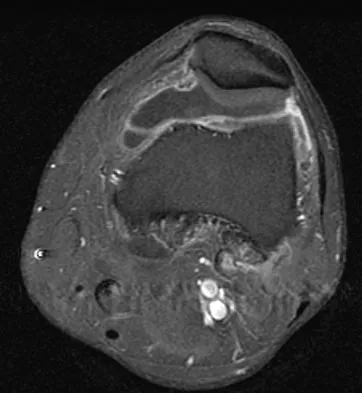

Explanation
The MRI scans show multiple low-signal intensity lesions scattered throughout the knee, extending posteriorly inferior to the tibial plateau. The low-signal intensity on both the T1- and T2-weighted images, the modest vascularity noted on the gadolinium image, and the "blooming" noted on the gradient echo image (ferrous-laden tissue) are all strongly suggestive of diffuse PVNS. Whereas synovial chondromatosis can present as diffuse masses in the knee, they present as nodule masses that have low T1- and high T2-weighted signal characteristics. Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4241-4252.
Question 25
Oxidation of polyethylene after sterilization occurs most rapidly when the implant undergoes
Explanation
The use of gamma radiation to sterilize polyethylene will result in the formation of free radicals in the material that increase the susceptibility of the material to oxidation and wear. The packaging can also have an impact. If the polyethylene is packaged in air, the oxygen in the packaging can significantly oxidize the material on the shelf prior to clinical use. Gas plasma and ethylene oxide sterilization do not appear to increase oxidation of polyethylene. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Wright TM: Ultra-high molecular weight polyethylene, in Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 37-46.
Question 26
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Explanation
The patient has a posterolateral rotatory instability (PLRI) of the elbow that is most likely the result of iatrogenic injury to the lateral ulnar collateral ligament, the main ligament implicated in PLRI. The anterior band of the medial collateral ligament is implicated in valgus instability. Injury to the radial nerve is unlikely, and the lateral radial collateral ligament makes less of a contribution to elbow stability than does the ulnar component. While the origin of the extensor carpi radialis brevis may contribute to elbow stability, it is not as important a stabilizer as the lateral ulnohumeral ligament. O'Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
Question 27
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?

Explanation
Multidirectional instability is a common finding in young female athletes. The anatomic structures are all intact but are hypermobile; therefore, CT and bone scans and scapular Y-views are often normal. Obtaining a weighted or AP stress view while applying downward traction on the arm will document instability and hypermobility of the joint. MRI generally is not indicated in this condition. Ultrasound is used primarily for rotator cuff pathology. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Question 28
Following ankle arthroscopy performed through a posterolateral portal, a patient notes numbness on the lateral half of the heel pad of the foot. What is the most likely injured structure?
Explanation
The lateral calcaneal nerve is a branch of the sural nerve that runs along the lateral border of the Achilles tendon to innervate the lateral heel pad. Ankle arthroscopy involves posterior portals that hug the Achilles tendon to avoid the main trunks of the sural nerve and tibial nerve; however, the lateral calcaneal branch remains potentially vulnerable. The first branch of the lateral plantar nerve is actually a medial structure that partially innervates the plantar fascia and the abductor digiti quinti. The deep peroneal nerve is anterior to the ankle. Sitler DF, Amendola A, Bailey CS, et al: Posterior ankle arthroscopy: An anatomic study. J Bone Joint Surg Am 2002;84:763-769.
Question 29
Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?
Explanation
Advocates of resurfacing hip arthroplasty cite preservation of the proximal femoral bone stock as the main advantage of this procedure over total hip arthroplasty. Fracture of the retained femoral neck has been reported following resurfacing arthroplasty. The exact etiology of the latter is unknown. Technical errors, such as notching of the femoral neck or possibly disruption of the blood supply to the femoral head during extensive soft-tissue exposure, may result in femoral neck fracture. Gabriel JL, Trousdale RT: Stem fracture after hemiresurfacing for femoral head osteonecrosis. J Arthroplasty 2003;18:96-99.
Question 30
A patient who sustained a knife wound to the axilla 4 months ago now has profound interosseous wasting and generalized hand weakness. A brachial plexus injury is likely at which of the following locations in Figure 29?

Explanation
Penetrating sharp wounds in proximity to major nerve or vascular structures should always be acutely explored. Because this patient did not seek treatment for a potentially treatable injury, interosseous wasting implies injury to the C8 and T1 nerve roots that contribute to ulnar nerve function. The most likely location for the brachial plexus injury is the location marked L or the inferior trunk. A wrist drop that is the result of radial nerve dysfunction would be expected with an injury at K or O. An upper brachial plexus palsy with loss of elbow flexion and shoulder abduction would be expected with an injury at B. A loss of elbow flexion alone would be expected following an injury at C. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29. Wolock B, Millesi H: Brachial plexus-applied anatomy and operative exposure, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1255-1272.
Question 31
High Yield
Figure 17 shows the radiograph of an 80-year-old woman who has left groin pain. She underwent a total hip arthroplasty 15 years ago and has no history of hip dislocation; however, she now reports that the pain results in functional impairment. Preoperative findings reveal that the component used has been discontinued, the locking mechanism is poor, and there is no replacement polyethylene available from the company. During surgery, the acetabular component is found to be well fixed, it is in satisfactory position, and adequate access can be obtained through the screw holes in the component to debride the osteolytic cavities. What is the best course of action for revision?

Detailed Explanation
The clinical result in this patient has been good, with no dislocations, suggesting that the components are in reasonably good position. The radiograph and examination at the time of surgery suggest that the acetabular component is well fixed. The surrounding bone of the acetabulum is osteopenic and there would most likely be considerable bone loss if the acetabular component is removed. Access to the osteolytic lesions is possible. Cementing an acetabular component into the retained socket will cause the least amount of bone loss, shorten the procedure, and most likely result in a functional hip. Maloney WJ: Socket retention: Staying in place. Orthopedics 2000;23:965-966.
Question 32
An 18-year-old man underwent open reduction and internal fixation of a tibial spine avulsion and a posterolateral corner repair. Two years later, he underwent lateral collateral ligament (LCL) and posterolateral corner reconstruction because of instability. Examination reveals a pronounced lateral varus knee thrust when ambulating. Varus stress in 30 degrees of flexion produces a 10-mm opening that is eliminated in extension. The Lachman's test is 2 mm with a firm end point, and the posterior drawer test is negative. Standing radiographs show widening of the lateral joint space and a 5-degree mechanical varus alignment. What is the most effective course of treatment?
Explanation
The patient has chronic posterolateral instability with a varus knee alignment; therefore, the most effective treatment is a valgus-producing HTO. A repeat soft-tissue reconstruction without correction of the varus alignment will most likely fail. An ACL reconstruction is not indicated with a normal Lachman's test. Physical therapy and bracing will have little effect. Naudie DD, Amendola A, Fowler PJ: Opening wedge high tibial osteotomy for symptomatic hyperextension-varus thrust. Am J Sports Med 2004;32:60-70.
Question 33
High Yield
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of

