Master ABOS Board Review: Skeletal Dysplasias & Metabolic Bone Diseases | Part 2
Key Takeaway
This ABOS Board Review covers essential orthopedic bone disorders including Cleidocranial Dysplasia (CCD), Osteogenesis Imperfecta (OI), and Hyperparathyroidism. Key topics include genetic inheritance, classic diagnostic signs, skeletal and non-skeletal manifestations, radiographic findings, and management strategies for these complex conditions. Ideal for exam preparation.
Question 1
A 7-year-old boy is brought to the clinic by his parents who are concerned about his unusual ability to approximate his shoulders anteriorly. Physical examination reveals a large, brachycephalic head with prominent frontal bossing and a wide, flat nasal bridge. Oral examination shows a high-arched palate and several unerupted teeth. Radiographs of the chest confirm bilateral clavicular hypoplasia.
View Answer & Explanation
Correct Answer: A
Rationale: Cleidocranial dysplasia (CCD) is explicitly stated to be a rare disorder of autosomal dominant inheritance. Autosomal recessive is incorrect as it does not describe the genetic pattern for CCD.
Question 2
A 10-year-old girl presents with a history of delayed tooth eruption and an unusual flexibility in her shoulder girdle. On examination, she demonstrates the ability to bring her shoulders together in front of her chest. Her skull appears large with wide sutures. Which of the following is the MOST characteristic skeletal finding responsible for her shoulder flexibility?
View Answer & Explanation
Correct Answer: C
Rationale: The ability to approximate the shoulders anteriorly is described as the classic diagnostic sign of cleidocranial dysplasia, directly related to clavicle hypoplasia or aplasia. Scapular dyskinesis is incorrect as it refers to abnormal scapular movement, not the underlying structural cause of shoulder approximation in CCD.
Question 3
A 5-year-old child is diagnosed with cleidocranial dysplasia. The parents inquire about potential long-term orthopedic issues. Based on the typical presentation of CCD, which of the following skeletal regions, in addition to the cranial vault and clavicles, is commonly affected?

View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that CCD causes disturbances in the growth of bones of the cranial vault, clavicles, maxilla, nasal and lacrimal bones, and the pelvis. The vertebral column is incorrect as it is not listed as a commonly affected region in the provided text.
Question 4
An 8-year-old boy with a known diagnosis of cleidocranial dysplasia presents for a routine check-up. His parents report concerns about his overall height. What is a common finding regarding stature in individuals with CCD?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context states, "Mild shortening of stature may be seen." Significantly increased stature is incorrect as the opposite is described.
Question 5
A 6-year-old girl is suspected of having cleidocranial dysplasia due to her ability to approximate her shoulders. Her mother also notes that the child's head appears unusually shaped. Which of the following cranial deformities is typical for CCD?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 1.71 a–c describes typical cranial deformities as "the head is large and brachycephalic, with a small face and bossing of the frontal, parietal, and occipital bones." Microcephaly with premature suture closure is incorrect as CCD is characterized by a large head and delayed suture closure.
Question 6
A 4-year-old boy presents with delayed closure of his skull sutures and a wide, flat nasal bridge. His parents also report that he has difficulty hearing. Which of the following is a common cause of hearing loss in patients with cleidocranial dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Hearing loss is common owing to abnormalities of the ossicles." Inner ear malformations is incorrect as the specific cause is identified as ossicle abnormalities.
Question 7
A 12-year-old girl with cleidocranial dysplasia is undergoing dental evaluation. Which of the following oral findings is highly characteristic of this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The text describes "Oral findings include a high-arched palate with delayed eruption of poorly formed and supernumerary teeth." Microdontia and early tooth eruption is incorrect as the teeth are poorly formed, often supernumerary, and eruption is delayed.
Question 8
A 3-year-old child is noted to have a wide interorbital distance and a flat nasal bridge. Radiographs show wide skull sutures and hypoplastic clavicles. These facial features are consistent with which aspect of cleidocranial dysplasia?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context for Fig. 1.71 states, "An increased interorbital distance may occur, with the bridge of the nose appearing wide and flat." Increased interorbital distance is synonymous with orbital hypertelorism. Maxillary hypoplasia is also mentioned as an affected bone, but hypertelorism directly describes the increased interorbital distance.
Question 9
A 1-year-old infant is being evaluated for a large head circumference and delayed fontanelle closure. Physical examination reveals a small face relative to the skull and bossing of the frontal bones. Which of the following bones are specifically mentioned as being affected in cleidocranial dysplasia, contributing to these cranial findings?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that CCD "causes disturbances in the growth of bones of the cranial vault." The other options are specific cranial bones but the cranial vault is the overarching structure mentioned as affected. The cranial deformities described (large head, bossing, wide sutures) are all features of cranial vault involvement.
Question 10
A 9-year-old boy with cleidocranial dysplasia presents with a complaint of knee pain. On examination, he is noted to have an angular deformity of his knees. Which of the following lower limb deformities is commonly associated with CCD?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states, "Genu valgum and short fingers can be seen." Genu varum is incorrect as the opposite deformity is described.
Question 11
A 6-year-old girl with cleidocranial dysplasia undergoes a chest radiograph. The radiograph shows bilateral clavicular abnormalities. Which specific part of the clavicle is typically affected by hypoplasia in CCD?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 1.72 a, b describes the radiograph showing "bilateral clavicular hypoplasia at the lateral side of the clavicles." The medial end is incorrect as the lateral side is specifically mentioned.
Question 12
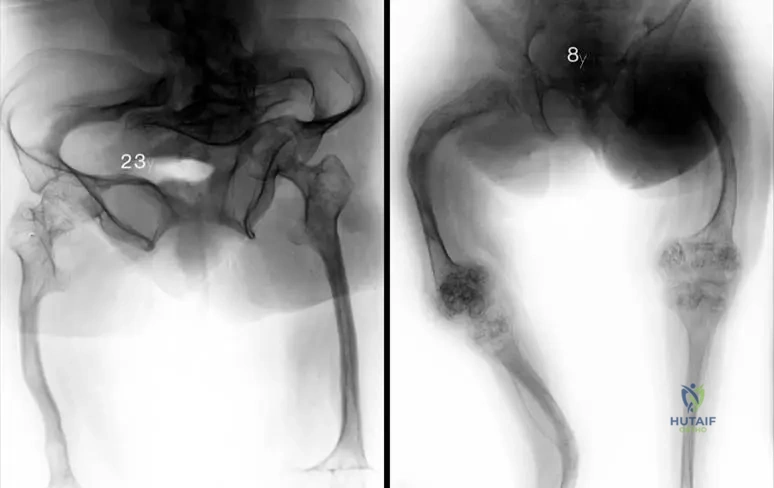
A 5-year-old child with cleidocranial dysplasia has an anteroposterior pelvic radiograph. The radiograph reveals delayed ossification of the pubic bones and the development of idiopathic coxa vara. This specific constellation of pelvic and cranial findings has led to an alternative name for this type of CCD. What is this alternative name?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 1.74 states, "This type of CCD called also pelvico–cranial dysostosis." Craniofacial dysostosis is incorrect as it is a broader term and not the specific alternative name given for CCD with pelvic involvement.
Question 13
A 10-year-old boy with cleidocranial dysplasia is observed to have unusually short fingers. This finding is consistent with the general skeletal manifestations of CCD. Which of the following is also a common associated finding in the hands of patients with CCD?
View Answer & Explanation
Correct Answer: C
Rationale: The text mentions "short fingers" as a feature of CCD. Brachydactyly is the medical term for short fingers. Polydactyly (extra digits) is incorrect.
Question 14
A 2-year-old child presents with a large head, wide fontanelles, and the ability to bring their shoulders close together. A diagnosis of cleidocranial dysplasia is suspected. Which of the following bones, in addition to the clavicles, maxilla, nasal, and lacrimal bones, are specifically mentioned as having growth disturbances in CCD?
View Answer & Explanation
Correct Answer: C
Rationale: The text states that CCD "causes disturbances in the growth of bones of the cranial vault, the clavicles, the maxilla, the nasal and lacrimal bones and the pelvis." The mandible is incorrect as it is not listed among the specifically affected bones in the provided text.
Question 15
A 7-year-old boy with cleidocranial dysplasia is noted to have a wide, flat nasal bridge and an increased interorbital distance. These findings are directly related to the involvement of which facial bones in CCD?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states that CCD "causes disturbances in the growth of bones of the cranial vault, the clavicles, the maxilla, the nasal and lacrimal bones and the pelvis." These bones directly contribute to the facial features described. Mandible and temporal bones are incorrect as they are not listed as primarily affected in this context.
Question 16
A 4-year-old child with a family history of cleidocranial dysplasia presents with delayed eruption of teeth and a high-arched palate. Radiographs confirm delayed closure of skull sutures and hypoplastic clavicles. Which of the following is the MOST likely underlying genetic mechanism for this condition?
View Answer & Explanation
Correct Answer: B
Rationale: Cleidocranial dysplasia is an autosomal dominant disorder, which typically arises from a point mutation or other small genetic change in a single gene (RUNX2 is the known gene, though not mentioned in the text, the mechanism of autosomal dominant inheritance points to a gene mutation). Deletion of a critical gene on the X chromosome would imply X-linked inheritance, which is incorrect.
Question 17
A 15-year-old patient with cleidocranial dysplasia is being evaluated for persistent wide skull sutures. What is a characteristic feature of the skull sutures in CCD?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 1.71 a–c states, "The skull sutures are wide, and their closure is delayed." Premature fusion is incorrect as the opposite is observed.
Question 18
A 5-year-old child is diagnosed with cleidocranial dysplasia. The parents are concerned about potential orthopedic complications. Besides clavicular and pelvic abnormalities, which of the following lower limb deformities is also mentioned as a possible finding?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "Genu valgum and short fingers can be seen." Clubfoot is incorrect as it is not mentioned as a feature of CCD in the provided text.
Question 19
A 10-year-old girl with cleidocranial dysplasia presents with a waddling gait. An anteroposterior pelvic radiograph shows delayed ossification of the pubic bones and coxa vara. What is the characteristic feature of coxa vara seen in CCD?
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 1.74 states that the pelvic radiograph shows "the development of idiopathic coxa vara." Congenital coxa vara is incorrect as the text specifies "idiopathic."
Question 20
A 8-year-old child is diagnosed with cleidocranial dysplasia. The parents are concerned about the prognosis and management. Given the wide range of skeletal abnormalities, which of the following is considered the classic diagnostic sign of this disorder?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states, "The ability to approximate the shoulders anteriorly is related to clavicle hypoplasia, and is the classic diagnostic sign of this disorder." While other options are features of CCD, they are not described as the "classic diagnostic sign."
Question 21
A 7-year-old boy presents with delayed tooth eruption, a wide head, and the ability to touch his shoulders together anteriorly. Radiographs show bilateral clavicular hypoplasia. His mother reports that her father had similar features.
View Answer & Explanation
Correct Answer: B
Rationale: Cleidocranial dysplasia (CCD) is explicitly stated to be a rare disorder of autosomal dominant inheritance. The presence of affected individuals in successive generations (boy, mother, grandfather) is consistent with this pattern. Autosomal recessive, X-linked, and mitochondrial inheritance patterns do not fit the described family history and genetic basis of CCD.
Question 22
A 12-year-old girl with a known diagnosis of cleidocranial dysplasia is referred for dental evaluation due to concerns about her dentition.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states that "Oral findings include a high-arched palate with delayed eruption of poorly formed and supernumerary teeth." This option directly reflects the described oral manifestations. Early eruption of teeth (D) is contrary to the described delayed eruption, and other options are not mentioned as characteristic oral findings for CCD.
