Open Reduction of Radial Head & DRUJ Dislocation
Key Takeaway
Surgical management of radial head and distal radioulnar joint (DRUJ) dislocations requires a profound understanding of forearm biomechanics. This comprehensive guide details the indications, surgical approaches, and reconstructive techniques for both acute and chronic instability. From annular ligament repair to complex DRUJ stabilization using the Bunnell and Liebolt techniques, orthopedic surgeons will find evidence-based protocols to optimize functional outcomes and prevent chronic osteoarthrosis.
INTRODUCTION TO FOREARM INSTABILITY
The forearm functions as a complex, articulated ring, mechanically linked by the proximal radioulnar joint (PRUJ), the interosseous membrane (IOM), and the distal radioulnar joint (DRUJ). Disruption of this delicate biomechanical linkage—whether through isolated radial head dislocation, complex fracture-dislocations of the elbow, or DRUJ instability—can lead to chronic persistent subluxation, severe functional impairment, and symptomatic osteoarthrosis.
The management of these injuries requires a highly nuanced, evidence-based approach. Failure to recognize and anatomically restore the stabilizing structures of both the proximal and distal radioulnar joints inevitably results in catastrophic failure of forearm kinematics. This masterclass details the operative indications, surgical anatomy, and step-by-step reconstructive techniques for managing dislocations of the radial head and the DRUJ.
OPEN REDUCTION OF RADIAL HEAD DISLOCATION
Isolated traumatic dislocations of the radial head in adults are exceedingly rare and should immediately raise clinical suspicion for an associated ulnar fracture (Monteggia variant) or longitudinal radioulnar dissociation (Essex-Lopresti lesion). Chronic, unreduced dislocations inevitably lead to degenerative changes, restricted pronosupination, and valgus instability of the elbow.
Pathoanatomy and Biomechanics
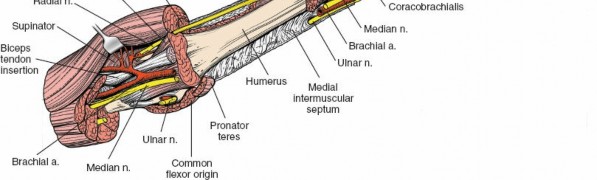
The radial head is primarily stabilized by the annular ligament, which encircles the radial neck and anchors to the anterior and posterior margins of the lesser sigmoid notch of the ulna. Secondary stabilizers include the radial collateral ligament (RCL) complex and the capitellum itself.
In acute dislocations, the annular ligament is typically avulsed or ruptured. If closed reduction is impeded, it is frequently due to the interposition of the torn annular ligament or the joint capsule.
Surgical Warning: A fractured coronoid process strongly suggests that the elbow had become at least partially dislocated at the time of injury. In these complex fracture-dislocations, the brachialis muscle may be torn, the anterior capsule avulsed, and the collateral ligaments ruptured. Severe soft-tissue damage dictates that closed methods will fail; aggressive surgical débridement and anatomical repair are mandatory.
Surgical Technique: Annular Ligament Repair and Reconstruction
When open reduction is indicated—either due to irreducibility or chronic instability—the surgical objective is to clear the joint of interposed tissue, reduce the radial head, and restore the integrity of the annular ligament.
Step 1: Surgical Approach
* The patient is positioned supine with the arm draped over a hand table. A tourniquet is applied to the proximal arm.
* A Kocher approach (interval between the anconeus and extensor carpi ulnaris) or a Kaplan approach (interval between the extensor digitorum communis and extensor carpi radialis brevis) is utilized.
* Care must be taken to protect the posterior interosseous nerve (PIN), particularly when dissecting distally. Pronating the forearm moves the PIN anteriorly, away from the surgical field.
Step 2: Joint Inspection and Debridement
* The radiocapitellar joint is exposed. The ruptured annular ligament is identified.
* Interposed capsular debris or osteochondral fragments are meticulously excised to allow concentric reduction of the radial head.
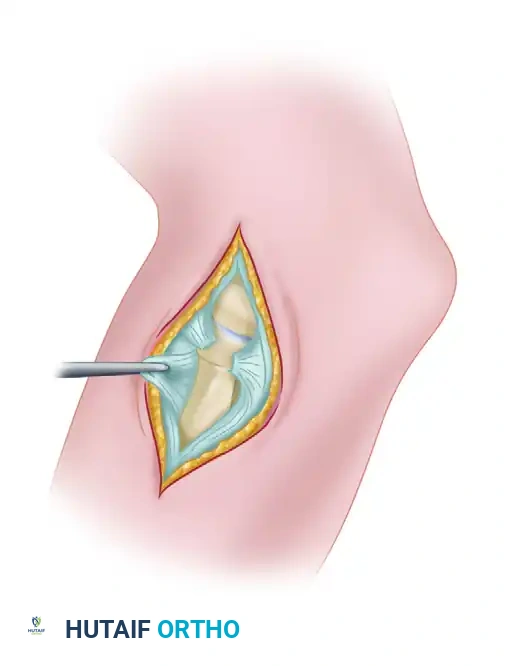
Figure: Dislocation of the radial head demonstrating a ruptured annular ligament. In acute settings, this ligament can often be sutured satisfactorily.
