Master ABOS Orthopedic Board Review: Pediatric Infections, Tumors, & Skeletal Dysplasias | Part 6
Key Takeaway
ABOS Pediatric Orthopedics Review Part 6 covers key topics in pediatric orthopedic pathology. It includes newborn septic coxitis, osteomyelitis, benign bone tumors like osteoblastoma, and a wide range of skeletal dysplasias such as achondroplasia, SED, and Morquio syndrome, focusing on their diagnosis, clinical features, and management strategies.
Question 1
A 5-month-old infant presents with a several-day history of fever, irritability, and reluctance to move the left lower extremity. Physical examination reveals a painful, limited range of motion in the left hip. This clinical picture is consistent with "Säuglings-coxitis." What is the typical age range for this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The first sentence of the provided text clearly defines the age group: "In newborns and in infants under the age of 1 year, osteomyelitis affects the epiphyses and the joints, and it is associated with arthritis, which may result in articular destruction (epiphyseal osteomyelitis)." The term "Säuglings-coxitis" itself translates to "infant's coxitis."
Question 2
A 1-month-old infant was treated for septic coxitis of the right hip. Despite initial management, the child later develops a severe hip deformity requiring reconstructive surgery in adolescence. Which of the following long-term sequelae is most characteristic of untreated or severe newborn's coxitis?
View Answer & Explanation
Correct Answer: B
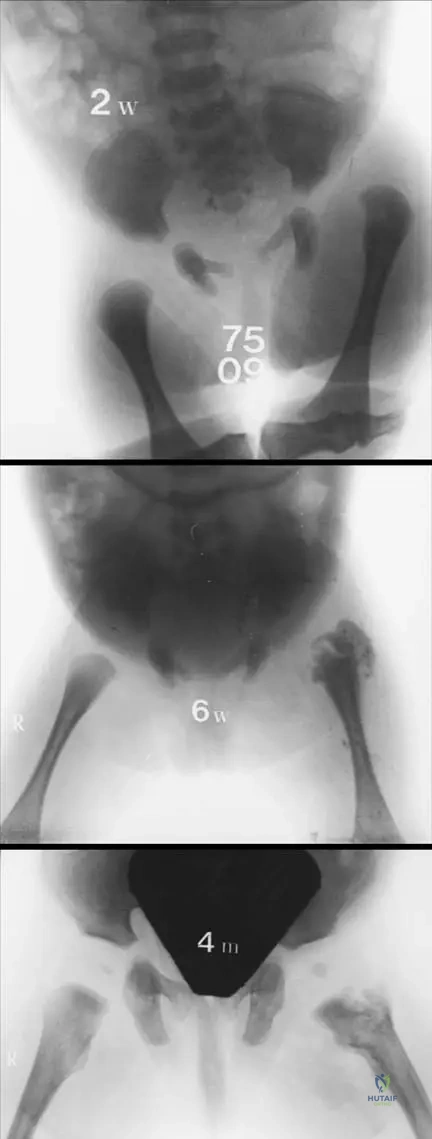
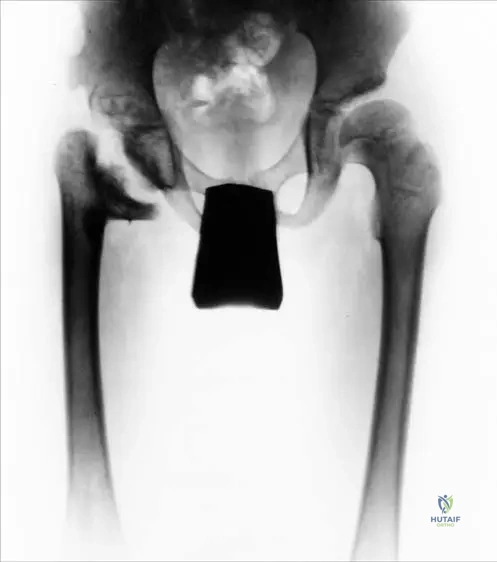
Rationale: Fig. 2.12 directly illustrates and describes the outcome: "the right femoral head and the neck are destroyed as a consequence of the newborn’s coxitis. The protruded lesser trochanter supports the deteriorated acetabulum. Severe hip deformity is already present at adolescent age." This destruction is often a result of avascular necrosis due to the inflammatory process and increased intra-articular pressure. While limb length discrepancy (A) and chronic osteomyelitis (C) can occur, the destruction of the femoral head and neck is a particularly devastating and characteristic long-term sequela highlighted by the image and text.
Question 3
A 4-month-old infant, previously treated for newborn's coxitis, undergoes follow-up radiographs. The images show changes consistent with osteomyelitis. In small children, what is the typical radiographic appearance of osteomyelitis?
View Answer & Explanation
Correct Answer: B
Rationale: The context for Fig. 2.10 states: "In small children osteomyelitis is a bone producing process, resulting in condensed, sclerotic bones, sometimes in overgrowth of the affected bone (b)." This describes the characteristic radiographic appearance in this age group, which can differ from osteomyelitis in older children or adults. Predominantly lytic lesions (A) are less typical for the chronic phase described here, and extensive soft tissue swelling (C) is an acute finding, not the bony change.
Question 4
A 6-week-old infant with a history of newborn's coxitis undergoes a CT scan due to persistent symptoms. The scan reveals a lytic site within a sclerotic zone, which is suspected to be filled with pus. What is the term for this specific radiographic finding?
View Answer & Explanation
Correct Answer: B
Rationale: The context for Fig. 2.10 explicitly defines this term: "Sequester is a lytic site inside the sclerotic zone, which is filled with pus, when surgically opened." A sequestrum (or sequester) is a piece of dead bone that has become separated from the surrounding healthy bone during necrosis. Brodie's abscess (A) is a specific type of chronic osteomyelitis, often in the metaphysis. Involucrum (C) is new bone formation around a sequestrum, and cloaca (D) is an opening in the involucrum. Osteophyte (E) is a bone spur.
Question 5
A 1-month-old infant presents with acute onset of fever and refusal to move the right leg. Physical examination reveals a painful, swollen right hip with limited range of motion. Ultrasound confirms a large joint effusion. If left untreated, what is the primary mechanism by which septic coxitis can lead to subluxation or complete dislocation of the femoral head in newborns?

View Answer & Explanation
Correct Answer: C
Rationale: The context for Fig. 2.9 states: "Because of pus formation in the hip joint, subluxation or complete dislocation of the femoral head may occur." The accumulation of pus within the confined joint space significantly increases intra-articular pressure, which can stretch and rupture the joint capsule and ligaments, leading to dislocation. While muscle spasm (D) can contribute to an antalgic position, the primary mechanical cause of dislocation is the pressure from the effusion.
Question 6
A 3-week-old infant is brought to the clinic by parents who report the baby has been unusually irritable and crying excessively, especially during diaper changes. On examination, the infant cries intensely when the left hip is gently moved. This finding is highly suggestive of a painful hip condition. What is the specific clinical sign described here that is characteristic of newborn's coxitis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly lists "painful hip movement (crying baby)" as a characteristic sign of newborn's coxitis. Ortolani and Barlow signs (A, B) are tests for developmental dysplasia of the hip, not typically for acute septic arthritis. Trendelenburg gait (D) and leg length discrepancy (E) are signs of chronic hip pathology, not acute presentation in a newborn.
Question 7
A 1-month-old infant presents with a high fever, lethargy, and a swollen, tender left hip. The infant holds the hip in a flexed, abducted, and externally rotated position. Given the highly septic nature of newborn's coxitis, what other systemic clinical finding is often observed?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text lists "lymphadenomegaly" as a characteristic finding of newborn's coxitis, indicating a systemic inflammatory response. While other systemic signs of sepsis (like tachycardia, hypotension, or even hypothermia in severe cases) can occur, lymphadenomegaly is specifically mentioned in the provided text as a characteristic feature of this condition.
Question 8
A 2-week-old infant is diagnosed with septic arthritis of the hip. The unique anatomy of the newborn's hip predisposes it to this condition. Specifically, the metaphyseal vessels, which carry bacteria, can directly penetrate into the epiphysis and the hip joint. What is the anatomical reason for this direct spread?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states: "The metaphyseal vessels of the femur contain bacteria, which may penetrate into the epiphysis and the hip joint, thus the metaphysis is localized intra-articular." This anatomical feature allows for direct communication between the infected metaphysis and the joint space, facilitating the spread of infection. While the femoral head is cartilaginous (A) and the acetabulum shallow (E), these are not the direct reasons for metaphyseal infection spreading *into* the joint.
Question 9
A 1-month-old infant presents with acute onset of fever and a painful, swollen left hip. Initial ultrasound confirms a large joint effusion and femoral head dislocation. Plain radiographs are also obtained. In the early stages of newborn's coxitis, what is the typical finding on plain radiographs?
View Answer & Explanation
Correct Answer: D
Rationale: While Fig. 2.10 shows radiographic progression over time, the text implies that early changes might be subtle. In the acute phase of septic arthritis in newborns, plain radiographs are often normal or show only subtle signs like soft tissue swelling or joint capsule distension, which are difficult to appreciate. Significant bone destruction and sclerosis (A) are later findings, as shown in Fig 2.10b and c. Ultrasound (as discussed in Q4) is superior for early detection of fluid and dislocation.
Question 10
A 2-month-old infant presents with fever, irritability, and decreased movement of the left lower extremity. Blood tests are performed, and the "Westergreen" level is reported as significantly elevated. What does "Westergreen" refer to in this clinical context?
View Answer & Explanation
Correct Answer: B
Rationale: The text states: "the lab tests show high Westergreen and white blood cell levels and a left shift in the qualitative blood test." "Westergreen" is a common historical and European term for the Westergren method of measuring the erythrocyte sedimentation rate (ESR), a non-specific marker of inflammation. While CRP (A) and Procalcitonin (C) are also inflammatory markers, and WBC (D) is mentioned separately, "Westergreen" specifically refers to ESR.
Question 11
A 1-month-old infant is admitted with suspected septic coxitis. A complete blood count (CBC) with differential is performed, revealing a "left shift" in the qualitative blood test. What does a "left shift" indicate in the context of a suspected bacterial infection?
View Answer & Explanation
Correct Answer: C
Rationale: A "left shift" refers to an increase in the number of immature neutrophils (such as band forms or metamyelocytes) in the peripheral blood. This is a classic indicator of an acute bacterial infection, where the bone marrow is rapidly producing and releasing neutrophils to combat the infection, leading to an increased proportion of less mature forms. An increase in mature neutrophils (A) is part of leukocytosis, but the "shift" specifically refers to immaturity. Lymphocyte predominance (D) is more typical of viral infections.
Question 12
A 3-week-old infant presents with fever and a painful, immobile right hip. Diagnostic workup confirms epiphyseal osteomyelitis associated with arthritis. What is the primary consequence of this specific pattern of infection in newborns and infants under 1 year?
View Answer & Explanation
Correct Answer: B
Rationale: The very first sentence of the provided text states: "In newborns and in infants under the age of 1 year, osteomyelitis affects the epiphyses and the joints, and it is associated with arthritis, which may result in articular destruction (epiphyseal osteomyelitis)." This highlights articular destruction as the primary and most severe consequence of this type of infection in this age group. While chronic pain (A) might follow, articular destruction is the direct pathological outcome.
Question 13
A 1-month-old infant is undergoing an ultrasound for suspected septic coxitis of the left hip. The sonographer notes a dilated joint
Question 13
A 1-month-old male infant presents with high fever, irritability, and refusal to move his left leg. On examination, the left hip is held in a flexion, abduction, and external rotation position, with severe pain on passive movement. Laboratory tests show elevated white blood cell count and Westergren sedimentation rate. An ultrasound of the hip reveals a dilated joint capsule with thick fluid formation and a dislocated femoral head.
View Answer & Explanation
Correct Answer: C
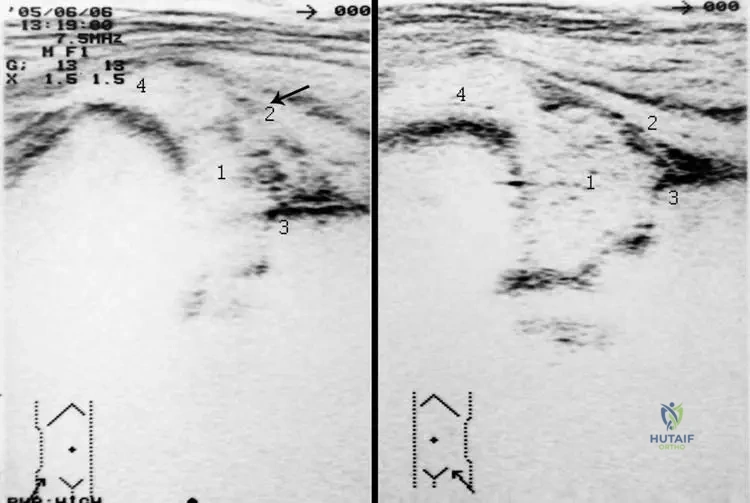
Rationale: The clinical presentation of high fever, irritability, a specific hip position (flexion, abduction, external rotation), painful movement, and laboratory findings of elevated inflammatory markers, coupled with ultrasound evidence of joint effusion and dislocation, are classic for septic arthritis (coxitis) in a newborn or infant. The image specifically shows a dilated capsule, thick fluid, and dislocated femoral head, consistent with septic coxitis. Transient synovitis typically presents with less systemic illness and inflammatory markers, and less severe imaging findings. DDH does not present with acute systemic illness or pain. Legg-Calvé-Perthes disease and Juvenile Idiopathic Arthritis are typically seen in older children and have different clinical and imaging characteristics.
