Mastering Foot Malunions: Advanced Surgical Management and Arthrodesis Techniques
Key Takeaway
Malunions of the foot present complex biomechanical challenges that can severely impair weight-bearing and gait. This comprehensive guide details the evidence-based surgical management of malunited fractures across the phalanges, metatarsals, tarsals, talus, and calcaneus. Emphasizing precise osteotomies, strategic arthrodesis, and meticulous soft-tissue handling, these protocols aim to restore a plantigrade, pain-free foot while mitigating risks such as osteonecrosis and post-traumatic arthrosis in the compromised orthopedic patient.
Introduction to Foot Malunions
The surgical management of foot malunions requires a profound understanding of lower extremity biomechanics, multi-planar joint kinematics, and the intricate soft-tissue envelope of the foot. A malunited fracture in the foot rarely presents as an isolated osseous deformity; it frequently alters the weight-bearing axis, disrupts the metatarsal parabola, and precipitates adjacent joint arthrosis. The overarching goal of intervention is not necessarily the restoration of pristine radiographic anatomy, but rather the recreation of a stable, plantigrade, and pain-free foot capable of accommodating standard footwear and enduring the dynamic loads of the gait cycle.
Phalanges of the Toes
Malunion of fractures involving the phalanges of the toes rarely causes sufficient functional disability to justify surgical intervention. The intrinsic mobility of the lesser toes often compensates for mild to moderate angular deformities. However, a severe deformity that causes intractable pain, impingement against footwear, or overriding of adjacent digits warrants correction.
Surgical Considerations
Correction can be achieved efficiently through a lateral or dorsal incision, meticulously placed to avoid injury to the extensor and flexor tendons.
Surgical Pearl: When addressing phalangeal malunions, prioritize soft-tissue balancing. A simple osteotomy and realignment of the fragments may be sufficient for mild deformities. However, for complete correction of chronic, rigid malunions, a wide resection arthroplasty or interphalangeal arthrodesis may be required. This can be performed with impunity, as highly skillful, independent movements of the lesser toes are not a prerequisite for normal gait.
Metatarsals
The metatarsals form the critical anterior pillar of the longitudinal arch. If malunion of the neck or shaft of a metatarsal is disabling, it is almost universally because the fragments have angulated toward the plantar surface of the foot. This plantarflexion deformity depresses the metatarsal head, producing a prominent osseous mass on the sole. This leads to intractable plantar keratosis (IPK) and severe transfer metatarsalgia. If the original fracture was severely comminuted, the resulting hypertrophic callus may even simulate a soft-tissue or osseous tumor.
Operative Strategy
Surgery should not aim to restore perfect cortical apposition and alignment. The primary objective is to correct the sagittal plane angulation so that weight-bearing forces are redistributed evenly across the metatarsal head parabola, eliminating painful focal pressure on the sole.
Surgical Technique: Metatarsal Osteotomy and Realignment
- Approach: Make a longitudinal incision on the dorsum of the forefoot parallel to the shaft of the affected bone. Often, a single strategically placed incision in the intermetatarsal space provides excellent access to two adjacent malunited metatarsals.
- Exposure and Osteotomy: Dissect sharply down to the bone, reflecting the periosteum minimally to preserve blood supply. Expose the old fracture site and divide the malunion with a small, sharp osteotome or oscillating saw.
- Deformity Correction: In instances of severe plantar angulation, a dorsally based closing wedge of bone must be removed to permit adequate elevation of the distal fragment.
Surgical Warning: Resection must not be so extensive that it creates a critical-sized defect leading to nonunion. Preserve the plantar cortex as a hinge if possible.
- Reduction: Raise the distal fragment into a slightly overcorrected (dorsiflexed) position by applying pressure from the plantar aspect of the foot while forcibly flexing the toes to utilize the windlass mechanism.
- Fixation: Fix the fragments with an intramedullary Kirschner wire (K-wire) driven retrograde through the metatarsal head, or utilize low-profile dorsal plating depending on bone quality.
Postoperative Protocol:
A well-molded short leg cast is applied from the tibial tubercle to the toes, specifically molded beneath the metatarsal heads to maintain the overcorrected position. At 3 weeks, any percutaneous intramedullary pins are removed, and the patient is transitioned to a walking boot cast with a felt pad inserted beneath the fractures to hold the toes in plantar flexion. At 6 weeks, the cast is discontinued, and the patient is fitted with a sturdy shoe incorporating a custom arch support and a metatarsal pad to offload the surgical site.
