Pediatric Hand Anomalies: Surgical Management of Congenital Trigger Digits and Constriction Ring Syndrome

Key Takeaway
Congenital trigger digits and constriction ring syndrome present unique challenges in pediatric hand surgery. Unlike adult stenosing tenosynovitis, pediatric trigger digits typically manifest as fixed flexion deformities requiring precise A1 pulley release. Congenital constriction rings necessitate staged multiple Z-plasty reconstructions to prevent distal ischemia and restore contour. This guide details the pathoanatomy, indications, and step-by-step surgical techniques for optimal functional outcomes in these pediatric anomalies.
MISCELLANEOUS PEDIATRIC HAND ANOMALIES
The pediatric hand can present with a myriad of congenital and developmental anomalies that require a nuanced understanding of both evolving pathoanatomy and future growth potential. Among these miscellaneous anomalies, congenital trigger digits and congenital constriction ring syndrome (amniotic band syndrome) represent two distinct pathologies that frequently necessitate surgical intervention. Successful management relies on precise timing, meticulous tissue handling, and a thorough understanding of pediatric digital biomechanics.
CONGENITAL TRIGGER DIGITS
Congenital trigger digit occurs when the normal, frictionless gliding movement of the flexor tendon is mechanically impeded within the digital flexor sheath. In stark contrast to the clinical presentation in adults with stenosing tendovaginitis—who typically present with painful snapping or true "triggering"—the congenitally involved pediatric digit usually demonstrates a persistent, fixed flexion deformity.
This is a relatively rare condition, with an estimated incidence of 2.3 per 1,000 children. It occurs far more commonly in the thumb (trigger thumb) than in the lesser digits and presents bilaterally in approximately 25% of affected patients. The condition occurs sporadically and is generally not believed to be an inherited genetic trait. While trigger digits typically occur as isolated anomalies without other systemic findings, an association with trisomy 13 has been reported in the literature. Furthermore, its association with metabolic storage disorders, specifically mucopolysaccharidosis, has also been well-described and should be considered in patients presenting with multiple involved digits or atypical systemic features.
Pathoanatomy and Biomechanics
The pathological anatomy responsible for pediatric trigger digits is characterized by a volumetric mismatch between the flexor tendon and its retinacular sheath. This includes narrowing, hypertrophy, and thickening of the first annular (A1) pulley, occasionally accompanied by the formation of a localized ganglion cyst.
More commonly, a distinct intratendinous nodule is present within the flexor pollicis longus (FPL) or flexor digitorum profundus (FDP) tendon, located just proximal to the A1 pulley. This localized thickening is eponymously referred to as Notta’s nodule. Chronic inflammation and tenosynovial proliferation are frequently observed upon histological examination. The mechanical block occurs when this nodular thickening cannot passively glide through the unyielding A1 pulley, resulting in the digit becoming locked in a flexed posture at the interphalangeal (IP) joint.
Clinical Presentation and Natural History
Despite the nomenclature, "congenital" trigger digits in children are more commonly acquired during early infancy rather than being present strictly at birth; only about 25% of cases are noted immediately postpartum. A landmark prospective study evaluating 5,765 newborns did not reveal a single case of true congenital trigger thumb, supporting the theory of an acquired developmental etiology.
Frequently, the condition goes unnoticed by parents until the child reaches 1 or 2 years of age. At this developmental milestone, as fine motor skills and pinch grips mature, the child is observed to have a relatively fixed flexion posture of the IP joint of the thumb.
FIGURE 79-81A: Clinical presentation of a trigger thumb in a 2-year-old child, demonstrating the classic fixed flexion deformity at the interphalangeal joint.
Even with the application of moderate passive force, it may be impossible to extend the IP joint fully. Although an occasional extension posture of the thumb and involvement of multiple digits have been reported, these are atypical. The abnormal clicking, snapping, or pain that serves as the hallmark presenting complaint in adults is usually absent in the pediatric population.
Clinical Pearl: Congenital trigger thumb must be carefully differentiated from the clasped thumb deformity. In a clasped thumb, the primary pathology involves metacarpophalangeal (MCP) joint flexion due to extensor mechanism hypoplasia or absence, whereas a trigger thumb presents with isolated IP joint flexion and a palpable Notta's nodule at the volar MCP flexion crease.
Fixed joint contractures are highly unlikely if the condition resolves spontaneously or is surgically corrected before the child reaches 3 years of age. Spontaneous resolution is a well-documented phenomenon:
* It occurs in approximately 30% of children in whom the condition appears within the first year of life.
* It occurs in about 12% of children in whom it appears between 6 months and 2 years of age.
