Welcome, colleagues, to the operating theater. Today, we are undertaking a comprehensive exploration of a fascinating, unforgiving, and often deceptively challenging set of injuries: distal interphalangeal (DIP) joint fracture-dislocations. While statistically less common than proximal interphalangeal (PIP) joint injuries due to the inherent geometric and ligamentous stability of the terminal digit, when DIP fracture-dislocations do occur, they demand meticulous attention to detail, precision engineering, and a profound understanding of the delicate micro-anatomy. Our goal today is not merely to achieve radiographic union; it is to restore precise kinetic function, prevent long-term functional disability, and avoid the dreaded cascade of secondary deformities such as the swan neck or chronic mallet posture.
Comprehensive Introduction and Patho-Epidemiology
The distal interphalangeal joint serves as the terminal effector of the hand's intricate kinetic chain. It is responsible for the fine pinch, the powerful grasp, and the subtle tactile feedback necessary for complex human interaction with the environment. Because it lies at the very end of the lever arm, the DIP joint is subjected to extraordinary biomechanical forces during both athletic endeavors and routine occupational tasks. When these forces exceed the physiological tolerance of the joint's stabilizing structures, catastrophic failure occurs, leading to fracture-dislocations.
Epidemiologically, these injuries are frequently encountered in young, active populations, particularly athletes involved in ball sports (basketball, baseball, football) and individuals engaged in heavy manual labor. The mechanism of injury typically dictates the patho-anatomic pattern. An axial load applied to an extended digit often results in a dorsal fracture-dislocation or a mallet variant, whereas a sudden, violent hyperextension force applied to an actively flexing digit classically produces a volar avulsion, synonymous with the "Jersey finger." High-energy crush injuries or complex twisting forces can yield highly unstable, multidirectional fracture-dislocations that severely compromise the soft tissue envelope.
The pathophysiology of these injuries is defined by the disruption of the delicate balance between the flexor and extensor mechanisms. The DIP joint operates under a constant state of dynamic tension. When the terminal extensor tendon or its bony insertion is compromised (mallet fracture), the unopposed pull of the flexor digitorum profundus (FDP) drives the joint into flexion, eventually leading to secondary PIP joint hyperextension (swan neck deformity) due to proximal retraction of the extensor apparatus. Conversely, an FDP avulsion leaves the terminal extensor unopposed, severely crippling grip strength and independent digit flexion.
Failure to recognize the severity of these injuries, or treating them with benign neglect, invariably leads to disastrous outcomes. Chronic subluxation rapidly progresses to post-traumatic osteoarthritis, profound stiffness, and chronic pain. Therefore, a comprehensive understanding of the pathomechanics is the absolute prerequisite for formulating an effective surgical strategy. We must approach these joints with the same intellectual rigor and technical precision as we would a major intra-articular fracture of the knee or elbow.
Detailed Surgical Anatomy and Biomechanics
Let us begin by reviewing the critical anatomical structures that provide stability to the DIP joint and are universally compromised in these high-energy injuries. The DIP joint is a ginglymus (hinge) joint, inherently stable due to its robust ligamentous architecture, tendinous insertions, and highly congruent articular geometry.
Osteology and Articular Geometry
The distal end of the middle phalanx presents a bicondylar head, characterized by two distinct convex condyles separated by a shallow intercondylar groove. This articulates precisely with the biconcave articular surface of the base of the distal phalanx. A prominent intercondylar ridge on the distal phalanx mates with the groove on the middle phalanx, providing substantial intrinsic resistance to radioulnar translation and rotatory forces.
The volar base of the distal phalanx features a prominent tubercle that serves as the broad insertion footprint for the FDP tendon. Dorsally, the base extends into a prominent lip, which provides the insertion site for the terminal extensor tendon. Mallet fractures involve an intra-articular bony avulsion from this dorsal base, whereas FDP avulsions involve the volar base. The precise calculation of the articular surface involved in these fractures is paramount, as fragments encompassing more than 30-50% of the articular arc invariably lead to dorsal or volar subluxation of the remaining distal phalanx.
Ligamentous and Capsular Structures
The collateral ligaments are the primary stabilizers against varus and valgus stress. These paired ligaments, radial and ulnar, originate from the lateral condylar recesses of the middle phalanx and insert obliquely onto the lateral base of the distal phalanx. Unlike the PIP joint, where the collateral ligaments undergo significant length changes during the arc of motion, the DIP collateral ligaments remain relatively isometric, providing consistent stability in both flexion and extension.
The volar plate is a robust, fibrocartilaginous structure that forms the floor of the joint. It is firmly attached to the volar margin of the distal phalanx and loosely attached proximally to the middle phalanx via thin, membranous checkrein ligaments. It functions to prevent hyperextension and deepens the articular concavity. In dorsal dislocations, the volar plate is frequently avulsed from its proximal attachment and can become interposed within the joint space, creating an irreducible dislocation that mandates open surgical intervention.
Tendinous Insertions and Pulley System