Question 13
A 2-month-old female infant is diagnosed with septic coxitis of the right hip. Initial management includes intravenous antibiotics and emergent surgical drainage. Despite appropriate treatment, follow-up radiographs at 4 months show significant changes. Which of the following radiographic findings is characteristic of osteomyelitis in small children, as described in the context of newborn's coxitis?
View Answer & Explanation
Correct Answer: B
Rationale: The provided text states, "In small children osteomyelitis is a bone producing process, resulting in condensed, sclerotic bones, sometimes in overgrowth of the affected bone." This is a key distinguishing feature of osteomyelitis in this age group. Diffuse osteopenia is not typical. Multiple lytic lesions without sclerosis or periosteal reaction limited to the diaphysis do not fully capture the described bone-producing nature. Premature physeal closure is a potential long-term complication but not the primary characteristic radiographic finding of the active process.
Question 13
A 1-month-old male infant presents with a painful, swollen left hip held in flexion, abduction, and external rotation. He has a history of a "wet" umbilicus since birth. Laboratory tests confirm a septic condition. Given the common pathogens for newborn's coxitis, which two organisms are most likely to be identified?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "S. aureus and Haemophilus influenzae are the most common bacteria causing coxitis in newborns." This directly answers the question regarding the most likely pathogens. While other bacteria can cause infections in newborns, these two are specifically highlighted as the most common for coxitis in this age group. Group B Streptococcus is a common cause of neonatal sepsis but not specifically highlighted for coxitis in the text.
Question 13
A 3-week-old female infant is diagnosed with septic coxitis. An ultrasound of the affected hip shows a dilated joint capsule, fluid collection, and a dislocated femoral head. The cartilaginous acetabulum is noted to be lifted, and the greater trochanter is in a high position. The osseous acetabulum appears intact. What is the primary mechanism leading to femoral head dislocation in this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Because of pus formation in the hip joint, subluxation or complete dislocation of the femoral head may occur." The accumulation of pus significantly increases intra-articular pressure, which can stretch the joint capsule and ligaments, leading to subluxation or complete dislocation of the femoral head. While muscle spasm can contribute to the painful positioning, the primary mechanical cause of dislocation is the pressure from the effusion. Congenital ligamentous laxity is associated with DDH, not acute infection. Bacterial destruction of the acetabular rim is less common as a primary cause of acute dislocation compared to pressure from pus. Epiphyseal growth plate arrest is a long-term sequela, not an acute cause of dislocation.
Question 13
A 1-month-old male infant presents with signs and symptoms consistent with septic coxitis. Initial laboratory tests reveal a high white blood cell count and an elevated Westergren sedimentation rate. The qualitative blood test also shows a "left shift." What does a "left shift" in the qualitative blood test specifically indicate in this clinical context?
View Answer & Explanation
Correct Answer: C
Rationale: A "left shift" refers to an increase in the number of immature neutrophils (band forms) in the peripheral blood. This indicates that the bone marrow is rapidly producing and releasing neutrophils in response to a severe infection, often before they have fully matured. It is a classic sign of acute bacterial infection and systemic inflammation, consistent with the "highly septic condition" described for newborn's coxitis. It does not indicate a decrease in WBC count, an increase in mature neutrophils (though total neutrophils may be up), or changes in red blood cells or lymphocytes.
Question 13
A 6-week-old female infant is diagnosed with septic coxitis of the left hip. Despite initial treatment, the infection progresses, leading to significant bone changes. Radiographs taken at 4 months show a lytic site within a sclerotic zone, which is described as being filled with pus when surgically opened. What is the specific term for this radiographic finding?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly defines a "Sequester" as "a lytic site inside the sclerotic zone, which is filled with pus, when surgically opened." This directly matches the description in the question. A Brodie's abscess is a subacute osteomyelitis, typically in the metaphysis. An involucrum is new bone formation around necrotic bone. A cloaca is an opening in the involucrum allowing pus to drain. An osteophyte is a bone spur, unrelated to infection.
Question 13
A 1-month-old male infant presents with a septic hip. The clinical context describes that in newborns, the metaphyseal vessels of the femur contain bacteria, which may penetrate into the epiphysis and the hip joint. This is due to a unique anatomical feature where the metaphysis is localized intra-articular. What is the primary clinical implication of this anatomical relationship in newborn's coxitis?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "the metaphyseal vessels of the femur contain bacteria, which may penetrate into the epiphysis and the hip joint, thus the metaphysis is localized intra-articular." This anatomical arrangement allows for the direct spread of infection from the metaphysis into the joint space, leading to septic arthritis. This is a critical factor in the pathogenesis of newborn's coxitis. While avascular necrosis can be a complication, the direct spread of infection is the primary implication of the intra-articular metaphysis. It does not enhance antibiotic penetration, reduce effusion, or protect the physis; in fact, it puts the physis at risk.
Question 13
A 2-month-old female infant is diagnosed with septic coxitis. Despite aggressive medical and surgical management, she develops severe long-term sequelae. At adolescent age, radiographs show destruction of the femoral head and neck, with a protruded lesser trochanter supporting a deteriorated acetabulum. What is the most likely cause of this severe hip deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The text and Fig 2.12 explicitly describe this outcome as a "consequence of the newborn’s coxitis," specifically mentioning "the right femoral head and the neck are destroyed." Septic arthritis in newborns can lead to severe articular cartilage destruction, epiphyseal damage, and growth plate involvement, resulting in significant long-term deformity and growth disturbances. The other options represent different pathologies not directly linked to the described sequelae of newborn's coxitis.
Question 13
A 1-month-old male infant presents with a painful, swollen hip and high fever. Physical examination reveals limited range of motion and a characteristic flexion-abduction-external rotation position of the affected hip. Which of the following is the most appropriate initial diagnostic imaging modality for evaluating suspected septic coxitis in this age group?
View Answer & Explanation
Correct Answer: D
Rationale: The text and accompanying images (Fig 2.8) highlight ultrasound as a crucial diagnostic tool for newborn's coxitis, showing findings like a dilated capsule, fluid formation, and femoral head dislocation. Ultrasound is non-invasive, does not involve radiation, and is excellent for detecting joint effusions and assessing cartilaginous structures in infants. While plain radiographs are often obtained, they may be normal in early stages (Fig 2.10a) and are less sensitive for early effusion. MRI and CT scans are more detailed but involve sedation and/or radiation, making ultrasound the preferred initial imaging modality for suspected septic hip in infants.
Question 13
A 6-week-old female infant is diagnosed with septic coxitis. The infection is believed to be hematogenously transmitted. The text mentions several potential primary infection sites. Which of the following is explicitly listed as a common primary source for bacterial transmission in newborn's coxitis?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "The bacteria are transmitted hematogenously, and the primary infection is mostly in a discharging ('wet') umbilicus, bacterial skin inflammation or otitis." Therefore, a discharging ("wet") umbilicus is a direct answer from the provided information. While other infections can occur in newborns, the question asks for what is explicitly listed in the context.
Question 13
A 1-month-old male infant presents with a painful, swollen left hip and high fever. Ultrasound confirms septic coxitis with a large effusion. Given the "highly septic condition" described, what is the most critical immediate management step after diagnosis and initiation of empiric antibiotics?
View Answer & Explanation
Correct Answer: C
Rationale: Septic arthritis of the hip in a newborn is an orthopedic emergency. The "highly septic condition" and the risk of rapid articular destruction and femoral head necrosis necessitate emergent surgical drainage of the hip joint to remove pus, decompress the joint, and obtain cultures. While antibiotics are crucial, drainage is equally vital to prevent devastating long-term sequelae. A Pavlik harness is for DDH. Observation alone is insufficient. NSAIDs are for pain but don't address the infection. Physical therapy is for rehabilitation, not acute management.
Question 13
A 3-week-old female infant is diagnosed with septic coxitis. Ultrasound findings include a dilated joint capsule, thick fluid formation, and a dislocated femoral head. The cartilaginous acetabulum is noted to be lifted (Fig 2.8a, labeled '2'). What is the significance of the lifted cartilaginous acetabulum in this context?
View Answer & Explanation
Correct Answer: C
Rationale: The lifting of the cartilaginous acetabulum (labeled '2' in Fig 2.8a) is a secondary effect caused by the significant joint effusion (thick fluid formation) and the superior displacement of the femoral head due to the increased intra-articular pressure and dislocation. It is not a primary developmental anomaly, a normal variant, or indicative of a benign condition in the context of septic coxitis. It is a sign of the severe pressure and displacement within the joint.
Question 13
A 1-month-old male infant presents with a septic hip. Radiographs taken at presentation may appear normal (Fig 2.10a). However, if the infection progresses, later radiographs (Fig 2.10b, c) show condensed, sclerotic bones and sometimes overgrowth. Which of the following additional diagnostic tools is specifically mentioned as useful for evaluating the extent of bone involvement, especially in cases with sequester formation?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Diagnostic tools are plain radiographs, fistulography and CT scans." CT scans are particularly useful for visualizing bone detail, including sclerotic changes, lytic lesions, and the presence of a sequester, which can be difficult to fully appreciate on plain radiographs alone. While MRI is excellent for soft tissue and marrow edema, CT is specifically mentioned for bone detail in this context. Arthrography and bone scintigraphy are not explicitly mentioned as primary tools for sequester evaluation in the text, and EMG is for muscle/nerve function.
Question 13
A 2-month-old female infant is diagnosed with septic coxitis. The infection is being treated with appropriate antibiotics and surgical drainage. Given the potential for severe long-term sequelae, what is the primary goal of early and aggressive management in newborn's coxitis?
View Answer & Explanation
Correct Answer: C
Rationale: The text highlights that newborn's coxitis "may result in articular destruction (epiphyseal osteomyelitis)" and shows images of severe femoral head and neck destruction (Fig 2.12). Therefore, the primary goal of early and aggressive management (antibiotics and drainage) is to preserve the delicate cartilaginous femoral head and acetabulum, which are highly susceptible to damage from infection and increased intra-articular pressure, thereby preventing devastating long-term deformities and functional impairment. While other options may be secondary benefits, preserving joint integrity is paramount.
Question 13
A 1-month-old male infant presents with a painful, swollen hip and high fever. The clinical picture is highly suggestive of septic coxitis. Which of the following physical examination findings, explicitly mentioned in the text, is characteristic of this condition?

View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly lists "painful hip movement (crying baby), limited range of motion" as characteristic of the condition. Fig 2.7 also shows the hip held in a painful position when moved passively. Ortolani and Barlow signs are associated with Developmental Dysplasia of the Hip, not acute infection. Leg length discrepancy is a chronic sequela, not an acute finding. High fever is characteristic, so absence of fever is incorrect. A normal gait pattern is impossible in a crying infant with a painful, septic hip.
Question 13
A 2-month-old female infant is diagnosed with septic coxitis. The infection is believed to be hematogenously transmitted. Besides a discharging umbilicus, which other primary infection sites are mentioned in the text as potential sources for the bacteria?
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "The bacteria are transmitted hematogenously, and the primary infection is mostly in a discharging ('wet') umbilicus, bacterial skin inflammation or otitis." Therefore, otitis and bacterial skin inflammation are explicitly mentioned as other primary sources. While other infections can occur, the question asks for those specifically listed in the provided text.
Question 13
A 1-month-old male infant is being evaluated for suspected septic coxitis. An ultrasound of the hip is performed (Fig 2.8a). The image shows the greater trochanter in a high position (labeled '4'). What does this finding most directly suggest?
View Answer & Explanation
Correct Answer: B
Rationale: The image (Fig 2.8a) explicitly labels the femoral head as dislocated ('1') and the greater trochanter in a high position ('4'). When the femoral head dislocates superiorly and/or posteriorly, the greater trochanter, which is part of the proximal femur, will also be displaced superiorly relative to the acetabulum. This finding is a direct consequence and indicator of femoral head subluxation or dislocation, which is common in septic coxitis due to joint effusion and pressure. It is not a normal variant or a primary congenital anomaly in this context.
Question 13
A 6-week-old female infant is diagnosed with septic coxitis. Radiographs taken at 6 weeks (Fig 2.10b) show condensed, sclerotic bones and potential overgrowth of the affected bone. The text describes osteomyelitis in small children as a "bone producing process." How does this characteristic differ from osteomyelitis typically seen in older children or adults?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifically highlights that in small children, osteomyelitis is a "bone producing process, resulting in condensed, sclerotic bones, sometimes in overgrowth." In contrast, osteomyelitis in older children and adults often presents with more pronounced lytic destruction and less exuberant new bone formation (sclerosis/overgrowth) in the acute phase, although chronic osteomyelitis can also involve sclerosis. Epiphyseal involvement is more characteristic of newborns/infants due to vascular anatomy. Sequestra can occur in all age groups with chronic osteomyelitis.
Question 13
A 1-month-old male infant presents with a septic hip. The clinical picture is consistent with newborn's coxitis. Given the "highly septic condition" and the risk of rapid joint destruction, what is the most appropriate initial empiric antibiotic regimen for this patient, considering the most common pathogens?
View Answer & Explanation
Correct Answer: B
Rationale: The most common pathogens for newborn's coxitis are *S. aureus* and *Haemophilus influenzae*. Given the "highly septic condition" and the need
Question 14
A 1-month-old male infant presents with high fever, irritability, and refusal to move his left leg. On examination, the left hip is held in a flexion, abduction, and external rotation position, with severe pain on passive movement. Laboratory tests show elevated white blood cell count and Westergren sedimentation rate. An ultrasound of the hip reveals a dilated joint capsule with thick fluid formation and a dislocated femoral head.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of high fever, irritability, a specific hip position (flexion, abduction, external rotation), painful movement, and laboratory findings of elevated inflammatory markers, coupled with ultrasound evidence of joint effusion and dislocation, are classic for septic arthritis (coxitis) in a newborn or infant. The image specifically shows a dilated capsule, thick fluid, and dislocated femoral head, consistent with septic coxitis. Transient synovitis typically presents with less systemic illness and inflammatory markers, and less severe imaging findings. DDH does not present with acute systemic illness or pain. Legg-Calvé-Perthes disease and Juvenile Idiopathic Arthritis are typically seen in older children and have different clinical and imaging characteristics.
