ABOS Orthopedic Board Review: Scoliosis, Ankylosing Spondylitis, Bone Tumors & Dysplasias | Part 31

Key Takeaway
This ABOS Orthopedic Board Review covers key topics in spinal deformities like infantile, juvenile, and adolescent scoliosis, Scheuermann's kyphosis, and Ankylosing Spondylitis. It also delves into bone dysplasias such as fibrous dysplasia, enchondromas, osteochondromas, and Ewing's sarcoma, providing essential knowledge for orthopedic surgeons preparing for their board examinations.
Question 1
A 1-year-old male is diagnosed with a 28-degree left thoracic scoliosis. His rib vertebral angle difference (RVAD) is 25 degrees. He has no neurological deficits. An MRI of the spine is normal.
View Answer & Explanation
Correct Answer: B
Rationale: In infantile idiopathic scoliosis (IIS), the rib vertebral angle difference (RVAD) is a critical prognostic indicator. An RVAD greater than 20 degrees (as in this case, 25 degrees) indicates a high likelihood of curve progression and a low chance of spontaneous resolution. These curves often require intervention, such as serial casting or growth-friendly surgery, to prevent severe deformity. Spontaneous resolution is more likely with an RVAD less than 20 degrees. Bracing can be used but often follows casting or is for less severe curves. Physical therapy does not prevent progression. Therefore, the curve is likely to progress and will likely require early intervention.
Question 2
A 7-year-old female is diagnosed with a 35-degree right thoracic scoliosis. She is Risser 0. An MRI of the spine is normal. The curve has shown progression from 25 degrees over the past 6 months.
View Answer & Explanation
Correct Answer: C
Rationale: Juvenile Idiopathic Scoliosis (JIS) is diagnosed in children between 3 and 9 years of age. Unlike infantile idiopathic scoliosis, JIS has a high rate of progression, with up to 70% of curves progressing to require surgical intervention if left untreated. Spontaneous resolution is rare. Therefore, a 35-degree progressive curve in a 7-year-old (Risser 0) carries a high risk of progression. Bracing is often the first line of treatment for progressive curves in this age group, and serial casting may also be considered. Surgical fusion is typically reserved for larger, progressive curves that fail non-operative management or are already severe, and is generally avoided if possible to allow for spinal growth.
Question 3
A 14-year-old male presents with a rigid thoracic kyphosis and mild back pain. On physical examination, he has a noticeable round back deformity that does not correct with hyperextension. Radiographs show a thoracic kyphosis measuring 70 degrees (normal 20-40 degrees) with anterior wedging of at least 5 degrees in three consecutive vertebral bodies from T7 to T10, and irregular endplates.
- A) Adolescent Idiopathic Scoliosis
- B) Congenital Kyphosis
- C) Scheuermann's Kyphosis
- D) Postural Kyphosis
- E)
Question 3
A 13-year-old female presents for a routine physical examination. On Adam's forward bend test, a noticeable right thoracic rib prominence is observed. Standing posteroanterior and lateral radiographs of the spine reveal a 22-degree right thoracic curve from T6 to T12 and a 15-degree left lumbar curve from T12 to L4. Her Risser sign is 0.
View Answer & Explanation
Correct Answer: C
Rationale: For adolescent idiopathic scoliosis (AIS) curves between 10-25 degrees in skeletally immature patients (Risser 0-2), observation with serial clinical and radiographic follow-up every 4-6 months is the standard of care. Bracing is typically indicated for curves >25 degrees in skeletally immature patients or for documented progression of curves between 20-25 degrees. Surgical consultation is reserved for larger, progressive curves, typically >45-50 degrees. Physical therapy alone has not been shown to alter the natural history of AIS. An MRI is indicated for atypical curves, rapid progression, neurological symptoms, or very young patients, none of which are present here.
Question 3
A 12-year-old female with adolescent idiopathic scoliosis (AIS) has been under observation for 18 months. Her initial Cobb angle was 24 degrees. Recent radiographs show a progression to a 32-degree right thoracic curve. She is premenarchal with a Risser sign of 1.
View Answer & Explanation
Correct Answer: B
Rationale: Bracing is indicated for skeletally immature patients (Risser 0-2, premenarchal) with progressive curves between 25-45 degrees. This patient has a 32-degree curve and a Risser 1, making her an ideal candidate for bracing to prevent further progression. Continuing observation is inappropriate given the documented progression and curve magnitude. Surgical evaluation is typically for curves >45-50 degrees. Physical therapy and anti-inflammatories do not alter curve progression. An MRI is not indicated unless there are atypical features or neurological symptoms.
Question 3
A 15-year-old female with adolescent idiopathic scoliosis (AIS) has a 55-degree right thoracic curve. She has been compliant with TLSO bracing for 2 years, but her curve has progressed from 42 degrees to 55 degrees during this time. She is Risser 4 and postmenarchal for 3 years. She reports increasing back pain and significant cosmetic deformity.
View Answer & Explanation
Correct Answer: B
Rationale: Surgical intervention is generally recommended for skeletally mature or nearly mature patients with progressive curves greater than 45-50 degrees, especially if associated with pain or significant cosmetic deformity. This patient meets these criteria, having failed bracing and exhibiting a 55-degree curve. Continuing bracing is unlikely to be effective given the progression. Physical therapy and chiropractic adjustments do not correct structural scoliosis. A bone scan is not indicated. Spontaneous stabilization is unlikely for a curve of this magnitude.
Question 3
A 6-month-old male is diagnosed with congenital scoliosis due to a fully segmented hemivertebra at T8. Radiographs show a 35-degree thoracic curve. The parents are concerned about associated anomalies.
View Answer & Explanation
Correct Answer: A
Rationale: Congenital scoliosis is frequently associated with other congenital anomalies, particularly those affecting the VACTERL association (Vertebral, Anorectal, Cardiac, Tracheoesophageal, Renal, Limb). Renal anomalies (e.g., absent kidney, horseshoe kidney) and cardiac anomalies (e.g., septal defects) are among the most common and clinically significant. Therefore, a renal ultrasound and cardiac evaluation (echocardiogram) are essential components of the initial workup. The other options are not routinely indicated unless specific symptoms or findings suggest them.
Question 3
A 10-year-old male with cerebral palsy (GMFCS Level V) presents with a rapidly progressive thoracolumbar scoliosis measuring 70 degrees, significant pelvic obliquity, and difficulty with seating and hygiene. He is non-ambulatory.
View Answer & Explanation
Correct Answer: C
Rationale: Neuromuscular scoliosis, especially in non-ambulatory patients with severe cerebral palsy, is often rapidly progressive and can lead to significant functional impairment, including seating difficulties, skin breakdown, and respiratory compromise. Curves typically progress beyond 40-50 degrees and often require surgical correction, frequently involving fusion to the pelvis to address pelvic obliquity and provide a stable base for seating. Observation and bracing are generally ineffective in preventing progression in severe neuromuscular scoliosis. Physical therapy and botulinum toxin injections may help with spasticity but do not correct structural deformity.
Question 3
A 14-year-old male presents with persistent mid-back pain and a stooped posture. On examination, he has a rigid thoracic kyphosis that does not correct with hyperextension. Standing lateral radiographs show anterior wedging of three consecutive thoracic vertebrae (T7, T8, T9) by more than 5 degrees each, and irregular endplates. There is no significant coronal plane deformity.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of rigid kyphosis and the radiographic findings of anterior wedging of at least three consecutive vertebrae by 5 degrees or more, along with irregular endplates (Schmorl's nodes), are pathognomonic for Scheuermann's kyphosis. Adolescent idiopathic scoliosis primarily involves coronal plane deformity. Congenital kyphosis would typically present earlier and with different vertebral anomalies. Postural kyphosis is flexible and corrects with hyperextension. A spinal tumor is less likely given the diffuse vertebral changes and lack of other red flag symptoms.
Question 3
A 55-year-old female presents with chronic low back pain and fatigue. She has a history of untreated adolescent idiopathic scoliosis (AIS) with a 60-degree right thoracic curve and a compensatory left lumbar curve. She reports increasing difficulty with prolonged standing and walking.
View Answer & Explanation
Correct Answer: D
Rationale: Untreated AIS curves, particularly those greater than 30-40 degrees, can progress in adulthood, often leading to degenerative changes, disc herniation, spinal stenosis, and the development of adult degenerative scoliosis. This can result in significant back pain, radiculopathy, and coronal and sagittal imbalance, which explains her symptoms. Neurological deficits are rare in AIS unless the curve is very severe or there's an underlying condition. Thoracic curves generally stabilize in adulthood, but lumbar curves may progress. Pulmonary compromise is typically seen with curves >80-90 degrees. Compensatory curves do not spontaneously resolve.
Question 3
A 14-year-old male undergoes posterior spinal fusion for a 65-degree right thoracic adolescent idiopathic scoliosis. On post-operative day 1, he complains of new-onset weakness in both lower extremities. Neurological examination reveals 2/5 strength in bilateral hip flexors and knee extensors, and absent ankle reflexes. Sensory examination is intact.
View Answer & Explanation
Correct Answer: C
Rationale: New-onset neurological deficit after scoliosis surgery is a surgical emergency. The most critical immediate step is to reduce any potential compression on the spinal cord. This often involves loosening or removing instrumentation to decompress the spinal cord. While an MRI is important for diagnosis, it should not delay decompression if instrumentation is suspected to be the cause. High-dose corticosteroids are sometimes used for spinal cord injury but are secondary to decompression. Monitoring for spontaneous recovery is inappropriate, and physical therapy is not an immediate treatment for acute neurological deficit.
Question 3
An 80-year-old female presents with severe low back pain, bilateral leg pain, and difficulty standing upright. Radiographs show a 40-degree thoracolumbar scoliosis with significant lumbar lordosis loss and sagittal imbalance. She has tried extensive non-operative management without relief.
View Answer & Explanation
Correct Answer: C
Rationale: This patient presents with severe adult degenerative scoliosis with significant sagittal imbalance and neurological symptoms (leg pain, difficulty standing upright) that have failed extensive non-operative management. Surgical correction, often involving long instrumented fusion and osteotomies to restore sagittal balance, is indicated to alleviate pain and improve function. Observation, bracing, and epidural injections are appropriate for less severe symptoms or as initial non-operative treatments, but not for this advanced stage. Reassurance is inappropriate given her severe symptoms.
Question 3
A 4-year-old male presents with a rapidly progressive 50-degree thoracic scoliosis. He has no neurological deficits or other congenital anomalies. Pulmonary function tests show early signs of restrictive lung disease. His Risser sign is 0.
View Answer & Explanation
Correct Answer: D
Rationale: This patient has early-onset scoliosis (EOS) with a severe, progressive curve and signs of pulmonary compromise. Definitive spinal fusion at this age would severely restrict thoracic growth and lung development, leading to thoracic insufficiency syndrome. Growing rod surgery (or other growth-friendly techniques like VEPTR) is the preferred treatment to control curve progression while allowing continued spinal and thoracic growth. Observation and bracing are unlikely to control such a severe, progressive curve. Vertebral body tethering is typically for larger, flexible curves in older, but still growing, adolescents.
Question 3
A 16-year-old female with adolescent idiopathic scoliosis (AIS) has a 60-degree right thoracic curve (T5-T12) and a 30-degree compensatory left lumbar curve (T12-L4). Her thoracic curve is rigid, while the lumbar curve is flexible on bending films. She is undergoing posterior spinal fusion.
Correct Answer: A
Rationale: For Lenke Type 1 curves (main thoracic curves with flexible lumbar compensatory curves), the goal is to fuse only the main thoracic curve, stopping at the stable vertebra or neutral vertebra distally. Fusing only the main thoracic curve allows the flexible lumbar curve to spontaneously correct, preserving lumbar motion segments. Fusing the entire spine or extending too far into the lumbar spine is overtreatment and sacrifices unnecessary motion. Fusing only the lumbar curve would not address the primary deformity. Hemi-vertebra excision is for congenital scoliosis, not AIS.
Question 3
A 12-year-old female undergoes a routine scoliosis screening at school. The school nurse notes a significant asymmetry of the trunk and a prominent right rib hump during the Adam's forward bend test.
View Answer & Explanation
Correct Answer: D
Rationale: A positive Adam's forward bend test indicates a potential spinal deformity and warrants further evaluation. The next appropriate step is to refer the patient to their primary care physician or an orthopedic specialist for a formal clinical examination and standing posteroanterior and lateral radiographs of the spine to measure the Cobb angle and confirm the diagnosis of scoliosis. Reassurance is inappropriate. Surgical consultation and bracing are premature without radiographic confirmation and curve measurement. Physical therapy alone does not correct structural scoliosis.
Question 3
A 13-year-old female is prescribed a thoracolumbosacral orthosis (TLSO) for a 30-degree progressive adolescent idiopathic scoliosis. Her parents ask how the brace works to correct the curve.
View Answer & Explanation
Correct Answer: C
Rationale: Bracing for AIS works by applying three-point corrective forces to the curve, aiming to prevent further progression of the curve during the remaining growth period. It does not typically reverse the curve or remodel vertebral bodies, nor does it work by traction or muscle strengthening. The primary goal is to hold the curve stable and prevent it from worsening, allowing the spine to grow straighter. It is not merely passive support, but an active corrective force.
Question 3
A 68-year-old female presents with mild to moderate low back pain and occasional left leg numbness. Radiographs show a 35-degree degenerative lumbar scoliosis with mild central canal stenosis. She has no significant functional limitations and is otherwise healthy.
View Answer & Explanation
Correct Answer: C
Rationale: For adult degenerative scoliosis with mild to moderate symptoms and no significant functional limitations, non-operative management is the first-line treatment. This includes observation, physical therapy (focusing on core strengthening, flexibility, and posture), and pain management with NSAIDs or other analgesics. Epidural steroid injections and nerve blocks can be considered for radicular symptoms if initial conservative measures fail. Surgical intervention is reserved for severe, progressive symptoms, neurological deficits, or significant deformity that has failed extensive non-operative treatment. Bracing is generally not effective for adult degenerative scoliosis. Vertebroplasty is for vertebral compression fractures, not scoliosis.
Question 3
During a posterior spinal fusion for a 70-degree adolescent idiopathic scoliosis, the surgical team utilizes intraoperative neurological monitoring to detect potential spinal cord compromise.
View Answer & Explanation
Correct Answer: B
Rationale: The gold standard for intraoperative spinal cord monitoring during scoliosis surgery involves a combination of Somatosensory Evoked Potentials (SSEPs) and Transcranial Motor Evoked Potentials (TcMEPs). SSEPs monitor the dorsal columns (sensory pathways), while TcMEPs monitor the corticospinal tracts (motor pathways). The combination provides comprehensive assessment of both sensory and motor function of the spinal cord, allowing for early detection of potential injury. EEG and EMG are less specific for spinal cord function. NCS and QST are diagnostic tools, not typically used for intraoperative monitoring. VEPs, BAEPs, and intracranial monitoring are not relevant to spinal cord function during scoliosis surgery.
Question 3
A 2-year-old female is diagnosed with congenital scoliosis due to a fully segmented hemivertebra at L2. Her initial curve measured 25 degrees. Which of the following factors is most predictive of curve progression in congenital scoliosis?
View Answer & Explanation
Correct Answer: C
Rationale: The type of vertebral anomaly is the most significant factor influencing curve progression in congenital scoliosis. Fully segmented hemivertebrae, especially those with contralateral bar formation, have the highest risk of progression due to continuous asymmetric growth. Block vertebrae or unsegmented bars without hemivertebrae have a lower risk. While initial curve magnitude can be a factor, the underlying anomaly dictates the growth potential. Gender and location (thoracic vs. lumbar) are less predictive than the specific anomaly. Associated cardiac anomalies are important for overall health but do not directly predict curve progression.
Question 3
A 14-year-old male presents with a rapidly progressive 50-degree thoracolumbar scoliosis. On examination, he is tall, thin, has arachnodactyly, and a positive wrist and thumb sign. An echocardiogram reveals aortic root dilation.
View Answer & Explanation
Correct Answer: B
Rationale: This patient's presentation is highly suggestive of Marfan syndrome. Patients with Marfan syndrome often have rapidly progressive scoliosis that is less responsive to bracing. Due to the rapid progression and potential for severe deformity, surgical intervention (spinal fusion) is often considered at lower curve magnitudes (e.g., 40-45 degrees) compared to idiopathic scoliosis. Marfan patients also have an increased risk of dural ectasia, which can complicate surgery, and a higher risk of pseudarthrosis due to poor bone quality. Postoperative pulmonary complications can be more common due to underlying lung issues.