Tarsals (Excluding Talus and Calcaneus)
Malunions of the midfoot (navicular, cuboid, and cuneiforms) are frequently the sequelae of violent, high-energy trauma (e.g., crush injuries, motor vehicle accidents). These injuries often involve severe comminution, multi-joint dislocations (Chopart or Lisfranc fracture-dislocations), and profound soft-tissue compromise.
The distal fragments are typically displaced dorsally, sometimes overlapping the proximal fragments. This creates a dual deformity: a painful bony prominence on the dorsum of the foot (causing shoe-wear impingement) and a corresponding mass on the plantar surface (causing weight-bearing pain).
Indications for Arthrodesis
While isolated osteotomies through the old fracture lines can occasionally preserve some lateral movement, midtarsal motion is usually already lost due to post-traumatic fibrosis and articular cartilage damage. Therefore, partial or total resection and arthrodesis of one or more tarsal joints are frequently required. Fusing these joints corrects the architectural position, relieves pain, and prevents progressive traumatic arthrosis.
Clinical Pearl: Because lateral movements are often already compromised, a well-positioned midfoot arthrodesis does not significantly add to the patient's functional disability, even in young, active individuals. If the subtalar joint is spared, its motion must be rigorously protected by fusing only the affected midtarsal joints.
Unless the deformity is exceptionally severe or skin breakdown is imminent, operative intervention for midfoot malunion should be delayed until a trial of conservative management (custom orthotics, rigid-sole shoes) has been attempted for 6 to 12 months.
Surgical Technique: Tarsal Reconstruction and Arthrodesis
- Approach: Make an incision either lateral to the extensor tendons on the dorsum of the foot or middorsally in line with the third metatarsal. Reflect the periosteum to expose the malunion.
- Osteotomy: If the injury is relatively recent (a few months old), divide the bones with an osteotome directly through the old fracture line. If the fragments overlap excessively, resect a small section from each to allow for anatomic reduction without excessive tension on the dorsal skin.
- Reduction: Using a bone skid, lamina spreader, or periosteal elevator, lever the fragments into their anatomic positions, restoring the medial and lateral column lengths.
- Fixation: While reduction may appear stable, rigid internal fixation using bone staples, crossed K-wires, or modern compression screws/plates is mandatory to maintain apposition and achieve fusion.
- Chronic Malunions: If the malunion has been present for years, the tarsus may be completely auto-fused, rendering the old fracture lines invisible. In these cases, perform corrective osteotomies based on the apex of the deformity, without regard to the obliterated joints. Severe deformities will require wide wedge resections.
- Adjunctive Procedures: If the malunion has caused chronic tenosynovitis of the extensor tendons and secondary dorsal contracture of the toes, these claw toe deformities can be addressed concurrently or in a staged procedure.
Postoperative Protocol:
The foot is immobilized at a neutral right angle in a short leg cast. Radiographs are obtained at 1 week to confirm maintenance of position. At 2 weeks, sutures are removed. If any residual deformity is noted, it can be manipulated under general anesthesia before applying a new cast. The patient remains non-weight-bearing for 1 month, followed by a well-molded walking boot cast for an additional 4 weeks. Custom arch supports are utilized for 4 to 6 months post-consolidation.
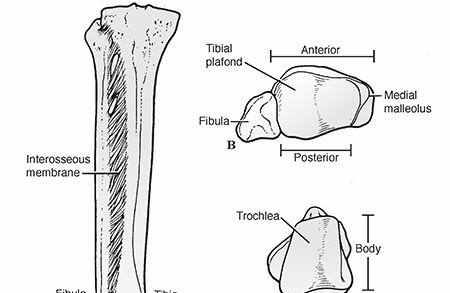
Talus
Malunion of a talar fracture is a devastating complication that almost universally results in severe disability. Deformities of the talar neck or body disrupt the congruency of the ankle, subtalar, and talonavicular joints, leading to rapid, multi-joint post-traumatic arthrosis.
Malunion of the Talar Neck
Talar neck malunions are biomechanically analogous to intracapsular femoral neck fractures. The initial trauma often disrupts the delicate retrograde blood supply (artery of the tarsal canal, branches of the dorsalis pedis), leading to osteonecrosis (AVN) of the talar body.
Union typically occurs with the distal fragment (talar head) in rotation, medial deviation, and dorsal displacement, producing a complex varus or valgus deformity. Valgus deformity is more common, presenting with the head deviated medially and dorsally.
- Varus Malunion: Historically treated with triple arthrodesis, though results are unpredictable due to the profound alteration of hindfoot mechanics. Modern techniques involve shortening the lateral column (calcaneocuboid joint) or lengthening the medial column to correct forefoot rotation.