Step 3: Ligament Repair or Reconstruction
* Primary Repair: If the tissue quality is robust, the annular ligament is repaired directly to its ulnar footprint using suture anchors or transosseous sutures.
* Reconstruction: In chronic cases (greater than 4-6 weeks) where the annular ligament is contracted, attenuated, or absent, reconstruction is required. A strip of autologous fascia lata or a slip of the triceps tendon can be utilized.
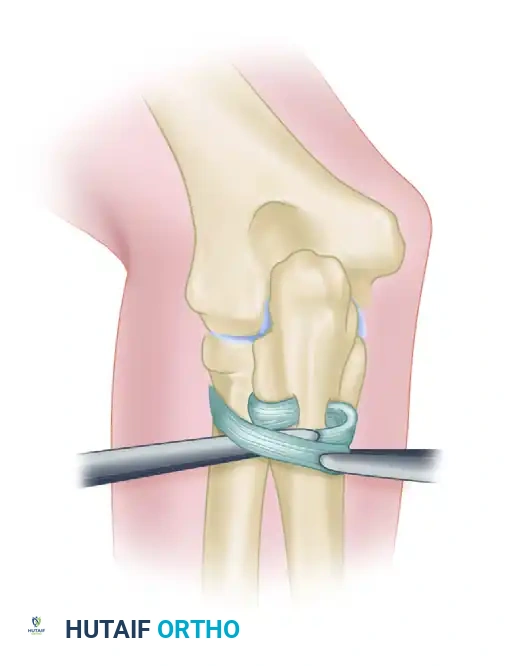
Figure: If primary repair is impossible, the annular ligament can be reconstructed using a strip of fascia lata passed around the radial neck.
- The graft is passed circumferentially around the radial neck and secured to the anterior and posterior margins of the sigmoid notch through drill holes.
- Tensioning must be precise: tight enough to prevent subluxation, but loose enough to permit full, unhindered pronation and supination.

Figure: Completed reconstruction of the annular ligament, restoring proximal radioulnar stability.
Management of Complex Elbow Fracture-Dislocations
In severe fracture-dislocations (e.g., the "terrible triad" of elbow dislocation, radial head fracture, and coronoid fracture), assessing the integrity of the DRUJ is critical. Large periarticular fractures adversely affect functional results.
If soft-tissue structures (collateral ligaments, anterior capsule) are repaired concurrently with bone fixation, the return of function is hastened, the final range of motion is improved, and the potential for heterotopic ossification (myositis ossificans) is significantly reduced.
THE DISTAL RADIOULNAR JOINT (DRUJ)
The chief function of the DRUJ is to stabilize the forearm during pronation and supination as the radius rotates around the fixed distal ulna. The distal ulna is completely covered by cartilage and articulates with the ulnar notch of the radius, except on its ulnar aspect.
Stabilizing Structures of the DRUJ
For the DRUJ to dislocate, significant disruption of the following stabilizing structures must occur:
1. The Triangular Fibrocartilage Complex (TFCC): The primary stabilizer, consisting of the articular disc attached to the base of the ulnar styloid and the margin of the ulnar notch of the radius.
2. Radioulnar Ligaments: The volar (anterior) and dorsal (posterior) radioulnar ligaments, which are integral thickenings of the joint capsule.
3. Ulnar Collateral Ligament (UCL): Attaches the tip of the ulnar styloid to the pisiform and triquetrum.
4. Pronator Quadratus: Spans the volar surface of the distal radius and ulna, providing dynamic stabilization.
Clinical Pearl: According to Milch, rupture of the distal radioulnar ligaments usually causes diastasis of the DRUJ. This separation, visible on standard PA radiographs, is a pathognomonic sign of ligamentous rupture.
Classification and Closed Management of DRUJ Dislocations
An injury to the DRUJ can occur in association with almost any forearm fracture (e.g., Galeazzi fracture) or as an isolated injury. Dislocation is classified by the position of the ulna relative to the radius.
