Comprehensive Introduction and Patho-Epidemiology
Onychocryptosis, universally recognized in clinical parlance as an ingrown toenail, represents a pervasive and frequently debilitating orthopedic and podiatric pathology. It is characterized by the painful, traumatic impingement of the lateral or medial margins of the nail plate into the adjacent periungual soft tissues, specifically the nail fold or ungual labia. This mechanical conflict incites a robust foreign-body inflammatory cascade, leading to localized erythema, profound edema, and the eventual proliferation of highly vascularized, friable hypergranulation tissue. While often dismissed as a minor ailment by the lay public, chronic onychocryptosis can result in significant functional impairment, altered gait mechanics, and severe secondary bacterial infections, particularly in patients with compromised vascular or immunologic profiles.

The epidemiological profile of onychocryptosis demonstrates a bimodal distribution, with a pronounced peak during adolescence and early adulthood, and a secondary peak in the geriatric population. In the adolescent cohort, the etiology is largely multifactorial, driven by rapid growth spurts, hyperhidrosis, participation in high-impact athletic activities, and the ubiquitous use of constricting, narrow-toe-box footwear. Furthermore, improper nail trimming techniques—specifically the aggressive rounding of the distal nail corners—exacerbate the condition by allowing the advancing nail edge to penetrate the lateral nail fold during the forward growth phase. In the geriatric population, the pathophysiology is more frequently associated with dystrophic nail changes, such as onychogryphosis or onychomycosis, compounded by peripheral edema and diminished manual dexterity, which precludes proper podiatric hygiene.
From a patho-anatomical perspective, the condition is most accurately classified using the Mozena or Heifitz staging systems, which dictate the therapeutic algorithm. Stage I is characterized by localized erythema, mild edema, and pain with direct pressure, without purulent drainage. Stage II involves the exacerbation of these symptoms with the addition of active infection and seropurulent exudate. Stage III is defined by chronic inflammation, the formation of exuberant hypergranulation tissue that hypertrophies over the nail plate, and profound lateral nail fold hypertrophy. While conservative measures—such as warm water hydrotherapy, proper nail trimming, footwear modification, and cotton-wick elevation—may be efficacious for Stage I disease, they are universally inadequate for Stage II and Stage III presentations.
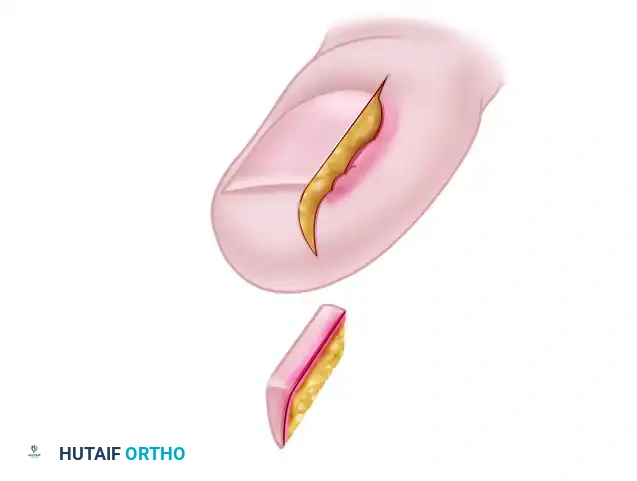
When conservative modalities are exhausted or clinically inappropriate, surgical intervention becomes the definitive standard of care. Nail fold removal or reduction procedures are explicitly designed to definitively resolve the mechanical conflict between the offending nail plate and the hypertrophic nail fold. These procedures consist of either the en bloc resection of the nail fold alongside a marginal border of normal tissue, or the precise resection of a soft-tissue wedge, the lateral nail plate, and the underlying matrix. While novice surgeons may initially gravitate toward chemical matrixectomies (e.g., phenol or sodium hydroxide application), excisional techniques offer superior biomechanical correction of the hypertrophic ungual labia and remain a highly acceptable, definitive treatment modality when executed with meticulous surgical precision. Preoperative patient counseling is paramount; the patient must explicitly understand the anatomical goals of the procedure, the expected postoperative aesthetic, and the inherent, albeit low, risk of recurrent nail spicules.