Detailed Explanation
The widening of the physis associated with incomplete reduction of this fracture suggests that periosteum is interposed at the fracture site. Clinical and animal study findings suggest that the interposed periosteum may lead to premature physeal closure. Repeated forceful attempts at reduction may subject the physis to further injury and should be avoided. Growth problems are common in children with Salter-Harris type I fractures of the lower extremities. Nonunions are rare in children with Salter-Harris type I fractures. Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibial physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 34
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of

Explanation
Periosteal new bone formation is a warning sign of prosthetic infection. Indomethacin may prevent heterotopic ossification if given early enough; however, it is irrelevant in this patient. A C-reactive protein and a sed rate are useful screening studies that add to the predictive value of the radiographs and may be performed routinely if sepsis is suspected. A bone scan obtained 4 months after surgery would show increased uptake in all cases. If results of a sed rate and C-reactive protein are normal, then a biopsy should be considered to rule out a neoplasm.
Question 35
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?


Explanation
The MRI scans show a complete disruption of the sesamoid complex with proximal retraction of the medial sesamoid and high signal originating from the site normally occupied by the plantar plate (metatarsophalangeal ligament). This injury is the result of a hyperextension injury and is a severe variant of a turf toe. Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Question 36
High Yield
Figure 48 shows an MRI scan of the knee. The arrow is pointing to what structure?

Explanation
The arrow points to the biceps femoris, which is inserted onto the fibula. The biceps femoris lies at the posterolateral aspect of the thigh. The semimembranosus and the semitendinous lie at the posterior medial aspect of the thigh. Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea and Febiger, 1918, 2000.
Question 37
Which of the following structures is most vulnerable during a medial sesamoidectomy of the hallux?
Explanation
The plantar-medial cutaneous nerve is at risk with the surgical approach to the medial sesamoid. It is found directly underlying an incision made at the junction of the glabrous skin of the hallux and must be identified before the approach can proceed. Transection will result in a painful neuroma that impinges on the plantar-medial surface of the toe and cause problems with shoe wear. The only other structure that lies near the surgical field is the abductor hallucis tendon which lies dorsal to the incision.
Question 38
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?


Explanation
Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a "dripping candle wax" appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the "smoke up chimney" appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 39
A 67-year-old retired steelworker was involved in a motor vehicle accident and sustained a midcervical spinal cord injury. Radiographs and MRI scans reveal severe cervical stenosis and spondylosis without fractures or dislocations. Neurologic examination reveals an ASIA C spinal cord impairment with greater motor involvement of the upper extremities than the lower extremities. What is the probability that the patient eventually will become ambulatory?
Explanation
The patient sustained an incomplete spinal cord injury known as central cord syndrome. Central cord syndrome characteristically has disproportionate involvement of the upper extremities with the lower extremities being relatively spared. It is most commonly seen after cervical injuries in elderly patients with spondylosis and spinal stenosis, often without fracture. Penrod and associates noted that 23 of 59 patients with central cord syndrome (ASIA C and D) ultimately walked. The poorest prognosis, however, was in ASIA C patients older than age 50, in which only 40% walked. Penrod LE, Hegde SK, Ditunno JF Jr: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Question 40
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Explanation
When attempting a revision anterior cervical approach from the side opposite the original approach, it is important to evaluate the function of the vocal cords. If this evaluation reveals dysfunction of the vocal cord on the side of the original approach, then an approach on the contralateral side should not be attempted. Injury to the stellate ganglion, which causes a Horner's syndrome, should not preclude an approach on the contralateral side. While the side of the symptomatology can influence the surgeon's choice as to the side of an anterior approach, it does not preclude a certain approach. When approaching the lower cervical spine from the right side, the recurrent laryngeal nerve can cross the surgical field and should be preserved. Excessive intraoperative pressure on the esophagus can increase the incidence of dysphagia, but its incidence is no different with either approach. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.
Question 41
High Yield
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?


Explanation
The radiographs reveal nonunion of a talar neck fracture. There is no radiographic evidence of osteonecrosis or significant degenerative arthritis. The results of talectomy are suboptimal. Arthrodesis would be indicated for degenerative arthritis. Revision ORIF is feasible and preserves motion. A vascularized graft should be considered whenever osteonecrosis is present, but the talar body appears viable in this case. Calvert E, Younger A, Penner M: Post talus neck fracture reconstruction. Foot Ankle Clin 2007;12:137-151.
Question 42
High Yield
A 42-year-old man with a history of renal cell carcinoma has progressive weakness in the lower extremities for the past 3 weeks. The patient desires intervention. A sagittal T2-weighted MRI scan is shown in Figure 9a, and a sagittal contrast enhanced T1-weighted MRI scan is shown in Figure 9b. He currently ambulates minimal distances with a walker. His life expectancy is 8 months. Treatment of the spine lesion should consist of


Detailed Explanation
The MRI scans show a metastatic lesion in two contiguous vertebral bodies in the lower thoracic spine. Posterior laminectomy is not indicated because this does not adequately decompress the neural elements and will lead to progressive kyphosis. A posterior fusion may prevent progressive kyphosis but will not decompress the spinal cord. Renal cell carcinoma is not radiosensitive; therefore, radiation therapy would not be helpful in relieving neurologic compression. The lesion should be treated by an anterior corpectomy and reconstruction. This will allow for complete decompression as well as reconstruction of the anterior column. Kyphoplasty is not indicated in a lesion with disruption of the posterior cortex and neurologic impairment. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
Question 43
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
Lateral scapular winging is characteristic of trapezius palsy, whereas medial scapular winging is characteristic of long thoracic nerve palsy. During sports activity, injury to the spinal accessory nerve is rare but may occur with blunt or stretching trauma. Patients often report an asymmetric neckline, drooping shoulder, winging of the scapula, and weakness of forward elevation. Evaluation should include a complete electrodiagnostic examination. Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16. Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27. Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546. Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Question 44
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of


Explanation
The complications of femoral neck fractures in children include osteonecrosis, malunion, nonunion, and premature physeal closure. It is presumed that the risk of osteonecrosis is directly related to the amount of displacement at the time of injury and is not affected by the type of treatment. The risk of the other complications can be decreased depending on the type of treatment. Anatomic reduction by either closed or open methods can reduce the risk of malunion. The addition of internal fixation allows for maintenance of the reduction. In young children who cannot comply with a partial or non-weight-bearing status, the addition of a spica cast gives added protection. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Question 45
What is the most common complication following surgical fixation of a distal humeral fracture?