Question 3
A 17-year-old female, 2 years status post posterior spinal fusion for adolescent idiopathic scoliosis, presents with persistent, localized back pain at the caudal end of her fusion. Radiographs show a slight loss of correction and lucency around one of the distal pedicle screws. A CT scan confirms a lack of bony bridging across the fusion mass at L1-L2.
View Answer & Explanation
Correct Answer: C
Rationale: The patient's symptoms (persistent, localized pain, loss of correction) combined with radiographic findings (lucency around hardware, lack of bony bridging on CT) are classic for pseudarthrosis, which is a failure of bony fusion. Adjacent segment disease would typically involve symptoms and degenerative changes at a level immediately above or below the fusion. Spinal infection would present with systemic signs (fever, elevated inflammatory markers) and different radiographic features. Hardware failure can be a consequence of pseudarthrosis, but the underlying issue is the lack of fusion. Normal post-fusion pain typically resolves over time, and new or persistent pain with loss of correction is concerning.
Question 3
A 72-year-old male with adult degenerative scoliosis presents with severe back pain, difficulty standing upright, and a forward-stooped posture. His standing lateral radiographs show a significant positive sagittal imbalance with a C7 plumb line falling 10 cm anterior to the sacrum.
View Answer & Explanation
Correct Answer: B
Rationale: In adult spinal deformity, sagittal imbalance (e.g., positive sagittal vertical axis, loss of lumbar lordosis) is a critical factor contributing to pain, disability, and functional limitations, often more so than coronal deformity. The forward-stooped posture and difficulty standing upright are
Question 4
A 13-year-old female presents for a routine physical examination. On Adam's forward bend test, a noticeable right thoracic rib prominence is observed. Standing posteroanterior and lateral radiographs of the spine reveal a 22-degree right thoracic curve from T6 to T12 and a 15-degree left lumbar curve from T12 to L4. Her Risser sign is 0.
View Answer & Explanation
Correct Answer: C
Rationale: For adolescent idiopathic scoliosis (AIS) curves between 10-25 degrees in skeletally immature patients (Risser 0-2), observation with serial clinical and radiographic follow-up every 4-6 months is the standard of care. Bracing is typically indicated for curves >25 degrees in skeletally immature patients or for documented progression of curves between 20-25 degrees. Surgical consultation is reserved for larger, progressive curves, typically >45-50 degrees. Physical therapy alone has not been shown to alter the natural history of AIS. An MRI is indicated for atypical curves, rapid progression, neurological symptoms, or very young patients, none of which are present here.
Question 5
A 12-year-old female with adolescent idiopathic scoliosis (AIS) has been under observation for 18 months. Her initial Cobb angle was 24 degrees. Recent radiographs show a progression to a 32-degree right thoracic curve. She is premenarchal with a Risser sign of 1.
View Answer & Explanation
Correct Answer: B
Rationale: Bracing is indicated for skeletally immature patients (Risser 0-2, premenarchal) with progressive curves between 25-45 degrees. This patient has a 32-degree curve and a Risser 1, making her an ideal candidate for bracing to prevent further progression. Continuing observation is inappropriate given the documented progression and curve magnitude. Surgical evaluation is typically for curves >45-50 degrees. Physical therapy and anti-inflammatories do not alter curve progression. An MRI is not indicated unless there are atypical features or neurological symptoms.
Question 6
A 15-year-old female with adolescent idiopathic scoliosis (AIS) has a 55-degree right thoracic curve. She has been compliant with TLSO bracing for 2 years, but her curve has progressed from 42 degrees to 55 degrees during this time. She is Risser 4 and postmenarchal for 3 years. She reports increasing back pain and significant cosmetic deformity.
View Answer & Explanation
Correct Answer: B
Rationale: Surgical intervention is generally recommended for skeletally mature or nearly mature patients with progressive curves greater than 45-50 degrees, especially if associated with pain or significant cosmetic deformity. This patient meets these criteria, having failed bracing and exhibiting a 55-degree curve. Continuing bracing is unlikely to be effective given the progression. Physical therapy and chiropractic adjustments do not correct structural scoliosis. A bone scan is not indicated. Spontaneous stabilization is unlikely for a curve of this magnitude.
Question 7
A 6-month-old male is diagnosed with congenital scoliosis due to a fully segmented hemivertebra at T8. Radiographs show a 35-degree thoracic curve. The parents are concerned about associated anomalies.
View Answer & Explanation
Correct Answer: A
Rationale: Congenital scoliosis is frequently associated with other congenital anomalies, particularly those affecting the VACTERL association (Vertebral, Anorectal, Cardiac, Tracheoesophageal, Renal, Limb). Renal anomalies (e.g., absent kidney, horseshoe kidney) and cardiac anomalies (e.g., septal defects) are among the most common and clinically significant. Therefore, a renal ultrasound and cardiac evaluation (echocardiogram) are essential components of the initial workup. The other options are not routinely indicated unless specific symptoms or findings suggest them.
Question 8
A 10-year-old male with cerebral palsy (GMFCS Level V) presents with a rapidly progressive thoracolumbar scoliosis measuring 70 degrees, significant pelvic obliquity, and difficulty with seating and hygiene. He is non-ambulatory.
View Answer & Explanation
Correct Answer: C
Rationale: Neuromuscular scoliosis, especially in non-ambulatory patients with severe cerebral palsy, is often rapidly progressive and can lead to significant functional impairment, including seating difficulties, skin breakdown, and respiratory compromise. Curves typically progress beyond 40-50 degrees and often require surgical correction, frequently involving fusion to the pelvis to address pelvic obliquity and provide a stable base for seating. Observation and bracing are generally ineffective in preventing progression in severe neuromuscular scoliosis. Physical therapy and botulinum toxin injections may help with spasticity but do not correct structural deformity.
Question 9
A 14-year-old male presents with persistent mid-back pain and a stooped posture. On examination, he has a rigid thoracic kyphosis that does not correct with hyperextension. Standing lateral radiographs show anterior wedging of three consecutive thoracic vertebrae (T7, T8, T9) by more than 5 degrees each, and irregular endplates. There is no significant coronal plane deformity.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of rigid kyphosis and the radiographic findings of anterior wedging of at least three consecutive vertebrae by 5 degrees or more, along with irregular endplates (Schmorl's nodes), are pathognomonic for Scheuermann's kyphosis. Adolescent idiopathic scoliosis primarily involves coronal plane deformity. Congenital kyphosis would typically present earlier and with different vertebral anomalies. Postural kyphosis is flexible and corrects with hyperextension. A spinal tumor is less likely given the diffuse vertebral changes and lack of other red flag symptoms.
Question 10
A 55-year-old female presents with chronic low back pain and fatigue. She has a history of untreated adolescent idiopathic scoliosis (AIS) with a 60-degree right thoracic curve and a compensatory left lumbar curve. She reports increasing difficulty with prolonged standing and walking.
View Answer & Explanation
Correct Answer: D
Rationale: Untreated AIS curves, particularly those greater than 30-40 degrees, can progress in adulthood, often leading to degenerative changes, disc herniation, spinal stenosis, and the development of adult degenerative scoliosis. This can result in significant back pain, radiculopathy, and coronal and sagittal imbalance, which explains her symptoms. Neurological deficits are rare in AIS unless the curve is very severe or there's an underlying condition. Thoracic curves generally stabilize in adulthood, but lumbar curves may progress. Pulmonary compromise is typically seen with curves >80-90 degrees. Compensatory curves do not spontaneously resolve.
Question 11
A 14-year-old male undergoes posterior spinal fusion for a 65-degree right thoracic adolescent idiopathic scoliosis. On post-operative day 1, he complains of new-onset weakness in both lower extremities. Neurological examination reveals 2/5 strength in bilateral hip flexors and knee extensors, and absent ankle reflexes. Sensory examination is intact.
View Answer & Explanation
Correct Answer: C
Rationale: New-onset neurological deficit after scoliosis surgery is a surgical emergency. The most critical immediate step is to reduce any potential compression on the spinal cord. This often involves loosening or removing instrumentation to decompress the spinal cord. While an MRI is important for diagnosis, it should not delay decompression if instrumentation is suspected to be the cause. High-dose corticosteroids are sometimes used for spinal cord injury but are secondary to decompression. Monitoring for spontaneous recovery is inappropriate, and physical therapy is not an immediate treatment for acute neurological deficit.
Question 12
An 80-year-old female presents with severe low back pain, bilateral leg pain, and difficulty standing upright. Radiographs show a 40-degree thoracolumbar scoliosis with significant lumbar lordosis loss and sagittal imbalance. She has tried extensive non-operative management without relief.
View Answer & Explanation
Correct Answer: C
Rationale: This patient presents with severe adult degenerative scoliosis with significant sagittal imbalance and neurological symptoms (leg pain, difficulty standing upright) that have failed extensive non-operative management. Surgical correction, often involving long instrumented fusion and osteotomies to restore sagittal balance, is indicated to alleviate pain and improve function. Observation, bracing, and epidural injections are appropriate for less severe symptoms or as initial non-operative treatments, but not for this advanced stage. Reassurance is inappropriate given her severe symptoms.
Question 13
A 4-year-old male presents with a rapidly progressive 50-degree thoracic scoliosis. He has no neurological deficits or other congenital anomalies. Pulmonary function tests show early signs of restrictive lung disease. His Risser sign is 0.
View Answer & Explanation
Correct Answer: D
Rationale: This patient has early-onset scoliosis (EOS) with a severe, progressive curve and signs of pulmonary compromise. Definitive spinal fusion at this age would severely restrict thoracic growth and lung development, leading to thoracic insufficiency syndrome. Growing rod surgery (or other growth-friendly techniques like VEPTR) is the preferred treatment to control curve progression while allowing continued spinal and thoracic growth. Observation and bracing are unlikely to control such a severe, progressive curve. Vertebral body tethering is typically for larger, flexible curves in older, but still growing, adolescents.
Question 14
A 16-year-old female with adolescent idiopathic scoliosis (AIS) has a 60-degree right thoracic curve (T5-T12) and a 30-degree compensatory left lumbar curve (T12-L4). Her thoracic curve is rigid, while the lumbar curve is flexible on bending films. She is undergoing posterior spinal fusion.
Correct Answer: A
Rationale: For Lenke Type 1 curves (main thoracic curves with flexible lumbar compensatory curves), the goal is to fuse only the main thoracic curve, stopping at the stable vertebra or neutral vertebra distally. Fusing only the main thoracic curve allows the flexible lumbar curve to spontaneously correct, preserving lumbar motion segments. Fusing the entire spine or extending too far into the lumbar spine is overtreatment and sacrifices unnecessary motion. Fusing only the lumbar curve would not address the primary deformity. Hemi-vertebra excision is for congenital scoliosis, not AIS.
Question 15
A 12-year-old female undergoes a routine scoliosis screening at school. The school nurse notes a significant asymmetry of the trunk and a prominent right rib hump during the Adam's forward bend test.
View Answer & Explanation
Correct Answer: D
Rationale: A positive Adam's forward bend test indicates a potential spinal deformity and warrants further evaluation. The next appropriate step is to refer the patient to their primary care physician or an orthopedic specialist for a formal clinical examination and standing posteroanterior and lateral radiographs of the spine to measure the Cobb angle and confirm the diagnosis of scoliosis. Reassurance is inappropriate. Surgical consultation and bracing are premature without radiographic confirmation and curve measurement. Physical therapy alone does not correct structural scoliosis.
Question 16
A 13-year-old female is prescribed a thoracolumbosacral orthosis (TLSO) for a 30-degree progressive adolescent idiopathic scoliosis. Her parents ask how the brace works to correct the curve.
View Answer & Explanation
Correct Answer: C
Rationale: Bracing for AIS works by applying three-point corrective forces to the curve, aiming to prevent further progression of the curve during the remaining growth period. It does not typically reverse the curve or remodel vertebral bodies, nor does it work by traction or muscle strengthening. The primary goal is to hold the curve stable and prevent it from worsening, allowing the spine to grow straighter. It is not merely passive support, but an active corrective force.
Question 17
A 68-year-old female presents with mild to moderate low back pain and occasional left leg numbness. Radiographs show a 35-degree degenerative lumbar scoliosis with mild central canal stenosis. She has no significant functional limitations and is otherwise healthy.
View Answer & Explanation
Correct Answer: C
Rationale: For adult degenerative scoliosis with mild to moderate symptoms and no significant functional limitations, non-operative management is the first-line treatment. This includes observation, physical therapy (focusing on core strengthening, flexibility, and posture), and pain management with NSAIDs or other analgesics. Epidural steroid injections and nerve blocks can be considered for radicular symptoms if initial conservative measures fail. Surgical intervention is reserved for severe, progressive symptoms, neurological deficits, or significant deformity that has failed extensive non-operative treatment. Bracing is generally not effective for adult degenerative scoliosis. Vertebroplasty is for vertebral compression fractures, not scoliosis.
Question 18
During a posterior spinal fusion for a 70-degree adolescent idiopathic scoliosis, the surgical team utilizes intraoperative neurological monitoring to detect potential spinal cord compromise.
View Answer & Explanation
Correct Answer: B
Rationale: The gold standard for intraoperative spinal cord monitoring during scoliosis surgery involves a combination of Somatosensory Evoked Potentials (SSEPs) and Transcranial Motor Evoked Potentials (TcMEPs). SSEPs monitor the dorsal columns (sensory pathways), while TcMEPs monitor the corticospinal tracts (motor pathways). The combination provides comprehensive assessment of both sensory and motor function of the spinal cord, allowing for early detection of potential injury. EEG and EMG are less specific for spinal cord function. NCS and QST are diagnostic tools, not typically used for intraoperative monitoring. VEPs, BAEPs, and intracranial monitoring are not relevant to spinal cord function during scoliosis surgery.
Question 19
A 2-year-old female is diagnosed with congenital scoliosis due to a fully segmented hemivertebra at L2. Her initial curve measured 25 degrees. Which of the following factors is most predictive of curve progression in congenital scoliosis?
View Answer & Explanation
Correct Answer: C
Rationale: The type of vertebral anomaly is the most significant factor influencing curve progression in congenital scoliosis. Fully segmented hemivertebrae, especially those with contralateral bar formation, have the highest risk of progression due to continuous asymmetric growth. Block vertebrae or unsegmented bars without hemivertebrae have a lower risk. While initial curve magnitude can be a factor, the underlying anomaly dictates the growth potential. Gender and location (thoracic vs. lumbar) are less predictive than the specific anomaly. Associated cardiac anomalies are important for overall health but do not directly predict curve progression.
Question 20
A 14-year-old male presents with a rapidly progressive 50-degree thoracolumbar scoliosis. On examination, he is tall, thin, has arachnodactyly, and a positive wrist and thumb sign. An echocardiogram reveals aortic root dilation.
View Answer & Explanation
Correct Answer: B
Rationale: This patient's presentation is highly suggestive of Marfan syndrome. Patients with Marfan syndrome often have rapidly progressive scoliosis that is less responsive to bracing. Due to the rapid progression and potential for severe deformity, surgical intervention (spinal fusion) is often considered at lower curve magnitudes (e.g., 40-45 degrees) compared to idiopathic scoliosis. Marfan patients also have an increased risk of dural ectasia, which can complicate surgery, and a higher risk of pseudarthrosis due to poor bone quality. Postoperative pulmonary complications can be more common due to underlying lung issues.
Question 21
A 17-year-old female, 2 years status post posterior spinal fusion for adolescent idiopathic scoliosis, presents with persistent, localized back pain at the caudal end of her fusion. Radiographs show a slight loss of correction and lucency around one of the distal pedicle screws. A CT scan confirms a lack of bony bridging across the fusion mass at L1-L2.
View Answer & Explanation
Correct Answer: C
Rationale: The patient's symptoms (persistent, localized pain, loss of correction) combined with radiographic findings (lucency around hardware, lack of bony bridging on CT) are classic for pseudarthrosis, which is a failure of bony fusion. Adjacent segment disease would typically involve symptoms and degenerative changes at a level immediately above or below the fusion. Spinal infection would present with systemic signs (fever, elevated inflammatory markers) and different radiographic features. Hardware failure can be a consequence of pseudarthrosis, but the underlying issue is the lack of fusion. Normal post-fusion pain typically resolves over time, and new or persistent pain with loss of correction is concerning.
