Master ABOS Orthopaedic Review: Bone Tumors, Skeletal Dysplasias & Arthritis Essentials | Part 29
Key Takeaway
This ABOS Board Review covers essential orthopaedic topics including Langerhans Cell Histiocytosis (LCH), Aneurysmal Bone Cysts (ABC), Multiple Epiphyseal Dysplasia (MED), and Psoriatic Arthritis (PsA). It details their diagnosis, clinical presentation, radiographic features, histology, and management, crucial for orthopaedic exam preparation.
Question 1
A 5-year-old female is diagnosed with Langerhans Cell Histiocytosis after presenting with a painful swelling in her rib. During her workup, the orthopaedic surgeon is aware that patients with LCH can develop systemic complications. Which of the following endocrine disorders is specifically mentioned as a potential complication?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states, "Patients may develop diabetes insipidus." This is a known systemic complication of LCH, particularly when the pituitary gland or hypothalamus is involved. The other endocrine disorders are not mentioned in the provided text as specific complications of LCH.
Question 2
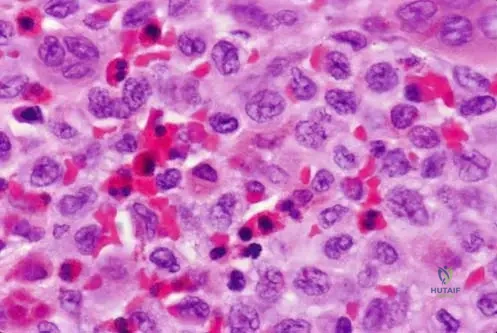
A 12-year-old male undergoes a biopsy for a lytic lesion in his ilium, suspected to be Langerhans Cell Histiocytosis. Histological examination is performed. Which of the following cell types is a characteristic feature of LCH lesions, often described with an indented nucleus?
View Answer & Explanation
Correct Answer: D
Rationale: The provided histological description states, "Langerhans cells usually have an indented nucleus and small nucleoli." While plasma cells are also present, the Langerhans cell itself is the pathognomonic cell type with the described nuclear morphology and gives the condition its name.
Question 3
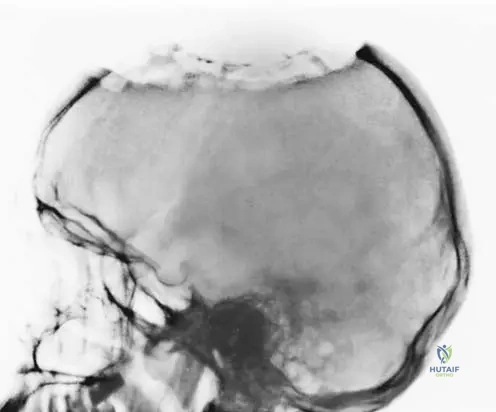
A 3-year-old female presents with a palpable swelling on her forehead. Radiographs of the skull reveal a destructive lesion. A biopsy confirms Langerhans Cell Histiocytosis. Which of the following best describes the typical radiographic appearance of such a lesion in the skull?
View Answer & Explanation
Correct Answer: C
Rationale: Figure 11.42 is captioned "Destruction of skull secondary to Langerhans cell histiocytosis," indicating a destructive pattern. The image itself shows an area of bone loss. While the text doesn't explicitly describe "ill-defined margins," destructive lesions often present this way, and it aligns with the image. Sclerotic lesions or well-circumscribed lesions with sclerotic rims are not characteristic of the destructive nature shown.
Question 4
A 15-year-old male presents with persistent pain and swelling in his left hip. Imaging reveals a lytic lesion in the ilium. A biopsy is performed, confirming Langerhans Cell Histiocytosis. Based on the provided information, which of the following statements regarding the presentation of LCH is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Lesions tend to be symptomatic (pain, swelling) and only rarely will an area of histiocytosis be discovered incidentally." This directly supports option C. Options A, B, and D contradict the provided information regarding symptoms, common sites, and age range, respectively. The text does not comment on the benign nature or intervention requirements.
Question 5
A 2-year-old child is evaluated for a new onset of hearing loss. Physical examination reveals no obvious external ear abnormalities. Imaging studies show a lytic lesion involving the mastoid bone. A biopsy is planned to investigate for Langerhans Cell Histiocytosis. What is the specific association between mastoid involvement and hearing loss in LCH?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "Those with mastoid involvement may have hearing loss." This directly confirms the association without specifying the exact type of hearing loss (conductive vs. sensorineural) or mechanism. Therefore, the most accurate answer based strictly on the provided text is that mastoid involvement is associated with hearing loss.
Question 6
A 10-year-old girl presents with a painful swelling over her left rib. Radiographs show a lytic lesion. A biopsy is performed, and the pathologist notes the presence of numerous eosinophils in addition to other inflammatory cells. Which of the following cell types is also typically abundant in Langerhans Cell Histiocytosis lesions, as described histologically?
View Answer & Explanation
Correct Answer: D
Rationale: The histological description states, "Histologically, lesions are composed of many cell types, including histiocytes, plasma cells, eosinophils, and other inflammatory cells." Therefore, plasma cells are explicitly mentioned as being present in LCH lesions. While macrophages and lymphocytes are generally inflammatory cells, plasma cells are specifically listed in the context of LCH histology.
Question 7
A 4-year-old boy is diagnosed with Langerhans Cell Histiocytosis affecting his skull. His parents inquire about the typical age range for this condition. Based on the provided clinical information, which statement best describes the age distribution of LCH?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Th is is a hematopoietic condition that can aff ect a variety of ages, although most patients are under age 30." This directly supports option C. The other options contradict this statement regarding the typical age distribution.
Question 8
A 25-year-old male presents with a painful, enlarging mass in his left femur. Radiographs show a lytic lesion. A biopsy is performed, and the pathology report describes a lesion composed of histiocytes, plasma cells, and numerous eosinophils. What is the characteristic nuclear feature of the Langerhans cells often observed in these lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The histological description explicitly states, "Langerhans cells usually have an indented nucleus and small nucleoli." This is a key diagnostic feature of Langerhans cells in LCH.
Question 9
A 6-year-old boy presents with a painful swelling in his skull, confirmed to be Langerhans Cell Histiocytosis. His parents ask about the origin of this condition. Based on the provided information, LCH is classified as which type of condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text begins by stating, "Th is is a hematopoietic condition that can aff ect a variety of ages..." This directly classifies LCH as a hematopoietic condition.
Question 10
A 1-year-old infant is found to have an enlarging skull lesion. Clinical examination reveals a soft, palpable mass. Radiographs show a lytic defect in the skull. A biopsy is performed, confirming Langerhans Cell Histiocytosis. What is the most common clinical finding associated with LCH lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Pain and swelling of the involved bone are the most common clinical fi ndings." This directly answers the question. The other options are not mentioned as the most common clinical findings in the provided text.
Question 11
A 14-year-old male presents with a several-week history of a tender, enlarging area on his forehead. Clinically, there is a noticeable enlargement of the skull in the affected region. Imaging confirms a destructive lesion. A biopsy is planned for suspected Langerhans Cell Histiocytosis. What does the clinical photograph of a skull lesion in LCH typically demonstrate?

View Answer & Explanation
Correct Answer: C
Rationale: Figure 11.43 is captioned, "Clinical photograph at the time of surgery showing enlargement of the skull." This directly indicates that enlargement of the skull is a typical clinical finding.
Question 12
A 9-year-old girl presents with a painful lump on her back. Radiographs reveal a lytic lesion in a rib. A biopsy confirms Langerhans Cell Histiocytosis. Besides the skull, femur, and ilium, which other bone is specifically mentioned as a predilection site for LCH?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "Any bone may be aff ected, but there is a predilection for the skull, femur, ribs, and ilium." Therefore, ribs are explicitly listed as a predilection site.
Question 13
A 2-year-old male presents with a painful, enlarging mass on his scalp. Radiographs show a destructive lesion in the parietal bone. A biopsy is performed, and the pathologist identifies numerous eosinophils and cells with indented nuclei. What is the primary cell type that gives Langerhans Cell Histiocytosis its name and is characterized by these indented nuclei?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Histologically, lesions are composed of many cell types, including histiocytes, plasma cells, eosinophils, and other infl ammatory cells. Langerhans cells usually have an indented nucleus..." Langerhans cells are a type of histiocyte. The condition is named after these specialized histiocytes. While eosinophils and plasma cells are present, histiocytes (specifically Langerhans cells) are the defining cell type.
Question 14
A 17-year-old female is diagnosed with Langerhans Cell Histiocytosis after presenting with a painful lesion in her ilium. Her physician is reviewing the potential systemic manifestations of LCH. Which of the following statements accurately describes the typical presentation of LCH lesions regarding symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Lesions tend to be symptomatic (pain, swelling) and only rarely will an area of histiocytosis be discovered incidentally." This directly supports option C and refutes options A and B.
Question 15
A 28-year-old male presents with a new onset of polyuria and polydipsia, along with a painful lesion in his skull. Imaging confirms a destructive lesion, and a biopsy reveals Langerhans Cell Histiocytosis. The patient's endocrine symptoms are consistent with diabetes insipidus. This systemic complication is a result of LCH affecting which part of the body?
View Answer & Explanation
Correct Answer: C
Rationale: While the provided text only states "Patients may develop diabetes insipidus," it is common knowledge in orthopaedic oncology that diabetes insipidus in LCH results from involvement of the pituitary gland or hypothalamus, which controls antidiuretic hormone (ADH) secretion. This question tests the understanding of the mechanism behind the stated complication.
Question 16
A 5-year-old boy presents with a painful swelling over his left parietal bone. Radiographs show a lytic lesion. A biopsy is performed, and the histological findings include a mixed inflammatory infiltrate with numerous eosinophils. Which of the following statements regarding the eosinophil presence in LCH lesions is accurate?
View Answer & Explanation
Correct Answer: C
Rationale: The histological description states, "Histologically, lesions are composed of many cell types, including histiocytes, plasma cells, eosinophils, and other infl ammatory cells... There may be many eosinophils present." This directly supports option C.