- Dorsal Dislocation of the Ulna: The most common variant. Reduction is usually accomplished by forceful supination of the forearm combined with direct volar pressure on the distal ulna.
- Volar Dislocation of the Ulna: Less common. Reduction is typically achieved by pronation of the forearm with dorsal pressure on the ulna.
Figure: Ulnar dorsal dislocation. The dislocation is maintained by the pull of the pronator quadratus muscle, which prevents overlapping of the bones.
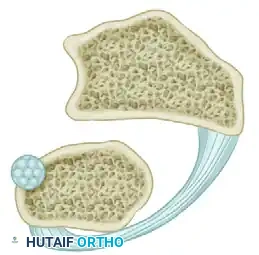
Figure: Ulnar volar dislocation. The pull of the pronator quadratus muscle produces overlapping of the distal radius and ulna.
If reduced early and immobilized for 4 weeks in a long-arm cast (in supination for dorsal dislocations, and pronation for volar dislocations), an excellent result can usually be expected.
Indications for Open Reduction of the DRUJ
Failure to recognize a simple DRUJ dislocation associated with a forearm fracture results in inadequate immobilization. Consequently, the TFCC fails to heal, leading to recurrent postoperative instability.
Open reduction is strictly indicated in the following scenarios:
1. Irreducible Acute Dislocation: Often caused by the entrapment of the extensor carpi ulnaris (ECU) tendon, the TFCC, or fracture fragments within the sigmoid notch.
2. Subacute Instability (< 2 months old): Where closed reduction cannot be maintained, necessitating open repair of the TFCC and transosseous pinning.
3. Chronic Instability (> 2 months old): Ligaments rarely heal well after 6 to 8 weeks. Degenerative changes in the articular surfaces may become so severe that restoring normal anatomy is undesirable. In these cases, salvage procedures (e.g., Darrach procedure or Sauvé-Kapandji procedure) or complex ligament reconstructions are required.
Surgical Pitfall: Operations to reconstruct permanently damaged ligaments of the DRUJ cannot be successful unless the component bones (radius and ulna) are undeformed. Malunions of the radius must be corrected via osteotomy prior to any soft-tissue reconstruction.
SURGICAL TECHNIQUES FOR DRUJ STABILIZATION
Because operations to stabilize the DRUJ are technically demanding and indicated only when conservative measures or primary repairs fail, several reconstructive techniques have been developed. The Bunnell and Liebolt techniques are classic, highly effective methods for restoring DRUJ stability using tendon grafts.
The Bunnell Technique
The Bunnell technique utilizes a tendon graft (often a split portion of the flexor carpi ulnaris or a free palmaris longus graft) to create a stabilizing loop, effectively reconstructing the radioulnar ligaments.
Step 1: Surgical Approach
* A dorsal longitudinal incision is made over the DRUJ, allowing access to both the radius and the ulna.
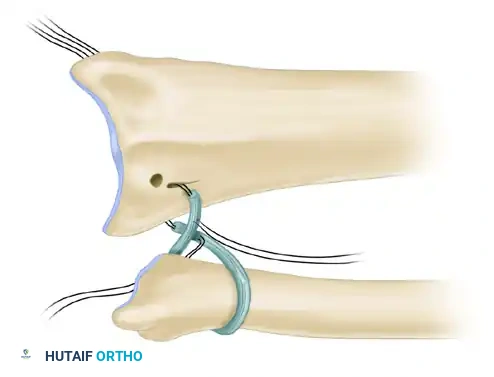
Figure: Skin incision for the Bunnell technique to stabilize the distal radioulnar joint.
Step 2: Graft Placement and Looping
* A small tendon graft is harvested.
* The graft is looped circumferentially around the neck of the ulna to act as a neo-ligament.
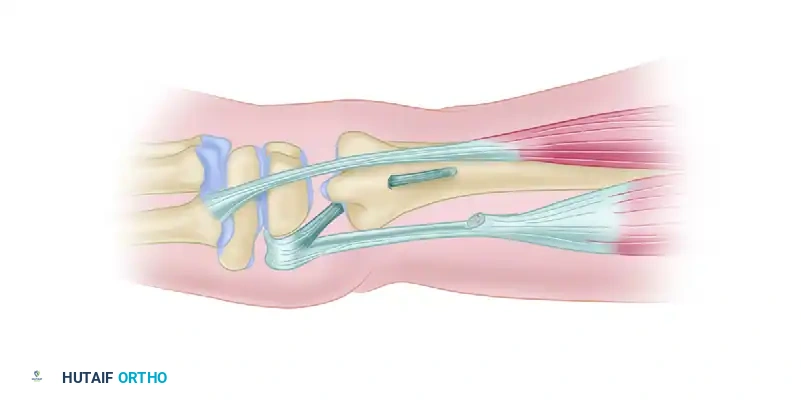
Figure: An annular ligament is formed by looping the small tendon graft around the neck of the ulna and preparing it for attachment to the radius.