- Osteotomy: A precise talar neck osteotomy at the apex of the deformity, supplemented with a rhomboid-shaped autogenous tricortical iliac crest bone graft, can restore alignment.
Surgical Warning: The extraosseous blood supply to the talus must be meticulously preserved during exposure to prevent iatrogenic osteonecrosis.
Malunion of the Talar Body and Osteonecrosis
If the talar body is avascular or the articular surfaces are grossly distorted but viable, arthrodesis is the procedure of choice.
* Ankle/Subtalar Fusion: If both superior (tibiotalar) and inferior (subtalar) surfaces are destroyed, a tibiotalocalcaneal (TTC) arthrodesis via a posterior or lateral approach is indicated.
* Calcaneotibial Arthrodesis: When the talar body is completely nonviable, fragmented, or infected, talectomy followed by calcaneotibial arthrodesis is required. To preserve limb length, Ilizarov circular fixation techniques with bone segment transport (corticotomy of the distal tibia) can be utilized. This demands a highly compliant patient and radical debridement of any necrotic/infected bone.
Calcaneus
Calcaneal malunions present with a constellation of symptoms: loss of heel height, increased heel width, varus/valgus malalignment, and subfibular impingement. Circumferential hindfoot pain is typically caused by subtalar arthrosis, while lateral pain is often due to impingement of the lateral calcaneal wall against the fibula, entrapping the peroneal tendons.
Diagnostic Pearl: An injection of 1% lidocaine into the subtalar joint under fluoroscopic guidance is highly effective in differentiating intra-articular subtalar pain from extra-articular lateral impingement pain.
Preoperative Optimization and Imaging
Smoking is a major risk factor for nonunion and wound breakdown, particularly with extensile lateral approaches. Patients must be counseled to cease smoking preoperatively.
Radiographic evaluation must include standard weight-bearing views, a Harris axial view, and Broden views. However, a CT scan in the transverse and coronal planes is the gold standard for assessing subtalar congruity, lateral wall blowout, and fibular impingement.
Stephens and Sanders Classification
Stephens and Sanders utilized CT imaging to classify calcaneal malunions into three distinct types, guiding surgical intervention:
Stephens and Sanders CT Classification of Calcaneal Malunions (Types I, II, and III).
Table 55-1 • Guidelines for Treatment of Calcaneal Malunions
* Type I: Lateral exostectomy through an extensile L-shaped lateral incision.
* Type II: Lateral exostectomy plus subtalar arthrodesis using the resected exostosis as local bone graft.
* Type III: Lateral exostectomy plus subtalar arthrodesis plus calcaneal osteotomy.
Surgical Techniques for Calcaneal Malunion
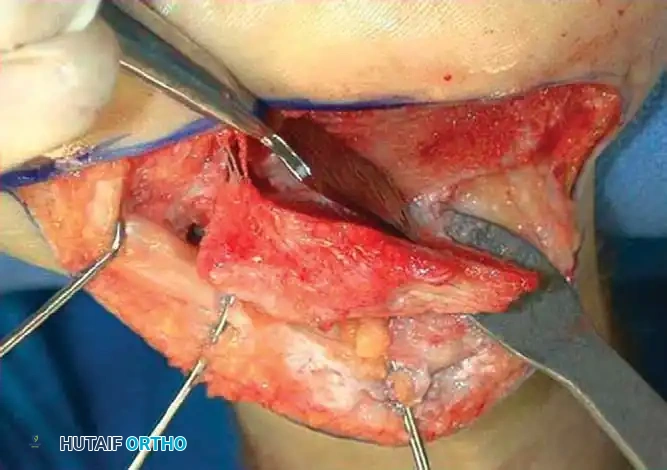
1. Lateral Exostectomy and Decompression
For Type I malunions, the primary issue is lateral impingement.
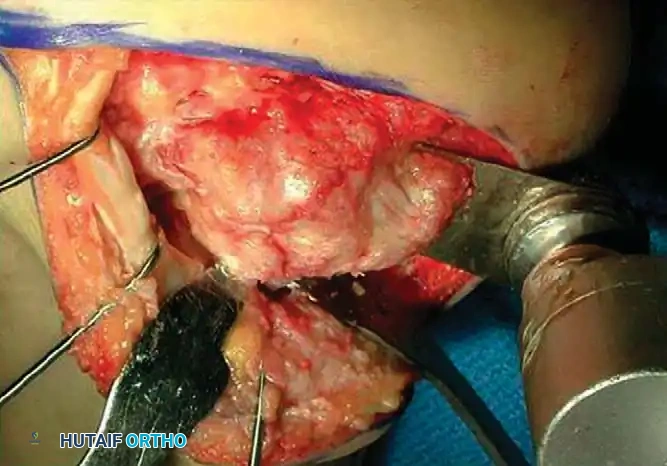
Intraoperative view demonstrating exposure of the lateral calcaneal wall and preparation for exostectomy.