Question 22
A 3-month-old male child is brought to the clinic by his parents due to multiple observed deformities since birth. Physical examination reveals an inclined position of the head, asymmetry of the skull, and a foot deformity. This constellation of findings is part of a recognized syndrome.
View Answer & Explanation
Correct Answer: C
Rationale: The "Syndrome of Seven Symptoms" explicitly lists dysplasia of the hip as one of its characteristic components, alongside scoliosis, lumbodorsal kyphosis, inclined position of the head (torticollis), asymmetry of the skull, asymmetry of the pelvis, and foot deformity. Craniosynostosis (D) can cause skull asymmetry but is not listed as a primary component of this specific syndrome.
Question 23
A 3-month-old female infant presents with the "Syndrome of Seven Symptoms," including scoliosis, lumbodorsal kyphosis, torticollis, skull asymmetry, hip dysplasia, pelvic asymmetry, and a foot deformity. Given the diagnosis of developmental dysplasia of the hip (DDH) as part of this syndrome, what is the most appropriate initial imaging modality for confirmation and assessment?
View Answer & Explanation
Correct Answer: C
Rationale: For infants up to 4-6 months of age, dynamic ultrasound of the hips is the gold standard for diagnosing and assessing developmental dysplasia of the hip (DDH). This is because the femoral head and acetabulum are largely cartilaginous at this age, making radiographs (A) less reliable for visualizing the bony anatomy and stability. MRI (B) and CT (D) are typically reserved for more complex cases or pre-operative planning, and arthrography (E) is an invasive procedure usually performed in the operating room.
Question 24
A 3-month-old male infant is diagnosed with the "Syndrome of Seven Symptoms," which includes an inclined position of the head (torticollis). Physical examination confirms right-sided congenital muscular torticollis.
View Answer & Explanation
Correct Answer: C
Rationale: The initial recommended treatment for congenital muscular torticollis in infants is physical therapy, focusing on passive stretching of the sternocleidomastoid muscle and active range of motion exercises. This approach is successful in the vast majority of cases. Surgical release (A) is reserved for refractory cases, typically after 6-12 months of failed conservative treatment. Observation (E) without active intervention is inappropriate as it can lead to persistent deformity and secondary issues like plagiocephaly.
Question 25
A 3-month-old female presents with the "Syndrome of Seven Symptoms," including a severe right clubfoot deformity. The foot exhibits equinus, varus, adduction, and cavus.
View Answer & Explanation
Correct Answer: B
Rationale: The Ponseti method, involving serial manipulation and casting, is the universally accepted initial non-operative treatment for congenital clubfoot. It aims to gradually correct all components of the deformity. Surgical release (A) is typically reserved for cases that fail Ponseti treatment or for recurrence. Dynamic bracing (C) is used *after* casting to maintain correction, not as the initial treatment. Observation and passive stretching (E) are insufficient for a true clubfoot deformity.
Question 26
A 3-month-old infant with the "Syndrome of Seven Symptoms" is noted to have scoliosis on physical examination. The curve appears flexible.
View Answer & Explanation
Correct Answer: D
Rationale: For non-ambulatory infants, supine anteroposterior (AP) and lateral spine radiographs are the most appropriate initial imaging studies to evaluate scoliosis. Standing radiographs (A) are not feasible for a 3-month-old. MRI (B) is indicated if there are neurological symptoms, rapid progression, or suspicion of congenital anomalies, but not as the initial screening for a flexible curve. Ultrasound (C) has limited utility for bony spinal deformities, and CT (E) involves higher radiation and is typically reserved for detailed bony anatomy assessment.
Question 27
A 3-month-old child presents with the "Syndrome of Seven Symptoms," a constellation of congenital deformities including scoliosis, lumbodorsal kyphosis, torticollis, skull asymmetry, hip dysplasia, pelvic asymmetry, and foot deformity.
- A) Isolated birth trauma
- B) Primary nutritional deficiency
- C) Underlying neuromuscular disorder or genetic syndrome
- D) Transient positional molding
- E
Question 27
A 3-month-old infant presents with an inclined head position to the right. On examination, the pediatrician notes a palpable mass in the sternocleidomastoid muscle and mild plagiocephaly. Given the "Syndrome of Seven Symptoms," which of the following additional findings would be *most consistent* with this diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The Syndrome of Seven Symptoms explicitly includes inclined position of the head (torticollis), asymmetry of the skull, and dysplasia of the hip. The vignette describes torticollis and skull asymmetry, making dysplasia of the hip a highly consistent additional finding from the syndrome's listed components. The other options are not listed components of this specific syndrome.
Question 27
A 3-month-old child is brought for evaluation due to concerns about their posture and head shape. Physical examination reveals a noticeable C-shaped curve in the spine and a flattened area on one side of the skull. The parents also report difficulty with diaper changes due to a perceived difference in leg length. Which of the following spinal deformities is a recognized component of the "Syndrome of Seven Symptoms"?
View Answer & Explanation
Correct Answer: C
Rationale: The Syndrome of Seven Symptoms explicitly lists "scoliosis" and "lumbodorsal kyphosis" as components. The vignette describes a C-shaped spinal curve (scoliosis) and a flattened skull (asymmetry of the skull), which are consistent with the syndrome. Lumbodorsal kyphosis is the other specific spinal deformity mentioned. Spondylolisthesis, Scheuermann's kyphosis, congenital block vertebrae, and atlantoaxial instability are not listed components of this specific syndrome.
Question 27
A 3-month-old infant is referred to orthopedics for evaluation of multiple congenital deformities. The orthopedist notes an inclined head position, asymmetry of the skull, and a foot deformity. Based on the "Syndrome of Seven Symptoms," which of the following foot deformities is *specifically mentioned* as a potential component?
View Answer & Explanation
Correct Answer: C
Rationale: The Syndrome of Seven Symptoms explicitly lists "foot deformity (e.g., clubfoot or calcaneal deformity)" as one of its components. Clubfoot is one of the two specific examples provided. Metatarsus adductus, vertical talus, pes planus, and tarsal coalition are not specifically mentioned in the description of this syndrome.
Question 27
A 3-month-old child presents with a complex array of musculoskeletal deformities, including an S-shaped spinal curve and an uneven appearance of the hips. The examining physician suspects the "Syndrome of Seven Symptoms." Which of the following is *not* a listed component of this syndrome?
View Answer & Explanation
Correct Answer: D
Rationale: The Syndrome of Seven Symptoms includes scoliosis, asymmetry of the pelvis, dysplasia of the hip, and inclined position of the head. Genu varum (bowlegs) is not mentioned as one of the seven symptoms that define this specific syndrome.
Question 27
A 3-month-old infant is seen in clinic with a constellation of findings including a noticeable head tilt, a flattened area on the back of the head, and a prominent curve in the lower back. The physician is considering the "Syndrome of Seven Symptoms." What is the *earliest age* at which this syndrome is typically described in the provided context?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for the Syndrome of Seven Symptoms explicitly refers to "a 3-month-old child" in the figure description, indicating this is the age at which these deformities are observed and the syndrome is described in this case. While some components might be present at birth, the syndrome is presented in the context of a 3-month-old.
Question 27
A 3-month-old male infant is evaluated for multiple congenital anomalies. On physical exam, he exhibits a fixed torticollis, a noticeable flattening of the occiput, and a prominent posterior spinal curvature in the thoracolumbar region. The physician notes these findings are consistent with the "Syndrome of Seven Symptoms." Which of the following deformities is *also* a characteristic feature of this syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: The Syndrome of Seven Symptoms includes inclined position of the head (torticollis), asymmetry of the skull, lumbodorsal kyphosis, and asymmetry of the pelvis. The vignette describes torticollis, skull asymmetry, and lumbodorsal kyphosis. Asymmetry of the pelvis is another listed component. Polydactyly, syndactyly, craniosynostosis, and brachial plexus palsy are not listed components of this specific syndrome.
Question 27
A 3-month-old child presents with a complex presentation of musculoskeletal issues. The clinical image provided (Fig. 13.7) depicts a child with multiple deformities consistent with the "Syndrome of Seven Symptoms." Which of the following deformities is *clearly visible or strongly suggested* in the provided image?
View Answer & Explanation
Correct Answer: C
Rationale: The image (Fig. 13.7) clearly demonstrates a significant lateral curvature of the spine, which is consistent with scoliosis, one of the described symptoms of the Syndrome of Seven Symptoms. The other options are not clearly visible or suggested in the provided image.
Question 27
A 3-month-old infant is diagnosed with the "Syndrome of Seven Symptoms" based on the presence of scoliosis, lumbodorsal kyphosis, torticollis, skull asymmetry, and a foot deformity. What *specific type* of foot deformity is mentioned as a possibility within this syndrome?
<img src='/media/Hutaiforthoatlas/atlas-1314-sy
Question 28
A 3-month-old infant presents with an inclined head position to the right. On examination, the pediatrician notes a palpable mass in the sternocleidomastoid muscle and mild plagiocephaly. Given the "Syndrome of Seven Symptoms," which of the following additional findings would be *most consistent* with this diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The Syndrome of Seven Symptoms explicitly includes inclined position of the head (torticollis), asymmetry of the skull, and dysplasia of the hip. The vignette describes torticollis and skull asymmetry, making dysplasia of the hip a highly consistent additional finding from the syndrome's listed components. The other options are not listed components of this specific syndrome.
Question 29
A 3-month-old child is brought for evaluation due to concerns about their posture and head shape. Physical examination reveals a noticeable C-shaped curve in the spine and a flattened area on one side of the skull. The parents also report difficulty with diaper changes due to a perceived difference in leg length. Which of the following spinal deformities is a recognized component of the "Syndrome of Seven Symptoms"?
View Answer & Explanation
Correct Answer: C
Rationale: The Syndrome of Seven Symptoms explicitly lists "scoliosis" and "lumbodorsal kyphosis" as components. The vignette describes a C-shaped spinal curve (scoliosis) and a flattened skull (asymmetry of the skull), which are consistent with the syndrome. Lumbodorsal kyphosis is the other specific spinal deformity mentioned. Spondylolisthesis, Scheuermann's kyphosis, congenital block vertebrae, and atlantoaxial instability are not listed components of this specific syndrome.
Question 30
A 3-month-old infant is referred to orthopedics for evaluation of multiple congenital deformities. The orthopedist notes an inclined head position, asymmetry of the skull, and a foot deformity. Based on the "Syndrome of Seven Symptoms," which of the following foot deformities is *specifically mentioned* as a potential component?
View Answer & Explanation
Correct Answer: C
Rationale: The Syndrome of Seven Symptoms explicitly lists "foot deformity (e.g., clubfoot or calcaneal deformity)" as one of its components. Clubfoot is one of the two specific examples provided. Metatarsus adductus, vertical talus, pes planus, and tarsal coalition are not specifically mentioned in the description of this syndrome.
Question 31
A 3-month-old child presents with a complex array of musculoskeletal deformities, including an S-shaped spinal curve and an uneven appearance of the hips. The examining physician suspects the "Syndrome of Seven Symptoms." Which of the following is *not* a listed component of this syndrome?
View Answer & Explanation
Correct Answer: D
Rationale: The Syndrome of Seven Symptoms includes scoliosis, asymmetry of the pelvis, dysplasia of the hip, and inclined position of the head. Genu varum (bowlegs) is not mentioned as one of the seven symptoms that define this specific syndrome.
Question 32
A 3-month-old infant is seen in clinic with a constellation of findings including a noticeable head tilt, a flattened area on the back of the head, and a prominent curve in the lower back. The physician is considering the "Syndrome of Seven Symptoms." What is the *earliest age* at which this syndrome is typically described in the provided context?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for the Syndrome of Seven Symptoms explicitly refers to "a 3-month-old child" in the figure description, indicating this is the age at which these deformities are observed and the syndrome is described in this case. While some components might be present at birth, the syndrome is presented in the context of a 3-month-old.
Question 33
A 3-month-old male infant is evaluated for multiple congenital anomalies. On physical exam, he exhibits a fixed torticollis, a noticeable flattening of the occiput, and a prominent posterior spinal curvature in the thoracolumbar region. The physician notes these findings are consistent with the "Syndrome of Seven Symptoms." Which of the following deformities is *also* a characteristic feature of this syndrome?
View Answer & Explanation
Correct Answer: C
Rationale: The Syndrome of Seven Symptoms includes inclined position of the head (torticollis), asymmetry of the skull, lumbodorsal kyphosis, and asymmetry of the pelvis. The vignette describes torticollis, skull asymmetry, and lumbodorsal kyphosis. Asymmetry of the pelvis is another listed component. Polydactyly, syndactyly, craniosynostosis, and brachial plexus palsy are not listed components of this specific syndrome.
Question 34
A 3-month-old child presents with a complex presentation of musculoskeletal issues. The clinical image provided (Fig. 13.7) depicts a child with multiple deformities consistent with the "Syndrome of Seven Symptoms." Which of the following deformities is *clearly visible or strongly suggested* in the provided image?
View Answer & Explanation
Correct Answer: C
Rationale: The image (Fig. 13.7) clearly demonstrates a significant lateral curvature of the spine, which is consistent with scoliosis, one of the described symptoms of the Syndrome of Seven Symptoms. The other options are not clearly visible or suggested in the provided image.
Question 35
A 28-year-old male presents with a 9-month history of insidious onset low back pain and stiffness. The pain is worse in the morning, lasts for several hours, and improves with activity. He reports occasional alternating buttock pain. Physical examination reveals decreased lumbar spine flexion and a positive Schober test. Radiographs of the pelvis show bilateral, symmetric sacroiliac joint erosions and sclerosis. Laboratory tests are notable for an elevated ESR and positive HLA-B27.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of inflammatory back pain (worse with rest, better with activity, morning stiffness), decreased spinal mobility, bilateral sacroiliitis on radiographs, elevated ESR, and positive HLA-B27 are classic diagnostic criteria for Ankylosing Spondylitis. Mechanical low back pain typically worsens with activity and improves with rest. Lumbar disc herniation usually presents with radicular symptoms. DISH is characterized by flowing ossification along the anterolateral spine and typically spares the sacroiliac joints. Psoriatic arthritis can involve the spine but often presents with asymmetric sacroiliitis and peripheral joint involvement, and the overall picture is less typical than for AS.
Question 36
A 35-year-old male with a confirmed diagnosis of Ankylosing Spondylitis is discussing the genetic predisposition of his condition with his physician. He asks about the most strongly associated genetic marker. Which of the following is the most significant genetic association with Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: D
Rationale: HLA-B27 is the most strongly associated genetic marker with Ankylosing Spondylitis, found in over 90% of Caucasian patients with the disease. While its presence is not diagnostic alone, it is a key predisposing factor. Rheumatoid Factor and Anti-CCP antibodies are associated with rheumatoid arthritis. HLA-DR4 is associated with rheumatoid arthritis. ANA is associated with systemic lupus erythematosus and other autoimmune conditions.
Question 37
A 22-year-old man presents with chronic low back pain. Physical examination reveals tenderness over the sacroiliac joints. Initial radiographs are ordered to evaluate for Ankylosing Spondylitis. Which of the following radiographic findings is typically the earliest and most characteristic sign of Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: Bilateral sacroiliitis, characterized by erosions, sclerosis, and joint space narrowing of the sacroiliac joints, is typically the earliest and most characteristic radiographic finding in Ankylosing Spondylitis. Squaring of vertebral bodies and syndesmophytes ("bamboo spine") are later manifestations of spinal involvement. Atlantoaxial subluxation is a rare, late complication. Diffuse osteopenia can occur but is not the earliest or most specific sign.
Question 38
A 55-year-old male with a long-standing history of Ankylosing Spondylitis presents with severe, fixed thoracolumbar kyphosis, limiting his ability to look forward and perform daily activities. Radiographs of his spine show extensive ossification of the anterior longitudinal ligament and intervertebral discs, leading to a characteristic appearance. Which of the following terms best describes this advanced radiographic finding?
View Answer & Explanation
Correct Answer: D
Rationale: "Bamboo spine" refers to the classic appearance of the spine in advanced Ankylosing Spondylitis, caused by extensive syndesmophyte formation and ossification of the spinal ligaments, leading to complete spinal fusion. Andersson lesions are destructive lesions of the vertebral bodies and discs. Romanus lesions (shiny corner sign) are early erosions at the vertebral body corners. Carrot stick fracture is a type of spinal fracture seen in fused spines, not the overall appearance of the fused spine itself.