Step 3: Radial Attachment
* Drill holes are created in the ulnar aspect of the distal radius.
* The free ends of the tendon graft are passed through the radius to secure the ulnar loop, effectively tethering the ulna to the sigmoid notch.

Figure: Cross-section of the wrist demonstrating the method of attaching the tendon graft through the radius.
Step 4: Ulnar Tenodesis
* To prevent proximal migration and provide additional longitudinal stability, a tenodesis of the distal end of the ulna is performed using a split portion of the flexor carpi ulnaris (FCU) tendon.
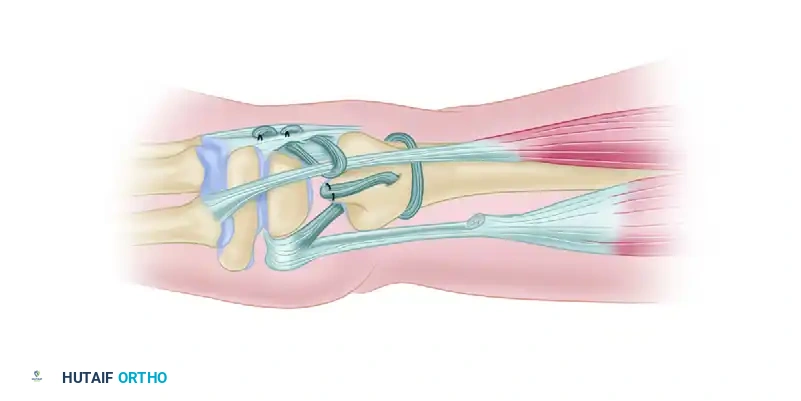
Figure: Tenodesis of the distal end of the ulna using a split portion of the flexor carpi ulnaris tendon.

Figure: Detailed view of the ulnar tenodesis securing the distal ulna.
Step 5: ECU Stabilization
* In chronic instability, the ECU tendon often subluxates volarly during wrist flexion and pronation.
* The ECU is anchored dorsally using a separate tendon loop or extensor retinaculum flap to maintain its position as a dynamic DRUJ stabilizer.
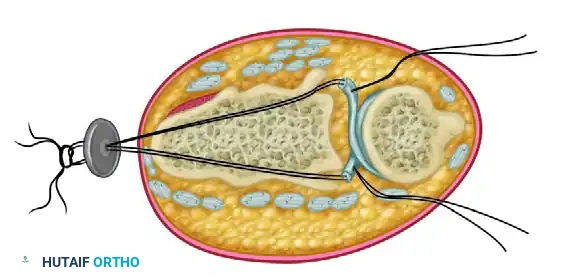
Figure: Final appearance after anchoring the extensor carpi ulnaris tendon dorsally by a separate tendon loop to prevent subluxation.
The Liebolt Technique
The Liebolt technique is an alternative reconstructive method that relies on precise transosseous routing of a tendon graft (or fascia lata) to recreate the volar and dorsal radioulnar ligaments simultaneously.
Step 1: Osseous Preparation
* Following exposure of the DRUJ, specific drill holes are created in both the distal radius and the distal ulna.
* Two holes are drilled in the radius (dorsal and volar to the sigmoid notch) and two corresponding holes are drilled in the ulnar neck.
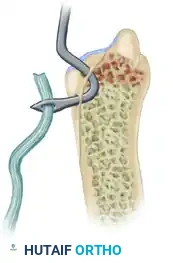
Figure: Location of the transosseous holes drilled in the distal radius and ulna for the Liebolt technique.
Step 2: Tendon Routing
* A robust graft (such as fascia lata or a free tendon) is passed in a figure-of-eight or box configuration through the drill holes.
* This routing mimics the anatomic vectors of the native dorsal and volar radioulnar ligaments.
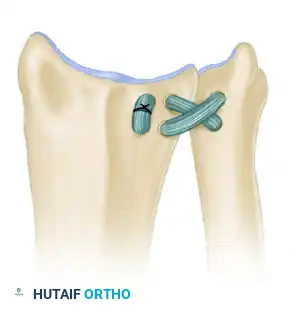
Figure: Method of passing the tendon graft through the radius and ulna to recreate the radioulnar ligaments.
Step 3: Tensioning and Fixation
* The joint is reduced and held in neutral rotation.
