Master ABOS Orthopedic Review: Psoriatic Arthritis, Skeletal Dysplasias, LCH & Rare Bone Conditions | Part 28
Key Takeaway
This ABOS Orthopedic Board Review covers Psoriatic Arthritis, Fibrodysplasia Ossificans Progressiva (FOP), various Skeletal Dysplasias (including MED, SEDC, SEDT, Pseudoachondroplasia, Diastrophic Dysplasia, Kniest Dysplasia, Chondrodysplasia Punctata, PPRD), and Langerhans Cell Histiocytosis (LCH). It provides essential insights into their diagnosis, clinical features, genetics, and management for board preparation.
Question 1
A 37-year-old female presents with a 1-year history of painful, swollen fingers and toes. She has a family history of psoriasis. On physical examination, she has diffuse swelling of several digits, consistent with "sausage fingers," and tenderness over multiple DIP joints. She also has pitting and onycholysis of her fingernails. Laboratory tests are negative for rheumatoid factor. Which of the following is a common associated condition with psoriatic arthritis, as described in the text?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "Oft en occurs with sacroileitis and/or spondylitis." This indicates a common association with psoriatic arthritis. While other conditions might coexist, sacroiliitis and spondylitis are specifically mentioned as frequently occurring with PsA. The other options are not mentioned as common associations in the provided text.
Question 2
A 41-year-old male presents with a 6-month history of joint pain and stiffness. He has a known history of psoriasis affecting his scalp and nails. On examination, he has swollen and tender DIP joints, and some periarticular swelling. Radiographs show erosive changes in the DIP joints and periostitis. Which of the following is a key component for establishing the diagnosis of psoriatic arthritis, according to the provided text?

View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Diagnosis of psoriatic arthritis is established in presence of skin or nail psoriasis and seronegative arthritis." This directly matches option C. Options A and E are incorrect as psoriatic arthritis is seronegative. ESR is a general inflammatory marker, not diagnostic. Biopsy is not mentioned as a primary diagnostic criterion.
Question 3
A 46-year-old female presents with a 1-year history of painful, swollen joints in her hands and feet. She has a long-standing history of psoriasis. On examination, she has well-demarcated erythematous plaques with silvery scales on her elbows and scalp. Multiple DIP joints are swollen and tender. Radiographs show erosive changes. Which of the following statements regarding the gender distribution of psoriatic arthritis is accurate?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "women get it earlier, but the gender proportion is equal." This makes option C the correct answer. Options A, B, D, and E contradict this information.
Question 4
A 39-year-old male presents with a 6-month history of painful, swollen fingers and toes. He has a known history of psoriasis affecting his nails and scalp. On examination, he has well-demarcated erythematous plaques with silvery scales on his extensor surfaces. Multiple DIP joints are swollen and tender. Radiographs show erosive changes. Which of the following is a characteristic location for psoriatic skin lesions?

View Answer & Explanation
Correct Answer: C
Rationale: The image description and clinical context state, "Most commonly involves the hairy area of the skull and the extensor surfaces of the limbs." This directly matches option C. The other options describe locations not typically characteristic of psoriatic skin lesions as per the provided text.
Question 5
A 43-year-old female presents with a 3-month history of pain and swelling in her right ankle and left wrist. She has a long-standing history of psoriasis. On examination, she has typical psoriatic skin lesions on her elbows and knees. Her rheumatoid factor and anti-CCP antibodies are negative. The presence of familial accumulation is characteristic of psoriatic arthritis. What is the approximate incidence of psoriasis vulgaris in the general population?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "Incidence of psoriasis vulgaris is 0.5–2%." This directly provides the answer. Options A, C, D, and E are incorrect based on the provided incidence data.
Question 6
A 36-year-old male presents with a 6-month history of painful, swollen fingers and toes. He has a known history of psoriasis. On examination, he has well-demarcated erythematous plaques with silvery scales on his extensor surfaces. Multiple DIP joints are swollen and tender, and he has diffuse swelling of his left ring finger. Radiographs show erosive changes in the DIP joints and periostitis. Which of the following describes the typical appearance of the skin lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The image description and clinical context state, "Well-defi ned erythematosus papulae and plaques covered with silver–gray lamellae." This translates to raised, red patches covered with silvery-gray scales. The other options describe different dermatological conditions.
Question 7
A 49-year-old female presents with a 1-year history of chronic heel pain, worse with activity. She also reports stiffness in her spine. She has a long-standing history of psoriasis. Physical examination reveals tenderness at the insertion of the Achilles tendon and on the plantar surface of her heel. Radiographs of her feet are unremarkable for fracture but show some soft tissue swelling at the tendon insertions. This patient's condition is characterized by inflammation at tendon and ligament insertions. Which of the following is a common site for this manifestation?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Enthesopathia is common, presenting usually on the plantar surface of the heel and at the attachment of Achilles tendon." This directly identifies the common sites for enthesopathy in psoriatic arthritis. While enthesopathy can occur at other sites, the text specifically highlights these two locations.
Question 8
A 32-year-old female presents with a 6-month history of painful, swollen fingers and toes. She has a known history of psoriasis. On examination, she has well-demarcated erythematous plaques with silvery scales on her extensor surfaces. Multiple DIP joints are swollen and tender. Radiographs show erosive changes in the DIP joints and periostitis. Which of the following best describes the radiographic finding of periostitis in the context of psoriatic arthritis?
View Answer & Explanation
Correct Answer: C
Rationale: The image description mentions "Distal interphalangeal joint involvement and periostitis." Periostitis refers to inflammation of the periosteum, the membrane covering the surface of bones. In psoriatic arthritis, this is a characteristic finding, often seen adjacent to the inflamed joints. Options A, B, D, and E describe other radiographic features, but not specifically periostitis.
Question 9
A 44-year-old male presents with a 1-year history of progressive joint pain and stiffness, predominantly affecting his hands and feet. He has a long-standing history of psoriasis. On examination, he has well-demarcated erythematous plaques with silvery scales on his elbows and scalp. Multiple DIP joints are swollen and tender, and he has dactylitis of his right middle finger. Laboratory tests are negative for rheumatoid factor and anti-CCP antibodies. Which of the following is a characteristic feature of the nail changes seen in psoriatic arthritis?
View Answer & Explanation
Correct Answer: C
Rationale: The text mentions "Psoriatic changes of skin and nails appeare along with polyarthritis." While specific nail changes are not detailed in the main text, the clinical context of psoriatic arthritis commonly includes onycholysis (nail separation from the bed) and pitting (small depressions in the nail plate). This is a well-known association. The other options describe nail changes associated with different conditions.
Question 10
A 35-year-old female presents with a 6-month history of painful, swollen fingers and toes. She has a known history of psoriasis. On examination, she has well-demarcated erythematous plaques with silvery scales on her extensor surfaces. Multiple DIP joints are swollen and tender, and she has diffuse swelling of her left ring finger. Radiographs show erosive changes in the DIP joints and periostitis. Which of the following statements is true regarding the serological findings in psoriatic arthritis?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines psoriatic arthritis as a "seronegative spondylarthritis" and states that "Diagnosis of psoriatic arthritis is established in presence of skin or nail psoriasis and seronegative arthritis." This implies negativity for rheumatoid factor and anti-CCP antibodies. Options A and B are incorrect as it is seronegative. Option D is incorrect as ANA is not universally positive or diagnostic. Option E is incorrect as CRP is a general inflammatory marker, not diagnostic on its own.
Question 11
A 45-year-old male presents with new onset joint pain and swelling in his hands. He reports a history of scaly skin patches on his elbows and scalp for several years.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states, "Th e skin changes usually precede the joint manifestations, but can happen vice-versa ('arthritis psoriatica sine psoriasis')." Option B is incorrect because joint manifestations can sometimes precede skin changes.
Question 12
A 38-year-old female presents with chronic pain and stiffness in her hands, particularly affecting the joints closest to her fingertips. Physical examination reveals swelling and tenderness of these joints.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that the polyarthritis in psoriatic arthritis "involves most commonly the DIP joints." While other joints can be involved, DIP joints are the most characteristic. PIP joints (Option B) are commonly affected in rheumatoid arthritis, but DIPs are more specific to psoriatic arthritis.
Question 13
A 50-year-old male presents with inflammatory arthritis affecting multiple joints. Laboratory tests are ordered to differentiate his condition from rheumatoid arthritis.
View Answer & Explanation
Correct Answer: C
Rationale: Psoriatic arthritis is classified as a "seronegative spondylarthritis," meaning it is typically negative for Rheumatoid Factor (RF) and anti-CCP antibodies. ESR and CRP (Options A and B) are acute phase reactants and are often elevated in inflammatory conditions, including psoriatic arthritis, so they do not differentiate it. HLA-B27 (Option E) can be positive in cases of spinal spread but is not a general seronegative marker for peripheral arthritis.
Question 14
A 42-year-old male with a history of psoriasis presents with diffuse swelling of his right index finger, making it appear uniformly enlarged and sausage-like. Radiographs show soft tissue swelling and some periarticular changes.
View Answer & Explanation
Correct Answer: C
Rationale: The text mentions, "Destructive arthritis of distal joints may be manifest in so-called sausage fi ngers." This uniform swelling of an entire digit, often seen in psoriatic arthritis, is medically termed dactylitis. Boutonnière and Swan neck deformities (Options A and B) are characteristic of rheumatoid arthritis, while mallet finger (Option D) and trigger finger (Option E) are distinct orthopedic conditions.
Question 15
A 35-year-old female with newly diagnosed psoriatic arthritis complains of severe heel pain, particularly when taking her first steps in the morning. Physical examination reveals tenderness at the insertion of the Achilles tendon and on the plantar surface of the heel.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Enthesopathia is common, presenting usually on the plantar surface of the heel and at the attachment of Achilles tendon." Enthesopathy refers to inflammation at the site where tendons or ligaments insert into bone. While tendinitis (Option D) involves the tendon itself, enthesopathy specifically refers to the insertion site.
Question 16
A 55-year-old male with psoriatic arthritis presents with chronic low back pain and stiffness, particularly worse in the mornings. Radiographs show evidence of sacroiliitis.
View Answer & Explanation
Correct Answer: B
Rationale: The text specifies, "HLAB27 antigen is positive only on cases of spinal spread." Sacroiliitis is a form of spinal involvement. RF and anti-CCP antibodies (Options E and C) are typically negative in psoriatic arthritis. HLA-DR4 (Option A) is associated with rheumatoid arthritis.
Question 17
A 48-year-old female presents with polyarticular joint pain and swelling. She also has a history of skin rashes. To establish a diagnosis of psoriatic arthritis, which combination of findings is essential?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Diagnosis of psoriatic arthritis is established in presence of skin or nail psoriasis and seronegative arthritis." Option A is incorrect as psoriatic arthritis is seronegative. While HLA-B27 and sacroiliitis (Option D) can be present, they are not universally required for diagnosis, especially in peripheral forms.
Question 18
A physician is counseling a patient newly diagnosed with psoriasis vulgaris about potential complications. The patient asks about the likelihood of developing joint problems.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Incidence of psoriasis vulgaris is 0.5–2%; out of this population 5–10% suff er joint involvement." Option B represents the incidence of psoriasis vulgaris itself, not the percentage of those with psoriasis who develop arthritis.
Question 19
A 28-year-old male presents with symptoms suggestive of psoriatic arthritis. His physician is considering the typical demographic profile for this condition.
View Answer & Explanation
Correct Answer: C
Rationale: The text indicates, "Th e disease appears between 30 and 50 years of age." While the patient in the vignette is slightly younger, the question asks for the typical age range. Option B is too early for the typical onset.
Question 20
A 32-year-old female and a 48-year-old male are both diagnosed with psoriatic arthritis. Their physician is discussing the typical gender distribution of the disease.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "women get it earlier, but the gender proportion is equal." Options A and B are incorrect as the overall proportion is equal. Option D is incorrect as women tend to get it earlier.
Question 21
A 40-year-old patient with a long history of psoriasis presents with worsening back pain and stiffness, particularly in the lower spine and buttocks. Radiographs are ordered to assess for specific involvement.
View Answer & Explanation
Correct Answer: C
Rationale: The text mentions that psoriatic arthritis "Oft en occurs with sacroileitis and/or spondylitis." These are inflammatory conditions affecting the sacroiliac joints and spine, respectively, and are characteristic of seronegative spondylarthropathies. The other options are not specific to psoriatic arthritis.
Question 22
A 52-year-old male with psoriatic arthritis has progressive joint damage despite treatment. His orthopedic surgeon is explaining the nature of the disease.
