Operative Management of Median and Superficial Radial Nerves at the Wrist
Key Takeaway
Division of the median nerve at the wrist severely compromises hand function. Successful restoration requires meticulous microsurgical repair, precise rotational alignment, and tension-free coaptation. This guide details the operative management of median nerve lacerations, recurrent motor branch variations, and the strategic handling of superficial radial nerve injuries to prevent debilitating neuromas and optimize both sensory and motor recovery in the hand.
Comprehensive Introduction and Patho-Epidemiology
Division of the median nerve at the wrist represents a common, yet functionally devastating, peripheral nerve injury that demands meticulous surgical intervention. The median nerve is frequently referred to as the "eye of the hand" due to its critical role in providing tactile gnosis to the palmar aspect of the thumb, index, middle, and radial half of the ring fingers. Because the vital sensory function of these digits depends entirely on the success of this repair, exacting microsurgical technique is mandatory. Furthermore, the median nerve at the wrist is a complex mixed nerve; it carries critical motor fibers to the thenar musculature. Failure to restore this motor function results in severe, often permanent impairment of thumb opposition, leading to a profound decrease in pinch strength and overall hand dexterity.
The patho-epidemiology of these injuries is closely tied to the anatomical vulnerability of the volar wrist. The median nerve lies relatively superficially as it enters the carpal tunnel, making it highly susceptible to penetrating trauma. Epidemiological data indicates that the majority of these lacerations occur secondary to glass injuries, industrial accidents involving sharp machinery, or deliberate self-harm attempts. In the context of self-inflicted lacerations, the injury is frequently accompanied by concomitant division of the palmaris longus, flexor carpi radialis, and the superficial flexor tendons, creating a complex "spaghetti wrist" scenario that requires exhaustive exploration and sequential reconstruction. The mechanism of injury dictates the zone of trauma; sharp lacerations cause localized axonal disruption, whereas crush or avulsion injuries result in extensive longitudinal zones of injury that complicate primary repair.
Following transection, the distal segment of the median nerve undergoes Wallerian degeneration, a highly orchestrated biological sequence characterized by axonal breakdown and subsequent clearing of myelin debris by Schwann cells and macrophages. According to Boyes' foundational principles of nerve repair, functional results are directly proportional to the accuracy of fascicular approximation and inversely proportional to the degree of postoperative scarring and fibrosis. The Schwann cells in the distal stump proliferate to form bands of Büngner, which serve as biological conduits for regenerating axonal growth cones. However, this regenerative potential is strictly time-dependent. Prolonged denervation leads to irreversible atrophy of the thenar motor endplates and endoneurial fibrosis, underscoring the necessity for timely intervention.
Conversely, the superficial radial nerve (SRN) presents an entirely distinct patho-epidemiological challenge. While it is purely sensory, providing cutaneous innervation to the dorsoradial aspect of the hand, its transection rarely results in a debilitating functional sensory deficit due to significant dermatomal overlap with the lateral antebrachial cutaneous nerve and the dorsal sensory branch of the ulnar nerve. The primary pathology associated with SRN injury is not the loss of sensation, but rather its notorious propensity for developing exquisitely painful neuromas. The SRN is subjected to immense mechanical excursion and shear forces during normal wrist flexion and ulnar deviation. When a neuroma forms in this highly mobile, superficial subcutaneous plane, it becomes mechanically tethered and repetitively traumatized, leading to debilitating neuropathic pain that often overshadows any concurrent injuries.
Detailed Surgical Anatomy and Biomechanics
The topographical and internal fascicular anatomy of the median nerve as it courses from the distal forearm into the carpal tunnel is of paramount importance to the operating surgeon. In the distal forearm, the median nerve lies deep to the flexor digitorum superficialis (FDS) muscle belly before emerging to lie superficial and slightly radial to the superficial flexor tendons. At the level of the proximal wrist crease, it is bordered radially by the flexor carpi radialis (FCR) tendon and ulnarly by the palmaris longus (PL) tendon. The internal architecture of the median nerve at this level is highly organized. Sunderland’s extensive anatomical studies demonstrated that the motor fibers destined for the thenar eminence are typically grouped in the radial-volar (anteroradial) quadrant of the nerve. Recognizing this consistent fascicular topography is a critical prerequisite for achieving accurate rotational alignment during neurorrhaphy.
