First MTP Arthrodesis & Adolescent Hallux Valgus: Surgical Guide
Key Takeaway
The molded ball-and-socket arthrodesis of the first metatarsophalangeal joint provides robust fixation while allowing precise multiplanar alignment. Optimal positioning requires 15 degrees of valgus, 25 degrees of extension relative to the first metatarsal axis, and neutral rotation. Concurrently, managing juvenile and adolescent hallux valgus demands careful assessment of the distal metatarsal articular angle and physeal status to minimize the high risk of deformity recurrence.
MOLDED (BALL-AND-SOCKET) ARTHRODESIS OF THE FIRST METATARSOPHALANGEAL JOINT
The molded, or "ball-and-socket," arthrodesis of the first metatarsophalangeal (MTP) joint is a highly reliable, definitive procedure for end-stage hallux rigidus, severe hallux valgus, inflammatory arthropathies, and salvage of failed previous forefoot reconstructions. Unlike flat-cut arthrodesis techniques, the ball-and-socket configuration preserves the intrinsic length of the first ray and allows for infinite, multiplanar micro-adjustments in dorsiflexion, valgus, and rotation prior to definitive fixation.
Biomechanics and Preoperative Planning
The primary goal of first MTP arthrodesis is to provide a painless, stable medial column that effectively transfers load during the toe-off phase of the gait cycle. Precise positioning is the most critical determinant of a successful clinical outcome. Malpositioning can lead to transfer metatarsalgia, interphalangeal joint arthritis, and significant shoe-wear limitations.
Clinical Pearl: The ideal position for first MTP arthrodesis is 10 to 15 degrees of valgus, 25 degrees of extension (dorsiflexion) relative to the longitudinal axis of the first metatarsal, and neutral rotation. When referenced to the floor, the proximal phalanx should rest at approximately 10 to 15 degrees of dorsiflexion, allowing the pulp of the hallux to rest comfortably on the ground during weight-bearing.
Step-by-Step Surgical Technique
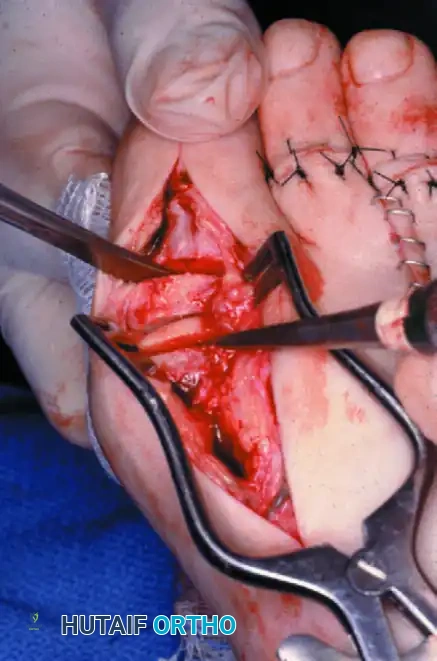
1. Surgical Approach and Exposure
* Initiate a midline medial incision extending from the midportion of the proximal phalanx to the junction of the neck and shaft of the first metatarsal.
* Carefully dissect through the subcutaneous tissues, taking care to identify and protect the dorsomedial cutaneous nerve.
* Raise the skin and joint capsule as a single, full-thickness flap both dorsally and plantarward. This subperiosteal dissection must be extensive enough to fully expose the articular surfaces of the metatarsal head and the base of the proximal phalanx, while preserving the vascularity of the capsular flaps for subsequent closure.
2. Joint Preparation (The Ball-and-Socket)
* Utilize a small rongeur to meticulously remove all remaining articular cartilage and subchondral bone from the metatarsal head. It is imperative to follow the natural convex contours of the metatarsal head to create the "ball."
* Prepare the base of the proximal phalanx by deepening its natural concave surface with a small rongeur, creating the corresponding "socket."
* If the subchondral bone at the base of the proximal phalanx is highly eburnated and sclerotic, utilize a small (1/8- to 1/4-inch) osteotome to "fish-scale" or shingle the surfaces. Follow this with a rongeur to penetrate the sclerotic plate and expose healthy, bleeding cancellous bone.