View Answer & Explanation
Correct Answer: C
Rationale: The text describes the polyarthritis in psoriatic arthritis as "erosive, destructive." This indicates a progressive and damaging form of arthritis. Options A, B, and D contradict this description. Option E describes a degenerative, not inflammatory, process.
Question 23
A 39-year-old female presents with polyarticular arthritis, negative Rheumatoid Factor, and a history of skin lesions. Her physician is considering differential diagnoses within the seronegative spondylarthropathies.
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "Psoriatic arthritis is one form of seronegative spondylarthritis (SNSA)." Ankylosing Spondylitis is another classic example of a seronegative spondylarthritis. Rheumatoid Arthritis (Option A) is seropositive (RF/anti-CCP positive). Systemic Lupus Erythematosus (Option B) is a connective tissue disease, and Osteoarthritis (Option C) is degenerative. Gout (Option E) is a crystal-induced arthropathy.
Question 24
A 41-year-old male with psoriatic arthritis presents for follow-up. During the examination, the physician notes pitting, onycholysis, and discoloration of his fingernails.
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Diagnosis of psoriatic arthritis is established in presence of skin or nail psoriasis and seronegative arthritis." Nail changes (pitting, onycholysis) are characteristic manifestations of nail psoriasis. Elevated uric acid (Option A) can occur but is not a diagnostic criterion. Anti-CCP antibodies (Option B) and rheumatoid nodules (Option E) are associated with rheumatoid arthritis.
Question 25
A 2-year-old boy presents with a history of recurrent painful swellings in his neck and back muscles, which resolve but leave behind palpable hard lumps. His parents also noticed that his great toes appear unusually short and malformed since birth. Radiographs show ectopic bone formation in the soft tissues of the neck and characteristic deformities of the great toes.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical presentation of recurrent painful muscle swellings leading to ectopic ossification, coupled with characteristic short and malformed great toes, is pathognomonic for Fibrodysplasia Ossificans Progressiva (FOP). Osteogenesis Imperfecta is characterized by brittle bones and frequent fractures, not ectopic ossification. Marfan Syndrome involves connective tissue abnormalities, Duchenne Muscular Dystrophy is a muscle wasting disorder, and Achondroplasia is a form of dwarfism, none of which fit this specific constellation of symptoms.
Question 26
A 5-year-old girl is diagnosed with Fibrodysplasia Ossificans Progressiva. Her parents are concerned about the risk of future children inheriting the condition and inquire about genetic counseling. They report no known family history of the disease.
View Answer & Explanation
Correct Answer: C
Rationale: Fibrodysplasia Ossificans Progressiva is described as a rare autosomal dominant disorder. While many cases arise from spontaneous mutations, the underlying inheritance pattern is dominant, meaning only one copy of the mutated gene is sufficient to cause the disorder. Autosomal recessive requires two copies of the mutated gene, and X-linked recessive primarily affects males.
Question 27
A 15-year-old girl presents with foot deformities that have been present since early childhood. On examination, her great toes are notably short with a "hallux valgus-like" malformation. Radiographs confirm the presence of absent phalanges in her great toes.

View Answer & Explanation
Correct Answer: C
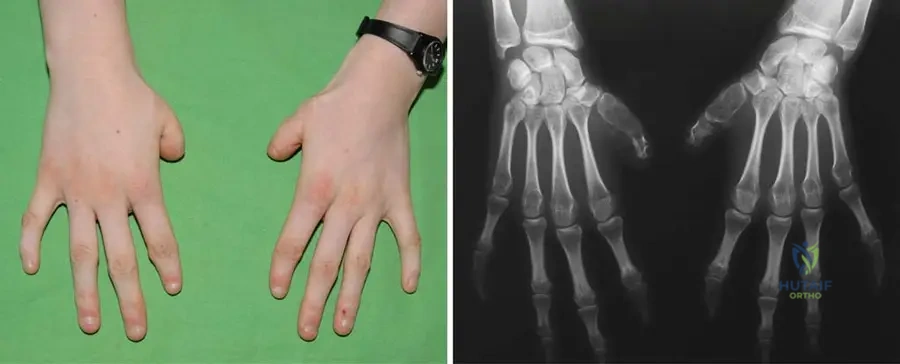
Rationale: The clinical context explicitly states that "typical short great toes with 'hallux valgus-like' malformations and absent phalanges" are characteristic defects in Fibrodysplasia Ossificans Progressiva, as shown in Fig. 12.9. Polydactyly refers to extra digits, syndactyly to fused digits, clubfoot is a complex foot deformity, and metatarsus adductus is an inward deviation of the forefoot, none of which precisely describe the specific malformation seen in FOP.
Question 28
A 7-year-old boy with Fibrodysplasia Ossificans Progressiva initially developed ossification in his neck muscles. Over the next few years, his parents observed new areas of stiffness and bony growths appearing in his shoulders, then his arms, and later his hips and legs.
View Answer & Explanation
Correct Answer: C
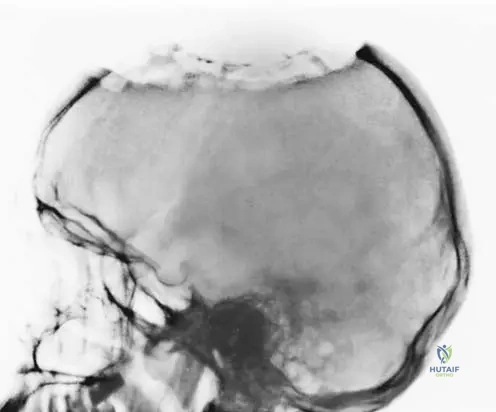
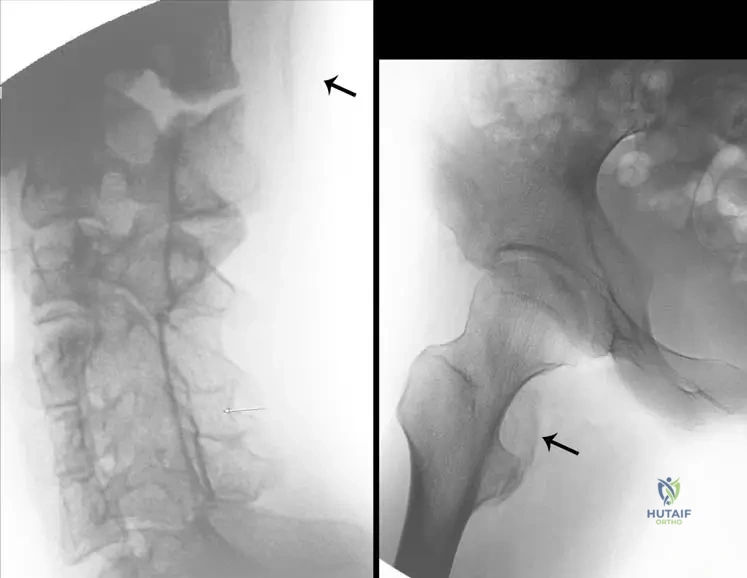
Rationale: The provided text and Fig. 12.11 explicitly state that the disease "begins with a distinct ossification line in the upper paraspinal muscles of the neck... and later spreads from axial to appendicular, cranial to caudal, and proximal to distal, also involving the muscles." This describes a highly characteristic and predictable pattern of progression. The other options describe incorrect or incomplete patterns.
Question 29
A 15-year-old girl with a known diagnosis of Fibrodysplasia Ossificans Progressiva presents with new onset painful swelling in her left chest wall and right hip region. An MRI is performed to assess disease activity.
View Answer & Explanation
Correct Answer: C
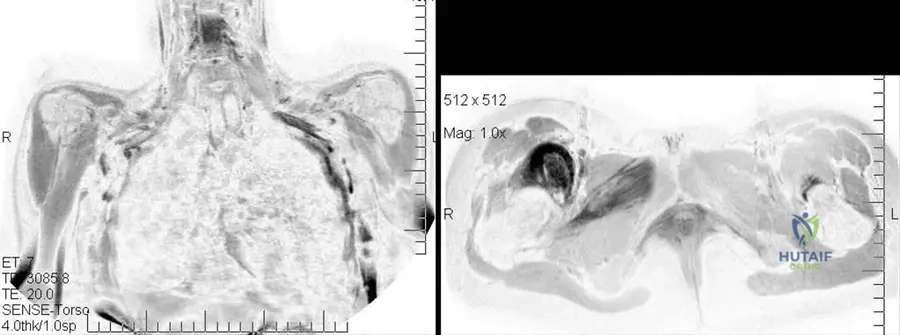
Rationale: The clinical context for Fig. 12.12 states, "On MR images the high signal intensity means the ongoing process of the progressive myositis ossificans." This indicates active inflammation and early heterotopic ossification. Terminal phase ossification is described as "less clearly visible on MR images" due to the lack of edema. Muscle atrophy, malignant transformation, or simple muscle strain are not indicated by high signal intensity in this specific context of FOP.
Question 30
A 3-year-old boy is diagnosed with Fibrodysplasia Ossificans Progressiva. His parents are seeking information regarding the long-term prognosis and expected level of disability for their child.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "There is no efficient treatment; the patients are confined to a chair by the age of 30 because of the serious contractures and decreased range of movement of the joints." This highlights the severe and progressive nature of the disability. The other options describe outcomes that are not characteristic of FOP.
Question 31
A patient with Fibrodysplasia Ossificans Progressiva undergoes a biopsy of a newly formed bony lesion adjacent to a major joint. Histological examination reveals mature lamellar bone within soft tissue.
View Answer & Explanation
Correct Answer: C
Rationale: The text states that in FOP, "The bony growths involve tendons, ligaments, fibrous muscle tissue, and connective tissue. In affected areas the bone slowly replaces the fibrotic muscles." This indicates a broad involvement of various soft connective tissues, not just muscle. The other options are too restrictive or incorrect regarding the tissues involved in ectopic ossification in FOP.
Question 32
A pediatrician encounters an infant with congenital malformations of the great toes and a recent history of unexplained painful muscle swelling. The pediatrician suspects Fibrodysplasia Ossificans Progressiva.
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "The onset of this disease is between age 0 and 15 years." This makes FOP a condition that manifests in childhood or adolescence. The other age ranges are incorrect for the typical onset of the disease.
Question 33
The parents of a 4-year-old boy recently diagnosed with Fibrodysplasia Ossificans Progressiva are desperate for treatment options to prevent the progression of the disease and preserve their son's mobility.
View Answer & Explanation
Correct Answer: D
Rationale: The text clearly states, "There is no efficient treatment." While research is ongoing, currently there is no widely accepted or curative treatment for FOP. Surgical excision can often exacerbate the condition, and corticosteroids offer only temporary relief, not a halt to progression. Gene therapy is experimental, and physical therapy cannot reverse ossification.
Question 34
A medical resident is reviewing a patient chart for a 10-year-old girl with a history of progressive muscle stiffness and ectopic bone formation. The chart lists "Münchmayer’s disease" as a potential diagnosis.
View Answer & Explanation
Correct Answer: D
Rationale: The text lists "progressive osseous heteroplasia, myositis ossificans progressiva, Münchmayer’s disease" as synonyms for Fibrodysplasia Ossificans Progressiva. Therefore, Myositis ossificans progressiva is a correct synonym. The other conditions are distinct bone or connective tissue disorders.
Question 35
A 3-year-old boy is suspected of having Fibrodysplasia Ossificans Progressiva due to characteristic toe malformations. To confirm the diagnosis and assess early disease activity, radiographs are ordered to identify the initial site of heterotopic ossification.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 12.11 and its accompanying text explicitly state, "The disease begins with a distinct ossification line in the upper paraspinal muscles of the neck (a, arrow)." This is the characteristic initial site of ectopic ossification in FOP. While other muscles can be involved later, they are not typically the starting point.
Question 36
A 15-year-old girl presents with congenital foot deformities. Clinical examination reveals short great toes with a "hallux valgus-like" appearance. Radiographs confirm absent phalanges in these toes.
View Answer & Explanation
Correct Answer: B
Rationale: The description of "typical short great toes with 'hallux valgus-like' malformations and absent phalanges" is a characteristic skeletal malformation specifically associated with Fibrodysplasia Ossificans Progressiva, as shown in Fig. 12.9. The other conditions listed do not typically present with this specific congenital foot malformation.
Question 37
A 15-year-old girl with Fibrodysplasia Ossificans Progressiva is noted to have short thumbs on clinical examination and radiographs.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context for Fig. 12.10, which shows short thumbs in a patient with FOP, explicitly states, "This malformation is not always present." This indicates variability in its manifestation among individuals with FOP. The other options contradict this statement or are not supported by the provided text.