As the median nerve traverses the carpal tunnel deep to the transverse carpal ligament, it gives off its terminal branches. The recurrent motor branch is arguably the most critical of these, and every surgical effort must be made to identify and repair it if severed. This branch typically projects from the main trunk radially and superficially, passing just over the distal margin of the transverse carpal ligament. It then courses slightly posteriorly and laterally to innervate the intrinsic thenar musculature, specifically the abductor pollicis brevis (APB), the opponens pollicis, and the superficial head of the flexor pollicis brevis (FPB). The biomechanical consequence of denervating these muscles is the loss of palmar abduction and pronation of the thumb, rendering the thumb incapable of true opposition to the fingertips.
Surgeons must possess an intimate familiarity with the anatomical variations of the recurrent motor branch to avoid iatrogenic injury and to facilitate accurate reconstruction. The Lanz classification systematically categorizes these variations into five distinct types. The standard or extraligamentous type (Lanz Group 1) branches distal to the transverse carpal ligament and recurrently enters the thenar musculature. The subligamentous type (Lanz Group 2) branches within the carpal tunnel and runs deep to the ligament before entering the muscle. The transligamentous type (Lanz Group 3) pierces directly through the substance of the transverse carpal ligament, making it exceptionally vulnerable during both trauma and endoscopic or open carpal tunnel releases. Less common variations include an ulnar origin (Lanz Group 4), where the branch originates from the ulnar aspect of the median nerve and crosses anterior to the main trunk, and a duplicated or bifurcated recurrent branch (Lanz Group 5).
The superficial radial nerve (SRN) exhibits a contrasting anatomical course. It emerges from beneath the brachioradialis muscle in the distal third of the forearm, approximately 9 centimeters proximal to the radial styloid. It pierces the deep fascia to become subcutaneous and subsequently bifurcates into multiple terminal dorsal digital branches. Biomechanically, the SRN undergoes significant longitudinal excursion—up to 1.5 to 2.0 centimeters—during extreme wrist flexion and ulnar deviation. This extensive mobility is the primary reason why SRN neuromas are so frequently symptomatic; any scar tethering in the dorsal subcutaneous tissues completely restricts this necessary physiological excursion, resulting in severe traction neuritis with every movement of the wrist joint.
Exhaustive Indications and Contraindications
The decision-making process for operative management of median and superficial radial nerve injuries relies on a thorough understanding of the mechanism of injury, the timing of presentation, and the specific nerve involved. For the median nerve, acute sharp lacerations (such as those from glass or knives) are absolute indications for immediate or early delayed primary repair, ideally performed within the first 1 to 3 weeks. Early intervention capitalizes on the optimal biological environment for axonal regeneration and minimizes the retraction of the nerve stumps. Delayed presentations, where the injury was missed or initially managed non-operatively due to severe contamination or polytrauma, necessitate secondary repair or interpositional nerve grafting. If a patient presents with a neuroma-in-continuity following a crush injury, the indication for surgery involves formal exploration, intraoperative nerve conduction monitoring, and potential resection with grafting if electrical conduction across the lesion is absent.
Contraindications to primary direct repair of the median nerve are primarily biomechanical and physiological. The most critical contraindication is the inability to achieve a completely tension-free coaptation. If the nerve ends cannot be approximated with the wrist in a neutral or slightly flexed position (no more than 20 to 30 degrees of flexion), primary repair is strictly contraindicated, as excessive tension will inevitably lead to intraneural ischemia, scar proliferation, and failure of axonal progression. Additionally, primary repair is contraindicated in the presence of gross purulent infection, massive soft tissue avulsion lacking adequate vascularized coverage, or when the nerve ends exhibit severe, extensive crush damage that cannot be adequately debrided without creating an insurmountable gap. In these scenarios, the wound should be aggressively debrided, the nerve ends tagged with non-absorbable sutures to prevent retraction, and reconstruction delayed until soft tissue equilibrium is achieved.
The indications for the surgical management of the superficial radial nerve differ drastically from those of the median nerve due to its purely sensory nature and high propensity for neuroma formation. Unless there is a highly unusual and specific occupational requirement for repairing the SRN, or the laceration is exceptionally clean and sharp without any soft tissue loss, the primary indication for a severed SRN is prophylactic resection proximal to the zone of injury. Repairing the SRN is relatively contraindicated in contaminated crush injuries or in patients with a history of poor wound healing, as the risk of developing a crippling dorsal wrist neuroma far outweighs the minor disability associated with the loss of sensibility over the dorsum of the thumb and index finger.