Question 15
A 2-month-old female infant is diagnosed with septic coxitis of the right hip. Initial management includes intravenous antibiotics and emergent surgical drainage. Despite appropriate treatment, follow-up radiographs at 4 months show significant changes. Which of the following radiographic findings is characteristic of osteomyelitis in small children, as described in the context of newborn's coxitis?
View Answer & Explanation
Correct Answer: B
Rationale: The provided text states, "In small children osteomyelitis is a bone producing process, resulting in condensed, sclerotic bones, sometimes in overgrowth of the affected bone." This is a key distinguishing feature of osteomyelitis in this age group. Diffuse osteopenia is not typical. Multiple lytic lesions without sclerosis or periosteal reaction limited to the diaphysis do not fully capture the described bone-producing nature. Premature physeal closure is a potential long-term complication but not the primary characteristic radiographic finding of the active process.
Question 16
A 1-month-old male infant presents with a painful, swollen left hip held in flexion, abduction, and external rotation. He has a history of a "wet" umbilicus since birth. Laboratory tests confirm a septic condition. Given the common pathogens for newborn's coxitis, which two organisms are most likely to be identified?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "S. aureus and Haemophilus influenzae are the most common bacteria causing coxitis in newborns." This directly answers the question regarding the most likely pathogens. While other bacteria can cause infections in newborns, these two are specifically highlighted as the most common for coxitis in this age group. Group B Streptococcus is a common cause of neonatal sepsis but not specifically highlighted for coxitis in the text.
Question 17
A 3-week-old female infant is diagnosed with septic coxitis. An ultrasound of the affected hip shows a dilated joint capsule, fluid collection, and a dislocated femoral head. The cartilaginous acetabulum is noted to be lifted, and the greater trochanter is in a high position. The osseous acetabulum appears intact. What is the primary mechanism leading to femoral head dislocation in this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Because of pus formation in the hip joint, subluxation or complete dislocation of the femoral head may occur." The accumulation of pus significantly increases intra-articular pressure, which can stretch the joint capsule and ligaments, leading to subluxation or complete dislocation of the femoral head. While muscle spasm can contribute to the painful positioning, the primary mechanical cause of dislocation is the pressure from the effusion. Congenital ligamentous laxity is associated with DDH, not acute infection. Bacterial destruction of the acetabular rim is less common as a primary cause of acute dislocation compared to pressure from pus. Epiphyseal growth plate arrest is a long-term sequela, not an acute cause of dislocation.
Question 18
A 1-month-old male infant presents with signs and symptoms consistent with septic coxitis. Initial laboratory tests reveal a high white blood cell count and an elevated Westergren sedimentation rate. The qualitative blood test also shows a "left shift." What does a "left shift" in the qualitative blood test specifically indicate in this clinical context?
View Answer & Explanation
Correct Answer: C
Rationale: A "left shift" refers to an increase in the number of immature neutrophils (band forms) in the peripheral blood. This indicates that the bone marrow is rapidly producing and releasing neutrophils in response to a severe infection, often before they have fully matured. It is a classic sign of acute bacterial infection and systemic inflammation, consistent with the "highly septic condition" described for newborn's coxitis. It does not indicate a decrease in WBC count, an increase in mature neutrophils (though total neutrophils may be up), or changes in red blood cells or lymphocytes.
Question 19
A 6-week-old female infant is diagnosed with septic coxitis of the left hip. Despite initial treatment, the infection progresses, leading to significant bone changes. Radiographs taken at 4 months show a lytic site within a sclerotic zone, which is described as being filled with pus when surgically opened. What is the specific term for this radiographic finding?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly defines a "Sequester" as "a lytic site inside the sclerotic zone, which is filled with pus, when surgically opened." This directly matches the description in the question. A Brodie's abscess is a subacute osteomyelitis, typically in the metaphysis. An involucrum is new bone formation around necrotic bone. A cloaca is an opening in the involucrum allowing pus to drain. An osteophyte is a bone spur, unrelated to infection.
Question 20
A 1-month-old male infant presents with a septic hip. The clinical context describes that in newborns, the metaphyseal vessels of the femur contain bacteria, which may penetrate into the epiphysis and the hip joint. This is due to a unique anatomical feature where the metaphysis is localized intra-articular. What is the primary clinical implication of this anatomical relationship in newborn's coxitis?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "the metaphyseal vessels of the femur contain bacteria, which may penetrate into the epiphysis and the hip joint, thus the metaphysis is localized intra-articular." This anatomical arrangement allows for the direct spread of infection from the metaphysis into the joint space, leading to septic arthritis. This is a critical factor in the pathogenesis of newborn's coxitis. While avascular necrosis can be a complication, the direct spread of infection is the primary implication of the intra-articular metaphysis. It does not enhance antibiotic penetration, reduce effusion, or protect the physis; in fact, it puts the physis at risk.
Question 21
A 2-month-old female infant is diagnosed with septic coxitis. Despite aggressive medical and surgical management, she develops severe long-term sequelae. At adolescent age, radiographs show destruction of the femoral head and neck, with a protruded lesser trochanter supporting a deteriorated acetabulum. What is the most likely cause of this severe hip deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The text and Fig 2.12 explicitly describe this outcome as a "consequence of the newborn’s coxitis," specifically mentioning "the right femoral head and the neck are destroyed." Septic arthritis in newborns can lead to severe articular cartilage destruction, epiphyseal damage, and growth plate involvement, resulting in significant long-term deformity and growth disturbances. The other options represent different pathologies not directly linked to the described sequelae of newborn's coxitis.
Question 22
A 1-month-old male infant presents with a painful, swollen hip and high fever. Physical examination reveals limited range of motion and a characteristic flexion-abduction-external rotation position of the affected hip. Which of the following is the most appropriate initial diagnostic imaging modality for evaluating suspected septic coxitis in this age group?
View Answer & Explanation
Correct Answer: D
Rationale: The text and accompanying images (Fig 2.8) highlight ultrasound as a crucial diagnostic tool for newborn's coxitis, showing findings like a dilated capsule, fluid formation, and femoral head dislocation. Ultrasound is non-invasive, does not involve radiation, and is excellent for detecting joint effusions and assessing cartilaginous structures in infants. While plain radiographs are often obtained, they may be normal in early stages (Fig 2.10a) and are less sensitive for early effusion. MRI and CT scans are more detailed but involve sedation and/or radiation, making ultrasound the preferred initial imaging modality for suspected septic hip in infants.
Question 23
A 6-week-old female infant is diagnosed with septic coxitis. The infection is believed to be hematogenously transmitted. The text mentions several potential primary infection sites. Which of the following is explicitly listed as a common primary source for bacterial transmission in newborn's coxitis?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "The bacteria are transmitted hematogenously, and the primary infection is mostly in a discharging ('wet') umbilicus, bacterial skin inflammation or otitis." Therefore, a discharging ("wet") umbilicus is a direct answer from the provided information. While other infections can occur in newborns, the question asks for what is explicitly listed in the context.
Question 24
A 1-month-old male infant presents with a painful, swollen left hip and high fever. Ultrasound confirms septic coxitis with a large effusion. Given the "highly septic condition" described, what is the most critical immediate management step after diagnosis and initiation of empiric antibiotics?
View Answer & Explanation
Correct Answer: C
Rationale: Septic arthritis of the hip in a newborn is an orthopedic emergency. The "highly septic condition" and the risk of rapid articular destruction and femoral head necrosis necessitate emergent surgical drainage of the hip joint to remove pus, decompress the joint, and obtain cultures. While antibiotics are crucial, drainage is equally vital to prevent devastating long-term sequelae. A Pavlik harness is for DDH. Observation alone is insufficient. NSAIDs are for pain but don't address the infection. Physical therapy is for rehabilitation, not acute management.
Question 25
A 3-week-old female infant is diagnosed with septic coxitis. Ultrasound findings include a dilated joint capsule, thick fluid formation, and a dislocated femoral head. The cartilaginous acetabulum is noted to be lifted (Fig 2.8a, labeled '2'). What is the significance of the lifted cartilaginous acetabulum in this context?
View Answer & Explanation
Correct Answer: C
Rationale: The lifting of the cartilaginous acetabulum (labeled '2' in Fig 2.8a) is a secondary effect caused by the significant joint effusion (thick fluid formation) and the superior displacement of the femoral head due to the increased intra-articular pressure and dislocation. It is not a primary developmental anomaly, a normal variant, or indicative of a benign condition in the context of septic coxitis. It is a sign of the severe pressure and displacement within the joint.
Question 26
A 1-month-old male infant presents with a septic hip. Radiographs taken at presentation may appear normal (Fig 2.10a). However, if the infection progresses, later radiographs (Fig 2.10b, c) show condensed, sclerotic bones and sometimes overgrowth. Which of the following additional diagnostic tools is specifically mentioned as useful for evaluating the extent of bone involvement, especially in cases with sequester formation?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Diagnostic tools are plain radiographs, fistulography and CT scans." CT scans are particularly useful for visualizing bone detail, including sclerotic changes, lytic lesions, and the presence of a sequester, which can be difficult to fully appreciate on plain radiographs alone. While MRI is excellent for soft tissue and marrow edema, CT is specifically mentioned for bone detail in this context. Arthrography and bone scintigraphy are not explicitly mentioned as primary tools for sequester evaluation in the text, and EMG is for muscle/nerve function.
Question 27
A 2-month-old female infant is diagnosed with septic coxitis. The infection is being treated with appropriate antibiotics and surgical drainage. Given the potential for severe long-term sequelae, what is the primary goal of early and aggressive management in newborn's coxitis?
View Answer & Explanation
Correct Answer: C
Rationale: The text highlights that newborn's coxitis "may result in articular destruction (epiphyseal osteomyelitis)" and shows images of severe femoral head and neck destruction (Fig 2.12). Therefore, the primary goal of early and aggressive management (antibiotics and drainage) is to preserve the delicate cartilaginous femoral head and acetabulum, which are highly susceptible to damage from infection and increased intra-articular pressure, thereby preventing devastating long-term deformities and functional impairment. While other options may be secondary benefits, preserving joint integrity is paramount.
Question 28
A 1-month-old male infant presents with a painful, swollen hip and high fever. The clinical picture is highly suggestive of septic coxitis. Which of the following physical examination findings, explicitly mentioned in the text, is characteristic of this condition?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly lists "painful hip movement (crying baby), limited range of motion" as characteristic of the condition. Fig 2.7 also shows the hip held in a painful position when moved passively. Ortolani and Barlow signs are associated with Developmental Dysplasia of the Hip, not acute infection. Leg length discrepancy is a chronic sequela, not an acute finding. High fever is characteristic, so absence of fever is incorrect. A normal gait pattern is impossible in a crying infant with a painful, septic hip.
Question 29
A 2-month-old female infant is diagnosed with septic coxitis. The infection is believed to be hematogenously transmitted. Besides a discharging umbilicus, which other primary infection sites are mentioned in the text as potential sources for the bacteria?
View Answer & Explanation
Correct Answer: A
Rationale: The text states, "The bacteria are transmitted hematogenously, and the primary infection is mostly in a discharging ('wet') umbilicus, bacterial skin inflammation or otitis." Therefore, otitis and bacterial skin inflammation are explicitly mentioned as other primary sources. While other infections can occur, the question asks for those specifically listed in the provided text.
Question 30
A 1-month-old male infant is being evaluated for suspected septic coxitis. An ultrasound of the hip is performed (Fig 2.8a). The image shows the greater trochanter in a high position (labeled '4'). What does this finding most directly suggest?
View Answer & Explanation
Correct Answer: B
Rationale: The image (Fig 2.8a) explicitly labels the femoral head as dislocated ('1') and the greater trochanter in a high position ('4'). When the femoral head dislocates superiorly and/or posteriorly, the greater trochanter, which is part of the proximal femur, will also be displaced superiorly relative to the acetabulum. This finding is a direct consequence and indicator of femoral head subluxation or dislocation, which is common in septic coxitis due to joint effusion and pressure. It is not a normal variant or a primary congenital anomaly in this context.
Question 31
A 6-week-old female infant is diagnosed with septic coxitis. Radiographs taken at 6 weeks (Fig 2.10b) show condensed, sclerotic bones and potential overgrowth of the affected bone. The text describes osteomyelitis in small children as a "bone producing process." How does this characteristic differ from osteomyelitis typically seen in older children or adults?
View Answer & Explanation
Correct Answer: C
Rationale: The text specifically highlights that in small children, osteomyelitis is a "bone producing process, resulting in condensed, sclerotic bones, sometimes in overgrowth." In contrast, osteomyelitis in older children and adults often presents with more pronounced lytic destruction and less exuberant new bone formation (sclerosis/overgrowth) in the acute phase, although chronic osteomyelitis can also involve sclerosis. Epiphyseal involvement is more characteristic of newborns/infants due to vascular anatomy. Sequestra can occur in all age groups with chronic osteomyelitis.
Question 32
A 17-year-old male presents with a 6-month history of intermittent back pain. Radiographs reveal a lesion in the posterior elements of the lumbar spine. Biopsy confirms a benign bone tumor.