Detailed Surgical Anatomy and Biomechanics
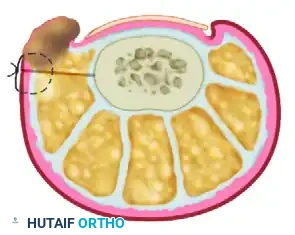
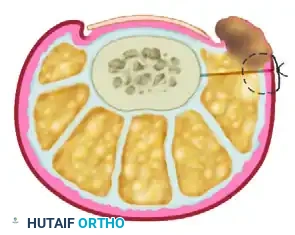
A profound, three-dimensional understanding of the perionychium and its surrounding osseous and neurovascular structures is absolute prerequisite for the orthopedic surgeon attempting to achieve successful, recurrence-free surgical outcomes. The perionychium represents a complex, highly specialized anatomical unit comprising the nail bed (further subdivided into the sterile matrix and germinal matrix) and the surrounding paronychium, which includes the lateral nail folds, the eponychium (cuticle), and the hyponychium. The nail plate itself is a keratinized appendage that acts as a rigid biomechanical counter-force to the plantar soft tissues during the toe-off phase of the gait cycle.
The germinal matrix is the paramount anatomical structure of concern during operative management. Located proximally, it extends from an area several millimeters proximal to the eponychium distally to the lunula—the visible, crescent-shaped whitish opacity at the base of the nail. The germinal matrix is responsible for generating approximately 90% of the nail plate's cellular volume via gradient parakeratosis. The lateral extents of the germinal matrix, known as the lateral horns, curve deeply and proximally around the base of the distal phalanx. Failure to completely identify, expose, and excise this lateral horn during a wedge resection is the singular most common technical error leading to the recurrence of painful nail spicules.
Distal to the lunula lies the sterile matrix, which extends to the hyponychium. Unlike the germinal matrix, the sterile matrix contributes only marginally to the thickness of the nail plate; its primary biomechanical function is to provide a highly adherent bed for the advancing nail plate. The transition between the germinal and sterile matrices is clinically identifiable during bloodless field surgery by a distinct color demarcation: the germinal matrix presents with a pale, whitish hue, whereas the sterile matrix is markedly erythematous and highly vascular. The lateral nail fold represents the soft tissue boundary that borders the nail plate; in chronic onychocryptosis, this tissue undergoes severe inflammatory hypertrophy, physically enveloping the lateral margin of the nail plate and exacerbating the impingement.
The neurovascular supply to the hallux demands meticulous respect during surgical dissection. Arterial perfusion is supplied by the proper plantar digital arteries, which travel plantomedially and plantolaterally, eventually forming a rich anastomotic arcade within the distal pulp and subungual space. Innervation is provided primarily by the proper plantar digital nerves, with variable contribution to the dorsal aspect from the dorsal digital nerves. Surgical incisions, particularly the deep plantar-lateral excisions utilized in the Bartlett procedure, must be carefully planned and executed to avoid iatrogenic transection of the plantar digital nerve. Furthermore, the proximity of the nail matrix to the periosteum of the distal phalanx tuft must be recognized; aggressive deep dissection can easily breach the periosteum, creating a direct conduit for osteomyelitis in the presence of a chronically infected nail fold.
Exhaustive Indications and Contraindications
The decision to proceed with operative management of onychocryptosis must be predicated on a comprehensive clinical evaluation, balancing the severity of the local pathology against the patient's systemic physiologic status. Surgical intervention is generally indicated for patients presenting with Stage II or Stage III onychocryptosis, characterized by persistent pain, recurrent paronychia, hypergranulation tissue, and failure of conservative therapies. Furthermore, patients with recurrent Stage I disease who experience significant functional limitations or an inability to participate in athletic or occupational activities are excellent candidates for definitive surgical correction.