Question 23
A 3-year-old child is evaluated for a large head and delayed fontanelle closure. Physical examination reveals bossing of the frontal and parietal bones.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text describes typical cranial deformities in CCD as "the head is large and brachycephalic." Brachycephaly refers to a head that is shorter than average from front to back and wider than average from side to side. Scaphocephaly (A) is a long, narrow head, which is the opposite of brachycephaly.
Question 24
A 10-year-old girl presents with an unusual ability to approximate her shoulders anteriorly. An anteroposterior chest radiograph is obtained.
View Answer & Explanation
Correct Answer: B
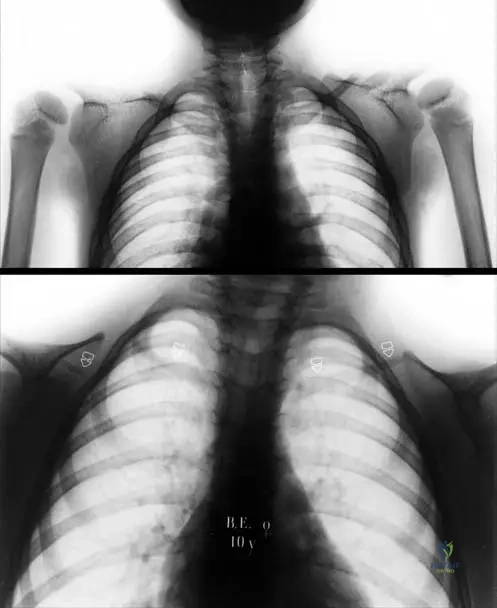
Rationale: The clinical text and Fig. 1.72 a, b explicitly state and show "Anteroposterior chest radiograph of the patient shows bilateral clavicular hypoplasia at the lateral side of the clavicles (a) and a girl with almost clavicular aplasia (b)." This is the characteristic radiographic finding. Medial clavicular hypertrophy (A) is the opposite of the described hypoplasia and is not characteristic of CCD.
Question 25
A 5-year-old child with suspected cleidocranial dysplasia undergoes a skeletal survey. An anteroposterior pelvic radiograph is shown.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 1.74 and its accompanying text state: "Anteroposterior pelvic radiograph in a 5-year-old child shows delayed ossification of pubic bones and the development of idiopathic coxa vara." This directly matches option C. While delayed ossification might lead to a wider appearance of the symphysis pubis (B), the specific findings mentioned in the text are delayed ossification and coxa vara.
Question 26
A 15-year-old male with a confirmed diagnosis of cleidocranial dysplasia is undergoing a routine check-up. His parents express concern about his academic performance, noting he often misses instructions.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text explicitly states: "Hearing loss is common owing to abnormalities of the ossicles." This non-skeletal manifestation could directly impact academic performance due to difficulty in hearing instructions. Intellectual disability (E) is not mentioned as a feature of CCD in the provided text, making it an incorrect distractor.
Question 27
A pediatrician suspects cleidocranial dysplasia in an 8-year-old child presenting with a large head and delayed tooth eruption. To confirm the diagnosis, the pediatrician performs a specific physical examination maneuver.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states: "Th e ability to approximate the shoulders anteriorly is related to clavicle hypoplasia, and is the classic diagnostic sign of this disorder." While other features like short stature (A), genu valgum (B), short fingers (D), and increased interorbital distance (E) can be seen, the ability to approximate shoulders is specifically highlighted as the "classic diagnostic sign."
Question 28
A 6-year-old girl is diagnosed with cleidocranial dysplasia. Her parents ask about other bones that might be affected by this condition, beyond the skull and clavicles.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states that CCD "causes disturbances in the growth of bones of the cranial vault, the clavicles, the maxilla, the nasal and lacrimal bones and the pelvis." Option C directly lists the maxilla, nasal, and lacrimal bones, which are facial bones mentioned as affected. While short fingers (involving metacarpals/phalanges) are mentioned, option E is too restrictive ("only") and option C is a more direct match to the listed bones beyond the skull and clavicles.
Question 29
A newborn is suspected of having cleidocranial dysplasia due to a large head and wide fontanelles noted at birth.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical text states: "The skull sutures are wide, and their closure is delayed." This directly describes the characteristic suture findings in CCD. Premature fusion of sutures (A) describes craniosynostosis, which is the opposite of what is seen in CCD.
Question 30
A 9-year-old boy with cleidocranial dysplasia is noted to have distinct facial characteristics during a routine physical examination.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical text describes "a small face and bossing of the frontal, parietal, and occipital bones. An increased interorbital distance may occur, with the bridge of the nose appearing wide and flat." Option B accurately combines these described facial features. While the head is large (macrocephaly), the face itself is described as small, making option E incorrect.
Question 31
A 7-year-old boy presents with a history of multiple fractures from minor trauma since infancy. Physical examination reveals short stature and blue sclerae. His parents report no family history of similar conditions. Which of the following is the most likely genetic inheritance pattern for this patient's condition?
View Answer & Explanation
Correct Answer: C
Rationale: Osteogenesis imperfecta type I, characterized by bone fragility, blue sclerae, and fractures after birth, is typically inherited in an autosomal dominant pattern due to mutations in COL1A1 or COL1A2 genes. While other types of OI can be autosomal recessive or X-linked, the classic presentation described points to Type I. Autosomal recessive inheritance is seen in some severe forms like Type II and Type III, but Type I is predominantly autosomal dominant. X-linked recessive inheritance is mentioned for some forms of Type IV, but Type I is not X-linked.
Question 32
A 9-year-old boy is evaluated for recurrent fractures and skeletal deformities. On examination, he has a mis-shaped skull with a triangular face and strikingly blue sclerae. Radiographs show thin cortices and narrow diaphyses of long bones. Which type of Osteogenesis Imperfecta is most consistent with these findings?

View Answer & Explanation
Correct Answer: A
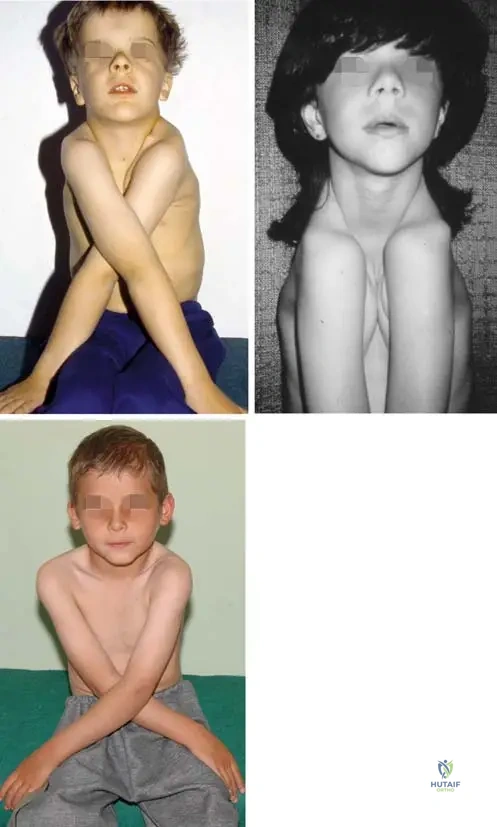
Rationale: The clinical presentation of a 9-year-old boy with a mis-shaped skull, triangular face, blue sclerae, and thin cortices/narrow diaphyses on radiographs is characteristic of Osteogenesis Imperfecta Type I. Type II is a lethal form, Type III presents with progressive deformity and typically normal sclerae, and Type IV also presents with normal sclerae. The image Fig. 1.88 a–c directly illustrates the blue sclerae and mis-shaped skull with triangular face seen in Type I OI.
Question 33
A prenatal ultrasound for a 30-year-old pregnant woman reveals a fetus with intrauterine curved and multiplex fractured long bones and beaded ribs. The pregnancy is complicated by severe polyhydramnios. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
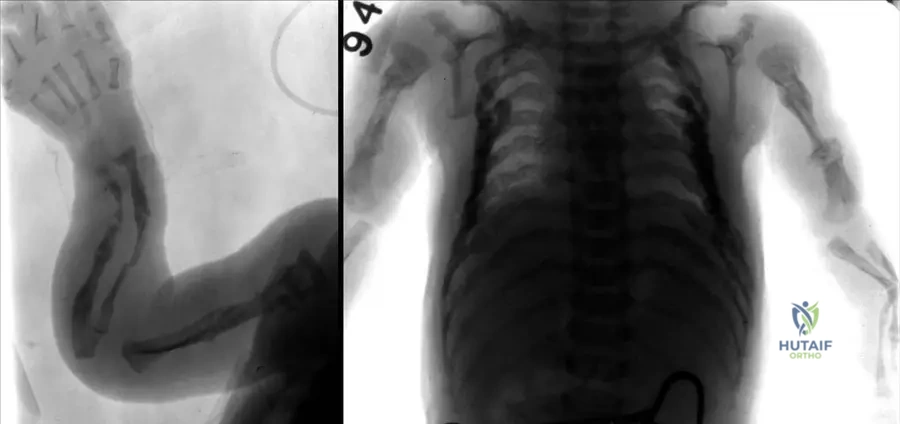
Rationale: The findings of intrauterine curved and multiplex fractured long bones and beaded ribs are pathognomonic for Osteogenesis Imperfecta Type II, which is the lethal form of OI. Type I, III, and IV are typically not lethal in utero and present with less severe or different radiographic features at birth. Achondroplasia is characterized by rhizomelic dwarfism but not typically by multiple intrauterine fractures or beaded ribs.
Question 34
An 8-year-old girl presents with a history of fractures at birth and progressive skeletal deformities. Her parents note that her sclerae are of normal color, and she has no reported hearing issues. Radiographs show significant bowing of long bones. Which type of Osteogenesis Imperfecta is most consistent with this presentation?
View Answer & Explanation
Correct Answer: C
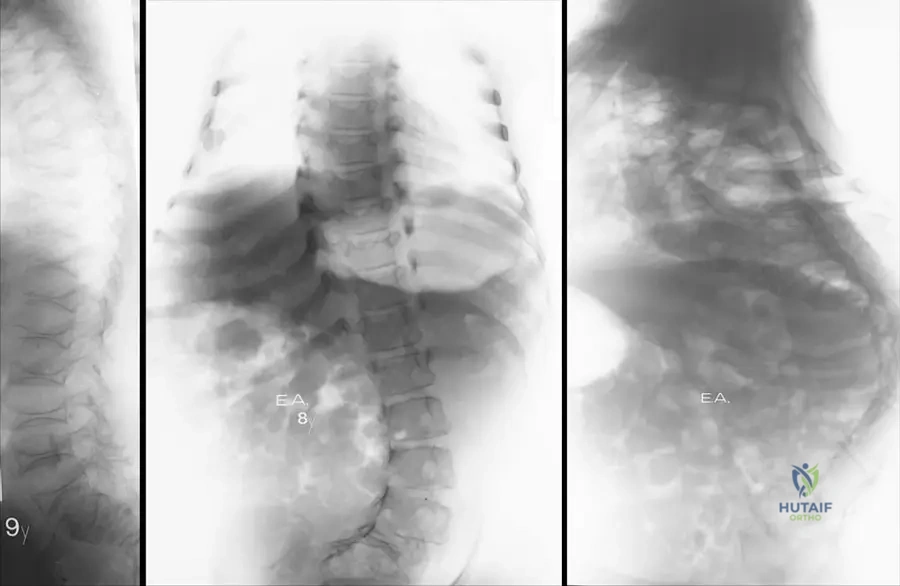
Rationale: Osteogenesis Imperfecta Type III is characterized by fractures at birth, progressive deformity, and notably, normal sclerae and hearing. This distinguishes it from Type I (blue sclerae) and Type II (lethal, intrauterine fractures). Type IV also has normal sclerae but typically presents with moderate deformities, not usually fractures at birth with progressive severe deformity. The image Fig. 1.93 b shows bowing and fractured long bones in an 8-year-old girl, consistent with Type III.