Question 38
A 4-year-old boy with advanced Fibrodysplasia Ossificans Progressiva develops skin breakdown over areas of significant heterotopic ossification on his back.
<img “hallux=”” (fop).<=”” a=”” absent=”” appearance.=”” birth.=”” confirm=”” examination=”” fibrodysplasia=”” great=”” in=”” ossificans=”” p=”” phalanges=”” physician=”” progressiva=”” radiographs=”” reveals=”” s=”” short=”” since=”” src=’/media/Hutaiforthoatlas/atlas-123-fibrodys
<div class=”aaos-static-mcq” markdown=”1”>
<h3>Question 21</h3>
<p class=”vignette”>A 3-year-old child is brought to the clinic by parents who noticed unusual malformations of the child’ suspects=”” the=”” toes=”” toes.=”” valgus-like”=”” with=”“/>
View Answer & Explanation
Correct Answer: A
Rationale: Fibrodysplasia Ossificans Progressiva is characterized by typical short great toes with "hallux valgus-like" malformations and often absent phalanges, which are often present at birth or early childhood. Polydactyly, syndactyly, clubfoot, and metatarsus adductus are distinct congenital foot anomalies not characteristic of FOP's specific toe malformation.
Question 39
A 5-year-old boy is diagnosed with Fibrodysplasia Ossificans Progressiva after presenting with progressive muscle stiffness and characteristic skeletal malformations. His parents are concerned about the risk for future children and ask about the genetic basis of the disorder.
View Answer & Explanation
Correct Answer: A
Rationale: Fibrodysplasia Ossificans Progressiva is a rare autosomal dominant disorder. This means only one copy of the mutated gene is needed to cause the disorder, and it can be inherited from an affected parent or arise from a new mutation. Autosomal recessive inheritance requires two copies of the mutated gene.
Question 40
A 7-year-old girl with a confirmed diagnosis of FOP initially presented with stiffness in her neck muscles. Over the past year, her parents have noticed increasing stiffness and limited range of motion in her shoulders and hips. This pattern of disease progression is characteristic of FOP.
View Answer & Explanation
Correct Answer: A
Rationale: The ectopic ossification in FOP typically spreads in a distinct pattern: from axial to appendicular, cranial to caudal, and proximal to distal. This explains the progression from neck (axial, cranial, proximal) to shoulders and hips (appendicular, caudal, more distal than neck). While trauma can trigger flares, the overall spread follows a predictable pattern, not random or solely trauma-induced.
Question 41
The parents of a 2-year-old boy recently diagnosed with Fibrodysplasia Ossificans Progressiva are seeking information regarding the long-term prognosis and expected functional limitations for their child.
View Answer & Explanation
Correct Answer: A
Rationale: Fibrodysplasia Ossificans Progressiva is a severely disabling condition. Due to progressive ectopic ossification and resulting serious contractures and decreased range of movement of the joints, patients are typically confined to a chair by the age of 30. There is no efficient treatment, and surgical interventions can often exacerbate the condition.
Question 42
A 5-year-old child with known FOP presents with new onset neck pain and stiffness. Radiographs are obtained to assess for new ossification. Based on the typical progression of the disease, where would the earliest distinct ossification line most commonly be observed?
View Answer & Explanation
Correct Answer: A
Rationale: The disease typically begins with a distinct ossification line in the upper paraspinal muscles of the neck. This is a characteristic early site of ectopic bone formation in FOP, consistent with its cranial-to-caudal progression. While other muscles can be affected later, the neck is a common initial site.
Question 43
A 15-year-old girl with Fibrodysplasia Ossificans Progressiva experiences a flare-up characterized by painful swelling and stiffness in her left intercostal muscles and right obturator externus muscle. An MRI is performed to evaluate the extent of the ongoing process.
View Answer & Explanation
Correct Answer: A
Rationale: During the ongoing process of progressive myositis ossificans in FOP, MR images typically show high signal intensity in the affected muscles. This high signal reflects the active inflammatory and edematous phase preceding ossification. Low signal intensity would typically indicate chronic, fibrotic, or fully ossified, inactive lesions.
Question 44
A pathologist is reviewing a biopsy specimen from a patient with Fibrodysplasia Ossificans Progressiva, showing early ectopic bone formation. The disease is known for involving various soft tissues.
View Answer & Explanation
Correct Answer: A
Rationale: In Fibrodysplasia Ossificans Progressiva, the ectopic bone formation involves a wide range of soft tissues, including striated muscles, tendons, ligaments, fibrous muscle tissue, and other connective tissues. It is not limited to articular cartilage or bone-related structures, nor does it primarily affect nerve or epithelial tissues.
Question 45
A 6-year-old child with Fibrodysplasia Ossificans Progressiva presents with a new flare-up of painful muscle swelling in the shoulder. The orthopedic surgeon is considering management strategies.
View Answer & Explanation
Correct Answer: A
Rationale: A critical principle in the management of FOP is the avoidance of trauma, including unnecessary surgical interventions, intramuscular injections, and aggressive physical therapy, as these can trigger or exacerbate flare-ups and induce new ectopic ossification. There is no efficient treatment, and surgical excision often leads to more aggressive bone formation.
Question 46
A newborn is noted to have bilateral short great toes with a "hallux valgus-like" appearance. The pediatrician is considering a diagnosis of Fibrodysplasia Ossificans Progressiva. In the differential diagnosis of congenital foot malformations, which of the following conditions is LEAST likely to present with similar early skeletal malformations of the great toes as seen in FOP?
View Answer & Explanation
Correct Answer: A
Rationale: Fibrodysplasia Ossificans Progressiva is characterized by short great toes with "hallux valgus-like" malformations and often absent phalanges. Polydactyly refers to the presence of extra digits, which is a distinct malformation and not typically associated with the specific great toe malformation of FOP. Brachydactyly (short digits) and hallux varus (a great toe deformity) are more similar in presentation to the FOP toe malformations than polydactyly.
Question 47
A 1-year-old child presents with characteristic great toe malformations and a recent episode of painful swelling in the neck muscles. The family history is negative for similar conditions. The physician is confirming the diagnosis of FOP and discussing the typical disease course.
View Answer & Explanation
Correct Answer: A
Rationale: The onset of Fibrodysplasia Ossificans Progressiva typically occurs between age 0 and 15 years, often with the characteristic skeletal malformations present at birth or early childhood, followed by episodes of painful muscle swelling and ossification. Onset in later age ranges is not typical for this condition.
Question 48
A 10-year-old girl with a confirmed diagnosis of FOP is undergoing a routine orthopedic examination. In addition to her characteristic great toe malformations, the physician notes a specific malformation in her hands.
View Answer & Explanation
Correct Answer: A
Rationale: While not always present, short thumbs are a recognized skeletal malformation that can be seen in patients with Fibrodysplasia Ossificans Progressiva, similar to the malformations of the great toes. Other options like polydactyly or syndactyly are not characteristic of FOP.
Question 49
A 40-year-old patient with long-standing FOP has extensive, mature ossifications around multiple joints, leading to severe functional limitations. A new area of stiffness is being evaluated with MRI to differentiate between active inflammation and mature ossification.
View Answer & Explanation
Correct Answer: A
Rationale: In the terminal phase of Fibrodysplasia Ossificans Progressiva, the disease primarily provokes ossification and calcification in muscles, and does not cause significant edema. Therefore, the terminal phase is less clearly visible on MR images compared to the active, inflammatory phase which shows high signal intensity due to edema.
Question 50
A 7-year-old boy presents with bilateral hip and knee pain, worse with activity, and a waddling gait. His parents note he has always been shorter than his peers but otherwise healthy. Physical examination reveals mild short stature, normal facial features, and restricted range of motion in his hips and knees. Radiographs show irregular, flattened, and fragmented epiphyses in the femoral heads, distal femurs, and proximal tibias. The vertebral bodies appear normal.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of joint pain, waddling gait, mild short stature, and characteristic radiographic findings of irregular, flattened, and fragmented epiphyses (especially in the hips and knees) with normal vertebral bodies is classic for Multiple Epiphyseal Dysplasia (MED), specifically the Fairbank type. Pseudoachondroplasia typically presents with more severe short stature, often normal at birth with onset of symptoms around 2-3 years, and can have mild platyspondyly. Spondyloepiphyseal Dysplasia Congenita presents at birth with severe short stature, significant platyspondyly, and often odontoid hypoplasia. Achondroplasia is a rhizomelic dwarfism with normal epiphyses, macrocephaly, and characteristic metaphyseal changes. Diastrophic Dysplasia has severe short stature, clubfoot, hitchhiker's thumb, and cauliflower ears, which are not described.
Question 51
A newborn male is diagnosed with severe short stature, a barrel chest, and a cleft palate. Radiographs reveal significant platyspondyly, particularly in the lumbar spine, and delayed, irregular ossification of the epiphyses, especially in the hips and knees. Further evaluation shows odontoid hypoplasia. Which of the following is the most critical immediate concern for this patient?
View Answer & Explanation
Correct Answer: C
Rationale: This clinical picture is highly suggestive of Spondyloepiphyseal Dysplasia Congenita (SEDC), an autosomal dominant condition caused by mutations in the COL2A1 gene. A hallmark feature of SEDC is odontoid hypoplasia, which predisposes patients to atlantoaxial instability. This instability can lead to spinal cord compression and is a critical immediate concern requiring careful monitoring and potential surgical stabilization. While progressive scoliosis, early onset osteoarthritis, genu varum, and retinal detachment (also associated with SEDC) are important long-term concerns, atlantoaxial instability poses the most immediate life-threatening risk due to potential neurological compromise.
Question 52
A 3-year-old girl presents with disproportionate short stature, a waddling gait, and joint laxity. Her head circumference is normal for her age. Radiographs show irregular, fragmented epiphyses, short, broad metaphyses, and mild platyspondyly. Her parents report she was of normal length at birth. Which of the following genetic mutations is most likely responsible for her condition?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of disproportionate short stature, waddling gait, joint laxity, normal head circumference, and onset after birth, along with radiographic findings of irregular epiphyses and short metaphyses, is characteristic of Pseudoachondroplasia. This condition is inherited in an autosomal dominant manner and is caused by mutations in the COMP (Cartilage Oligomeric Matrix Protein) gene. FGFR3 mutations cause Achondroplasia, which presents with macrocephaly and rhizomelic dwarfism, and normal epiphyses. COL2A1 mutations are associated with SED Congenita and Kniest Dysplasia. SLC26A2 mutations are found in Diastrophic Dysplasia and some forms of recessive MED. TRAPPC2 mutations cause Spondyloepiphyseal Dysplasia Tarda.
Question 53
An 11-year-old boy presents with chronic back pain and a progressive waddling gait. He has mild short stature, primarily truncal. Radiographs of the spine show characteristic "hump-shaped" or "pear-shaped" vertebral bodies, particularly in the lumbar region, with significant platyspondyly. Epiphyseal dysplasia is noted in the hips. His mother reports that his maternal uncle had similar issues. What is the most likely inheritance pattern for this condition?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of an 11-year-old boy with back pain, waddling gait, truncal short stature, and characteristic "hump-shaped" or "pear-shaped" platyspondyly, along with epiphyseal dysplasia, is classic for Spondyloepiphyseal Dysplasia Tarda (SEDT). The report of a maternal uncle having similar issues strongly suggests an X-linked recessive inheritance pattern, as males are primarily affected and the gene is passed from carrier mothers. SEDT is caused by mutations in the TRAPPC2 gene located on the X chromosome. Spondyloepiphyseal Dysplasia Congenita is autosomal dominant.
Question 54
A 1-year-old infant presents with severe short stature, bilateral clubfeet, and a "hitchhiker's thumb" deformity. Physical examination also reveals cauliflower-like ears and a history of cleft palate repair. Radiographs show generalized epiphyseal and metaphyseal changes, with short, broad long bones. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: D
Rationale: The constellation of severe short stature, bilateral clubfeet, "hitchhiker's thumb" (abducted thumb), cauliflower ears, and cleft palate is pathognomonic for Diastrophic Dysplasia. This is an autosomal recessive condition caused by mutations in the SLC26A2 gene. While other dysplasias can cause short stature and joint involvement, these specific extraskeletal and limb deformities are highly characteristic of Diastrophic Dysplasia. Multiple Epiphyseal Dysplasia primarily affects epiphyses and lacks these specific deformities. SED Congenita involves severe platyspondyly and odontoid hypoplasia. Pseudoachondroplasia presents later with joint laxity and epiphyseal changes but lacks the specific hand/ear/foot deformities. Achondroplasia has distinct rhizomelic dwarfism and macrocephaly.
