Mastering Open Reduction and Internal Fixation of Noncomminuted Proximal Interphalangeal Joint Fracture-Dislocations

Key Takeaway
Open reduction and internal fixation of noncomminuted proximal interphalangeal (PIP) joint fracture-dislocations is indicated when the volar lip fragment comprises at least 50% of the articular surface. Utilizing a midlateral approach, the fragment is anatomically reduced and secured with Kirschner wires. Precise restoration of the articular congruity and volar plate integrity is paramount to restoring joint stability and preventing chronic subluxation.
Introduction to Proximal Interphalangeal Joint Fracture-Dislocations
The proximal interphalangeal (PIP) joint is the critical functional hinge of the digit, responsible for the majority of finger flexion and overall grip strength. Fracture-dislocations of the PIP joint present a formidable challenge to the orthopedic surgeon. These injuries typically involve an axial load combined with hyperextension, resulting in a volar lip fracture of the middle phalanx base and subsequent dorsal subluxation or dislocation of the remaining middle phalanx.
Understanding the biomechanics of this injury is paramount. The proper collateral ligaments and the volar plate insert onto the volar base of the middle phalanx. When a fracture involves 50% or more of the articular surface, the collateral ligaments remain attached to the fractured volar fragment. Consequently, the remaining dorsal portion of the middle phalanx is stripped of its primary ligamentous stabilizers, leading to profound dorsal instability. In these scenarios, closed reduction is invariably unstable, and surgical intervention is mandated to restore articular congruity and joint kinematics.
The following comprehensive guide details the operative technique for the open reduction and internal fixation (ORIF) of noncomminuted PIP joint fracture-dislocations, alongside adjunctive management strategies for complex or chronic presentations.
Indications and Preoperative Planning
Surgical Indications
The specific technique of open reduction and Kirschner wire (K-wire) fixation is strictly indicated under the following parameters:
* Noncomminuted Fracture Pattern: The volar fragment must be a single, solid piece. Highly comminuted fractures (pilon-type) require alternative techniques such as dynamic external fixation, volar plate arthroplasty, or hemi-hamate autograft reconstruction.
* Fragment Size: The osseous fragment must be large enough—comprising at least 50% of the articular surface—to safely accommodate and hold a K-wire without iatrogenic fragmentation.
* Dorsal Instability: Inability to maintain concentric joint reduction in less than 30 degrees of flexion.
💡 Clinical Pearl: The "V" Sign
On a true lateral radiograph, dorsal subluxation of the middle phalanx creates a dorsal opening of the PIP joint space, known as the "V" sign. The presence of this sign indicates a lack of concentric reduction and is an absolute indication for surgical intervention if it cannot be corrected with closed extension-block splinting.
Radiographic Evaluation
Standard posteroanterior (PA), true lateral, and oblique radiographs are mandatory. The true lateral view is the most critical for assessing the percentage of articular surface involvement and the degree of dorsal subluxation.