An extensile lateral approach is utilized to elevate the full-thickness fasciocutaneous flap. The sural nerve and peroneal tendons are identified and protected. The hypertrophic lateral wall of the calcaneus is resected using an osteotome or oscillating saw, thoroughly decompressing the subfibular space.
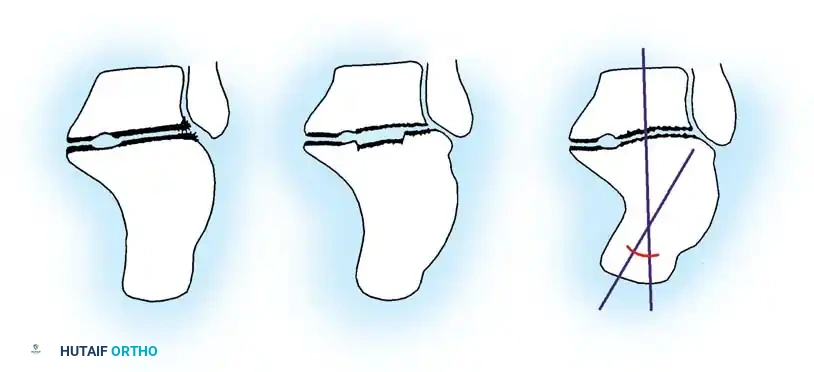
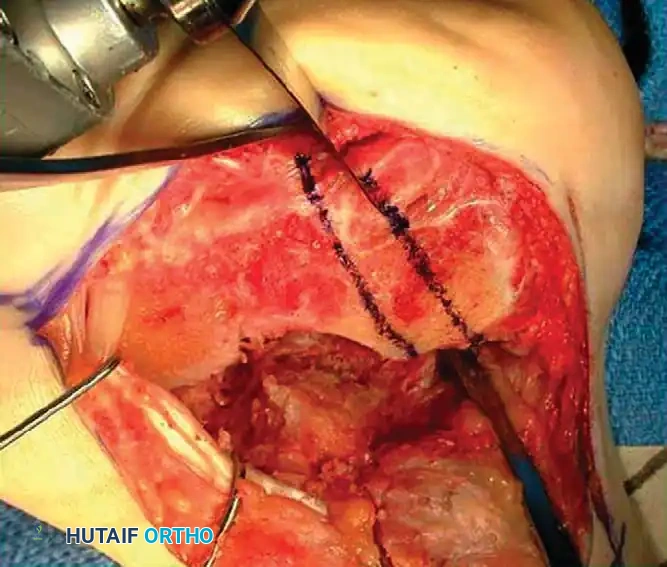
2. Calcaneal Osteotomy and Realignment Arthrodesis (Type II & III)
For severe deformities with loss of heel height and subtalar arthrosis, a distraction bone-block arthrodesis is indicated.

Intraoperative marking of the planned calcaneal osteotomy lines to correct varus/valgus malalignment.
Levering and distraction of the osteotomy site to restore calcaneal height and correct the talar declination angle.
The technique involves a lateral decompression, medial subtalar capsulotomy, and aggressive distraction of the subtalar joint. A lamina spreader is inserted to restore the talocalcaneal height.