Question 55
A 6-year-old boy is diagnosed with Multiple Epiphyseal Dysplasia (MED) based on his clinical presentation of joint pain, waddling gait, and radiographic findings of irregular and flattened epiphyses in multiple joints. His parents are healthy and have no history of skeletal dysplasia. Genetic testing is recommended. Which of the following genes is most commonly implicated in the autosomal dominant form of MED?
View Answer & Explanation
Correct Answer: C
Rationale: The most common cause of autosomal dominant Multiple Epiphyseal Dysplasia (MED) is a mutation in the COMP (Cartilage Oligomeric Matrix Protein) gene. COMP mutations are also responsible for Pseudoachondroplasia, which is a more severe phenotype. FGFR3 mutations cause Achondroplasia. COL2A1 mutations are associated with Spondyloepiphyseal Dysplasia Congenita and Kniest Dysplasia. SLC26A2 mutations cause Diastrophic Dysplasia and the autosomal recessive form of MED. TRAPPC2 mutations cause Spondyloepiphyseal Dysplasia Tarda.
Question 56
A 5-year-old girl with Spondyloepiphyseal Dysplasia Congenita (SEDC) is being evaluated for progressive visual impairment. She has a known history of severe short stature, platyspondyly, and hip dysplasia. Her condition is due to a mutation in the COL2A1 gene. Which of the following ocular complications is commonly associated with SEDC and other type II collagenopathies?
View Answer & Explanation
Correct Answer: C
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDC) is a type II collagenopathy, and mutations in COL2A1 can affect not only cartilage but also other connective tissues, including the vitreous humor of the eye. Patients with SEDC are at increased risk for severe myopia and retinal detachment, which can lead to significant visual impairment. While other ocular issues can occur, retinal detachment is a particularly common and serious complication associated with COL2A1-related disorders like SEDC and Stickler syndrome. Cataracts are more commonly associated with conditions like Chondrodysplasia Punctata.
Question 57
A 4-year-old boy with Pseudoachondroplasia presents for orthopedic follow-up. His parents are concerned about his increasing joint pain and waddling gait. They recall he was of normal size at birth but developed short stature and gait abnormalities around age 2. Radiographs confirm irregular and fragmented epiphyses. The underlying genetic defect in Pseudoachondroplasia primarily affects which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: Pseudoachondroplasia is caused by mutations in the COMP (Cartilage Oligomeric Matrix Protein) gene. COMP is an extracellular matrix protein found in cartilage, tendons, and ligaments, and plays a role in chondrocyte proliferation and organization. Mutations in COMP lead to its accumulation within chondrocytes, causing endoplasmic reticulum stress and premature chondrocyte death, ultimately impairing endochondral ossification. Fibroblast growth factor receptor 3 (FGFR3) signaling is affected in Achondroplasia. Type II collagen synthesis is affected in Spondyloepiphyseal Dysplasia Congenita and Kniest Dysplasia. Sulfate transport is affected in Diastrophic Dysplasia and recessive MED (SLC26A2). Lysosomal enzyme activity is affected in mucopolysaccharidoses.
Question 58
A 2-year-old boy is noted to have mild, asymmetric flattening and irregularity of the femoral capital epiphyses on radiographs obtained for a limp. He has no other skeletal abnormalities, and his growth is otherwise normal. His physical examination is unremarkable except for the mild limp. The orthopedic surgeon reassures the parents that this condition is often self-limiting and may resolve spontaneously. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The description of mild, often asymmetric, flattening and irregularity of the femoral capital epiphyses in a young child, with an otherwise normal skeleton and a self-limiting course, is characteristic of Meyer's Dysplasia (Dysplasia Epiphysealis Capitis Femoris). This is considered a mild, often transient, form of epiphyseal dysplasia primarily affecting the femoral heads. Legg-Calve-Perthes disease is avascular necrosis of the femoral head, which can look similar but typically has a more distinct progression of collapse and reossification. Spondyloepiphyseal Dysplasia Tarda and Pseudoachondroplasia involve more widespread and severe epiphyseal and often spinal changes. Multiple Epiphyseal Dysplasia is typically more generalized and progressive, affecting multiple epiphyses and leading to early osteoarthritis.
Question 59
A newborn is evaluated for severe short stature and limb shortening. Radiographs reveal striking punctate calcifications within the epiphyses and metaphyses, particularly in the long bones, along with coronal clefts in the vertebral bodies. The infant also has cataracts. Which of the following conditions is characterized by these radiographic findings?
View Answer & Explanation
Correct Answer: C
Rationale: The presence of punctate (stippled) calcifications within the epiphyses and metaphyses, along with coronal clefts in the vertebral bodies and cataracts, is the classic radiographic hallmark of Chondrodysplasia Punctata (CDP). This is a heterogeneous group of disorders, with Rhizomelic Chondrodysplasia Punctata being a severe autosomal recessive form. Achondroplasia does not involve epiphyseal stippling. Kniest Dysplasia is characterized by "Swiss cheese" cartilage appearance and dumbbell-shaped long bones. SED Congenita involves platyspondyly and irregular epiphyses but not punctate calcifications. Multiple Epiphyseal Dysplasia presents later in childhood without stippling.
Question 60
A 5-year-old boy presents with a progressive waddling gait and bilateral hip pain. His parents report he has always been shorter than his peers. Physical examination reveals limited hip abduction and internal rotation. Radiographs show bilateral, symmetric, irregular, and flattened femoral capital epiphyses, with normal vertebral bodies. Which of the following conditions is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The presentation of a 5-year-old with progressive waddling gait, bilateral hip pain, short stature, and symmetric, irregular, and flattened femoral capital epiphyses with normal vertebral bodies is highly characteristic of Multiple Epiphyseal Dysplasia (MED). Legg-Calve-Perthes disease is typically unilateral, though it can be bilateral in about 10-15% of cases, but usually presents with a more acute onset and distinct phases of avascular necrosis and reossification. Bilateral SCFE typically occurs in adolescents, often overweight, and involves a posterior and inferior slip of the epiphysis. Transient synovitis is an acute, self-limiting condition, usually unilateral, without chronic radiographic changes. Juvenile Idiopathic Arthritis can cause joint pain and radiographic changes, but the specific epiphyseal flattening and irregularity in multiple joints are more indicative of a dysplasia.
Question 61
A 3-year-old boy with a known diagnosis of Spondyloepiphyseal Dysplasia Congenita (SEDC) presents to the emergency department after a minor fall, complaining of neck pain and weakness in his upper extremities. Physical examination reveals hyperreflexia and clonus. Given his underlying condition, which of the following is the most likely cause of his neurological symptoms?
View Answer & Explanation
Correct Answer: A
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDC) is frequently associated with odontoid hypoplasia, which leads to atlantoaxial instability. Even minor trauma can cause subluxation at the C1-C2 level, resulting in spinal cord compression and neurological symptoms such as neck pain, weakness, hyperreflexia, and clonus. This is a critical complication requiring urgent evaluation and management. While other spinal issues can occur in skeletal dysplasias, atlantoaxial instability due to odontoid hypoplasia is a hallmark and severe complication of SEDC. Thoracolumbar kyphosis is more common in conditions like Diastrophic Dysplasia or Morquio syndrome, and spinal stenosis is less common in SEDC than atlantoaxial instability. Diastematomyelia and syringomyelia are congenital spinal cord anomalies not directly linked to SEDC.
Question 62
A 9-year-old girl is diagnosed with a severe form of Multiple Epiphyseal Dysplasia (MED) that also involves mild platyspondyly and short, broad metaphyses. Her parents are first cousins and are both unaffected. Genetic testing reveals a mutation in the SLC26A2 gene. This gene is also associated with which other skeletal dysplasia?
View Answer & Explanation
Correct Answer: D
Rationale: The SLC26A2 gene (also known as DTDST, for diastrophic dysplasia sulfate transporter) encodes a sulfate transporter protein critical for cartilage matrix formation. Mutations in this gene cause a spectrum of skeletal dysplasias, including Diastrophic Dysplasia (the most severe phenotype), Achondrogenesis type 1B, Atelosteogenesis type 2, and the autosomal recessive form of Multiple Epiphyseal Dysplasia (MED). The description of a severe MED with mild platyspondyly and metaphyseal changes, inherited recessively (parents are first cousins and unaffected), is consistent with recessive MED due to SLC26A2 mutation. Therefore, Diastrophic Dysplasia is also caused by mutations in the same gene. Achondroplasia is FGFR3. SED Congenita and Kniest Dysplasia are COL2A1. Pseudoachondroplasia is COMP.
Question 63
A 6-year-old boy presents with severe short stature, joint stiffness, and a "barrel chest." Radiographs show markedly flattened vertebral bodies (platyspondyly) and dumbbell-shaped long bones with irregular, enlarged epiphyses. MRI of the joints reveals a characteristic "Swiss cheese" appearance of the cartilage. Which of the following diagnoses is most consistent with these findings?
View Answer & Explanation
Correct Answer: B
Rationale: The combination of severe short stature, joint stiffness, platyspondyly, dumbbell-shaped long bones, and the distinctive "Swiss cheese" appearance of cartilage on MRI is pathognomonic for Kniest Dysplasia. This is an autosomal dominant condition caused by mutations in the COL2A1 gene. While Spondyloepiphyseal Dysplasia Tarda and Pseudoachondroplasia involve epiphyseal and spinal changes, they do not typically present with dumbbell-shaped long bones or the "Swiss cheese" cartilage appearance. Multiple Epiphyseal Dysplasia is generally milder and lacks these specific features. Achondroplasia has distinct radiographic findings of rhizomelic dwarfism and normal epiphyses.
Question 64
A 10-year-old girl with mild short stature and early-onset osteoarthritis is diagnosed with a skeletal dysplasia. She also has a history of severe myopia requiring corrective lenses and a repaired cleft palate. Her family history reveals similar features in her father. Which of the following conditions, often associated with type II collagen defects, best fits this clinical picture?
View Answer & Explanation
Correct Answer: C
Rationale: The combination of mild short stature, early-onset osteoarthritis (arthropathy), severe myopia, and cleft palate, with an autosomal dominant inheritance pattern (father affected), is highly suggestive of Stickler Syndrome. Stickler Syndrome is a connective tissue disorder, primarily affecting type II and XI collagen, and often presents with ocular (myopia, retinal detachment), craniofacial (cleft palate, Pierre Robin sequence), auditory (hearing loss), and articular (arthropathy, hypermobility) manifestations. While Spondyloepiphyseal Dysplasia Congenita (SEDC) is also a type II collagenopathy and can have ocular and palatal issues, it typically presents with more severe short stature and platyspondyly from birth. Diastrophic Dysplasia, Pseudoachondroplasia, and Achondroplasia do not typically present with this specific combination of ocular and craniofacial features alongside arthropathy.
Question 65
A 12-year-old boy with Multiple Epiphyseal Dysplasia (MED) presents with chronic bilateral hip pain that is significantly impacting his daily activities. Radi
Question 65
A 6-year-old boy presents with waddling gait and bilateral hip pain, worse with activity. His parents note he has always been shorter than his peers. Physical exam reveals limited range of motion in both hips, particularly abduction and internal rotation. Radiographs show flattened and irregular femoral epiphyses, especially at the femoral heads, and mild epiphyseal changes in the knees and ankles. The spine appears normal. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Multiple Epiphyseal Dysplasia (MED) is characterized by a waddling gait, hip pain, and short stature, typically presenting in early childhood. Radiographs show flattened and irregular epiphyses, predominantly affecting the hips, knees, and ankles, with a relatively normal spine. Pseudoachondroplasia would typically show more severe short stature, disproportionate dwarfism, and significant metaphyseal involvement in addition to epiphyseal changes. Spondyloepiphyseal Dysplasia Congenita involves significant spinal changes (platyspondyly) and often presents at birth or in infancy.
Question 65
A 7-year-old girl with a known diagnosis of Multiple Epiphyseal Dysplasia (MED) is being evaluated for worsening knee pain. Her radiographs demonstrate irregular and fragmented epiphyses in the distal femurs and proximal tibias, with widening of the intercondylar notch. Which gene mutation is most commonly associated with the Fairbank type of MED?
View Answer & Explanation
Correct Answer: B
Rationale: Mutations in the COMP (cartilage oligomeric matrix protein) gene are the most common cause of the Fairbank type of Multiple Epiphyseal Dysplasia (MED), accounting for approximately 70% of cases. COL2A1 mutations are associated with Spondyloepiphyseal Dysplasia Congenita and some forms of Stickler syndrome. TRPV4 mutations are linked to some forms of MED and metatropic dysplasia. SLC26A2 mutations cause diastrophic dysplasia. FGFR3 mutations cause achondroplasia and hypochondroplasia, which are primarily growth plate disorders, not epiphyseal dysplasias.
