Open Reduction and Internal Fixation of Proximal Humeral Fractures: A Comprehensive Surgical Masterclass

Key Takeaway
Open reduction and internal fixation (ORIF) of proximal humeral fractures requires meticulous surgical technique, anatomic reduction of the tuberosities, and stable fixation to prevent varus collapse. This comprehensive guide details patient positioning, the deltopectoral approach, advanced reduction strategies using traction sutures, and biomechanically optimized locking plate application to ensure optimal functional outcomes in complex three- and four-part fracture patterns.
Comprehensive Introduction and Patho-Epidemiology
Proximal humeral fractures represent approximately 5% to 6% of all adult fractures, making them the third most common fracture pattern in patients over the age of 65, following proximal femur and distal radius fractures. The epidemiological profile of these injuries demonstrates a classic bimodal distribution. In younger cohorts, these fractures are typically the result of high-energy trauma, such as motor vehicle collisions or falls from a significant height, often presenting with severe comminution, soft tissue compromise, and concomitant injuries. Conversely, in the elderly demographic, they predominantly manifest as low-energy fragility fractures secondary to osteoporotic bone microarchitecture following a simple fall from a standing height. As the global population continues to age, the incidence of these osteoporotic fractures is projected to rise exponentially, presenting a escalating challenge to orthopedic trauma systems worldwide.
The pathophysiology of proximal humeral fracture displacement is dictated by the predictable biomechanical pull of the surrounding musculature on the discrete fracture fragments, a concept originally codified by Charles Neer in his seminal four-part classification system. Neer defined a "part" not merely by the presence of a fracture line, but by clinically significant displacement—specifically, greater than 1 centimeter of translation or more than 45 degrees of angulation. The four potential segments include the articular segment (humeral head), the greater tuberosity, the lesser tuberosity, and the humeral shaft. Understanding the pathoanatomy of these specific segments is paramount, as the deforming forces dictate the required reduction maneuvers.
Historically, the management of displaced proximal humeral fractures was fraught with high rates of complication. Conservative management often resulted in symptomatic malunion and debilitating stiffness, while early attempts at operative intervention utilizing conventional, non-locking plates were plagued by catastrophic hardware failure, screw pullout, and varus collapse, particularly in osteopenic bone. The advent of anatomically contoured, fixed-angle locking plate technology (such as the Proximal Humeral Interlocking System, or PHILOS) revolutionized the operative paradigm. By acting as an internal fixator rather than relying on friction between the plate and bone, locking plates provide superior stability in poor-quality bone.
Despite these technological advancements, the primary goal of Open Reduction and Internal Fixation (ORIF) remains fundamentally biological and mechanical. The surgeon must meticulously restore the anatomic relationship of the articular surface to optimize glenohumeral kinematics, reconstruct the tuberosities to re-establish the critical rotator cuff force couples, and provide a construct stable enough to permit early, controlled range of motion. Successful outcomes are heavily reliant on meticulous surgical technique, preservation of the fragile vascular supply, and rigid restoration of the medial calcar hinge to prevent mechanical failure.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the complex osteology, myology, and vascularity of the proximal humerus is the foundation of successful surgical intervention. The proximal humerus consists of the articular head, which sits at a retroversion angle of approximately 20 to 30 degrees relative to the transepicondylar axis of the distal humerus, and a neck-shaft angle of approximately 130 to 135 degrees. The anatomical neck separates the articular surface from the tuberosities, while the surgical neck lies distal to the tuberosities, representing the weakest structural point and the most common site of fracture. The bicipital groove (intertubercular sulcus) serves as a critical anatomical landmark separating the greater and lesser tuberosities, housing the long head of the biceps tendon and the ascending branch of the anterior humeral circumflex artery.
The deforming muscular forces acting on the proximal humerus must be anticipated and neutralized during reduction. The greater tuberosity serves as the insertion site for the supraspinatus, infraspinatus, and teres minor; thus, when fractured, it is predictably displaced superiorly and posteriorly. The lesser tuberosity, serving as the insertion for the subscapularis, is forcefully retracted medially and internally rotated when fractured. The humeral shaft is subjected to the powerful medial and anterior pull of the pectoralis major, latissimus dorsi, and teres major, while the deltoid exerts a superior migratory force. Overcoming these opposing forces requires strategic patient positioning, pharmacological paralysis, and the judicious use of traction sutures and mechanical levers.