Question 35
An 8-year-old girl is diagnosed with Osteogenesis Imperfecta. Her sclerae are normal, and she has no dentinogenesis imperfecta. Radiographs show moderate deformities of long bones and platyspondyly of the thoracolumbar spine. What is the most likely type of Osteogenesis Imperfecta?
View Answer & Explanation
Correct Answer: D
Rationale: Osteogenesis Imperfecta Type IV is characterized by bone fragility, normal sclerae and hearing, and can present with or without dentinogenesis imperfecta. The description of moderate deformities and platyspondyly with normal sclerae aligns well with Type IV. Type I has blue sclerae, Type II is lethal, and Type III presents with more severe progressive deformities and fractures at birth, although it also has normal sclerae. The image Fig. 1.96 a, b shows platyspondyly in a girl with Type IV OI.
Question 36
A 9-year-old boy with Osteogenesis Imperfecta Type I undergoes a skull radiograph. Which of the following characteristic findings is most likely to be observed on this imaging?

View Answer & Explanation
Correct Answer: C
Rationale: Wormian bones (intrasutural bones) are a common radiographic finding in the skull of patients with Osteogenesis Imperfecta, particularly Type I and III. While other skull abnormalities can occur, wormian bones are a classic and frequently observed feature. The image Fig. 1.90 c specifically highlights "wormian bones" on a skull radiograph of a 9-year-old boy with OI Type I.
Question 37
A 54-year-old patient with a long-standing diagnosis of Osteogenesis Imperfecta Type I presents for a routine check-up. Beyond skeletal fragility, which of the following non-skeletal manifestations is commonly associated with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: Nonskeletal abnormalities in Osteogenesis Imperfecta Type I can include deafness, blue-colored tympanic membrane, cackling laugh, and squeaky voice. Renal calculi, pancreatitis, diabetes mellitus, and hypothyroidism are not typically associated non-skeletal manifestations of OI.
Question 38
A 12-year-old girl with Osteogenesis Imperfecta Type I is noted to have soft, translucent, and brownish deciduous and permanent teeth. This specific dental abnormality is known as:
View Answer & Explanation
Correct Answer: B
Rationale: The description of soft, translucent, and brownish deciduous or permanent teeth is characteristic of dentinogenesis imperfecta, a common feature in Osteogenesis Imperfecta, particularly in Type IB and Type IVB. Amelogenesis imperfecta affects the enamel, while enamel hypoplasia is a defect in enamel formation. Periodontitis and dental caries are common dental diseases but not specific to OI in this manner.
Question 39
A 45-year-old male with Osteogenesis Imperfecta Type I presents to the emergency department with sudden onset chest pain radiating to his back. Given his underlying condition, which of the following cardiac manifestations should be a primary concern?
View Answer & Explanation
Correct Answer: B
Rationale: Cardiac manifestations in Osteogenesis Imperfecta can include vascular fragility with arterial or aortic dissection. This is a critical and potentially life-threatening complication. While other cardiac issues can occur in the general population, aortic dissection is a known specific risk in OI due to connective tissue abnormalities affecting vessel walls. Mitral valve prolapse can also be seen, but aortic dissection is a more acute and severe concern with the presented symptoms.
Question 40
A 17-year-old female with Osteogenesis Imperfecta Type I presents with a healed fracture of the left tibia. Radiographs show a prominent, enlarged callus formation at the fracture site. This finding is best described as:
View Answer & Explanation
Correct Answer: C
Rationale: Patients with Osteogenesis Imperfecta, particularly Type I, can exhibit hyperplastic callus formation following fractures. This is an exaggerated healing response that can sometimes be mistaken for a tumor. Atrophic nonunion and pseudarthrosis refer to failed or poor healing, while malunion describes healing in an incorrect alignment. Osteomyelitis is an infection. The image Fig. 1.89 b clearly shows hyperplastic callus formation on the left tibia after fracture healing.
Question 41
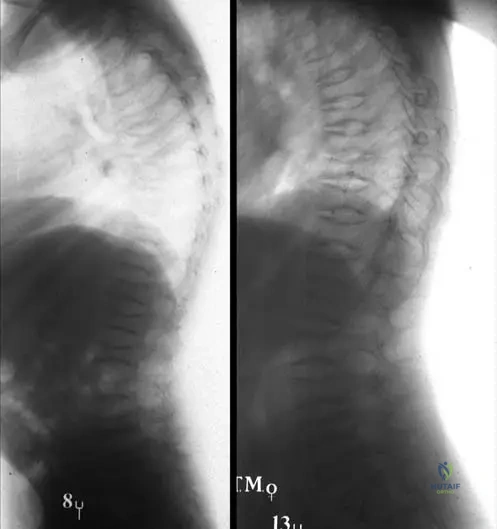
A 9-year-old girl with Osteogenesis Imperfecta Type I undergoes a thoracolumbar X-ray. The radiograph reveals flattened vertebral bodies. This specific spinal deformity is known as:
View Answer & Explanation
Correct Answer: D
Rationale: Platyspondyly, characterized by flattened vertebral bodies, is a common finding in the thoracolumbar spine of patients with Osteogenesis Imperfecta, seen in types such as Type I and Type IV. Kyphosis and lordosis refer to abnormal spinal curvature, while spondylolisthesis is a slippage of one vertebra over another. Vertebral wedging is a specific type of deformity but platyspondyly describes the overall flattening. The image Fig. 1.91 a shows platyspondyly of the thoracolumbar spine in a 9-year-old girl with OI Type I.
Question 42
A 23-year-old male with Osteogenesis Imperfecta Type III presents with hip pain. Radiographs of the pelvis show the femoral heads protruding into the acetabulum, resulting in a "trefoil" shaped pelvis. This finding is termed:
View Answer & Explanation
Correct Answer: C
Rationale: Acetabular protrusion, where the femoral head migrates medially past the ilioischial line, leading to a "trefoil" shaped pelvis, is a characteristic feature seen in more severe forms of Osteogenesis Imperfecta, such as Type III. Hip dysplasia refers to abnormal development of the hip joint, avascular necrosis is bone death due to lack of blood supply, femoroacetabular impingement is abnormal contact between the femur and acetabulum, and slipped capital femoral epiphysis is a displacement of the femoral head. The image Fig. 1.93 a clearly depicts acetabular protrusion with a "trefoil" shape pelvis in a 23-year-old male with OI Type III.
Question 43
An archive radiograph of a neonate diagnosed with a lethal form of Osteogenesis Imperfecta (Type II) shows multiple intrauterine fractures of long bones. Additionally, a specific finding in the chest wall is visible. What is this characteristic rib abnormality?
View Answer & Explanation
Correct Answer: C
Rationale: Beaded ribs, characterized by multiple small fractures and subsequent callus formation along the ribs, are a distinctive radiographic feature of Osteogenesis Imperfecta Type II, the lethal form. Pectus excavatum is a chest wall deformity, flail chest is a segment of the rib cage that breaks away from the rest of the chest wall, rib notching is erosion of the inferior rib margins, and bifid ribs are a congenital anomaly. The image Fig. 1.92 b explicitly points out "Beaded ribs" in a patient with lethal OI Type II.
Question 44
A 9-year-old boy with Osteogenesis Imperfecta Type I presents for follow-up. Radiographs of his hands and fingers show:
View Answer & Explanation
Correct Answer: C
Rationale: Radiographs in Osteogenesis Imperfecta Type I typically demonstrate decreased bone density, leading to thin cortices and narrow diaphyses, making the bones more prone to fracture. Widened metaphyses, thickened cortices, increased bone density, and enchondromas are not characteristic features of OI Type I. The image Fig. 1.90 a shows "thin cortices and narrow diaphyses at the metacarpals and fingers" in a 9-year-old boy with OI Type I.
Question 45
A 9-year-old boy with Osteogenesis Imperfecta Type I is noted to have a distinctive facial appearance. Which of the following best describes the typical facial features associated with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: Patients with Osteogenesis Imperfecta Type I often present with a mis-shaped skull and a triangular face, in addition to blue sclerae. This is a characteristic craniofacial manifestation of the condition. The other options describe features seen in different genetic syndromes. The image Fig. 1.88 a clearly shows a "Mis-shaped skull with triangular face and blue sclerae of 9-year-old boy" with OI Type I.
Question 46
An 8-year-old girl with Osteogenesis Imperfecta Type III is being examined. In addition to bowing and fractured long bones, which of the following musculoskeletal findings is commonly observed in this type of OI?
View Answer & Explanation
Correct Answer: C
Rationale: In Osteogenesis Imperfecta Type III, hyperelastic joints and luxation or subluxation of joints are common findings, reflecting the underlying connective tissue disorder. Joint ankylosis (stiffening), contractures (shortening of soft tissues around a joint), muscle hypertrophy, and shortened tendons are not typical features of OI Type III; in fact, the opposite (laxity) is more common. The text explicitly states "In other cases hyperelastic joints and luxation or subluxation of joints are also common" for Type III.
Question 47
A 5-year-old boy is diagnosed with Osteogenesis Imperfecta Type I. Genetic testing is performed to confirm the diagnosis. Mutations in which of the following genes are most commonly associated with this type of OI?
View Answer & Explanation
Correct Answer: B
Rationale: Osteogenesis Imperfecta Type I is typically caused by mutations in the COL1A1 and COL1A2 genes, which encode for type I collagen. These mutations lead to abnormal collagen production, affecting bone and other connective tissues. FGFR3 mutations are associated with achondroplasia, SOX9 with campomelic dysplasia, GNAS with McCune-Albright syndrome, and ACAN with spondyloepiphyseal dysplasia. The text explicitly states "In patients of type I the collagen is usually abnormal as a result of mutations in the COL1A1 and COL1A2 genes."
Question 48
A 13-year-old girl with Osteogenesis Imperfecta Type I, who previously had platyspondyly, is now noted to have a significant lateral curvature of her thoracolumbar spine. This progressive spinal deformity is known as:
View Answer & Explanation
Correct Answer: C
Rationale: Progressive scoliosis is a common and significant spinal deformity that develops in more severe cases of Osteogenesis Imperfecta, including Type I. Spondylosis refers to degenerative changes in the spine, spondylolysis is a defect in the pars interarticularis, kyphosis is an excessive posterior curvature, and lordosis is an excessive anterior curvature. The image Fig. 1.91 b, c shows progressive scoliosis developing in a girl with OI Type I.