The flexor digitorum profundus (FDP) is the sole flexor of the DIP joint. It originates proximally in the forearm, traverses the carpal tunnel, and inserts broadly onto the volar base of the distal phalanx. The integrity of this insertion is a massive stabilizer against dorsal translation. The FDP tendon is mechanically optimized by a complex pulley system. At the level of the DIP joint, the A4 and A5 annular pulleys, along with the C3 cruciate pulley, are critically relevant. The A4 pulley, located over the middle phalanx, is essential for preventing bowstringing; its preservation during surgical exposure is an absolute necessity.
The vascular supply to the FDP tendon is tenuous and highly relevant to surgical timing. Blood is supplied via the vinculum longus profundus (VLP) and vinculum brevis profundus (VBP), thin mesenteries that attach the tendon to the dorsal aspect of the flexor sheath. Type I FDP avulsions, which retract violently into the palm, completely disrupt these vinculae, leading to rapid ischemic necrosis of the tendon stump and demanding urgent surgical intervention within 7 to 10 days.
The extensor mechanism at this level is a complex aponeurotic confluence. The lateral bands merge dorsally over the middle phalanx to form the terminal extensor tendon, which inserts onto the dorsal base of the distal phalanx. This insertion is remarkably robust, averaging 10.1 mm in transverse width and 5.6 mm in longitudinal length. It sits mere millimeters (typically 1.4 mm) proximal to the germinal matrix of the fingernail. Disruption of this insertion, either purely tendinous or via a bony avulsion, yields the classic "mallet finger."
Neurovascular Topography
The proper digital nerves and arteries run along the radial and ulnar aspects of each digit, situated volar to the collateral ligaments and dorsal to the flexor tendon sheath (Cleland's ligaments). At the level of the DIP joint, these vessels arborize extensively to supply the terminal pulp, the nail bed, and the joint capsule.
They are acutely susceptible to iatrogenic injury during surgical dissection, particularly with aggressive longitudinal incisions or overzealous retraction. The vascularity of the dorsal skin and nail matrix relies heavily on delicate dorsal branches of the proper digital arteries. When executing dorsal approaches for mallet fractures, meticulous handling of the skin flaps is critical to prevent full-thickness necrosis and subsequent hardware exposure.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for DIP joint fracture-dislocations hinges on a careful analysis of joint stability, articular congruity, and the functional demands of the patient. While many closed injuries can be managed with rigorous splinting protocols, surgical intervention is mandated when conservative measures fail to restore the precise mechanical environment required for healing.
Operative indications for mallet fractures (dorsal avulsion injuries) are generally reserved for fractures complicated by volar subluxation of the distal phalanx, or those involving a massive critical portion of the articular surface (traditionally cited as >30% to 50%). If the joint cannot be concentrically reduced and maintained in a closed splint, surgery is required to prevent rapid-onset osteoarthritis.
For FDP avulsions (Jersey fingers), operative treatment is universally recommended for all acute injuries. The Leddy and Packard classification dictates the urgency. Type I injuries (retraction into the palm) require urgent repair (within 7-10 days) due to the complete loss of vincula blood supply. Type II and III injuries, where the tendon is held at the PIP joint or A4 pulley respectively, allow for a slightly more forgiving surgical window, but early anatomic repair remains the gold standard.
Contraindications to surgical intervention are primarily related to severe patient comorbidities that preclude anesthesia, non-compliance, or a severely compromised soft tissue envelope that would inevitably lead to infection or hardware exposure. In highly uncooperative patients, the risks of pin-tract infections, hardware migration, and catastrophic failure often outweigh the benefits of anatomic reduction.
| Category | Operative Indications | Non-Operative Indications / Contraindications |
|---|---|---|
| Mallet Fractures | Volar subluxation of the distal phalanx; Articular involvement > 30-50%; Failure of closed splinting; Open fractures. | Articular involvement < 30%; No subluxation; Patient unable to comply with post-op pin care; Severe peripheral vascular disease. |
| FDP Avulsions | All acute injuries (Leddy-Packard Types I-IV); Chronic injuries in high-demand patients (may require staged reconstruction). | Low-demand elderly patients with chronic, asymptomatic injuries (Type I late presentation); Active local infection. |
| Dislocations | Irreducible closed dislocation (suspected volar plate or FDP interposition); Gross instability post-reduction; Associated unstable fractures. | Stable, concentrically reduced closed dislocations with congruent articular surfaces and intact collateral ligaments. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock upon which surgical success is built. Before the scalpel touches the skin, the surgeon must have a three-dimensional understanding of the fracture pattern, an anticipation of potential intraoperative pitfalls, and a clear, sequential strategy for reduction and fixation.
Clinical Evaluation and Imaging
The clinical examination must be rigorous. Hand dominance, occupation, and avocation profoundly influence treatment goals. A concert violinist with a mallet fracture requires a vastly different functional outcome than a retired individual with low functional demands. Test active DIP flexion to assess FDP integrity; complete inability to flex the terminal phalanx is pathognomonic for a complete avulsion. Test active DIP extension to evaluate the terminal tendon. Assess collateral ligament stability with gentle varus and valgus stress testing under digital block if necessary.