The vascular anatomy of the proximal humerus is arguably the most critical factor in predicting fracture healing and the risk of avascular necrosis (AVN). Historically, the anterior humeral circumflex artery (AHCA), specifically its anterolateral ascending branch (the arcuate artery of Laing), was considered the primary blood supply to the humeral head. However, modern quantitative perfusion studies have demonstrated that the posterior humeral circumflex artery (PHCA) provides the dominant arterial contribution to the articular segment. Hertel’s seminal research identified specific radiographic predictors of ischemia, noting that the risk of AVN approaches 97% when a fracture exhibits a disrupted medial hinge, a short metaphyseal head extension (calcar length less than 8 mm), and an anatomical neck fracture pattern. Preservation of soft tissue attachments, particularly the posteromedial periosteum, is vital during surgical exposure.
Biomechanically, the proximal humerus is subjected to immense shear and bending forces, particularly during shoulder abduction. Fixed-angle locking plates mitigate these forces by creating a rigid construct where the screws lock directly into the plate, preventing toggle and subsequent screw pullout. However, the most critical biomechanical concept in proximal humeral ORIF is the restoration of the medial column. If the medial cortex (calcar) is comminuted or left unreduced, the locking plate is subjected to massive varus cantilever bending forces. This inevitably leads to construct failure, typically manifesting as the proximal screws cutting out through the superior articular surface. The insertion of inferomedial calcar screws into the dense subchondral bone of the inferior humeral head provides a mechanical buttress, effectively neutralizing these varus forces and significantly increasing the load-to-failure of the construct.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a proximal humeral fracture is highly nuanced, requiring a complex calculus that balances fracture morphology with patient-specific physiological factors. The primary objective is to maximize functional recovery while minimizing the risk of iatrogenic complications. Non-operative management remains the gold standard for minimally displaced fractures (accounting for approximately 80% of all proximal humeral fractures), where the inherent stability of the soft tissue envelope allows for early rehabilitation and predictable healing.
Absolute indications for surgical intervention are relatively rare but definitive. They include open fractures requiring immediate irrigation and debridement, fractures associated with an acute vascular injury (such as axillary artery disruption) necessitating repair, and fractures with an irreducible glenohumeral dislocation. Polytrauma patients also represent a strong indication for early fixation to facilitate nursing care, mobilization, and pulmonary toilet. Additionally, fractures presenting with progressive neurological deficits, particularly involving the brachial plexus, may warrant exploration and stabilization.
Relative indications encompass the majority of operative cases and revolve around the degree of displacement and the anticipated functional deficit if left untreated. Displaced two-part surgical neck fractures with significant angulation or translation that fail closed reduction are prime candidates for ORIF. Displaced three-part and four-part fractures in physiologically young, active patients are strongly considered for ORIF to restore the rotator cuff footprint and glenohumeral kinematics. Isolated greater tuberosity fractures displaced by more than 5 mm (or even 3 mm in elite athletes) represent a specific indication for intervention, as superior migration will inevitably lead to severe subacromial impingement, blocking forward elevation and abduction.
Contraindications to ORIF must be rigorously respected to avoid catastrophic failures. Severe osteoporosis, where the bone stock is insufficient to hold even locked screws, is a primary contraindication; in these scenarios, particularly with complex three- or four-part fractures in elderly patients, a Reverse Total Shoulder Arthroplasty (RTSA) is the preferred alternative. Medically unstable patients who cannot tolerate general anesthesia or the physiological stress of surgery should be managed conservatively. Furthermore, patients with severe pre-existing cognitive impairment (e.g., advanced dementia) or psychiatric conditions that preclude compliance with the strict postoperative rehabilitation protocols are poor candidates for internal fixation, as premature weight-bearing or aggressive mobilization will reliably result in hardware failure.
| Category | Indications for ORIF | Contraindications for ORIF |
|---|---|---|
| Absolute | Open fractures; Concomitant vascular injury; Irreducible fracture-dislocation | Active surgical site infection; Medically unfit for anesthesia (ASA IV/V) |
| Relative | Displaced 2-part, 3-part, and select 4-part fractures; GT displacement >5mm; Polytrauma | Severe osteoporosis (favor RTSA); Head-split fractures >20% articular surface (favor RTSA) |
| Patient Factors | Physiologically young; High functional demand; Compliant with rehabilitation | Advanced dementia; Non-compliance; Pre-existing severe rotator cuff arthropathy |
| Anatomical | Intact medial calcar hinge; Adequate bone stock for screw purchase | Complete disruption of medial hinge with severe comminution in elderly |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful proximal humeral fracture fixation. The evaluation begins with a high-quality trauma radiographic series, which must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. The axillary view is absolutely non-negotiable, as it is the only reliable method to definitively rule out an associated anterior or posterior glenohumeral dislocation, evaluate the degree of lesser tuberosity displacement, and assess the articular version. If the patient is in too much pain to abduct the arm for a standard axillary view, a Velpeau axillary view can be obtained with the patient remaining in the sling.