Question 49
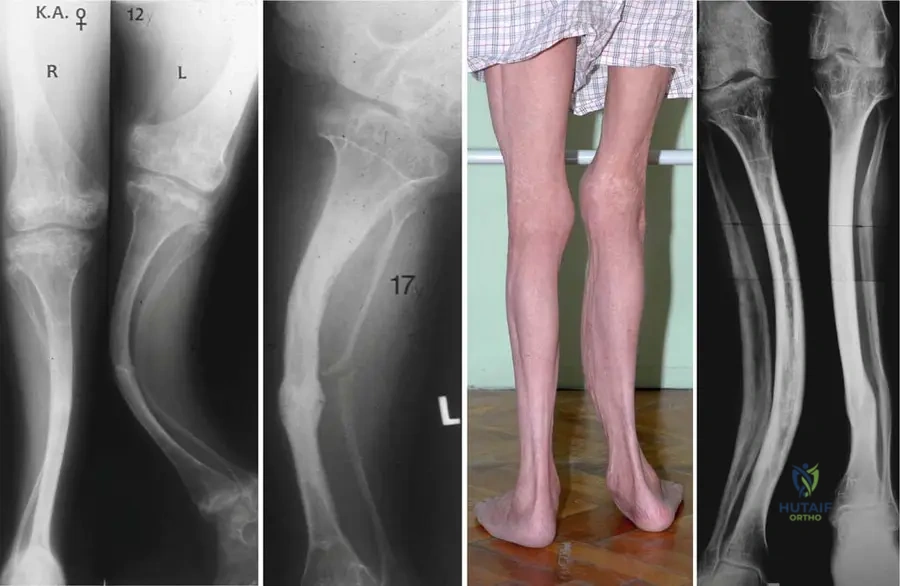
A 15-year-old boy with Osteogenesis Imperfecta Type III undergoes radiographs of his lower extremities. The images reveal moderate bowing of the tibia and a distinctive appearance of the femoral metaphysis. This metaphyseal finding is described as:

View Answer & Explanation
Correct Answer: C
Rationale: In Osteogenesis Imperfecta Type III, radiographs can show cystic and "trumpet" shaped metaphyses of long bones, in addition to bowing and fractures. This is a specific radiographic characteristic for this type. Sclerotic and dense bones are seen in osteopetrosis, not OI. The image Fig. 1.94 b clearly shows a "cystic and 'trumpet' shaped metaphysis of femur" in a 15-year-old boy with OI Type III.
Question 50
A patient with Osteogenesis Imperfecta Type III presents with severely deformed forearms. On physical examination, the skin overlying the forearms is noted to be:

View Answer & Explanation
Correct Answer: C
Rationale: Due to the underlying connective tissue disorder, patients with Osteogenesis Imperfecta, particularly Type III, can have thin and distensible skin. This is another manifestation of the widespread collagen defect. The image Fig.
Question 50
A 9-year-old boy presents with a history of recurrent fractures since early childhood. On physical examination, he has a mis-shaped skull with a triangular face and noticeably blue sclerae. Radiographs reveal thin cortices and narrow diaphyses of long bones, along with wormian bones in the skull.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of recurrent fractures, blue sclerae, mis-shaped skull, triangular face, thin cortices, and wormian bones is classic for Osteogenesis Imperfecta Type I. Type I is characterized by bone fragility with fracture onset after birth and blue sclerae. Type II is lethal, Type III presents with progressive deformity and normal sclerae (as per text), and Type IV has normal sclerae. Hypophosphatasia is a disorder of bone mineralization, not collagen, and presents differently.
Question 50
A 9-year-old boy with a known diagnosis of Osteogenesis Imperfecta Type I undergoes a skull radiograph. Which of the following findings is most likely to be observed?
View Answer & Explanation
Correct Answer: C
Rationale: The provided clinical image (Fig. 1.90 c) explicitly shows "wormian bones" on a skull radiograph of a 9-year-old boy with Osteogenesis Imperfecta Type I. Beaded ribs are characteristic of Type II, a trefoil-shaped pelvis and cystic metaphysis are seen in Type III. Intracranial calcifications are not a described feature of OI in the provided text.
Question 50
An 8-year-old girl with Osteogenesis Imperfecta Type I presents for follow-up. Her thoracolumbar X-ray is reviewed. Which of the following spinal findings is commonly associated with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.91 a–c specifically states "Platyspondyly of the thoracolumbar spine at the age of 9 years" in a girl with Osteogenesis Imperfecta Type I, and notes that progressive scoliosis can also develop. Platyspondyly refers to flattened vertebral bodies, a common finding in OI due to bone fragility. The other options are not specifically mentioned as common findings in OI in the provided text.
Question 50
A 17-year-old female patient with Osteogenesis Imperfecta Type I presents with a healed left tibia fracture. Radiographs of her lower extremity are obtained. What specific characteristic of fracture healing is often observed in patients with OI, as depicted in the provided image?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context for Fig. 1.89 b explicitly mentions "after fracture healing with hyperplastic callus formation on left tibia" in a 17-year-old female patient with Osteogenesis Imperfecta Type I. This is a known feature of OI, where the body overproduces callus in an attempt to stabilize the fragile bone. The other options describe complications or different types of callus that are not specifically highlighted as characteristic of OI in the provided text.
Question 50
A 54-year-old patient with Osteogenesis Imperfecta Type I reports a progressive decline in hearing. Which of the following non-skeletal abnormalities is a known manifestation of OI and could explain this symptom?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that "Nonskeletal abnormalities can develop too, as deafness, blue-colored tympanic membrane, cackling laugh and squeaky voice." Therefore, deafness is a known non-skeletal manifestation of Osteogenesis Imperfecta. The other options are not mentioned in the provided text as associated with OI.
Question 50
A 23-year-old male with a history of Osteogenesis Imperfecta Type III presents with chest pain and shortness of breath. While evaluating for potential complications of his underlying condition, which of the following cardiac manifestations should be considered?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Cardiac manifestations such as vascular fragility with arterial or aortic dissection are also known." This directly links cardiac symptoms to vascular fragility and dissection in OI patients. The other options are general cardiac conditions not specifically highlighted as manifestations of OI in the provided text.
Question 50
A 9-year-old boy is diagnosed with Osteogenesis Imperfecta Type I based on clinical features including blue sclerae, recurrent fractures, and radiographic findings of thin cortices and wormian bones. Genetic testing is performed to confirm the diagnosis. Mutations in which of the following genes are typically associated with Type I OI?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states, "In patients of type I the collagen is usually abnormal as a result of mutations in the COL1A1 and COL1A2 genes." These genes encode for Type I collagen, which is primarily affected in OI. The other genes are associated with different skeletal dysplasias (e.g., FGFR3 with achondroplasia).
Question 50
A 12-year-old female presents with bowing of both tibias and a history of multiple fractures. Her sclerae are blue, and she has dentinogenesis imperfecta. Osteogenesis Imperfecta is suspected. This condition is fundamentally classified as a heritable disorder of which type of tissue?
View Answer & Explanation
Correct Answer: D
Rationale: The introductory sentence of the teaching case states, "Osteogenesis imperfecta is a heritable disorder of the connective tissue (affecting both bone and soft tissue) with decreased bone density..." This directly identifies OI as a connective tissue disorder. The other options are incorrect tissue types.
Question 50
A 9-year-old boy with Osteogenesis Imperfecta Type I is noted to have dental abnormalities. His deciduous and permanent teeth are described as soft, translucent, and brownish. This specific dental manifestation is known as:
View Answer & Explanation
Correct Answer: B
Rationale: The text describes OI as being characterized by "dentinogenesis imperfecta with soft, translucent and brownish deciduous or permanent teeth." This directly matches the clinical description provided. Amelogenesis imperfecta affects enamel, not dentin. The other options are unrelated dental conditions.
Question 50
Archive radiographs of a patient reveal intrauterine curved and multiplex fractured long bones on the upper extremity, along with beaded ribs. The patient unfortunately experienced a lethal outcome shortly after birth. These findings are most consistent with which type of Osteogenesis Imperfecta?
View Answer & Explanation
Correct Answer: B
Rationale: The text describes Osteogenesis Imperfecta Type II as "Autosomal recessive; death before or after birth; intrauterine curved and multiplex fractured long bones; beaded ribs; blue sclera." The vignette's description of intrauterine fractures, beaded ribs, and lethal outcome perfectly matches Type II. The image (Fig. 1.92 a, b) also illustrates these features for Type II.
Question 50
A 23-year-old male with Osteogenesis Imperfecta Type III presents with hip pain. Radiographs of his pelvis are obtained. Which of the following specific pelvic deformities is characteristic of Type III OI and is depicted in the provided image?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context for Fig. 1.93 a explicitly states "Acetabular protrusion with 'trefoil' shape pelvis of a 23-year-old male" with Osteogenesis Imperfecta Type III. This is a characteristic deformity seen in more severe forms of OI. Coxa vara can occur but is not the specific pelvic shape described. The other options are not characteristic findings for OI in the provided text.
Question 50
A 15-year-old boy with Osteogenesis Imperfecta Type III undergoes radiographs of his lower extremities. Which of the following metaphyseal findings is characteristic of Type III OI and is shown in the provided image?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.94 b describes "Radiograph of cystic and 'trumpet' shaped metaphysis of femur and moderate bowing of tibia of a 15-year-old boy" with Osteogenesis Imperfecta Type III. This specific metaphyseal appearance is a recognized feature of Type III OI. The other options describe different metaphyseal abnormalities not specifically associated with OI in the text.
Question 50
A patient with Osteogenesis Imperfecta Type III presents with severely deformed forearms. On physical examination, the skin over the forearms is noted to have a distinct characteristic. Which of the following skin findings is described for patients with Type III OI?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.95 a, b explicitly states "Severely deformed forearms with thin and distensible skin on left (a) and right (b) side of a patient" with Osteogenesis Imperfecta Type III. This reflects the generalized connective tissue disorder affecting skin as well. The other options are not described skin findings for OI in the provided text.
Question 50
A 9-year-old boy is diagnosed with Osteogenesis Imperfecta Type I, characterized by blue sclerae, recurrent fractures after birth, and thin cortices on radiographs. What is the typical inheritance pattern for Osteogenesis Imperfecta Type I?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states under the "Types" section that Type I is "Autosomal dominant; bone fragility with fracture onset after birth; blue sclerae; without (type A) or with dentinogenesis imperfecta (type B)".
Question 50
A newborn is diagnosed with Osteogenesis Imperfecta Type II, presenting with intrauterine curved and multiplex fractured long bones and beaded ribs, leading to a lethal outcome. What is the typical inheritance pattern for Osteogenesis Imperfecta Type II?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states under the "Types" section that Type II is "Autosomal recessive; death before or after birth; intrauterine curved and multiplex fractured long bones; beaded ribs; blue sclera".
Question 50
An 8-year-old girl is diagnosed with Osteogenesis Imperfecta Type III, characterized by fractures at birth, progressive deformity, and normal sclerae. What is the typical inheritance pattern for this specific type of Osteogenesis Imperfecta as described in the provided text?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states under the "Types" section that Type III is "Autosomal recessive; fractures at birth; progressive deformity; normal sclerae and hearing". While Type III can also be autosomal dominant, the question specifically asks based on the provided text, which lists it as autosomal recessive.
Question 50
A 9-year-old boy presents with recurrent fractures and moderate deformities of his long bones. His sclerae appear normal. Radiographs show thin cortices and bowing of the humerus. Based on the scleral appearance, which type of Osteogenesis Imperfecta is most likely, distinguishing it from Type I?
View Answer & Explanation
Correct Answer: D
Rationale: The text distinguishes Type IV as having "normal sclerae and hearing" with bone fragility, similar to Type I in severity but lacking the blue sclerae. Type I explicitly has blue sclerae. Type II is lethal, and Type III also has normal sclerae but typically presents with more severe progressive deformity and fractures at birth. Given "moderate deformities" and "normal sclerae," Type IV is the best fit for distinguishing from Type I based on scleral color.