Surgical Warning: Do not over-resect the medial eminence during the initial preparation. It is critical to leave a bony "shoulder" where the medial eminence meets the metatarsal shaft. This ridge of bone acts as an essential buttress for the screw head during compression.
3. Subchondral Fenestration
* To maximize osteogenesis and fusion rates, drill multiple fenestration holes using a 0.062-inch Kirschner wire (K-wire) into both the prepared base of the proximal phalanx and the metatarsal head. This stimulates the release of marrow-derived osteoprogenitor cells.
4. Alignment and Provisional Fixation
* Manually align the joint surfaces into the optimal position: 15 degrees of valgus, 25 degrees of extension relative to the first metatarsal longitudinal axis, and neutral rotation.
* Impact the surfaces together to ensure maximal bony apposition.
* Provisionally hold the arthrodesis with two 0.062-inch K-wires driven from the metatarsal head into the proximal phalanx, directed from medial to lateral.
* Place the first K-wire dorsal to the midline. Place the second K-wire plantar to the midline, typically anchoring it in the flare of the plantar surface of the metatarsal head.
* Rigorously evaluate the final position using fluoroscopy and a simulated weight-bearing test (loading the foot with a flat plate). If any multiplanar adjustments are required, remove the K-wires, reposition the joint, and re-pin.
5. Definitive Internal Fixation
* Utilize a 2.0-mm drill bit through a tissue protection sleeve to drill a pilot hole from the medial aspect of the metatarsal head, directing it distally and laterally into the proximal phalanx.
* To achieve a true lag effect, over-ream the near cortex (the metatarsal side of the arthrodesis) using a 3.5-mm drill bit.
* Measure the appropriate screw length using a depth gauge, and tap the far cortex with a 4.0-mm cancellous tap.
* Crucial Step: Before inserting the screw, use a countersink on the medial metatarsal cortex. This allows the head of the screw to rest flush inside the cortex without levering distally, which could catastrophically fracture the cortical bridge.
* Insert a fully threaded, 4.0-mm cancellous screw to compress the arthrodesis site. The previously preserved medial eminence shoulder will buttress the screw head.
* Assess stability. The single lag screw often provides sufficient compression and rigid fixation to allow removal of the provisional K-wires. However, if rotational instability persists, one or both K-wires may be left in place, cut flush beneath the skin, to augment fixation.
Postoperative Care Protocol
- Phase 1 (0-3 Weeks): The patient is placed in a removable short-leg walking boot and allowed to bear weight to tolerance on the heel and lateral border of the foot. The initial surgical dressing is maintained and changed at 14 to 21 days postoperatively, at which point sutures are removed.
- Phase 2 (3-6 Weeks): The removable walking boot is utilized for an additional 3 weeks. Weight-bearing is progressively normalized as tolerated.
- Phase 3 (6-12 Weeks): Clinical and radiographic evaluation is performed to confirm consolidation of the arthrodesis. All protective immobilization can typically be discontinued between 6 to 12 weeks.
- Note on Compliance: If patient compliance is questionable, a short-leg non-weight-bearing cast for 3 to 4 weeks, followed by a walking cast for an additional 3 to 4 weeks, is strongly advised.
JUVENILE AND ADOLESCENT HALLUX VALGUS
While arthrodesis is a powerful tool for end-stage adult deformity, the management of juvenile and adolescent hallux valgus presents a distinctly different and highly complex biomechanical challenge. The etiology in this demographic is rarely related to footwear; rather, it is driven by intrinsic pathoanatomy, including hypermobility of the first ray, ligamentous laxity, and abnormal articular geometry.
Pathoanatomy and Clinical Evaluation
Any adolescent between 12 and 18 years of age presenting with a cosmetically unacceptable, progressive hallux valgus deformity—especially with a positive family history—warrants careful evaluation. Pain over the medial eminence and difficulty with shoe-fitting are the primary indications for operative intervention.
Surgical Warning: The patient and their parents must be explicitly counseled regarding the high risk of recurrence. Furthermore, if the patient is asymptomatic prior to surgery, they must understand that surgical intervention carries the risk of introducing postoperative pain where none previously existed.