Question 17
A 19-year-old male presents with a painful, enlarging mass in his right femur. Imaging reveals a lytic lesion. A biopsy confirms Langerhans Cell Histiocytosis. Given the hematopoietic nature of LCH, which of the following best describes its origin?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Th is is a hematopoietic condition..." Hematopoietic refers to the formation of blood cellular components. Therefore, it is derived from cells of the blood-forming system.
Question 18
A 10-year-old female presents with a several-month history of a painful, palpable mass on her left rib. Radiographs show a lytic lesion. A biopsy is performed, confirming Langerhans Cell Histiocytosis. Which of the following statements accurately reflects the typical presentation of LCH in terms of symptom onset?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Lesions tend to be symptomatic (pain, swelling) and only rarely will an area of histiocytosis be discovered incidentally." This directly supports option C. Options A and B are contradicted by the text.
Question 19
A 14-year-old female presents with a 3-month history of progressive pain and swelling in her proximal tibia. Physical examination reveals localized tenderness and mild warmth. Radiographs show an expansile lytic lesion in the metaphysis.
View Answer & Explanation
Correct Answer: B
Rationale: Aneurysmal bone cysts typically occur in the first two decades of life, aligning with the patient's age. While some may present in the first decade, the most encompassing period is the first two. Options C, D, and E represent older age groups less commonly affected by primary ABCs.
Question 20
A 10-year-old male presents to the clinic with a chief complaint of persistent pain in his distal femur, which has been worsening over the past several weeks. He also notes some swelling in the area. Physical examination confirms local tenderness and palpable swelling.
View Answer & Explanation
Correct Answer: D
Rationale: Patients with aneurysmal bone cysts typically present with pain and swelling of the involved area, as described in the clinical context. While a pathological fracture can occur, it is a complication rather than the primary presenting symptom. Fever, chills, weight loss, and night sweats are more indicative of infectious or malignant processes.
Question 21
During surgical curettage of an expansile lesion in the proximal humerus of a 16-year-old patient, the surgeon encounters tissue within the bone cavity. The image below shows the typical gross appearance of this tissue.

View Answer & Explanation
Correct Answer: C
Rationale: As shown in Fig. 11.12 and described in the text, the gross appearance of an aneurysmal bone cyst tissue can range from brownish to more hemorrhagic, often with notable intralesional septations. Options A, B, D, and E describe features of other types of bone lesions or infections.
Question 22
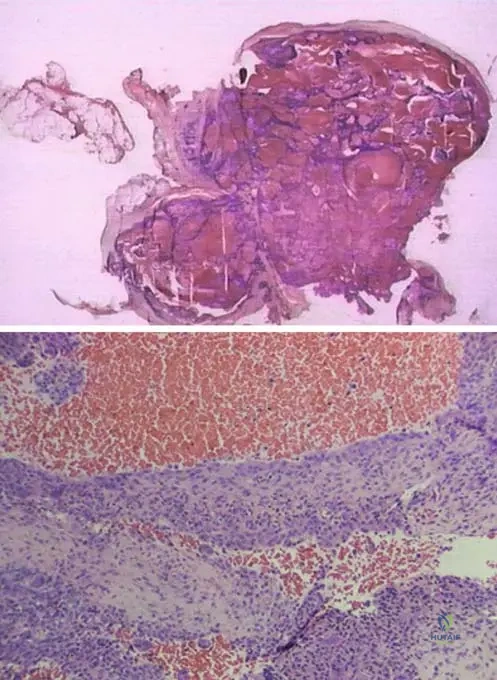
A biopsy is performed on a 12-year-old girl with an expansile lytic lesion in her distal femur. The photomicrograph below shows the characteristic histological features of the lesion.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.14 and its context state that photomicrographs of an aneurysmal bone cyst show blood-filled cystic spaces with lining, and giant cells are often present. This is the hallmark histological feature. Options A, B, D, and E describe features of chondroid tumors, fibrous histiocytoma, Ewing sarcoma, and non-ossifying fibroma/xanthoma, respectively.
Question 23
A 15-year-old male presents with progressive pain and swelling in his distal femur. Radiographs show an expansile lytic lesion. Based on the description, an aneurysmal bone cyst is best characterized as:
View Answer & Explanation
Correct Answer: B
Rationale: The provided text explicitly states that aneurysmal bone cysts are "benign, locally aggressive cystic lesions." They are not malignant, metastatic, infectious, or metabolic. Option A is incorrect because ABCs are benign. Option C is incorrect as they are primary bone lesions.
Question 24
A 13-year-old patient undergoes curettage for an aneurysmal bone cyst in the proximal tibia. The surgeon is discussing the prognosis and potential for recurrence with the patient's parents.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical text states that aneurysmal bone cysts "tend to recur in high percentage following curettage (20–50%)". This high recurrence rate is a significant characteristic of ABCs treated with curettage alone. Options A, B, C, and E are outside this stated range.
Question 25
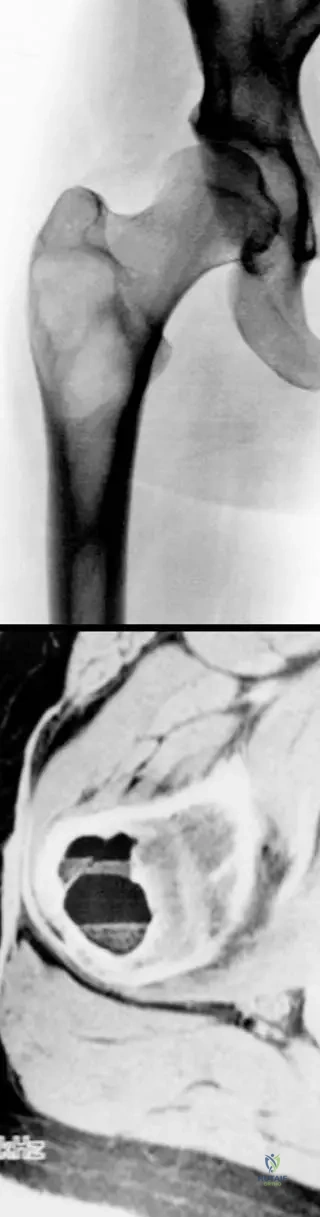
A 17-year-old female with a known history of fibrous dysplasia in her proximal femur presents with new onset pain and swelling. An MRI is performed, revealing fluid-fluid levels within the lesion, as shown in the image below.
View Answer & Explanation
Correct Answer: C
Rationale: The provided text and Fig. 11.11 explicitly state that "Conditions such as fibrous dysplasia can develop secondary aneurysmal bone cyst." The vignette describes a patient with known fibrous dysplasia developing symptoms consistent with a secondary ABC. Options A, B, D, and E are other bone lesions, but only fibrous dysplasia is listed in the text as a condition that can lead to secondary ABC formation.
Question 26
A 12-year-old boy presents with pain in his distal tibia. An MRI is ordered to further characterize an expansile lytic lesion seen on radiographs. The image below shows a characteristic finding on the MRI.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.11b, which depicts an MRI of a secondary aneurysmal bone cyst, explicitly shows "the fluid levels of the components of secondary aneurysmal bone cyst." Fluid-fluid levels are a classic MRI finding for ABCs, representing sedimentation of blood products within cystic spaces. Options A, B, D, and E are characteristic of other bone pathologies (e.g., osteosarcoma, chronic osteomyelitis).
Question 27
A 14-year-old female is diagnosed with an aneurysmal bone cyst. Her physician explains that ABCs can sometimes arise as a secondary phenomenon from other underlying bone lesions.
View Answer & Explanation
Correct Answer: D
Rationale: The provided text states that aneurysmal bone cysts can occur as secondary phenomena in "other conditions such as giant cell tumor, fibrous dysplasia, and chondroblastoma." Osteosarcoma is a malignant tumor and is not listed as a precursor for secondary ABC formation. Non-ossifying fibroma is a benign lesion but also not listed in the text as a primary cause for secondary ABC.
Question 28
A 16-year-old patient presents with a painful, expansile lesion in her distal femur. After diagnostic workup, she is diagnosed with an aneurysmal bone cyst. When discussing the epidemiology of this condition, the physician notes a slight predilection for a particular gender.
View Answer & Explanation
Correct Answer: B
Rationale: The provided text explicitly states that aneurysmal bone cysts "are slightly more common in women." Therefore, females have a slight predilection. Options A, C, D, and E are incorrect based on the provided information.
Question 29
A surgeon is performing an intraoperative procedure for an aneurysmal bone cyst in the lower extremity of a 15-year-old patient. The image below shows the typical appearance of the lesion during surgery.

View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.15b, an intraoperative photograph, clearly shows "multiple septations and blood-filled spaces" within the aneurysmal bone cyst. This is a characteristic gross finding during surgery. Options A, B, D, and E describe features of other bone lesions or conditions.
Question 30
A pathologist receives a tissue specimen from an excised aneurysmal bone cyst. The image below shows the typical characteristics of the tissue.

View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.13 and its context state that "Tissue from within an aneurysmal bone cyst is usually friable and brownish-red in color." This description matches the image and the nature of the blood-filled cystic spaces. Options A, B, D, and E describe characteristics not typical of ABC tissue.
Question 31
A 10-year-old boy presents with a 2-month history of pain and swelling in his distal radius. On physical examination, the physician notes localized findings related to the suspected aneurysmal bone cyst.
View Answer & Explanation
Correct Answer: C
Rationale: The provided text states that "Physical findings include local tenderness, swelling, and limited range of motion" for aneurysmal bone cysts. These are direct local effects of the lesion. Options A, B, D, and E are less common or not typical physical findings for an uncomplicated ABC.
Question 32
Histological examination of an aneurysmal bone cyst reveals numerous blood-filled cystic spaces. The text notes that these spaces have a "lining."
View Answer & Explanation
Correct Answer: D
Rationale: Fig. 11.14 and its context state "Photomicrographs show blood-filled cystic spaces with lining. Giant cells are often present." This lining is typically fibrous tissue, and the presence of giant cells is a key histological feature. Options A, B, C, and E describe features inconsistent with the histology of an ABC.
Question 33
A 16-year-old male undergoes curettage for a large aneurysmal bone cyst in his proximal tibia. Given the high recurrence rate associated with curettage alone, the surgeon considers an adjuvant treatment to reduce the risk of recurrence.