Question 50
A 12-year-old female patient presents with significant bowing of both tibias and a history of multiple fractures since birth. Her sclerae are noted to be normal in color. This presentation helps differentiate her condition from Osteogenesis Imperfecta Type I, which is characterized by:
View Answer & Explanation
Correct Answer: C
Rationale: The key distinguishing feature mentioned in the text between Type I and other types (like Type III, which often presents with normal sclerae and fractures at birth) is the presence of "blue sclerae" in Type I. Normal sclerae in a patient with fractures helps rule out Type I. Type I is autosomal dominant, not recessive, and is not typically lethal. Fractures are characteristic of all OI types, and short stature is common.
Question 50
A 9-year-old boy is diagnosed with Osteogenesis Imperfecta Type I. His parents recall that his first fracture occurred when he was a toddler, and he has had several since then. Based on the classification provided, when do fractures typically begin to manifest in patients with Type I OI?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states for Type I: "bone fragility with fracture onset after birth." This distinguishes it from Type II (intrauterine) and Type III (at birth). The vignette's description of fractures starting in toddlerhood is consistent with "after birth."
Question 50
A neonate is born with severe skeletal deformities, including curved and multiplex fractured long bones and beaded ribs, evident on prenatal imaging and confirmed at birth. The condition is rapidly progressive and deemed lethal. Based on the provided classification, when do fractures typically begin to manifest in this severe form of Osteogenesis Imperfecta?
View Answer & Explanation
Correct Answer: D
Rationale: The description of the neonate's condition (intrauterine curved and multiplex fractured long bones, beaded ribs, lethal) is characteristic of Osteogenesis Imperfecta Type II. The text explicitly states for Type II: "intrauterine curved and multiplex fractured long bones." This indicates that fractures begin during the intrauterine period.
Question 51
A 9-year-old boy presents with a history of recurrent fractures since early childhood. On physical examination, he has a mis-shaped skull with a triangular face and noticeably blue sclerae. Radiographs reveal thin cortices and narrow diaphyses of long bones, along with wormian bones in the skull.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of recurrent fractures, blue sclerae, mis-shaped skull, triangular face, thin cortices, and wormian bones is classic for Osteogenesis Imperfecta Type I. Type I is characterized by bone fragility with fracture onset after birth and blue sclerae. Type II is lethal, Type III presents with progressive deformity and normal sclerae (as per text), and Type IV has normal sclerae. Hypophosphatasia is a disorder of bone mineralization, not collagen, and presents differently.
Question 52
A 9-year-old boy with a known diagnosis of Osteogenesis Imperfecta Type I undergoes a skull radiograph. Which of the following findings is most likely to be observed?
View Answer & Explanation
Correct Answer: C
Rationale: The provided clinical image (Fig. 1.90 c) explicitly shows "wormian bones" on a skull radiograph of a 9-year-old boy with Osteogenesis Imperfecta Type I. Beaded ribs are characteristic of Type II, a trefoil-shaped pelvis and cystic metaphysis are seen in Type III. Intracranial calcifications are not a described feature of OI in the provided text.
Question 53
An 8-year-old girl with Osteogenesis Imperfecta Type I presents for follow-up. Her thoracolumbar X-ray is reviewed. Which of the following spinal findings is commonly associated with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.91 a–c specifically states "Platyspondyly of the thoracolumbar spine at the age of 9 years" in a girl with Osteogenesis Imperfecta Type I, and notes that progressive scoliosis can also develop. Platyspondyly refers to flattened vertebral bodies, a common finding in OI due to bone fragility. The other options are not specifically mentioned as common findings in OI in the provided text.
Question 54
A 17-year-old female patient with Osteogenesis Imperfecta Type I presents with a healed left tibia fracture. Radiographs of her lower extremity are obtained. What specific characteristic of fracture healing is often observed in patients with OI, as depicted in the provided image?
View Answer & Explanation
Correct Answer: D
Rationale: The clinical context for Fig. 1.89 b explicitly mentions "after fracture healing with hyperplastic callus formation on left tibia" in a 17-year-old female patient with Osteogenesis Imperfecta Type I. This is a known feature of OI, where the body overproduces callus in an attempt to stabilize the fragile bone. The other options describe complications or different types of callus that are not specifically highlighted as characteristic of OI in the provided text.
Question 55
A 54-year-old patient with Osteogenesis Imperfecta Type I reports a progressive decline in hearing. Which of the following non-skeletal abnormalities is a known manifestation of OI and could explain this symptom?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that "Nonskeletal abnormalities can develop too, as deafness, blue-colored tympanic membrane, cackling laugh and squeaky voice." Therefore, deafness is a known non-skeletal manifestation of Osteogenesis Imperfecta. The other options are not mentioned in the provided text as associated with OI.
Question 56
A 23-year-old male with a history of Osteogenesis Imperfecta Type III presents with chest pain and shortness of breath. While evaluating for potential complications of his underlying condition, which of the following cardiac manifestations should be considered?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Cardiac manifestations such as vascular fragility with arterial or aortic dissection are also known." This directly links cardiac symptoms to vascular fragility and dissection in OI patients. The other options are general cardiac conditions not specifically highlighted as manifestations of OI in the provided text.
Question 57
A 9-year-old boy is diagnosed with Osteogenesis Imperfecta Type I based on clinical features including blue sclerae, recurrent fractures, and radiographic findings of thin cortices and wormian bones. Genetic testing is performed to confirm the diagnosis. Mutations in which of the following genes are typically associated with Type I OI?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states, "In patients of type I the collagen is usually abnormal as a result of mutations in the COL1A1 and COL1A2 genes." These genes encode for Type I collagen, which is primarily affected in OI. The other genes are associated with different skeletal dysplasias (e.g., FGFR3 with achondroplasia).
Question 58
A 12-year-old female presents with bowing of both tibias and a history of multiple fractures. Her sclerae are blue, and she has dentinogenesis imperfecta. Osteogenesis Imperfecta is suspected. This condition is fundamentally classified as a heritable disorder of which type of tissue?
View Answer & Explanation
Correct Answer: D
Rationale: The introductory sentence of the teaching case states, "Osteogenesis imperfecta is a heritable disorder of the connective tissue (affecting both bone and soft tissue) with decreased bone density..." This directly identifies OI as a connective tissue disorder. The other options are incorrect tissue types.
Question 59
A 9-year-old boy with Osteogenesis Imperfecta Type I is noted to have dental abnormalities. His deciduous and permanent teeth are described as soft, translucent, and brownish. This specific dental manifestation is known as:
View Answer & Explanation
Correct Answer: B
Rationale: The text describes OI as being characterized by "dentinogenesis imperfecta with soft, translucent and brownish deciduous or permanent teeth." This directly matches the clinical description provided. Amelogenesis imperfecta affects enamel, not dentin. The other options are unrelated dental conditions.
Question 60
Archive radiographs of a patient reveal intrauterine curved and multiplex fractured long bones on the upper extremity, along with beaded ribs. The patient unfortunately experienced a lethal outcome shortly after birth. These findings are most consistent with which type of Osteogenesis Imperfecta?
View Answer & Explanation
Correct Answer: B
Rationale: The text describes Osteogenesis Imperfecta Type II as "Autosomal recessive; death before or after birth; intrauterine curved and multiplex fractured long bones; beaded ribs; blue sclera." The vignette's description of intrauterine fractures, beaded ribs, and lethal outcome perfectly matches Type II. The image (Fig. 1.92 a, b) also illustrates these features for Type II.
Question 61
A 23-year-old male with Osteogenesis Imperfecta Type III presents with hip pain. Radiographs of his pelvis are obtained. Which of the following specific pelvic deformities is characteristic of Type III OI and is depicted in the provided image?
View Answer & Explanation
Correct Answer: B
Rationale: The clinical context for Fig. 1.93 a explicitly states "Acetabular protrusion with 'trefoil' shape pelvis of a 23-year-old male" with Osteogenesis Imperfecta Type III. This is a characteristic deformity seen in more severe forms of OI. Coxa vara can occur but is not the specific pelvic shape described. The other options are not characteristic findings for OI in the provided text.
Question 62
A 15-year-old boy with Osteogenesis Imperfecta Type III undergoes radiographs of his lower extremities. Which of the following metaphyseal findings is characteristic of Type III OI and is shown in the provided image?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.94 b describes "Radiograph of cystic and 'trumpet' shaped metaphysis of femur and moderate bowing of tibia of a 15-year-old boy" with Osteogenesis Imperfecta Type III. This specific metaphyseal appearance is a recognized feature of Type III OI. The other options describe different metaphyseal abnormalities not specifically associated with OI in the text.
Question 63
A patient with Osteogenesis Imperfecta Type III presents with severely deformed forearms. On physical examination, the skin over the forearms is noted to have a distinct characteristic. Which of the following skin findings is described for patients with Type III OI?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical context for Fig. 1.95 a, b explicitly states "Severely deformed forearms with thin and distensible skin on left (a) and right (b) side of a patient" with Osteogenesis Imperfecta Type III. This reflects the generalized connective tissue disorder affecting skin as well. The other options are not described skin findings for OI in the provided text.
Question 64
A 9-year-old boy is diagnosed with Osteogenesis Imperfecta Type I, characterized by blue sclerae, recurrent fractures after birth, and thin cortices on radiographs. What is the typical inheritance pattern for Osteogenesis Imperfecta Type I?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states under the "Types" section that Type I is "Autosomal dominant; bone fragility with fracture onset after birth; blue sclerae; without (type A) or with dentinogenesis imperfecta (type B)".
Question 65
A newborn is diagnosed with Osteogenesis Imperfecta Type II, presenting with intrauterine curved and multiplex fractured long bones and beaded ribs, leading to a lethal outcome. What is the typical inheritance pattern for Osteogenesis Imperfecta Type II?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states under the "Types" section that Type II is "Autosomal recessive; death before or after birth; intrauterine curved and multiplex fractured long bones; beaded ribs; blue sclera".
Question 66
An 8-year-old girl is diagnosed with Osteogenesis Imperfecta Type III, characterized by fractures at birth, progressive deformity, and normal sclerae. What is the typical inheritance pattern for this specific type of Osteogenesis Imperfecta as described in the provided text?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states under the "Types" section that Type III is "Autosomal recessive; fractures at birth; progressive deformity; normal sclerae and hearing". While Type III can also be autosomal dominant, the question specifically asks based on the provided text, which lists it as autosomal recessive.
Question 67
A 9-year-old boy presents with recurrent fractures and moderate deformities of his long bones. His sclerae appear normal. Radiographs show thin cortices and bowing of the humerus. Based on the scleral appearance, which type of Osteogenesis Imperfecta is most likely, distinguishing it from Type I?
View Answer & Explanation
Correct Answer: D
Rationale: The text distinguishes Type IV as having "normal sclerae and hearing" with bone fragility, similar to Type I in severity but lacking the blue sclerae. Type I explicitly has blue sclerae. Type II is lethal, and Type III also has normal sclerae but typically presents with more severe progressive deformity and fractures at birth. Given "moderate deformities" and "normal sclerae," Type IV is the best fit for distinguishing from Type I based on scleral color.
Question 68
A 12-year-old female patient presents with significant bowing of both tibias and a history of multiple fractures since birth. Her sclerae are noted to be normal in color. This presentation helps differentiate her condition from Osteogenesis Imperfecta Type I, which is characterized by:
View Answer & Explanation
Correct Answer: C
Rationale: The key distinguishing feature mentioned in the text between Type I and other types (like Type III, which often presents with normal sclerae and fractures at birth) is the presence of "blue sclerae" in Type I. Normal sclerae in a patient with fractures helps rule out Type I. Type I is autosomal dominant, not recessive, and is not typically lethal. Fractures are characteristic of all OI types, and short stature is common.