For all complex fracture patterns—specifically three-part, four-part, head-split, and highly comminuted surgical neck fractures—a non-contrast Computed Tomography (CT) scan with two-dimensional multiplanar reformats and three-dimensional surface rendering is highly recommended. The CT scan provides invaluable data regarding the spatial orientation of the tuberosities, the degree of articular surface impaction, and the precise length of the intact medial calcar segment. Digital preoperative templating should be performed to estimate plate length, anticipate the trajectory of the inferomedial calcar screws, and identify potential zones of poor bone density. The surgeon must mentally rehearse the reduction sequence, deciding whether the tuberosities will be reduced to the head first, or the head to the shaft.
Patient positioning in the operating theater must optimize both surgical access and unhindered fluoroscopic visualization. The modified beach chair position is the standard of care. The patient is placed on a radiolucent table with the torso elevated to approximately 30 to 40 degrees. This semi-upright posture offers several distinct advantages: it reduces venous pressure at the surgical site, thereby minimizing intraoperative hemorrhage; it allows gravity to assist in longitudinal traction of the arm; and it provides excellent access to the superior and anterior aspects of the shoulder. Careful attention must be paid to securing the head in a neutral position to avoid cervical spine hyperextension or lateral flexion, which can cause devastating brachial plexus traction injuries.
The fluoroscopy setup must be established and verified prior to the commencement of the surgical prep. The C-arm is typically positioned on the contralateral side of the table, entering perpendicular to the patient. The monitor must be placed at the foot of the bed or directly across from the surgeon to ensure an ergonomic line of sight. The surgeon must confirm that perfect AP and axillary/lateral views can be obtained without obstruction from the table base or patient positioning devices. The operative arm is then prepped and draped entirely free, utilizing a sterile U-drape and impervious stockinette, allowing for unrestricted manipulation, traction, and rotation of the limb during the reduction maneuvers.
Step-by-Step Surgical Approach and Fixation Technique
The Deltopectoral Approach (Primary Approach)
The deltopectoral approach remains the versatile workhorse for the vast majority of proximal humeral fracture fixations. It offers extensile exposure to the anterior humerus, lesser tuberosity, and glenohumeral joint without violating the deltoid muscle, thereby preserving its function.
The incision begins just lateral to the tip of the coracoid process and extends distally and slightly laterally toward the insertion of the deltoid on the humeral shaft. The superficial dissection identifies the cephalic vein, the critical landmark demarcating the internervous plane between the deltoid (innervated by the axillary nerve) and the pectoralis major (innervated by the medial and lateral pectoral nerves). The cephalic vein is generally retracted laterally with the deltoid to preserve its primary venous drainage, though medial retraction is acceptable if the lateral tributary branches are excessively tethered.
Deep dissection involves retracting the conjoined tendon (short head of the biceps and coracobrachialis) medially. To achieve adequate visualization of the inferior surgical neck and proximal shaft, the superior 1 to 2 centimeters of the pectoralis major insertion may be released. The clavipectoral fascia is incised lateral to the conjoined tendon, exposing the underlying subscapularis and the fracture site. The long head of the biceps tendon is identified within the bicipital groove; this is a vital landmark, as the rotator interval lies immediately superior to it, separating the greater and lesser tuberosities.
Alternative: The Anterolateral Deltoid-Splitting Approach
For specific fracture morphologies—such as isolated greater tuberosity fractures, valgus-impacted proximal humerus fractures, or when utilizing minimally invasive lateral plating systems or intramedullary nails—the anterolateral deltoid-splitting approach is highly advantageous. It provides direct, orthogonal access to the lateral aspect of the greater tuberosity.