Below is a comparative table detailing the specific indications and contraindications for operative management of both nerves at the wrist.
| Nerve | Surgical Strategy | Primary Indications | Contraindications / Relative Contraindications |
|---|---|---|---|
| Median Nerve | Primary Repair | Acute sharp lacerations (< 3 weeks); clean wounds; tension-free approximation possible. | Gap requiring > 30° wrist flexion to close; gross infection; severe crush with unidentifiable healthy fascicles. |
| Median Nerve | Nerve Grafting | Delayed presentation with gap; secondary reconstruction; failed primary repair; resection of neuroma-in-continuity. | Poorly vascularized soft tissue bed; lack of viable proximal/distal fascicular architecture. |
| SRN | Proximal Resection | Any traumatic transection (sharp or crush); symptomatic neuroma; delayed presentation. | Unique occupational requirement for dorsal thumb sensation (relative contraindication to resection). |
| SRN | Primary Repair | Exceptionally clean, sharp laceration in a compliant patient; rare specific sensory requirements. | Crush injuries; contaminated wounds; any tension on the repair; history of keloid/hypertrophic scarring. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative evaluation and meticulous planning are the cornerstones of successful peripheral nerve surgery. Clinical assessment must meticulously document both sensory and motor deficits, serving as both a medicolegal baseline and a guide for surgical exploration. Sensory evaluation requires the measurement of static and moving two-point discrimination (2PD) in the autonomous zones, which for the median nerve is strictly the volar tip of the index finger. Motor assessment demands careful palpation of the APB muscle belly during resisted palmar abduction of the thumb. The surgeon must remain highly cognizant of potential anatomical confounders, such as Martin-Gruber anastomoses in the forearm or Riche-Cannieu anastomoses in the hand, which can mask a complete median nerve transection by providing anomalous ulnar innervation to the thenar musculature.
In cases of delayed presentation or suspected neuroma-in-continuity, preoperative electromyography (EMG) and nerve conduction studies (NCS) are invaluable. However, the surgeon must understand the temporal limitations of these modalities; Wallerian degeneration takes approximately 3 to 4 weeks to manifest fully on EMG as fibrillation potentials and positive sharp waves. Therefore, an EMG performed immediately after an acute injury will yield falsely reassuring results. For late reconstructions, templating the anticipated nerve gap is crucial. The surgeon must plan for potential autologous graft harvest, most commonly the sural nerve, and ensure that the patient is thoroughly consented for the harvest site morbidity, including the resultant lateral foot numbness and the possibility of a symptomatic donor site neuroma.
Patient positioning and operating room setup must be optimized for prolonged microsurgical work. The patient is placed in the supine position with the affected arm extended on a rigid, radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, typically inflated to 250 mmHg or 100 mmHg above the patient's systolic blood pressure. The procedure absolutely must be performed under high-quality optical magnification; surgical loupes ranging from 3.5x to 4.5x are sufficient for the initial exposure and macro-dissection, but an operating microscope is highly recommended for the definitive fascicular alignment and epineurial neurorrhaphy, particularly when dealing with the recurrent motor branch or deploying interpositional cable grafts.
The surgical armamentarium must be prepared in advance. A dedicated microsurgical instrument tray containing jeweler's forceps, microscissors, and micro-needle holders is essential. The surgeon should have a variety of microsutures available, predominantly 8-0 or 9-0 nylon for the external epineurial repair of the main trunk, and 10-0 or 11-0 nylon for internal group fascicular repair and the recurrent motor branch. Additionally, the availability of fibrin tissue adhesive can be considered to augment the suture repair, reducing the number of required sutures and theoretically minimizing foreign body reaction and subsequent fibrosis at the coaptation site.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach begins with an extensile incision that incorporates the traumatic laceration while respecting the local biomechanical skin lines. The incision should cross the wrist flexion creases obliquely or in a zigzag fashion (Bruner-type incisions) to prevent the development of postoperative longitudinal flexion contractures. The incision is extended distally into the palm, completely dividing the transverse carpal ligament to decompress the median nerve and allow for extensive proximal and distal mobilization. It is a fundamental principle of nerve surgery to identify the normal, uninjured nerve proximally and distally in virgin tissue planes before tracing it centrally into the zone of injury and scar tissue. This "outside-in" approach minimizes the risk of iatrogenic damage to the nerve or its branches during the dissection.