Question 69
A 9-year-old boy is diagnosed with Osteogenesis Imperfecta Type I. His parents recall that his first fracture occurred when he was a toddler, and he has had several since then. Based on the classification provided, when do fractures typically begin to manifest in patients with Type I OI?
View Answer & Explanation
Correct Answer: C
Rationale: The text explicitly states for Type I: "bone fragility with fracture onset after birth." This distinguishes it from Type II (intrauterine) and Type III (at birth). The vignette's description of fractures starting in toddlerhood is consistent with "after birth."
Question 70
A 62-year-old female presents with diffuse bone pain, muscle weakness, and a recent low-energy wrist fracture. Laboratory findings reveal serum calcium of 11.8 mg/dL (normal 8.5-10.2 mg/dL), serum phosphorus of 2.1 mg/dL (normal 2.5-4.5 mg/dL), and an elevated parathyroid hormone (PTH) level of 180 pg/mL (normal 10-65 pg/mL). Radiographs show generalized osteopenia and subperiosteal bone resorption in the phalanges.
View Answer & Explanation
Correct Answer: C
Rationale: The classic biochemical triad of primary hyperparathyroidism includes hypercalcemia, hypophosphatemia, and an elevated parathyroid hormone (PTH) level. The patient's symptoms of bone pain, muscle weakness, and fragility fracture, along with radiographic evidence of osteopenia and subperiosteal resorption, are highly consistent with primary hyperparathyroidism. Malignancy-associated hypercalcemia typically presents with suppressed PTH. Vitamin D intoxication would show elevated 25-hydroxyvitamin D and suppressed PTH. Tertiary hyperparathyroidism occurs in patients with long-standing secondary hyperparathyroidism (often due to chronic kidney disease) where the parathyroid glands become autonomous, but the initial presentation is usually different. Familial hypocalciuric hypercalcemia is characterized by hypercalcemia with inappropriately normal or mildly elevated PTH, but with low urinary calcium excretion, which is not described here as the primary finding.
Question 71
A 55-year-old male with a history of recurrent kidney stones and generalized fatigue undergoes evaluation. Blood tests show hypercalcemia and elevated parathyroid hormone. A skeletal survey is performed. Which of the following radiographic findings is most characteristic of advanced hyperparathyroidism?
View Answer & Explanation
Correct Answer: C
Rationale: Subperiosteal bone resorption, especially along the radial aspect of the middle phalanges, is a pathognomonic radiographic sign of hyperparathyroidism. This finding reflects increased osteoclastic activity stimulated by excess PTH. Sclerotic lesions (A) are more typical of osteoblastic metastases or Paget's disease. Periosteal new bone formation (B) can be seen in various conditions like trauma, infection, or hypertrophic osteoarthropathy. Widening of growth plates (D) is characteristic of rickets or osteomalacia in children. Osteophytes and joint space narrowing (E) are signs of osteoarthritis.
Question 72
A 48-year-old female presents with a painful, expansile lytic lesion in her distal femur. Biopsy reveals a cellular lesion composed of multinucleated giant cells, spindle cells, and hemorrhage. Laboratory tests show hypercalcemia and elevated PTH. What is the most likely diagnosis for this bone lesion?
View Answer & Explanation
Correct Answer: C
Rationale: Brown tumors are focal areas of osteoclastic bone resorption filled with fibrous tissue, hemorrhage, and multinucleated giant cells, occurring as a direct consequence of severe hyperparathyroidism. The presence of hypercalcemia and elevated PTH in conjunction with the described histology is diagnostic. While giant cell tumors (A) also contain multinucleated giant cells, they are typically not associated with hyperparathyroidism. Aneurysmal bone cysts (B) are expansile, lytic lesions with blood-filled spaces but lack the specific association with PTH abnormalities. Chondroblastoma (D) is a cartilaginous tumor. Fibrous dysplasia (E) is a developmental anomaly of bone, not typically associated with hyperparathyroidism.
Question 73
A 70-year-old male is diagnosed with primary hyperparathyroidism. He has symptomatic hypercalcemia, significant bone loss (T-score -3.0 at the femoral neck), and a history of vertebral compression fractures. What is the definitive treatment for this patient?
View Answer & Explanation
Correct Answer: D
Rationale: For symptomatic primary hyperparathyroidism, especially with complications like significant bone loss (osteoporosis) and fragility fractures, parathyroidectomy is the definitive and curative treatment. Bisphosphonates (A) can help manage hypercalcemia and improve bone mineral density but do not cure the underlying disease. Cinacalcet (B) is a calcimimetic that lowers PTH and calcium but is typically used for patients who are not surgical candidates or for secondary/tertiary hyperparathyroidism. Vitamin D supplementation (C) is important if the patient is deficient, but it does not treat the primary cause of hyperparathyroidism and can sometimes acutely worsen hypercalcemia. Close observation (E) is only appropriate for asymptomatic patients who do not meet surgical criteria.
Question 74
A 35-year-old female with end-stage renal disease (ESRD) on hemodialysis presents with severe bone pain and proximal muscle weakness. Laboratory tests show hypocalcemia, hyperphosphatemia, and markedly elevated PTH levels (over 1000 pg/mL). Radiographs reveal osteosclerosis and subperiosteal resorption. What type of hyperparathyroidism is most likely?
View Answer & Explanation
Correct Answer: B
Rationale: This patient's presentation with ESRD, hypocalcemia, hyperphosphatemia, and markedly elevated PTH is classic for secondary hyperparathyroidism. In ESRD, impaired phosphate excretion leads to hyperphosphatemia, which directly stimulates PTH release and also reduces active vitamin D production. Reduced vitamin D production further impairs calcium absorption, leading to hypocalcemia, which is another potent stimulus for PTH. Primary hyperparathyroidism (A) is characterized by hypercalcemia. Tertiary hyperparathyroidism (C) develops after prolonged secondary hyperparathyroidism where the glands become autonomous, leading to hypercalcemia. Familial hypocalciuric hypercalcemia (D) is a genetic disorder with hypercalcemia and inappropriately normal/mildly elevated PTH. Parathyroid carcinoma (E) is rare and usually presents with severe hypercalcemia and very high PTH.
Question 75
A 68-year-old male with a long history of secondary hyperparathyroidism due to chronic kidney disease, previously managed with medical therapy, now presents with persistent hypercalcemia (serum calcium 11.5 mg/dL) despite adequate vitamin D and phosphate binders. His PTH remains significantly elevated. What is the most appropriate diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Tertiary hyperparathyroidism occurs when parathyroid glands, after prolonged stimulation in secondary hyperparathyroidism (e.g., due to chronic kidney disease), become autonomous and secrete PTH independently of calcium levels, leading to hypercalcemia. The key distinguishing feature from secondary hyperparathyroidism (B) is the presence of hypercalcemia. Primary hyperparathyroidism (A) is not secondary to another disease process like kidney failure. Humoral hypercalcemia of malignancy (D) would typically show suppressed PTH. Adynamic bone disease (E) is characterized by low bone turnover and often low or normal PTH, not hypercalcemia and very high PTH.
Question 76
A 58-year-old female with newly diagnosed primary hyperparathyroidism complains of intermittent pain and swelling in her right knee. Arthrocentesis reveals positively birefringent rhomboid-shaped crystals. What is the most likely associated crystal deposition disease?
View Answer & Explanation
Correct Answer: B
Rationale: Hyperparathyroidism is a known risk factor for calcium pyrophosphate dihydrate (CPPD) crystal deposition disease, also known as pseudogout. The description of positively birefringent rhomboid-shaped crystals in the synovial fluid is characteristic of CPPD. Gout (A) involves negatively birefringent needle-shaped monosodium urate crystals. Basic calcium phosphate (C) crystals are typically non-birefringent and very small. Calcium oxalate (D) and cholesterol (E) crystals are rare causes of arthritis and have distinct morphologies.
Question 77
A 72-year-old male undergoes parathyroidectomy for symptomatic primary hyperparathyroidism. On the first postoperative day, he develops perioral numbness, muscle cramps, and a positive Chvostek sign. What is the most likely cause of these symptoms?
View Answer & Explanation
Correct Answer: D
Rationale: Hungry bone syndrome is a well-known complication after parathyroidectomy, especially in patients with severe preoperative bone disease. It is characterized by a rapid and profound drop in serum calcium and phosphate levels due to accelerated remineralization of the skeleton, which was previously demineralized by high PTH levels. Symptoms like perioral numbness, muscle cramps, and a positive Chvostek sign are indicative of hypocalcemia. Hypomagnesemia (B) can also cause similar symptoms but is not the primary cause in this context. Hyperkalemia (C) would present with cardiac arrhythmias and muscle weakness. Recurrent laryngeal nerve injury (E) would cause hoarseness or vocal cord paralysis, not tetany. Postoperative infection (A) would typically present with fever, pain, and wound issues.
Question 78
A 60-year-old female with primary hyperparathyroidism is being evaluated for surgical intervention. Preoperative imaging with a Sestamibi scan shows a solitary adenoma in the inferior right parathyroid gland. What is the primary mechanism by which elevated PTH affects bone?
View Answer & Explanation
Correct Answer: C
Rationale: Parathyroid hormone (PTH) primarily acts on bone by stimulating osteoclast activity, leading to increased bone resorption and release of calcium into the bloodstream. While PTH also has anabolic effects on bone at intermittent low doses, chronic elevation, as seen in hyperparathyroidism, leads to net bone loss. PTH indirectly stimulates osteoblasts to produce RANKL, which then activates osteoclasts. Increased renal reabsorption of calcium (B) and enhanced intestinal absorption of calcium (D) are also effects of PTH, contributing to hypercalcemia, but the primary effect on bone leading to skeletal manifestations is resorption. PTH does not directly inhibit osteoblast activity (A) or promote collagen synthesis (E) in a way that causes the observed bone pathology in hyperparathyroidism.
Question 79
A 50-year-old male presents with chronic back pain and a history of multiple fragility fractures. Radiographs of his skull show a diffuse granular appearance with multiple small lucencies and indistinct cortical margins, often described as a "salt-and-pepper" pattern. This finding is highly suggestive of which condition?
View Answer & Explanation
Correct Answer: C
Rationale: The "salt-and-pepper" skull appearance, characterized by diffuse granular demineralization with small lucencies and indistinct cortical margins, is a classic radiographic sign of hyperparathyroidism. It reflects widespread osteoclastic activity and bone resorption in the calvarium. Paget's disease (A) often shows thickened, sclerotic bone (cotton wool appearance) or osteolytic lesions. Multiple myeloma (B) typically presents with discrete "punched-out" lytic lesions. Osteoporosis (D) shows generalized decreased bone density but not this specific granular pattern. Metastatic prostate cancer (E) usually causes osteoblastic (sclerotic) lesions.
Question 80
A 65-year-old female with asymptomatic primary hyperparathyroidism (serum calcium 10.8 mg/dL, PTH 80 pg/mL) is being considered for non-surgical management. Which of the following criteria would generally NOT be an indication for parathyroidectomy?
View Answer & Explanation
Correct Answer: E
Rationale: The presence of a single parathyroid adenoma on a Sestamibi scan (E) is a common finding in primary hyperparathyroidism and helps localize the abnormal gland for surgery, but it is not, by itself, an indication for surgery. Surgical indications for asymptomatic primary hyperparathyroidism, according to guidelines, include: serum calcium > 1.0 mg/dL above the upper limit of normal (A), creatinine clearance < 60 mL/min (B), bone mineral density T-score < -2.5 at any site (C), and age < 50 years (D). These criteria indicate increased risk of complications or progression of the disease, warranting surgical intervention.