View Answer & Explanation
Correct Answer: B
Rationale: The provided text explicitly states, "Osteoblastoma is a rare benign bone tumor." It is a bone-forming tumor, distinguishing it from cartilaginous or metastatic lesions. Option A is incorrect as osteoblastoma is benign, not malignant.
Question 33
A 19-year-old male reports persistent, dull pain in his sacrum for several months. Physical examination is unremarkable. Radiographs show a sclerotic lesion in the left sacrum.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "The usual age of onset is adolescence to early adulthood, but the clinical presentation is variable. Males are aff ected more commonly than females." This demographic aligns with the patient in the vignette.
Question 34
A 22-year-old female presents with a 3-month history of increasing pain in her cervical spine. Initial radiographs showed a subtle lesion, but follow-up imaging 3 months later demonstrates significant expansion.
View Answer & Explanation
Correct Answer: B
Rationale: The text notes, "Th e clinical course is usually slow and indolent, but osteoblastomas can progress rapidly, mimicking a malignant process." This rapid progression can be a diagnostic challenge.
Question 35
A 15-year-old male presents with chronic low back pain and muscle spasm. Physical exam reveals a painful scoliosis. Radiographs of the lumbar spine show an expansile lesion.
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "Spinal osteoblastomas occur in the posterior elements." This is a classic location for osteoblastoma in the spine.
Question 36
A 20-year-old male presents with deep-seated pain in his left buttock. Radiographs of the pelvis are obtained.

View Answer & Explanation
Correct Answer: B
Rationale: The clinical context for Fig. 8.12 states, "AP radiograph of the pelvis shows a densely sclerotic osteoblastoma in the left sacrum. Due to the extent of sclerosis, this lesion was initially mistaken for an osteosarcoma."
Question 37
A 16-year-old male undergoes biopsy for a lytic lesion in his lumbar spine. The pathologist reviews the low-power photomicrograph.
View Answer & Explanation
Correct Answer: C
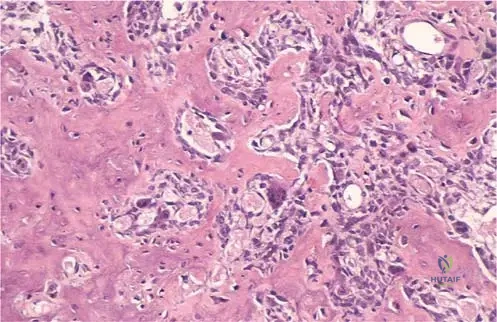
Rationale: The clinical context for Fig. 8.17 directly identifies this image as a "Photomicrograph of osteoblastoma. The lowpower fi gure demonstrates a permeative growth pattern, with mature cortical bone on the left surrounded by osteoblastoma."
Question 38
A 21-year-old female has a biopsy of a sclerotic lesion in her cervical spine. The pathologist examines the high-power photomicrograph.
View Answer & Explanation
Correct Answer: C
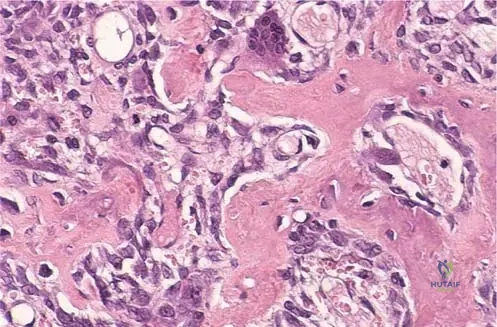
Rationale: The clinical context for Fig. 8.18 states, "Photomicrograph of osteoblastoma. Osteoblastomas typically have loose, fi brovascular connective tissue intermixed with irregular osteoid. Mitotic fi gures may be present." These are classic histological features of osteoblastoma.
Question 39
A 17-year-old male presents with chronic neck pain. Radiographs of his cervical spine show a sclerotic lesion in the posterior elements. Another 15-year-old male presents with low back pain, and radiographs show a lytic lesion in the lumbar posterior elements.
View Answer & Explanation
Correct Answer: C
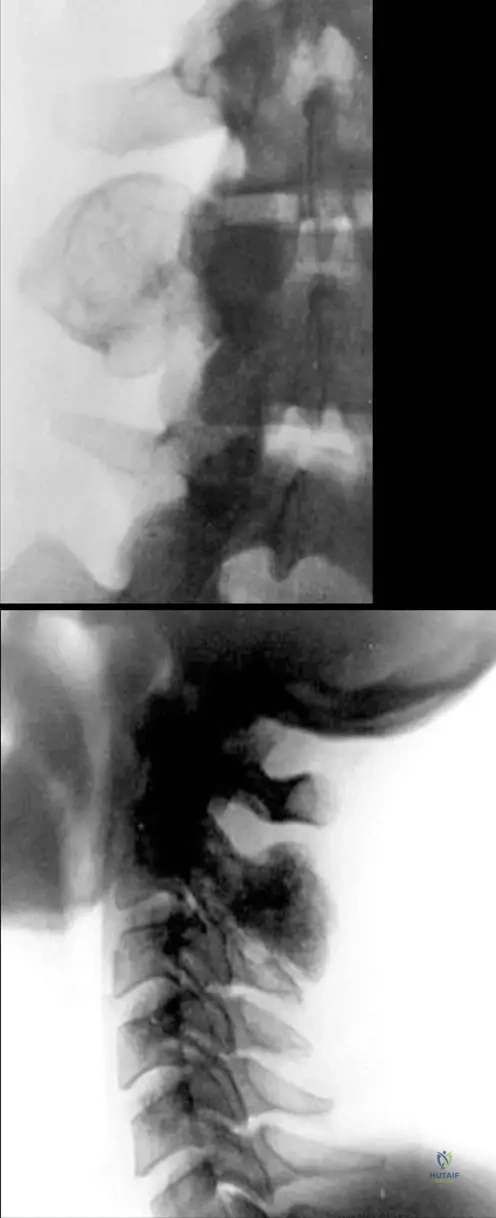
Rationale: The clinical context for Fig. 8.16 states, "Osteoblastoma in the spine are typically expansile, but may be primarily lytic (a) or sclerotic (b)." This highlights the variable radiographic appearance.
Question 40
A 14-year-old male presents with a 4-month history of intermittent pain in his thoracic spine. The pain is not relieved by over-the-counter analgesics. Physical exam shows mild tenderness.
- A) Constant, severe, nocturnal pain relieved by NSAIDs
- B) Intermittent episodes of pain
- C) Pain only with strenuous activity
- D)
Question 40
A 16-year-old male presents with a 6-month history of intermittent, dull pain in his lower back that is worse at night. He reports that the pain sometimes resolves completely for a few days before returning. Physical examination reveals mild tenderness to palpation over the lumbar spine. Radiographs are pending.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states that patients with osteoblastoma often complain of "intermittent episodes of pain," which aligns with the description of pain with periods of resolution. This characteristic intermittent nature is a key feature. Constant, severe pain (A) or pain consistently worse in the morning (B) are less typical for osteoblastoma, and sharp radiating pain (D) is more suggestive of nerve root compression. Pain primarily associated with weight-bearing (E) is non-specific.
Question 40
A 19-year-old male presents with chronic, progressive pain in his cervical spine. Imaging reveals an expansile lesion in the posterior elements. Based on the typical epidemiology of osteoblastoma, which of the following patient demographics is most commonly affected?
View Answer & Explanation
Correct Answer: D
Rationale: The provided text explicitly states, "The usual age of onset is adolescence to early adulthood... Males are affected more commonly than females." This directly supports males in adolescence to early adulthood as the most commonly affected demographic. Other options contradict either the age range or gender predominance.
Question 40
A 17-year-old male presents with persistent back pain and muscle spasm. Radiographs of the lumbar spine show a lytic lesion. Given the typical spinal location for osteoblastoma, which anatomical region is most likely involved?

View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states, "Spinal osteoblastomas occur in the posterior elements." This makes the posterior elements the most typical location for osteoblastomas within the spine. While other structures might be secondarily affected, the primary involvement is in the posterior elements, as shown in Fig. 8.16.
Question 40
A 22-year-old female presents with chronic neck pain. Lateral radiographs of the cervical spine reveal a sclerotic lesion in the posterior elements. Based on the provided information, what is a characteristic radiographic appearance of osteoblastoma in the spine?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 8.16 and its caption state, "Osteoblastoma in the spine are typically expansile, but may be primarily lytic (a) or sclerotic (b)." This indicates a variable radiographic appearance, encompassing expansile, lytic, and sclerotic patterns. Options A, B, D, and E describe overly restrictive or incorrect radiographic features for osteoblastoma.
Question 40
A 25-year-old male presents with left buttock pain. An AP radiograph of the pelvis reveals a densely sclerotic lesion in the left sacrum, as shown. Due to its appearance, the lesion was initially mistaken for a more aggressive tumor. Which of the following conditions was it initially mistaken for?
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 8.12 explicitly states, "Due to the extent of sclerosis, this lesion was initially mistaken for an osteosarcoma." Osteosarcoma is a malignant bone tumor that can present with significant sclerosis, leading to this diagnostic confusion. The other options are typically benign lesions with different radiographic characteristics (e.g., enchondroma, fibrous dysplasia, NOF, SBC are generally lytic or mixed, not densely sclerotic to the extent of mimicking osteosarcoma).
Question 40
A 15-year-old male undergoes biopsy for a painful spinal lesion. Histopathological examination is performed. Which of the following microscopic features is characteristic of osteoblastoma?

View Answer & Explanation
Correct Answer: C
Rationale: The text and Fig. 8.18 caption state, "Osteoblastomas typically have loose, fibrovascular connective tissue intermixed with irregular osteoid." This is the defining histological characteristic. The other options describe features of different bone tumors (e.g., plasma cells for multiple myeloma, chondrocytes for chondrosarcoma/enchondroma, giant cells for giant cell tumor).
Question 40
A 20-year-old female presents with a 3-month history of increasing pain and swelling in her sacrum. Initial radiographs showed a subtle lytic lesion, but follow-up imaging 3 months later demonstrates significant progression and sclerosis. What is a known characteristic of the clinical course of osteoblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states, "The clinical course is usually slow and indolent, but osteoblastomas can progress rapidly, mimicking a malignant process." This highlights the potential for aggressive behavior despite its benign nature. Options A, B, D, and E contradict this variability and potential for rapid progression.
Question 40
A 14-year-old male presents with chronic back pain and a noticeable curvature of his spine. Physical examination reveals muscle spasm in the paraspinal region and a painful scoliosis. Which of the following is a recognized physical finding associated with spinal osteoblastomas?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Patients have minimal physical findings, although some have muscle atrophy or muscle spasm. Spinal osteoblastomas occur in the posterior elements; muscle spasm in this area can lead to a painful scoliosis." This directly supports muscle atrophy, spasm, and painful scoliosis as physical findings. The other options are not described as typical physical findings for osteoblastoma in the provided text.
Question 40
A 18-year-old female undergoes a biopsy of a sacral lesion. The photomicrograph, as shown, demonstrates a specific growth pattern where the tumor infiltrates existing bone. What is this growth pattern called?

View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 8.17 explicitly states, "The lowpower figure demonstrates a permeative growth pattern, with mature cortical bone on the left surrounded by osteoblastoma." Permeative growth describes the infiltration of tumor cells through existing bone, which can be seen in both benign and malignant lesions. The other options describe different growth patterns or processes.
Question 40
A 16-year-old male presents with a 4-month history of increasing pain in his lumbar spine. Radiographs, as shown, reveal a lytic lesion in the posterior elements. What is a common characteristic of osteoblastomas in the spine, as illustrated by this image?
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 8.16 states, "Osteoblastoma in the spine are typically expansile, but may be primarily lytic (a) or sclerotic (b)." This indicates that expansile growth is a common feature, even if the lesion can also be lytic or sclerotic. Options A, C, D, and E are incorrect based on the provided text and images.
Question 40
A 21-year-old male presents with a rapidly growing, painful mass in his sacrum. Initial biopsy results are inconclusive, and the clinical picture suggests an aggressive process. Despite being a benign tumor, osteoblastoma can sometimes present with a clinical course that mimics which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "The clinical course is usually slow and indolent, but osteoblastomas can progress rapidly, mimicking a malignant process." This highlights the potential for osteoblastoma to present aggressively, leading to concern for malignancy. The other options describe conditions that are generally not mimicked by the rapid progression of an osteoblastoma.
Question 40
A 23-year-old female presents with chronic lower back pain. An AP radiograph of the pelvis, as shown, reveals a densely sclerotic lesion in the left sacrum. What is the most likely diagnosis for this lesion, given its appearance and location?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 8.12 is explicitly labeled as "AP radiograph of the pelvis shows a densely sclerotic osteoblastoma in the left sacrum." Therefore, osteoblastoma is the correct diagnosis. While other tumors can occur in the sacrum, the image directly identifies this specific lesion as an osteoblastoma, and its sclerotic nature is a known presentation.
Question 40
A 17-year-old male undergoes a biopsy of a spinal lesion. Histopathological examination, as shown, reveals loose fibrovascular connective tissue intermixed with irregular osteoid. The pathologist notes the presence of mitotic figures. What is the significance of mitotic figures in the context of osteoblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 8.18 states, "Mitotic figures may be present." This indicates that their presence is not uncommon in osteoblastoma, a benign tumor, and therefore does not automatically signify malignancy. It's important for pathologists to recognize that mitotic activity can be seen in benign osteoblastomas without necessarily implying malignant transformation.
Question 40
A 15-year-old female presents with a 9-month history of intermittent pain in her thoracic spine. Imaging reveals an expansile lesion in the posterior elements. Based on the overall classification, osteoblastoma is best described as which type of bone tumor?