* Long-term observational studies (e.g., Baek et al.) have noted spontaneous resolution in up to 63% of patients over a median observation period of 48 months.
Trigger Finger vs. Trigger Thumb
Several academic reviews have emphasized the critical biomechanical and surgical differences between congenital trigger finger and trigger thumb.
1. Presentation: Trigger finger is less frequently associated with a rigid, fixed flexion deformity compared to the thumb.
2. Surgical Response: More importantly, a pediatric trigger finger may not respond to a simple A1 pulley release.
3. Anatomical Complexity: The flexor digitorum superficialis (FDS) decussation (Camper's chiasm) and the relationship with the FDP create a more complex gliding mechanism. When surgical intervention for a trigger finger is undertaken, the surgeon must be prepared for a more extensive exploration of the flexor mechanism. This may necessitate the excision of one or both slips of the FDS tendon and the sequential release of the A3 pulley to achieve full, unhindered excursion.
Non-Operative Management
Because spontaneous resolution can be expected in a significant percentage of children whose condition becomes apparent within the first year of life, a period of observation combined with gentle passive manipulation by the parents is highly appropriate.
Extension splinting of the IP joint can be attempted; literature reports a success rate of up to 66% with compliant, full-time splinting protocols. However, compliance in toddlers is notoriously poor, and the psychosocial burden on the family must be weighed against the relatively minor nature of a surgical release.
Surgical Indications and Timing
If the thumb remains rigidly locked or becomes painful, surgical release is definitively recommended. Intermittent, nonpainful triggering can be followed safely in hopes of spontaneous resolution if this is the strong preference of the parents; the timing of surgery in these intermittent cases probably has no detrimental effect on the ultimate functional outcome.
However, there is little clinical justification for subjecting a child to years of triggering and functional limitation, especially considering that surgical release has been proven to be exceptionally safe, definitive, and effective. Ignoring a fixed problem in the mere hope of resolution is not an appealing or evidence-based strategy.
- Standard Timing: Surgical release of the first annular (A1) pulley should be performed at approximately age 2 years if spontaneous resolution has not occurred.
- Early Intervention: In the rare instance in which multiple trigger digits are fixed in extension, preventing the child from making a fist and hindering global hand development, surgical intervention should be expedited (around 1 year of age).
Surgical Warning: Percutaneous trigger thumb release using a needle or specialized knife has been reported in children. However, due to the extreme proximity of the digital nerves—particularly the radial digital nerve of the thumb, which crosses obliquely over the flexor sheath—blind percutaneous release carries an unacceptable risk of irogenic nerve transection. We do not recommend percutaneous release in the pediatric population.
Surgical Technique: Open Release of Pediatric Trigger Thumb
- Anesthesia and Positioning: The procedure is performed under general anesthesia. The patient is positioned supine with the arm extended on a radiolucent hand table. A pediatric pneumatic tourniquet is applied to the upper arm.
- Incision Design: Make a shallow, 1.5 to 2.0 cm transverse incision exactly within the volar flexion crease of the metacarpophalangeal (MCP) joint.
- Superficial Dissection: Accidental nerve injury is avoided by utilizing blunt dissection with tenotomy scissors immediately deep to the dermis.
- Nerve Identification: Carefully identify and protect the radial and ulnar digital neurovascular bundles. The radial digital nerve is particularly vulnerable as it courses obliquely from ulnar to radial across the volar aspect of the flexor sheath at the level of the MCP joint. Retract the nerves gently using small blunt retractors.
- Pulley Exposure and Release: Clear the overlying adventitia to expose the A1 pulley. Identify Notta's nodule within the FPL tendon. Using a #15 blade or fine scissors, longitudinally incise the A1 pulley in its entirety, from its proximal edge to its distal margin.
- Confirmation of Release:
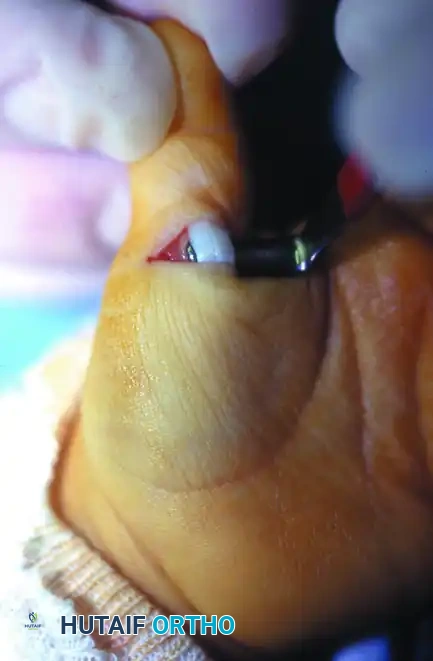
FIGURE 79-81B: Intraoperative view after successful division of the A1 pulley. The Notta's nodule is visible, and the FPL tendon now glides freely.