Question 81
A 52-year-old male with a history of primary hyperparathyroidism is being managed medically due to contraindications for surgery. His serum calcium is persistently elevated at 11.2 mg/dL. Which medication primarily acts by increasing the sensitivity of the calcium-sensing receptor on the parathyroid gland, thereby reducing PTH secretion?
View Answer & Explanation
Correct Answer: C
Rationale: Cinacalcet is a calcimimetic agent that increases the sensitivity of the calcium-sensing receptor on the parathyroid gland to extracellular calcium. This leads to a reduction in PTH secretion, which in turn lowers serum calcium and phosphorus levels. It is used in primary hyperparathyroidism in patients who cannot undergo surgery, and in secondary/tertiary hyperparathyroidism. Alendronate (A) is a bisphosphonate that inhibits osteoclast activity and reduces bone resorption, primarily used for osteoporosis. Calcitriol (B) is active vitamin D, which can suppress PTH but can also worsen hypercalcemia in primary hyperparathyroidism. Furosemide (D) is a loop diuretic that can increase urinary calcium excretion but is not a primary treatment for hyperparathyroidism. Denosumab (E) is an anti-RANKL antibody that inhibits osteoclast formation and function, used for osteoporosis and hypercalcemia of malignancy, but not directly targeting PTH secretion via the calcium-sensing receptor.
Question 82
A 45-year-old female with chronic kidney disease (CKD) stage 5 on dialysis develops severe bone pain and multiple pathological fractures. Her PTH levels are extremely high (over 1500 pg/mL), and she has progressive vascular calcification. What is the most appropriate surgical intervention for her bone disease?
View Answer & Explanation
Correct Answer: A
Rationale: For severe secondary or tertiary hyperparathyroidism in patients with ESRD, especially with complications like severe bone disease, pathological fractures, and vascular calcification, total parathyroidectomy with autotransplantation of a small portion of parathyroid tissue into a forearm muscle is often the preferred surgical approach. This aims to remove all hyperplastic parathyroid tissue while preserving some parathyroid function to prevent permanent hypoparathyroidism. Subtotal parathyroidectomy (B) removes 3.5 glands. Excision of a single adenoma (C) is for primary hyperparathyroidism. Thyroidectomy (D) and adrenalectomy (E) are unrelated to parathyroid disease.
Question 83
A 60-year-old male presents with a history of recurrent wrist and ankle fractures. His bone mineral density scan shows severe osteoporosis. Laboratory tests reveal hypercalcemia and elevated PTH. Which of the following is the most common skeletal manifestation of primary hyperparathyroidism?
View Answer & Explanation
Correct Answer: C
Rationale: Osteoporosis, leading to fragility fractures, is the most common skeletal manifestation of primary hyperparathyroidism in the modern era. While classic severe hyperparathyroidism can lead to osteitis fibrosa cystica (characterized by subperiosteal resorption and brown tumors), milder forms often present primarily with generalized bone loss, particularly affecting cortical bone. Osteosclerosis (A) is typically seen in secondary hyperparathyroidism (renal osteodystrophy) or other conditions like myelofibrosis. Osteomalacia (B) is due to defective mineralization. Paget's disease (D) is a localized disorder of bone remodeling. Avascular necrosis (E) is not directly caused by hyperparathyroidism.
Question 84
A 75-year-old female with a long-standing history of primary hyperparathyroidism, managed conservatively, develops acute onset severe hip pain after a minor fall. Radiographs show a subtrochanteric fracture. Her serum calcium is 11.0 mg/dL and PTH is 95 pg/mL. What is the most important factor contributing to her increased fracture risk?
View Answer & Explanation
Correct Answer: C
Rationale: Chronic elevation of PTH in primary hyperparathyroidism preferentially affects cortical bone, leading to cortical bone thinning and increased porosity. This significantly weakens the bone structure and increases the risk of fragility fractures, especially in areas rich in cortical bone like the femoral neck and distal radius. Increased bone mineral density (A), decreased osteoclast activity (B), enhanced bone formation (D), and increased trabecular bone volume (E) are contrary to the effects of chronic hyperparathyroidism on bone.
Question 85
A 68-year-old male with primary hyperparathyroidism is undergoing preoperative evaluation for parathyroidectomy. Which of the following laboratory parameters is most crucial to monitor closely in the immediate postoperative period to prevent complications?
View Answer & Explanation
Correct Answer: C
Rationale: Monitoring serum calcium is critical in the immediate postoperative period after parathyroidectomy due to the risk of hypocalcemia, particularly "hungry bone syndrome." This complication can lead to severe symptoms such as tetany, seizures, and cardiac arrhythmias. While other parameters like serum creatinine (A) are important for overall kidney function, and potassium (B), glucose (D), and WBC count (E) are part of routine postoperative care, serum calcium directly reflects the success of the surgery and the risk of the most common and serious acute complication.
Question 86
A 55-year-old female presents with diffuse bone pain and muscle weakness. Her laboratory tests show hypercalcemia, hypophosphatemia, and elevated PTH. A Sestamibi scan identifies a single parathyroid adenoma. Which of the following conditions is most likely to be mistaken for primary hyperparathyroidism due to similar hypercalcemia, but typically has suppressed PTH?
View Answer & Explanation
Correct Answer: C
Rationale: Malignancy-associated hypercalcemia is the most common cause of hypercalcemia in hospitalized patients and can mimic some symptoms of primary hyperparathyroidism. However, it is typically characterized by suppressed PTH levels (due to PTHrP secretion or direct bone metastases), which helps differentiate it from primary hyperparathyroidism where PTH is elevated or inappropriately normal. Tertiary hyperparathyroidism (A) has elevated PTH. Familial hypocalciuric hypercalcemia (B) has inappropriately normal or mildly elevated PTH. Lithium (D) and thiazide diuretics (E) can cause hypercalcemia by affecting calcium-sensing receptors or renal calcium excretion, respectively, and are usually associated with normal or mildly elevated PTH, but malignancy is the most common and often most challenging differential in terms of severity and presentation.
Question 87
A 40-year-old male with a history of recurrent nephrolithiasis is found to have hypercalcemia and elevated PTH. He has no other symptoms. A DEXA scan shows normal bone mineral density. What is the most appropriate initial management strategy for this patient?
View Answer & Explanation
Correct Answer: D
Rationale: While the patient is currently asymptomatic in terms of bone disease, recurrent nephrolithiasis is a clear indication for parathyroidectomy in primary hyperparathyroidism, regardless of bone mineral density or other symptoms. Therefore, referral for surgical evaluation is the most appropriate next step. Immediate parathyroidectomy (A) is the goal, but evaluation is needed first. Bisphosphonate therapy (B) and Cinacalcet (C) are medical management options for patients who are not surgical candidates or as adjunctive therapy. Close observation (E) is only for truly asymptomatic patients without any surgical indications.
Question 88
A 60-year-old female with primary hyperparathyroidism is found to have a lytic lesion in her proximal tibia. A bone biopsy is performed. Which of the following histological features would be most characteristic of osteitis fibrosa cystica, a severe manifestation of hyperparathyroidism?
View Answer & Explanation
Correct Answer: C
Rationale: Osteitis fibrosa cystica, the classic bone disease of severe hyperparathyroidism, is characterized histologically by increased bone turnover, extensive osteoclastic bone resorption (including dissecting cortical resorption), fibrous replacement of the bone marrow, and the presence of brown tumors (which are essentially collections of osteoclasts and fibrous tissue). Predominance of mature lamellar bone (A) is normal bone. Increased osteoid seams without mineralization (B) is characteristic of osteomalacia. Cartilaginous matrix with calcification (D) would suggest an enchondroma or chondrosarcoma. Sheets of plasma cells (E) are indicative of multiple myeloma.
Question 89
A 70-
Question 89
A 62-year-old woman presents with chronic fatigue, generalized muscle weakness, and a recent diagnosis of nephrolithiasis. Laboratory tests reveal elevated serum calcium and parathyroid hormone (PTH) levels. A DEXA scan shows significant bone loss in the lumbar spine and femoral neck.
View Answer & Explanation
Correct Answer: D
Rationale: In developed countries, with earlier diagnosis of primary hyperparathyroidism, osteoporosis (particularly cortical bone loss) is the most common skeletal manifestation. While subperiosteal bone resorption (C) is a classic and pathognomonic radiographic sign of hyperparathyroidism, it is less frequently observed than generalized osteoporosis in contemporary practice. Osteitis fibrosa cystica (A) and brown tumors (B) represent more severe forms of bone disease, which are now less common due to earlier detection and treatment.
Question 89
A 48-year-old male with end-stage renal disease (ESRD) on hemodialysis presents with severe bone pain, proximal muscle weakness, and pruritus. Laboratory findings include hypocalcemia, hyperphosphatemia, and markedly elevated parathyroid hormone (PTH) levels (e.g., >800 pg/mL).
View Answer & Explanation
Correct Answer: C
Rationale: This patient's presentation is classic for secondary hyperparathyroidism, which is most commonly caused by chronic kidney disease. In ESRD, the kidneys fail to convert 25-hydroxyvitamin D to its active form, 1,25-dihydroxyvitamin D (calcitriol). This leads to impaired intestinal calcium absorption and hypocalcemia. The persistent hypocalcemia, along with hyperphosphatemia (which also stimulates PTH release), chronically stimulates the parathyroid glands, leading to hyperplasia and elevated PTH levels. A parathyroid adenoma (A) or carcinoma (B) would typically cause primary hyperparathyroidism with hypercalcemia. Autonomous hyperplasia (D) is characteristic of tertiary hyperparathyroidism, which develops after prolonged secondary hyperparathyroidism and typically presents with hypercalcemia.
Question 89
A 55-year-old woman with long-standing, untreated primary hyperparathyroidism presents with generalized bone pain and tenderness. Radiographs show diffuse demineralization and a lytic lesion in the distal femur. Further skeletal survey reveals specific changes.
View Answer & Explanation
Correct Answer: C
Rationale: Subperiosteal bone resorption, especially along the radial aspect of the middle phalanges, is the most characteristic and pathognomonic radiographic finding of osteitis fibrosa cystica, the classic bone disease of severe hyperparathyroidism. This finding reflects increased osteoclastic activity at the bone surface. Sclerotic lesions (A) are not typical. Periosteal new bone formation (B) can occur in other conditions but is not specific. Widened growth plates (D) are seen in rickets/osteomalacia in children. Increased bone density in the skull (E), or "cotton wool appearance," is characteristic of Paget's disease of bone.
Question 89
A 35-year-old man with a known history of primary hyperparathyroidism undergoes biopsy of a lytic lesion identified in his tibia. Histopathological examination of the lesion reveals a collection of multinucleated giant cells (osteoclast-like cells), fibroblasts, and hemosiderin-laden macrophages within a vascularized fibrous stroma.
View Answer & Explanation
Correct Answer: C
Rationale: The described histological findings (multinucleated giant cells, fibroblasts, and hemosiderin-laden macrophages) are characteristic of a brown tumor, which is a reparative granuloma-like lesion that occurs in severe hyperparathyroidism. These lesions are not true neoplasms but rather areas of intense osteoclastic activity, hemorrhage, and fibrous tissue replacement. While a giant cell tumor of bone (E) also contains multinucleated giant cells, brown tumors are distinguished by the presence of hemosiderin and their direct association with hyperparathyroidism. Osteosarcoma (A) and chondrosarcoma (B) are malignant tumors with distinct histological features. Fibrous dysplasia (D) is characterized by immature woven bone within a fibrous stroma.