Explanation
In most series, elbow stiffness is the most common complication and can be overcome by achieving stable fixation and initiating early motion after surgery. All of the other complications are seen but to a lesser degree than elbow stiffness. Sanders RA, Raney EM, Pipkin S: Operative treatment of bicondylar intra-articular fractures of the distal humerus. Orthopedics 1992;15:159-163.
Question 46
High Yield
A 10-year-old girl has a right elbow deformity that is the result of trauma 5 years ago. She has no pain despite the arm deformity. The radiographs in Figures 42a and 42b show complete healing. This radiographic appearance demonstrates what complication?


Detailed Explanation
Cubitus varus is a common complication of displaced supracondylar humeral fractures that are treated with closed reduction and cast immobilization. Treatment with closed reduction and percutaneous pinning decreases the incidence of this complication. Cubitus varus also can occur in minimally displaced fractures when unrecognized collapse of the medial column of the distal humerus is not corrected with manipulation. This can be detected on physical examination of the carrying angle or on radiographs measuring Baumann's angle, both in comparison to the opposite side. Cubitus varus may result in unacceptable cosmesis and may predispose the patient to fractures of the lateral condyle. The lateral radiograph demonstrates the crescent sign from overlap of the distal humerus with the olecranon seen in patients with cubitus varus. Patients with growth arrest to the medial trochlear physis would have atrophy of the trochlea on radiographs. Flynn JM, Sarwark JF, Waters PM, et al: The surgical management of pediatric fractures of the upper extremity. Instr Course Lect 2003;52:635-45. Papandrea R, Waters PM: Posttraumatic reconstruction of the elbow in the pediatric patient. Clin Orthop 2000;370:115-126.
Question 47
High Yield
A 53-year-old patient is seen in the emergency department after sustaining a fall onto her left hip. A current radiograph is shown in Figure 40. What is the best treatment option?

Explanation
The patient has sustained a Vancouver B2 periprosthetic femoral fracture (a femoral fracture that occurs around or just distal to a loose stem, with adequate proximal bone stock). The stem is no longer fixed to proximal bone; therefore, retention of the femoral component is not recommended. Nonsurgical management is contraindicated because of the high risk of nonunion and malunion with significant component settling in the distal fragment and leg shortening. Revision femoral arthoplasty must attain distal fixation in adequate host bone, which is usually successful with a porous-coated cylindrical stem. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 48
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
SIS is a devastating but preventable complication of head injury. It occurs when return to activities is allowed prior to complete resolution of the symptoms of the first head injury. A second, sometimes trivial, head injury can lead to a devastating series of events that can result in sudden death. The symptoms tend to progress rapidly and often involve the brain stem. The prognosis is poor. Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44. Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Question 49
High Yield
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management?



Detailed Explanation
The history, examination, and MRI scan findings are consistent with a midsubstance partial rupture of the rectus femoris muscle. This is an injury masquerading as a "pseudo tumor." The lack of an appreciable mass effect on the T1-weighted MRI scan, the defined fluid signal on the T2-weighted scans, and the lack of significant contrast enhancement after gadolinium are all most consistent with injury rather than a neoplasm. Most of these injuries respond to nonsurgical management; a few will benefit from late debridement and repair if symptoms fail to resolve in 3 to 6 months. The treatment of choice is nonsurgical management with a follow-up MRI scan to verify that the findings are resolving. Hughes C IV, Hasselman CT, Best TM, et al: Incomplete, intrasubstance strain injuries of the rectus femoris muscle. Am J Sports Med 1995;23:500-506.
Question 50
An 11-year-old boy has right shoulder pain and has been unwilling to use the arm after throwing a baseball in a Little League game 3 weeks ago. Examination reveals upper arm and shoulder tenderness with swelling. A radiograph and MRI scan are shown in Figures 27a and 27b. Management should consist of


Explanation
The radiograph is consistent with a unicameral (simple) bone cyst. The MRI scan reveals that the cyst is juxtaposed to the physis and therefore can be classified as active (latent cysts are more than 1 cm away from the physis). Active cysts are treated with aspiration and steroid injection, although repeated injections may be necessary. Curettage and bone grafting results in more reliable healing but may lead to growth arrest in active cysts. Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 945-946.
Question 51
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of




Explanation
The biopsy specimens show a chondromyxoid fibroma with varying amounts of cartilage, benign fibrous tissue, giant cells, and loose myxoid areas. Chondromyxoid fibroma is a benign active bone lesion that is best treated with aggressive curettage and bone grafting. Although recurrences are common, more aggressive treatment is not warranted initially. Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Question 52
Figures 48a and 48b show the elbow radiographs of a 5-year-old boy who fell from a tree after dinner. Examination reveals that he is unable to extend his wrist. Management should consist of immediate


Explanation
In the absence of vascular compromise, there has been no proven value to proceeding immediately to surgery, especially when the patient has a full stomach and runs a significant risk of perioperative aspiration. It would be more prudent to wait until the next morning with a surgical plan of closed reduction and pinning. Open reduction should be reserved for the unusual case of where closed treatment has not been successful. The implication that there may be a radial nerve injury associated with this fracture does not alter the treatment plan, and with a high level of certainty would be expected to resolve. Attempting closed reduction in the emergency department creates the opportunity for uncertain results and is not tolerated well by most patients. Skeletal traction, with its associated lengthy hospitalization and the technical difficulties associated with both the traction and radiographic evaluations, has fallen into disfavor for typical clinical situations. Iyengar SR, Hoffinger SA, Townsend DR: Early versus delayed reduction and pinning of type III displaced supracondylar fractures of the humerus in children: A comparative study. J Orthop Trauma 1999;13:51-55.
Question 53
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?