View Answer & Explanation
Correct Answer: C
Rationale: The very first sentence of the clinical text states, "Osteoblastoma is a rare benign bone tumor." This directly classifies it as a benign bone tumor. The other options describe different categories of tumors.
Question 40
A 17-year-old male presents with chronic lower back pain. An AP radiograph of the lumbar spine, as shown, reveals a lytic lesion in the posterior elements. What is the predominant radiographic characteristic of this specific osteoblastoma in the lumbar spine?
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 8.16 states, "AP radiographs of the lumbar spine (a) and lateral radiographs of the cervical spine (b) both illustrate osteoblastomas... Osteoblastoma in the spine are typically expansile, but may be primarily lytic (a) or sclerotic (b)." Image (a) specifically shows a lytic lesion in the lumbar spine. Therefore, this osteoblastoma is primarily lytic.
Question 40
A 20-year-old female presents with chronic neck pain. A lateral radiograph of the cervical spine, as shown, illustrates an osteoblastoma in the posterior elements. What is the predominant radiographic characteristic of this specific osteoblastoma in the cervical spine?
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 8.16 states, "AP radiographs of the lumbar spine (a) and lateral radiographs of the cervical spine (b) both illustrate osteoblastomas... Osteoblastoma in the spine are typically expansile, but may be primarily lytic (a) or sclerotic (b)." Image (b) specifically shows a sclerotic lesion in the cervical spine. Therefore, this osteoblastoma is primarily sclerotic.
Question 40
A 16-year-old male presents with a several-month history of intermittent back pain. Physical examination is largely unremarkable except for mild tenderness. Given the variable clinical presentation and radiographic appearances of osteoblastoma, what is considered essential for accurate diagnosis?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "Radiographic correlation is essential (Figs. 8.12–8.19)." This emphasizes the critical role of imaging in diagnosing osteoblastoma, especially given its variable presentation. While other diagnostic tools might be used, radiographic correlation is highlighted as essential.
Question 40
A 19-year-old male undergoes curettage for a benign bone tumor in his sacrum. The gross specimen, as shown, is obtained during the procedure. What does this image represent?

View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 8.19 explicitly states, "Gross appearance of curetted osteoblastoma." This directly identifies the image as representing the gross appearance of the tumor after curettage, a common surgical treatment for benign bone tumors. The other options are incorrect descriptions of the image.
Question 40
A 15-year-old male presents with chronic, intermittent pain in his lumbar spine. On physical examination, the physician notes mild muscle atrophy in the paraspinal region. Which of the following physical findings is specifically mentioned as potentially associated with osteoblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Patients have minimal physical findings, although some have muscle atrophy or muscle spasm." This directly identifies muscle atrophy or spasm as potential physical findings. The other options are not mentioned in the provided text as being associated with osteoblastoma.
Question 40
A 20-year-old male undergoes biopsy for a sacral lesion. The photomicrograph, as shown, reveals mature cortical bone on the left surrounded by tumor tissue. This pattern of growth is described as permeative. What does a permeative growth pattern imply in the context of osteoblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 8.17 describes a "permeative growth pattern, with mature cortical bone on the left surrounded by osteoblastoma." Permeative growth, in general, refers to the infiltration of tumor cells through the existing bone structure, growing between trabeculae rather than forming a well-demarcated mass. This can be seen in both benign and malignant lesions. Options A, B, D, and E describe different or incorrect growth characteristics.
Question 41
A 16-year-old male presents with a 6-month history of intermittent, dull pain in his lower back that is worse at night. He reports that the pain sometimes resolves completely for a few days before returning. Physical examination reveals mild tenderness to palpation over the lumbar spine. Radiographs are pending.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states that patients with osteoblastoma often complain of "intermittent episodes of pain," which aligns with the description of pain with periods of resolution. This characteristic intermittent nature is a key feature. Constant, severe pain (A) or pain consistently worse in the morning (B) are less typical for osteoblastoma, and sharp radiating pain (D) is more suggestive of nerve root compression. Pain primarily associated with weight-bearing (E) is non-specific.
Question 42
A 19-year-old male presents with chronic, progressive pain in his cervical spine. Imaging reveals an expansile lesion in the posterior elements. Based on the typical epidemiology of osteoblastoma, which of the following patient demographics is most commonly affected?
View Answer & Explanation
Correct Answer: D
Rationale: The provided text explicitly states, "The usual age of onset is adolescence to early adulthood... Males are affected more commonly than females." This directly supports males in adolescence to early adulthood as the most commonly affected demographic. Other options contradict either the age range or gender predominance.
Question 43
A 17-year-old male presents with persistent back pain and muscle spasm. Radiographs of the lumbar spine show a lytic lesion. Given the typical spinal location for osteoblastoma, which anatomical region is most likely involved?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states, "Spinal osteoblastomas occur in the posterior elements." This makes the posterior elements the most typical location for osteoblastomas within the spine. While other structures might be secondarily affected, the primary involvement is in the posterior elements, as shown in Fig. 8.16.
Question 44
A 22-year-old female presents with chronic neck pain. Lateral radiographs of the cervical spine reveal a sclerotic lesion in the posterior elements. Based on the provided information, what is a characteristic radiographic appearance of osteoblastoma in the spine?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 8.16 and its caption state, "Osteoblastoma in the spine are typically expansile, but may be primarily lytic (a) or sclerotic (b)." This indicates a variable radiographic appearance, encompassing expansile, lytic, and sclerotic patterns. Options A, B, D, and E describe overly restrictive or incorrect radiographic features for osteoblastoma.
Question 45
A 25-year-old male presents with left buttock pain. An AP radiograph of the pelvis reveals a densely sclerotic lesion in the left sacrum, as shown. Due to its appearance, the lesion was initially mistaken for a more aggressive tumor. Which of the following conditions was it initially mistaken for?
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 8.12 explicitly states, "Due to the extent of sclerosis, this lesion was initially mistaken for an osteosarcoma." Osteosarcoma is a malignant bone tumor that can present with significant sclerosis, leading to this diagnostic confusion. The other options are typically benign lesions with different radiographic characteristics (e.g., enchondroma, fibrous dysplasia, NOF, SBC are generally lytic or mixed, not densely sclerotic to the extent of mimicking osteosarcoma).
Question 46
A 15-year-old male undergoes biopsy for a painful spinal lesion. Histopathological examination is performed. Which of the following microscopic features is characteristic of osteoblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The text and Fig. 8.18 caption state, "Osteoblastomas typically have loose, fibrovascular connective tissue intermixed with irregular osteoid." This is the defining histological characteristic. The other options describe features of different bone tumors (e.g., plasma cells for multiple myeloma, chondrocytes for chondrosarcoma/enchondroma, giant cells for giant cell tumor).
Question 47
A 20-year-old female presents with a 3-month history of increasing pain and swelling in her sacrum. Initial radiographs showed a subtle lytic lesion, but follow-up imaging 3 months later demonstrates significant progression and sclerosis. What is a known characteristic of the clinical course of osteoblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states, "The clinical course is usually slow and indolent, but osteoblastomas can progress rapidly, mimicking a malignant process." This highlights the potential for aggressive behavior despite its benign nature. Options A, B, D, and E contradict this variability and potential for rapid progression.
Question 48
A 14-year-old male presents with chronic back pain and a noticeable curvature of his spine. Physical examination reveals muscle spasm in the paraspinal region and a painful scoliosis. Which of the following is a recognized physical finding associated with spinal osteoblastomas?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Patients have minimal physical findings, although some have muscle atrophy or muscle spasm. Spinal osteoblastomas occur in the posterior elements; muscle spasm in this area can lead to a painful scoliosis." This directly supports muscle atrophy, spasm, and painful scoliosis as physical findings. The other options are not described as typical physical findings for osteoblastoma in the provided text.
Question 49
A 18-year-old female undergoes a biopsy of a sacral lesion. The photomicrograph, as shown, demonstrates a specific growth pattern where the tumor infiltrates existing bone. What is this growth pattern called?
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 8.17 explicitly states, "The lowpower figure demonstrates a permeative growth pattern, with mature cortical bone on the left surrounded by osteoblastoma." Permeative growth describes the infiltration of tumor cells through existing bone, which can be seen in both benign and malignant lesions. The other options describe different growth patterns or processes.
Question 50
A 16-year-old male presents with a 4-month history of increasing pain in his lumbar spine. Radiographs, as shown, reveal a lytic lesion in the posterior elements. What is a common characteristic of osteoblastomas in the spine, as illustrated by this image?
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 8.16 states, "Osteoblastoma in the spine are typically expansile, but may be primarily lytic (a) or sclerotic (b)." This indicates that expansile growth is a common feature, even if the lesion can also be lytic or sclerotic. Options A, C, D, and E are incorrect based on the provided text and images.
Question 51
A 21-year-old male presents with a rapidly growing, painful mass in his sacrum. Initial biopsy results are inconclusive, and the clinical picture suggests an aggressive process. Despite being a benign tumor, osteoblastoma can sometimes present with a clinical course that mimics which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "The clinical course is usually slow and indolent, but osteoblastomas can progress rapidly, mimicking a malignant process." This highlights the potential for osteoblastoma to present aggressively, leading to concern for malignancy. The other options describe conditions that are generally not mimicked by the rapid progression of an osteoblastoma.
Question 52
A 23-year-old female presents with chronic lower back pain. An AP radiograph of the pelvis, as shown, reveals a densely sclerotic lesion in the left sacrum. What is the most likely diagnosis for this lesion, given its appearance and location?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 8.12 is explicitly labeled as "AP radiograph of the pelvis shows a densely sclerotic osteoblastoma in the left sacrum." Therefore, osteoblastoma is the correct diagnosis. While other tumors can occur in the sacrum, the image directly identifies this specific lesion as an osteoblastoma, and its sclerotic nature is a known presentation.
Question 53
A 17-year-old male undergoes a biopsy of a spinal lesion. Histopathological examination, as shown, reveals loose fibrovascular connective tissue intermixed with irregular osteoid. The pathologist notes the presence of mitotic figures. What is the significance of mitotic figures in the context of osteoblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The caption for Fig. 8.18 states, "Mitotic figures may be present." This indicates that their presence is not uncommon in osteoblastoma, a benign tumor, and therefore does not automatically signify malignancy. It's important for pathologists to recognize that mitotic activity can be seen in benign osteoblastomas without necessarily implying malignant transformation.
Question 54
A 15-year-old female presents with a 9-month history of intermittent pain in her thoracic spine. Imaging reveals an expansile lesion in the posterior elements. Based on the overall classification, osteoblastoma is best described as which type of bone tumor?
View Answer & Explanation
Correct Answer: C
Rationale: The very first sentence of the clinical text states, "Osteoblastoma is a rare benign bone tumor." This directly classifies it as a benign bone tumor. The other options describe different categories of tumors.
Question 55
A 17-year-old male presents with chronic lower back pain. An AP radiograph of the lumbar spine, as shown, reveals a lytic lesion in the posterior elements. What is the predominant radiographic characteristic of this specific osteoblastoma in the lumbar spine?
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 8.16 states, "AP radiographs of the lumbar spine (a) and lateral radiographs of the cervical spine (b) both illustrate osteoblastomas... Osteoblastoma in the spine are typically expansile, but may be primarily lytic (a) or sclerotic (b)." Image (a) specifically shows a lytic lesion in the lumbar spine. Therefore, this osteoblastoma is primarily lytic.
Question 56
A 20-year-old female presents with chronic neck pain. A lateral radiograph of the cervical spine, as shown, illustrates an osteoblastoma in the posterior elements. What is the predominant radiographic characteristic of this specific osteoblastoma in the cervical spine?
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 8.16 states, "AP radiographs of the lumbar spine (a) and lateral radiographs of the cervical spine (b) both illustrate osteoblastomas... Osteoblastoma in the spine are typically expansile, but may be primarily lytic (a) or sclerotic (b)." Image (b) specifically shows a sclerotic lesion in the cervical spine. Therefore, this osteoblastoma is primarily sclerotic.
Question 57
A 16-year-old male presents with a several-month history of intermittent back pain. Physical examination is largely unremarkable except for mild tenderness. Given the variable clinical presentation and radiographic appearances of osteoblastoma, what is considered essential for accurate diagnosis?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "Radiographic correlation is essential (Figs. 8.12–8.19)." This emphasizes the critical role of imaging in diagnosing osteoblastoma, especially given its variable presentation. While other diagnostic tools might be used, radiographic correlation is highlighted as essential.
Question 58
A 19-year-old male undergoes curettage for a benign bone tumor in his sacrum. The gross specimen, as shown, is obtained during the procedure. What does this image represent?
View Answer & Explanation
Correct Answer: B
Rationale: The caption for Fig. 8.19 explicitly states, "Gross appearance of curetted osteoblastoma." This directly identifies the image as representing the gross appearance of the tumor after curettage, a common surgical treatment for benign bone tumors. The other options are incorrect descriptions of the image.
Question 59
A 15-year-old male presents with chronic, intermittent pain in his lumbar spine. On physical examination, the physician notes mild muscle atrophy in the paraspinal region. Which of the following physical findings is specifically mentioned as potentially associated with osteoblastoma?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Patients have minimal physical findings, although some have muscle atrophy or muscle spasm." This directly identifies muscle atrophy or spasm as potential physical findings. The other options are not mentioned in the provided text as being associated with osteoblastoma.