Conversely, absolute contraindications are primarily related to severe peripheral arterial disease (PAD) and profound vascular insufficiency. In patients with an Ankle-Brachial Index (ABI) of less than 0.5, or absent palpable pedal pulses combined with non-compressible vessels, any surgical insult to the digit carries an unacceptably high risk of ischemic necrosis, delayed wound healing, and subsequent gangrene leading to amputation. Relative contraindications include poorly controlled diabetes mellitus with an elevated Hemoglobin A1c, severe peripheral neuropathy, and active, spreading cellulitis. In the presence of acute ascending cellulitis or systemic signs of infection, surgical intervention should be delayed until the patient has been adequately treated with a course of culture-directed oral or intravenous antibiotics.
| Clinical Parameter | Indications for Surgical Intervention | Absolute/Relative Contraindications |
|---|---|---|
| Disease Severity | Stage II (Infection/Drainage), Stage III (Hypergranulation) | Stage I (responsive to conservative care) |
| Vascular Status | Normal perfusion, palpable pulses, ABI > 0.8 | Absolute: Severe PAD (ABI < 0.5), ischemic rest pain, gangrene |
| Neurologic Status | Intact protective sensation | Relative: Severe peripheral neuropathy (requires extreme caution) |
| Infectious State | Localized paronychia, localized abscess | Relative: Ascending cellulitis, systemic sepsis (treat medically first) |
| Patient History | Recurrent episodes, failed conservative management | Non-compliant patient, inability to follow post-op offloading protocols |
| Anatomical Factors | Severe lateral nail fold hypertrophy, pincer nail deformity | Concomitant untreated subungual exostosis (requires alternative approach) |
It is also critical to consider the specific surgical technique indicated for the patient's unique anatomical presentation. For instance, a patient with a relatively normal, flat nail plate but massive, hypertrophic ungual labia may benefit most from a soft-tissue reduction technique (such as the Persichetti or Bartlett procedure), which spares the nail matrix while debulking the offending soft tissue. Conversely, a patient with a severely incurvated "pincer" nail and a normal nail fold is better served by a Watson-Cheyne wedge resection or a complete matrixectomy. The surgeon must tailor the operative approach to the specific biomechanical derangement present in the individual digit.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative preparation is essential for minimizing intraoperative complications and optimizing functional outcomes. The clinical evaluation begins with a meticulous physical examination of the affected digit, assessing the extent of erythema, the presence of fluctuance, and the volume of hypergranulation tissue. The surgeon must carefully probe the lateral nail fold to determine the depth of nail plate penetration. In cases of chronic, recalcitrant onychocryptosis, or in patients with a history of recurrent trauma, orthogonal radiographs (Anteroposterior and Lateral views of the hallux) are mandatory to rule out underlying osseous pathology, such as a subungual exostosis, osteochondroma, or radiographic evidence of distal phalangeal osteomyelitis.
Microbiological evaluation is highly recommended in the presence of active, seropurulent drainage. While empirical antibiotic therapy is often initiated, collecting deep swab cultures or tissue cultures prior to surgical preparation allows for targeted antimicrobial therapy. Staphylococcus aureus remains the most frequently isolated pathogen; however, in diabetic, immunocompromised, or chronically macerated environments, polymicrobial infections involving Pseudomonas aeruginosa, Gram-negative enterics, and anaerobes are increasingly prevalent. Preoperative laboratory evaluation, including a complete blood count (CBC), basic metabolic panel (BMP), and Hemoglobin A1c, should be obtained in patients with systemic comorbidities.