Explanation
The Thompson posterior approach is used in treatment of fractures of the proximal radius. Dissection is carried out through the interval between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve). To identify this interval, the forearm is pronated and the mobile lateral wad of muscles (the ulnar-most belly is the extensor carpi radialis brevis) is grasped with the thumb and finger and pulled from the much less mobile mass of the extensor digitorum communis. The furrow created is marked with a skin marker for subsequent skin incision. The skin incision follows a line from the lateral epicondyle of the humerus to a point corresponding to the middle of the posterior aspect of the wrist. Distally, the intermuscular plane is between the extensor carpi radialis brevis and the extensor pollicis longus. Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129. Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Question 54
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist's office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?

Explanation
The privacy rules do not require an individual's written authorization for certain permitted or required uses and disclosures of the medical records. Patient or parental authorization is not required for disclosures for certain purposes related to treatment, payment, or health care operations. Specifically, HIPAA does not require a covered entity to obtain patient authorization for many of the health care industry's most fundamental activities such as providing care. Carroll R: Risk Management Handbook for Health Care Organizations, ed 4. Hoboken, NJ, Jossey-Bass, 2003, p 1142.
Question 55
High Yield
A 17-year-old boy has had a mass in his right thigh for the past 6 months. He denies any history of trauma. Examination reveals that the mass is painless and firm. A radiograph and axial MRI scan are shown in Figures 49a and 49b. What is the most likely diagnosis?


Detailed Explanation
Osteochondroma typically occurs as a bony projection or a sessile growth on the bone, and there can be flaring of the metaphysis. The radiograph shows continuity from the adjacent cancellous bone into the lesion itself. There is no soft-tissue mass or bone destruction to suggest osteosarcoma or Ewing's sarcoma. Periosteal chondroma has a scalloped out radiographic appearance. Chondroblastoma typically is an epiphyseal-based lesion.
Question 56
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?


Explanation
The MRI scans reveal a large postoperative hematoma causing significant thecal compression. An epidural hematoma with neurologic deficit is a surgical emergency requiring immediate evacuation of the hematoma. Although the incidence of postoperative epidural hematomas is rare, the consequences of a missed diagnosis can be catastrophic. Early recognition and evacuation are essential in preserving or restoring neurologic function. Uribe and associates attributed delayed postoperative hematomas to previous multiple lumbar surgeries as a possible contributing factor. Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.
Question 57
High Yield
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?
Explanation
Internal impingement of the shoulder is a leading cause of shoulder pain in the throwing athlete. The primary lesion in pathologic internal impingement is excessive tightening of the posterior band of the inferior glenohumeral ligament complex. To obtain an accurate assessment of true glenohumeral rotation, the scapula is stabilized during examination. A loss of 20 degrees or more of internal rotation, as measured with the shoulder positioned in 90 degrees of abduction, indicates excessive tightness of the posterior band of the inferior glenohumeral ligament complex. Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Question 58
High Yield
A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed to provide relief. Examination reveals tenderness in the lateral aspect of the proximal forearm and exacerbation of symptoms with resisted finger extension. Radiographs of the elbow reveal no abnormalities. Which of the following studies will aid in diagnosis?
Explanation
It is often difficult to accurately discern between lateral epicondylitis and radial tunnel syndrome. Neither MRI nor a bone scan is likely to reveal abnormalities. Electrodiagnostic studies are often inconclusive, and radial tunnel syndrome often presents without motor weakness. The symptoms of radial tunnel syndrome are expected to improve with an injection of lidocaine into the radial tunnel; therefore, this is the test of choice in this clinical scenario. Radiographs of the wrist will not assist in making the diagnosis. Eversmann WW Jr: Entrapment and compression neuropathies, in Green DP (ed): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingston, 1993, pp 1341-1385.
Question 59
According to the Third National Acute Spinal Cord Injury Study (NASCIS 3), what is the recommended protocol for a patient who sustained a spinal cord injury 7 hours ago?
Explanation
NASCIS 2 established the recommended doses of methylprednisolone for spinal cord injury. This included an initial bolus of 30 mg/kg over 1 hour, followed by an infusion of 5.4 mg/kg/h for an additional 23 hours. If the injury was more than 8 hours old, the methylprednisolone was not recommended. NASCIS 3 changed the dosing schedule based on the time from injury. If the time from injury to treatment was less than 3 hours, the standard protocol was followed (30 mg/kg bolus followed by 5.4 mg/kg/h for 23 hours). If the time from injury to treatment was between 3 and 8 hours, the infusion was continued at 5.4 mg/kg for an additional 23 hours (48 hours total). In this situation with a time of injury 7 hours ago, treatment should consist of a bolus and further steroid therapy for 48 hours. Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 60
A 14-year-old girl reports hip pain that is exacerbated by weight bearing. A radiograph and biopsy specimen are shown in Figures 16a and 16b. The best course of management should be