View Answer & Explanation
Correct Answer: C
Rationale: While not explicitly detailed as a treatment in the provided text, the high recurrence rate (20-50%) after curettage implies that curettage alone is often insufficient. Intralesional sclerotherapy is a recognized adjuvant treatment for ABCs, aiming to reduce recurrence by inducing fibrosis and thrombosis within the cystic spaces. Options A, D, and E are generally inappropriate for a benign lesion. Radiation therapy is typically reserved for difficult-to-access locations (e.g., spine) due to risks of secondary malignancy, and not a primary adjuvant to curettage in this context.
Question 34
A 15-year-old male presents with progressive pain and swelling in his distal femur. Radiographs show an expansile lytic lesion. Based on the description, an aneurysmal bone cyst is best characterized as:
- A) Malignant and metastatic
- B) Benign and non-aggressive
- C) Benign and locally aggressive
-
Question 34
A 14-year-old female presents with a 3-month history of progressive pain and swelling in her distal femur. Physical examination reveals local tenderness and limited range of motion. Radiographs show an expansile lytic lesion in the metaphysis. Given the typical demographic for aneurysmal bone cyst, what is the most common age range for presentation?
View Answer & Explanation
Correct Answer: B
Rationale: Aneurysmal bone cysts usually occur in the first two decades of life. This demographic information is a key characteristic of the lesion. Main Distractor: Option A (First decade of life) is too narrow; while it can occur, the text specifies "first two decades," making it a less complete answer.
Question 34
A 12-year-old male presents with a 6-week history of worsening pain in his proximal humerus. He denies any trauma. On examination, there is palpable swelling and tenderness over the affected area. Radiographs demonstrate an expansile, lytic lesion. What is the most common presenting symptom for an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: Patients with aneurysmal bone cysts typically present with pain and swelling of the involved area, as stated in the clinical context. Main Distractor: Option A (Pathologic fracture) can occur but is not described as the *typical* or *most common* presenting symptom in the provided text, which emphasizes pain and swelling.
Question 34
During surgical curettage of an expansile lesion in the tibia of a 16-year-old female, the surgeon encounters friable tissue within cystic spaces. Based on the gross appearance described for aneurysmal bone cysts, what color would the tissue most likely be?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 11.12 a, b state that aneurysmal bone cyst tissue can range in color from brownish to more hemorrhagic. Fig. 11.13 further describes it as usually friable and brownish-red. Main Distractor: Option A (White and cartilaginous) describes tissue more typical of cartilaginous tumors, not ABC.
Question 34
A biopsy is performed on a lytic lesion in the spine of a 10-year-old boy. The pathologist describes blood-filled cystic spaces with lining and the presence of giant cells. Which of the following histological features is characteristic of an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.14 a, b and its description explicitly state that photomicrographs show blood-filled cystic spaces with lining, and giant cells are often present, which are hallmark histological features of an aneurysmal bone cyst. Main Distractor: Option E (Mature lamellar bone with fibrous stroma) describes fibrous dysplasia or other benign bone lesions, not ABC.
Question 34
A 15-year-old female undergoes curettage for a large aneurysmal bone cyst in her distal radius. She is concerned about the possibility of the lesion returning. What is the reported recurrence rate following curettage for aneurysmal bone cysts?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context explicitly states that aneurysmal bone cysts tend to recur in a high percentage following curettage (20–50%). Main Distractor: Option C (10-20%) is lower than the stated range, underestimating the significant recurrence risk.
Question 34
A 13-year-old boy presents with a lytic lesion in his proximal femur. MRI reveals fluid levels within the lesion, and a previous biopsy showed features consistent with fibrous dysplasia. Which of the following conditions is known to develop a secondary aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 11.11 a, b specifically mention that aneurysmal bone cysts can occur as secondary phenomena in other conditions such as giant cell tumor, fibrous dysplasia, and chondroblastoma. Main Distractor: Option A (Osteosarcoma) is a malignant tumor and is not listed as a condition that develops secondary ABC.
Question 34
A 17-year-old female presents with pain and swelling in her distal tibia. Radiographs show an expansile lytic lesion. An MRI is ordered to further characterize the lesion. What specific MRI finding is often associated with aneurysmal bone cysts, particularly secondary ones?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.11 b explicitly states that "The MRI shows the fluid levels of the components of secondary aneurysmal bone cyst." Fluid levels are a classic MRI finding for ABCs. Main Distractor: Option A (Solid enhancement with contrast) is a non-specific finding and not the most characteristic for ABC compared to fluid levels.
Question 34
A 9-year-old boy is diagnosed with an aneurysmal bone cyst in his calcaneus. His parents are concerned about the nature of the lesion. How is an aneurysmal bone cyst best characterized biologically?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context defines aneurysmal bone cysts as "benign, locally aggressive cystic lesions." Main Distractor: Option B (Benign, non-aggressive) is incorrect because ABCs are specifically described as "locally aggressive," which implies a potential for local destruction and recurrence.
Question 34
A 16-year-old patient presents with symptoms suggestive of an aneurysmal bone cyst. When discussing the epidemiology of this condition, which gender is slightly more commonly affected?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context states that aneurysmal bone cysts "are slightly more common in women." Main Distractor: Option A (Males) is incorrect as the text specifies a slight female predilection.
Question 34
During an intraoperative procedure for an aneurysmal bone cyst in the lower extremity of a 14-year-old, the surgeon notes specific features within the lesion. What characteristic intraoperative finding is typically observed in an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 11.15 b, an intraoperative photo, explicitly shows "multiple septations and blood-filled spaces," which is a classic finding for ABC. Fig. 11.12 also notes intralesional septations. Main Distractor: Option D (Clear, serous fluid without septations) describes a simple bone cyst, which is distinct from an ABC.
Question 34
A 10-year-old girl undergoes biopsy for an expansile lesion in her proximal tibia. Histological examination reveals blood-filled cystic spaces lined by fibrous tissue, with numerous multinucleated giant cells scattered throughout the stroma. The presence of giant cells in this context necessitates differentiation from which other bone lesion often associated with secondary ABC?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context states that aneurysmal bone cysts can occur as secondary phenomena in conditions such as giant cell tumor. Both ABC and giant cell tumor contain giant cells, making differentiation important, especially when considering secondary ABC. Main Distractor: Option B (Enchondroma) is a cartilaginous tumor and typically does not feature prominent giant cells in a way that would cause confusion with ABC or GCT.
Question 34
A 12-year-old boy presents with recurrent pain and swelling at the site of a previously treated aneurysmal bone cyst in his femur. He has undergone two prior curettages. What does the presence of multiple surgical scars, as shown in the clinical image, suggest about the management of ABCs?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.15 a shows "scars from prior surgery for recurrences," and the text states a high recurrence rate (20-50%) following curettage. This strongly implies that ABCs often recur and may require repeat surgical interventions. Main Distractor: Option B (Single curettage is usually curative for ABCs) directly contradicts the information provided about high recurrence rates and the image showing scars from prior recurrences.
Question 34
A 13-year-old girl complains of pain in her wrist for several months. On physical examination, the orthopaedic surgeon notes swelling and tenderness over the distal radius, and the patient has difficulty with wrist flexion. Which of the following physical findings is consistent with an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context states that "Physical findings include local tenderness, swelling, and limited range of motion" for aneurysmal bone cysts. Main Distractor: Option A (Warmth and erythema without tenderness) is less specific and doesn't include tenderness, which is a key finding.
Question 34
A 15-year-old male presents with a lytic lesion in his proximal femur, which on MRI shows fluid levels. This lesion is identified as a secondary aneurysmal bone cyst arising from fibrous dysplasia. What is a key characteristic of the underlying fibrous dysplasia that can lead to secondary ABC formation?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that fibrous dysplasia can develop secondary aneurysmal bone cyst. Fibrous dysplasia itself is a benign bone lesion, and the development of a secondary ABC implies a process of cystic degeneration or hemorrhage within the primary lesion. Main Distractor: Option A (Its highly malignant potential) is incorrect; fibrous dysplasia is a benign condition, not malignant.
Question 34
A 10-year-old girl is diagnosed with an aneurysmal bone cyst. Her physician is reviewing the possibility of it being a secondary lesion. Which of the following conditions is NOT listed as one that can develop a secondary aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context lists giant cell tumor, fibrous dysplasia, and chondroblastoma as conditions that can develop secondary aneurysmal bone cysts. Osteosarcoma is not mentioned in this list. Main Distractor: Option E (None of the above) is incorrect because Osteosarcoma is indeed not listed as an associated condition for secondary ABC.
Question 34
A 14-year-old boy undergoes a biopsy of an expansile lesion in his proximal tibia. The pathologist notes that the lesion consists of numerous cystic spaces. What is the primary content typically found within these cystic spaces in an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: The term "aneurysmal" implies vascular involvement, and the histological description (Fig. 11.14) and gross appearance (Fig. 11.15) explicitly mention "blood-filled cystic spaces" and "hemorrhagic" tissue. Main Distractor: Option A (Serous fluid) is characteristic of a simple bone cyst, not an aneurysmal bone cyst.
Question 34
During surgical exploration of an aneurysmal bone cyst in a 17-year-old patient, the surgeon attempts to debride the lesion. What is the typical consistency of the tissue encountered within an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.13 explicitly states, "Tissue from within an aneurysmal bone cyst is usually friable and brownish-red in color." Main Distractor: Option A (Hard and sclerotic) describes dense bone or certain benign tumors like osteomas, which is contrary to the cystic, hemorrhagic nature of ABC.
Question 34
A 12-year-old female presents with a lytic lesion in her proximal humerus. MRI demonstrates multiple fluid-fluid levels within the lesion. This specific MRI finding is highly suggestive of what characteristic feature of an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: Fluid levels on MRI (as shown in Fig. 11.11 b) are a classic sign of aneurysmal bone cysts, representing the layering of blood products (serum and red blood cells) within the cystic spaces due to gravity. Main Distractor: Option A (Intralesional calcification) is not the primary interpretation of fluid levels; calcification would appear as signal void or specific patterns on different sequences.