Patient positioning and anesthesia are critical components of the preoperative workflow. The patient is placed in the supine position on the operating table. The affected foot and lower leg are prepped with a chlorhexidine or povidone-iodine solution and draped in a standard sterile fashion. Anesthesia is typically achieved via a digital block at the base of the hallux, utilizing a combination of 1% lidocaine and 0.5% bupivacaine to provide both rapid onset and prolonged postoperative analgesia. Historically, the use of epinephrine in digital blocks was strictly contraindicated due to the theoretical risk of digital ischemia; however, a robust body of modern orthopedic and dermatologic literature has definitively demonstrated that the judicious use of epinephrine (1:100,000 or 1:200,000) is safe in healthy patients without peripheral arterial disease, and it significantly aids in intraoperative hemostasis.
To ensure a pristine, bloodless surgical field—which is absolutely vital for identifying the subtle visual demarcation between the germinal and sterile matrices—a digital tourniquet is applied. This can be achieved using a sterile Penrose drain tightly wrapped and secured at the base of the digit with a hemostat, or via a commercial sterile digital ring tourniquet. The digit is exsanguinated by elevating the foot and milking the toe from distal to proximal prior to tourniquet inflation or tightening. The tourniquet time should be strictly monitored and recorded, generally not exceeding 30 to 45 minutes to prevent ischemic neuropraxia to the digital nerves.
Step-by-Step Surgical Approach and Fixation Technique
The operative management of onychocryptosis encompasses several well-described techniques, each tailored to address specific patho-anatomical variants of the disease. The following sections detail the three most prominent surgical approaches: the Watson-Cheyne wedge resection, the Persichetti soft tissue wedge resection, and the Bartlett nail fold removal procedure.
Surgical Technique 87-6: Wedge Resection of Nail, Nail Bed, and Nail Fold (Watson-Cheyne)
The Watson-Cheyne technique, historically modified by Burghard, O’Donoghue, and Mogensen, represents the gold standard for comprehensive wedge resection. This procedure definitively removes the offending lateral nail plate, the underlying sterile and germinal matrices, and the hypertrophic lateral nail fold en bloc.
- Nail Plate Elevation: The procedure commences with the elevation of the lateral one-fourth of the nail plate. A small, flat dissector, such as a Freer elevator or a specialized nail spatula, is introduced beneath the distal free edge of the nail. The instrument is carefully advanced proximally, separating the nail plate from the underlying sterile matrix. It is imperative that the dissector is advanced fully beneath the eponychium to release the proximal nail root completely.
- Nail Plate Resection: Once elevated, straight, heavy tissue scissors or an English anvil nail splitter are utilized to longitudinally divide the nail plate. The cut must be clean and extend entirely under the eponychium. The lateral portion of the nail plate is then grasped with a sturdy hemostat and extracted with a rolling motion toward the midline to avoid tearing the delicate matrix.
- Primary Incision: Utilizing a #15 scalpel blade, a linear incision is made parallel to the lateral nail fold. This incision begins approximately 1 cm proximal to the lunula (in the skin of the proximal nail fold) and extends distally to the hyponychium. This incision is carried sharply down through the dermis and subcutaneous tissue directly to the periosteum of the distal phalanx.
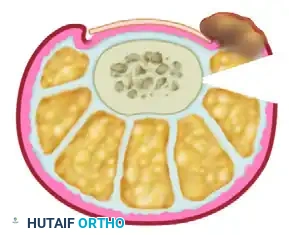
- Secondary Incision (Wedge Creation): A second incision is initiated 2 to 3 mm lateral to the inner edge of the lateral nail fold. This incision is curved obliquely at a 45-degree angle, directing the blade toward the depth of the initial incision. The goal is to encompass the hypertrophic soft tissue and intersect the first incision at the periosteal level, creating a three-dimensional wedge.
- Matrix Excision: The exposure and meticulous, complete excision of the proximal corner (the lateral horn) of the germinal matrix is the most critical technical step of the operation. The surgeon must utilize the bloodless field to identify the whitish hue of the germinal matrix, which contrasts sharply with the reddish, highly vascular sterile matrix.

