Open Reduction and Internal Fixation of Bennett Fractures
Key Takeaway
Open reduction and internal fixation of a Bennett fracture is indicated when closed reduction fails to achieve an articular step-off of less than 1 to 2 millimeters. Utilizing the Wagner approach, surgeons can directly visualize the first carpometacarpal joint, anatomically reduce the volar ulnar fragment, and secure it using Kirschner wires or small-fragment screws. Precise restoration of articular congruity is paramount to preventing post-traumatic osteoarthritis and preserving thumb biomechanics.
INTRODUCTION AND BIOMECHANICS
The Bennett fracture is a classic intra-articular fracture-subluxation involving the base of the first metacarpal. First described by Edward Hallaran Bennett in 1882, this injury is characterized by the avulsion of the volar ulnar aspect of the metacarpal base. Understanding the deforming forces at play is critical for achieving and maintaining an anatomic reduction.
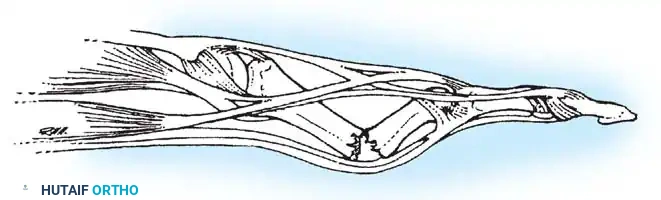
The small volar ulnar fragment remains anatomically secured to the trapezium by the robust anterior oblique ligament (AOL), maintaining its position within the carpometacarpal (CMC) joint. Conversely, the larger metacarpal shaft fragment is subjected to powerful, uninhibited muscular forces. The abductor pollicis longus (APL) exerts a strong proximal, dorsal, and radial pull on the metacarpal base, while the adductor pollicis pulls the metacarpal head toward the palm, resulting in a supination and adduction deformity of the thumb ray.
Because of these persistent deforming forces, closed reduction and cast immobilization are frequently insufficient to maintain articular congruity. When conservative measures fail, or when the articular step-off exceeds acceptable parameters, open reduction and internal fixation (ORIF) becomes the gold standard of treatment to prevent early-onset post-traumatic osteoarthritis.
INDICATIONS FOR OPEN REDUCTION
The primary goal in the management of a Bennett fracture is the restoration of a congruent CMC joint and the stabilization of the first metacarpal shaft to allow for early rehabilitation. Open reduction is strictly indicated under the following circumstances:
- Failure of Closed Reduction: Inability to achieve or maintain an articular step-off of less than 1 to 2 mm via closed reduction and percutaneous pinning.
- Large Articular Fragment: When the volar ulnar fragment constitutes more than 20% to 25% of the articular surface, making percutaneous capture technically difficult and mechanically unstable.
- Displacement: Articular displacement or gap greater than 2 mm.
- Delayed Presentation: Fractures presenting several weeks post-injury where early callus formation prevents closed manipulation.
- Polytrauma or Open Fractures: Cases requiring immediate rigid stabilization to facilitate comprehensive hand rehabilitation or soft tissue management.
💡 Clinical Pearl
Do not rely solely on standard anteroposterior (AP) and lateral radiographs of the hand. A true AP of the thumb (Robert's view) and a true lateral of the first CMC joint are mandatory to accurately assess the size of the volar ulnar fragment and the degree of articular step-off.
SURGICAL ANATOMY AND PREOPERATIVE PLANNING
Thorough knowledge of the dorsoradial anatomy of the thumb is essential to safely execute the surgical approach. The superficial radial nerve (SRN) and the lateral antebrachial cutaneous nerve (LABC) arborize over the first CMC joint. Iatrogenic injury to these sensory branches can result in debilitating neuromas.
The first dorsal compartment, housing the APL and extensor pollicis brevis (EPB), lies directly over the surgical field. The radial artery courses dorsally through the anatomic snuffbox, crossing the scaphoid and trapezium just proximal to the CMC joint. Preoperative planning should include a careful assessment of the fragment size to determine the optimal fixation strategy—either multiple Kirschner wires (K-wires) or small-fragment lag screws (2.0 mm or 2.7 mm).
PATIENT POSITIONING AND PREPARATION
- Positioning: The patient is placed in the supine position with the affected upper extremity extended on a radiolucent hand table.
- Anesthesia: Regional anesthesia (supraclavicular or axillary brachial plexus block) is preferred, though general anesthesia may be utilized based on patient factors.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage to ensure a bloodless surgical field.
- Equipment: A mini-C-arm fluoroscopy unit must be positioned to allow unimpeded orthogonal views of the thumb CMC joint throughout the procedure.
SURGICAL APPROACH: THE WAGNER INCISION
The Wagner approach provides excellent, direct visualization of the first CMC joint and the base of the first metacarpal, facilitating precise anatomic reduction.