Question 39
A 30-year-old male with recently diagnosed Ankylosing Spondylitis reports recurrent episodes of painful, red eyes, often accompanied by photophobia and blurred vision. He has seen an ophthalmologist who diagnosed him with anterior uveitis. Which of the following extra-articular manifestations is most commonly associated with Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: Anterior uveitis (or iritis) is the most common extra-articular manifestation of Ankylosing Spondylitis, affecting up to 40% of patients. While Inflammatory Bowel Disease, aortic insufficiency, and pulmonary fibrosis can occur, they are less common than uveitis. Psoriasis is a primary feature of psoriatic arthritis, another spondyloarthropathy, but not the most common extra-articular manifestation of AS itself.
Question 40
A 25-year-old male is diagnosed with early Ankylosing Spondylitis based on inflammatory back pain, positive HLA-B27, and early sacroiliitis on MRI. His symptoms are moderate, and he has no significant extra-articular manifestations. What is generally considered the first-line pharmacologic treatment for managing pain and stiffness in Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: D
Rationale: Nonsteroidal Anti-inflammatory Drugs (NSAIDs) are the first-line pharmacologic treatment for pain and stiffness in Ankylosing Spondylitis. They are effective in reducing inflammation and improving symptoms in many patients. TNF-α inhibitors are typically reserved for patients who have an inadequate response to NSAIDs. Methotrexate is generally not effective for axial symptoms of AS. Oral corticosteroids are used for acute flares or specific extra-articular manifestations but not as a long-term first-line treatment due to side effects. Opioid analgesics are not recommended for chronic management due to risks of dependence and lack of anti-inflammatory effect.
Question 41
A 38-year-old female with Ankylosing Spondylitis has been managed with maximal dose NSAIDs and regular physical therapy for 6 months. Despite adherence to treatment, she continues to experience significant inflammatory back pain, morning stiffness, and functional impairment, as evidenced by a high Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) score. Her rheumatologist is considering escalating her treatment. Which of the following medications would be the most appropriate next step?
View Answer & Explanation
Correct Answer: C
Rationale: For patients with Ankylosing Spondylitis who have persistent high disease activity despite an adequate trial of NSAIDs, biologic agents, particularly TNF-α inhibitors (e.g., etanercept, adalimumab, infliximab), are the recommended next step. Sulfasalazine and hydroxychloroquine are generally ineffective for axial symptoms of AS. Oral prednisone is used for short-term flares but not as a long-term disease-modifying agent. Colchicine is used for gout.
Question 42
A 68-year-old male with a 40-year history of Ankylosing Spondylitis, characterized by a rigid, fused spine, presents to the emergency department after a low-energy fall from standing height. He complains of severe, localized back pain that is different from his usual chronic pain. Neurological examination is intact. Radiographs show a transverse fracture through the mid-thoracic spine. Given his underlying condition, what is the most critical concern regarding this type of fracture?
View Answer & Explanation
Correct Answer: C
Rationale: Spinal fractures in patients with Ankylosing Spondylitis, even from low-energy trauma, are highly unstable and carry a significant risk of neurological compromise. The fused, osteoporotic spine acts as a long lever arm, concentrating stress at the fracture site, often leading to a three-column injury. These fractures are often difficult to diagnose on plain radiographs and require CT or MRI. They are rarely managed non-operatively due to the inherent instability.
Question 43
A 50-year-old male with advanced Ankylosing Spondylitis sustains a C6-C7 fracture-dislocation after a motor vehicle accident. He presents with new-onset quadriparesis. Imaging confirms a highly unstable three-column injury. What is the most appropriate management strategy for this patient's spinal fracture?
View Answer & Explanation
Correct Answer: D
Rationale: Unstable spinal fractures in patients with Ankylosing Spondylitis, especially those with neurological deficits, require urgent surgical stabilization. The fused, osteoporotic spine is highly susceptible to unstable three-column injuries, and non-operative management carries a very high risk of further neurological deterioration and poor outcomes. Surgical fixation provides stability and allows for early mobilization. Steroids may be considered for acute spinal cord injury but do not address the instability.
Question 44
A 45-year-old male with long-standing Ankylosing Spondylitis presents with severe, fixed thoracolumbar kyphosis, preventing him from looking straight ahead (chin-on-chest deformity) and significantly impairing his quality of life. Medical management has failed to improve his spinal deformity. Which surgical procedure is most commonly performed to correct severe fixed kyphosis in patients with Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: For severe, fixed kyphosis in Ankylosing Spondylitis, vertebral column resection techniques, such as pedicle subtraction osteotomy (PSO) or Ponte osteotomy, are commonly performed. These procedures involve removing a wedge of bone from the vertebral body and posterior elements to achieve significant angular correction and restore sagittal balance. Laminectomy and discectomy are not designed for kyphosis correction. Spinal fusion alone would not correct the fixed deformity. Kyphoplasty is used for vertebral compression fractures, not for correcting severe fixed kyphosis.
Question 45
A 40-year-old male with Ankylosing Spondylitis presents with severe, bilateral hip pain and stiffness, significantly limiting his ambulation. Radiographs show advanced bilateral hip osteoarthritis with joint space narrowing, osteophytes, and subchondral sclerosis. He has failed conservative management, including NSAIDs and physical therapy. Which surgical intervention is most likely to provide significant pain relief and functional improvement for this patient?
View Answer & Explanation
Correct Answer: C
Rationale: Total hip arthroplasty (THA) is a highly effective surgical intervention for severe, end-stage hip osteoarthritis secondary to Ankylosing Spondylitis, providing significant pain relief and functional improvement. Hip arthroscopy is typically for milder conditions or labral tears. Core decompression is for avascular necrosis. Hip fusion would eliminate motion and is generally not preferred for bilateral disease. Femoral osteotomy is used for specific deformities but not end-stage arthritis.
Question 46
A 70-year-old male presents with chronic back stiffness and radiographs showing extensive flowing ossification along the anterior longitudinal ligament of the thoracic spine. He denies inflammatory back pain or morning stiffness. His sacroiliac joints appear normal. Which of the following conditions is the most important differential diagnosis to distinguish from Ankylosing Spondylitis in this patient?
View Answer & Explanation
Correct Answer: C
Rationale: Diffuse Idiopathic Skeletal Hyperostosis (DISH) is a crucial differential diagnosis for Ankylosing Spondylitis, especially in older patients, due to its characteristic flowing ossification along the spine. However, DISH typically spares the sacroiliac joints, involves the right side of the thoracic spine more often, and does not present with inflammatory back pain or elevated inflammatory markers. Ankylosing Spondylitis is characterized by sacroiliitis and thin, vertical syndesmophytes, often with inflammatory symptoms. Rheumatoid arthritis primarily affects peripheral joints. Psoriatic and reactive arthritis are spondyloarthropathies but have distinct clinical and radiographic features. Osteoarthritis is degenerative and does not involve ligamentous ossification in this manner.
Question 47
A 30-year-old male with suspected Ankylosing Spondylitis undergoes a physical examination to assess his spinal mobility. The physician marks a point 10 cm above and 5 cm below the L5 spinous process. The patient is then asked to maximally flex his lumbar spine. The distance between the two marks is measured again. Which specific physical examination test is being performed?
View Answer & Explanation
Correct Answer: C
Rationale: The described maneuver is the Schober test, which is used to assess lumbar spine flexion. A normal increase in distance between the two marks is typically 5 cm or more. In Ankylosing Spondylitis, reduced lumbar flexion due to spinal stiffness and fusion results in a smaller increase, indicating impaired mobility. The Faber test and Gaenslen test assess sacroiliac joint pain. The straight leg raise test assesses sciatic nerve irritation. The Trendelenburg test assesses hip abductor strength.
Question 48
A 28-year-old male with Ankylosing Spondylitis complains of chronic pain and tenderness at the insertion of his Achilles tendon and plantar fascia. Physical examination confirms localized tenderness and swelling at these sites. This inflammatory process at the insertion of tendons and ligaments into bone is a common feature of spondyloarthropathies. What is the medical term for this condition?
View Answer & Explanation
Correct Answer: C
Rationale: Enthesitis is the inflammation at the site where tendons, ligaments, or joint capsules insert into bone. It is a hallmark feature of Ankylosing Spondylitis and other spondyloarthropathies, commonly affecting the Achilles tendon, plantar fascia, and costochondral junctions. Bursitis is inflammation of a bursa. Tendinitis is inflammation of a tendon body. Synovitis is inflammation of the synovial membrane. Osteomyelitis is bone infection.
Question 49
A 32-year-old male presents with inflammatory back pain and stiffness. His physician orders a panel of laboratory tests. While some lab markers are often elevated in Ankylosing Spondylitis, which of the following is considered a non-specific marker of inflammation and may or may not be elevated in active disease, making it less reliable for diagnosis than clinical and imaging findings?
View Answer & Explanation
Correct Answer: B
Rationale: The Erythrocyte Sedimentation Rate (ESR) and C-reactive protein (CRP) are non-specific markers of inflammation. While they can be elevated in active Ankylosing Spondylitis, they are not consistently elevated in all patients, and their levels do not always correlate with disease activity. Therefore, they are less reliable for diagnosis than clinical features and imaging. HLA-B27 is a genetic marker, not an inflammatory marker, and while strongly associated, its presence alone is not diagnostic. Rheumatoid Factor and Anti-CCP antibodies are specific for rheumatoid arthritis.
Question 50
A 60-year-old male with long-standing, severe Ankylosing Spondylitis develops new-onset bilateral lower extremity weakness, numbness, and bowel/bladder dysfunction over several weeks. Physical examination reveals diminished sensation in a saddle distribution and reduced anal tone. Imaging of the lumbar spine shows dural ectasia and arachnoiditis. What is the most likely diagnosis for these new neurological symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: Cauda equina syndrome is a rare but recognized late complication of long-standing Ankylosing Spondylitis. It is thought to be caused by chronic arachnoiditis leading to dural ectasia and compression of the cauda equina nerve roots. The symptoms of bilateral lower extremity weakness, sensory deficits (especially saddle anesthesia), and bowel/bladder dysfunction are classic for cauda equina syndrome. While disc herniation or spinal stenosis can cause similar symptoms, the context of severe, long-standing AS with dural ectasia points strongly to AS-related cauda equina syndrome. Transverse myelitis and peripheral neuropathy have different clinical presentations and underlying pathologies.
Question 51
A 58-year-old male with advanced Ankylosing Spondylitis presents with new complaints of neck pain, occipital headaches, and progressive difficulty with fine motor tasks in his hands. He reports occasional Lhermitte's sign. On examination, he has hyperreflexia in the upper extremities and a positive Babinski sign. Which of the following complications of Ankylosing Spondylitis should be suspected?
View Answer & Explanation
Correct Answer: C
Rationale: Atlantoaxial subluxation (AAS) is a serious, albeit rare, complication of advanced Ankylosing Spondylitis due to inflammatory erosion and laxity of the transverse ligament and other supporting structures at the C1-C2 level. The symptoms of neck pain, occipital headaches, and myelopathy (fine motor difficulty, hyperreflexia, Babinski sign, Lhermitte's sign) are indicative of spinal cord compression at the craniocervical junction. While cervical disc herniation or spinal stenosis can cause myelopathy, AAS is a specific and critical concern in AS patients with these symptoms. Thoracic outlet syndrome and vertebral artery dissection have different presentations.
Question 52
A 30-year-old male with Ankylosing Spondylitis is being monitored for disease progression and treatment effectiveness. His rheumatologist regularly assesses his symptoms, physical examination findings, and laboratory markers. Which of the following is a commonly used patient-reported outcome measure specifically designed to assess disease activity in Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) is a validated, patient-reported questionnaire specifically designed to measure disease activity in Ankylosing Spondylitis. It assesses fatigue, spinal pain, peripheral joint pain/swelling, enthesitis, and morning stiffness. While VAS for pain is a general pain measure, and ODI is a general back pain disability index, BASDAI is specific to AS disease activity. WOMAC is for osteoarthritis, and ASA is for surgical risk assessment.
Question 53
A 27-year-old male with early Ankylosing Spondylitis undergoes follow-up radiographs of his lumbar spine. In addition to early sacroiliitis, the radiologist notes a subtle change in the shape of the vertebral bodies. Which of the following early vertebral body changes is characteristic of Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: Squaring of vertebral bodies is an early and characteristic radiographic finding in Ankylosing Spondylitis. It results from erosion of the anterior superior and inferior vertebral body corners (Romanus lesions) followed by reactive new bone formation, leading to a loss of the normal anterior concavity of the vertebral body. Vertebral body collapse is typically due to trauma or osteoporosis. Schmorl's nodes are disc herniations into the vertebral body. Hemivertebrae are congenital anomalies. Degenerative osteophytes are different in morphology and etiology.
Question 54
A 48-year-old male with advanced Ankylosing Spondylitis has radiographs demonstrating extensive spinal fusion. The ossification bridging the vertebral bodies is described as thin, vertical, and marginal, originating from the outer fibers of the annulus fibrosus. What is the specific term for these characteristic bony bridges seen in Ankylosing Spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: Syndesmophytes are the characteristic bony bridges seen in Ankylosing Spondylitis. They are typically thin, vertical, and marginal, arising from the outer fibers of the annulus fibrosus and eventually bridging adjacent vertebral bodies, leading to spinal fusion and the "bamboo spine" appearance. Oste
Question 54
A 28-year-old male presents with a 9-month history of insidious onset low back pain and stiffness, worse in the morning and improving with activity. He reports waking up in the second half of the night due to pain. Physical examination reveals limited lumbar spine flexion and tenderness over the sacroiliac joints. Plain radiographs of the lumbar spine are unremarkable, but sacroiliac joint films show subtle sclerosis. His C-reactive protein (CRP) is mildly elevated.
View Answer & Explanation
Correct Answer: C
Rationale: In a patient with inflammatory back pain suggestive of ankylosing spondylitis, MRI of the sacroiliac joints is the most sensitive imaging modality for detecting early inflammatory changes (bone marrow edema) that may not be visible on plain radiographs. This allows for earlier diagnosis and initiation of appropriate treatment. Lumbar spine MRI would be less specific for early AS, and plain radiographs are often normal in early disease. HLA-B27 is a genetic marker associated with AS but is not diagnostic on its own, as many HLA-B27 positive individuals do not develop AS. EMG is used for nerve root compression, not inflammatory arthritis.
Question 54
A 35-year-old male with a 10-year history of ankylosing spondylitis presents to the emergency department with acute onset of unilateral eye pain, redness, and photophobia. He denies any trauma or recent infections. Ophthalmic examination reveals ciliary flush and constricted pupil.
View Answer & Explanation
Correct Answer: D
Rationale: Acute anterior uveitis (iritis) is the most common extra-articular manifestation of ankylosing spondylitis, affecting up to 40% of patients. Symptoms typically include acute onset of unilateral eye pain, redness (ciliary flush), photophobia, and blurred vision. It requires prompt treatment with topical corticosteroids to prevent complications. Conjunctivitis is usually bilateral and lacks severe pain and photophobia. Glaucoma, cataract, and retinal detachment are less common or present differently.
Question 54
A 55-year-old male with long-standing, poorly controlled ankylosing spondylitis undergoes routine follow-up radiographs of his spine. The lateral view of the lumbar spine demonstrates ossification of the outer fibers of the annulus fibrosus, bridging adjacent vertebral bodies. This finding is characteristic of the disease progression.
View Answer & Explanation
Correct Answer: C
Rationale: Syndesmophytes are characteristic radiographic findings in ankylosing spondylitis, representing ossification of the outer annulus fibrosus and longitudinal ligaments, leading to bony bridges between vertebral bodies. These typically start at the thoracolumbar and cervicothoracic junctions and progress upwards and downwards. This is distinct from degenerative osteophytes, which are typically larger, more irregular, and arise from the vertebral endplates. Disc space narrowing is a degenerative change, and spondylolisthesis is vertebral slippage. Schmorl's nodes are disc herniations into the vertebral body.
Question 54
A 30-year-old male is being evaluated for suspected ankylosing spondylitis. During the physical examination, the physician marks two points on the patient's lower back, 10 cm apart, while the patient is standing erect. The patient is then asked to maximally flex his spine. The distance between the two marks is re-measured. This specific test is performed to assess lumbar spine mobility.