- Deep Tissue Removal: The entire wedge—comprising the nail margin, the sterile matrix, the germinal matrix, and the hypertrophic nail fold—is excised en bloc. The surgeon must aggressively curette or sharply excise the tissue down to the periosteum in the proximal lateral corner. Exposing the underlying fat and subcutaneous tissue in this recess is necessary to definitively ensure the complete eradication of the germinal matrix.

- Closure and Dressing: Following copious irrigation, the tourniquet is released, and hemostasis is achieved via direct pressure or selective electrocautery. The resulting defect is typically left open to heal by secondary intention, though it may be loosely approximated with a single simple suture if tension allows. A nonadherent dressing (e.g., Adaptic, Xeroform, or a silver-impregnated mesh) is applied, followed by a bulky, sterile compression wrap.
Surgical Technique 87-7: Soft Tissue Wedge ResECTION (Persichetti et al. / Chapeskie)
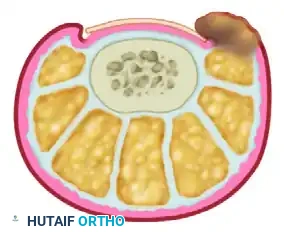
This technique operates on a fundamentally different biomechanical principle. Rather than excising the nail matrix, it focuses on reducing the soft tissue volume of the hypertrophic nail fold at a distance from the involved nail margin. By excising a laterally based wedge of skin and closing the defect, the hypertrophic nail fold is physically retracted and everted away from the lateral nail border.
- Incision Marking: Following standard prep and block, an ellipse of skin is meticulously marked on the lateral aspect of the digit. The medial border of this ellipse must begin exactly 4 mm lateral to the inflamed nail fold. Maintaining this 4 mm soft-tissue bridge is absolutely crucial to ensure the vascular viability of the remaining nail fold and prevent margin necrosis.

- Debridement: The offending lateral margin of the nail plate is removed to provide immediate mechanical decompression. Any associated hypergranulation tissue within the nail groove is aggressively debrided using a curette or scalpel.
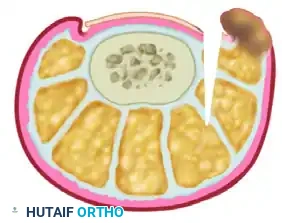
- Wedge Excision: The outlined wedge-shaped ellipse of skin and subcutaneous tissue is sharply excised. The apex of this wedge must extend deeply into the subcutaneous fat layer, often down to the lateral capsule of the interphalangeal joint or the periosteum, to ensure adequate mobilization of the lateral soft tissues.

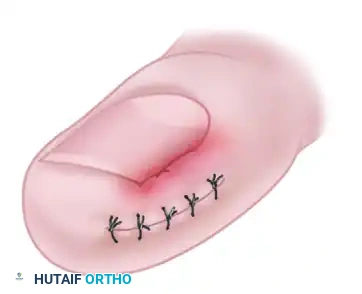
- Wound Approximation: The margins of the resulting elliptical defect are approximated using strong, nonabsorbable sutures (e.g., 3-0 or 4-0 nylon) in a simple interrupted or horizontal mattress fashion. As these sutures are tensioned and tied, the 4 mm bridge and the hypertrophic nail fold will visibly evert, significantly reducing its convexity and pulling it away from the nail plate.


- Suture Management: Because this closure relies on mechanical tension to remodel the soft tissue architecture, the sutures must remain in place longer than standard dermatologic closures. They are typically left intact for 10 to 15 days postoperatively to ensure the tissue heals securely in its new, everted position.
Surgical Technique 87-8: Nail Fold Removal (Bartlett Procedure)
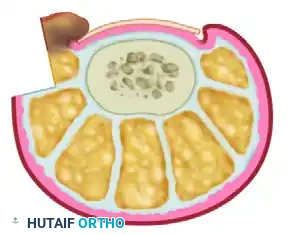
The Bartlett procedure is another highly effective soft-tissue reduction technique that entirely avoids direct trauma to the nail matrix. It relies on the excision of a substantial elliptical wedge of tissue from the plantar-lateral aspect of the toe to mechanically retract the nail fold downward and away from the nail plate.