- Incision: Begin a curved incision on the dorsoradial aspect of the first metacarpal shaft. Extend the incision proximally, curving it volarward at the level of the wrist crease.
- Superficial Dissection: Carefully bluntly dissect through the subcutaneous tissues. It is imperative to identify, mobilize, and meticulously protect the sensory branches of the superficial radial nerve crossing this area. Retract these branches gently using vessel loops.
- Deep Dissection: Identify the interval between the APL/EPB tendons and the thenar musculature.
- Exposure of the Metacarpal: To expose the fracture, partially strip the soft tissue and periosteum from the proximal end of the metacarpal shaft. Elevate the thenar muscles (opponens pollicis and abductor pollicis brevis) subperiosteally and retract them volarward.
- Capsulotomy: Incise the carpometacarpal joint capsule longitudinally or via a T-shaped incision to expose the articular surface and the fracture hematoma.
⚠️ Surgical Warning
Avoid excessive stripping of the volar ulnar fragment. The anterior oblique ligament attaches to this fragment and provides its sole blood supply. Overzealous dissection can lead to avascular necrosis of the fragment.
SURGICAL TECHNIQUE: OPEN REDUCTION AND INTERNAL FIXATION
Joint Exposure and Debridement
Once the CMC joint is opened, irrigate the joint space to clear the fracture hematoma. Use a dental pick or a small curette to gently remove any interposed soft tissue or small, non-viable osteochondral debris from the fracture site. Inspect the articular surface of the trapezium for any concomitant chondral injury.
Fracture Reduction Maneuvers
Reduction of the Bennett fracture requires reversing the deforming forces.
1. Apply longitudinal traction to the thumb ray.
2. Pronate the thumb to correct the supination deformity.
3. Apply palmar abduction and direct pressure over the dorsal base of the first metacarpal to push the shaft fragment volarly and ulnarly, reducing it to the captive volar ulnar fragment.
4. Align the articular surface of the larger metacarpal shaft fragment with that of the smaller volar ulnar fragment under direct vision.
Kirschner Wire Fixation
Once anatomic reduction is achieved and visually confirmed, provisional fixation is required.
- Under direct vision, drill a small-caliber K-wire (typically 0.035-inch or 0.045-inch) across the joint fracture site to maintain the reduction.
- Crucial Step: Often, fixation by a single wire is insecure and acts only as an axis of rotation. Additional wires must be added to the provisional, smaller-caliber K-wires to achieve rotational stability and rigid fixation.
- These wires can be driven from the metacarpal shaft into the volar ulnar fragment, or, if the fragment is too small, the wires can be driven across the CMC joint into the trapezium to neutralize the deforming forces of the APL.
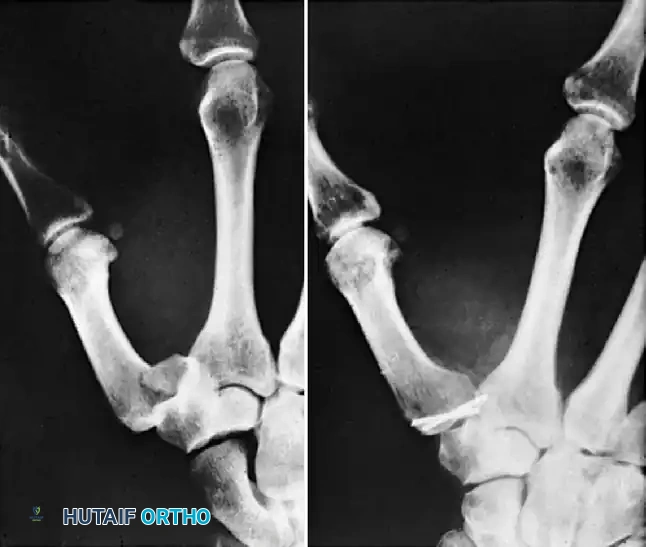
FIGURE 67-12: Comminuted Bennett fracture treated by open reduction. Two Kirschner wires were necessary to keep articular fragments reduced. Note the parallel placement to ensure rotational control.
Screw Fixation Alternative
As an alternative to K-wire fixation, rigid internal fixation can be achieved with a 2.0-mm or 2.7-mm lag screw. This technique is highly dependent on the size of the volar ulnar fragment.
- The volar ulnar fragment must be at least three times the diameter of the screw to prevent iatrogenic comminution during drilling and tapping.
- Use a reduction forceps with pointed tines to hold the reduction.
- Drill a gliding hole in the near cortex (metacarpal shaft) and a thread hole in the far cortex (volar ulnar fragment).
- Countersink the near cortex to prevent the screw head from causing soft tissue irritation or stress risers.
- Insert the appropriate length screw, achieving interfragmentary compression.
- Confirm the reduction and hardware placement with fluoroscopy in multiple planes.