Preparation of the nerve ends is arguably the most critical step in delayed or secondary repairs. The proximal stump, which forms a disorganized neuroma, must be carefully and sequentially excised using a fresh scalpel blade or specialized nerve-cutting scissors. Serial sectioning is performed in 1-millimeter increments until healthy, pouting fascicles—often described as "mushrooming" from the epineurium—are clearly visualized under high magnification. The distal stump, which forms a glioma (or Schwannoma) consisting of collapsed endoneurial tubes and fibrotic tissue, must similarly be excised until a healthy fascicular architecture is reached. Concurrently, the surrounding scar tissue must be radically excised to provide a healthy, well-vascularized soft-tissue bed for the repaired nerve. A nerve repaired over a bed of avascular scar will inevitably fail to regenerate due to localized ischemia.
Achieving perfect rotational alignment is paramount because the median nerve is a mixed motor and sensory nerve; rotational mismatch will result in motor fibers regenerating down sensory endoneurial tubes, leading to absolute functional failure. The most reliable landmark for securing proper rotational alignment is the vasa nervorum. A longitudinal epineurial vessel usually lies on the anterior surface of the median nerve, running parallel with its long axis. Aligning this vessel proximally and distally provides an excellent external guide. Internally, the surgeon must match the size and grouping of the fascicles. The distinct motor group, located in the radial-volar quadrant, must be aligned with absolute precision. Placing a single 8-0 nylon epineurial marking suture in each segment prior to the final resection can greatly aid in maintaining proper rotation during the subsequent repair process.
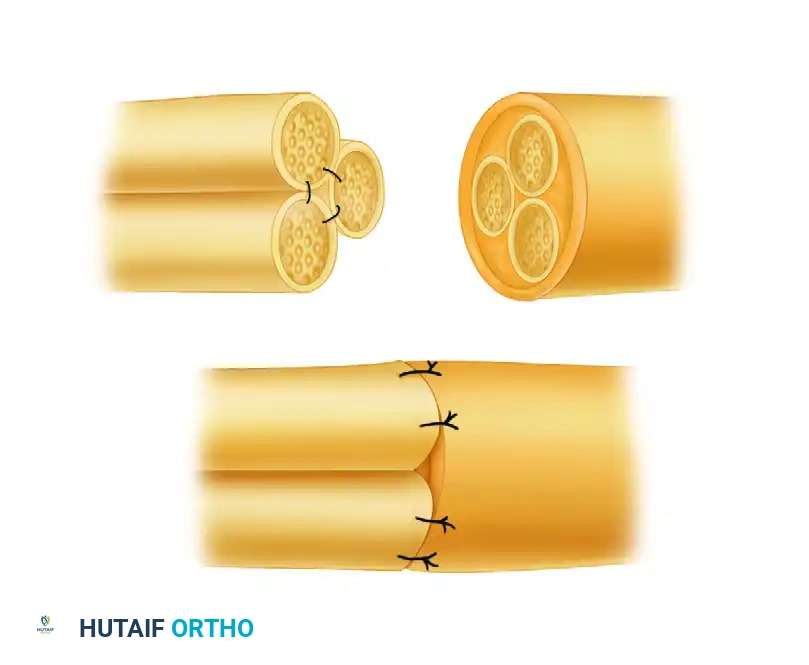
When a tension-free primary repair is impossible, interpositional nerve grafting is mandatory. Sural nerve autografts remain the gold standard. The grafts are harvested, cut to the appropriate length (allowing for 10-15% shrinkage), and strictly reversed in orientation to prevent regenerating axons from escaping through the side branches of the graft. For segmental gaps in a large nerve like the median nerve, bundle suturing techniques (as illustrated in the provided figure) are employed. Multiple cable grafts are utilized to bridge the specific fascicular groups, securing them with 9-0 or 10-0 nylon sutures.