View Answer & Explanation
Correct Answer: C
Rationale: The Schober test is a specific and widely used clinical measure to assess lumbar spine flexion. A normal increase in distance between the two marks (10 cm apart, with an additional 5 cm mark above) should be at least 5 cm (total 15 cm) upon maximal flexion. In ankylosing spondylitis, reduced lumbar flexion is an early and common finding, making the Schober test a valuable diagnostic and monitoring tool. The other tests listed assess different aspects: Straight Leg Raise for sciatica, FABER and Gaenslen for sacroiliac joint pain, and Trendelenburg for hip abductor weakness.
Question 54
A 25-year-old male is diagnosed with ankylosing spondylitis based on clinical symptoms and radiographic evidence of sacroiliitis. His rheumatologist discusses the genetic predisposition for the disease, noting a strong association with a particular human leukocyte antigen (HLA) allele.
View Answer & Explanation
Correct Answer: B
Rationale: HLA-B27 is the strongest known genetic risk factor for ankylosing spondylitis, present in 90-95% of Caucasian patients with the disease. While its presence is not diagnostic (as many HLA-B27 positive individuals do not develop AS), it significantly increases susceptibility and is often used as a supportive diagnostic criterion. The other HLA alleles are associated with different autoimmune conditions or have a weaker association with AS.
Question 54
A 32-year-old female is newly diagnosed with ankylosing spondylitis. She experiences mild to moderate inflammatory back pain and morning stiffness, which partially improves with over-the-counter pain relievers. Her physical examination shows mild reduction in spinal mobility, and her inflammatory markers are slightly elevated. There is no evidence of peripheral arthritis or extra-articular manifestations.
View Answer & Explanation
Correct Answer: C
Rationale: Non-steroidal anti-inflammatory drugs (NSAIDs) are considered the first-line pharmacological treatment for patients with active ankylosing spondylitis, especially those with axial symptoms. They effectively reduce pain and stiffness and can slow radiographic progression in some patients. Methotrexate and sulfasalazine are typically used for peripheral arthritis in spondyloarthropathies but are less effective for axial disease. TNF-alpha inhibitors are biologics reserved for patients who have failed adequate trials of NSAIDs. Oral prednisone is generally not recommended for long-term management due to side effects, though it may be used for acute flares or specific extra-articular manifestations.
Question 54
A 68-year-old male with a 40-year history of severe ankylosing spondylitis presents for follow-up. He has significant kyphosis and severely restricted spinal mobility. Radiographs of his entire spine demonstrate extensive fusion of the vertebral bodies due to widespread syndesmophyte formation, giving a characteristic appearance.
View Answer & Explanation
Correct Answer: C
Rationale: The "bamboo spine" appearance is a classic radiographic finding in advanced ankylosing spondylitis, resulting from diffuse ossification of the annulus fibrosus and anterior longitudinal ligament, leading to complete fusion of the vertebral bodies. Romanus lesions (erosions at vertebral corners) and Andersson lesions (inflammatory lesions at disc-vertebral body junctions) are earlier or less common findings. A "carrot stick fracture" refers to a specific type of spinal fracture in a rigid AS spine, and "pugilistic spine" is not a recognized term for AS.
Question 54
An 80-year-old male with severe, long-standing ankylosing spondylitis, characterized by a fused, rigid spine, sustains a low-energy fall. He immediately experiences severe, localized back pain and new neurological deficits, including lower extremity weakness and numbness. Given his underlying condition, what is the most concerning complication?
View Answer & Explanation
Correct Answer: E
Rationale: Patients with long-standing ankylosing spondylitis develop a rigid, osteoporotic spine that acts as a single, long bone. Even minor trauma can lead to unstable fractures, often through a fused segment (sometimes called a "carrot stick fracture"). These fractures are highly unstable and carry a significant risk of neurological injury, including spinal cord injury or cauda equina syndrome. While compression fractures can occur, the concern for an unstable fracture through a fused segment with neurological compromise is paramount. Disc herniation is less likely in a fused spine. Atlantoaxial subluxation is a known complication but typically presents differently and is less likely to be acutely triggered by a low-energy fall in the lumbar region. Spinal stenosis exacerbation is also less likely to cause acute, severe neurological deficits from a fall.
Question 54
A 40-year-old male with ankylosing spondylitis has failed to achieve adequate symptom control despite optimal use of NSAIDs and physical therapy. His rheumatologist decides to initiate treatment with a biologic agent. Which class of biologic medications is most commonly used as a second-line treatment for axial ankylosing spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: TNF-alpha inhibitors (e.g., adalimumab, etanercept, infliximab) are the most established and widely used class of biologic agents for ankylosing spondylitis when NSAIDs fail. They have demonstrated significant efficacy in reducing disease activity, improving function, and slowing radiographic progression. While other biologics like IL-17 inhibitors (e.g., secukinumab, ixekizumab) are also effective and approved for AS, TNF-alpha inhibitors remain the most common and often first-choice biologic class. IL-6 inhibitors, B-cell inhibitors, JAK inhibitors, and T-cell costimulation blockers are primarily used for other rheumatic conditions like rheumatoid arthritis, though some JAK inhibitors are approved for AS.
Question 54
A 38-year-old male presents with chronic inflammatory back pain, morning stiffness, and fatigue. He also reports a history of recurrent skin rashes, particularly on his elbows and knees, which are scaly and red. Physical examination reveals mild sacroiliac joint tenderness and some nail pitting. Radiographs show early sacroiliitis. His HLA-B27 test is positive.
View Answer & Explanation
Correct Answer: C
Rationale: The patient's presentation with inflammatory back pain, sacroiliitis, and a history of psoriatic skin lesions (rashes on elbows/knees, nail pitting) is highly suggestive of Psoriatic Arthritis (PsA). PsA is a seronegative spondyloarthropathy that can affect the axial skeleton, mimicking ankylosing spondylitis, and is also associated with HLA-B27. While Reactive Arthritis can also cause sacroiliitis and skin lesions (keratoderma blennorrhagicum), the description of the rash is more consistent with psoriasis. Rheumatoid arthritis typically affects small joints symmetrically and is seropositive. Osteoarthritis is degenerative, and DISH involves ossification of ligaments but typically spares the SI joints and presents in older individuals without inflammatory markers or skin manifestations.
Question 54
A 60-year-old male with a 30-year history of severe ankylosing spondylitis presents with progressive shortness of breath and a chronic cough. Pulmonary function tests show a restrictive pattern. A chest CT scan reveals fibrotic changes predominantly in the upper lobes of his lungs.
View Answer & Explanation
Correct Answer: C
Rationale: Upper lobe pulmonary fibrosis (also known as apical fibrobullous disease) is a recognized, albeit uncommon, pulmonary complication of long-standing ankylosing spondylitis. It typically presents with progressive dyspnea and cough, and imaging shows fibrotic changes in the upper lung fields. The restrictive pattern on PFTs can also be exacerbated by reduced chest wall expansion due to costovertebral joint involvement in AS. Asthma and COPD are common but not specific to AS. Pleural effusion is not a characteristic pulmonary manifestation of AS. Pulmonary hypertension can be a secondary complication but is not the primary lung pathology described.
Question 54
A 50-year-old male with a 20-year history of ankylosing spondylitis reports new onset of exertional dyspnea and palpitations. On physical examination, a diastolic murmur is noted at the right sternal border. Echocardiography reveals dilation of the aortic root and mild aortic regurgitation.
View Answer & Explanation
Correct Answer: C
Rationale: Aortic insufficiency (or aortic regurgitation) is the most common cardiac manifestation of ankylosing spondylitis, particularly in long-standing disease. It results from inflammation and dilation of the aortic root and valve leaflets. The diastolic murmur at the right sternal border and echocardiographic findings are classic for aortic insufficiency. Pericarditis can occur but is less common. Mitral valve prolapse, myocarditis, and atrial fibrillation are not specifically associated with AS as primary cardiac complications.
Question 54
A 65-year-old male with severe, advanced ankylosing spondylitis has developed a fixed, severe thoracolumbar kyphosis, preventing him from looking straight ahead and significantly impairing his daily activities. He experiences difficulty with balance and eating. Non-surgical management has failed to improve his posture or function. Which surgical procedure is most appropriate to address his deformity?
View Answer & Explanation
Correct Answer: D
Rationale: For severe, fixed kyphosis in ankylosing spondylitis that significantly impairs function and quality of life, a spinal osteotomy (e.g., pedicle subtraction osteotomy) is the most effective surgical option. This procedure involves removing a wedge of bone from the vertebral column to correct the sagittal imbalance and restore a more upright posture, allowing the patient to look forward. Laminectomy and discectomy are typically performed for spinal decompression. Spinal fusion is often part of the osteotomy procedure but is not the primary corrective maneuver for severe kyphosis. Vertebroplasty is used for vertebral compression fractures, not for correcting fixed kyphotic deformities.
Question 54
A 22-year-old male presents with a 6-month history of inflammatory back pain. His physical exam is notable for mild sacroiliac joint tenderness. Initial plain radiographs of the lumbar spine are normal. To confirm the diagnosis of ankylosing spondylitis, the physician orders plain radiographs of the sacroiliac joints. What is the earliest characteristic radiographic change expected on these films?
View Answer & Explanation
Correct Answer: C
Rationale: Sacroiliitis (inflammation of the sacroiliac joints) is the hallmark and earliest radiographic change seen in ankylosing spondylitis. It typically begins with blurring of the subchondral bone, followed by erosions, sclerosis, and eventually fusion of the sacroiliac joints. This is often bilateral and symmetric. Syndesmophytes and "bamboo spine" are later manifestations of axial disease. Disc space narrowing and facet joint fusion are also later or less specific findings.
Question 54
A 70-year-old male with a 45-year history of ankylosing spondylitis, characterized by a fused lumbar spine, presents with new onset of bilateral lower extremity weakness, saddle anesthesia, and bowel and bladder incontinence. Magnetic resonance imaging (MRI) of the lumbar spine reveals dural ectasia and arachnoiditis in the lumbosacral region.
View Answer & Explanation
Correct Answer: D
Rationale: Cauda equina syndrome is a rare but serious neurological complication of long-standing ankylosing spondylitis. It is thought to result from chronic inflammation leading to dural ectasia, arachnoiditis, and compression of the nerve roots in the lumbosacral region. The classic symptoms include bilateral lower extremity weakness, saddle anesthesia, and bowel/bladder dysfunction. Spinal cord compression and myelopathy are less likely in the lumbar region. Lumbar radiculopathy would typically be unilateral or affect a single nerve root distribution. Peripheral neuropathy is a more generalized nerve disorder.
Question 54
A 45-year-old male with ankylosing spondylitis is well-controlled on a TNF-alpha inhibitor and NSAIDs. He asks his physician about additional measures he can take to manage his condition and maintain spinal mobility. Which non-pharmacological intervention is considered most crucial for patients with ankylosing spondylitis?
View Answer & Explanation
Correct Answer: D
Rationale: A daily, structured exercise program, including stretching, strengthening, and aerobic exercises, is paramount in the management of ankylosing spondylitis. It helps maintain spinal mobility, reduce stiffness, improve posture, and enhance overall physical function. Bed rest can worsen stiffness and deconditioning. While heat therapy can provide symptomatic relief, it's not a primary management strategy. Spinal bracing is generally discouraged as it can lead to muscle atrophy and further stiffness. Elimination diets lack strong evidence for widespread efficacy in AS.
Question 54
A 30-year-old female with ankylosing spondylitis is on a stable treatment regimen. Her rheumatologist wants to regularly assess her disease activity and treatment response. While inflammatory markers (ESR, CRP) are useful, which patient-reported outcome measure is specifically designed and widely used to monitor disease activity in ankylosing spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) is a validated, patient-reported questionnaire specifically designed to assess disease activity in ankylosing spondylitis. It includes questions about fatigue, spinal pain, peripheral joint pain/swelling, localized tenderness, and morning stiffness. While VAS for pain is a component, BASDAI provides a comprehensive measure of disease activity. HAQ is a general functional assessment. DAS28 is used for rheumatoid arthritis. WOMAC is for osteoarthritis.
Question 54
A 42-year-old male with ankylosing spondylitis complains of pain and tenderness at the insertion of his Achilles tendon into the calcaneus, as well as pain at the plantar fascia insertion. Physical examination confirms localized tenderness at these sites without significant swelling of the adjacent joints. This inflammatory process at tendon and ligament insertion sites is a characteristic feature of spondyloarthropathies.
Question 55
A 28-year-old male presents with a 9-month history of insidious onset low back pain and stiffness, worse in the morning and improving with activity. He reports waking up in the second half of the night due to pain. Physical examination reveals limited lumbar spine flexion and tenderness over the sacroiliac joints. Plain radiographs of the lumbar spine are unremarkable, but sacroiliac joint films show subtle sclerosis. His C-reactive protein (CRP) is mildly elevated.
View Answer & Explanation
Correct Answer: C
Rationale: In a patient with inflammatory back pain suggestive of ankylosing spondylitis, MRI of the sacroiliac joints is the most sensitive imaging modality for detecting early inflammatory changes (bone marrow edema) that may not be visible on plain radiographs. This allows for earlier diagnosis and initiation of appropriate treatment. Lumbar spine MRI would be less specific for early AS, and plain radiographs are often normal in early disease. HLA-B27 is a genetic marker associated with AS but is not diagnostic on its own, as many HLA-B27 positive individuals do not develop AS. EMG is used for nerve root compression, not inflammatory arthritis.
Question 56
A 35-year-old male with a 10-year history of ankylosing spondylitis presents to the emergency department with acute onset of unilateral eye pain, redness, and photophobia. He denies any trauma or recent infections. Ophthalmic examination reveals ciliary flush and constricted pupil.
View Answer & Explanation
Correct Answer: D
Rationale: Acute anterior uveitis (iritis) is the most common extra-articular manifestation of ankylosing spondylitis, affecting up to 40% of patients. Symptoms typically include acute onset of unilateral eye pain, redness (ciliary flush), photophobia, and blurred vision. It requires prompt treatment with topical corticosteroids to prevent complications. Conjunctivitis is usually bilateral and lacks severe pain and photophobia. Glaucoma, cataract, and retinal detachment are less common or present differently.
Question 57
A 55-year-old male with long-standing, poorly controlled ankylosing spondylitis undergoes routine follow-up radiographs of his spine. The lateral view of the lumbar spine demonstrates ossification of the outer fibers of the annulus fibrosus, bridging adjacent vertebral bodies. This finding is characteristic of the disease progression.
View Answer & Explanation
Correct Answer: C
Rationale: Syndesmophytes are characteristic radiographic findings in ankylosing spondylitis, representing ossification of the outer annulus fibrosus and longitudinal ligaments, leading to bony bridges between vertebral bodies. These typically start at the thoracolumbar and cervicothoracic junctions and progress upwards and downwards. This is distinct from degenerative osteophytes, which are typically larger, more irregular, and arise from the vertebral endplates. Disc space narrowing is a degenerative change, and spondylolisthesis is vertebral slippage. Schmorl's nodes are disc herniations into the vertebral body.
Question 58
A 30-year-old male is being evaluated for suspected ankylosing spondylitis. During the physical examination, the physician marks two points on the patient's lower back, 10 cm apart, while the patient is standing erect. The patient is then asked to maximally flex his spine. The distance between the two marks is re-measured. This specific test is performed to assess lumbar spine mobility.
View Answer & Explanation
Correct Answer: C
Rationale: The Schober test is a specific and widely used clinical measure to assess lumbar spine flexion. A normal increase in distance between the two marks (10 cm apart, with an additional 5 cm mark above) should be at least 5 cm (total 15 cm) upon maximal flexion. In ankylosing spondylitis, reduced lumbar flexion is an early and common finding, making the Schober test a valuable diagnostic and monitoring tool. The other tests listed assess different aspects: Straight Leg Raise for sciatica, FABER and Gaenslen for sacroiliac joint pain, and Trendelenburg for hip abductor weakness.
Question 59
A 25-year-old male is diagnosed with ankylosing spondylitis based on clinical symptoms and radiographic evidence of sacroiliitis. His rheumatologist discusses the genetic predisposition for the disease, noting a strong association with a particular human leukocyte antigen (HLA) allele.
View Answer & Explanation
Correct Answer: B
Rationale: HLA-B27 is the strongest known genetic risk factor for ankylosing spondylitis, present in 90-95% of Caucasian patients with the disease. While its presence is not diagnostic (as many HLA-B27 positive individuals do not develop AS), it significantly increases susceptibility and is often used as a supportive diagnostic criterion. The other HLA alleles are associated with different autoimmune conditions or have a weaker association with AS.