The pathoanatomy of adolescent hallux valgus is frequently characterized by an increased Distal Metatarsal Articular Angle (DMAA). Valgus angulation of the MTP joint is caused not only by lateral displacement of the hallux but also by the lateral tilting of the articular surface of the metatarsal head relative to its longitudinal axis. Failure to recognize and correct an abnormal DMAA will inevitably lead to an incongruous joint and rapid recurrence. Additionally, an abnormal obliquity of the metatarsal-cuneiform articulation, which allows the first metatarsal to slide into varus (metatarsus primus varus), is a primary deforming force.
The most notoriously difficult combination of deformities to correct includes:
1. Hypermobile flatfoot
2. Metatarsus primus varus
3. Hallux valgus
Surgical Decision Making and Techniques
Surgical intervention must be tailored to the severity of the deformity, the magnitude of the intermetatarsal angle (IMA), the DMAA, and critically, the status of the first metatarsal physis.
1. Soft Tissue Procedures
For mild deformities characterized by a lower intermetatarsal angle, a normal DMAA, and a low hallux valgus angle (HVA), soft tissue realignment may suffice. Recommended procedures include:
* Adductor hallucis tenotomy
* Lateral capsulotomy
* Medial eminence excision (bunionectomy)
* Medial capsulorrhaphy (imbrication)
2. Management in the Immature Foot (Open Physis)
If the first metatarsal physis is fully open, proximal osteotomies that risk physeal arrest are contraindicated.
* Medial Opening Wedge Osteotomy: A medial opening wedge osteotomy performed distal to the open physis is the procedure of choice. The resected medial eminence can be utilized as an autograft to fill the opening wedge.
3. Proximal Metatarsal Osteotomies (Closed or Closing Physis)
For adolescents with closed or nearly closed physes and moderate-to-severe deformities (IMA > 13 degrees), a proximal osteotomy is required to achieve adequate angular correction.
* Proximal Crescentic Osteotomy: This is highly recommended as it allows multiplanar correction without significantly altering the length of the first metatarsal. Rigid internal fixation is mandatory.
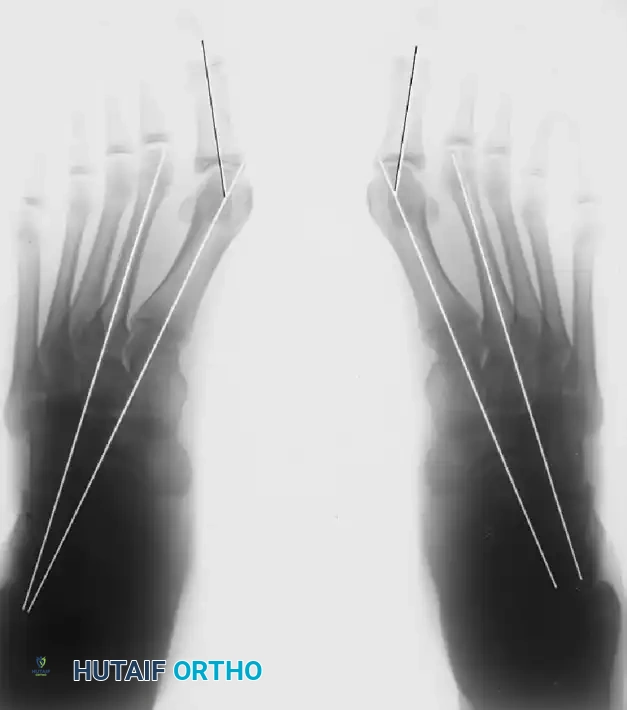
Preoperative standing radiographs of an adolescent with severe hallux valgus and metatarsus primus varus.
Postoperative standing radiographs following proximal osteotomy, adductor tendon release, medial capsular imbrication, and medial eminence removal. Note the incongruous MTP joint on the right, likely resulting from overcorrection of the intermetatarsal angle without addressing the DMAA.
Clinical Pearl: Pronation of the great toe in juveniles is often a result of pronation of the entire first ray, not just the hallux. Derotation to a neutral position must be performed concurrently with the correction of the metatarsal varus inclination.