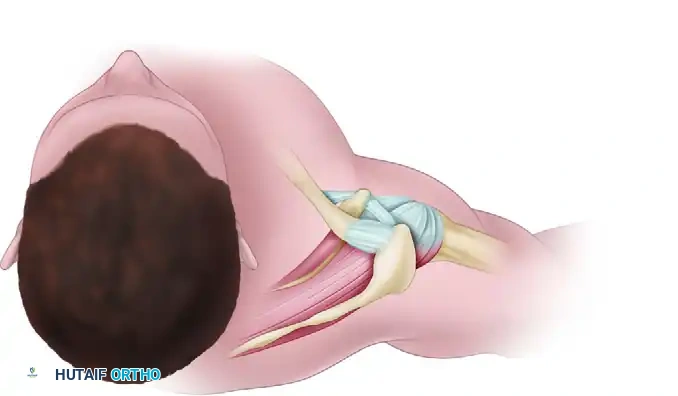
Figure A: Diagrammatic representation of the anterolateral approach. A diagonal incision from the anterolateral corner of the acromion splits the deltoid in line with its fibers in the raphe between the anterior and middle thirds.
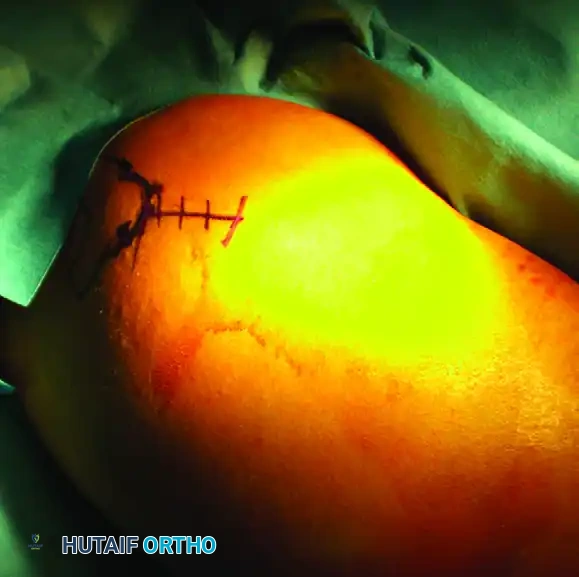
Figure B: Clinical photograph demonstrating the precise location of the anterolateral incision marked on the skin, centered over the greater tuberosity.
The incision is centered over the lateral edge of the acromion, extending distally for approximately 4 to 5 centimeters. The deltoid fascia is incised, and the muscle fibers are split bluntly along the natural raphe separating the anterior and middle heads of the deltoid.
Figure C: Establishment of the surgical portal. Deep retractors are placed to expose the lateral aspect of the proximal humerus while carefully protecting the axillary nerve, which crosses the field approximately 5 to 7 cm distal to the lateral acromial edge.
The paramount concern during this approach is the protection of the axillary nerve, which courses transversely across the deep surface of the deltoid, approximately 5 to 7 centimeters distal to the lateral edge of the acromion. A stay suture or a specifically designed self-retaining retractor must be placed at the distal apex of the split to prevent inadvertent distal propagation of the dissection and subsequent iatrogenic nerve palsy.
Fracture Reduction Techniques
Achieving an anatomic, or near-anatomic, reduction prior to plate application is the most critical determinant of success. The locking plate is an internal fixator; it will rigidly hold the bone in whatever position it is placed, meaning it will perfectly maintain a malreduction.
For the articular segment, if the head is angulated or rotated, a 2.5 mm or 3.0 mm threaded Schanz pin is inserted percutaneously into the lateral or posterior aspect of the humeral head. This pin acts as a powerful "joystick," allowing the surgeon to elevate, disimpact, and derotate the head segment back into its anatomic position relative to the shaft. Once reduced, the head is provisionally pinned to the intact shaft using 2.0 mm Kirschner wires (K-wires) driven from lateral to medial.
Management of the tuberosities in three- and four-part fractures requires the placement of heavy, non-absorbable traction sutures (e.g., #2 or #5 ultra-high-molecular-weight polyethylene sutures like FiberWire). These are passed through the tendon-bone interface of the supraspinatus, infraspinatus, and subscapularis. These sutures serve as vital traction handles, allowing the surgeon to pull the displaced tuberosities out of the subacromial space or glenohumeral joint and reduce them around the articular segment.