Question 60
A 32-year-old female is newly diagnosed with ankylosing spondylitis. She experiences mild to moderate inflammatory back pain and morning stiffness, which partially improves with over-the-counter pain relievers. Her physical examination shows mild reduction in spinal mobility, and her inflammatory markers are slightly elevated. There is no evidence of peripheral arthritis or extra-articular manifestations.
View Answer & Explanation
Correct Answer: C
Rationale: Non-steroidal anti-inflammatory drugs (NSAIDs) are considered the first-line pharmacological treatment for patients with active ankylosing spondylitis, especially those with axial symptoms. They effectively reduce pain and stiffness and can slow radiographic progression in some patients. Methotrexate and sulfasalazine are typically used for peripheral arthritis in spondyloarthropathies but are less effective for axial disease. TNF-alpha inhibitors are biologics reserved for patients who have failed adequate trials of NSAIDs. Oral prednisone is generally not recommended for long-term management due to side effects, though it may be used for acute flares or specific extra-articular manifestations.
Question 61
A 68-year-old male with a 40-year history of severe ankylosing spondylitis presents for follow-up. He has significant kyphosis and severely restricted spinal mobility. Radiographs of his entire spine demonstrate extensive fusion of the vertebral bodies due to widespread syndesmophyte formation, giving a characteristic appearance.
View Answer & Explanation
Correct Answer: C
Rationale: The "bamboo spine" appearance is a classic radiographic finding in advanced ankylosing spondylitis, resulting from diffuse ossification of the annulus fibrosus and anterior longitudinal ligament, leading to complete fusion of the vertebral bodies. Romanus lesions (erosions at vertebral corners) and Andersson lesions (inflammatory lesions at disc-vertebral body junctions) are earlier or less common findings. A "carrot stick fracture" refers to a specific type of spinal fracture in a rigid AS spine, and "pugilistic spine" is not a recognized term for AS.
Question 62
An 80-year-old male with severe, long-standing ankylosing spondylitis, characterized by a fused, rigid spine, sustains a low-energy fall. He immediately experiences severe, localized back pain and new neurological deficits, including lower extremity weakness and numbness. Given his underlying condition, what is the most concerning complication?
View Answer & Explanation
Correct Answer: E
Rationale: Patients with long-standing ankylosing spondylitis develop a rigid, osteoporotic spine that acts as a single, long bone. Even minor trauma can lead to unstable fractures, often through a fused segment (sometimes called a "carrot stick fracture"). These fractures are highly unstable and carry a significant risk of neurological injury, including spinal cord injury or cauda equina syndrome. While compression fractures can occur, the concern for an unstable fracture through a fused segment with neurological compromise is paramount. Disc herniation is less likely in a fused spine. Atlantoaxial subluxation is a known complication but typically presents differently and is less likely to be acutely triggered by a low-energy fall in the lumbar region. Spinal stenosis exacerbation is also less likely to cause acute, severe neurological deficits from a fall.
Question 63
A 40-year-old male with ankylosing spondylitis has failed to achieve adequate symptom control despite optimal use of NSAIDs and physical therapy. His rheumatologist decides to initiate treatment with a biologic agent. Which class of biologic medications is most commonly used as a second-line treatment for axial ankylosing spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: TNF-alpha inhibitors (e.g., adalimumab, etanercept, infliximab) are the most established and widely used class of biologic agents for ankylosing spondylitis when NSAIDs fail. They have demonstrated significant efficacy in reducing disease activity, improving function, and slowing radiographic progression. While other biologics like IL-17 inhibitors (e.g., secukinumab, ixekizumab) are also effective and approved for AS, TNF-alpha inhibitors remain the most common and often first-choice biologic class. IL-6 inhibitors, B-cell inhibitors, JAK inhibitors, and T-cell costimulation blockers are primarily used for other rheumatic conditions like rheumatoid arthritis, though some JAK inhibitors are approved for AS.
Question 64
A 38-year-old male presents with chronic inflammatory back pain, morning stiffness, and fatigue. He also reports a history of recurrent skin rashes, particularly on his elbows and knees, which are scaly and red. Physical examination reveals mild sacroiliac joint tenderness and some nail pitting. Radiographs show early sacroiliitis. His HLA-B27 test is positive.
View Answer & Explanation
Correct Answer: C
Rationale: The patient's presentation with inflammatory back pain, sacroiliitis, and a history of psoriatic skin lesions (rashes on elbows/knees, nail pitting) is highly suggestive of Psoriatic Arthritis (PsA). PsA is a seronegative spondyloarthropathy that can affect the axial skeleton, mimicking ankylosing spondylitis, and is also associated with HLA-B27. While Reactive Arthritis can also cause sacroiliitis and skin lesions (keratoderma blennorrhagicum), the description of the rash is more consistent with psoriasis. Rheumatoid arthritis typically affects small joints symmetrically and is seropositive. Osteoarthritis is degenerative, and DISH involves ossification of ligaments but typically spares the SI joints and presents in older individuals without inflammatory markers or skin manifestations.
Question 65
A 60-year-old male with a 30-year history of severe ankylosing spondylitis presents with progressive shortness of breath and a chronic cough. Pulmonary function tests show a restrictive pattern. A chest CT scan reveals fibrotic changes predominantly in the upper lobes of his lungs.
View Answer & Explanation
Correct Answer: C
Rationale: Upper lobe pulmonary fibrosis (also known as apical fibrobullous disease) is a recognized, albeit uncommon, pulmonary complication of long-standing ankylosing spondylitis. It typically presents with progressive dyspnea and cough, and imaging shows fibrotic changes in the upper lung fields. The restrictive pattern on PFTs can also be exacerbated by reduced chest wall expansion due to costovertebral joint involvement in AS. Asthma and COPD are common but not specific to AS. Pleural effusion is not a characteristic pulmonary manifestation of AS. Pulmonary hypertension can be a secondary complication but is not the primary lung pathology described.
Question 66
A 50-year-old male with a 20-year history of ankylosing spondylitis reports new onset of exertional dyspnea and palpitations. On physical examination, a diastolic murmur is noted at the right sternal border. Echocardiography reveals dilation of the aortic root and mild aortic regurgitation.
View Answer & Explanation
Correct Answer: C
Rationale: Aortic insufficiency (or aortic regurgitation) is the most common cardiac manifestation of ankylosing spondylitis, particularly in long-standing disease. It results from inflammation and dilation of the aortic root and valve leaflets. The diastolic murmur at the right sternal border and echocardiographic findings are classic for aortic insufficiency. Pericarditis can occur but is less common. Mitral valve prolapse, myocarditis, and atrial fibrillation are not specifically associated with AS as primary cardiac complications.
Question 67
A 65-year-old male with severe, advanced ankylosing spondylitis has developed a fixed, severe thoracolumbar kyphosis, preventing him from looking straight ahead and significantly impairing his daily activities. He experiences difficulty with balance and eating. Non-surgical management has failed to improve his posture or function. Which surgical procedure is most appropriate to address his deformity?
View Answer & Explanation
Correct Answer: D
Rationale: For severe, fixed kyphosis in ankylosing spondylitis that significantly impairs function and quality of life, a spinal osteotomy (e.g., pedicle subtraction osteotomy) is the most effective surgical option. This procedure involves removing a wedge of bone from the vertebral column to correct the sagittal imbalance and restore a more upright posture, allowing the patient to look forward. Laminectomy and discectomy are typically performed for spinal decompression. Spinal fusion is often part of the osteotomy procedure but is not the primary corrective maneuver for severe kyphosis. Vertebroplasty is used for vertebral compression fractures, not for correcting fixed kyphotic deformities.
Question 68
A 22-year-old male presents with a 6-month history of inflammatory back pain. His physical exam is notable for mild sacroiliac joint tenderness. Initial plain radiographs of the lumbar spine are normal. To confirm the diagnosis of ankylosing spondylitis, the physician orders plain radiographs of the sacroiliac joints. What is the earliest characteristic radiographic change expected on these films?
View Answer & Explanation
Correct Answer: C
Rationale: Sacroiliitis (inflammation of the sacroiliac joints) is the hallmark and earliest radiographic change seen in ankylosing spondylitis. It typically begins with blurring of the subchondral bone, followed by erosions, sclerosis, and eventually fusion of the sacroiliac joints. This is often bilateral and symmetric. Syndesmophytes and "bamboo spine" are later manifestations of axial disease. Disc space narrowing and facet joint fusion are also later or less specific findings.
Question 69
A 70-year-old male with a 45-year history of ankylosing spondylitis, characterized by a fused lumbar spine, presents with new onset of bilateral lower extremity weakness, saddle anesthesia, and bowel and bladder incontinence. Magnetic resonance imaging (MRI) of the lumbar spine reveals dural ectasia and arachnoiditis in the lumbosacral region.
View Answer & Explanation
Correct Answer: D
Rationale: Cauda equina syndrome is a rare but serious neurological complication of long-standing ankylosing spondylitis. It is thought to result from chronic inflammation leading to dural ectasia, arachnoiditis, and compression of the nerve roots in the lumbosacral region. The classic symptoms include bilateral lower extremity weakness, saddle anesthesia, and bowel/bladder dysfunction. Spinal cord compression and myelopathy are less likely in the lumbar region. Lumbar radiculopathy would typically be unilateral or affect a single nerve root distribution. Peripheral neuropathy is a more generalized nerve disorder.
Question 70
A 45-year-old male with ankylosing spondylitis is well-controlled on a TNF-alpha inhibitor and NSAIDs. He asks his physician about additional measures he can take to manage his condition and maintain spinal mobility. Which non-pharmacological intervention is considered most crucial for patients with ankylosing spondylitis?
View Answer & Explanation
Correct Answer: D
Rationale: A daily, structured exercise program, including stretching, strengthening, and aerobic exercises, is paramount in the management of ankylosing spondylitis. It helps maintain spinal mobility, reduce stiffness, improve posture, and enhance overall physical function. Bed rest can worsen stiffness and deconditioning. While heat therapy can provide symptomatic relief, it's not a primary management strategy. Spinal bracing is generally discouraged as it can lead to muscle atrophy and further stiffness. Elimination diets lack strong evidence for widespread efficacy in AS.
Question 71
A 30-year-old female with ankylosing spondylitis is on a stable treatment regimen. Her rheumatologist wants to regularly assess her disease activity and treatment response. While inflammatory markers (ESR, CRP) are useful, which patient-reported outcome measure is specifically designed and widely used to monitor disease activity in ankylosing spondylitis?
View Answer & Explanation
Correct Answer: C
Rationale: The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) is a validated, patient-reported questionnaire specifically designed to assess disease activity in ankylosing spondylitis. It includes questions about fatigue, spinal pain, peripheral joint pain/swelling, localized tenderness, and morning stiffness. While VAS for pain is a component, BASDAI provides a comprehensive measure of disease activity. HAQ is a general functional assessment. DAS28 is used for rheumatoid arthritis. WOMAC is for osteoarthritis.
Question 72
A 12-year-old boy presents with a 6-month history of dull, aching pain in his right anterior tibia. Physical examination reveals mild tenderness over the mid-diaphysis. Radiographs show an eccentric, lytic lesion with a sclerotic rim in the anterior cortex of the tibia, associated with cortical thickening and bowing. There is no periosteal reaction or soft tissue mass.
View Answer & Explanation
Correct Answer: B
Rationale: Osteofibrous dysplasia (OFD) is a benign fibro-osseous lesion almost exclusively found in the tibia (and rarely fibula) of young children, typically under 10 years old. It presents as an eccentric, lytic lesion with cortical thickening and bowing, often with a sclerotic rim. It is histologically similar to fibrous dysplasia but contains osteoblast-lined woven bone trabeculae within a fibrous stroma. Fibrous dysplasia can occur in the tibia but is less common to present with bowing and cortical thickening in
Question 72
A 14-year-old male presents with a 6-month history of dull aching pain in his right proximal femur. Physical examination reveals mild tenderness over the greater trochanter. Radiographs show an expansile, lytic lesion in the metaphysis of the proximal femur with a characteristic "ground-glass" matrix and an intact cortex. There are no other skeletal lesions identified.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of a lytic, expansile lesion with a "ground-glass" matrix in the metaphysis of a long bone in an adolescent, without other systemic findings, is classic for monostotic fibrous dysplasia. Enchondromas typically have a chondroid matrix (rings and arcs calcification) and are often asymptomatic. Aneurysmal bone cysts are expansile and lytic but typically multiloculated and fluid-filled. Non-ossifying fibromas are usually cortically based, eccentric, and have a sclerotic rim. Low-grade chondrosarcomas are less common in this age group and would typically show more aggressive features or chondroid matrix calcifications.
Question 72
A 7-year-old girl is evaluated for multiple bone lesions, café-au-lait spots with irregular "coast of Maine" borders, and a history of vaginal bleeding and breast development since age 5. Radiographs demonstrate multiple lytic, expansile lesions in the long bones and pelvis with a "ground-glass" appearance. Laboratory tests confirm elevated estrogen levels.
View Answer & Explanation
Correct Answer: C
Rationale: The classic triad of polyostotic fibrous dysplasia, café-au-lait skin pigmentation, and precocious puberty (due to endocrine hyperfunction) is diagnostic of McCune-Albright syndrome. Ollier disease and Maffucci syndrome involve multiple enchondromas, not fibrous dysplasia. Neurofibromatosis type 1 can have café-au-lait spots but typically presents with neurofibromas and different skeletal manifestations (e.g., pseudarthrosis, scoliosis). Paget's disease is a disorder of bone remodeling, typically affecting older adults, and does not present with precocious puberty or café-au-lait spots.
Question 72
A 55-year-old man with a long-standing history of polyostotic fibrous dysplasia presents with new onset of severe, unremitting pain in his right proximal humerus, where he has a known fibrous dysplasia lesion. Over the past 3 months, he has noted rapid enlargement of the area. Radiographs show cortical destruction, soft tissue mass, and a more aggressive lytic pattern within the previously stable fibrous dysplasia lesion. Biopsy reveals malignant cells.
View Answer & Explanation
Correct Answer: C
Rationale: Malignant transformation of fibrous dysplasia is rare but a recognized complication, particularly in polyostotic forms or those treated with radiation. The most common malignant transformation is osteosarcoma, followed by chondrosarcoma and fibrosarcoma. The presentation of rapid growth, new pain, and aggressive radiographic features in a pre-existing fibrous dysplasia lesion is highly suspicious for malignant degeneration. Ewing sarcoma is typically a tumor of childhood and adolescence, and malignant fibrous histiocytoma is a less common transformation.
Question 72
A 6-year-old boy presents with progressive bowing of his left leg and shortening of his left arm. Physical examination reveals multiple palpable bony masses in the metaphyses of the long bones of the left upper and lower extremities. Radiographs show multiple radiolucent lesions with speckled calcifications, consistent with enchondromas, predominantly affecting one side of the body. There are no associated soft tissue vascular lesions.
View Answer & Explanation
Correct Answer: C
Rationale: The presence of multiple enchondromas, often unilateral or asymmetric, leading to limb deformity and shortening, without associated soft tissue hemangiomas, is characteristic of Ollier disease (enchondromatosis). Maffucci syndrome is similar but includes soft tissue hemangiomas. Multiple hereditary exostoses involve osteochondromas, not enchondromas. Dysplasia epiphysealis hemimelica is a localized epiphyseal osteochondroma. Fibrous dysplasia has a different radiographic appearance ("ground-glass").
Question 72
A 10-year-old girl presents with multiple firm, palpable masses in her hands and feet, causing deformity and pain. She also has several bluish, compressible soft tissue lesions on her extremities. Radiographs reveal multiple enchondromas in the phalanges and metacarpals, as well as in the long bones. MRI confirms the presence of multiple soft tissue hemangiomas.
View Answer & Explanation
Correct Answer: C
Rationale: Maffucci syndrome is characterized by the combination of multiple enchondromas and soft tissue hemangiomas. Ollier disease involves multiple enchondromas but lacks the hemangiomas. Klippel-Trenaunay syndrome involves capillary malformations, venous malformations, lymphatic malformations, and limb overgrowth, but not typically enchondromas. Proteus syndrome is a complex overgrowth syndrome with various manifestations, but not specifically enchondromas and hemangiomas as the primary defining features. Sturge-Weber syndrome involves facial port-wine stain, leptomeningeal angiomatosis, and ocular involvement.