Question 65
A 10-year-old boy with Multiple Epiphyseal Dysplasia (MED) is being considered for surgical intervention for severe bilateral coxa vara. His genetic testing revealed a mutation in the COMP gene. What is the typical inheritance pattern for MED caused by COMP mutations?
View Answer & Explanation
Correct Answer: C
Rationale: Multiple Epiphyseal Dysplasia (MED) caused by mutations in the COMP gene (Fairbank type) is inherited in an autosomal dominant pattern. This means only one copy of the mutated gene is needed to cause the disorder. Autosomal recessive inheritance is seen in some rarer forms of MED (e.g., DTDST/SLC26A2 mutations) and diastrophic dysplasia. X-linked inheritance patterns are not typical for MED.
Question 65
A newborn is noted to have severe short-trunk dwarfism, a barrel chest, and clubfeet. Radiographs reveal severe platyspondyly, delayed ossification of the epiphyses, and a pear-shaped vertebral body in the lumbar spine. The femoral necks are short and broad, and the epiphyses are small and irregular. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDC) is characterized by severe short-trunk dwarfism, platyspondyly (flattened vertebral bodies), and delayed epiphyseal ossification, often presenting at birth. The pear-shaped lumbar vertebral body is a classic radiographic sign. While MED and Pseudoachondroplasia involve epiphyseal changes, they typically present later in childhood and do not have the severe spinal involvement or congenital presentation of SEDC. Achondroplasia is a rhizomelic dwarfism with normal trunk length and different radiographic features (e.g., bullet-shaped vertebrae, short pedicles). Kniest dysplasia shares some features but often has more distinctive joint contractures and a "Swiss cheese" appearance of cartilage.
Question 65
A 3-year-old boy with Spondyloepiphyseal Dysplasia Congenita (SEDC) is being evaluated for progressive kyphoscoliosis. In addition to the characteristic platyspondyly and epiphyseal irregularities, what other common orthopedic finding is associated with SEDC?
View Answer & Explanation
Correct Answer: C
Rationale: Talipes equinovarus (clubfoot) is a common orthopedic finding associated with Spondyloepiphyseal Dysplasia Congenita (SEDC), often present at birth. Genu varum and valgum can occur, but clubfoot is more specifically associated with SEDC. Brachydactyly is not a primary feature. Metaphyseal flaring is more characteristic of metaphyseal dysplasias or rickets, not typically SEDC which is predominantly epiphyseal and spinal.
Question 65
A 5-year-old girl with Spondyloepiphyseal Dysplasia Congenita (SEDC) is undergoing genetic counseling. Her parents are concerned about the risk of recurrence in future pregnancies. Which gene mutation is responsible for SEDC?
View Answer & Explanation
Correct Answer: B
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDC) is caused by mutations in the COL2A1 gene, which encodes for type II collagen, a major component of cartilage. COL1A1 mutations are associated with osteogenesis imperfecta. COL10A1 mutations are linked to Schmid Metaphyseal Chondrodysplasia. COL11A1 and COL11A2 mutations are associated with Stickler syndrome and some forms of SED. COL9A1 mutations are associated with some forms of MED.
Question 65
A 12-year-old boy presents with progressive back pain and stiffness, particularly in the morning. He has a history of mild short stature, but his parents describe him as having a relatively normal appearance until early adolescence. Radiographs show generalized platyspondyly, particularly in the thoracic and lumbar spine, with irregular and flattened vertebral endplates. The peripheral epiphyses appear relatively normal or mildly irregular. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Spondyloepiphyseal Dysplasia Tarda (SEDT) typically presents in late childhood or early adolescence with back pain, stiffness, and mild short stature. Radiographs show characteristic generalized platyspondyly with irregular endplates, often with a "humped" or "camel-back" appearance of the vertebral bodies. SEDC presents at birth with more severe short stature. MED primarily affects peripheral epiphyses with less severe spinal involvement. Scheuermann's disease involves vertebral wedging and endplate irregularities but is not a generalized platyspondyly. Juvenile Idiopathic Arthritis would have more prominent inflammatory markers and joint effusions.
Question 65
A 14-year-old boy with Spondyloepiphyseal Dysplasia Tarda (SEDT) is being evaluated for hip pain. Radiographs of his hips would most likely show which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: While the primary involvement in SEDT is spinal, peripheral epiphyses, particularly the femoral heads, can also be affected. Radiographs typically show mild to moderate flattening and irregularity of the femoral heads, which can lead to premature osteoarthritis. Severe flattening and fragmentation are more characteristic of MED or SEDC. Metaphyseal flaring is not typical. Avascular necrosis can be a complication but is not the primary radiographic feature. Dysplastic acetabula with subluxation is more common in other conditions like developmental dysplasia of the hip or some forms of spondyloepimetaphyseal dysplasia.
Question 65
A 16-year-old male with Spondyloepiphyseal Dysplasia Tarda (SEDT) is undergoing genetic counseling. His mother is concerned about the risk for his younger brother. What is the inheritance pattern for SEDT?
View Answer & Explanation
Correct Answer: C
Rationale: Spondyloepiphyseal Dysplasia Tarda (SEDT) is inherited in an X-linked recessive pattern, caused by mutations in the TRAPPC2 gene (formerly SEDL). This explains why it predominantly affects males, with females typically being asymptomatic carriers. Autosomal dominant and recessive patterns are seen in other skeletal dysplasias but not SEDT.
Question 65
A 4-year-old boy presents with disproportionate short stature, a waddling gait, and joint laxity. His parents note that his trunk appears relatively normal in length, but his limbs are significantly shortened. Radiographs show irregular and fragmented epiphyses, particularly in the hips and knees, and prominent metaphyseal irregularities. The spine shows mild platyspondyly and anterior wedging. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Pseudoachondroplasia is characterized by disproportionate short stature (rhizomelic or mesomelic), waddling gait, and joint laxity, with onset typically in early childhood. Radiographs show significant epiphyseal and metaphyseal irregularities, distinguishing it from MED (primarily epiphyseal) and achondroplasia (primarily growth plate, with different radiographic features and no joint laxity). SEDC has more severe spinal involvement and presents congenitally. Hypochondroplasia is a milder form of achondroplasia.
Question 65
A 6-year-old girl with Pseudoachondroplasia is being evaluated for progressive genu valgum. Radiographs of her knees would most likely show which of the following features?
View Answer & Explanation
Correct Answer: B
Rationale: Pseudoachondroplasia is characterized by small, irregular, and fragmented epiphyses, along with irregular metaphyses, particularly prominent in the knees, hips, and ankles. This combination of epiphyseal and metaphyseal involvement is key. Normal epiphyses with metaphyseal flaring would suggest a metaphyseal dysplasia. Bullet-shaped vertebrae and short pedicles are characteristic of achondroplasia. Epiphyseal stippling is seen in chondrodysplasia punctata. Severe platyspondyly with pear-shaped lumbar vertebrae is characteristic of SEDC.
Question 65
A 9-year-old boy with Pseudoachondroplasia is undergoing genetic testing. Which gene mutation is responsible for this condition?
View Answer & Explanation
Correct Answer: B
Rationale: Pseudoachondroplasia is caused by mutations in the COMP (cartilage oligomeric matrix protein) gene, which is also associated with Multiple Epiphyseal Dysplasia (MED). The specific mutation and its effect on protein function determine the phenotype. COL2A1 mutations cause SEDC. MATN3 mutations are associated with a milder form of MED. TRPV4 mutations are linked to some forms of MED and metatropic dysplasia. DTDST (SLC26A2) mutations cause diastrophic dysplasia and some recessive forms of MED.
Question 65
A 2-year-old child presents with short stature, joint stiffness, and a "cauliflower ear" deformity. Radiographs show flattened and irregular epiphyses, particularly in the hips and knees, and significant metaphyseal flaring. The spine shows mild platyspondyly. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Diastrophic Dysplasia is characterized by short stature, joint contractures (stiffness), and distinctive features such as "cauliflower ear" (auricular hematoma and calcification), hitchhiker's thumb, and often clubfoot. Radiographs show epiphyseal and metaphyseal changes, often with cystic changes in the epiphyses. While MED and Pseudoachondroplasia involve epiphyseal changes, they lack the specific ear and thumb deformities. SEDC has more severe spinal involvement and different peripheral features. Kniest dysplasia has a "Swiss cheese" cartilage appearance and often cleft palate, but the ear deformity is less specific than in diastrophic dysplasia.
Question 65
A 15-year-old male with Spondyloepiphyseal Dysplasia Tarda (SEDT) is experiencing severe, debilitating hip pain due to advanced osteoarthritis. Conservative management has failed. What is the most appropriate surgical intervention for his hip pain?
View Answer & Explanation
Correct Answer: D
Rationale: For advanced osteoarthritis of the hip in a skeletally mature patient with a skeletal dysplasia, total hip arthroplasty (THA) is often the most effective treatment for pain relief and improved function. While osteotomies can be considered in younger patients with less severe disease, they are less effective for advanced arthritis. Hip arthrodesis is a salvage procedure that sacrifices motion and is generally reserved for cases where THA is not feasible or has failed. Core decompression is used for early avascular necrosis, not advanced osteoarthritis.
Question 65
A 1-year-old infant is diagnosed with Kniest Dysplasia. In addition to severe short stature and joint enlargement, what other systemic complication should be monitored in this child?
View Answer & Explanation
Correct Answer: C
Rationale: Kniest Dysplasia, caused by COL2A1 mutations, is often associated with progressive hearing loss, as well as ocular abnormalities (myopia, retinal detachment) and cleft palate. These are important systemic complications to monitor. Renal, cardiac, liver, and hematological issues are not typically primary features of Kniest Dysplasia.
Question 65
A newborn is found to have rhizomelic short stature, facial dysmorphism, and cataracts. Radiographs show characteristic punctate calcifications in the epiphyses, particularly around the hips and knees, and vertebral bodies. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Chondrodysplasia Punctata is characterized by rhizomelic short stature, facial dysmorphism, cataracts, and the pathognomonic radiographic finding of punctate calcifications (stippling) in the epiphyses and other cartilaginous structures. MED, SEDC, and Pseudoachondroplasia involve epiphyseal irregularities but not the distinct punctate calcifications. Achondroplasia has different radiographic features and does not typically involve cataracts or epiphyseal stippling.
Question 65
A 10-year-old boy presents with progressive joint pain and stiffness, particularly in the interphalangeal joints, wrists, and knees. He has mild short stature and a waddling gait. Radiographs show irregular, enlarged, and flattened epiphyses with joint space narrowing, resembling juvenile idiopathic arthritis. However, inflammatory markers are normal. Genetic testing reveals a mutation in the WISP3 gene. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Progressive Pseudorheumatoid Dysplasia (PPRD) is an autosomal recessive skeletal dysplasia caused by mutations in the WISP3 gene. It presents in early childhood with progressive joint pain, stiffness, and swelling, mimicking juvenile idiopathic arthritis (JIA), but without inflammatory markers. Radiographs show characteristic epiphyseal and metaphyseal irregularities, joint space narrowing, and often cystic changes. MED and SEDT have different genetic causes and typically less severe and widespread joint involvement mimicking arthritis. Pseudoachondroplasia has different radiographic features and often joint laxity rather than stiffness.
Question 65
A 7-year-old girl with Spondyloepiphyseal Dysplasia Congenita (SEDC) is being evaluated for visual problems. Which ocular finding is commonly associated with SEDC and other COL2A1-related disorders?
View Answer & Explanation
Correct Answer: B
Rationale: Retinal detachment, often secondary to severe myopia and vitreoretinal degeneration, is a common and serious ocular complication associated with Spondyloepiphyseal Dysplasia Congenita (SEDC) and other type II collagenopathies, including Stickler syndrome. Regular ophthalmologic surveillance is crucial. While strabismus and nystagmus can occur in children with visual impairment, retinal detachment is a specific and high-yield association with COL2A1 mutations.
Question 65
A 5-year-old boy presents with short stature, a waddling gait, and progressive genu valgum. His radiographs show irregular and flattened epiphyses, particularly in the hips and knees. His spine appears normal. His genetic testing is negative for COMP and COL2A1 mutations. Which of the following conditions, also primarily affecting epiphyses, should be considered in the differential diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of short stature, waddling gait, genu valgum, and irregular/flattened epiphyses with a normal spine is highly suggestive of Multiple Epiphyseal Dysplasia (MED). If COMP (Fairbank type) and COL2A1 (SEDC) are ruled out, other forms of MED, such as the Ribbing type (caused by MATN3 mutations), should be considered. Metaphyseal chondrodysplasia primarily affects metaphyses. Spondyloepimetaphyseal dysplasia involves both spine, epiphyses, and metaphyses. Achondroplasia and hypochondroplasia are growth plate disorders with different radiographic features and typically normal spines.