For the superficial radial nerve, the surgical technique is focused entirely on resection and neuroma prevention. The SRN is identified proximal to the zone of injury in the distal forearm. Gentle distal traction is applied to the nerve, and it is transected sharply with a fresh scalpel. The proximal stump is then allowed to retract deeply into the proximal forearm musculature, typically deep to the brachioradialis muscle belly. The surgeon must ensure that the nerve end lies in a well-vascularized area of minimal scar tissue, completely isolated from the mechanical excursion of the wrist joint and the overlying skin. Burying the proximal stump directly into the muscle belly or capping the nerve end with a synthetic conduit can further reduce the incidence of symptomatic neuroma formation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous microsurgical technique, complications following median and superficial radial nerve surgery at the wrist are relatively common and can profoundly impact patient outcomes. The most frequent complication is the failure of adequate motor recovery, particularly concerning the thenar intrinsic muscles. The distance from the wrist to the motor endplates of the APB is relatively short, yet factors such as advanced patient age, delayed repair, and excessive tension can halt axonal progression. If no clinical or electrical signs of motor recovery are present by 6 to 9 months postoperatively, irreversible motor endplate atrophy has likely occurred. In these instances, salvage procedures in the form of secondary tendon transfers are highly indicated to restore thumb opposition. The Burkhalter transfer (Extensor Indicis Proprius to APB) or the Camitz transfer (Palmaris Longus extended with palmar fascia to APB) are excellent salvage options that reliably restore functional palmar abduction.
Neuroma formation is the most debilitating sensory complication. While neuromas-in-continuity can occur in the median nerve, resulting in a severe Tinel's sign and hyperesthesia, terminal neuromas of the superficial radial nerve are notoriously problematic. The incidence of symptomatic SRN neuromas following primary repair attempts is alarmingly high, approaching 30-40% in some series. These neuromas cause crippling neuropathic pain that is exacerbated by wrist flexion and ulnar deviation. Salvage management for a failed SRN repair or a symptomatic neuroma involves re-exploration, proximal resection of the neuroma, and deep intramuscular burying of the proximal stump into the brachioradialis or pronator teres, ensuring the nerve end is entirely shielded from mechanical sheer forces.
Complex Regional Pain Syndrome (CRPS) is a severe, centrally mediated complication that can occur following any nerve injury or surgery at the wrist. Characterized by disproportionate pain, allodynia, sudomotor changes, and trophic skin alterations, CRPS requires immediate, aggressive multidisciplinary management. Early recognition is vital. Treatment involves intensive hand therapy focused on active range of motion and stress-loading protocols, combined with pharmacological interventions such as gabapentinoids, tricyclic antidepressants, and short courses of oral corticosteroids. In refractory cases, stellate ganglion blocks or spinal cord stimulators may be required as salvage therapies.
Below is a comprehensive table outlining the primary complications, their estimated incidence rates, and the accepted salvage management strategies.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Failure of Motor Recovery | 15 - 25% | Delayed repair (>6 months); severe crush; advanced age; tension at repair site. | Tendon transfers (e.g., EIP to APB - Burkhalter; FDS to APB; Camitz transfer). |
| Symptomatic SRN Neuroma | 30 - 40% (if repaired) | Attempted primary repair of SRN; superficial scarring tethering the nerve. | Proximal resection and deep intramuscular burying (Brachioradialis); TMR (Targeted Muscle Reinnervation). |
| Neuroma-in-Continuity (Median) | 10 - 15% | Tension on repair; poor fascicular alignment; avascular soft tissue bed. | Re-exploration, neurolysis, intraoperative NCS. Resection and grafting if conduction is absent. |
| Complex Regional Pain Syndrome | 5 - 10% | Severe trauma; delayed mobilization; psychological factors; tight cast/splint. | Aggressive hand therapy (stress loading); Gabapentinoids; Stellate ganglion blocks; Vitamin C prophylaxis. |
| Joint Contracture | 10 - 20% | Prolonged immobilization in extreme flexion to overcome nerve gap tension. | Dynamic splinting; serial casting; surgical capsulotomy/tenolysis if conservative measures fail. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following median nerve repair is as critical to the final functional outcome as the microsurgical repair itself. The protocol is strictly phased to balance the protection of the delicate neurorrhaphy with the prevention of debilitating tendon adhesions and joint contractures. Phase 1, the Immobilization Phase, spans from postoperative day 0 to week 3. Immediately following surgery, the wrist is immobilized in a custom-fabricated dorsal blocking splint. The wrist is positioned in neutral to slight flexion (approximately 10 to 20 degrees) to entirely remove tension from the median nerve repair site. However, absolute immobilization of the digits is contraindicated. Active and passive digital range of motion (ROM) is encouraged immediately to prevent flexor tendon adhesions within the carpal tunnel, provided that this digital motion does not place transmitted tension on the nerve repair.