Explanation
The patient has a unicameral bone cyst. Because the subtrochanteric part of the femur is a high-stress region, the treatment of choice is bone curettage and grafting. Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420.
Question 61
The parents of a 3-year-old girl who has had pain and swelling in the right ankle for the past 3 months now report that she has a limp and that the right knee and both ankles are painful and swollen. The limp and difficulty walking are most severe in the morning when the child first gets out of bed and are also more severe after extended walking. The parents deny fever, chills, weight loss, or night pain. Examination shows mild swelling and slightly restricted motion of the right knee and both ankles but is otherwise normal. In addition to initiation of treatment, the child should be referred to which of the following specialists?
Explanation
Pauciarticular juvenile rheumatoid arthritis (JRA) is the most common subgroup of JRA. It typically presents between the ages of 2 to 4 years with a mild swelling of one to four joints. Girls are affected four times more often than boys. The ankle and knee are commonly involved, and limping is typically worse in the morning and after extended activity. The diagnosis of pauciarticular JRA is typically one of exclusion because laboratory studies, including erythrocyte sedimentation rate and rheumatoid factor, are usually within normal limits. Pauciarticular JRA has the highest incidence of chronic uveitis, and in the subgroup with elevated antinuclear antibody (ANA) titers, the incidence is 75%. In JRA, uveitis usually occurs after the onset of synovitis but may precede the joint symptoms. At the early stage of uveitis, the patient is asymptomatic. If the eye condition is not detected and treated, progressive loss of vision may occur. Orthopaedic surgeons may be instrumental in making the diagnosis of pauciarticular JRA. Pauciarticular JRA is not associated with conditions that require input from the other specialists. Carey TP: Inflammatory arthritides: Juvenile rheumatoid arthritis, seronegative spondyloarthropathies, transient synovitis, hemophilic arthropathy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1315-1321.
Question 62
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
Explanation
V-Y advancement flaps are ideal for fingertip amputations that are transverse or dorsal oblique in nature. Healing by secondary intention is contraindicated with exposed bone. Shortening of exposed bone to allow primary skin closure is a possible alternative, as long as significant shortening of the index finger is avoided. A Moberg flap is useful only for distal amputations of the thumb. The first dorsal metacarpal artery-island pedicled flap uses tissue from the dorsum of the proximal index finger, and is typically used to resurface defects of the thumb. Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Question 63
High Yield
A 7-year-old boy sustained an acute puncture wound of the foot after stepping barefoot on a piece of glass 1 day ago. His mother states that she is not sure if she got the piece of glass out; however, she reports that his immunizations are up-to-date. Examination reveals that the wound is slightly erythematous, less than 1 mm in length on the heel, and is not currently draining. What is the next most appropriate step im management?

Detailed Explanation
The child has an up-to-date tetanus; therefore, a booster is not recommended. Pseudomonas coverage is most likely not needed because the child was barefoot. It is too early to evaluate for abscess or osteomyelitis with MRI, and a formal debridement is rarely indicated without signs of an abscess or a retained foreign body. Radiographs with soft-tissue penetration should be obtained to check for a retained foreign body. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-205.
Question 64
Figure 40 shows the radiograph of a 30-year-old woman who has a painful elbow. Examination reveals a deformed skull, multiple cafe-au-lait spots, and bone deformities. What is the most likely diagnosis?

Explanation
Findings in patients with McCune-Albright syndrome include polyostotic fibrous dysplasia, multiple cafe-au-lait spots, and precocious puberty. The bone changes in NF-1 resemble nonossifying fibromas, not fibrous dysplasia. NF-2 has little bony change with typical ocular abnormalities. Paget's disease occurs in older individuals and does not present with cafe-au-lait spots. Ollier's disease (multiple enchondromatosis) may show bone changes but not the other findings. Albright F, Butler AM, Hampton AO, et al: Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction with precocious puberty in females. N Engl J Med 1937;216:727-746. Danon M, Robboy SJ, Kim S, Scully R, Crawford JD: Cushing syndrome, sexual precocity, and polyostotic fibrous dysplasia (Albright syndrome) in infancy. J Pediatr 1975;87:917-921.
Question 65
High Yield
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the

Detailed Explanation
The sciatic nerve is formed by the roots of the lumbosacral plexus. It exits the pelvis through the greater sciatic notch and appears in the buttock anterior to the piriformus. From that point, the sciatic nerve passes posteriorly over the superior gemellus, obturator internus, inferior gemellus, and quadratus femoris before it passes deep to the biceps femoris. The tendon of the obturator internus passes through the lesser sciatic notch. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 347. Anderson JE: Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-34, 4-36.
Question 66
Radial nerve palsy is most commonly associated with which of the following types of humeral fractures?
Explanation
Although the Holstein-Lewis fracture, described as an oblique distal one third fracture, is best known for its association with neurologic injury, radial nerve palsy is most commonly associated with middle one third humeral fractures. Most nerve injuries are neurapraxias or axonotmeses, with up to 90% resolving in 3 to 4 months. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 67
High Yield
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
The patient has an evolving acute carpal tunnel syndrome. Initial management for this injury is to relieve all external pressure that may elevate the neural compression. Surgical decompression of the median nerve at the carpal tunnel is the optimal intervention. Further nonsurgical interventions (cast removal or further bivalving) are insufficient to alleviate the neural compression. Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Question 68
High Yield
Risk of fat embolism is greatest during what step of total hip arthroplasty?
Detailed Explanation
Embolization of fat and bone marrow elements during total hip arthroplasty has been studied intraoperatively using transesophageal echocardiography. These studies showed the occurrence of a large number of embolic events during the insertion of a cemented femoral stem. Embolic events were rare during insertion of a cementless stem. Femoral broaching caused some embolic events, but they were not nearly as significant as those that occurred following insertion of a cemented stem. Additionally, relocation of the cemented hip was accompanied by significant embolic events. This may be related to the untwisting of blood vessels, with the subsequent release of emboli that were most likely generated during insertion of a cemented femoral stem. Pitto RP, Koessler M, Kuehle JW: Comparison of fixation of the femoral component without cement and fixation with use of a bone-vacuum cementing technique for the prevention of fat embolism during total hip arthroplasty. J Bone Joint Surg Am 1999;81:831-843.
Question 69
High Yield
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient's neurologic recovery can be best determined by
Explanation
The patient has spinal shock. Steroid administration and MRI are appropriate therapeutic and diagnostic procedures. Myelography with CT is of little value unless there is an unusual skeletal variant. Spinal cord-evoked potentials have no value. The best method to determine the patient's neurologic recovery is repeated physical examinations over the first 48 to 72 hours. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Question 70
High Yield
The fracture shown in Figure 32 is strongly indicative of what diagnosis?