POSTOPERATIVE CARE AND REHABILITATION
Meticulous postoperative care is essential to ensure union while preventing stiffness.
- Immediate Postoperative Phase: After closing the wound in layers, apply a bulky, sterile dressing and a well-molded thumb spica forearm cast or rigid splint.
- Wound Inspection: The cast is removed for wound inspection and suture removal at 2 to 3 weeks.
- Immobilization Duration: Following the wound check, the cast is replaced and worn continuously until 4 weeks after surgery.
- Hardware Removal: If K-wires were used and left protruding through the skin, they are typically removed in the clinic at 4 to 6 weeks, provided there is radiographic evidence of early clinical union. However, immobilization in a thermoplastic splint may be necessary for 2 to 4 more weeks depending on the stability of the fracture.
- Accelerated Protocol for Screw Fixation: If rigid screw fixation is used, the rehabilitation timeline can be accelerated. Active range of motion (AROM) of the CMC joint and intermittent splinting can be initiated at 10 to 14 days in a compliant patient with sure, rigid fixation.
COMPLICATIONS AND MANAGEMENT
Post-Traumatic Arthritis
The most significant complication following a Bennett fracture is malunion with persistent subluxation. Even a 1 to 2 mm articular step-off alters the contact stresses across the CMC joint exponentially. This incongruity inevitably progresses to painful carpometacarpal joint osteoarthritis.
🚨 Surgical Pitfall
Reduction of a Bennett fracture should not be attempted after 6 weeks. By this time, significant remodeling, soft tissue contracture, and early degenerative changes have occurred. Forcible reduction attempts will likely result in iatrogenic cartilage damage and joint stiffness.
Management of Malunion: Corrective Osteotomy
For a malunion that is recognized early—before frank degenerative changes are noted on radiographs—a corrective osteotomy is indicated to restore joint congruity and biomechanics. Giachino described a highly effective technique for corrective osteotomy of a malunited Bennett fracture.
The Giachino Corrective Osteotomy Technique:
- Osteotomy Planning: The malunited metacarpal base is exposed via the Wagner approach. The site of the previous fracture is identified. An osteotomy cut is planned to separate the malunited shaft from the volar ulnar fragment.
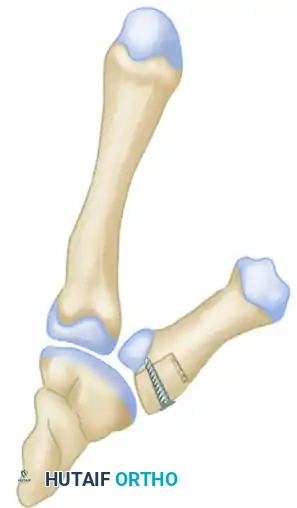
Surgical Diagram A: Identification of the malunion and the planned trajectory for the corrective osteotomy cut to mobilize the metacarpal shaft.
- Restoring Alignment and Length: Once the osteotomy is performed, the metacarpal shaft is mobilized. Because the shaft has typically shortened and adducted due to chronic muscle pull, it must be distracted and realigned. A structural bone graft (often harvested from the distal radius or iliac crest) is fashioned into a block and inserted into the osteotomy gap. This graft restores the anatomic length of the metacarpal and corrects the articular alignment.
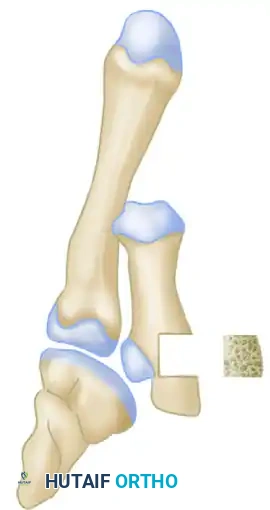
Surgical Diagram B: Distraction of the osteotomy site and insertion of a precisely contoured structural bone graft block to restore metacarpal length and articular congruity.
- Rigid Fixation: The newly reconstructed metacarpal base, incorporating the structural bone graft, must be rigidly fixed to allow for graft incorporation and early mobilization. A lag screw is passed through the metacarpal shaft, through the bone graft block, and into the volar ulnar fragment, compressing the entire construct.

Surgical Diagram C: Final construct demonstrating rigid internal fixation with a lag screw compressing the metacarpal shaft, the interpositional bone graft, and the articular fragment.
Late-Stage Degenerative Arthritis
When a malunion is neglected and advanced degenerative arthritis has already developed, joint-preserving osteotomies are no longer viable. In these late-stage scenarios, salvage procedures are advised. Depending on the patient's age, functional demands, and manual labor requirements, the surgeon should proceed with either a first CMC joint arthrodesis (providing a stable, pain-free, but stiff joint for heavy laborers) or a trapeziectomy with ligament reconstruction and tendon interposition (LRTI) arthroplasty (providing excellent pain relief and mobility for lower-demand patients).
You Might Also Like