FIG 1 • Lateral radiographs usually are the most helpful in identifying a mallet fracture. Note that in this image, the avulsed fragment includes more than 50% of the articular surface. There is no significant volar subluxation in this case.
High-quality imaging is non-negotiable. Standard posteroanterior (PA), true lateral, and oblique radiographs of the affected digit are mandatory. The true lateral view is the most critical image for evaluating DIP joint congruency and quantifying the size of articular avulsion fragments.
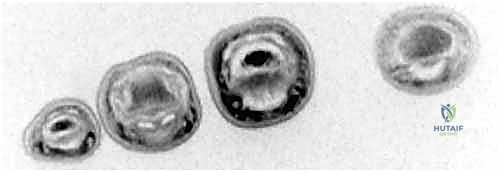
FIG 2 • A. Flexor digitorum profundus (FDP) avulsion in which a bony fragment has been caught up at the A4 pulley.
In cases of suspected FDP avulsion without a clear bony fragment on plain films, advanced imaging is highly beneficial. Ultrasound is an excellent, dynamic, and cost-effective modality for locating the retracted tendon stump in the acute setting. Magnetic Resonance Imaging (MRI) is the gold standard for subacute or chronic cases, providing unparalleled visualization of soft tissue integrity, tendon retraction levels, and the condition of the flexor sheath.
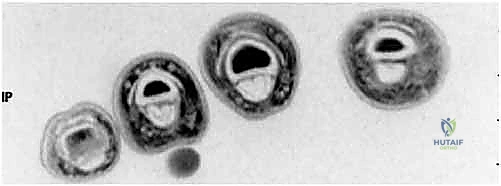
FIG 2 • C. Axial cut MRI at the level of the proximal phalanx shows both FDP and flexor digitorum superficialis (FDS) tendons are present. D. At the level of the middle phalanx, only the FDS tendon can be seen.
Equipment, Templating, and Anesthesia
Surgical instrumentation must be specifically tailored for hand surgery. A standard mini-fragment or micro-fragment set (1.0 mm, 1.3 mm, 1.5 mm screws) should be available. Smooth Kirschner wires (K-wires) in sizes 0.035-inch and 0.045-inch are the workhorses of DIP joint fixation. Preoperative templating on digital radiographs helps anticipate the trajectory of K-wires and the appropriate length of micro-screws if ORIF is planned.
Anesthetic choice is evolving. While regional blocks (axillary or supraclavicular) combined with a proximal tourniquet remain standard, the WALANT (Wide Awake Local Anesthesia No Tourniquet) technique is gaining massive traction. WALANT utilizes lidocaine with epinephrine, providing excellent hemostasis without a tourniquet, and crucially allows the surgeon to assess active tendon excursion and joint stability intraoperatively by asking the awake patient to move the digit.
Patient Positioning and Operating Room Setup
The patient is positioned supine with the affected upper extremity extended onto a radiolucent hand table. A flexible aluminum hand-holder (lead hand) is indispensable for maintaining digit positioning, particularly during volar approaches for FDP repair.
If WALANT is not utilized, a well-padded pneumatic tourniquet is applied to the upper arm and inflated to 250 mmHg after exsanguination with an Esmarch bandage. The fluoroscopy C-arm (preferably a mini C-arm for maneuverability) is draped sterilely and positioned perpendicular to the hand table, allowing for seamless transition between PA and lateral views without disrupting the surgical field.
Step-by-Step Surgical Approach and Fixation Technique
We will now detail the intraoperative execution of the most common and effective techniques for managing these complex injuries, focusing on the extension-block pinning technique for mallet fractures and the principles of FDP repair.
I. Extension-Block Pinning for Mallet Fractures
Pioneered by Ishiguro, the extension-block pinning technique is a highly elegant, minimally invasive method for treating mallet fractures with dorsal subluxation or large articular fragments. The core principle is to utilize a dorsal K-wire to block the avulsed fragment from displacing dorsally, while a second K-wire transfixes the joint in extension, utilizing the intact volar soft tissues to hinge the joint and anatomically reduce the fracture.
1. Anesthesia, Tourniquet, and Initial Assessment:
Following anesthesia and exsanguination, baseline fluoroscopic images are obtained to confirm the fracture pattern and the degree of volar subluxation of the distal phalanx.