Passively flex and extend the IP joint of the thumb to confirm that the mechanical block has been completely eliminated and that the FPL tendon glides smoothly without catching. - Closure: Deflate the tourniquet and achieve meticulous hemostasis. Lacerated digital nerves or tendons (if iatrogenically injured) must be repaired immediately under microsurgical conditions. Close the skin with absorbable sutures (e.g., 5-0 chromic gut or fast-absorbing plain gut) to avoid the need for suture removal in an awake toddler.
- Postoperative Care: Apply a soft, bulky compressive dressing. A rigid splint is generally not required for isolated trigger thumb release. Active use of the hand is encouraged as tolerated. Recurrence is exceedingly unlikely if the surgical release of the A1 pulley is adequate.
CONGENITAL CONSTRICTION RING SYNDROME (AMNIOTIC BAND SYNDROME)
Congenital constriction ring syndrome is a complex spectrum of anomalies characterized by fibrous bands that encircle fetal limbs or digits in utero. The depth of these rings can vary from superficial cutaneous indentations to deep fascial constrictions that compromise lymphatic, venous, and arterial flow, potentially leading to autoamputation.
When a congenital ring is deep and completely encircles a limb or finger, surgical intervention is required to release the tethering, restore normal contour, and prevent distal lymphedema or ischemic compromise. The gold standard for reconstruction is the multiple Z-plasty release.
Biomechanics of the Z-Plasty in Constriction Rings
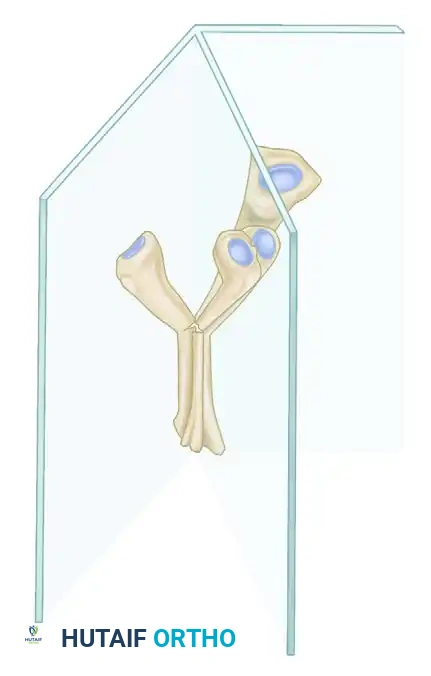
The Z-plasty is a fundamental tissue-rearrangement technique that serves two critical purposes in constriction ring syndrome:
1. Lengthening the Scar: By transposing two triangular flaps, the Z-plasty recruits lateral tissue laxity to increase the longitudinal length of the contracted ring. A standard 60-degree Z-plasty theoretically increases length by 73%.
2. Breaking the Linear Constriction: A circumferential scar acts as a non-yielding tourniquet. Multiple Z-plasties break this linear scar into a zigzag pattern, allowing the limb to expand as the child grows.
Surgical Warning (The 50% Rule): If a constriction ring completely encircles a digit or limb, never attempt to excise and reconstruct the entire 360-degree circumference in a single surgical setting. Circumferential dissection disrupts the entire superficial venous and lymphatic drainage, and potentially the arterial supply, leading to catastrophic distal necrosis. Plan to correct only 50% (half) of the ring during the initial procedure.
Surgical Technique: Multiple Z-Plasty Release of a Congenital Ring
-
Preoperative Planning and Marking:
- If the congenital ring is deep and completely encircles the limb or finger, plan to correct only the volar or dorsal half of the ring in the initial procedure.
- Before inflating the tourniquet, meticulously mark out the multiple Z-plasty sites along the constricting ring. The central limb of each Z-plasty lies directly within the depth of the constriction band. The limbs of the Z should be drawn at approximately 60-degree angles to the central limb to optimize lengthening and flap viability.

FIGURE 79-80A: Preoperative marking. The band is completely excised after it is ascertained that no deep fascial constriction remains. Only the volar half of the ring should be corrected at the initial procedure. -
Preparation and Tourniquet: Exsanguinate the limb using an Esmarch bandage (or elevation in very small infants), and inflate the pneumatic tourniquet to the appropriate pediatric pressure.