Internal Fixation and Plate Application
Once provisional reduction is achieved and verified via orthogonal fluoroscopy, the anatomically contoured locking plate is introduced. Plate positioning is exact: the superior edge of the plate must sit 5 to 8 millimeters distal to the superior tip of the greater tuberosity to avoid subacromial impingement during shoulder abduction. Anteroposteriorly, the plate must be positioned 2 to 4 millimeters posterior to the bicipital groove. Placing the plate too anteriorly risks violating the bicipital groove and causing iatrogenic injury to the ascending branch of the anterior humeral circumflex artery.
The screw insertion sequence typically begins proximally. Two locking screws are placed through the proximal holes into the humeral head, ensuring subchondral placement (within 5 mm of the articular cartilage) without joint penetration. Next, a non-locking cortical screw is placed in the elongated dynamic hole in the humeral shaft; this allows the plate to be drawn down tightly to the bone, correcting any minor lateral translation.
The most critical step in the fixation sequence is the placement of the inferomedial calcar screws. These screws must be directed into the dense bone of the inferior quadrant of the humeral head. They act as a structural buttress, resisting the varus bending moments that predictably lead to construct failure. Finally, the previously placed heavy rotator cuff traction sutures are passed through the dedicated suture holes in the proximal plate and tied securely. This incorporates the rotator cuff into the construct, creating a tension-band effect that neutralizes the deforming pull of the muscles and dramatically increases the overall stability of the repair.
Radiographic Confirmation and Closure
Prior to closure, a rigorous and exhaustive fluoroscopic examination is mandatory. The AP view must confirm a restored neck-shaft angle of approximately 130 degrees and verify that the plate is positioned adequately distal to the tuberosity tip. The axillary view confirms the concentric reduction of the tuberosities and ensures no screws are violating the anterior or posterior glenohumeral joint. Finally, the surgeon must perform a "live fluoroscopy" check, taking the shoulder through a full, gentle range of motion while visualizing the joint space to definitively rule out intra-articular screw penetration.
The wound is irrigated copiously. The deltopectoral interval is allowed to fall together and is closed loosely to prevent hematoma formation. The subcutaneous tissues are reapproximated, and the skin is closed with a subcuticular suture or staples. Depending on the extent of dead space and intraoperative hemostasis, a closed suction drain may be placed deep to the fascia for 24 hours.
Complications, Incidence Rates, and Salvage Management
Despite meticulous preoperative planning and precise surgical execution, the operative management of complex proximal humeral fractures carries a substantial risk of complications. The learning curve associated with locked plating technology is steep, and complications are most frequently associated with technical errors, unrecognized poor bone quality, or severe initial fracture displacement.
The most common mechanical complication is varus collapse with secondary screw cutout, occurring in up to 10% to 15% of cases. This catastrophic failure is driven by cantilever bending forces overwhelming the construct. It is almost exclusively the result of a failure to restore the medial cortical hinge or a failure to place adequate inferomedial calcar screws. When varus collapse occurs, the rigid proximal locking screws inevitably penetrate the superior articular cartilage, leading to severe pain, glenoid destruction, and profound functional loss. Salvage management typically requires hardware removal and, in older patients, conversion to a Reverse Total Shoulder Arthroplasty (RTSA).
Avascular Necrosis (AVN) of the humeral head is a devastating biological complication, with incidence rates ranging from 4% in simple two-part fractures to over 30% in complex four-part fractures. The risk is directly correlated with the initial disruption of the vascular supply (PHCA and AHCA) and the severity of the trauma. Interestingly, not all radiographic AVN is clinically symptomatic. If the articular surface remains congruent, patients may be managed conservatively. However, if subchondral collapse and secondary osteoarthritis develop, symptomatic patients will require arthroplasty.