Question 34
A 16-year-old male undergoes open biopsy for an expansile lesion in his distal femur. Upon opening the lesion, the surgeon observes multiple internal divisions within the cystic cavity. What is this gross pathological feature called?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 11.12 a, b and Fig. 11.15 b both explicitly mention and show "intralesional septations" and "multiple septations" as a characteristic gross finding of aneurysmal bone cysts. Main Distractor: Option A (Trabeculation) refers to the internal bony architecture, which is different from the fibrous divisions within the cystic spaces of an ABC.
Question 34
A 10-year-old girl is diagnosed with an aneurysmal bone cyst in her sacrum. Her parents are concerned about the potential for the lesion to spread or cause significant damage. Based on the provided description, what is the most accurate characterization of the biological behavior of an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context clearly states, "Aneurysmal bone cysts are benign, locally aggressive cystic lesions." This accurately describes their biological behavior. Main Distractor: Option C (Benign and self-limiting) is incorrect because while benign, they are "locally aggressive" and have a high recurrence rate, indicating they are not typically self-limiting without intervention.
Question 35
A 14-year-old female presents with a 3-month history of progressive pain and swelling in her distal femur. Physical examination reveals local tenderness and limited range of motion. Radiographs show an expansile lytic lesion in the metaphysis. Given the typical demographic for aneurysmal bone cyst, what is the most common age range for presentation?
View Answer & Explanation
Correct Answer: B
Rationale: Aneurysmal bone cysts usually occur in the first two decades of life. This demographic information is a key characteristic of the lesion. Main Distractor: Option A (First decade of life) is too narrow; while it can occur, the text specifies "first two decades," making it a less complete answer.
Question 36
A 12-year-old male presents with a 6-week history of worsening pain in his proximal humerus. He denies any trauma. On examination, there is palpable swelling and tenderness over the affected area. Radiographs demonstrate an expansile, lytic lesion. What is the most common presenting symptom for an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: Patients with aneurysmal bone cysts typically present with pain and swelling of the involved area, as stated in the clinical context. Main Distractor: Option A (Pathologic fracture) can occur but is not described as the *typical* or *most common* presenting symptom in the provided text, which emphasizes pain and swelling.
Question 37
During surgical curettage of an expansile lesion in the tibia of a 16-year-old female, the surgeon encounters friable tissue within cystic spaces. Based on the gross appearance described for aneurysmal bone cysts, what color would the tissue most likely be?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 11.12 a, b state that aneurysmal bone cyst tissue can range in color from brownish to more hemorrhagic. Fig. 11.13 further describes it as usually friable and brownish-red. Main Distractor: Option A (White and cartilaginous) describes tissue more typical of cartilaginous tumors, not ABC.
Question 38
A biopsy is performed on a lytic lesion in the spine of a 10-year-old boy. The pathologist describes blood-filled cystic spaces with lining and the presence of giant cells. Which of the following histological features is characteristic of an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.14 a, b and its description explicitly state that photomicrographs show blood-filled cystic spaces with lining, and giant cells are often present, which are hallmark histological features of an aneurysmal bone cyst. Main Distractor: Option E (Mature lamellar bone with fibrous stroma) describes fibrous dysplasia or other benign bone lesions, not ABC.
Question 39
A 15-year-old female undergoes curettage for a large aneurysmal bone cyst in her distal radius. She is concerned about the possibility of the lesion returning. What is the reported recurrence rate following curettage for aneurysmal bone cysts?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context explicitly states that aneurysmal bone cysts tend to recur in a high percentage following curettage (20–50%). Main Distractor: Option C (10-20%) is lower than the stated range, underestimating the significant recurrence risk.
Question 40
A 13-year-old boy presents with a lytic lesion in his proximal femur. MRI reveals fluid levels within the lesion, and a previous biopsy showed features consistent with fibrous dysplasia. Which of the following conditions is known to develop a secondary aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context and Fig. 11.11 a, b specifically mention that aneurysmal bone cysts can occur as secondary phenomena in other conditions such as giant cell tumor, fibrous dysplasia, and chondroblastoma. Main Distractor: Option A (Osteosarcoma) is a malignant tumor and is not listed as a condition that develops secondary ABC.
Question 41
A 17-year-old female presents with pain and swelling in her distal tibia. Radiographs show an expansile lytic lesion. An MRI is ordered to further characterize the lesion. What specific MRI finding is often associated with aneurysmal bone cysts, particularly secondary ones?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.11 b explicitly states that "The MRI shows the fluid levels of the components of secondary aneurysmal bone cyst." Fluid levels are a classic MRI finding for ABCs. Main Distractor: Option A (Solid enhancement with contrast) is a non-specific finding and not the most characteristic for ABC compared to fluid levels.
Question 42
A 9-year-old boy is diagnosed with an aneurysmal bone cyst in his calcaneus. His parents are concerned about the nature of the lesion. How is an aneurysmal bone cyst best characterized biologically?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context defines aneurysmal bone cysts as "benign, locally aggressive cystic lesions." Main Distractor: Option B (Benign, non-aggressive) is incorrect because ABCs are specifically described as "locally aggressive," which implies a potential for local destruction and recurrence.
Question 43
A 16-year-old patient presents with symptoms suggestive of an aneurysmal bone cyst. When discussing the epidemiology of this condition, which gender is slightly more commonly affected?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context states that aneurysmal bone cysts "are slightly more common in women." Main Distractor: Option A (Males) is incorrect as the text specifies a slight female predilection.
Question 44
During an intraoperative procedure for an aneurysmal bone cyst in the lower extremity of a 14-year-old, the surgeon notes specific features within the lesion. What characteristic intraoperative finding is typically observed in an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 11.15 b, an intraoperative photo, explicitly shows "multiple septations and blood-filled spaces," which is a classic finding for ABC. Fig. 11.12 also notes intralesional septations. Main Distractor: Option D (Clear, serous fluid without septations) describes a simple bone cyst, which is distinct from an ABC.
Question 45
A 10-year-old girl undergoes biopsy for an expansile lesion in her proximal tibia. Histological examination reveals blood-filled cystic spaces lined by fibrous tissue, with numerous multinucleated giant cells scattered throughout the stroma. The presence of giant cells in this context necessitates differentiation from which other bone lesion often associated with secondary ABC?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context states that aneurysmal bone cysts can occur as secondary phenomena in conditions such as giant cell tumor. Both ABC and giant cell tumor contain giant cells, making differentiation important, especially when considering secondary ABC. Main Distractor: Option B (Enchondroma) is a cartilaginous tumor and typically does not feature prominent giant cells in a way that would cause confusion with ABC or GCT.
Question 46
A 12-year-old boy presents with recurrent pain and swelling at the site of a previously treated aneurysmal bone cyst in his femur. He has undergone two prior curettages. What does the presence of multiple surgical scars, as shown in the clinical image, suggest about the management of ABCs?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.15 a shows "scars from prior surgery for recurrences," and the text states a high recurrence rate (20-50%) following curettage. This strongly implies that ABCs often recur and may require repeat surgical interventions. Main Distractor: Option B (Single curettage is usually curative for ABCs) directly contradicts the information provided about high recurrence rates and the image showing scars from prior recurrences.
Question 47
A 13-year-old girl complains of pain in her wrist for several months. On physical examination, the orthopaedic surgeon notes swelling and tenderness over the distal radius, and the patient has difficulty with wrist flexion. Which of the following physical findings is consistent with an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context states that "Physical findings include local tenderness, swelling, and limited range of motion" for aneurysmal bone cysts. Main Distractor: Option A (Warmth and erythema without tenderness) is less specific and doesn't include tenderness, which is a key finding.
Question 48
A 15-year-old male presents with a lytic lesion in his proximal femur, which on MRI shows fluid levels. This lesion is identified as a secondary aneurysmal bone cyst arising from fibrous dysplasia. What is a key characteristic of the underlying fibrous dysplasia that can lead to secondary ABC formation?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that fibrous dysplasia can develop secondary aneurysmal bone cyst. Fibrous dysplasia itself is a benign bone lesion, and the development of a secondary ABC implies a process of cystic degeneration or hemorrhage within the primary lesion. Main Distractor: Option A (Its highly malignant potential) is incorrect; fibrous dysplasia is a benign condition, not malignant.
Question 49
A 10-year-old girl is diagnosed with an aneurysmal bone cyst. Her physician is reviewing the possibility of it being a secondary lesion. Which of the following conditions is NOT listed as one that can develop a secondary aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context lists giant cell tumor, fibrous dysplasia, and chondroblastoma as conditions that can develop secondary aneurysmal bone cysts. Osteosarcoma is not mentioned in this list. Main Distractor: Option E (None of the above) is incorrect because Osteosarcoma is indeed not listed as an associated condition for secondary ABC.
Question 50
A 14-year-old boy undergoes a biopsy of an expansile lesion in his proximal tibia. The pathologist notes that the lesion consists of numerous cystic spaces. What is the primary content typically found within these cystic spaces in an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: The term "aneurysmal" implies vascular involvement, and the histological description (Fig. 11.14) and gross appearance (Fig. 11.15) explicitly mention "blood-filled cystic spaces" and "hemorrhagic" tissue. Main Distractor: Option A (Serous fluid) is characteristic of a simple bone cyst, not an aneurysmal bone cyst.
Question 51
During surgical exploration of an aneurysmal bone cyst in a 17-year-old patient, the surgeon attempts to debride the lesion. What is the typical consistency of the tissue encountered within an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 11.13 explicitly states, "Tissue from within an aneurysmal bone cyst is usually friable and brownish-red in color." Main Distractor: Option A (Hard and sclerotic) describes dense bone or certain benign tumors like osteomas, which is contrary to the cystic, hemorrhagic nature of ABC.
Question 52
A 12-year-old female presents with a lytic lesion in her proximal humerus. MRI demonstrates multiple fluid-fluid levels within the lesion. This specific MRI finding is highly suggestive of what characteristic feature of an aneurysmal bone cyst?
View Answer & Explanation
Correct Answer: C
Rationale: Fluid levels on MRI (as shown in Fig. 11.11 b) are a classic sign of aneurysmal bone cysts, representing the layering of blood products (serum and red blood cells) within the cystic spaces due to gravity. Main Distractor: Option A (Intralesional calcification) is not the primary interpretation of fluid levels; calcification would appear as signal void or specific patterns on different sequences.