Figure 67-52 (A-C): Anterior, lateral, and oblique radiographic views of a markedly comminuted and unstable PIP joint fracture-dislocation in a 15-year-old softball player. Note the severe dorsal subluxation and loss of articular congruity.
Surgical Anatomy and the Midlateral Approach
The midlateral approach provides excellent exposure to the collateral ligaments, volar plate, and the articular surface of the PIP joint while safely avoiding the volar neurovascular bundles.
- Incision Placement: The incision is placed along the midaxial line of the digit, connecting the apices of the flexion creases when the finger is fully flexed. It extends from the mid-portion of the proximal phalanx to the mid-portion of the middle phalanx.
- Neurovascular Protection: The neurovascular bundle lies volar to the midaxial line. By staying strictly midlateral and dissecting dorsal to Cleland's ligaments, the bundle is protected and falls volarly with the skin flap.
- Retinacular System: The transverse retinacular ligament runs vertically from the volar fascia to the lateral band. This must be divided to access the joint capsule.
Step-by-Step Surgical Technique: Open Reduction of Noncomminuted Fractures
1. Exposure and Soft Tissue Dissection
- Incision: Make a precise midlateral incision centered over the PIP joint.
- Deep Dissection: Identify and divide the transverse retinacular ligament parallel to the lateral band. Retract the lateral band dorsally and the neurovascular bundle volarly. This exposes the collateral ligament and the joint capsule.
- Ligamentous Release: Detach the accessory collateral ligament at its distal insertion on the middle phalanx. This critical step allows the surgeon to reflect the ligament dorsally and exposes the fibrocartilaginous volar plate and the fracture site.
2. Fragment Mobilization
- Identification: Locate the avulsed volar osseous fragment.
- Periosteal Preservation: Crucial Step: Preserve the soft tissue and periosteal attachments to the volar fragment (specifically the volar plate insertion). Stripping these attachments will devascularize the fragment, leading to avascular necrosis and subsequent collapse of the articular surface.
- Joint Debridement: Irrigate the joint to remove hematoma and small osteochondral debris that may block anatomical reduction.
3. Anatomical Reduction and Fixation
- Reduction: Using a dental pick or a small freer elevator, gently manipulate the fragment into its anatomical bed. Ensure perfect articular congruity under direct visualization.
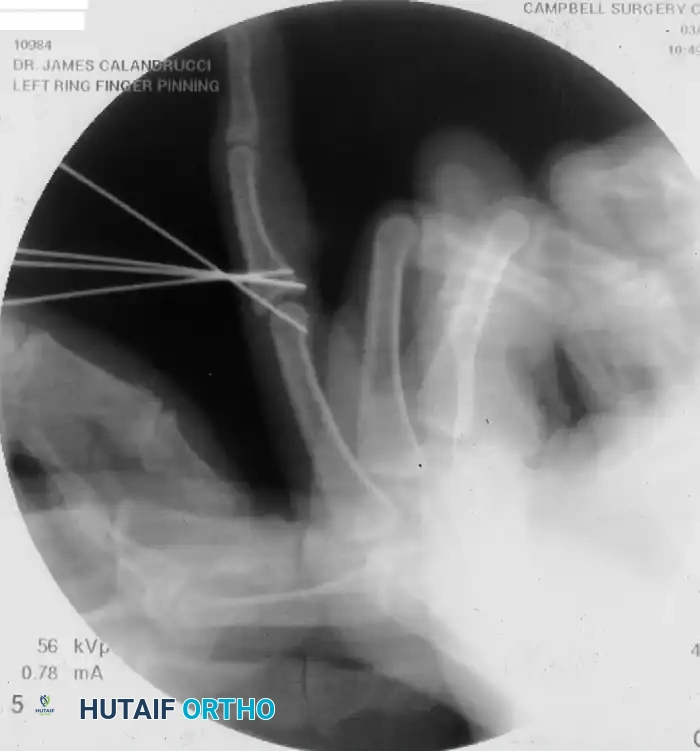
- Primary Fixation: Fix the fragment in position using a small Kirschner wire (typically 0.028-inch or 0.035-inch).
- Trajectory: Insert the K-wire in a dorsal direction (from volar-distal to dorsal-proximal).
- Subchondral Burial: Draw the wire dorsally until its volar end lies just beneath the articular surface of the fragment. It is imperative that the wire does not protrude into the joint space, as this would mechanically interfere with joint flexion and cause rapid chondrolysis.
- Wire Trimming: Cut the wire flush with the dorsal surface of the middle phalanx to prevent soft tissue irritation beneath the extensor mechanism.
4. Joint Stabilization
- Functional Positioning: Once the articular surface is reconstructed, reduce the PIP joint and place it in a functional position (approximately 20 to 30 degrees of flexion).
- Transarticular Pinning: Fix the joint in this position with a second, obliquely inserted K-wire crossing the PIP joint. This neutralizes shear forces across the newly fixed fracture during the early healing phase.
5. Closure
- Capsuloligamentous Repair: Meticulously suture the accessory collateral ligament back to its insertion. Repair the transverse retinacular ligament to prevent dorsal subluxation of the lateral band (which could lead to a swan-neck deformity).
- Skin Closure: Close the skin with non-absorbable monofilament sutures.
⚠️ Surgical Warning: Volar Approach Pitfalls
While a volar approach (using a Brunner zigzag incision) can be utilized for direct visualization of the volar plate, it carries a higher risk of postoperative stiffness and flexor tendon adhesions.
Figure 67-52 (D, E): In this 15-year-old patient, reduction was obtained through a volar approach. However, persistent joint enlargement and limited motion resulted despite a subsequent dorsal capsulectomy and aggressive physical therapy, highlighting the high risk of stiffness associated with extensive volar dissection.