TECH FIG 1 • C. PA fluoroscopic image confirms good bony purchase in both the dorsal and volar phalanx.
2. Joint Flexion and Fragment Mobilization:
The critical first maneuver is to flex the DIP joint to approximately 90 degrees. This action is twofold: it relaxes the terminal extensor mechanism, neutralizing its proximal pull on the avulsed fragment, and it allows the fracture fragment to settle volarly into its anatomic bed. This flexion maneuver is the key to unlocking the reduction.

TECH FIG 1 • A. The DIP joint is flexed to 90 degrees to pull the avulsed fragment distally.
3. Insertion of the Dorsal Blocking Pin:
With the joint held firmly in 90 degrees of flexion, the dorsal blocking pin is introduced. A 0.045-inch (or 0.035-inch for smaller digits) smooth K-wire is driven percutaneously from dorsal-distal to volar-proximal. The entry point is critical: it must be immediately dorsal to the avulsed fragment, utilizing the pin to "block" the fragment from migrating dorsally. The pin is driven into the head of the middle phalanx, achieving bicortical purchase.
TECH FIG 1 • B. A 0.045-inch K-wire is inserted dorsally into the middle phalanx head, just proximal to the fracture fragment.
It is paramount that this blocking pin does not skewer the fracture fragment itself, as this would prevent subsequent reduction. Fluoroscopy is utilized extensively during this step to ensure the pin is perfectly positioned to act as a buttress.