- Excision of the Band: Excise the marked half of the constricting ring. It is imperative to carry this excision down through the subcutaneous tissue and deep fascia. The underlying pathology is not merely cutaneous; the deep, unyielding fascial band must be completely resected until healthy, unconstricted fat and muscle/tendon are visualized.
- Flap Elevation: Sharply incise the marked Z-plasty limbs. Elevate the triangular flaps, ensuring a robust subcutaneous base is maintained to preserve the subdermal vascular plexus. Handle the apices of the flaps with extreme care (using skin hooks rather than crushing forceps) to prevent tip necrosis.
-
Transposition and Closure: Transpose the flaps. Suture the flaps in an appropriate interdigitating fashion to allow for the immediate lengthening and expansion of the constricting ring. Use fine, interrupted absorbable or non-absorbable sutures depending on surgeon preference and the child's age.

FIGURE 79-80B: Z-plasty closure. The flaps are interdigitated, effectively breaking the linear constriction and lengthening the tissue. -
Dressing and Immobilization: Deflate the tourniquet and assess the perfusion of the distal limb and the transposed flaps. Apply a non-adherent dressing followed by a bulky, soft dressing. Immobilize the extremity with a short-arm or long-arm splint, depending on the level of the release, to protect the delicate skin flaps from shear forces during the healing phase.
Postoperative Care and Staging
- Immobilization: The splinting is strictly maintained for 2 to 3 weeks to allow for undisturbed revascularization and healing of the Z-plasty flaps.
- Suture Removal: If non-absorbable sutures were utilized, they are removed in the clinic (or under light sedation if necessary) after 10 to 14 days.
- Second Stage: The remaining, unoperated half of the constricting ring can be safely reconstructed using an identical multiple Z-plasty technique after a minimum interval of 2 to 3 months. This delay ensures that the venous and lymphatic drainage established during the first stage is robust enough to support the distal extremity during the second stage of the release.
📚 Medical References
- Cardon LJ, Ezaki M, Carter PR: Trigger fi nger in children, J Hand Surg 24A:1156, 1999.
- Dellon AL, Hansen FC: Bilateral inability to grasp due to multiple (ten) congenital trigger fi ngers, J Hand Surg 5A:470, 1980.
- Dinham JM, Meggitt DF: Trigger thumbs in children, J Bone Joint Surg 56B:153, 1974.
- Moon WN, Suh SW, Kim IC: Trigger digits in children, J Hand Surg 26B:11, 2001.
- Ruiz-Iban MA, Gonzalez-Herranz P, Lopez-Mondejar JA: Percutaneous trigger thumb release in children, J Pediatr Orthop 26:67, 2006.
- Tan AHC, Lam KS, Lee EH: The treatment outcome of trigger thumb in children, J Pediatr Orthop B 11:256, 2002.
- Camptodactyly Engber WM, Flatt AE: Camptodactyly: an analysis of sixty-six patients and twenty-four operations, J Hand Surg 2A:216, 1977.
- Flatt AE: The care of congenital hand anomalies, St Louis, 1977, Mosby. Hori M, Nakamura R, Inoue G, et al: Nonoperative treatment of camptodactyly, J Hand Surg 12A:1061, 1987.
- Kilgore ES Jr, Graham WP III: Camptodactyly. In The hand, Philadelphia, 1977, Lea & Febiger. Koman LA, Toby EB, Poehling GG: Congenital fl exion deformities of the proximal interphalangeal joint in children: a subgroup of camptodactyly, J Hand Surg 15A:582, 1990.
- Lankford LL: Correspondence club letter, no 1975-1, Dallas, Tex, May 1975.
- McFarlane RM, Curry GJ, Evans HB: Anomalies of the intrinsic muscles in camptodactyly, J Hand Surg 8A:531, 1983.
- Millesi H: Camptodactyly. In Littler JW, Cramer LM, Smith JW, eds: Symposium on reconstructive hand surgery, St Louis, 1974, Mosby. Miura T: Non-traumatic fl exion deformity of the proximal interphalangeal joint: its pathogenesis and treatment, Hand 15:25, 1983.
- Smith PJ, Grobbelaar AO: Camptodactyly: a unifying theory and approach to surgical treatment, J Hand Surg 23A:14, 1998.
- Smith RJ, Kaplan EB: Camptodactyly and similar atraumatic fl exion deformities of the proximal interphalangeal joints of the fi ngers, J Bone Joint Surg 50A:1187, 1968.
- Tordai P, Engkvist O: Trigger fi ngers in children, J Hand Surg 24A:1162, 1999.
- Van Heest AE, House J, Krivit W, et al: Surgical treatment of
You Might Also Like