Management of Chronic or Neglected Fracture-Dislocations
When a PIP joint fracture-dislocation presents late (1 month old or older), the surgical complexity increases exponentially due to soft tissue contracture, fracture consolidation in a malreduced position, and cartilage degradation.
Osteotomy and Bone Grafting
- Mobilization: The contracted collateral ligaments and volar plate must be released. If necessary for the reduction of the chronic dislocation, both collateral ligaments can be detached from their proximal origins.
- Osteotomy: An osteotomy is performed through the malunion site to free the small volar fragment.
- Defect Management: Freeing the fragment often leaves a significant osseous defect due to bone resorption. This defect must be filled with structural autograft.
- Graft Harvest: Bone graft is typically harvested from the proximal ulna (olecranon) or the volar side of the proximal phalanx. The graft is contoured to match the defect and supports the articular fragment, which is then pinned as described in the acute setting.
Alternative and Adjunctive Techniques
While the primary text focuses on noncomminuted fractures, the orthopedic surgeon must be prepared to utilize alternative techniques when intraoperative findings reveal severe comminution or crush injuries.
Dynamic External Fixation for Crush Injuries
In cases of severe fragmentation where internal fixation is impossible, dynamic external fixation (such as the Suzuki frame) is the treatment of choice. This utilizes the principle of ligamentotaxis to maintain joint space and alignment while allowing early active motion.


Figure 67-53 (A, B): Severe crush injury resulting in fragmentation of the middle phalanx base and a concomitant bony mallet finger.




Figure 67-53 (C-F): Application of an external fixation frame composed of 0.045-inch Kirschner wires and portions of a disposable neurotip tube (acting as a dynamic rubber band system). Early motion is possible because the axis pin passes precisely through the center of rotation of the proximal phalanx head.


Figure 67-53 (G, H): Excellent clinical result and restoration of functional flexion/extension 10 weeks after surgery utilizing the dynamic external fixator.
Extension-Block Splinting
For fractures that are stable in flexion but subluxate in extension, or as a step-down therapy following pin removal, extension-block splinting is highly effective.


Figure 67-54: Extension-block splinting technique. The splint is fabricated to block PIP joint extension at the exact angle where concentric reduction is maintained, while allowing full active flexion to prevent tendon adhesions and joint stiffness.
Postoperative Care and Rehabilitation Protocol
The postoperative management of PIP joint ORIF requires a delicate balance between protecting the fragile osteosynthesis and preventing debilitating joint stiffness.
Phase I: Immobilization (Weeks 0-3)
- Splinting: Immediately postoperatively, a protective dorsal blocking splint is applied. The PIP joint is immobilized in the functional position dictated by the transarticular K-wire.
- Edema Control: Strict elevation and compressive dressings are utilized to minimize digital swelling, which is a primary contributor to secondary stiffness.
- Uninvolved Joints: Active range of motion (ROM) of the metacarpophalangeal (MCP) and distal interphalangeal (DIP) joints is encouraged immediately to prevent extensor mechanism tethering.
Phase II: Pin Removal and Early Motion (Week 3)
- Hardware Removal: At exactly 3 weeks postoperatively, the transarticular Kirschner wire is removed in the clinic. The intra-osseous wire holding the fragment is left buried.
- Initiation of Motion: Active and active-assisted PIP joint motion is begun slowly.
- Protective Splinting: An extension-block splint or buddy taping is utilized between exercise sessions to protect against sudden hyperextension forces.
Phase III: Strengthening and Maturation (Weeks 6-12)
- Radiographic Check: Radiographs are obtained at 6 weeks to confirm clinical union of the volar fragment.
- Dynamic Splinting: If a flexion contracture develops, dynamic extension splinting may be initiated cautiously at 6 to 8 weeks, provided the fracture is solidly healed.
- Strengthening: Grip and pinch strengthening exercises are introduced. Maximum medical improvement may take up to 6 to 12 months, and patients must be counseled that some permanent loss of terminal extension or mild joint enlargement is common despite optimal surgical management.
💡 Clinical Pearl: Managing Expectations
The PIP joint is notoriously unforgiving. Even with perfect anatomical reduction and rigid fixation, patients frequently experience residual stiffness and soft tissue thickening. Preoperative counseling regarding the necessity of rigorous, prolonged hand therapy is just as critical as the surgical execution itself.
You Might Also Like