Phase 2, the Early Mobilization Phase, occurs between weeks 3 and 6. At this stage, the initial epineurial healing has occurred, and the tensile strength of the repair site is increasing. The dorsal blocking splint is gradually adjusted to bring the wrist from slight flexion into a neutral position, and eventually into slight extension by week 6. Active and active-assisted ROM of the wrist is initiated under the strict supervision of a certified hand therapist. Crucially, nerve gliding exercises are introduced cautiously during this phase. These exercises are designed to promote longitudinal excursion of the median nerve within the carpal tunnel, preventing the nerve from adhering to the surrounding fibrotic bed, which would otherwise lead to traction neuritis upon full wrist extension.
Phase 3, the Strengthening and Sensory Re-education Phase, begins at week 6 and continues for several months to years. Progressive strengthening of the forearm and hand musculature is initiated using putty, grip strengtheners, and resistance bands. As the regenerating axons progress distally—at an average rate of 1 millimeter per day, or roughly 1 inch per month—the advancing Tinel's sign will reach the palm and eventually the digits. Once the patient begins to perceive protective sensation (typically 30 Hz vibration) in the fingertips, formal sensory re-education programs are instituted. Based on Dellon's protocols, this involves intensive cortical remapping exercises. Patients are exposed to various textures, temperatures, and blindfolded object recognition tasks to train the somatosensory cortex to interpret the altered, often distorted afferent signals arriving from the newly reinnervated receptors.
Concurrently during Phase 3, rigorous motor monitoring is essential. The APB muscle is monitored clinically for signs of voluntary contraction and via electromyography (EMG) at 3, 6, and 9 months postoperatively to confirm reinnervation potentials (nascent motor units). The patient is instructed in isolated thumb palmar abduction exercises to specifically recruit the APB. If the patient demonstrates functional sensory recovery but complete failure of motor recovery by the 9-month mark, the rehabilitation protocol pivots toward preparing the patient for a salvage tendon transfer, focusing on maximizing the strength and excursion of the intended donor muscle (e.g., the Extensor Indicis Proprius).
Summary of Landmark Literature and Clinical Guidelines
The operative management of median and superficial radial nerves at the wrist is heavily guided by decades of foundational orthopedic and microsurgical literature. The biological principles of nerve regeneration and the critical importance of tension-free repair were definitively established by Boyes and later expanded upon by Sunderland. Sunderland’s classification of nerve injury (spanning from neuropraxia to complete neurotmesis) and his exhaustive mapping of the internal fascicular topography of the median nerve remain the anatomical basis for all modern group fascicular repairs. His work demonstrated that the spatial orientation of motor and sensory fascicles is highly consistent at the wrist, dictating the necessity for precise rotational alignment during neurorrhaphy.
The management of nerve gaps was revolutionized by the landmark studies of Millesi in the 1970s. Millesi definitively proved that a nerve repaired under tension will undergo severe intraneural fibrosis and fail to regenerate. He established the clinical guideline that if a gap cannot be closed with the wrist in a neutral or slightly flexed position, an interpositional nerve graft is mandatory. His techniques for utilizing reversed sural nerve cable grafts established the modern gold standard for managing segmental nerve defects, shifting the paradigm away from extreme joint flexion and extensive skeletal shortening, which were previously used to overcome nerve gaps but resulted in disastrous joint contractures.
Regarding the recurrent motor branch of the median nerve, the anatomical classification published by Lanz in 1977 remains the definitive clinical guideline. Lanz’s anatomical dissections highlighted the high variability of the motor branch, particularly the transligamentous variant, which has profoundly influenced how surgeons approach carpal tunnel releases and trauma explorations. His work mandates that surgeons must actively anticipate anatomical variations rather than relying on a standard extraligamentous course, thereby significantly reducing the incidence of iatrogenic denervation of the thenar musculature.
Finally, the management of the superficial radial nerve has been shaped by the extensive literature on neuroma pathophysiology by Dellon and Mackinnon. Their clinical series demonstrated the unacceptably high failure rates of primary SRN repair and the devastating impact of dorsal wrist neuromas. Current clinical guidelines, heavily influenced by their research, advocate for the prophylactic resection and deep intramuscular burying of the SRN following transection, prioritizing the prevention of neuropathic pain over the restoration of a non-critical sensory dermatome. Recent advancements in the literature are now exploring Targeted Muscle Reinnervation (TMR) and specialized nerve conduits as adjunctive techniques to further minimize neuroma formation following SRN resection.