* The graft is tensioned and sutured to itself. The stability of the DRUJ is tested through a full range of pronation and supination before final closure.
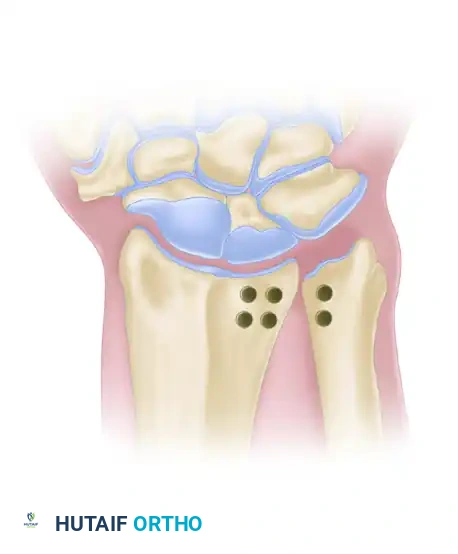
Figure: Final appearance after the joint has been stabilized using the Liebolt technique.
POSTOPERATIVE REHABILITATION PROTOCOL
The success of both radial head and DRUJ open reductions relies heavily on strict adherence to postoperative rehabilitation protocols.
Phase I: Maximum Protection (Weeks 0-4)
- Immobilization: The arm is placed in a well-molded long-arm splint or cast.
- For isolated radial head repairs: Immobilize in 90 degrees of elbow flexion and neutral forearm rotation.
- For DRUJ dorsal dislocations: Immobilize in supination.
- For DRUJ volar dislocations: Immobilize in pronation.
- Edema Control: Strict elevation and digital range of motion (ROM) exercises are initiated immediately to prevent hand stiffness.
Phase II: Controlled Mobilization (Weeks 4-8)
- Orthotics: Transition to a custom hinged elbow brace (for proximal injuries) or a Muenster/sugar-tong splint (for DRUJ injuries).
- ROM Exercises: Initiate active and active-assisted ROM.
- Avoid passive stretching, which can stretch out the newly reconstructed ligaments.
- Pronation and supination are introduced gradually, avoiding the extremes of rotation that stress the specific repair.
Phase III: Strengthening and Return to Function (Weeks 8-12+)
- Strengthening: Begin isometric exercises, progressing to isotonic strengthening of the forearm musculature (especially the pronator quadratus and ECU, which act as dynamic stabilizers).
- Return to Activity: Heavy lifting and high-impact sports are restricted until at least 4 to 6 months postoperatively, pending clinical stability and radiographic evidence of joint congruency.
CONCLUSION
Dislocations of the radial head and the distal radioulnar joint represent severe disruptions of the forearm's biomechanical ring. While acute, simple dislocations may respond to closed reduction and precise immobilization, complex fracture-dislocations, irreducible joints, and chronic instability demand expert surgical intervention.
By mastering the anatomic repair of the annular ligament and employing advanced reconstructive procedures like the Bunnell and Liebolt techniques for the DRUJ, the orthopedic surgeon can restore forearm kinematics, alleviate pain, and prevent the rapid onset of debilitating osteoarthrosis. Meticulous surgical technique, combined with a rigid, evidence-based postoperative rehabilitation protocol, is the cornerstone of achieving excellent long-term functional outcomes in these challenging clinical scenarios.
📚 Medical References
- radial head dislocation in children, part 1: pathologic changes preventing stable reduction and surgical correction, J Pediatr Orthop 22:583, 2002.
- Kim HT, Park BG, Suh JT, et al: Chronic radial head dislocation in children, part 2: results of open treatment and factors affecting fi nal outcome, J Pediatr Orthop 22:591, 2002.
- Lancaster S, Horowitz M: Lateral idiopathic subluxation of the radial head: case report, Clin Orthop Relat Res 214:170, 1987.
- Luke DL, Schoenecker PL, Gilula LA: Imaging rounds 100: congenital dislocation of the radial head, Orthop Rev 18:911, 1989.
- Menio GJ, Wenner SM: Radial head dislocations in children with below-elbow defi ciencies, J Hand Surg 17A:891, 1992.
- Miura T: Congenital dislocation of the radial head, J Bone Joint Surg 72B:477, 1990.
- Mizuno K, Usui Y, Kohyama K, et al: Familial congenital unilateral anterior dislocation of the radial head: differentiation from traumatic dislocation by means of arthrography: a case report, J Bone Joint Surg 73A:1086, 1991.
- Woo CC: Traumatic radial head subluxation in young children: a case report and literature review, J Manip Physiol Ther 10:191, 1987.
You Might Also Like