- Incision Planning: The marking begins 4 to 5 mm from the lateral nail margin, situated near the midlateral line of the digit. The widest diameter of the planned elliptical excision should measure approximately 4 to 5 mm. It is a crucial requirement that this incision is placed entirely within normal, noninflamed, and noninfected tissue to ensure proper primary healing and robust suture retention.
- Depth of Dissection: The incision is carried deeply down to the bone, both dorsally and plantarward. During the execution of the plantar half of the elliptical incision, meticulous surgical dissection is required. The surgeon must be acutely aware of the anatomical course of the plantar digital nerve and artery to avoid iatrogenic transection.
- Wound Closure: The deep defect is closed using interrupted nonabsorbable sutures (e.g., 3-0 nylon). As the sutures are tightened, the mechanical force vectors will pull the hypertrophic nail fold inferiorly and laterally, effectively decompressing the impingement against the lateral nail margin.
- Adjunctive Resection: While matrixectomy is not the primary goal of the Bartlett procedure, the lateral 2 to 3 mm of the nail edge may be resected if necessary to provide immediate symptomatic relief. The wound is then dressed with a sterile, non-adherent compressive dressing.
Complications, Incidence Rates, and Salvage Management
While nail fold reduction and wedge resection procedures are highly successful and generally safe, complications can and do arise, primarily stemming from technical errors during the execution of the operation. A rigorous understanding of these potential pitfalls is essential for prompt recognition and effective salvage management.
The most frequent and frustrating complication is the recurrence of nail spicules. This occurs almost exclusively due to the incomplete excision of the proximal lateral horn of the germinal matrix during a Watson-Cheyne or similar wedge resection procedure. When a remnant of the germinal matrix is left behind, it continues to generate keratinized nail tissue. Because this tissue is trapped deep within the healing surgical site, it forms a sharp, aberrant spicule that pierces the newly healed lateral nail fold from the inside out, causing severe pain, recurrent inflammation, and foreign body granuloma formation.
Infection is another significant complication, particularly if the preoperative environment was heavily contaminated with hypergranulation tissue and seropurulent exudate, and adequate debridement was not achieved. Postoperative cellulitis can rapidly ascend the digit and foot, requiring aggressive intervention. Iatrogenic nerve injury, specifically to the proper plantar digital nerve during deep wedge excisions (such as the Bartlett procedure), can result in permanent numbness or the formation of a painful postoperative neuroma. Finally, epidermal inclusion cysts can develop if fragments of the sterile matrix or epidermis are driven deeply into the wound bed and buried during closure.
| Complication | Estimated Incidence | Etiology / Pathophysiology | Salvage Management / Treatment |
|---|---|---|---|
| Recurrent Nail Spicule | 5% - 15% | Retained lateral horn of the germinal matrix | Revision surgery: deep excision of the spicule and remnant matrix, or targeted phenolization. |
| Postoperative Infection | 2% - 5% | Inadequate debridement, retained necrotic tissue, poor hygiene | Oral broad-spectrum antibiotics (e.g., Cephalexin, Doxycycline), wound exploration if abscess forms. |
| Digital Nerve Neuroma | < 1% | Iatrogenic transection of the plantar digital nerve during deep wedge cuts | Conservative: offloading, gabapentin. Surgical: targeted neuroma excision and nerve end burying. |
| Epidermal Inclusion Cyst | 1% - 2% | Epidermal/matrix cells trapped in deep subcutaneous tissue during closure | Complete surgical excision of the cyst capsule to prevent recurrence. |
| Cosmetic Deformity | Variable | Over-resection of the nail plate resulting in a narrow, aesthetically displeasing nail | Preoperative counseling is key. No reliable surgical salvage once matrix is destroyed. |
Salvage management for recurrent spicules typically necessitates a return to the operating room for a revision procedure. The surgeon must meticulously