Question 72
A 45-year-old man with a known history of Ollier disease presents with increasing pain and swelling in his left thigh over the past 4 months. Radiographs show enlargement of a previously stable enchondroma in the distal femur, with new cortical erosion and periosteal reaction. A biopsy is performed, confirming a low-grade chondrosarcoma.
View Answer & Explanation
Correct Answer: C
Rationale: Patients with Ollier disease have a significantly increased risk of malignant transformation of their enchondromas into chondrosarcomas. The reported risk ranges from 25% to 50%, with some studies suggesting even higher rates, especially in Maffucci syndrome. This risk is a critical consideration in the long-term management and monitoring of these patients.
Question 72
A 9-year-old boy is brought to the clinic by his parents due to multiple hard, bony lumps around his knees, shoulders, and wrists. He reports occasional pain and limited range of motion in his right elbow. His father also has similar bony growths. Physical examination reveals multiple exostoses arising from the metaphyses of long bones. Radiographs confirm multiple osteochondromas.
View Answer & Explanation
Correct Answer: D
Rationale: The presence of multiple osteochondromas (exostoses) with an autosomal dominant inheritance pattern (father also affected) is characteristic of multiple hereditary exostoses (MHE), also known as hereditary multiple osteochondromas. Solitary osteochondroma is a single lesion. Ollier disease involves multiple enchondromas. Fibrous dysplasia has a different radiographic appearance. Dysplasia epiphysealis hemimelica is a localized epiphyseal osteochondroma-like lesion, typically unilateral and affecting a single joint.
Question 72
An 11-year-old girl with multiple hereditary exostoses presents with progressive bowing of her left forearm and limited supination and pronation. Radiographs show multiple osteochondromas around the distal radius and ulna, with significant shortening of the ulna relative to the radius and widening of the interosseous space.
View Answer & Explanation
Correct Answer: C
Rationale: Ulnar shortening and radial head dislocation are common complications of multiple hereditary exostoses affecting the forearm, due to growth disturbance caused by osteochondromas at the distal ulna. This leads to relative overgrowth of the radius, bowing of the radius, and subsequent dislocation of the radial head. While Madelung deformity can involve ulnar shortening and radial bowing, it is a specific congenital growth disturbance of the distal radius and ulna, distinct from the direct effects of osteochondromas in MHE. Carpal tunnel syndrome, scaphoid nonunion, and distal radius fracture are less directly related to the primary pathology of MHE in the forearm.
Question 72
A 38-year-old man with a history of multiple hereditary exostoses notices a rapidly growing, painful mass on his left scapula. The mass was previously a stable, asymptomatic exostosis. Radiographs and MRI show an enlarging lesion with irregular margins, cortical destruction, and a soft tissue component. Biopsy confirms malignancy.
View Answer & Explanation
Correct Answer: C
Rationale: The most common malignant transformation of an osteochondroma in patients with multiple hereditary exostoses is chondrosarcoma. The risk of malignant transformation is estimated to be around 1-5% in MHE, significantly higher than in solitary osteochondromas. Rapid growth, new pain, and radiographic signs of aggression in a previously stable osteochondroma are red flags for malignant degeneration. Osteosarcoma, fibrosarcoma, and Ewing sarcoma are much less common transformations.
Question 72
A 4-year-old boy presents with a painless bony mass on the medial side of his right ankle, causing a valgus deformity. Physical examination reveals a firm, irregular mass arising from the medial malleolus. Radiographs show an irregular, lobulated mass originating from the epiphysis of the distal tibia, with a cartilaginous cap, growing into the joint space.
View Answer & Explanation
Correct Answer: C
Rationale: Dysplasia epiphysealis hemimelica (Trevor's disease) is a rare, localized developmental anomaly characterized by an osteochondroma-like growth arising from an epiphysis, often affecting a single joint and causing deformity. The key features are its epiphyseal origin and unilateral involvement. Solitary osteochondromas typically arise from the metaphysis. Multiple hereditary exostoses involve multiple metaphyseal osteochondromas. Ollier disease involves enchondromas. Fibrous dysplasia has a distinct radiographic appearance.
Question 72
A 7-year-old girl is diagnosed with Dysplasia Epiphysealis Hemimelica (Trevor's disease) affecting her lower extremity. She presents with increasing pain and limited range of motion in the affected joint.
View Answer & Explanation
Correct Answer: D
Rationale: Dysplasia epiphysealis hemimelica most commonly affects the lower extremities, with the knee (distal femur or proximal tibia) and ankle (distal tibia or talus) being the most frequent sites. The medial side of the joint is more commonly involved. While other joints can be affected, the knee is the most prevalent location.
Question 72
A 28-year-old man presents with chronic pain and stiffness in his right lower extremity. Physical examination reveals mild limb length discrepancy and skin thickening over the affected limb. Radiographs of the right femur and tibia show irregular, linear areas of increased bone density along the cortex, resembling "flowing candle wax" or "dripping candle wax."
View Answer & Explanation
Correct Answer: C
Rationale: The classic radiographic description of "flowing candle wax" or "dripping candle wax" appearance, characterized by irregular cortical hyperostosis and sclerosis, is pathognomonic for melorheostosis. Osteopoikilosis presents as multiple small, round or ovoid sclerotic foci. Osteopathia striata shows linear striations of increased density. Fibrous dysplasia has a ground-glass appearance. Paget's disease involves disorganized bone remodeling with cortical thickening and trabecular coarsening, but not the "flowing" pattern of melorheostosis.
Question 72
A 40-year-old woman diagnosed with melorheostosis affecting her left forearm and hand reports progressive pain, joint stiffness, and difficulty with fine motor tasks. She also notes changes in the skin overlying the affected limb.
View Answer & Explanation
Correct Answer: D
Rationale: Melorheostosis is a sclerosing bone dysplasia that can affect bone, soft tissue, and skin. Common clinical features include chronic pain, joint contractures, limb length discrepancy (either shortening or lengthening), and characteristic scleroderma-like skin changes (thickening and induration) overlying the affected areas. Vascular malformations can also be associated. Therefore, all the listed options are common associated clinical features.
Question 72
A 50-year-old asymptomatic man undergoes a routine chest X-ray and incidental radiographs of his pelvis and femurs for an unrelated issue. The images reveal numerous small, well-defined, round to ovoid sclerotic foci scattered throughout the epiphyses and metaphyses of multiple bones, particularly prominent in the pelvis and proximal femurs. There is no evidence of bone destruction or periosteal reaction.
View Answer & Explanation
Correct Answer: C
Rationale: The radiographic finding of multiple small, well-defined, round or ovoid sclerotic foci, typically in the epiphyses and metaphyses, in an asymptomatic patient, is characteristic of osteopoikilosis (also known as osteopathia condensans disseminata). Osteoblastic metastases would be a primary concern, but they are usually more irregular in shape, vary in size, and often associated with a known primary malignancy. Bone infarcts can cause sclerotic areas but are typically more irregular and often have a serpiginous border. Melorheostosis has a "flowing candle wax" appearance. Osteopathia striata shows linear striations.
Question 72
A 30-year-old woman is diagnosed with osteopoikilosis after incidental radiographic findings. She reports that her mother and maternal grandfather also have similar findings on their X-rays. Genetic testing reveals a mutation in the LEMD3 gene.
View Answer & Explanation
Correct Answer: D
Rationale: Osteopoikilosis is inherited in an autosomal dominant pattern, often associated with mutations in the LEMD3 gene. The family history provided (mother and maternal grandfather affected) is consistent with autosomal dominant inheritance, where the trait appears in every generation and affects both males and females.
Question 72
A 12-year-old boy undergoes radiographs for evaluation of mild scoliosis. Incidental findings include multiple linear striations of increased bone density running parallel to the long axis of the bone in the metaphyses and diaphyses of the long bones, particularly the femurs and tibias. He is otherwise asymptomatic and has no other skeletal abnormalities.
View Answer & Explanation
Correct Answer: C
Rationale: The radiographic appearance of linear striations of increased bone density, running longitudinally in the metaphyses and diaphyses, is characteristic of osteopathia striata. Osteopoikilosis presents as small, round sclerotic foci. Melorheostosis has a "flowing candle wax" appearance. Stress fractures would typically be localized, painful, and show a different pattern of periosteal reaction or callus. Osteoblastic metastases are usually more irregular and associated with a primary malignancy.
Question 72
A 3-year-old child presents with progressive enlargement of the second and third digits of the right hand since birth. Physical examination reveals significant overgrowth of the soft tissues, bone, and nerves of these digits, leading to functional impairment. Doppler ultrasound confirms associated vascular anomalies within the affected digits.
View Answer & Explanation
Correct Answer: C
Rationale: Localized gigantism, or macrodactyly when affecting digits, is characterized by the progressive overgrowth of all mesenchymal tissues (bone, soft tissue, nerve, fat, and often associated with vascular anomalies) in a localized segment or digit. It is not merely isolated hypertrophy of one tissue type. The involvement of all tissues distinguishes it from simple vascular malformations or isolated bone/soft tissue lesions.
Question 72
A 1-year-old infant is diagnosed with hemihypertrophy affecting the entire right side of her body, including the right upper and lower extremities. Her pediatrician is concerned about associated risks.
View Answer & Explanation
Correct Answer: C
Rationale: Children with isolated hemihypertrophy or syndromes associated with hemihypertrophy (e.g., Beckwith-Wiedemann syndrome) have an increased risk of developing certain embryonal tumors, most notably Wilms' tumor (nephroblastoma), hepatoblastoma, and adrenocortical carcinoma. Regular screening with abdominal ultrasound is recommended to detect these tumors
Question 73
A 14-year-old male presents with a 6-month history of dull aching pain in his right proximal femur. Physical examination reveals mild tenderness over the greater trochanter. Radiographs show an expansile, lytic lesion in the metaphysis of the proximal femur with a characteristic "ground-glass" matrix and an intact cortex. There are no other skeletal lesions identified.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of a lytic, expansile lesion with a "ground-glass" matrix in the metaphysis of a long bone in an adolescent, without other systemic findings, is classic for monostotic fibrous dysplasia. Enchondromas typically have a chondroid matrix (rings and arcs calcification) and are often asymptomatic. Aneurysmal bone cysts are expansile and lytic but typically multiloculated and fluid-filled. Non-ossifying fibromas are usually cortically based, eccentric, and have a sclerotic rim. Low-grade chondrosarcomas are less common in this age group and would typically show more aggressive features or chondroid matrix calcifications.
Question 74
A 7-year-old girl is evaluated for multiple bone lesions, café-au-lait spots with irregular "coast of Maine" borders, and a history of vaginal bleeding and breast development since age 5. Radiographs demonstrate multiple lytic, expansile lesions in the long bones and pelvis with a "ground-glass" appearance. Laboratory tests confirm elevated estrogen levels.
View Answer & Explanation
Correct Answer: C
Rationale: The classic triad of polyostotic fibrous dysplasia, café-au-lait skin pigmentation, and precocious puberty (due to endocrine hyperfunction) is diagnostic of McCune-Albright syndrome. Ollier disease and Maffucci syndrome involve multiple enchondromas, not fibrous dysplasia. Neurofibromatosis type 1 can have café-au-lait spots but typically presents with neurofibromas and different skeletal manifestations (e.g., pseudarthrosis, scoliosis). Paget's disease is a disorder of bone remodeling, typically affecting older adults, and does not present with precocious puberty or café-au-lait spots.
Question 75
A 55-year-old man with a long-standing history of polyostotic fibrous dysplasia presents with new onset of severe, unremitting pain in his right proximal humerus, where he has a known fibrous dysplasia lesion. Over the past 3 months, he has noted rapid enlargement of the area. Radiographs show cortical destruction, soft tissue mass, and a more aggressive lytic pattern within the previously stable fibrous dysplasia lesion. Biopsy reveals malignant cells.
View Answer & Explanation
Correct Answer: C
Rationale: Malignant transformation of fibrous dysplasia is rare but a recognized complication, particularly in polyostotic forms or those treated with radiation. The most common malignant transformation is osteosarcoma, followed by chondrosarcoma and fibrosarcoma. The presentation of rapid growth, new pain, and aggressive radiographic features in a pre-existing fibrous dysplasia lesion is highly suspicious for malignant degeneration. Ewing sarcoma is typically a tumor of childhood and adolescence, and malignant fibrous histiocytoma is a less common transformation.
Question 76
A 6-year-old boy presents with progressive bowing of his left leg and shortening of his left arm. Physical examination reveals multiple palpable bony masses in the metaphyses of the long bones of the left upper and lower extremities. Radiographs show multiple radiolucent lesions with speckled calcifications, consistent with enchondromas, predominantly affecting one side of the body. There are no associated soft tissue vascular lesions.
View Answer & Explanation
Correct Answer: C
Rationale: The presence of multiple enchondromas, often unilateral or asymmetric, leading to limb deformity and shortening, without associated soft tissue hemangiomas, is characteristic of Ollier disease (enchondromatosis). Maffucci syndrome is similar but includes soft tissue hemangiomas. Multiple hereditary exostoses involve osteochondromas, not enchondromas. Dysplasia epiphysealis hemimelica is a localized epiphyseal osteochondroma. Fibrous dysplasia has a different radiographic appearance ("ground-glass").
Question 77
A 10-year-old girl presents with multiple firm, palpable masses in her hands and feet, causing deformity and pain. She also has several bluish, compressible soft tissue lesions on her extremities. Radiographs reveal multiple enchondromas in the phalanges and metacarpals, as well as in the long bones. MRI confirms the presence of multiple soft tissue hemangiomas.
View Answer & Explanation
Correct Answer: C
Rationale: Maffucci syndrome is characterized by the combination of multiple enchondromas and soft tissue hemangiomas. Ollier disease involves multiple enchondromas but lacks the hemangiomas. Klippel-Trenaunay syndrome involves capillary malformations, venous malformations, lymphatic malformations, and limb overgrowth, but not typically enchondromas. Proteus syndrome is a complex overgrowth syndrome with various manifestations, but not specifically enchondromas and hemangiomas as the primary defining features. Sturge-Weber syndrome involves facial port-wine stain, leptomeningeal angiomatosis, and ocular involvement.
Question 78
A 45-year-old man with a known history of Ollier disease presents with increasing pain and swelling in his left thigh over the past 4 months. Radiographs show enlargement of a previously stable enchondroma in the distal femur, with new cortical erosion and periosteal reaction. A biopsy is performed, confirming a low-grade chondrosarcoma.
View Answer & Explanation
Correct Answer: C
Rationale: Patients with Ollier disease have a significantly increased risk of malignant transformation of their enchondromas into chondrosarcomas. The reported risk ranges from 25% to 50%, with some studies suggesting even higher rates, especially in Maffucci syndrome. This risk is a critical consideration in the long-term management and monitoring of these patients.
Question 79
A 9-year-old boy is brought to the clinic by his parents due to multiple hard, bony lumps around his knees, shoulders, and wrists. He reports occasional pain and limited range of motion in his right elbow. His father also has similar bony growths. Physical examination reveals multiple exostoses arising from the metaphyses of long bones. Radiographs confirm multiple osteochondromas.
View Answer & Explanation
Correct Answer: D
Rationale: The presence of multiple osteochondromas (exostoses) with an autosomal dominant inheritance pattern (father also affected) is characteristic of multiple hereditary exostoses (MHE), also known as hereditary multiple osteochondromas. Solitary osteochondroma is a single lesion. Ollier disease involves multiple enchondromas. Fibrous dysplasia has a different radiographic appearance. Dysplasia epiphysealis hemimelica is a localized epiphyseal osteochondroma-like lesion, typically unilateral and affecting a single joint.
Question 80
An 11-year-old girl with multiple hereditary exostoses presents with progressive bowing of her left forearm and limited supination and pronation. Radiographs show multiple osteochondromas around the distal radius and ulna, with significant shortening of the ulna relative to the radius and widening of the interosseous space.
View Answer & Explanation
Correct Answer: C
Rationale: Ulnar shortening and radial head dislocation are common complications of multiple hereditary exostoses affecting the forearm, due to growth disturbance caused by osteochondromas at the distal ulna. This leads to relative overgrowth of the radius, bowing of the radius, and subsequent dislocation of the radial head. While Madelung deformity can involve ulnar shortening and radial bowing, it is a specific congenital growth disturbance of the distal radius and ulna, distinct from the direct effects of osteochondromas in MHE. Carpal tunnel syndrome, scaphoid nonunion, and distal radius fracture are less directly related to the primary pathology of MHE in the forearm.