Detailed Explanation
Fractures that occur through the primary spongiosa at the subphyseal region of the metaphysis are highly specific for child abuse. On radiographic studies, the metaphyseal lucency in these injuries may appear as either the so-called "bucket-handle" or "metaphyseal corner" fracture. These fractures are not typical features of osteogenesis imperfecta or vitamin D-resistant rickets. The ingestion of lead may lead to thick, transverse bands of increased density at the distal metaphysis. Fractures in the subphyseal region of the metaphysis are not typically seen in children who have osteomyelitis. Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
Question 71
High Yield
Reconstruction of the posterior cruciate ligament (PCL) via the inlay technique involves exposure of the PCL tibial insertion site by a posterior
Explanation
The posterior medial approach through the semimembranosus/medial gastrocnemius interval is used in the inlay technique for PCL reconstruction. Exposure of the posterior capsule of the knee through this interval provides the greatest margin of safety to avoid injury to the tibial nerve, motor branch of the medial gastrocnemius, and the peroneal nerve. The direct posterior approach using the medial sural cutaneous nerve allows exposure of the popliteal neurovascular structures, but deep dissection through this interval places the motor branch of the medial gastrocnemius at risk. The interval between the semitendinosus and semimembranosus is used in accessory incisions with medial meniscus repairs but does not allow exposure of the PCL insertion. Berg EE: Posterior cruciate tibial inlay reconstruction. Arthroscopy 1995;11:69-76.
Question 72
High Yield
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Detailed Explanation
The maximum stress in a bone occurs at the periosteal surface (the greatest distance from the center of the bone). The magnitude of the stress is equal to the magnitude of the applied moment (M) multiplied by the distance to the surface (roughly the radius of the bone, r) divided by the area moment of inertia (I), so that stress = Mr/I. Of the possible answers, only area moment of inertia of the cross section contains any of these three items. The stress can also depend on the length of the bone, but it cannot be determined without knowing the location at which the bending load is applied, information that was not given in the problem. The type of structural support may influence local stresses where the support contacts the bone, but it has little effect on the maximum stress in the bone. The cross-sectional area is not as important as the area moment of inertia because the stress is not evenly distributed over the cross-section. Plastic modulus is a material property, not a geometric or structural property, and it does not affect stress. Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Question 73
High Yield
A 40-year-old woman who is an avid tennis player reports the insidious onset of progressive left shoulder pain for the past 2 months. Examination reveals full range of motion with a positive impingement sign. Strength in the supraspinatus and infraspinatus muscles is normal, although stress testing is painful. An earlier subacromial cortisone injection provided good, but only temporary relief. An AP radiograph of the left shoulder is shown in Figure 10. Management should now consist of

Explanation
The radiograph shows calcific deposits within the substance of the supraspinatus tendon. Patients with this condition are prone to recurrent bouts of acute inflammation in the shoulder. While the response to cortisone injection is often dramatic, repeated injections are not recommended because of injury to the collagen fibers. Good results have been obtained with arthroscopic evacuation of the calcium deposits. In one study, the addition of a subacromial decompression did not improve the results. Jerosch J, Strauss JM, Schmiel S: Arthroscopic treatment of calcific tendinitis of the shoulder. J Shoulder Elbow Surg 1998;7:30-37.
Question 74
Figures 21a and 21b show the radiographs of a 12-year-old patient with an L4-level myelomeningocele who has scoliosis that has been slowly progressing for the past several years. There has been no loss of motor function. An MRI scan shows no syringomyelia or increased hydrocephalus. Management should consist of


Explanation
Scoliosis is a common occurrence in children with myelomeningocele, with the incidence increasing as the neurologic level moves cephalad. The rate of pseudarthrosis for isolated anterior or posterior fusions has been reported as high as 75%. The combination of anterior and posterior fusions with some type of instrumentation has been shown to decrease the rate of pseudarthrosis to 20%. Brace treatment in smaller curves can be used as a temporizing measure to delay surgery, but as with idiopathic scoliosis, the brace is ineffective for larger curves. Observation is not indicated with a curve of this magnitude. Ward WT, Wenger DR, Roach JW: Surgical correction of myelomeningocele scoliosis: A critical appraisal of various spinal instrumentation systems. J Pediatr Orthop 1989;9:262-268.
Question 75
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
Patients with chronic ACL-deficient knees typically have lower than normal net quadriceps activity during the middle portion of the stance phase; the net moment about the knee reverses from one that demands quadriceps activity to one that demands increased hamstring activity. This type of gait is termed "quadriceps avoidance." This avoidance is believed to be a functional adaptation to reduce anterior tibial translation, and it is most prevalent as the knee moves from 45 degrees of flexion toward full extension, the arc of motion through which the ACL is most responsible for stability. Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20. Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Question 76
High Yield
Following fixation of a displaced intra-articular fracture of the distal humerus through a posterior approach, what is the expected outcome?

Explanation
Following repair of a displaced intra-articular distal humerus fracture, the ability to regain full elbow range of motion is rare. Recent reports of olecranon osteotomy have yielded healing rates of between 95% to 100%. According to McKee and associates, patients can be expected to have residual loss of elbow flexion strength of 25%. McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 77
High Yield
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
Changing from a solid keel to a keel with a sagittal split allows an amputee to navigate uneven terrain more easily. Changing the length of the keel affects the responsiveness of the prosthesis but does not address the surface conditions for ambulation. The SACH is not used as frequently anymore, because overload problems to the nonamputated foot have been observed. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Question 78
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?


Explanation
The radiographs show early ectopic bone formation originating between the ulna and the radius. The development of ectopic bone in this area following a two-incision approach for anatomic repair of the distal biceps tendon is thought to be related to exposure of the periosteum of the lateral ulna during surgery. This can be avoided by the use of a muscle-splitting incision between the extensor carpi ulnaris and common extensor muscles. Full pronation of the forearm allows for the necessary exposure of the radial tuberosity during the procedure and for fixation of the tendon at its maximal length. Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Question 79
In the spine, osteoblastomas usually originate in the

Explanation
Osteoblastomas are benign lesions that represent less than 5% of benign bone tumors. Most lesions are located in the spine, followed by the femur, tibia, and skull. Patients with spinal lesions usually have pain that may be associated with scoliosis. The most common location in the spine is within the posterior elements.
Question 80
What process is often found associated with other neoplasms?

Explanation
Aneurysmal bone cyst may be either a "pattern" or a "diagnosis." Therefore, aneurysmal bone cyst should be viewed as a diagnosis of exclusion. Hemorrhage into a variety of primary bone lesions (eg, giant cell tumor of bone, chondroblastoma, osteoblastoma, fibrous dysplasia, osteosarcoma, or vascular neoplasms) may result in intralesional, membrane-bone blood-filled cysts. Such secondary changes may be confused with aneurysmal bone cyst, resulting in inappropriate therapy because assessment should be focused on identifying the underlying primary process. The entire specimen should be examined histologically in an effort to locate an underlying primary bone tumor. Bonakdarpour A, Levy WM, Aegerter E: Primary and secondary aneurysmal bone cyst: A radiological study of 75 cases. Radiology 1978;126:75-83. Levy WM, Miller AS, Bonakdarpour A, Aegerter E: Aneurysmal bone cyst secondary to other osseous lesions: Report of 57 cases. Am J Clin Pathol 1975;63:1-8.
Question 81
High Yield
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?