Question 65
A 13-year-old girl with Multiple Epiphyseal Dysplasia (MED) due to a COMP gene mutation is being evaluated for chronic hip pain. Her parents ask about the long-term prognosis for joint health. Which of the following is the most accurate statement regarding the prognosis of joints in patients with predominantly epiphyseal dysplasias?
View Answer & Explanation
Correct Answer: B
Rationale: Skeletal dysplasias with predominantly epiphyseal involvement, such as MED, lead to abnormal cartilage and bone formation in the joints. This predisposes patients to early-onset and progressive osteoarthritis, often requiring joint replacement (e.g., total hip arthroplasty) in adolescence or early adulthood. Joint function does not typically improve with age. While conservative management is initially attempted, it often fails to control pain in the long term. Spinal cord compression is a concern in some dysplasias (e.g., achondroplasia, SEDC), but not the primary long-term issue for peripheral joints in MED. Joint laxity can be seen in some dysplasias (e.g., pseudoachondroplasia), but progressive osteoarthritis is the hallmark of epiphyseal dysplasias.
Question 66
A 6-year-old boy presents with waddling gait and bilateral hip pain, worse with activity. His parents note he has always been shorter than his peers. Physical exam reveals limited range of motion in both hips, particularly abduction and internal rotation. Radiographs show flattened and irregular femoral epiphyses, especially at the femoral heads, and mild epiphyseal changes in the knees and ankles. The spine appears normal. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Multiple Epiphyseal Dysplasia (MED) is characterized by a waddling gait, hip pain, and short stature, typically presenting in early childhood. Radiographs show flattened and irregular epiphyses, predominantly affecting the hips, knees, and ankles, with a relatively normal spine. Pseudoachondroplasia would typically show more severe short stature, disproportionate dwarfism, and significant metaphyseal involvement in addition to epiphyseal changes. Spondyloepiphyseal Dysplasia Congenita involves significant spinal changes (platyspondyly) and often presents at birth or in infancy.
Question 67
A 7-year-old girl with a known diagnosis of Multiple Epiphyseal Dysplasia (MED) is being evaluated for worsening knee pain. Her radiographs demonstrate irregular and fragmented epiphyses in the distal femurs and proximal tibias, with widening of the intercondylar notch. Which gene mutation is most commonly associated with the Fairbank type of MED?
View Answer & Explanation
Correct Answer: B
Rationale: Mutations in the COMP (cartilage oligomeric matrix protein) gene are the most common cause of the Fairbank type of Multiple Epiphyseal Dysplasia (MED), accounting for approximately 70% of cases. COL2A1 mutations are associated with Spondyloepiphyseal Dysplasia Congenita and some forms of Stickler syndrome. TRPV4 mutations are linked to some forms of MED and metatropic dysplasia. SLC26A2 mutations cause diastrophic dysplasia. FGFR3 mutations cause achondroplasia and hypochondroplasia, which are primarily growth plate disorders, not epiphyseal dysplasias.
Question 68
A 10-year-old boy with Multiple Epiphyseal Dysplasia (MED) is being considered for surgical intervention for severe bilateral coxa vara. His genetic testing revealed a mutation in the COMP gene. What is the typical inheritance pattern for MED caused by COMP mutations?
View Answer & Explanation
Correct Answer: C
Rationale: Multiple Epiphyseal Dysplasia (MED) caused by mutations in the COMP gene (Fairbank type) is inherited in an autosomal dominant pattern. This means only one copy of the mutated gene is needed to cause the disorder. Autosomal recessive inheritance is seen in some rarer forms of MED (e.g., DTDST/SLC26A2 mutations) and diastrophic dysplasia. X-linked inheritance patterns are not typical for MED.
Question 69
A newborn is noted to have severe short-trunk dwarfism, a barrel chest, and clubfeet. Radiographs reveal severe platyspondyly, delayed ossification of the epiphyses, and a pear-shaped vertebral body in the lumbar spine. The femoral necks are short and broad, and the epiphyses are small and irregular. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDC) is characterized by severe short-trunk dwarfism, platyspondyly (flattened vertebral bodies), and delayed epiphyseal ossification, often presenting at birth. The pear-shaped lumbar vertebral body is a classic radiographic sign. While MED and Pseudoachondroplasia involve epiphyseal changes, they typically present later in childhood and do not have the severe spinal involvement or congenital presentation of SEDC. Achondroplasia is a rhizomelic dwarfism with normal trunk length and different radiographic features (e.g., bullet-shaped vertebrae, short pedicles). Kniest dysplasia shares some features but often has more distinctive joint contractures and a "Swiss cheese" appearance of cartilage.
Question 70
A 3-year-old boy with Spondyloepiphyseal Dysplasia Congenita (SEDC) is being evaluated for progressive kyphoscoliosis. In addition to the characteristic platyspondyly and epiphyseal irregularities, what other common orthopedic finding is associated with SEDC?
View Answer & Explanation
Correct Answer: C
Rationale: Talipes equinovarus (clubfoot) is a common orthopedic finding associated with Spondyloepiphyseal Dysplasia Congenita (SEDC), often present at birth. Genu varum and valgum can occur, but clubfoot is more specifically associated with SEDC. Brachydactyly is not a primary feature. Metaphyseal flaring is more characteristic of metaphyseal dysplasias or rickets, not typically SEDC which is predominantly epiphyseal and spinal.
Question 71
A 5-year-old girl with Spondyloepiphyseal Dysplasia Congenita (SEDC) is undergoing genetic counseling. Her parents are concerned about the risk of recurrence in future pregnancies. Which gene mutation is responsible for SEDC?
View Answer & Explanation
Correct Answer: B
Rationale: Spondyloepiphyseal Dysplasia Congenita (SEDC) is caused by mutations in the COL2A1 gene, which encodes for type II collagen, a major component of cartilage. COL1A1 mutations are associated with osteogenesis imperfecta. COL10A1 mutations are linked to Schmid Metaphyseal Chondrodysplasia. COL11A1 and COL11A2 mutations are associated with Stickler syndrome and some forms of SED. COL9A1 mutations are associated with some forms of MED.
Question 72
A 12-year-old boy presents with progressive back pain and stiffness, particularly in the morning. He has a history of mild short stature, but his parents describe him as having a relatively normal appearance until early adolescence. Radiographs show generalized platyspondyly, particularly in the thoracic and lumbar spine, with irregular and flattened vertebral endplates. The peripheral epiphyses appear relatively normal or mildly irregular. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Spondyloepiphyseal Dysplasia Tarda (SEDT) typically presents in late childhood or early adolescence with back pain, stiffness, and mild short stature. Radiographs show characteristic generalized platyspondyly with irregular endplates, often with a "humped" or "camel-back" appearance of the vertebral bodies. SEDC presents at birth with more severe short stature. MED primarily affects peripheral epiphyses with less severe spinal involvement. Scheuermann's disease involves vertebral wedging and endplate irregularities but is not a generalized platyspondyly. Juvenile Idiopathic Arthritis would have more prominent inflammatory markers and joint effusions.
Question 73
A 14-year-old boy with Spondyloepiphyseal Dysplasia Tarda (SEDT) is being evaluated for hip pain. Radiographs of his hips would most likely show which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: While the primary involvement in SEDT is spinal, peripheral epiphyses, particularly the femoral heads, can also be affected. Radiographs typically show mild to moderate flattening and irregularity of the femoral heads, which can lead to premature osteoarthritis. Severe flattening and fragmentation are more characteristic of MED or SEDC. Metaphyseal flaring is not typical. Avascular necrosis can be a complication but is not the primary radiographic feature. Dysplastic acetabula with subluxation is more common in other conditions like developmental dysplasia of the hip or some forms of spondyloepimetaphyseal dysplasia.
Question 74
A 16-year-old male with Spondyloepiphyseal Dysplasia Tarda (SEDT) is undergoing genetic counseling. His mother is concerned about the risk for his younger brother. What is the inheritance pattern for SEDT?
View Answer & Explanation
Correct Answer: C
Rationale: Spondyloepiphyseal Dysplasia Tarda (SEDT) is inherited in an X-linked recessive pattern, caused by mutations in the TRAPPC2 gene (formerly SEDL). This explains why it predominantly affects males, with females typically being asymptomatic carriers. Autosomal dominant and recessive patterns are seen in other skeletal dysplasias but not SEDT.
Question 75
A 4-year-old boy presents with disproportionate short stature, a waddling gait, and joint laxity. His parents note that his trunk appears relatively normal in length, but his limbs are significantly shortened. Radiographs show irregular and fragmented epiphyses, particularly in the hips and knees, and prominent metaphyseal irregularities. The spine shows mild platyspondyly and anterior wedging. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Pseudoachondroplasia is characterized by disproportionate short stature (rhizomelic or mesomelic), waddling gait, and joint laxity, with onset typically in early childhood. Radiographs show significant epiphyseal and metaphyseal irregularities, distinguishing it from MED (primarily epiphyseal) and achondroplasia (primarily growth plate, with different radiographic features and no joint laxity). SEDC has more severe spinal involvement and presents congenitally. Hypochondroplasia is a milder form of achondroplasia.
Question 76
A 6-year-old girl with Pseudoachondroplasia is being evaluated for progressive genu valgum. Radiographs of her knees would most likely show which of the following features?
View Answer & Explanation
Correct Answer: B
Rationale: Pseudoachondroplasia is characterized by small, irregular, and fragmented epiphyses, along with irregular metaphyses, particularly prominent in the knees, hips, and ankles. This combination of epiphyseal and metaphyseal involvement is key. Normal epiphyses with metaphyseal flaring would suggest a metaphyseal dysplasia. Bullet-shaped vertebrae and short pedicles are characteristic of achondroplasia. Epiphyseal stippling is seen in chondrodysplasia punctata. Severe platyspondyly with pear-shaped lumbar vertebrae is characteristic of SEDC.
Question 77
A 9-year-old boy with Pseudoachondroplasia is undergoing genetic testing. Which gene mutation is responsible for this condition?
View Answer & Explanation
Correct Answer: B
Rationale: Pseudoachondroplasia is caused by mutations in the COMP (cartilage oligomeric matrix protein) gene, which is also associated with Multiple Epiphyseal Dysplasia (MED). The specific mutation and its effect on protein function determine the phenotype. COL2A1 mutations cause SEDC. MATN3 mutations are associated with a milder form of MED. TRPV4 mutations are linked to some forms of MED and metatropic dysplasia. DTDST (SLC26A2) mutations cause diastrophic dysplasia and some recessive forms of MED.
Question 78
A 2-year-old child presents with short stature, joint stiffness, and a "cauliflower ear" deformity. Radiographs show flattened and irregular epiphyses, particularly in the hips and knees, and significant metaphyseal flaring. The spine shows mild platyspondyly. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Diastrophic Dysplasia is characterized by short stature, joint contractures (stiffness), and distinctive features such as "cauliflower ear" (auricular hematoma and calcification), hitchhiker's thumb, and often clubfoot. Radiographs show epiphyseal and metaphyseal changes, often with cystic changes in the epiphyses. While MED and Pseudoachondroplasia involve epiphyseal changes, they lack the specific ear and thumb deformities. SEDC has more severe spinal involvement and different peripheral features. Kniest dysplasia has a "Swiss cheese" cartilage appearance and often cleft palate, but the ear deformity is less specific than in diastrophic dysplasia.
Question 79
A 15-year-old male with Spondyloepiphyseal Dysplasia Tarda (SEDT) is experiencing severe, debilitating hip pain due to advanced osteoarthritis. Conservative management has failed. What is the most appropriate surgical intervention for his hip pain?
View Answer & Explanation
Correct Answer: D
Rationale: For advanced osteoarthritis of the hip in a skeletally mature patient with a skeletal dysplasia, total hip arthroplasty (THA) is often the most effective treatment for pain relief and improved function. While osteotomies can be considered in younger patients with less severe disease, they are less effective for advanced arthritis. Hip arthrodesis is a salvage procedure that sacrifices motion and is generally reserved for cases where THA is not feasible or has failed. Core decompression is used for early avascular necrosis, not advanced osteoarthritis.
Question 80
A 1-year-old infant is diagnosed with Kniest Dysplasia. In addition to severe short stature and joint enlargement, what other systemic complication should be monitored in this child?