Question 60
A 3-year-old boy presents with disproportionate short stature, characterized by rhizomelic limb shortening, a large head, and a prominent forehead. Physical examination reveals thoracolumbar kyphosis and lumbar hyperlordosis. Radiographs show short pedicles, bullet-shaped vertebrae, and a narrowed interpedicular distance in the lumbar spine, along with a small foramen magnum.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical presentation of disproportionate short stature with rhizomelic limb shortening, large head, prominent forehead, thoracolumbar kyphosis, and lumbar hyperlordosis, combined with radiographic findings of short pedicles, bullet-shaped vertebrae, narrowed interpedicular distance in the lumbar spine, and a small foramen magnum, is classic for achondroplasia. Spondyloepiphyseal dysplasia congenita typically presents with short trunk dwarfism and more severe platyspondyly. Diastrophic dysplasia is characterized by hitchhiker's thumb and clubfoot. Kniest dysplasia involves a "Swiss cheese" appearance of vertebrae. Morquio syndrome presents with severe platyspondyly and odontoid hypoplasia but typically has more generalized epiphyseal involvement and different facial features.
Question 61
A 4-year-old girl with known achondroplasia presents with increasing difficulty walking, leg weakness, and urinary incontinence. Her parents report she has been falling more frequently. On examination, she has hyperreflexia and clonus in her lower extremities. Radiographs confirm the typical features of achondroplasia, including a narrowed foramen magnum.
View Answer & Explanation
Correct Answer: D
Rationale: The symptoms of leg weakness, hyperreflexia, clonus, and urinary incontinence in a young child with achondroplasia, especially with a narrowed foramen magnum, are highly suggestive of cervicomedullary junction compression. While lumbar spinal stenosis is common in older achondroplastic patients, these severe neurological signs in a young child point to the more proximal compression. Progressive thoracolumbar kyphosis can occur but typically causes different neurological deficits or pain. Atlantoaxial instability is not a primary feature of achondroplasia. Diastematomyelia is a congenital spinal anomaly not directly linked to achondroplasia.
Question 62
A 6-month-old infant is diagnosed with Spondyloepiphyseal Dysplasia Congenita (SEDC). The parents are concerned about potential spinal complications. On physical exam, the child has a short trunk and mild platyspondyly is noted on radiographs. Which of the following spinal complications is MOST critical to monitor for in early childhood in this condition?
View Answer & Explanation
Correct Answer: C
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDC) is frequently associated with odontoid hypoplasia, which can lead to significant atlantoaxial instability. This instability poses a risk of spinal cord compression and is a critical complication to monitor for, often requiring early surgical stabilization. While scoliosis and kyphosis can occur, and lumbar stenosis may develop later, atlantoaxial instability is a hallmark and often life-threatening early complication. Sacral agenesis is associated with caudal regression syndrome, not SEDC.
Question 63
A 10-year-old boy with Diastrophic Dysplasia presents with severe, rapidly progressive scoliosis measuring 70 degrees. He also has characteristic "hitchhiker's thumbs" and clubfeet. Previous bracing attempts have failed to control the curve progression. Neurological examination is normal.
View Answer & Explanation
Correct Answer: C
Rationale: Diastrophic dysplasia is known for severe, rapidly progressive scoliosis that is often rigid and poorly responsive to bracing. A 70-degree curve in a 10-year-old, especially with documented progression despite bracing, is an indication for surgical spinal fusion with instrumentation to prevent further progression and potential cardiopulmonary compromise. Continued bracing or observation is inappropriate for such a severe and progressive curve. Growth modulation techniques like VBT are generally considered for more flexible curves in younger patients and may not be suitable for the rigid curves seen in diastrophic dysplasia.
Question 64
A 7-year-old girl with a history of Kniest Dysplasia presents for follow-up. Her radiographs show marked platyspondyly with a "Swiss cheese" appearance of the vertebral bodies, along with short long bones and enlarged joints. What is the most common spinal deformity requiring intervention in patients with Kniest Dysplasia?
View Answer & Explanation
Correct Answer: E
Rationale: Kniest dysplasia is frequently associated with progressive scoliosis, which can be severe and require surgical intervention. While other spinal issues like platyspondyly and cervical instability can occur, scoliosis is the most common spinal deformity requiring intervention. Atlantoaxial instability is more characteristic of SEDC or Morquio. Lumbar spinal stenosis is more common in achondroplasia. Progressive thoracolumbar kyphosis can occur but scoliosis is more prevalent as a primary deformity.
Question 65
A 2-year-old boy with Morquio Syndrome (MPS IV) is brought to the clinic. He has disproportionate short stature, a short neck, and a waddling gait. Radiographs reveal severe platyspondyly, anterior wedging of vertebral bodies, and significant odontoid hypoplasia. What is the primary spinal concern in this patient that warrants immediate attention?
View Answer & Explanation
Correct Answer: C
Rationale: Morquio Syndrome is characterized by severe odontoid hypoplasia, which leads to significant atlantoaxial instability. This instability places the spinal cord at high risk of compression, making it the most critical and potentially life-threatening spinal concern requiring immediate attention and often early surgical stabilization. While thoracolumbar kyphosis and scoliosis can occur, the cervical spine instability is the most urgent issue. Lumbar hyperlordosis is less critical, and sacral agenesis is not associated with Morquio syndrome.
Question 66
A 15-year-old male with achondroplasia presents with bilateral lower extremity numbness, tingling, and claudication-like symptoms after walking short distances. Physical examination reveals diminished sensation in a stocking-glove distribution and decreased ankle reflexes. Radiographs show severe narrowing of the spinal canal in the lumbar region.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical picture of bilateral lower extremity numbness, tingling, claudication-like symptoms, and diminished reflexes in an adolescent with achondroplasia, coupled with radiographic evidence of severe lumbar spinal canal narrowing, is classic for lumbar spinal stenosis. Achondroplasia is characterized by congenitally short pedicles and reduced interpedicular distance, predisposing to early and severe lumbar stenosis. Cervical myelopathy would present with upper motor neuron signs and typically affects the upper extremities more. Peripheral neuropathy is less likely to be the primary cause given the spinal canal narrowing. Thoracic disc herniation and sacroiliac joint dysfunction do not fit the overall clinical and radiographic presentation.
Question 67
A 5-year-old boy with a known skeletal dysplasia presents with a rigid, angular kyphosis at the thoracolumbar junction (T12-L1) and a waddling gait. Radiographs show anterior wedging and hypoplasia of the T12 and L1 vertebral bodies, creating a sharp gibbus deformity. This type of deformity is most commonly associated with which group of skeletal dysplasias?
View Answer & Explanation
Correct Answer: C
Rationale: A rigid, angular thoracolumbar kyphosis (gibbus deformity) due to anterior wedging and hypoplasia of vertebral bodies is a classic spinal manifestation of the Mucopolysaccharidoses (MPS), particularly MPS I (Hurler syndrome) and MPS IV (Morquio syndrome). These conditions involve abnormal storage of glycosaminoglycans, leading to dysplastic changes in cartilage and bone. While other dysplasias can have kyphosis, the characteristic gibbus deformity is most strongly associated with MPS. FGFR3 disorders (like achondroplasia) primarily cause lumbar lordosis and stenosis. Collagenopathies like OI can have scoliosis/kyphosis but typically not this specific gibbus. Spondyloepiphyseal dysplasias are more known for platyspondyly and atlantoaxial instability.
Question 68
A 1-year-old infant with achondroplasia is found to have significant thoracolumbar kyphosis measuring 55 degrees, which is flexible on prone extension radiographs. The child is not yet walking independently. What is the most appropriate initial management for this kyphosis?
View Answer & Explanation
Correct Answer: C
Rationale: For a flexible thoracolumbar kyphosis in a pre-ambulatory infant with achondroplasia, bracing with a TLSO is the most appropriate initial management. The goal is to prevent progression and allow the spine to develop more normally as the child gains ambulation. Surgical fusion is reserved for rigid, progressive curves or those with neurological compromise. Observation alone is insufficient for a 55-degree curve. Physical therapy is supportive but not the primary treatment for curve correction. Genetic counseling is important but not the immediate management for the kyphosis.
Question 69
A 12-year-old boy with Spondyloepiphyseal Dysplasia Tarda (SEDT) presents with chronic back pain and progressive gait disturbance. Radiographs show severe platyspondyly, particularly in the lumbar spine, and significant narrowing of the spinal canal. He has a history of mild short stature and early-onset osteoarthritis. What is the most likely cause of his neurological symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: Spondyloepiphyseal Dysplasia Tarda (SEDT) is characterized by platyspondyly, particularly in the lumbar spine, which can lead to premature degenerative changes and severe lumbar spinal stenosis. The symptoms of chronic back pain and progressive gait disturbance, combined with radiographic findings of severe platyspondyly and spinal canal narrowing, are highly indicative of lumbar spinal stenosis. Atlantoaxial instability is more common in SEDC. Cervical myelopathy and thoracic kyphosis are less typical primary manifestations of SEDT. Peripheral nerve entrapment is a less likely primary cause given the diffuse spinal canal narrowing.
Question 70
A 6-year-old child with a skeletal dysplasia presents with a C1-C2 instability due to odontoid hypoplasia. Neurological examination reveals hyperreflexia in the lower extremities and a positive Babinski sign. What is the most appropriate management for this patient?
View Answer & Explanation
Correct Answer: C
Rationale: C1-C2 instability with neurological signs (hyperreflexia, Babinski) indicates spinal cord compression and requires surgical stabilization. Posterior C1-C2 fusion is the standard treatment for atlantoaxial instability due to odontoid hypoplasia in children, providing immediate stability and decompression. Observation or non-surgical methods like a cervical collar or halo vest are insufficient to address the underlying instability and ongoing neurological compromise. Anterior cervical discectomy and fusion is typically for disc pathology, not C1-C2 instability.
Question 71
A 9-month-old infant with achondroplasia is noted to have a persistent, rigid thoracolumbar kyphosis of 70 degrees despite appropriate bracing for 3 months. MRI shows no evidence of spinal cord compression. The child is not yet walking. What is the next most appropriate step in management?
View Answer & Explanation
Correct Answer: C
Rationale: A rigid thoracolumbar kyphosis of 70 degrees in an infant with achondroplasia, especially one that has failed bracing, is an indication for surgical intervention. While ambulation can sometimes improve flexible curves, a rigid 70-degree curve is unlikely to resolve spontaneously and carries a high risk of progression and potential neurological compromise. Posterior spinal fusion is the standard surgical treatment for rigid, progressive kyphosis in achondroplasia. Anterior vertebral body tethering is typically for scoliosis and not suitable for rigid kyphosis in this age group. Genetic counseling is important but not the next step for managing the kyphosis.
Question 72
A 14-year-old girl with a skeletal dysplasia presents with severe short stature, a barrel chest, and progressive scoliosis. Radiographs show significant platyspondyly, particularly in the thoracic spine, and a "double-hump" appearance of the vertebral bodies. She also has a history of hearing loss. Which of the following dysplasias is most consistent with these findings?
View Answer & Explanation
Correct Answer: D
Rationale: Metatropic dysplasia is characterized by severe short stature, a barrel chest, progressive scoliosis, and marked platyspondyly, often with a "double-hump" appearance of the vertebral bodies. Hearing loss can also be associated. Initially, it can mimic achondroplasia but progresses to a more severe short trunk dwarfism. Achondroplasia has rhizomelic shortening and different vertebral morphology. Diastrophic dysplasia has hitchhiker's thumb and clubfoot. SEDC has platyspondyly and odontoid hypoplasia but typically not the "double-hump" vertebrae. Pseudoachondroplasia has normal facial features and later onset of skeletal changes.
Question 73
A 3-year-old boy with a known mucopolysaccharidosis (MPS I, Hurler syndrome) presents with a progressive thoracolumbar gibbus deformity. He has coarse facial features and hepatosplenomegaly. What is the primary goal of surgical intervention for this spinal deformity?
View Answer & Explanation
Correct Answer: B
Rationale: The primary goal of surgical intervention for a progressive thoracolumbar gibbus deformity in MPS is the prevention of neurological compromise. The sharp angulation can lead to spinal cord compression, causing myelopathy. While pulmonary function may indirectly benefit from improved spinal alignment, and back pain may be reduced, the most critical indication for surgery is to protect neurological function. Cosmetic improvement and correction of short stature are secondary considerations.
Question 74
A 1-year-old child with achondroplasia is undergoing routine screening. MRI of the brain and cervical spine is recommended. What is the most critical finding to assess for at the cervicomedullary junction in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: Foramen magnum stenosis is a hallmark feature of achondroplasia and is the most critical finding to assess for at the cervicomedullary junction in infants. This narrowing can lead to compression of the brainstem and spinal cord, causing apnea, hypotonia, and sudden death. While Chiari I malformation can be associated, the primary issue in achondroplasia is the bony stenosis of the foramen magnum. Basilar invagination is less common. Odontoid hypoplasia is characteristic of SEDC and MPS, not achondroplasia. Cervical disc herniation is rare in infants.
Question 75
A 16-year-old male with a skeletal dysplasia presents with severe, rigid scoliosis and significant short stature. He has a history of multiple joint contractures and a characteristic "mask-like" facial appearance. Radiographs show severe platyspondyly and a "pear-shaped" appearance of the vertebral bodies. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: E
Rationale: The combination of severe short stature, rigid scoliosis, joint contractures, "mask-like" facial appearance, severe platyspondyly, and "pear-shaped" vertebral bodies is highly suggestive of Spondyloepimetaphyseal Dysplasia, Strudwick type. This is a severe form of SED. Achondroplasia has rhizomelic shortening and different spinal features. Kniest dysplasia has a "Swiss cheese" appearance of vertebrae. SEDC has odontoid hypoplasia and platyspondyly but typically not the "pear-shaped" vertebrae. Pseudoachondroplasia has normal facial features and less severe platyspondyly.