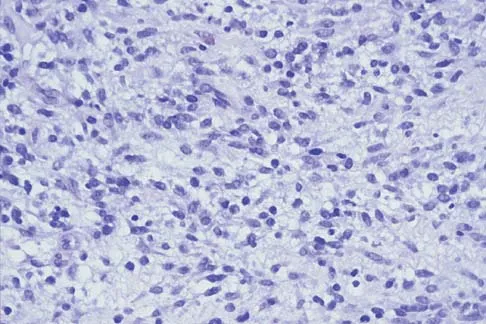
Explanation
The patient has infantile fibrosarcoma. For unresectable lesions, the treatment of choice is chemotherapy with vincristine, actinomycin-D, and cyclophosphamide, followed by excision if there is an adequate decrease in the size of the lesion.
Question 82
High Yield
What type of metastatic tumor most often has a lytic radiographic appearance?

Detailed Explanation
Lung carcinoma most often has a lytic radiographic appearance. Bladder and prostate carcinoma are usually blastic. Breast carcinoma can be both blastic and lytic. Thyroid carcinoma may be difficult to visualize radiographically and may be seen only on MRI scans. Metastatic osteosarcomas typically produce bone. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 83
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction. Rockwood and Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Question 84
High Yield
Figures 47a through 47f show the AP radiograph, bone scan, CT scan, MRI scan, and biopsy specimens of a 30-year-old woman who has had vague left shoulder pain for 1 year. Management should consist of




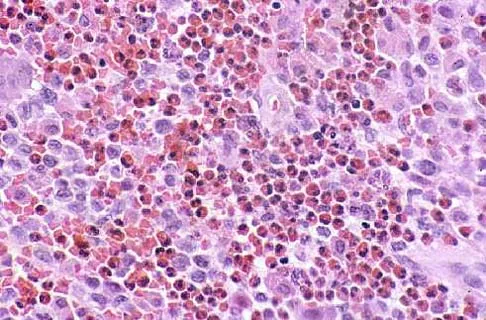
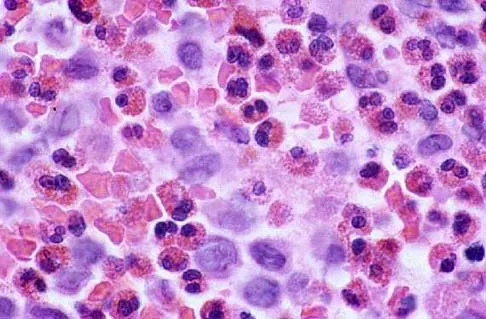
Explanation
The histology shows eosinophils with a background of larger cells (Langerhans' cells). This is consistent with eosinophilic granuloma. Localized sites are best treated with curettage, steroid injection, or observation. Chemotherapy is used only if there is systemic involvement. Mirra JM: Eosinophilic granuloma, in Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. London, England, Lea and Febiger, 1989, pp 1023-1060. Sessa S, Sommelet D, Lascombes P, Prevot J: Treatment of Langerhans-cell histiocytosis in children: Experience at the Children's Hospital of Nancy. J Bone Joint Surg Am 1994;76:1513-1525.
Question 85
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of

Explanation
The patient has a symptomatic painful atrophic midclavicular nonunion, and the treatment of choice is rigid internal fixation with a dynamic compression plate and autogenous bone grafting. A tension band effect is desired and achieved by placing the plate superiorly. Excellent success rates of 90% to 100% have been reported using this technique. Intramedullary screw fixation without bone grafting has a decreased success rate. Partial claviculectomy is not a preferred option. Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Question 86
High Yield
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include

Explanation
In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
Question 87
Figure 13 shows the radiographs of a 20-year-old intercollegiate basketball player who was injured 6 weeks prior to the start of the season. What is the most appropriate treatment?

Explanation
A Jones fracture occurs at the metaphyseal-diaphyseal junction of the fifth metatarsal. It is often an acute fracture in conjunction with a chronic stress-related injury. It requires either a short leg cast with strict non-weight-bearing or surgical fixation. In the high performance athlete, the need for rapid return to sport activity usually requires surgical intervention, most commonly with an intramedullary screw. Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, vol 2, pp 2391-2409.
Question 88
High Yield
Design and manufacturing of a metal-on-metal articulation has an important influence on the tribology. Which of the following statements best characterizes the type of contact that is best for metal-on-metal articulations?
Detailed Explanation
It is important that the radii of a metal-on-metal head to cup articulation be such that there is polar contact. As the radii become closer to equal, conditions favor higher frictional torque and equatorial seizing. The "bedding in" of metal-on-metal surfaces and their stiffness are both components of the properties considered in the design of polar contact surfaces.
Question 89
High Yield
In a longitudinal study of children with spastic diplegia, analysis of long-term function will most likely reveal
Detailed Explanation
In a longitudinal study of 18 patients with spastic diplegia over a period of 32 months, three-dimensional gait analysis revealed a deterioration of gait stability with increases in double support time and decreases in single support time. Kinematic data also identified a loss of excursion about the knee, ankle, and pelvis. Interestingly, the static examination of the children showed a decrease in the popliteal angle over time. The authors concluded that ambulatory ability tends to worsen over time in children with spastic diplegia.
Question 90
High Yield
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Detailed Explanation
When attempting a revision anterior cervical approach from the side opposite the original approach, it is important to evaluate the function of the vocal cords. If this evaluation reveals dysfunction of the vocal cord on the side of the original approach, then an approach on the contralateral side should not be attempted. Injury to the stellate ganglion, which causes a Horner's syndrome, should not preclude an approach on the contralateral side. While the side of the symptomatology can influence the surgeon's choice as to the side of an anterior approach, it does not preclude a certain approach. When approaching the lower cervical spine from the right side, the recurrent laryngeal nerve can cross the surgical field and should be preserved. Excessive intraoperative pressure on the esophagus can increase the incidence of dysphagia, but its incidence is no different with either approach. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.
Question 91
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
Sexual dysfunction is a common condition after extensive anterior lumbar surgical dissection. Erectile dysfunction usually is nonorganic but may be related to parasympathetic injury. The parasympathetic nerves are deep in the pelvis at the level of S2-3 and S3-4 and usually are not involved in the surgical field for anterior L4-5 and L5-S1 procedures. Retrograde ejaculation is the result of injury to the sympathetic chain on the anterior surface of the major vessels crossing the L4-5 level and at the L5-S1 interspace. Erectile function and orgasm are not affected by sympathetic injury. The pudendal nerve is primarily a somatic nerve and is not located in the surgical field. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Question 92
A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm3. What is the most common organism in this scenario?