View Answer & Explanation
Correct Answer: C
Rationale: Kniest Dysplasia, caused by COL2A1 mutations, is often associated with progressive hearing loss, as well as ocular abnormalities (myopia, retinal detachment) and cleft palate. These are important systemic complications to monitor. Renal, cardiac, liver, and hematological issues are not typically primary features of Kniest Dysplasia.
Question 81
A newborn is found to have rhizomelic short stature, facial dysmorphism, and cataracts. Radiographs show characteristic punctate calcifications in the epiphyses, particularly around the hips and knees, and vertebral bodies. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Chondrodysplasia Punctata is characterized by rhizomelic short stature, facial dysmorphism, cataracts, and the pathognomonic radiographic finding of punctate calcifications (stippling) in the epiphyses and other cartilaginous structures. MED, SEDC, and Pseudoachondroplasia involve epiphyseal irregularities but not the distinct punctate calcifications. Achondroplasia has different radiographic features and does not typically involve cataracts or epiphyseal stippling.
Question 82
A 10-year-old boy presents with progressive joint pain and stiffness, particularly in the interphalangeal joints, wrists, and knees. He has mild short stature and a waddling gait. Radiographs show irregular, enlarged, and flattened epiphyses with joint space narrowing, resembling juvenile idiopathic arthritis. However, inflammatory markers are normal. Genetic testing reveals a mutation in the WISP3 gene. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Progressive Pseudorheumatoid Dysplasia (PPRD) is an autosomal recessive skeletal dysplasia caused by mutations in the WISP3 gene. It presents in early childhood with progressive joint pain, stiffness, and swelling, mimicking juvenile idiopathic arthritis (JIA), but without inflammatory markers. Radiographs show characteristic epiphyseal and metaphyseal irregularities, joint space narrowing, and often cystic changes. MED and SEDT have different genetic causes and typically less severe and widespread joint involvement mimicking arthritis. Pseudoachondroplasia has different radiographic features and often joint laxity rather than stiffness.
Question 83
A 7-year-old girl with Spondyloepiphyseal Dysplasia Congenita (SEDC) is being evaluated for visual problems. Which ocular finding is commonly associated with SEDC and other COL2A1-related disorders?
View Answer & Explanation
Correct Answer: B
Rationale: Retinal detachment, often secondary to severe myopia and vitreoretinal degeneration, is a common and serious ocular complication associated with Spondyloepiphyseal Dysplasia Congenita (SEDC) and other type II collagenopathies, including Stickler syndrome. Regular ophthalmologic surveillance is crucial. While strabismus and nystagmus can occur in children with visual impairment, retinal detachment is a specific and high-yield association with COL2A1 mutations.
Question 84
A 5-year-old boy presents with short stature, a waddling gait, and progressive genu valgum. His radiographs show irregular and flattened epiphyses, particularly in the hips and knees. His spine appears normal. His genetic testing is negative for COMP and COL2A1 mutations. Which of the following conditions, also primarily affecting epiphyses, should be considered in the differential diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of short stature, waddling gait, genu valgum, and irregular/flattened epiphyses with a normal spine is highly suggestive of Multiple Epiphyseal Dysplasia (MED). If COMP (Fairbank type) and COL2A1 (SEDC) are ruled out, other forms of MED, such as the Ribbing type (caused by MATN3 mutations), should be considered. Metaphyseal chondrodysplasia primarily affects metaphyses. Spondyloepimetaphyseal dysplasia involves both spine, epiphyses, and metaphyses. Achondroplasia and hypochondroplasia are growth plate disorders with different radiographic features and typically normal spines.
Question 85
A 7-year-old male presents with a 2-month history of localized pain and swelling over his left parietal skull. Physical examination reveals a tender, firm, non-mobile mass. Radiographs demonstrate a well-defined lytic lesion in the parietal bone.
View Answer & Explanation
Correct Answer: A
Rationale: Langerhans Cell Histiocytosis (LCH) is a hematopoietic condition that commonly affects patients under 30, with a predilection for the skull, presenting with pain and swelling of the involved bone. Osteosarcoma and Ewing Sarcoma are malignant bone tumors that can present with lytic lesions and pain, but LCH is a more common consideration for a lytic skull lesion in this age group. Osteomyelitis is an infection, and while it can cause lytic lesions, the clinical picture here is more suggestive of LCH. Fibrous dysplasia typically presents as a ground-glass lesion rather than a purely lytic one.
Question 86
A 12-year-old female presents with a 3-month history of persistent pain and swelling localized to her right rib cage. Physical examination reveals tenderness and a palpable mass over the 7th rib. Radiographs show a lytic lesion within the rib. Given the predilection of Langerhans Cell Histiocytosis (LCH), which of the following bones is also a common site for involvement?
View Answer & Explanation
Correct Answer: A
Rationale: The provided text states that LCH has a predilection for the skull, femur, ribs, and ilium. Therefore, the skull is a commonly affected bone. The tibia, humerus, patella, and phalanges are less common sites of predilection for LCH compared to the skull, ribs, femur, and ilium.
Question 87
A 16-year-old male presents with a 6-month history of increasing pain in his left hip, with radiographs showing a lytic lesion in the ilium. He also reports new onset of excessive thirst and frequent urination. Physical examination is otherwise unremarkable. What systemic complication is most commonly associated with Langerhans Cell Histiocytosis (LCH) in this context?
View Answer & Explanation
Correct Answer: A
Rationale: The clinical vignette describes polyuria and polydipsia, which are classic symptoms of diabetes insipidus. The provided text explicitly states that "Patients may develop diabetes insipidus" in the context of Langerhans Cell Histiocytosis. Hypercalcemia, renal failure, hypothyroidism, and adrenal insufficiency are not specifically mentioned as common systemic complications of LCH in the provided text.
Question 88
A 5-year-old girl is brought to the clinic due to progressive hearing loss in her right ear over the past 3 months. Physical examination reveals a bulging tympanic membrane and a tender mastoid process. CT scan of the temporal bone shows a destructive lesion involving the mastoid. What is the most likely underlying diagnosis?
View Answer & Explanation
Correct Answer: A
Rationale: The provided text specifically states, "Those with mastoid involvement may have hearing loss" in the context of Langerhans Cell Histiocytosis. While cholesteatoma, chronic otitis media, and mastoiditis can cause hearing loss and mastoid involvement, the presence of a destructive lesion in a young child, combined with the specific association mentioned in the text, makes LCH the most likely diagnosis. Rhabdomyosarcoma is a rare malignant tumor but not specifically linked to mastoid involvement and hearing loss in the provided text.
Question 89
A 3-year-old boy presents with a rapidly enlarging, tender mass on his scalp. Physical examination reveals a palpable, firm lesion over the left parietal region. Radiographs of the skull, similar to the image provided, demonstrate significant bone destruction.
View Answer & Explanation
Correct Answer: A
Rationale: The image (Fig. 11.42) is explicitly captioned as "Destruction of skull secondary to Langerhans cell histiocytosis." This, combined with the clinical vignette of a young child with a rapidly enlarging, tender skull mass and lytic destruction, strongly points to LCH. While other conditions can cause lytic skull lesions, the direct correlation with the provided image and its caption makes LCH the definitive answer. Metastatic neuroblastoma can cause lytic lesions, but the image is specifically labeled for LCH. Epidermoid cysts are typically well-demarcated and less destructive, and fibrous dysplasia has a characteristic ground-glass appearance.
Question 90
A 10-year-old girl is brought to the clinic by her parents due to a noticeable, progressive enlargement of her skull over the past few months. Physical examination reveals a prominent, firm, non-tender mass on the left side of her head, as depicted in a clinical photograph similar to the one provided.

View Answer & Explanation
Correct Answer: A
Rationale: The image (Fig. 11.43) is captioned as "Clinical photograph at the time of surgery showing enlargement of the skull" in the context of Langerhans Cell Histiocytosis. This direct association, along with the clinical presentation of skull enlargement in a child, makes LCH the most likely diagnosis. Paget's disease typically affects older adults. Osteomas are usually smaller, solitary, and benign. Meningiomas are intracranial tumors, and while they can cause skull changes, the image specifically relates to LCH. A subgaleal hematoma would typically be acute and resolve, not cause progressive enlargement.
Question 91
A 6-year-old boy undergoes a biopsy of a lytic lesion in his femur. Histological examination, similar to the description provided, reveals a mixed cellular infiltrate. The pathologist identifies characteristic cells with an indented nucleus and small nucleoli.
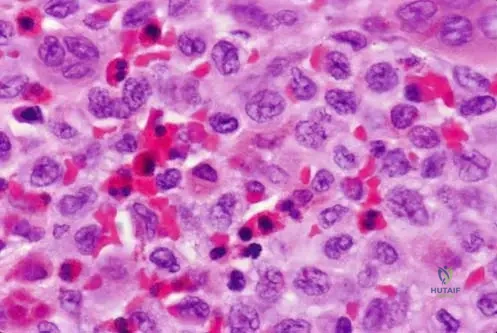
View Answer & Explanation
Correct Answer: A
Rationale: The provided text and image caption (Fig. 11.44) explicitly state that "Langerhans cells usually have an indented nucleus and small nucleoli." This is the defining characteristic of the pathological cell in Langerhans Cell Histiocytosis. While plasma cells, eosinophils, and other inflammatory cells are present, and macrophages are related, the specific description points directly to Langerhans cells. Osteoclasts are involved in bone resorption but do not have this specific nuclear morphology in the context of LCH.
Question 92
A biopsy of a destructive bone lesion from a 14-year-old male, consistent with Langerhans Cell Histiocytosis, is examined histologically. The report notes a mixed inflammatory infiltrate. In addition to the primary pathological cells, which other inflammatory cell type is frequently abundant in these lesions, as described in the provided text?
View Answer & Explanation
Correct Answer: A
Rationale: The provided text states, "Histologically, lesions are composed of many cell types, including histiocytes, plasma cells, eosinophils, and other inflammatory cells... There may be many eosinophils present." Therefore, eosinophils are frequently abundant. While other inflammatory cells may be present, eosinophils are specifically highlighted as often numerous. Neutrophils, lymphocytes, basophils, and mast cells are not specifically mentioned as being frequently abundant in the provided text.
Question 93
A 10-year-old presents with a painful lytic lesion in the femur. Biopsy confirms Langerhans Cell Histiocytosis. Based on the provided information, this condition is best characterized as a:
View Answer & Explanation
Correct Answer: A
Rationale: The first sentence of the provided text states, "This is a hematopoietic condition that can affect a variety of ages..." This directly characterizes LCH. While it can mimic a tumor or infection clinically, its underlying pathology is hematopoietic. It is not classified as a metabolic bone disease.
Question 94
A 5-year-old presents with localized pain and swelling over a rib, which has been present for several weeks. Physical examination reveals a tender, firm mass. Radiographs show a lytic lesion within the rib. Biopsy confirms Langerhans Cell Histiocytosis. Which statement best describes the typical presentation of this condition?
View Answer & Explanation
Correct Answer: A
Rationale: The provided text states, "Lesions tend to be symptomatic (pain, swelling) and only rarely will an area of histiocytosis be discovered incidentally." This directly supports that pain and swelling are the most common clinical findings. Therefore, options B and C are incorrect. While pathological fractures can occur, the text emphasizes pain and swelling as the most common findings, and fever and chills are not highlighted as common associations.
Question 95
A 25-year-old female presents with a 4-month history of progressive pain and swelling over her right ilium. Physical examination reveals a palpable, tender mass. Radiographs show a lytic lesion in the iliac wing. Biopsy confirms Langerhans Cell Histiocytosis. While this condition can affect a variety of ages, the majority of patients are typically under what age?
View Answer & Explanation
Correct Answer: A
Rationale: The provided text states, "This is a hematopoietic condition that can affect a variety of ages, although most patients are under age 30." This directly answers the question. While many patients are children (under 10 or 20), the broader category for "most patients" is under 30. The other age ranges are either too specific or too broad based on the text.
Question 96
A 7-year-old boy presents with a palpable, tender mass on his skull, which has been slowly growing for several weeks. Physical examination confirms a firm, non-mobile mass over the frontal bone. Radiographs reveal a lytic lesion with ill-defined margins. Given the common presentation and affected sites, which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: A
Rationale: Langerhans Cell Histiocytosis commonly affects children under 30 and has a strong predilection for the skull, presenting with pain and swelling (or a palpable mass) and lytic lesions. Osteosarcoma and Ewing Sarcoma are malignant bone tumors that can occur in this age group but are less common in the skull compared to LCH. Fibrous dysplasia typically has a "ground-glass" appearance, and osteoid osteoma is usually smaller and associated with a nidus and reactive sclerosis, not diffuse lytic destruction of this nature.