4. Distal Metatarsal Osteotomies
- Chevron Osteotomy: The chevron osteotomy is highly effective for moderate deformities (HVA < 30 degrees, IMA < 12-15 degrees). If the physis is open, the distal location of the chevron osteotomy is highly advantageous as it avoids physeal injury.

Clinical photograph demonstrating moderately severe hallux valgus in a 17-year-old patient.

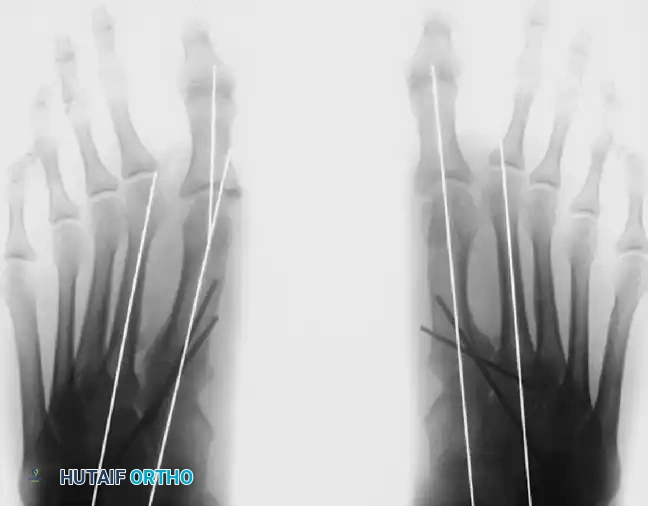
Preoperative radiograph of the same patient. Note the congenital shortening of the second metatarsal, which alters forefoot biomechanics and load distribution.

Postoperative radiograph demonstrating excellent alignment following a distal chevron osteotomy combined with an adductor release.
5. Diaphyseal Osteotomies
- Scarf Osteotomy: The scarf (Z-step cut) osteotomy is utilized for moderate to severe adolescent hallux valgus. It offers the advantage of high intrinsic stability, allowing for early weight-bearing, and versatility in correcting both IMA and DMAA. However, literature regarding its use in adolescents is contradictory, with some authors warning of high recurrence rates. Careful patient selection is paramount.
6. Complex and Severe Deformities
For severe, recalcitrant deformities (HVA > 35 degrees, IMA > 15 degrees, DMAA > 15 degrees, and a widened 1st-5th metatarsal angle > 30 degrees), single osteotomies are insufficient.
* Double First Metatarsal Osteotomy: Described by Peterson and Newman, this involves a proximal opening wedge osteotomy to correct the IMA, combined with a distal closing wedge osteotomy to correct the abnormal DMAA.
* Triple Osteotomy: In extreme cases with a markedly splayed forefoot, a triple procedure may be necessary: a medial cuneiform opening wedge osteotomy, a distal metatarsal osteotomy (to correct DMAA), and an Akin osteotomy (proximal phalangeal closing wedge) to correct residual hallux valgus interphalangeus.
7. Lateral Hemiepiphyseodesis
Lateral hemiepiphyseodesis of the first metatarsal base is an alternative, growth-modulation technique for symptomatic, progressive juvenile hallux valgus in children with at least 2 years of remaining growth. The rationale is that tethering the lateral physis allows continued medial growth, gradually correcting the metatarsus primus varus and improving forefoot loading.
* Evidence Base: While theoretically sound, literature is largely limited to small case series. Davids et al. reported on 7 children (11 feet), noting that while appropriate for patients failing conservative care, the average angular corrections achieved were small (HVA improved by 2.3 degrees; IMA improved by 3.5 degrees), with significant correction achieved in only about half of the cohort.
Conclusion on Adolescent Hallux Valgus
The surgical management of juvenile and adolescent hallux valgus requires a profound understanding of forefoot biomechanics and physeal anatomy. Any procedure that successfully relieves discomfort, retains a functional range of motion at the MTP joint, corrects the excessive valgus posture, and narrows the forefoot will yield high patient satisfaction. However, surgeons must remain vigilant regarding the correction of the DMAA and the management of hypermobility to mitigate the ever-present risk of deformity recurrence.
You Might Also Like