Question 53
A 16-year-old male undergoes open biopsy for an expansile lesion in his distal femur. Upon opening the lesion, the surgeon observes multiple internal divisions within the cystic cavity. What is this gross pathological feature called?
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 11.12 a, b and Fig. 11.15 b both explicitly mention and show "intralesional septations" and "multiple septations" as a characteristic gross finding of aneurysmal bone cysts. Main Distractor: Option A (Trabeculation) refers to the internal bony architecture, which is different from the fibrous divisions within the cystic spaces of an ABC.
Question 54
A 7-year-old boy presents with bilateral knee pain, a waddling gait, and decreased range of motion in his hips and knees. Radiographs reveal irregular and fragmented epiphyses in the hips, knees, and ankles, with flat articular surfaces. The metaphyses appear normal, and there is mild shortening of the tubular bones. His height is within the lower range of normal for his age, with normal body proportions.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of lower extremity joint pain, limping, decreased range of motion, and the radiographic findings of irregular, fragmented epiphyses, flat articular surfaces, normal metaphyses, and mild shortening of tubular bones are classic for Multiple Epiphyseal Dysplasia (MED). Achondroplasia typically presents with disproportionate dwarfism and abnormal metaphyses. Spondyloepiphyseal dysplasia primarily affects the spine and epiphyses, but the "normal metaphyses" and "mild shortening of tubular bones" are more characteristic of MED. Pseudoachondroplasia also has normal metaphyses but typically presents with more severe short stature and ligamentous laxity.
Question 55
A 10-year-old girl is diagnosed with Multiple Epiphyseal Dysplasia after presenting with chronic hip and knee pain. Her parents are concerned about the risk of recurrence in future children and the genetic implications for her siblings. Which of the following is the most common mode of inheritance for this condition?
View Answer & Explanation
Correct Answer: C
Rationale: Multiple Epiphyseal Dysplasia (MED) is usually transmitted in an autosomal dominant manner. While autosomal recessive transmission has also been reported, the autosomal dominant form is the most common. Understanding the inheritance pattern is crucial for genetic counseling and family planning.
Question 56
A 5-year-old boy presents with a history of a waddling gait and mild short stature. Radiographs show widespread epiphyseal irregularities and fragmentation. The underlying pathological disturbance in Multiple Epiphyseal Dysplasia primarily involves which of the following processes?
View Answer & Explanation
Correct Answer: B
Rationale: Multiple Epiphyseal Dysplasia (MED) is characterized by the disturbance of enchondral ossification involving numerous epiphyses. Enchondral ossification is the process by which most bones, especially long bones, are formed, involving cartilage templates. Defective intramembranous ossification is characteristic of conditions like cleidocranial dysplasia, not MED.
Question 57
A 9-year-old boy with a known diagnosis of Multiple Epiphyseal Dysplasia presents for a routine follow-up. His primary complaints are joint pain and limping. Based on the typical presentation of MED, which group of joints is most dominantly affected?
View Answer & Explanation
Correct Answer: B
Rationale: In Multiple Epiphyseal Dysplasia (MED), the lower extremity joints are most commonly affected, with hips, knees, and ankles being dominantly involved. This explains the common complaints of lower extremity joint pain and limping. While upper extremities can be involved, it's typically to a lesser or more variable extent.
Question 58
A 6-year-old girl presents with bilateral hip pain and a limping gait. Radiographs of her pelvis and lower extremities are obtained. Which of the following radiographic findings is most characteristic of Multiple Epiphyseal Dysplasia?
View Answer & Explanation
Correct Answer: B
Rationale: The hallmark radiographic findings in Multiple Epiphyseal Dysplasia (MED) are irregular, fragmented epiphyses and flat articular surfaces. This directly reflects the disturbance in enchondral ossification of the epiphyses. Sclerotic metaphyses are not typical, and normal epiphyses would rule out MED. Vertebral plana is seen in conditions like Scheuermann's disease or some mucopolysaccharidoses, and generalized osteopenia suggests other metabolic bone diseases.
Question 59
A 12-year-old boy with a family history of Multiple Epiphyseal Dysplasia undergoes radiographic evaluation. His radiographs show typical epiphyseal abnormalities in his hips and knees. When evaluating the long bones, what is the expected appearance of the metaphyses in MED?
View Answer & Explanation
Correct Answer: C
Rationale: A key distinguishing feature of Multiple Epiphyseal Dysplasia (MED) is the presence of normal metaphyses, despite the significant involvement of the epiphyses. This helps differentiate it from other skeletal dysplasias where metaphyseal abnormalities are prominent, such as achondroplasia (widened/splayed) or rickets (cupped/frayed).
Question 60
A 4-year-old girl is suspected of having Multiple Epiphyseal Dysplasia due to early onset joint pain and a waddling gait. Her parents are concerned about her growth. What is the typical presentation regarding height and body proportions in patients with MED?
View Answer & Explanation
Correct Answer: B
Rationale: Patients with Multiple Epiphyseal Dysplasia (MED) typically present with normal or moderately short height, but importantly, they maintain normal body proportions. This contrasts with conditions like achondroplasia (disproportionate dwarfism with short limbs) or spondyloepiphyseal dysplasia (short trunk dwarfism).
Question 61
A 15-year-old male presents with chronic knee pain and early degenerative changes on radiographs, which also show fragmented epiphyses and normal metaphyses. Given these findings, which of the following conditions would be the most important to differentiate from Multiple Epiphyseal Dysplasia, particularly considering the normal metaphyses?
View Answer & Explanation
Correct Answer: C
Rationale: Pseudoachondroplasia is a key differential diagnosis for Multiple Epiphyseal Dysplasia (MED) because both conditions present with normal metaphyses and epiphyseal abnormalities. However, pseudoachondroplasia typically involves more severe short stature, ligamentous laxity, and often more pronounced metaphyseal flaring, despite being "normal" in the sense of not having the specific changes of achondroplasia or rickets. Achondroplasia and Rickets both have distinct metaphyseal abnormalities. Morquio Syndrome has severe spondyloepiphyseal dysplasia and systemic features. Osteogenesis Imperfecta is a disorder of collagen synthesis leading to brittle bones.
Question 62
A 7-year-old boy diagnosed with Multiple Epiphyseal Dysplasia is noted to have hand deformities during a physical examination. Radiographs of his hands are obtained.
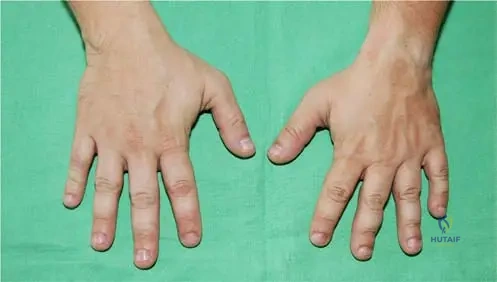
Based on the provided image (Fig. 1.4) and the typical presentation of MED, what is the characteristic finding in the fingers?
View Answer & Explanation
Correct Answer: B
Rationale: The provided image (Fig. 1.4) clearly shows that the fingers are equally shortened, which is a characteristic finding in the upper extremity involvement of Multiple Epiphyseal Dysplasia. While upper extremity involvement can vary, this specific pattern of shortening is noted. Other options describe findings not typical of MED or are contradictory to the image.
Question 63
A 10-year-old girl with Multiple Epiphyseal Dysplasia presents with foot pain and difficulty wearing shoes. Radiographs of her feet are obtained.

Based on the provided image (Fig. 1.5) and the typical presentation of MED, what is the characteristic finding in the toes?
View Answer & Explanation
Correct Answer: C
Rationale: The provided image (Fig. 1.5) demonstrates that the toes are variably shortened, which is a characteristic finding in the lower extremity involvement of Multiple Epiphyseal Dysplasia. This variability contrasts with the more uniform shortening often seen in the fingers. Uniform elongation, absence of phalanges, or severe hallux valgus are not typical features of MED.
Question 64
A 13-year-old boy with Multiple Epiphyseal Dysplasia complains of chronic anterior knee pain, especially with activity. A lateral radiograph of his knee is obtained.

Based on the provided image (Fig. 1.3) and the clinical context of MED, what specific radiographic finding is observed in the patella?
View Answer & Explanation
Correct Answer: C
Rationale: The provided image (Fig. 1.3) specifically highlights "fragmentation and moderate deformity of the patella" in a knee joint affected by Multiple Epiphyseal Dysplasia. This is a common manifestation of the epiphyseal involvement in the knee. Patella alta or baja, or aplasia, are not the characteristic findings described or shown for MED in this context.
Question 65
A 6-year-old child is brought to the orthopedic clinic by parents who report that the child has been experiencing increasing difficulty with walking and occasional pain in the lower extremities. They also note a subtle change in gait. What is the most common initial complaint that leads to the diagnosis of Multiple Epiphyseal Dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states that "Usually lower extremity joint pain with decreased range of motions and limping are the main complaints" in Multiple Epiphyseal Dysplasia. This is due to the dominant involvement of hips, knees, and ankles. Other options are not typical primary presenting complaints for MED.
Question 66
A 3-year-old presents with a waddling gait and mild bilateral hip pain. Radiographs show delayed and irregular ossification of the femoral heads and acetabular dysplasia. The metaphyses are normal. Given the nature of Multiple Epiphyseal Dysplasia, at what age range are symptoms most likely to become apparent and lead to diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: While the exact age of presentation can vary, symptoms of Multiple Epiphyseal Dysplasia, such as joint pain, limping, and decreased range of motion, typically become apparent in early childhood (2-10 years) as children become more active and the epiphyseal abnormalities become more pronounced. The vignette describes a 3-year-old, fitting this range. Infancy might be too early for significant symptoms, and adolescence/adulthood would be later stages of presentation or complications.
Question 67
A 5-year-old boy presents with short stature, but his parents note that his trunk and limbs appear to be in proportion. He has a waddling gait and bilateral hip pain. Radiographs show irregular epiphyseal ossification and normal metaphyses. Which of the following features helps distinguish Multiple Epiphyseal Dysplasia from Achondroplasia?