Question 97
A 15-year-old male presents with localized pain and swelling in his distal femur, which has worsened over 2 months. Physical examination reveals tenderness and warmth over the affected area. Radiographs show a lytic lesion in the metadiaphyseal region of the femur. Which of the following conditions, known for its predilection for the femur, is the most likely diagnosis?
View Answer & Explanation
Correct Answer: A
Rationale: The provided text explicitly lists the femur as a bone with a predilection for Langerhans Cell Histiocytosis. The clinical presentation of pain, swelling, and a lytic lesion in an adolescent is consistent with LCH. Osteochondromas are exostoses. Non-ossifying fibromas and enchondromas are typically asymptomatic and often incidental findings, though they can cause pain if fractured. Simple bone cysts are usually metaphyseal and often asymptomatic until fracture.
Question 98
A 6-year-old girl presents with chest wall pain and a palpable mass over her left 5th rib. Physical examination confirms a tender, firm mass. Imaging reveals a lytic lesion of the rib. Based on the provided information, what is the most likely diagnosis?
View Answer & Explanation
Correct Answer: A
Rationale: The provided text lists the ribs as a site of predilection for Langerhans Cell Histiocytosis, which commonly presents with pain, swelling, and lytic lesions in children. Chondrosarcoma is rare in this age group. Metastatic neuroblastoma is a possibility for lytic lesions in children, but LCH is a primary consideration given the specific predilection mentioned. A rib fracture would typically have a clear traumatic history and different radiographic appearance. Costochondritis is inflammation of cartilage, not a lytic bone lesion.
Question 99
Question 99
A 7-year-old male presents with a several-month history of a progressively enlarging, painful mass on his scalp. Physical examination reveals a palpable, tender, firm lesion over the parietal bone. Radiographs demonstrate a lytic lesion with ill-defined margins in the skull. Given the suspected diagnosis of Langerhans Cell Histiocytosis, which of the following bones is also a common site of involvement?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text states that while any bone may be affected, there is a predilection for the skull, femur, ribs, and ilium. Therefore, the femur is a common site of involvement. The other options are less commonly cited as predilection sites for LCH in the provided text.
Question 99
A 5-year-old female is diagnosed with Langerhans Cell Histiocytosis after presenting with a painful swelling in her rib. During her workup, the orthopaedic surgeon is aware that patients with LCH can develop systemic complications. Which of the following endocrine disorders is specifically mentioned as a potential complication?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states, "Patients may develop diabetes insipidus." This is a known systemic complication of LCH, particularly when the pituitary gland or hypothalamus is involved. The other endocrine disorders are not mentioned in the provided text as specific complications of LCH.
Question 99
A 12-year-old male undergoes a biopsy for a lytic lesion in his ilium, suspected to be Langerhans Cell Histiocytosis. Histological examination is performed. Which of the following cell types is a characteristic feature of LCH lesions, often described with an indented nucleus?
View Answer & Explanation
Correct Answer: D
Rationale: The provided histological description states, "Langerhans cells usually have an indented nucleus and small nucleoli." While plasma cells are also present, the Langerhans cell itself is the pathognomonic cell type with the described nuclear morphology and gives the condition its name.
Question 99
A 3-year-old female presents with a palpable swelling on her forehead. Radiographs of the skull reveal a destructive lesion. A biopsy confirms Langerhans Cell Histiocytosis. Which of the following best describes the typical radiographic appearance of such a lesion in the skull?
View Answer & Explanation
Correct Answer: C
Rationale: Figure 11.42 is captioned "Destruction of skull secondary to Langerhans cell histiocytosis," indicating a destructive pattern. The image itself shows an area of bone loss. While the text doesn't explicitly describe "ill-defined margins," destructive lesions often present this way, and it aligns with the image. Sclerotic lesions or well-circumscribed lesions with sclerotic rims are not characteristic of the destructive nature shown.
Question 99
A 15-year-old male presents with persistent pain and swelling in his left hip. Imaging reveals a lytic lesion in the ilium. A biopsy is performed, confirming Langerhans Cell Histiocytosis. Based on the provided information, which of the following statements regarding the presentation of LCH is most accurate?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Lesions tend to be symptomatic (pain, swelling) and only rarely will an area of histiocytosis be discovered incidentally." This directly supports option C. Options A, B, and D contradict the provided information regarding symptoms, common sites, and age range, respectively. The text does not comment on the benign nature or intervention requirements.
Question 99
A 2-year-old child is evaluated for a new onset of hearing loss. Physical examination reveals no obvious external ear abnormalities. Imaging studies show a lytic lesion involving the mastoid bone. A biopsy is planned to investigate for Langerhans Cell Histiocytosis. What is the specific association between mastoid involvement and hearing loss in LCH?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "Those with mastoid involvement may have hearing loss." This directly confirms the association without specifying the exact type of hearing loss (conductive vs. sensorineural) or mechanism. Therefore, the most accurate answer based strictly on the provided text is that mastoid involvement is associated with hearing loss.
Question 99
A 10-year-old girl presents with a painful swelling over her left rib. Radiographs show a lytic lesion. A biopsy is performed, and the pathologist notes the presence of numerous eosinophils in addition to other inflammatory cells. Which of the following cell types is also typically abundant in Langerhans Cell Histiocytosis lesions, as described histologically?
View Answer & Explanation
Correct Answer: D
Rationale: The histological description states, "Histologically, lesions are composed of many cell types, including histiocytes, plasma cells, eosinophils, and other inflammatory cells." Therefore, plasma cells are explicitly mentioned as being present in LCH lesions. While macrophages and lymphocytes are generally inflammatory cells, plasma cells are specifically listed in the context of LCH histology.
Question 99
A 4-year-old boy is diagnosed with Langerhans Cell Histiocytosis affecting his skull. His parents inquire about the typical age range for this condition. Based on the provided clinical information, which statement best describes the age distribution of LCH?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Th is is a hematopoietic condition that can aff ect a variety of ages, although most patients are under age 30." This directly supports option C. The other options contradict this statement regarding the typical age distribution.
Question 99
A 25-year-old male presents with a painful, enlarging mass in his left femur. Radiographs show a lytic lesion. A biopsy is performed, and the pathology report describes a lesion composed of histiocytes, plasma cells, and numerous eosinophils. What is the characteristic nuclear feature of the Langerhans cells often observed in these lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The histological description explicitly states, "Langerhans cells usually have an indented nucleus and small nucleoli." This is a key diagnostic feature of Langerhans cells in LCH.
Question 99
A 6-year-old boy presents with a painful swelling in his skull, confirmed to be Langerhans Cell Histiocytosis. His parents ask about the origin of this condition. Based on the provided information, LCH is classified as which type of condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text begins by stating, "Th is is a hematopoietic condition that can aff ect a variety of ages..." This directly classifies LCH as a hematopoietic condition.
Question 99
A 1-year-old infant is found to have an enlarging skull lesion. Clinical examination reveals a soft, palpable mass. Radiographs show a lytic defect in the skull. A biopsy is performed, confirming Langerhans Cell Histiocytosis. What is the most common clinical finding associated with LCH lesions?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Pain and swelling of the involved bone are the most common clinical fi ndings." This directly answers the question. The other options are not mentioned as the most common clinical findings in the provided text.
Question 99
A 14-year-old male presents with a several-week history of a tender, enlarging area on his forehead. Clinically, there is a noticeable enlargement of the skull in the affected region. Imaging confirms a destructive lesion. A biopsy is planned for suspected Langerhans Cell Histiocytosis. What does the clinical photograph of a skull lesion in LCH typically demonstrate?
View Answer & Explanation
Correct Answer: C
Rationale: Figure 11.43 is captioned, "Clinical photograph at the time of surgery showing enlargement of the skull." This directly indicates that enlargement of the skull is a typical clinical finding.
Question 99
A 9-year-old girl presents with a painful lump on her back. Radiographs reveal a lytic lesion in a rib. A biopsy confirms Langerhans Cell Histiocytosis. Besides the skull, femur, and ilium, which other bone is specifically mentioned as a predilection site for LCH?
View Answer & Explanation
Correct Answer: D
Rationale: The text states, "Any bone may be aff ected, but there is a predilection for the skull, femur, ribs, and ilium." Therefore, ribs are explicitly listed as a predilection site.
Question 99
A 2-year-old male presents with a painful, enlarging mass on his scalp. Radiographs show a destructive lesion in the parietal bone. A biopsy is performed, and the pathologist identifies numerous eosinophils and cells with indented nuclei. What is the primary cell type that gives Langerhans Cell Histiocytosis its name and is characterized by these indented nuclei?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Histologically, lesions are composed of many cell types, including histiocytes, plasma cells, eosinophils, and other infl ammatory cells. Langerhans cells usually have an indented nucleus..." Langerhans cells are a type of histiocyte. The condition is named after these specialized histiocytes. While eosinophils and plasma cells are present, histiocytes (specifically Langerhans cells) are the defining cell type.
Question 99
A 17-year-old female is diagnosed with Langerhans Cell Histiocytosis after presenting with a painful lesion in her ilium. Her physician is reviewing the potential systemic manifestations of LCH. Which of the following statements accurately describes the typical presentation of LCH lesions regarding symptoms?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Lesions tend to be symptomatic (pain, swelling) and only rarely will an area of histiocytosis be discovered incidentally." This directly supports option C and refutes options A and B.
Question 99
A 28-year-old male presents with a new onset of polyuria and polydipsia, along with a painful lesion in his skull. Imaging confirms a destructive lesion, and a biopsy reveals Langerhans Cell Histiocytosis. The patient's endocrine symptoms are consistent with diabetes insipidus. This systemic complication is a result of LCH affecting which part of the body?
View Answer & Explanation
Correct Answer: C
Rationale: While the provided text only states "Patients may develop diabetes insipidus," it is common knowledge in orthopaedic oncology that diabetes insipidus in LCH results from involvement of the pituitary gland or hypothalamus, which controls antidiuretic hormone (ADH) secretion. This question tests the understanding of the mechanism behind the stated complication.
Question 99
A 5-year-old boy presents with a painful swelling over his left parietal bone. Radiographs show a lytic lesion. A biopsy is performed, and the histological findings include a mixed inflammatory infiltrate with numerous eosinophils. Which of the following statements regarding the eosinophil presence in LCH lesions is accurate?
View Answer & Explanation
Correct Answer: C
Rationale: The histological description states, "Histologically, lesions are composed of many cell types, including histiocytes, plasma cells, eosinophils, and other infl ammatory cells... There may be many eosinophils present." This directly supports option C.
Question 99
A 19-year-old male presents with a painful, enlarging mass in his right femur. Imaging reveals a lytic lesion. A biopsy confirms Langerhans Cell Histiocytosis. Given the hematopoietic nature of LCH, which of the following best describes its origin?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Th is is a hematopoietic condition..." Hematopoietic refers to the formation of blood cellular components. Therefore, it is derived from cells of the blood-forming system.
Question 99
A 10-year-old female presents with a several-month history of a painful, palpable mass on her left rib. Radiographs show a lytic lesion. A biopsy is performed, confirming Langerhans Cell Histiocytosis. Which of the following statements accurately reflects the typical presentation of LCH in terms of symptom onset?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Lesions tend to be symptomatic (pain, swelling) and only rarely will an area of histiocytosis be discovered incidentally." This directly supports option C. Options A and B are contradicted by the text.
Question 99
A 7-year-old male presents with a painful, enlarging mass in his skull. Imaging reveals a destructive lesion. A biopsy is performed, and the pathologist notes the presence of histiocytes, plasma cells, and eosinophils. The Langerhans cells are described as having an indented nucleus and small nucleoli. Which of these cell types is considered the defining characteristic cell of this condition?
View Answer & Explanation
Correct Answer: D
Rationale: The condition is named Langerhans Cell Histiocytosis, and the text describes "Langerhans cells usually have an indented nucleus and small nucleoli." While plasma cells and eosinophils are present, the Langerhans cell (a type of histiocyte) is the defining and characteristic cell type for this condition.
Question 100
A 7-year-old male presents with a several-month history of a progressively enlarging, painful mass on his scalp. Physical examination reveals a palpable, tender, firm lesion over the parietal bone. Radiographs demonstrate a lytic lesion with ill-defined margins in the skull. Given the suspected diagnosis of Langerhans Cell Histiocytosis, which of the following bones is also a common site of involvement?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text states that while any bone may be affected, there is a predilection for the skull, femur, ribs, and ilium. Therefore, the femur is a common site of involvement. The other options are less commonly cited as predilection sites for LCH in the provided text.