Question 81
A 38-year-old man with a history of multiple hereditary exostoses notices a rapidly growing, painful mass on his left scapula. The mass was previously a stable, asymptomatic exostosis. Radiographs and MRI show an enlarging lesion with irregular margins, cortical destruction, and a soft tissue component. Biopsy confirms malignancy.
View Answer & Explanation
Correct Answer: C
Rationale: The most common malignant transformation of an osteochondroma in patients with multiple hereditary exostoses is chondrosarcoma. The risk of malignant transformation is estimated to be around 1-5% in MHE, significantly higher than in solitary osteochondromas. Rapid growth, new pain, and radiographic signs of aggression in a previously stable osteochondroma are red flags for malignant degeneration. Osteosarcoma, fibrosarcoma, and Ewing sarcoma are much less common transformations.
Question 82
A 4-year-old boy presents with a painless bony mass on the medial side of his right ankle, causing a valgus deformity. Physical examination reveals a firm, irregular mass arising from the medial malleolus. Radiographs show an irregular, lobulated mass originating from the epiphysis of the distal tibia, with a cartilaginous cap, growing into the joint space.
View Answer & Explanation
Correct Answer: C
Rationale: Dysplasia epiphysealis hemimelica (Trevor's disease) is a rare, localized developmental anomaly characterized by an osteochondroma-like growth arising from an epiphysis, often affecting a single joint and causing deformity. The key features are its epiphyseal origin and unilateral involvement. Solitary osteochondromas typically arise from the metaphysis. Multiple hereditary exostoses involve multiple metaphyseal osteochondromas. Ollier disease involves enchondromas. Fibrous dysplasia has a distinct radiographic appearance.
Question 83
A 7-year-old girl is diagnosed with Dysplasia Epiphysealis Hemimelica (Trevor's disease) affecting her lower extremity. She presents with increasing pain and limited range of motion in the affected joint.
View Answer & Explanation
Correct Answer: D
Rationale: Dysplasia epiphysealis hemimelica most commonly affects the lower extremities, with the knee (distal femur or proximal tibia) and ankle (distal tibia or talus) being the most frequent sites. The medial side of the joint is more commonly involved. While other joints can be affected, the knee is the most prevalent location.
Question 84
A 28-year-old man presents with chronic pain and stiffness in his right lower extremity. Physical examination reveals mild limb length discrepancy and skin thickening over the affected limb. Radiographs of the right femur and tibia show irregular, linear areas of increased bone density along the cortex, resembling "flowing candle wax" or "dripping candle wax."
View Answer & Explanation
Correct Answer: C
Rationale: The classic radiographic description of "flowing candle wax" or "dripping candle wax" appearance, characterized by irregular cortical hyperostosis and sclerosis, is pathognomonic for melorheostosis. Osteopoikilosis presents as multiple small, round or ovoid sclerotic foci. Osteopathia striata shows linear striations of increased density. Fibrous dysplasia has a ground-glass appearance. Paget's disease involves disorganized bone remodeling with cortical thickening and trabecular coarsening, but not the "flowing" pattern of melorheostosis.
Question 85
A 40-year-old woman diagnosed with melorheostosis affecting her left forearm and hand reports progressive pain, joint stiffness, and difficulty with fine motor tasks. She also notes changes in the skin overlying the affected limb.
View Answer & Explanation
Correct Answer: D
Rationale: Melorheostosis is a sclerosing bone dysplasia that can affect bone, soft tissue, and skin. Common clinical features include chronic pain, joint contractures, limb length discrepancy (either shortening or lengthening), and characteristic scleroderma-like skin changes (thickening and induration) overlying the affected areas. Vascular malformations can also be associated. Therefore, all the listed options are common associated clinical features.
Question 86
A 50-year-old asymptomatic man undergoes a routine chest X-ray and incidental radiographs of his pelvis and femurs for an unrelated issue. The images reveal numerous small, well-defined, round to ovoid sclerotic foci scattered throughout the epiphyses and metaphyses of multiple bones, particularly prominent in the pelvis and proximal femurs. There is no evidence of bone destruction or periosteal reaction.
View Answer & Explanation
Correct Answer: C
Rationale: The radiographic finding of multiple small, well-defined, round or ovoid sclerotic foci, typically in the epiphyses and metaphyses, in an asymptomatic patient, is characteristic of osteopoikilosis (also known as osteopathia condensans disseminata). Osteoblastic metastases would be a primary concern, but they are usually more irregular in shape, vary in size, and often associated with a known primary malignancy. Bone infarcts can cause sclerotic areas but are typically more irregular and often have a serpiginous border. Melorheostosis has a "flowing candle wax" appearance. Osteopathia striata shows linear striations.
Question 87
A 30-year-old woman is diagnosed with osteopoikilosis after incidental radiographic findings. She reports that her mother and maternal grandfather also have similar findings on their X-rays. Genetic testing reveals a mutation in the LEMD3 gene.
View Answer & Explanation
Correct Answer: D
Rationale: Osteopoikilosis is inherited in an autosomal dominant pattern, often associated with mutations in the LEMD3 gene. The family history provided (mother and maternal grandfather affected) is consistent with autosomal dominant inheritance, where the trait appears in every generation and affects both males and females.
Question 88
A 12-year-old boy undergoes radiographs for evaluation of mild scoliosis. Incidental findings include multiple linear striations of increased bone density running parallel to the long axis of the bone in the metaphyses and diaphyses of the long bones, particularly the femurs and tibias. He is otherwise asymptomatic and has no other skeletal abnormalities.
View Answer & Explanation
Correct Answer: C
Rationale: The radiographic appearance of linear striations of increased bone density, running longitudinally in the metaphyses and diaphyses, is characteristic of osteopathia striata. Osteopoikilosis presents as small, round sclerotic foci. Melorheostosis has a "flowing candle wax" appearance. Stress fractures would typically be localized, painful, and show a different pattern of periosteal reaction or callus. Osteoblastic metastases are usually more irregular and associated with a primary malignancy.
Question 89
A 3-year-old child presents with progressive enlargement of the second and third digits of the right hand since birth. Physical examination reveals significant overgrowth of the soft tissues, bone, and nerves of these digits, leading to functional impairment. Doppler ultrasound confirms associated vascular anomalies within the affected digits.
View Answer & Explanation
Correct Answer: C
Rationale: Localized gigantism, or macrodactyly when affecting digits, is characterized by the progressive overgrowth of all mesenchymal tissues (bone, soft tissue, nerve, fat, and often associated with vascular anomalies) in a localized segment or digit. It is not merely isolated hypertrophy of one tissue type. The involvement of all tissues distinguishes it from simple vascular malformations or isolated bone/soft tissue lesions.
Question 90
A 12-year-old male presents with a 3-month history of progressive pain and swelling in his left thigh. Physical examination reveals a palpable, tender mass. Radiographs show a permeative lesion in the femoral diaphysis with periosteal reaction.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text states that Ewing's sarcoma "most commonly present in the first three decades of life." This encompasses children, adolescents, and young adults, which aligns with the typical presentation of this tumor. Main Distractor: A) While Ewing's sarcoma is common in the first decade, the text specifies "first three decades" as the broader, most common range, making option B more accurate.
Question 91
A 15-year-old female presents with right forearm pain. Radiographs, as shown in Fig. 8.98a, reveal a lytic lesion in the proximal radius.

View Answer & Explanation
Correct Answer: C
Rationale: The clinical text and the description for Fig. 8.98a explicitly state that Ewing's sarcoma presents with a "permeative pattern, broad zone of transition, and periosteal reaction." The image clearly demonstrates these features. Main Distractor: A) A well-defined sclerotic margin with a narrow zone of transition is characteristic of a benign or slow-growing lesion, which is contrary to the aggressive nature of Ewing's sarcoma.
Question 92
A 7-year-old boy presents with a painful mass in his tibia. Biopsy is performed. A low-power photomicrograph, similar to Fig. 8.101, is obtained.
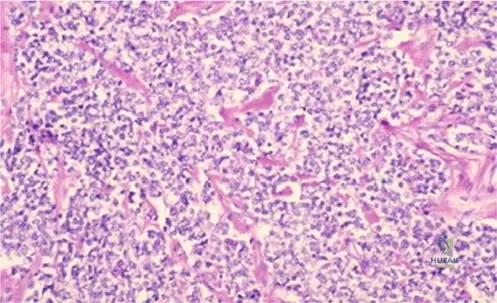
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text and the description for Fig. 8.101 explicitly state that histologically, Ewing's sarcoma tumors are "composed of small, round, blue cells." The image also shows this uniform population. Main Distractor: A) Spindle cell proliferation with osteoid formation is characteristic of osteosarcoma, a different type of bone tumor.
Question 93
A 10-year-old male presents with persistent pain in his left humerus. Physical exam reveals localized tenderness. Radiographs show a lytic lesion in the mid-diaphysis.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text states, "Lesions typically present in the diaphysis or metadiaphysis of long bones, although flat bones such as the pelvis and scapula may also be involved." Main Distractor: A) The epiphysis of long bones is a less common location for Ewing's sarcoma, being more typical for tumors like chondroblastoma.
Question 94
A 16-year-old athlete reports increasing pain in his right femur over the past two months, which is worse at night and wakes him from sleep. Physical exam is unremarkable except for mild tenderness.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states, "Most patients will have pain at rest or at night." This is a classic symptom of malignant bone tumors, including Ewing's sarcoma. Main Distractor: A) Pain exclusively with activity and relieved by rest is more characteristic of mechanical issues, stress fractures, or benign conditions, not typically a malignant bone tumor.
Question 95
A 5-year-old girl presents with a rapidly growing mass in her pelvis. Biopsy reveals a tumor composed of small, round, blue cells.
View Answer & Explanation
Correct Answer: D
Rationale: Ewing's sarcoma is classified as a "round cell sarcoma." Lymphoma is another prominent member of the "small, round, blue cell tumor" differential diagnosis in bone, especially in children and young adults. Other common small round blue cell tumors include rhabdomyosarcoma, neuroblastoma,
Question 95
A 10-year-old boy presents with right thigh pain for 2 months, accompanied by low-grade fever and localized swelling. Laboratory tests reveal elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Radiographs show a permeative lesion in the femoral diaphysis with periosteal reaction.
View Answer & Explanation
Correct Answer: B
Rationale: Ewing's sarcoma often presents with signs and symptoms that mimic infection, such as pain, swelling, fever, and elevated inflammatory markers, leading to diagnostic challenges. While pathologic fractures can occur, they are not the most common initial presentation. Joint effusions are not typical, and the tumor is rarely asymptomatic.
Question 95
A 14-year-old male presents with progressive pain in his proximal forearm. Radiographs are obtained.
View Answer & Explanation
Correct Answer: B
Rationale: As described in the clinical context for Fig. 8.98a, Ewing's sarcoma typically presents with a permeative pattern, a broad zone of transition, and periosteal reaction on radiographs, indicating an aggressive lesion. Well-defined sclerotic margins are characteristic of benign or less aggressive lesions, and epiphyseal involvement is uncommon.
Question 95
A biopsy is performed on a 12-year-old girl with a diaphyseal lesion of the tibia. Low-power microscopic examination of the tissue is shown.
View Answer & Explanation
Correct Answer: B
Rationale: As stated in the clinical context for Fig. 8.101, Ewing's sarcoma is histologically characterized by a uniform population of small, round, blue cells. Spindle cells, chondroid matrix, osteoid formation, and giant cells are characteristic features of other bone tumors.
Question 95
Further high-power microscopic examination of the same biopsy specimen from the 12-year-old girl is performed.
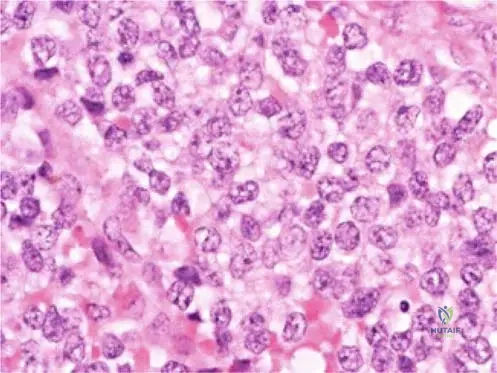
View Answer & Explanation
Correct Answer: B
Rationale: As described in the clinical context for Fig. 8.102, high-power microscopy of Ewing's sarcoma typically shows uniform cells and prominent nucleoli, often with little mitotic activity. Marked pleomorphism and high mitotic activity are characteristic of many high-grade sarcomas but the uniformity is a key feature of Ewing's. True rosettes are more characteristic of neuroblastoma.
Question 95
A 7-year-old boy presents with persistent pain in his left upper arm. Imaging reveals a destructive lesion.
View Answer & Explanation
Correct Answer: C
Rationale: Ewing's sarcoma typically presents in the diaphysis or metadiaphysis of long bones. Epiphyseal involvement is rare for this tumor, distinguishing it from other pediatric bone tumors like chondroblastoma.
Question 95
A patient is diagnosed with Ewing's sarcoma.
View Answer & Explanation
Correct Answer: B
Rationale: Ewing's sarcoma most commonly presents in the first three decades of life, making it primarily a tumor of children, adolescents, and young adults. It is relatively rare in infants or older adults.
Question 95
A 16-year-old male is diagnosed with Ewing's sarcoma of the femur.
View Answer & Explanation
Correct Answer: C
Rationale: By definition, Ewing's sarcoma is considered a high-grade malignant lesion, reflecting its aggressive biological behavior and propensity for metastasis. It is never considered benign or low-grade.
Question 95
A 13-year-old girl presents with pain and swelling in her proximal radius. An MRI is performed.
View Answer & Explanation
Correct Answer: B
Rationale: As described in the clinical context for Fig. 8.98b, the MRI clearly shows significant bone destruction and a large soft tissue mass extending beyond the bone, which is characteristic of aggressive bone sarcomas like Ewing's.
Question 96
A 10-year-old boy presents with right thigh pain for 2 months, accompanied by low-grade fever and localized swelling. Laboratory tests reveal elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Radiographs show a permeative lesion in the femoral diaphysis with periosteal reaction.
View Answer & Explanation
Correct Answer: B
Rationale: Ewing's sarcoma often presents with signs and symptoms that mimic infection, such as pain, swelling, fever, and elevated inflammatory markers, leading to diagnostic challenges. While pathologic fractures can occur, they are not the most common initial presentation. Joint effusions are not typical, and the tumor is rarely asymptomatic.
Question 97
A 14-year-old male presents with progressive pain in his proximal forearm. Radiographs are obtained.
View Answer & Explanation
Correct Answer: B
Rationale: As described in the clinical context for Fig. 8.98a, Ewing's sarcoma typically presents with a permeative pattern, a broad zone of transition, and periosteal reaction on radiographs, indicating an aggressive lesion. Well-defined sclerotic margins are characteristic of benign or less aggressive lesions, and epiphyseal involvement is uncommon.
Question 98
A biopsy is performed on a 12-year-old girl with a diaphyseal lesion of the tibia. Low-power microscopic examination of the tissue is shown.
View Answer & Explanation
Correct Answer: B
Rationale: As stated in the clinical context for Fig. 8.101, Ewing's sarcoma is histologically characterized by a uniform population of small, round, blue cells. Spindle cells, chondroid matrix, osteoid formation, and giant cells are characteristic features of other bone tumors.
Question 99
Further high-power microscopic examination of the same biopsy specimen from the 12-year-old girl is performed.
View Answer & Explanation
Correct Answer: B
Rationale: As described in the clinical context for Fig. 8.102, high-power microscopy of Ewing's sarcoma typically shows uniform cells and prominent nucleoli, often with little mitotic activity. Marked pleomorphism and high mitotic activity are characteristic of many high-grade sarcomas but the uniformity is a key feature of Ewing's. True rosettes are more characteristic of neuroblastoma.
Question 100
A 7-year-old boy presents with persistent pain in his left upper arm. Imaging reveals a destructive lesion.
View Answer & Explanation
Correct Answer: C
Rationale: Ewing's sarcoma typically presents in the diaphysis or metadiaphysis of long bones. Epiphyseal involvement is rare for this tumor, distinguishing it from other pediatric bone tumors like chondroblastoma.