View Answer & Explanation
Correct Answer: B
Rationale: A key distinguishing feature of Multiple Epiphyseal Dysplasia (MED) from Achondroplasia is that MED presents with normal or moderately short height but with normal body proportions. Achondroplasia, in contrast, is characterized by disproportionate dwarfism with rhizomelic (proximal) limb shortening. Both can have joint pain, autosomal dominant inheritance (though achondroplasia is almost always de novo), and shortening of tubular bones, and lower extremity involvement.
Question 68
A 25-year-old woman with a history of Multiple Epiphyseal Dysplasia since childhood presents with severe, chronic hip and knee pain that significantly impacts her daily activities. Radiographs show advanced joint space narrowing, subchondral sclerosis, and osteophyte formation in both hips and knees. This clinical scenario is a common long-term complication of MED due to which underlying issue?
View Answer & Explanation
Correct Answer: C
Rationale: The irregular, fragmented epiphyses and flat articular surfaces characteristic of Multiple Epiphyseal Dysplasia lead to abnormal joint mechanics and premature wear and tear on the cartilage. This predisposes individuals to early onset osteoarthritis, often requiring joint replacement surgery in adulthood. The radiographic findings described (joint space narrowing, sclerosis, osteophytes) are classic for osteoarthritis. While other complications can occur, early osteoarthritis is the most common and debilitating long-term issue.
Question 69
A 4-year-old boy is diagnosed with Multiple Epiphyseal Dysplasia. His parents ask about the treatment options for his condition. What is the general principle of management for MED?
View Answer & Explanation
Correct Answer: C
Rationale: There is no cure for Multiple Epiphyseal Dysplasia (MED). Management is primarily symptomatic and supportive, focusing on pain relief, maintaining joint function, and addressing specific deformities as they arise. Surgical interventions, such as osteotomies or joint replacements, are reserved for severe pain, significant functional limitations, or progressive deformities. Gene therapy is not currently available. Aggressive early surgery is generally not indicated, and growth hormone therapy or dietary modifications are not primary treatments for MED.
Question 70
A 14-year-old girl with Multiple Epiphyseal Dysplasia presents with increasing hip pain and a Trendelenburg gait. Radiographs of her hips show flattened and irregular femoral heads, with widening of the femoral neck and shallow acetabula. These findings are consistent with the epiphyseal involvement in MED, which often leads to what specific hip deformity?
View Answer & Explanation
Correct Answer: C
Rationale: The irregular and fragmented epiphyses in the hip, along with flat articular surfaces, commonly lead to deformities such as coxa magna (enlarged femoral head) and coxa plana (flattened femoral head) in Multiple Epiphyseal Dysplasia. These deformities contribute to early osteoarthritis and pain. While SCFE, Perthes, DDH, and FAI are hip pathologies, the description of flattened and irregular femoral heads with widening of the femoral neck is most consistent with the characteristic epiphyseal dysplasia leading to coxa magna/plana.
Question 71
A 8-year-old boy is diagnosed with Multiple Epiphyseal Dysplasia. His parents are concerned about his overall growth. While his height is moderately short, his body proportions are normal. What is the typical radiographic finding regarding the length of the tubular bones in MED?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states that "mild shortening of the tubular bones can be observed" in Multiple Epiphyseal Dysplasia. This contributes to the moderately short stature seen in these patients, while still maintaining normal body proportions. Severe shortening with bowing is more characteristic of conditions like achondroplasia or rickets.
Question 72
A 6-year-old girl presents with chronic bilateral knee pain and a waddling gait. Radiographs show irregular and fragmented epiphyses in her hips and knees, with normal metaphyses. Her parents are considering having more children and want to understand the genetic risk. What is the primary indication for genetic testing in this family?
View Answer & Explanation
Correct Answer: D
Rationale: While genetic testing can confirm the diagnosis (A), its primary indication in the context of family planning and counseling for an autosomal dominant condition like Multiple Epiphyseal Dysplasia is to identify affected individuals or unaffected carriers (if an autosomal recessive form is suspected in other contexts, though less common for MED) to assess recurrence risk for future pregnancies. It is less about predicting severity or guiding surgical decisions, and not related to growth hormone therapy eligibility.
Question 73
A 9-year-old boy with Multiple Epiphyseal Dysplasia is followed longitudinally. Over several years, his joint pain and stiffness have progressively worsened, particularly in his hips and knees. This progressive nature of joint symptoms in MED is primarily due to:
View Answer & Explanation
Correct Answer: C
Rationale: The progressive worsening of joint symptoms in Multiple Epiphyseal Dysplasia is a direct consequence of the underlying disturbance in enchondral ossification, which leads to abnormally formed and irregular epiphyses and flat articular surfaces. This abnormal joint architecture results in premature wear and tear, and degeneration of the articular cartilage, culminating in early-onset osteoarthritis. It is not due to continuous growth plate fusion (which is a normal process), metabolic waste accumulation, increased bone density, or a systemic inflammatory response.
Question 74
A 7-year-old boy presents with chronic bilateral knee pain and a noticeable limp. Physical examination reveals decreased range of motion in both knees. Radiographs of the knee joints are obtained.
View Answer & Explanation
Correct Answer: B
Rationale: The provided image (Fig. 1.3) and the clinical context for Multiple Epiphyseal Dysplasia (MED) specifically describe "fragmentation and moderate deformity of the patella" in a normally developed knee joint. This is a characteristic radiographic finding in MED. The main distractor, C) Metaphyseal flaring, is incorrect because MED is characterized by normal metaphyses, distinguishing it from metaphyseal dysplasias.
Question 75
A 9-year-old girl is diagnosed with Multiple Epiphyseal Dysplasia after presenting with hip and knee pain and radiographic findings of irregular epiphyses. Her father and paternal grandfather also have a history of similar joint issues.
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states that Multiple Epiphyseal Dysplasia (MED) is "usually transmitted in an autosomal dominant manner." The family history described (father and grandfather affected) is consistent with an autosomal dominant inheritance pattern. While A) Autosomal recessive transmission has also been reported, it is not the usual or most common mode of inheritance, making it the main distractor.
Question 76
An 8-year-old boy presents with chronic joint pain and limping. Radiographs reveal irregular and fragmented epiphyses in multiple joints, with normal metaphyses. Genetic testing confirms a diagnosis of Multiple Epiphyseal Dysplasia.
View Answer & Explanation
Correct Answer: B
Rationale: The teaching case explicitly states that Multiple Epiphyseal Dysplasia (MED) is "characterized by the disturbance of enchondral ossification involving numerous epiphyses." Enchondral ossification is the process by which most bones, especially long bones, form from cartilage models. A) Intramembranous ossification is the process by which flat bones (like the skull) form directly from mesenchymal tissue, and is not the primary process disturbed in MED, making it the main distractor.
Question 77
A 6-year-old girl is evaluated for short stature and joint pain. Radiographs show irregular and flattened epiphyses in her hips and knees. Her overall height is moderately short, but her body proportions are normal.
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case explicitly states that in Multiple Epiphyseal Dysplasia (MED), "normal metaphyses" are observed. This is a key distinguishing feature from other skeletal dysplasias. A) Epiphyseal morphology is incorrect as the epiphyses are described as "irregular, fragmented," making it a primary affected area and a strong distractor.
Question 78
An 8-year-old boy presents to the clinic with a 6-month history of worsening pain in his hips and knees, particularly after physical activity. His parents also note that he has started limping more frequently.
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case states, "Usually lower extremity joint pain with decreased range of motions and limping are the main complaints." This directly aligns with the patient's presentation. A) Upper extremity weakness is incorrect. While upper extremity involvement can occur, it is described as deformities, not typically weakness, and not the *main* complaint, making it a plausible distractor.
Question 79
A 10-year-old girl with a confirmed diagnosis of Multiple Epiphyseal Dysplasia reports pain and stiffness. On examination, she has limited movement in her hips, knees, and ankles. Radiographs show characteristic epiphyseal changes in these areas.
View Answer & Explanation
Correct Answer: A
Rationale: The teaching case explicitly states, "Dominantly hips, knees, and ankles are affected" in patients with Multiple Epiphyseal Dysplasia. B) Shoulders and elbows are upper extremity joints. While upper extremity involvement can occur, the question asks for *dominantly* affected lower extremity joints, making this a less accurate choice and a distractor.
Question 80
A 12-year-old boy with Multiple Epiphyseal Dysplasia presents for a follow-up. While his primary complaints are in his lower extremities, his parents also express concern about the appearance of his hands, which show some mild shortening of the fingers.
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case states, "Upper extremity involvement may differ from minimal to severe with significant deformities." This indicates a wide spectrum of presentation in the upper limbs. A) Always severe with contractures is incorrect because the involvement can be minimal, making it a strong distractor.
Question 81
A 7-year-old girl is referred for evaluation of her height. Her parents are concerned she is shorter than her peers. On physical examination, her limbs appear proportionate to her trunk, and she has no obvious dysmorphic features.
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case mentions, "Normal or moderately short height with normal proportions" as a characteristic of patients with Multiple Epiphyseal Dysplasia. This aligns with the vignette's description. A) Severely short stature with disproportionate limbs is characteristic of other skeletal dysplasias like achondroplasia, not MED, making it a key distractor.
Question 82
A 9-year-old boy with Multiple Epiphyseal Dysplasia presents with joint pain. During the physical examination, the clinician observes that his fingers appear shorter than expected for his age.
View Answer & Explanation
Correct Answer: B
Rationale: The provided image (Fig. 1.4) is captioned "Fingers are equally shortened." This is a specific clinical finding associated with Multiple Epiphyseal Dysplasia. A) Variably shortened is incorrect for fingers; this description applies to the toes in MED, making it the main distractor.
Question 83
An 11-year-old girl with Multiple Epiphyseal Dysplasia complains of foot pain and difficulty wearing certain shoes. On examination, her toes appear shorter than average, but not uniformly so.
View Answer & Explanation
Correct Answer: C
Rationale: The provided image (Fig. 1.5) is captioned "Toes are variably shortened." This is a specific clinical finding associated with Multiple Epiphyseal Dysplasia. A) Equally shortened is incorrect for toes; this description applies to the fingers in MED, making it the main distractor.