Explanation
The most common bacterial etiologic agent following varicella is group A beta-hemolytic streptococcus. The other organisms are much less common. Staphylococcus aureus is the most common bone infection organism. Staphylococcus epidermidis is increasingly a bone infection organism. Group B streptococcus occurs more commonly in newborns. Kingella kingae is a common joint pathogen but is not as common following varicella. Schreck P, Schreck P, Bradley J, et al: Musculoskeletal complications of varicella. J Bone Joint Surg Am 1996;78:1713-1719.
Question 93
A 38-year-old man caught his index finger in a volleyball net. He noted an angular deformity of the finger that was reduced when a teammate pulled on his finger. Three weeks later, he now reports trouble extending his finger. A clinical photograph is shown in Figure 55. What anatomic structure is most likely injured?

Explanation
The clinical photograph shows a classic boutonniere deformity. It is likely that the patient sustained a volar dislocation of the proximal interphalangeal joint, with a concomitant rupture of the central slip insertion of the extensor tendon. Peimer CA, Sullivan DJ, Wild DR: Palmar dislocation of the proximal interphalangeal joint. J Hand Surg Am 1984;9:39-48.
Question 94
High Yield
Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?
Explanation
Long-term survivorship studies have attempted to clarify patient factors related to good outcomes in HTO. One particular study showed that a patient age of less than 50 years was related to good outcomes in those who had good preoperative knee flexion. The same study found no relation between HTO failure and the presence of postoperative infection or deep venous thrombosis. The presence of a lateral tibial thrust is a contraindication to performing this surgery. As expected, good patient selection is critical to obtaining good long-term results with HTO. Naudie D, Borne RB, Rorabeck CH, Bourne TJ: Survivorship of the high tibial valgus osteotomy: A 10- to 22-year followup study. Clin Orthop 1999;367:18-27. Rinonapoli E, Mancini GB, Corvaglia A, Musiello S: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Question 95
A 37-year-old man has left shoulder pain and weakness. Coronal T1- and axial T2-weighted MRI scans are shown in Figures 17a and 17b. The biopsy specimen is shown in Figure 17c. What is the most likely diagnosis?



Explanation
A ganglion cyst arising from the posterior labrum of the shoulder is a known cause of suprascapular nerve impingement. The MRI characteristics of low-signal intensity on T1 and high-signal intensity on T2 are seen in lesions with a high fluid content. The histology shows a cavity with a thin fibrous lining. Ferrick MR, Marzo JM: Suprascapular entrapment neuropathy and ganglion cysts about the shoulder. Orthopedics 1999;22:430-434.
Question 96
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?

Explanation
There is no evidence that early weight bearing enhances ultimate rehabilitation. At the other extreme, weight bearing should not be delayed for a prolonged period of time. In a young, healthy individual, the rigid plaster dressing appears to be the safest method of protecting the wound during the early postoperative period. If the wound appears to be secure, early partial weight bearing can be safely initiated. Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Question 97
High Yield
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of


Explanation
The hallux varus seen in this patient is most likely the result of a combination of causes. Based on the degenerative changes and the significant shortening of the first metatarsal relative to the second metatarsal, a metatarsophalangeal arthrodesis is the treatment of choice. The other surgical approaches are not expected to provide a satisfactory result. Coughlin MJ, Mann RA: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby-Year Book, 2000, pp 150-269.
Question 98
High Yield
The mother of a healthy 8-month-old boy reports that her son refuses to use his left arm. Examination reveals that the arm hangs limp at his side in an adducted and internally rotated position, and the affected shoulder subluxates posteriorly. Passive external rotation measures 15 degrees. Management should consist of

Detailed Explanation
Injury to the upper trunk of the brachial plexus during birth (Erb's palsy) occurs in approximately 1 in 3,000 births. In a complete lesion, paralysis of the deltoid, supraspinatus, infraspinatus, teres minor, biceps, and brachioradialis results in the findings described above. Spontaneous recovery may occur for up to 2 years. Passive exercises administered daily by the parents are the initial recommended treatment at this age. If significant contracture results in posterior dislocation, surgical correction may be considered. Neer CS: Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 452-454. Pearl ML: Arthroscopy release of shoulder contracture secondary to birth palsy: An early report on findings and surgical technique. Arthroscopy 2003;19:577-582.
Question 99
High Yield
A 50-year-old electrician who is right-hand dominant has had right shoulder pain and stiffness after sustaining an electric shock 2 months ago. An AP radiograph obtained at the time of injury was considered negative, and the patient was diagnosed with a shoulder sprain. The patient now reports continued shoulder pain and restricted motion. AP and axillary radiographs and a CT scan are shown in Figures 41a through 41c. Management should consist of



Explanation
Open reduction and transfer of the subscapularis and lesser tuberosity into the humeral head defect is the treatment of choice for chronic posterior dislocations in which the articular defect consists of 20% to 40% of the articular surfaces. Closed reduction can be used if the dislocation is recognized early and the articular defect is less than 20% of the articular surface. Humeral arthroplasty is reserved for patients with an articular defect that is greater than 45% to 50% of the head. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 100
High Yield
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20 degrees. Management should consist of
Explanation
Indications for surgical treatment of spondylolisthesis include pain and/or progression of deformity. Specifically, surgery is necessary when there is persistent pain or a neurologic deficit that fails to respond to nonsurgical therapy, there is significant slip progression, or the slip is greater than 50%. For patients with mild spondylolisthesis, in situ posterolateral L5-S1 fusion is adequate. In patients with more severe slips (greater than 50%), extension of the fusion to L4 offers better mechanical advantage. Postoperative immobilization may be achieved with instrumentation, casting, or both. In patients with a slip angle of greater than 45 degrees, reduction of the lumbosacral kyphosis with instrumentation or casting is desirable to prevent slip progression. Laminectomy alone is contraindicated in a child. Nerve root decompression is indicated if radiculopathy is present clinically. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