Question 76
A 5-year-old boy with a skeletal dysplasia is being evaluated for progressive scoliosis. Genetic testing reveals a mutation in the SLC26A2 gene. What other musculoskeletal finding is highly characteristic of this dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: A mutation in the SLC26A2 gene (formerly DTDST) is responsible for Diastrophic Dysplasia. A highly characteristic musculoskeletal finding of Diastrophic Dysplasia is the "hitchhiker's thumb" (abducted thumb due to a short first metacarpal and abnormal first metacarpophalangeal joint). Rhizomelic limb shortening and narrowed foramen magnum are associated with achondroplasia. Odontoid hypoplasia is seen in SEDC and MPS. "Swiss cheese" vertebrae are characteristic of Kniest dysplasia.
Question 77
A 2-year-old child with achondroplasia presents with a 60-degree thoracolumbar kyphosis that is rigid on prone extension views. There are no neurological deficits. What is the most appropriate surgical approach for this deformity?
View Answer & Explanation
Correct Answer: B
Rationale: For a rigid thoracolumbar kyphosis of 60 degrees in a 2-year-old with achondroplasia, posterior spinal fusion with instrumentation is the most appropriate surgical approach. While combined anterior and posterior fusion might be considered for very severe or complex rigid deformities, a posterior-only approach is often sufficient for rigid kyphosis in this age group, especially without neurological deficits. Anterior vertebral column resection is a more aggressive procedure typically reserved for severe, angular, and often congenital kyphosis. Vertebral body tethering is for scoliosis. Growing rod surgery is for progressive scoliosis or kyphosis in younger children to allow for continued growth, but for a rigid kyphosis of this magnitude, fusion is generally preferred.
Question 78
A 10-year-old boy with a skeletal dysplasia presents with progressive scoliosis and significant joint laxity. Radiographs show generalized osteopenia, biconcave vertebral bodies ("codfish vertebrae"), and multiple healed fractures. He has blue sclerae. What is the most likely underlying condition?
View Answer & Explanation
Correct Answer: C
Rationale: The combination of progressive scoliosis, generalized osteopenia, biconcave vertebral bodies ("codfish vertebrae"), multiple healed fractures, and blue sclerae is classic for Osteogenesis Imperfecta (OI). OI is a collagenopathy characterized by bone fragility. Achondroplasia has different radiographic features and no blue sclerae. SEDC involves platyspondyly and odontoid hypoplasia. Marfan syndrome involves arachnodactyly, aortic root dilation, and scoliosis but not generalized osteopenia or multiple fractures. Hypophosphatasia involves impaired bone mineralization but typically presents with different skeletal features and often rickets-like changes.
Question 79
A 7-year-old girl with a skeletal dysplasia is being evaluated for chronic neck pain and neurological symptoms including gait disturbance and upper extremity weakness. MRI reveals significant C1-C2 instability with spinal cord compression. She has a history of short trunk dwarfism and vision impairment. Which of the following dysplasias is most likely?
- A) Achondroplasia
- B) Diastrophic dysplasia
- C) Spondyloepiphyseal dysplasia congenita
- D) Pseudoachondroplasia
- E)
Question 79
A 5-year-old boy with known achondroplasia presents with progressive leg weakness and difficulty walking. Physical exam reveals hyperreflexia and clonus in the lower extremities. Radiographs show narrowing of the spinal canal in the lumbar region.
View Answer & Explanation
Correct Answer: C
Rationale: Lumbar spinal stenosis is a hallmark complication of achondroplasia due to shortened pedicles and decreased interpedicular distance, leading to progressive neurological symptoms in the lower extremities. Atlantoaxial instability (A) is more common in other skeletal dysplasias like SEDC or MPS, but less so as a primary cause of progressive lumbar neurological symptoms in achondroplasia.
Question 79
A 3-year-old girl presents with short stature, a waddling gait, and a prominent thoracolumbar kyphosis. Lateral spine radiographs demonstrate anterior wedging of the vertebral bodies, particularly at the thoracolumbar junction, and some platyspondyly. She has no signs of hydrocephalus.
View Answer & Explanation
Correct Answer: A
Rationale: The combination of short stature, waddling gait, and a prominent thoracolumbar kyphosis with anterior wedging and mild platyspondyly is highly characteristic of achondroplasia. While Spondyloepiphyseal dysplasia congenita (B) also presents with short stature and spinal involvement, the specific pattern of thoracolumbar kyphosis with anterior wedging is more classic for achondroplasia in this age group.
Question 79
A 7-year-old boy with Spondyloepiphyseal Dysplasia Congenita (SEDC) is evaluated for increasing neck pain and gait unsteadiness. Physical exam reveals hyperreflexia in all four extremities and a positive Babinski sign. Lateral flexion-extension radiographs of the cervical spine show an increased atlanto-dens interval (ADI) and significant C1-C2 instability.
View Answer & Explanation
Correct Answer: C
Rationale: Given the C1-C2 instability with neurological signs in SEDC, a posterior occipitocervical fusion is the most appropriate surgical management to achieve stable fixation and prevent further neurological compromise. Laminectomy C1-C2 (E) without stabilization would decompress but worsen instability, making it contraindicated in this scenario.
Question 79
A newborn is diagnosed with achondroplasia based on characteristic clinical and radiographic features including rhizomelic shortening, frontal bossing, and a narrow interpedicular distance in the lumbar spine.
View Answer & Explanation
Correct Answer: B
Rationale: Achondroplasia is caused by a gain-of-function mutation in the Fibroblast Growth Factor Receptor 3 (FGFR3) gene. COL1A1 (A) is associated with osteogenesis imperfecta, a different skeletal dysplasia.
Question 79
A 4-year-old girl presents with short stature, clubfeet, and a severe progressive kyphoscoliosis. She has a history of multiple joint contractures and "hitchhiker's thumbs." Radiographs show platyspondyly, coronal clefts in the vertebral bodies, and severe scoliosis.
View Answer & Explanation
Correct Answer: C
Rationale: The constellation of short stature, clubfeet, severe progressive kyphoscoliosis, joint contractures, "hitchhiker's thumbs," platyspondyly, and coronal clefts is pathognomonic for diastrophic dysplasia. Achondroplasia (A) typically presents with different spinal features and lacks the characteristic hand and foot deformities.
Question 79
A 6-year-old boy with Hurler syndrome (MPS I) is brought for evaluation of progressive gait disturbance and neck stiffness. Physical exam reveals hyperreflexia and clonus in the lower extremities. Lateral cervical spine radiographs show C1-C2 instability and an os odontoideum.
View Answer & Explanation
Correct Answer: C
Rationale: In Hurler syndrome (MPS I), atlantoaxial instability due to odontoid hypoplasia or an os odontoideum is a critical and potentially life-threatening spinal complication, especially when associated with neurological signs. While thoracolumbar kyphosis (A) is also common in MPS, the neurological symptoms and C1-C2 instability indicate a more urgent and critical issue.
Question 79
A 10-year-old boy with short stature and a barrel chest is evaluated. Radiographs of the spine show severe platyspondyly with anterior beaking of the vertebral bodies, particularly in the thoracolumbar region, and irregular endplates. The odontoid process is hypoplastic.
View Answer & Explanation
Correct Answer: C
Rationale: Severe platyspondyly with anterior beaking of the vertebral bodies (especially in the thoracolumbar region), irregular endplates, and odontoid hypoplasia are classic radiographic features of Morquio syndrome (MPS IV). Spondyloepiphyseal dysplasia congenita (B) also presents with platyspondyly and odontoid hypoplasia, but the prominent anterior vertebral beaking is more characteristic of Morquio syndrome.
Question 79
A 12-year-old girl with Spondyloepiphyseal Dysplasia Tarda (SEDT) presents with a progressive thoracolumbar kyphoscoliosis measuring 70 degrees. She has significant truncal imbalance. Surgical correction is planned.
View Answer & Explanation
Correct Answer: C
Rationale: Patients with skeletal dysplasias often have abnormal bone quality, poor healing capacity, and altered biomechanics, leading to a significantly increased risk of pseudarthrosis following spinal fusion. Pedicle morphology (B) is often abnormal, making screw placement challenging, not normal.
Question 79
A 30-year-old male with achondroplasia presents with neurogenic claudication, characterized by bilateral leg pain and numbness that worsens with walking and improves with sitting. Physical exam reveals diminished sensation in the lower extremities. MRI confirms severe lumbar spinal stenosis.
View Answer & Explanation
Correct Answer: C
Rationale: The primary anatomical reason for lumbar spinal stenosis in achondroplasia is the congenital abnormality of shortened pedicles and a progressively decreasing interpedicular distance from L1 to L5, leading to a trefoil-shaped canal. While ligamentum flavum hypertrophy (A) and disc herniation can contribute, the underlying bony architecture is the main predisposing factor.
Question 79
A 6-year-old boy with Kniest dysplasia presents with severe short stature, a "pear-shaped" trunk, and a progressive kyphoscoliosis. Radiographs show severe platyspondyly with coronal clefts, and dumbbell-shaped long bones.
View Answer & Explanation
Correct Answer: C
Rationale: Progressive and severe kyphoscoliosis is a very common and challenging spinal deformity in Kniest dysplasia, often requiring surgical intervention. While fixed thoracic kyphosis (D) can be part of the picture, the combination with scoliosis and its progressive nature is more characteristic.
Question 79
A 2-year-old child is found to have severe platyspondyly on a skeletal survey performed for short stature. The child also has significant metaphyseal flaring and epiphyseal irregularities.
View Answer & Explanation
Correct Answer: E
Rationale: Osteogenesis imperfecta (E) is a collagen disorder characterized by bone fragility and fractures, not typically severe platyspondyly as a primary feature. All other options (A, B, C, D) are skeletal dysplasias that commonly present with varying degrees of platyspondyly.
Question 79
A 1-year-old infant with achondroplasia is noted to have a flexible thoracolumbar kyphosis of 45 degrees. Neurological exam is normal.
View Answer & Explanation
Correct Answer: C
Rationale: Flexible thoracolumbar kyphosis in infants with achondroplasia often resolves spontaneously with prone positioning and strengthening of paraspinal muscles as they begin to walk. Surgical fusion (A) is reserved for rigid, progressive curves, especially with neurological compromise. Bracing (B) is generally ineffective for this type of kyphosis.
Question 79
A 5-year-old boy with pseudoachondroplasia presents with a waddling gait and increasing difficulty with activities. Radiographs show severe platyspondyly, irregular endplates, and significant epiphyseal dysplasia. He has no history of hydrocephalus or atlantoaxial instability.
<ul
Question 80
A 5-year-old boy with known achondroplasia presents with progressive leg weakness and difficulty walking. Physical exam reveals hyperreflexia and clonus in the lower extremities. Radiographs show narrowing of the spinal canal in the lumbar region.
View Answer & Explanation
Correct Answer: C
Rationale: Lumbar spinal stenosis is a hallmark complication of achondroplasia due to shortened pedicles and decreased interpedicular distance, leading to progressive neurological symptoms in the lower extremities. Atlantoaxial instability (A) is more common in other skeletal dysplasias like SEDC or MPS, but less so as a primary cause of progressive lumbar neurological symptoms in achondroplasia.
Question 81
A 3-year-old girl presents with short stature, a waddling gait, and a prominent thoracolumbar kyphosis. Lateral spine radiographs demonstrate anterior wedging of the vertebral bodies, particularly at the thoracolumbar junction, and some platyspondyly. She has no signs of hydrocephalus.
View Answer & Explanation
Correct Answer: A
Rationale: The combination of short stature, waddling gait, and a prominent thoracolumbar kyphosis with anterior wedging and mild platyspondyly is highly characteristic of achondroplasia. While Spondyloepiphyseal dysplasia congenita (B) also presents with short stature and spinal involvement, the specific pattern of thoracolumbar kyphosis with anterior wedging is more classic for achondroplasia in this age group.
Question 82
A 7-year-old boy with Spondyloepiphyseal Dysplasia Congenita (SEDC) is evaluated for increasing neck pain and gait unsteadiness. Physical exam reveals hyperreflexia in all four extremities and a positive Babinski sign. Lateral flexion-extension radiographs of the cervical spine show an increased atlanto-dens interval (ADI) and significant C1-C2 instability.
View Answer & Explanation
Correct Answer: C
Rationale: Given the C1-C2 instability with neurological signs in SEDC, a posterior occipitocervical fusion is the most appropriate surgical management to achieve stable fixation and prevent further neurological compromise. Laminectomy C1-C2 (E) without stabilization would decompress but worsen instability, making it contraindicated in this scenario.
Question 83
A newborn is diagnosed with achondroplasia based on characteristic clinical and radiographic features including rhizomelic shortening, frontal bossing, and a narrow interpedicular distance in the lumbar spine.
View Answer & Explanation
Correct Answer: B
Rationale: Achondroplasia is caused by a gain-of-function mutation in the Fibroblast Growth Factor Receptor 3 (FGFR3) gene. COL1A1 (A) is associated with osteogenesis imperfecta, a different skeletal dysplasia.
Question 84
A 4-year-old girl presents with short stature, clubfeet, and a severe progressive kyphoscoliosis. She has a history of multiple joint contractures and "hitchhiker's thumbs." Radiographs show platyspondyly, coronal clefts in the vertebral bodies, and severe scoliosis.
View Answer & Explanation
Correct Answer: C
Rationale: The constellation of short stature, clubfeet, severe progressive kyphoscoliosis, joint contractures, "hitchhiker's thumbs," platyspondyly, and coronal clefts is pathognomonic for diastrophic dysplasia. Achondroplasia (A) typically presents with different spinal features and lacks the characteristic hand and foot deformities.