Adhesive capsulitis (postoperative stiffness) is the most ubiquitous complication, affecting nearly all patients to some degree. The proximity of the surgical dissection to the joint capsule, combined with postoperative immobilization, predictably leads to fibrosis. Management is primarily preventative, emphasizing early, controlled passive range of motion.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Varus Collapse / Screw Cutout | 10% - 15% | Failure to restore medial hinge; Lack of calcar screws; Severe osteoporosis | Hardware removal; Revision ORIF with bone grafting; Conversion to RTSA |
| Avascular Necrosis (AVN) | 4% - 35% (varies by fracture complexity) | Disruption of PHCA/AHCA; Short calcar (<8mm); Disrupted medial hinge | Observation if asymptomatic; Hemiarthroplasty or RTSA if subchondral collapse occurs |
| Adhesive Capsulitis (Stiffness) | 20% - 40% | Prolonged immobilization; Inadequate rehabilitation; Capsular scarring | Aggressive physical therapy; Manipulation under anesthesia (MUA); Arthroscopic capsular release |
| Infection (Deep) | 1% - 3% | Prolonged operative time; Diabetes; Immunosuppression; Hematoma | Aggressive I&D; Intravenous antibiotics; Hardware removal once union is achieved |
| Axillary Nerve Palsy | 1% - 5% | Iatrogenic traction during deltopectoral approach; Direct injury in lateral approach | Observation and EMG at 3 months; Nerve exploration/grafting if no recovery |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional success of a proximal humeral fracture ORIF is as dependent on the postoperative rehabilitation program as it is on the surgical execution. The rehabilitation protocol represents a delicate, continuous balance between protecting the fragile osteosynthesis construct (particularly the tuberosity repairs) and preventing the onset of debilitating adhesive capsulitis. Protocols must be highly individualized, taking into account the patient's bone quality, the rigidity of the fixation achieved intraoperatively, and the specific fracture pattern.
Phase I (Weeks 0 to 4) focuses on tissue protection and the initiation of early, safe motion. The patient is placed in a well-padded shoulder immobilizer or sling immediately postoperatively. An early rehabilitation program is initiated within the first 3 to 5 days, focusing exclusively on passive and active-assisted range-of-motion (ROM) exercises. Patients are instructed in classic Codman's pendulum exercises, allowing gravity to gently distract the joint. Passive forward elevation in the scapular plane is permitted, typically utilizing a pulley system or therapist assistance. Crucially, external rotation is strictly limited (usually to neutral or a maximum of 30 degrees) to protect the lesser tuberosity and subscapularis repair from undue tension. Active elbow, wrist, and hand ROM are encouraged immediately to prevent distal edema.
Phase II (Weeks 4 to 8) marks the transition to active motion, coinciding with early radiographic evidence of soft callus formation and clinical stability. The sling is progressively discontinued, initially during the day and eventually at night. The patient advances to full active ROM exercises in all planes. Scapulothoracic mechanics become a primary focus during this phase; physical therapists work on periscapular stabilization to prevent compensatory shoulder shrugging, which can lead to subacromial impingement. Gentle isometric strengthening of the deltoid and rotator cuff may be initiated late in this phase, provided there is no pain at the fracture site.
Phase III (Weeks 8 to 12 and beyond) is the strengthening and functional restoration phase. Once definitive clinical and radiographic union is achieved (typically around 8 to 10 weeks), the patient begins a comprehensive isotonic strengthening program. This involves progressive resistance exercises utilizing elastic bands and light weights, focusing on the rotator cuff force couples and the deltoid. Patients must be counseled that maximal functional recovery following a complex proximal humeral fracture ORIF is a protracted process, often taking 12 to 18 months. Return to heavy manual labor, high-impact sports, or overhead athletic activities is strictly prohibited until at least 4 to 6 months postoperatively, and only after demonstrating symmetric strength and full, pain-free range of motion.
Summary of Landmark Literature and Clinical Guidelines
The management of proximal humeral fractures has been the subject of intense academic debate and rigorous clinical investigation over the past two decades. A thorough understanding of the landmark literature is essential for evidence-based surgical decision-making.
The most widely discussed and debated study in recent history is the PROFHER (PROximal Fracture of the Humerus: Evaluation by Randomisation) trial, published in 2015. This pragmatic, multicenter randomized controlled trial compared surgical intervention (ORIF or arthroplasty) with non-operative management for displaced surgical neck fractures in adults. The study concluded that there was no statistically significant difference in clinical outcomes (Oxford Shoulder Score) or quality of life between the surgical and non-surgical groups at two years follow-up. While provocative, the PROFHER trial has faced significant criticism within the orthopedic community regarding its inclusion criteria, the heterogeneity of surgical techniques utilized, and the lack of standardization in rehabilitation protocols. Consequently, while it highlights that many displaced fractures can do well without surgery, it has not eliminated the role of ORIF in appropriately selected patients.
Conversely, extensive biomechanical and clinical literature supports the superiority of fixed-angle locking plates over conventional plating systems, particularly in osteoporotic bone. Studies by Egol et al. and others have consistently demonstrated that locking plates provide significantly higher load-to-failure rates and better maintenance of reduction in cyclic loading models. Furthermore, the clinical