Question 84
A 6-year-old boy with a history of chronic hip pain undergoes radiography. The images reveal irregular epiphyseal ossification and a distinct alteration in the shape of the joint surfaces.
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case describes characteristic radiographic findings in Multiple Epiphyseal Dysplasia (MED) as "irregular, fragmented epiphyses and flat articular surfaces." A) Deepened articular surfaces is the opposite of what is described and is therefore incorrect, serving as a strong distractor.
Question 85
A 10-year-old girl is diagnosed with Multiple Epiphyseal Dysplasia. Her radiographs show not only epiphyseal abnormalities but also a mild reduction in the length of certain bones in her limbs.
View Answer & Explanation
Correct Answer: E
Rationale: The teaching case states that in Multiple Epiphyseal Dysplasia (MED), "mild shortening of the tubular bones can be observed." Tubular bones include the long bones of the limbs (femur, tibia, fibula, humerus, radius, ulna) and the short bones of the hands and feet (phalanges, metacarpals, metatarsals). A) Flat bones (e.g., skull, scapula) are not typically described as shortened in MED, making it a distractor.
Question 86
A 7-year-old boy presents with a history of progressive difficulty walking and a noticeable alteration in his gait. His parents report that he often complains of discomfort in his legs after playing.
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case explicitly lists "limping" as one of the main complaints in patients with Multiple Epiphyseal Dysplasia, particularly related to lower extremity involvement. A) Muscle atrophy is not a primary complaint of MED, though it could be a secondary consequence of disuse due to pain. However, limping is a direct and common complaint, making muscle atrophy a less accurate choice and a distractor.
Question 87
A 9-year-old girl with Multiple Epiphyseal Dysplasia undergoes a physical examination. The orthopaedic surgeon assesses the mobility of her hip and knee joints, noting a consistent pattern of restriction.
View Answer & Explanation
Correct Answer: C
Rationale: The teaching case states that "decreased range of motions" is one of the main complaints associated with lower extremity joint involvement in Multiple Epiphyseal Dysplasia. A) Joint hypermobility is the opposite of what is described and is therefore incorrect, serving as a strong distractor.
Question 88
A family presents with two children diagnosed with Multiple Epiphyseal Dysplasia. The younger child has mild hip pain and minimal radiographic changes, while the older sibling has severe knee and ankle deformities requiring surgical intervention.
View Answer & Explanation
Correct Answer: D
Rationale: The teaching case explicitly states, "Different levels of deformities may be present in one patient" with Multiple Epiphyseal Dysplasia. This highlights the variable expressivity of the condition, even within the same individual or family. A) Uniform severity of deformities across all affected joints is incorrect, as the case text indicates variability, making it the main distractor.
Question 89
A 5-year-old boy presents with short stature and waddling gait. Radiographs show irregular and fragmented epiphyses, flat articular surfaces, and mild shortening of tubular bones. Crucially, the metaphyses appear normal.
View Answer & Explanation
Correct Answer: A
Rationale: The presence of "normal metaphyses" is a key diagnostic feature of Multiple Epiphyseal Dysplasia (MED) that helps differentiate it from conditions primarily affecting the metaphyses, such as metaphyseal dysplasias (e.g., Schmid type). B) Spondyloepiphyseal dysplasias also affect epiphyses (and the spine), so the distinction based solely on normal metaphyses is less direct compared to metaphyseal dysplasias, making it a less precise distractor in this context.
Question 90
A 45-year-old male with a 10-year history of plaque psoriasis presents with insidious onset of pain and swelling in his right knee, left ankle, and the distal interphalangeal (DIP) joint of his left index finger. He also reports morning stiffness lasting over an hour. Physical examination reveals erythematous, scaly plaques on his elbows and scalp, pitting of several fingernails, and tenderness with effusion in the affected joints. Radiographs show erosions and new bone formation in the left DIP joint.
View Answer & Explanation
Correct Answer: D
Rationale: This patient's presentation with a history of psoriasis, characteristic nail changes (pitting), involvement of DIP joints, asymmetric oligoarthritis, and radiographic findings of erosions and new bone formation is classic for Psoriatic Arthritis. Rheumatoid Arthritis typically spares the DIP joints, is often symmetric, and usually presents with positive Rheumatoid Factor and anti-CCP antibodies. Gout would involve acute, severe pain, often monoarticular, with crystal identification in synovial fluid. Osteoarthritis is degenerative and lacks inflammatory markers and skin/nail findings. Reactive Arthritis usually follows an infection and may involve conjunctivitis or urethritis.
Question 91
A 38-year-old female with a known history of psoriasis presents with a painful, swollen right middle finger that resembles a "sausage." She denies any recent trauma or infection. Her skin psoriasis is well-controlled with topical agents. On examination, the entire digit is diffusely swollen, erythematous, and tender to palpation. Radiographs show soft tissue swelling and early periostitis of the phalanges.
View Answer & Explanation
Correct Answer: C
Rationale: Dactylitis, often referred to as a "sausage digit," is a characteristic feature of psoriatic arthritis and other spondyloarthropathies. It involves inflammation of the entire digit, including the joints, tendons, and soft tissues. Boutonnière and Swan neck deformities are specific joint deformities seen in rheumatoid arthritis. Heberden's nodes are bony enlargements of the DIP joints in osteoarthritis. Podagra refers to acute gout of the first metatarsophalangeal joint.
Question 92
A 52-year-old male presents with chronic pain and stiffness in multiple joints, particularly his hands and feet. He has a long-standing history of skin lesions on his trunk and scalp. On examination, several of his fingernails show small indentations and separation from the nail bed. His joint examination reveals tenderness and swelling in the DIP joints of both hands.
View Answer & Explanation
Correct Answer: C
Rationale: Nail changes such as pitting, onycholysis (separation from the nail bed), and hyperkeratosis are highly characteristic of psoriasis and are present in a significant proportion of patients with psoriatic arthritis. The presence of these nail changes, along with skin lesions and DIP joint involvement, strongly points to Psoriatic Arthritis. While fungal nail infections can cause onycholysis, they typically do not cause pitting and are not associated with systemic joint inflammation. Rheumatoid Arthritis does not typically involve the DIP joints or cause these specific nail changes.
Question 93
A 60-year-old female with severe, long-standing psoriatic arthritis presents with significant deformity and functional impairment of her hands. Radiographs of her hands reveal marked osteolysis of the distal phalanges with telescoping of the digits, giving a characteristic appearance.
View Answer & Explanation
Correct Answer: C
Rationale: The "pencil-in-cup" deformity is a classic and highly specific radiographic finding in psoriatic arthritis, particularly in the severe form known as arthritis mutilans. It results from extensive osteolysis of the distal phalanx (the "pencil") fitting into an eroded, widened base of the middle phalanx (the "cup"). While joint space narrowing and marginal erosions can be seen in PsA, they are not as specific as the pencil-in-cup deformity. Periarticular osteopenia is more characteristic of rheumatoid arthritis.
Question 94
A 48-year-old male with a 15-year history of psoriasis presents with chronic pain and swelling in his right foot. Physical examination demonstrates tenderness along the Achilles tendon insertion and diffuse swelling of the toes. Radiographs of the foot demonstrate fluffy periostitis along the shafts of the metatarsals and phalanges, as well as new bone formation at the Achilles tendon insertion.
Correct Answer: D
Rationale: Psoriatic arthritis is characterized by both erosive changes and new bone formation (osteoproliferation), including periostitis and enthesophytes (new bone formation at tendon/ligament insertions). The fluffy periostitis and new bone formation at the Achilles tendon insertion are highly characteristic of psoriatic arthritis and other spondyloarthropathies. Rheumatoid arthritis typically presents with periarticular osteopenia and marginal erosions, but not significant new bone formation. Gout involves erosions with sclerotic margins and often an overhanging edge. Osteoarthritis is degenerative with osteophytes and joint space narrowing.
Question 95
A 55-year-old male with a history of psoriasis and peripheral arthritis complains of chronic low back pain and stiffness, particularly worse in the morning and improving with activity. He also reports alternating buttock pain. Physical examination reveals limited spinal mobility. Sacroiliac joint compression tests elicit pain. Radiographs of the pelvis show bilateral sacroiliitis with erosions and sclerosis.
View Answer & Explanation
Correct Answer: C
Rationale: The axial involvement in psoriatic arthritis, including sacroiliitis and spondylitis, shares many clinical and radiographic features with Ankylosing Spondylitis (AS). Both conditions are part of the spondyloarthropathy family. The inflammatory back pain pattern (worse in morning, improves with activity) and radiographic sacroiliitis are hallmarks. Rheumatoid arthritis does not typically involve the sacroiliac joints or the axial spine in this manner. DISH involves flowing ossification along the anterior spine but typically spares the sacroiliac joints.
Question 96
A 40-year-old female presents with symmetric polyarthritis affecting her metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints, as well as her wrists and knees. She has significant morning stiffness. Laboratory tests reveal an elevated ESR and CRP. However, her Rheumatoid Factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies are negative. She also reports a history of a chronic skin rash on her elbows and scalp.
View Answer & Explanation
Correct Answer: C
Rationale: While psoriatic arthritis can present with symmetric polyarthritis mimicking rheumatoid arthritis, the combination of negative RF and anti-CCP antibodies (seronegativity) along with a history of psoriasis is a strong indicator for psoriatic arthritis. Most patients with psoriatic arthritis are seronegative for RF and anti-CCP, whereas these are typically positive in rheumatoid arthritis. Elevated inflammatory markers and morning stiffness are common to both conditions. Involvement of MCP and PIP joints can occur in both, though DIP involvement is more specific to PsA.
Question 97
A 62-year-old male with a history of psoriasis presents with acute onset of severe pain, swelling, and erythema in his right great toe. He reports a similar episode in the past that resolved spontaneously. He denies any recent trauma. Physical examination reveals a hot, swollen, exquisitely tender first metatarsophalangeal (MTP) joint. Arthrocentesis is performed, and synovial fluid analysis shows inflammatory cells but no crystals. His serum uric acid level is normal.