Question 85
A 6-year-old boy with Hurler syndrome (MPS I) is brought for evaluation of progressive gait disturbance and neck stiffness. Physical exam reveals hyperreflexia and clonus in the lower extremities. Lateral cervical spine radiographs show C1-C2 instability and an os odontoideum.
View Answer & Explanation
Correct Answer: C
Rationale: In Hurler syndrome (MPS I), atlantoaxial instability due to odontoid hypoplasia or an os odontoideum is a critical and potentially life-threatening spinal complication, especially when associated with neurological signs. While thoracolumbar kyphosis (A) is also common in MPS, the neurological symptoms and C1-C2 instability indicate a more urgent and critical issue.
Question 86
A 10-year-old boy with short stature and a barrel chest is evaluated. Radiographs of the spine show severe platyspondyly with anterior beaking of the vertebral bodies, particularly in the thoracolumbar region, and irregular endplates. The odontoid process is hypoplastic.
View Answer & Explanation
Correct Answer: C
Rationale: Severe platyspondyly with anterior beaking of the vertebral bodies (especially in the thoracolumbar region), irregular endplates, and odontoid hypoplasia are classic radiographic features of Morquio syndrome (MPS IV). Spondyloepiphyseal dysplasia congenita (B) also presents with platyspondyly and odontoid hypoplasia, but the prominent anterior vertebral beaking is more characteristic of Morquio syndrome.
Question 87
A 12-year-old girl with Spondyloepiphyseal Dysplasia Tarda (SEDT) presents with a progressive thoracolumbar kyphoscoliosis measuring 70 degrees. She has significant truncal imbalance. Surgical correction is planned.
View Answer & Explanation
Correct Answer: C
Rationale: Patients with skeletal dysplasias often have abnormal bone quality, poor healing capacity, and altered biomechanics, leading to a significantly increased risk of pseudarthrosis following spinal fusion. Pedicle morphology (B) is often abnormal, making screw placement challenging, not normal.
Question 88
A 30-year-old male with achondroplasia presents with neurogenic claudication, characterized by bilateral leg pain and numbness that worsens with walking and improves with sitting. Physical exam reveals diminished sensation in the lower extremities. MRI confirms severe lumbar spinal stenosis.
View Answer & Explanation
Correct Answer: C
Rationale: The primary anatomical reason for lumbar spinal stenosis in achondroplasia is the congenital abnormality of shortened pedicles and a progressively decreasing interpedicular distance from L1 to L5, leading to a trefoil-shaped canal. While ligamentum flavum hypertrophy (A) and disc herniation can contribute, the underlying bony architecture is the main predisposing factor.
Question 89
A 6-year-old boy with Kniest dysplasia presents with severe short stature, a "pear-shaped" trunk, and a progressive kyphoscoliosis. Radiographs show severe platyspondyly with coronal clefts, and dumbbell-shaped long bones.
View Answer & Explanation
Correct Answer: C
Rationale: Progressive and severe kyphoscoliosis is a very common and challenging spinal deformity in Kniest dysplasia, often requiring surgical intervention. While fixed thoracic kyphosis (D) can be part of the picture, the combination with scoliosis and its progressive nature is more characteristic.
Question 90
A 2-year-old child is found to have severe platyspondyly on a skeletal survey performed for short stature. The child also has significant metaphyseal flaring and epiphyseal irregularities.
View Answer & Explanation
Correct Answer: E
Rationale: Osteogenesis imperfecta (E) is a collagen disorder characterized by bone fragility and fractures, not typically severe platyspondyly as a primary feature. All other options (A, B, C, D) are skeletal dysplasias that commonly present with varying degrees of platyspondyly.
Question 91
A 1-year-old infant with achondroplasia is noted to have a flexible thoracolumbar kyphosis of 45 degrees. Neurological exam is normal.
View Answer & Explanation
Correct Answer: C
Rationale: Flexible thoracolumbar kyphosis in infants with achondroplasia often resolves spontaneously with prone positioning and strengthening of paraspinal muscles as they begin to walk. Surgical fusion (A) is reserved for rigid, progressive curves, especially with neurological compromise. Bracing (B) is generally ineffective for this type of kyphosis.
Question 92
A 7-year-old boy presents with bilateral hip pain and a waddling gait. His parents report he has always been shorter than his peers. Physical examination reveals limited range of motion in both hips, particularly abduction and internal rotation. Radiographs of the hips show flattened and irregular femoral epiphyses with delayed ossification. The spine appears normal. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Multiple Epiphyseal Dysplasia (MED), particularly the Fairbank type, is characterized by flattened and irregular epiphyses, often presenting in childhood with hip and knee pain, waddling gait, and mild short stature. The spine is typically spared. Pseudoachondroplasia also presents with significant epiphyseal involvement and short stature but often has more severe metaphyseal changes and a distinctive waddling gait. Spondyloepiphyseal Dysplasia Congenita (SEDc) would involve the spine, which is noted as normal here. Achondroplasia primarily affects endochondral ossification at the growth plate, leading to rhizomelic dwarfism, but typically has normal epiphyses. Diastrophic dysplasia involves multiple joints, clubfoot, and ear deformities, which are not mentioned.
Question 93
A 12-year-old girl presents with progressive knee pain and stiffness. She has a history of mild short stature and has been diagnosed with genu valgum. Radiographs demonstrate irregular and fragmented epiphyses in the distal femurs and proximal tibias, with premature degenerative changes. Genetic testing reveals a mutation in the *COMP* gene. Which of the following conditions is most consistent with these findings?
View Answer & Explanation
Correct Answer: D
Rationale: Pseudoachondroplasia is an autosomal dominant disorder caused by mutations in the *COMP* (cartilage oligomeric matrix protein) gene. It is characterized by severe short stature, waddling gait, joint laxity followed by early osteoarthritis, and significant epiphyseal and metaphyseal irregularities. Multiple Epiphyseal Dysplasia (MED) can also be caused by *COMP* mutations but typically presents with milder short stature and less severe metaphyseal changes. However, the description of "irregular and fragmented epiphyses" with "premature degenerative changes" and "progressive knee pain and stiffness" is highly characteristic of pseudoachondroplasia, which is often more severe than typical MED. Spondyloepiphyseal Dysplasia Tarda (SEDT) primarily affects the spine and hips, and is X-linked. Kniest dysplasia involves a "Swiss cheese" appearance of cartilage and distinct facial features. Chondrodysplasia punctata is characterized by stippled epiphyses in infancy.
Question 94
A 3-year-old boy is brought to the clinic due to delayed motor milestones and a noticeable short trunk. Physical examination reveals a barrel chest and a flattened midface. Radiographs of the spine show platyspondyly (flattened vertebral bodies) and odontoid hypoplasia. Hip radiographs demonstrate small, irregular femoral epiphyses. What is the most appropriate diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDc) is an autosomal dominant disorder characterized by short-trunk dwarfism, platyspondyly, odontoid hypoplasia (leading to atlantoaxial instability), and epiphyseal dysplasia, particularly in the hips. The barrel chest and flattened midface are also common features. Achondroplasia is a rhizomelic dwarfism with normal spine length and primarily metaphyseal involvement. Multiple Epiphyseal Dysplasia typically spares the spine. Diastrophic dysplasia presents with clubfoot, hitchhiker thumbs, and ear deformities, along with epiphyseal changes. Metaphyseal chondrodysplasia, Schmid type, primarily affects the metaphyses and does not typically involve the spine as prominently.
Question 95
An 18-month-old girl presents with bilateral clubfoot and contractures of the large joints. Her parents note short limbs and a "hitchhiker thumb" deformity. Radiographs show delayed and irregular ossification of the epiphyses, particularly in the hips and knees, and a characteristic "dumbbell" shape of the long bones. What is the most likely underlying genetic condition?
View Answer & Explanation
Correct Answer: C
Rationale: Diastrophic Dysplasia is an autosomal recessive disorder characterized by short-limb dwarfism, clubfoot, joint contractures, hitchhiker thumbs (abducted thumbs), and often ear deformities. Radiographically, it shows delayed and irregular epiphyseal ossification, and the long bones can have a characteristic "dumbbell" shape due to metaphyseal flaring and epiphyseal hypoplasia. Achondroplasia and hypochondroplasia are rhizomelic dwarfisms with different radiographic features and no hitchhiker thumbs or severe joint contractures. Spondyloepiphyseal Dysplasia Tarda primarily affects the spine and hips, and Multiple Epiphyseal Dysplasia typically lacks the severe contractures and specific hand/foot deformities.
Question 96
A 4-year-old boy with known Spondyloepiphyseal Dysplasia Congenita (SEDc) is being evaluated. Which of the following orthopedic complications is he at highest risk for and requires careful monitoring?
View Answer & Explanation
Correct Answer: B
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDc) is characterized by odontoid hypoplasia, which significantly increases the risk of atlantoaxial instability. This can lead to spinal cord compression and neurological deficits, making it a critical complication requiring careful monitoring and often surgical stabilization. While other orthopedic issues like genu valgum (not varum) and hip dysplasia are common, atlantoaxial instability is the most life-threatening and specific to the spinal involvement in SEDc. Radial head subluxation is more common in conditions like multiple hereditary exostoses or specific forms of MED. Talipes equinovarus is characteristic of diastrophic dysplasia. Osteochondritis dissecans is a general orthopedic condition not specifically heightened in SEDc compared to other epiphyseal dysplasias.
Question 97
A 10-year-old boy presents with progressive back pain and stiffness, particularly in the morning. He has a history of mild short stature, primarily truncal. Radiographs show generalized platyspondyly with a "humped" appearance of the posterior vertebral bodies, and irregular, flattened epiphyses in the hips. The parents report no significant issues until late childhood. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Spondyloepiphyseal Dysplasia Tarda (SEDT) is an X-linked recessive disorder that typically presents in late childhood or adolescence with short-trunk dwarfism, back pain, and early degenerative changes in the spine and hips. Radiographically, it shows generalized platyspondyly with a characteristic "humped" or "pear-shaped" appearance of the posterior vertebral bodies, and irregular, flattened femoral epiphyses. Spondyloepiphyseal Dysplasia Congenita (SEDc) presents at birth or early infancy. Multiple Epiphyseal Dysplasia primarily affects the epiphyses of long bones and typically spares the spine. Achondroplasia is a rhizomelic dwarfism with normal trunk length. Morquio Syndrome is a mucopolysaccharidosis with distinct skeletal features, including severe platyspondyly and odontoid hypoplasia, but also involves corneal clouding and other systemic features not mentioned.
Question 98
A 6-year-old girl is evaluated for short stature and a waddling gait. Her parents are of normal height. Physical examination reveals bilateral coxa vara and limited hip abduction. Radiographs show flattened and irregular epiphyses in the femoral heads, with mild metaphyseal irregularities. The spine appears normal. Genetic testing is pending. Which gene mutation is most commonly associated with this presentation?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of short stature, waddling gait, coxa vara, and flattened/irregular femoral epiphyses with mild metaphyseal irregularities, and a normal spine, is highly suggestive of Multiple Epiphyseal Dysplasia (MED) or Pseudoachondroplasia. Mutations in the *COMP* (cartilage oligomeric matrix protein) gene are responsible for a significant proportion of both MED and pseudoachondroplasia cases. *FGFR3* mutations cause achondroplasia and hypochondroplasia, which have different radiographic patterns. *COL2A1* mutations are associated with Spondyloepiphyseal Dysplasia Congenita and other type II collagenopathies, which typically involve the spine. *SOX9* mutations are linked to Campomelic Dysplasia. *TRPV4* mutations are associated with certain forms of MED and SED, but *COMP* is the most common gene for this specific presentation.
Question 99
A 2-year-old boy presents with disproportionate short stature, primarily affecting his limbs. He has a history of recurrent otitis media and myopia. Physical examination reveals mild joint hypermobility. Radiographs show flattened vertebral bodies, particularly in the lumbar spine, and small, irregular epiphyses in the long bones. He has a cleft palate. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Stickler Syndrome is a group of genetic disorders, primarily involving mutations in *COL2A1*, *COL11A1*, or *COL11A2*, which are genes for type II and XI collagen. It is characterized by ocular abnormalities (myopia, retinal detachment), hearing loss (recurrent otitis media), craniofacial abnormalities (cleft palate, midface hypoplasia), and mild spondyloepiphyseal dysplasia, leading to joint hypermobility and early arthritis. The combination of short stature, flattened vertebral bodies, irregular epiphyses, and the specific extra-skeletal features (otitis media, myopia, cleft palate) points strongly to Stickler Syndrome. While some features overlap with other dysplasias, the systemic involvement is key. Achondroplasia, Diastrophic Dysplasia, Pseudoachondroplasia, and Multiple Epiphyseal Dysplasia do not typically present with this specific constellation of ocular, auditory, and craniofacial findings.
Question 100
A 5-year-old girl with a known diagnosis of Multiple Epiphyseal Dysplasia (MED) is being followed. Her radiographs show significant flattening and fragmentation of the femoral heads. Which of the following surgical interventions is most commonly considered for managing hip involvement in MED to prevent or delay severe degenerative arthritis?
View Answer & Explanation
Correct Answer: B
Rationale: Femoral osteotomy (e.g., varus derotation osteotomy) is a common surgical intervention in children and adolescents with MED and significant hip involvement (such as coxa vara or severe epiphyseal flattening) to improve joint congruity, reduce pain, and delay the onset of severe degenerative arthritis. Total hip arthroplasty is typically reserved for older patients with end-stage arthritis. Hip arthrodesis is rarely performed in children with dysplasia. Core decompression is used for avascular necrosis, which can be a complication but not the primary management for the underlying dysplasia. Resection arthroplasty is a salvage procedure.