TECH FIG 1 • D. Lateral fluoroscopic image confirming the position of the dorsal blocking pin.
4. Joint Extension and Anatomic Reduction:
Once the blocking pin is secure, the DIP joint is carefully extended. As the distal phalanx extends, the intact volar hinge (volar plate and FDP) forces the avulsed dorsal fragment against the rigid blocking pin. This dynamic maneuver effectively squeezes the fracture into an anatomic reduction.

TECH FIG 2 • A. The DIP joint is extended, reducing the fracture fragment against the blocking pin.
The surgeon must avoid forceful hyperextension, which can distract the fracture volarly or cause iatrogenic fragmentation of the dorsal lip. A true lateral fluoroscopic image is obtained to confirm absolute articular congruity.

TECH FIG 2 • B. Lateral fluoroscopic image confirming anatomic reduction of the articular surface.
5. Transarticular Fixation:
With the fracture anatomically reduced and held in extension, a second 0.045-inch K-wire is driven longitudinally across the DIP joint. This pin is introduced through the tip of the distal phalanx, passing just volar to the fracture site, and driven into the medullary canal of the middle phalanx.

TECH FIG 3 • A. A second K-wire is driven longitudinally across the DIP joint to maintain reduction.
This transarticular pin neutralizes all deforming forces and maintains the joint in neutral extension. Both pins are then cut outside the skin and bent to prevent migration and facilitate future removal in the clinic.

TECH FIG 3 • B. Final lateral fluoroscopic view demonstrating stable fixation and excellent articular congruity.

TECH FIG 3 • C. Clinical appearance of the digit after extension-block pinning.
II. Open Reduction and Internal Fixation (ORIF)
In cases where closed extension-block pinning fails to achieve an anatomic reduction (often due to soft tissue interposition or chronic delay), or when dealing with massive, single-piece articular fragments, ORIF is indicated.
1. Surgical Approach:
A dorsal H-shaped, Y-shaped, or lazy-S incision is utilized over the DIP joint. Full-thickness skin flaps are elevated, meticulously preserving the delicate dorsal venous network and the germinal matrix of the nail bed.

TECH FIG 4 • A. Dorsal approach to the DIP joint for ORIF of a complex mallet fracture.
2. Fracture Preparation and Fixation:
The terminal extensor tendon is identified, and the fracture hematoma is cleared. The joint is inspected for interposed capsule or cartilage debris. The fracture is anatomically reduced under direct visualization using a sharp dental pick or a small reduction clamp.

TECH FIG 4 • B. Direct visualization of the fracture fragment prior to fixation.
Fixation can be achieved using multiple techniques depending on fragment size. For large, solid fragments, 1.0 mm or 1.3 mm micro-screws provide excellent interfragmentary compression. Alternatively, a dorsal hook plate can be utilized to buttress the fragment without violating the small bone with a drill bit.

TECH FIG 4 • C. Application of a dorsal hook plate for rigid internal fixation.
Regardless of the hardware used, a transarticular K-wire is often placed to protect the fixation construct during the initial healing phase.

TECH FIG 4 • D. Final fluoroscopic confirmation of ORIF with a hook plate and transarticular pin.
III. Flexor Digitorum Profundus (FDP) Avulsion Repair
The surgical management of FDP avulsions requires meticulous handling of the tendon to prevent scarring and strict adherence to biomechanical principles to ensure a repair strong enough to withstand early active motion protocols.
1. Exposure and Tendon Retrieval:
A volar Bruner (zigzag) or mid-lateral incision is made over the affected digit, extending into the palm if a Type I injury is suspected. The flexor sheath is exposed. The A4 pulley must be meticulously preserved. If the tendon has retracted proximally, it is retrieved using a small pediatric feeding tube or a specialized tendon retriever. The tendon is gently threaded back through the intact pulley system.
2. Reattachment Techniques:
The volar base of the distal phalanx is prepared by decorticating a small footprint to bleeding bone to promote tendon-to-bone healing.
Historically, the pull-out button technique (Bunnell) was the gold standard, where sutures are passed through the tendon, drilled through the distal phalanx, and tied over a button on the dorsal nail plate.