View Answer & Explanation
Correct Answer: C
Rationale: Psoriatic arthritis can mimic gout, especially with acute monoarticular flares, dactylitis, or involvement of the foot. The classic presentation of podagra (first MTP joint involvement) is misleading here. The absence of crystals in the
Question 97
A 45-year-old male presents with a 6-month history of pain and swelling in his right index finger DIP joint and left knee. He also reports a scaly rash on his elbows and scalp. Physical examination reveals erythema and silvery scales on the extensor surfaces of his elbows and scalp, along with tenderness and swelling of the right index finger DIP joint and left knee effusion. Radiographs show erosions and new bone formation in the right index finger DIP joint. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of a scaly rash (psoriasis), DIP joint involvement, oligoarthritis (right index finger DIP and left knee), and radiographic evidence of erosions and new bone formation are classic features of psoriatic arthritis. DIP joint involvement is highly characteristic and less common in other arthritides. Main Distractor Rationale: Rheumatoid arthritis (A) typically spares the DIP joints, involves symmetric polyarthritis, and usually presents with positive RF/anti-CCP (not mentioned here, but a key differentiator). Gout (B) presents with acute, severe monoarticular inflammation, often in the MTP joint of the great toe, and is associated with hyperuricemia and crystal findings, which are not described. Osteoarthritis (C) can affect DIP joints but typically lacks inflammatory features like erythema, significant swelling, and the associated skin rash. Reactive arthritis (E) is often preceded by an infection and presents with a triad of arthritis, urethritis, and conjunctivitis, and while it can involve enthesitis and sacroiliitis, the prominent skin psoriasis and DIP involvement make psoriatic arthritis more likely.
Question 97
A 38-year-old female with a known history of psoriasis presents with diffuse swelling and pain involving her entire left middle finger. The finger appears sausage-like, erythematous, and tender to palpation. Radiographs show soft tissue swelling and periostitis of the phalanges of the affected finger. This specific manifestation is best described as:
View Answer & Explanation
Correct Answer: C
Rationale: Dactylitis, often referred to as a "sausage digit," is a characteristic inflammatory manifestation of psoriatic arthritis, involving diffuse swelling of an entire digit (finger or toe) due to inflammation of the joints, tendons, and soft tissues. The radiographic finding of periostitis further supports this diagnosis. Main Distractor Rationale: Tenosynovitis (D) involves inflammation of the tendon sheath, which can contribute to dactylitis but does not describe the entire digit swelling. Boutonnière (A) and swan neck (B) deformities are specific joint deformities, typically seen in rheumatoid arthritis, and do not describe the diffuse swelling of the entire digit. Mallet finger (E) is a deformity caused by injury to the extensor tendon at the DIP joint.
Question 97
A 52-year-old male with psoriatic arthritis complains of changes in his fingernails. On examination, you observe pitting, onycholysis, and subungual hyperkeratosis. These nail changes are most commonly associated with which of the following conditions?
View Answer & Explanation
Correct Answer: C
Rationale: Nail changes such as pitting, onycholysis (separation of the nail from the nail bed), and subungual hyperkeratosis (thickening of the nail bed) are highly characteristic and common manifestations of psoriasis and psoriatic arthritis. They are often present in patients with psoriatic arthritis, even in the absence of extensive skin lesions. Main Distractor Rationale: Onychomycosis (A) can cause nail thickening and discoloration but typically lacks the characteristic pitting and onycholysis seen in psoriasis. Rheumatoid arthritis (B) and Systemic lupus erythematosus (D) are not typically associated with these specific nail changes. Raynaud's phenomenon (E) affects blood flow to the digits and does not cause these structural nail changes.
Question 97
A 60-year-old male with long-standing psoriatic arthritis presents with severe pain and deformity in his right hand. Radiographs of the hand reveal significant erosive changes, particularly in the interphalangeal joints, with a characteristic "pencil-in-cup" appearance in the right 4th DIP joint. This radiographic finding is pathognomonic for:
View Answer & Explanation
Correct Answer: D
Rationale: The "pencil-in-cup" deformity, characterized by resorption of the distal phalanx creating a pointed, "pencil" appearance that fits into an eroded, "cup-shaped" proximal phalanx, is a classic and highly specific radiographic finding for psoriatic arthritis, particularly in the DIP joints. It represents severe erosive changes. Main Distractor Rationale: Rheumatoid arthritis (A) causes erosions but typically spares DIP joints and does not produce this specific deformity. Osteoarthritis (B) is characterized by joint space narrowing, osteophytes, and subchondral sclerosis, not erosions or "pencil-in-cup." Gout (C) can cause erosions with overhanging edges but not the "pencil-in-cup" appearance. Ankylosing spondylitis (E) primarily affects the axial skeleton and entheses, not typically causing this type of peripheral joint destruction.
Question 97
A 48-year-old female presents with symmetric polyarthritis affecting her MCP and PIP joints, morning stiffness lasting over an hour, and fatigue. She has a positive rheumatoid factor (RF) and anti-CCP antibody. However, she also has a history of psoriasis. Which of the following features would most strongly suggest psoriatic arthritis over rheumatoid arthritis in this patient, despite the overlapping symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: While psoriatic arthritis can mimic rheumatoid arthritis with symmetric polyarthritis, morning stiffness, and elevated inflammatory markers, and even rarely positive RF/anti-CCP, the presence of dactylitis (sausage digits) is a highly characteristic and specific feature of psoriatic arthritis that is not typically seen in rheumatoid arthritis. This would be a strong indicator to differentiate between the two conditions in a patient with psoriasis. Main Distractor Rationale: Symmetric joint involvement (A), elevated ESR and CRP (B), and morning stiffness > 60 minutes (D) are common features of both rheumatoid arthritis and polyarticular psoriatic arthritis, making them less useful for differentiation. Positive RF and anti-CCP antibodies (E) are hallmarks of rheumatoid arthritis, and while they can be positive in a small percentage of PsA patients, their presence generally points towards RA. Therefore, dactylitis is the most distinguishing feature among the options provided.
Question 97
A 55-year-old male with psoriatic arthritis reports recent onset of eye redness, pain, and photophobia. Ophthalmic examination reveals anterior uveitis. This extra-articular manifestation is most commonly associated with which subtype of psoriatic arthritis?
Correct Answer: E
Rationale: Anterior uveitis (iritis) is a common extra-articular manifestation of spondyloarthropathies, including psoriatic arthritis, particularly in those with axial involvement (spondylitis) or sacroiliitis. It is less commonly associated with purely peripheral forms of psoriatic arthritis. Main Distractor Rationale: While uveitis can occur in any subtype of psoriatic arthritis, its association is strongest with the axial forms. Predominant DIP involvement (A), oligoarticular arthritis (B), polyarticular arthritis (C), and arthritis mutilans (D) are primarily classifications of peripheral joint involvement and do not carry the same strong association with uveitis as spondylitis.
Question 98
A 45-year-old male presents with a 6-month history of pain and swelling in his right index finger DIP joint and left knee. He also reports a scaly rash on his elbows and scalp. Physical examination reveals erythema and silvery scales on the extensor surfaces of his elbows and scalp, along with tenderness and swelling of the right index finger DIP joint and left knee effusion. Radiographs show erosions and new bone formation in the right index finger DIP joint. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of a scaly rash (psoriasis), DIP joint involvement, oligoarthritis (right index finger DIP and left knee), and radiographic evidence of erosions and new bone formation are classic features of psoriatic arthritis. DIP joint involvement is highly characteristic and less common in other arthritides. Main Distractor Rationale: Rheumatoid arthritis (A) typically spares the DIP joints, involves symmetric polyarthritis, and usually presents with positive RF/anti-CCP (not mentioned here, but a key differentiator). Gout (B) presents with acute, severe monoarticular inflammation, often in the MTP joint of the great toe, and is associated with hyperuricemia and crystal findings, which are not described. Osteoarthritis (C) can affect DIP joints but typically lacks inflammatory features like erythema, significant swelling, and the associated skin rash. Reactive arthritis (E) is often preceded by an infection and presents with a triad of arthritis, urethritis, and conjunctivitis, and while it can involve enthesitis and sacroiliitis, the prominent skin psoriasis and DIP involvement make psoriatic arthritis more likely.
Question 99
A 38-year-old female with a known history of psoriasis presents with diffuse swelling and pain involving her entire left middle finger. The finger appears sausage-like, erythematous, and tender to palpation. Radiographs show soft tissue swelling and periostitis of the phalanges of the affected finger. This specific manifestation is best described as:
View Answer & Explanation
Correct Answer: C
Rationale: Dactylitis, often referred to as a "sausage digit," is a characteristic inflammatory manifestation of psoriatic arthritis, involving diffuse swelling of an entire digit (finger or toe) due to inflammation of the joints, tendons, and soft tissues. The radiographic finding of periostitis further supports this diagnosis. Main Distractor Rationale: Tenosynovitis (D) involves inflammation of the tendon sheath, which can contribute to dactylitis but does not describe the entire digit swelling. Boutonnière (A) and swan neck (B) deformities are specific joint deformities, typically seen in rheumatoid arthritis, and do not describe the diffuse swelling of the entire digit. Mallet finger (E) is a deformity caused by injury to the extensor tendon at the DIP joint.
Question 100
A 52-year-old male with psoriatic arthritis complains of changes in his fingernails. On examination, you observe pitting, onycholysis, and subungual hyperkeratosis. These nail changes are most commonly associated with which of the following conditions?
View Answer & Explanation
Correct Answer: C
Rationale: Nail changes such as pitting, onycholysis (separation of the nail from the nail bed), and subungual hyperkeratosis (thickening of the nail bed) are highly characteristic and common manifestations of psoriasis and psoriatic arthritis. They are often present in patients with psoriatic arthritis, even in the absence of extensive skin lesions. Main Distractor Rationale: Onychomycosis (A) can cause nail thickening and discoloration but typically lacks the characteristic pitting and onycholysis seen in psoriasis. Rheumatoid arthritis (B) and Systemic lupus erythematosus (D) are not typically associated with these specific nail changes. Raynaud's phenomenon (E) affects blood flow to the digits and does not cause these structural nail changes.