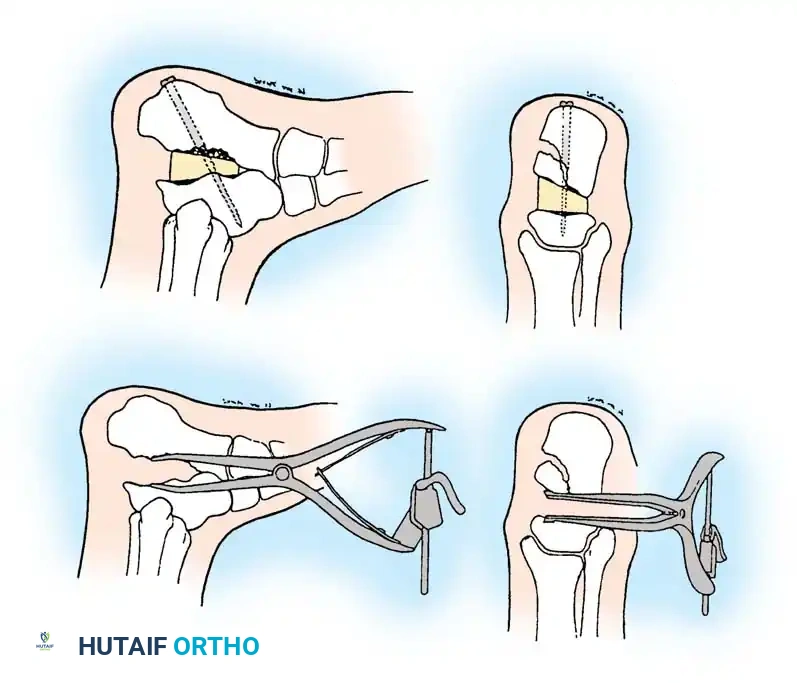
Diagrammatic representation of subtalar distraction and realignment arthrodesis using a tapered wedge bone graft.
A tricortical iliac crest bone graft (or the resected lateral wall exostosis) is fashioned into a tapered wedge and impacted into the distracted subtalar joint. This bone block restores heel height, improves talar inclination, and corrects varus/valgus malalignment.
Surgical Warning: The use of structural allografts in subtalar bone block arthrodesis has been associated with significantly higher nonunion rates compared to autograft. Autogenous bone is strongly recommended.
Fixation and Radiographic Confirmation
Rigid fixation is typically achieved with large-diameter (6.5mm or 7.3mm) cannulated cancellous screws placed from the posterior calcaneal tuberosity into the talar body and neck.
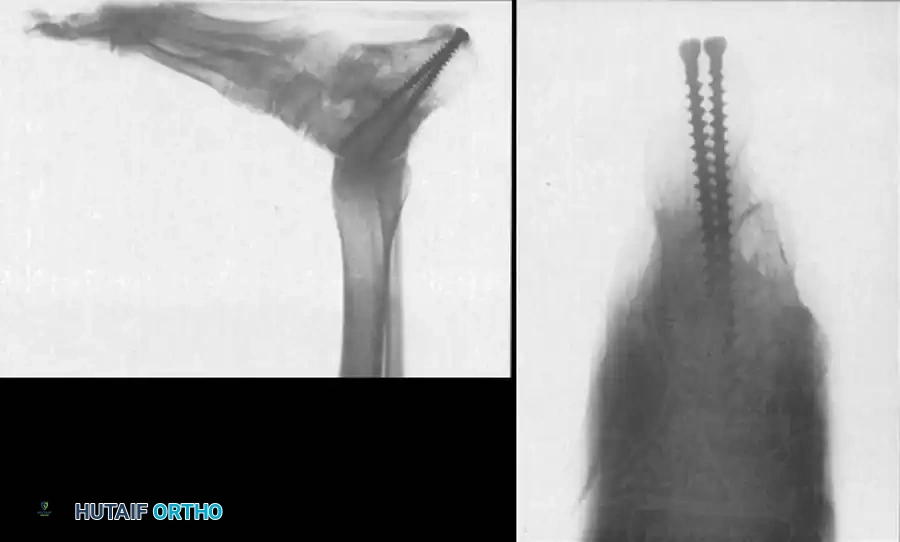
Lateral radiograph demonstrating robust screw fixation across the subtalar joint following realignment.
Coronal CT scan confirming solid osseous integration of the bone block and hardware placement within the subtalar joint.

Final lateral radiograph showing restored talocalcaneal alignment and a solid fusion mass.
Triple Arthrodesis vs. Isolated Subtalar Fusion
For severe crushing fractures, some authors historically recommended primary triple arthrodesis, arguing that the talonavicular and calcaneocuboid joints are inevitably deranged. However, modern consensus dictates that unless the midtarsal joints are overtly arthritic or unstable, arthrodesis should be strictly limited to the subtalar joint. Preserving midtarsal motion is crucial for accommodating uneven terrain and reducing adjacent-segment stress.
Posterior Subtalar Arthrodesis (Gallie Technique)
Historically, Gallie advised arthrodesis of the subtalar joint via a posterior approach. While technically simpler and avoiding the lateral soft-tissue envelope, this approach does not allow for the correction of varus/valgus deformities, restoration of heel height, or decompression of lateral impingement. Therefore, its use in modern orthopedic surgery is largely reserved for isolated, in-situ fusions where no structural realignment is required.
You Might Also Like