Question 89
A 70-year-old asymptomatic woman is found to have a serum calcium level of 10.8 mg/dL (normal range 8.5-10.2 mg/dL) and a parathyroid hormone (PTH) level of 95 pg/mL (normal range 10-65 pg/mL). Her 24-hour urine calcium excretion is 350 mg (normal <300 mg). A DEXA scan reveals a T-score of -2.8 at the lumbar spine.
View Answer & Explanation
Correct Answer: D
Rationale: According to current guidelines for primary hyperparathyroidism, a T-score less than -2.5 at any skeletal site (lumbar spine, femoral neck, total hip, or distal 1/3 radius) is a clear indication for parathyroidectomy. While age over 50 (not 65) is a consideration, it's not a standalone indication. Her serum calcium (10.8 mg/dL) is elevated but not >1.0 mg/dL above the upper limit of normal (10.2 + 1.0 = 11.2 mg/dL). She is asymptomatic, so B is not an indication for surgery. There is no mention of nephrolithiasis (E) in the vignette. Therefore, the T-score is the strongest surgical indication presented.
Question 89
A 58-year-old man undergoes successful parathyroidectomy for primary hyperparathyroidism. On post-operative day 2, he develops perioral numbness, tingling in his fingertips, and carpopedal spasms. Laboratory tests reveal a significant drop in serum calcium levels (7.0 mg/dL).
View Answer & Explanation
Correct Answer: B
Rationale: The symptoms of hypocalcemia (perioral numbness, tingling, carpopedal spasms) developing after parathyroidectomy, especially with a significant drop in serum calcium, are characteristic of hungry bone syndrome. This occurs when the sudden removal of excess PTH leads to rapid remineralization of previously demineralized bone, causing a profound and prolonged influx of calcium and phosphate into the bone. While hypomagnesemia (A) can also cause hypocalcemia and similar symptoms, hungry bone syndrome is the primary and most common cause of severe post-parathyroidectomy hypocalcemia. Recurrent laryngeal nerve injury (C) would cause voice changes. Surgical site infection (D) would present with local signs of inflammation and fever. Hyperkalemia (E) has different clinical manifestations.
Question 89
A 50-year-old male with a 15-year history of end-stage renal disease (ESRD) on hemodialysis, who previously had well-controlled secondary hyperparathyroidism, now presents with persistent hypercalcemia (serum calcium 11.5 mg/dL) despite medical management, and markedly elevated parathyroid hormone (PTH) levels (e.g., 1200 pg/mL).
View Answer & Explanation
Correct Answer: C
Rationale: This patient's presentation is classic for tertiary hyperparathyroidism. This condition develops in patients with long-standing secondary hyperparathyroidism (often due to ESRD) where the parathyroid glands become autonomous and continue to secrete excessive PTH even after the underlying stimulus (hypocalcemia) is corrected or in the presence of hypercalcemia. This leads to persistent hypercalcemia and very high PTH levels. Secondary hyperparathyroidism (B) typically presents with hypocalcemia or normal calcium. Primary hyperparathyroidism (A) is not related to ESRD as the initial cause. Parathyroid carcinoma (D) is possible but less common and usually presents with even more extreme hypercalcemia and PTH levels, often with a palpable mass. Familial hypocalciuric hypercalcemia (E) is a genetic disorder not typically associated with ESRD.
Question 89
A 40-year-old man presents with a history of recurrent peptic ulcers, nephrolithiasis, and a recently diagnosed pituitary microadenoma. Laboratory tests reveal hypercalcemia and elevated parathyroid hormone (PTH) levels.
View Answer & Explanation
Correct Answer: C
Rationale: This constellation of findings is highly suggestive of Multiple Endocrine Neoplasia type 1 (MEN1), also known as Wermer syndrome. MEN1 is characterized by the "3 Ps": Parathyroid tumors (causing primary hyperparathyroidism and hypercalcemia, leading to nephrolithiasis), Pituitary tumors (like the microadenoma), and Pancreatic neuroendocrine tumors (such as gastrinomas, which cause recurrent peptic ulcers). MEN2A (A) involves parathyroid hyperplasia, medullary thyroid carcinoma, and pheochromocytoma. MEN2B (B) involves medullary thyroid carcinoma, pheochromocytoma, and mucosal neuromas/marfanoid habitus. Von Hippel-Lindau disease (D) and Neurofibromatosis type 1 (E) are not typically associated with this specific endocrine tumor profile.
Question 89
A 68-year-old woman is diagnosed with primary hyperparathyroidism based on persistent hypercalcemia and elevated PTH. She meets surgical criteria and is scheduled for parathyroidectomy. Her surgeon requests imaging to localize the parathyroid adenoma prior to the procedure.
View Answer & Explanation
Correct Answer: D
Rationale: The Technetium-99m Sestamibi scan (D) is considered the most sensitive and specific imaging modality for localizing a parathyroid adenoma prior to initial surgery. It relies on differential washout kinetics, where parathyroid adenomas retain the tracer longer than thyroid tissue. Ultrasound of the neck (C) is also commonly used as a first-line study due to its accessibility and lack of radiation, but its sensitivity can be lower, especially for ectopic glands or smaller adenomas. CT (A) and MRI (B) can be used for localization, particularly for ectopic or recurrent disease, but are generally less specific than Sestamibi for initial localization. PET scan (E) is not routinely used for parathyroid adenoma localization.
Question 89
A 75-year-old man with known primary hyperparathyroidism presents to the emergency department with altered mental status, severe dehydration, nausea, and vomiting. His serum calcium level is critically elevated at 15.2 mg/dL.
View Answer & Explanation
Correct Answer: C
Rationale: This patient is experiencing a hypercalcemic crisis, a medical emergency. The initial management focuses on rapidly lowering serum calcium and correcting dehydration. The cornerstone of initial therapy is aggressive intravenous hydration with normal saline (to restore intravascular volume and promote calciuresis) followed by loop diuretics (e.g., furosemide) once euvolemia is achieved, to further enhance calcium excretion. Immediate parathyroidectomy (A) is not the initial treatment for an acute crisis. Oral calcitonin (B) has a rapid but mild and transient effect. Oral bisphosphonates (D) take several days to exert their full effect and are not suitable for acute crisis management. Cinacalcet (E) is used for chronic management but not for acute, severe hypercalcemia.
Question 89
A 50-year-old male presents with persistent hypercalcemia. Subsequent laboratory evaluation reveals a suppressed parathyroid hormone (PTH) level.
View Answer & Explanation
Correct Answer: D
Rationale: Hypercalcemia with suppressed PTH is a critical diagnostic clue. When PTH is suppressed, it indicates that the parathyroid glands are appropriately responding to high calcium levels by reducing PTH secretion, meaning the hypercalcemia is not primarily due to parathyroid overactivity. The most common cause of hypercalcemia with suppressed PTH is malignancy-associated hypercalcemia, either through the secretion of parathyroid hormone-related protein (PTHrP) or direct bone metastases. Primary hyperparathyroidism (A) and parathyroid adenoma (C) are characterized by elevated or inappropriately normal PTH levels. Secondary hyperparathyroidism (B) typically presents with hypocalcemia and elevated PTH. Familial hypocalciuric hypercalcemia (E) has inappropriately normal PTH, but not suppressed, and is characterized by low urine calcium excretion.
Question 89
A medical student asks about the direct effects of chronically elevated parathyroid hormone (PTH) on bone, particularly in the context of primary hyperparathyroidism.
View Answer & Explanation
Correct Answer: C
Rationale: Chronically elevated PTH, as seen in hyperparathyroidism, primarily stimulates osteoclast activity, leading to increased bone resorption. This effect is particularly pronounced in cortical bone, resulting in subperiosteosteal resorption and generalized cortical thinning. While PTH does stimulate bone remodeling (B) by affecting both osteoblasts and osteoclasts,
Question 90
A 62-year-old woman presents with chronic fatigue, generalized muscle weakness, and a recent diagnosis of nephrolithiasis. Laboratory tests reveal elevated serum calcium and parathyroid hormone (PTH) levels. A DEXA scan shows significant bone loss in the lumbar spine and femoral neck.
View Answer & Explanation
Correct Answer: D
Rationale: In developed countries, with earlier diagnosis of primary hyperparathyroidism, osteoporosis (particularly cortical bone loss) is the most common skeletal manifestation. While subperiosteal bone resorption (C) is a classic and pathognomonic radiographic sign of hyperparathyroidism, it is less frequently observed than generalized osteoporosis in contemporary practice. Osteitis fibrosa cystica (A) and brown tumors (B) represent more severe forms of bone disease, which are now less common due to earlier detection and treatment.
Question 91
A 48-year-old male with end-stage renal disease (ESRD) on hemodialysis presents with severe bone pain, proximal muscle weakness, and pruritus. Laboratory findings include hypocalcemia, hyperphosphatemia, and markedly elevated parathyroid hormone (PTH) levels (e.g., >800 pg/mL).
View Answer & Explanation
Correct Answer: C
Rationale: This patient's presentation is classic for secondary hyperparathyroidism, which is most commonly caused by chronic kidney disease. In ESRD, the kidneys fail to convert 25-hydroxyvitamin D to its active form, 1,25-dihydroxyvitamin D (calcitriol). This leads to impaired intestinal calcium absorption and hypocalcemia. The persistent hypocalcemia, along with hyperphosphatemia (which also stimulates PTH release), chronically stimulates the parathyroid glands, leading to hyperplasia and elevated PTH levels. A parathyroid adenoma (A) or carcinoma (B) would typically cause primary hyperparathyroidism with hypercalcemia. Autonomous hyperplasia (D) is characteristic of tertiary hyperparathyroidism, which develops after prolonged secondary hyperparathyroidism and typically presents with hypercalcemia.
Question 92
A 55-year-old woman with long-standing, untreated primary hyperparathyroidism presents with generalized bone pain and tenderness. Radiographs show diffuse demineralization and a lytic lesion in the distal femur. Further skeletal survey reveals specific changes.
View Answer & Explanation
Correct Answer: C
Rationale: Subperiosteal bone resorption, especially along the radial aspect of the middle phalanges, is the most characteristic and pathognomonic radiographic finding of osteitis fibrosa cystica, the classic bone disease of severe hyperparathyroidism. This finding reflects increased osteoclastic activity at the bone surface. Sclerotic lesions (A) are not typical. Periosteal new bone formation (B) can occur in other conditions but is not specific. Widened growth plates (D) are seen in rickets/osteomalacia in children. Increased bone density in the skull (E), or "cotton wool appearance," is characteristic of Paget's disease of bone.
Question 93
A 35-year-old man with a known history of primary hyperparathyroidism undergoes biopsy of a lytic lesion identified in his tibia. Histopathological examination of the lesion reveals a collection of multinucleated giant cells (osteoclast-like cells), fibroblasts, and hemosiderin-laden macrophages within a vascularized fibrous stroma.
View Answer & Explanation
Correct Answer: C
Rationale: The described histological findings (multinucleated giant cells, fibroblasts, and hemosiderin-laden macrophages) are characteristic of a brown tumor, which is a reparative granuloma-like lesion that occurs in severe hyperparathyroidism. These lesions are not true neoplasms but rather areas of intense osteoclastic activity, hemorrhage, and fibrous tissue replacement. While a giant cell tumor of bone (E) also contains multinucleated giant cells, brown tumors are distinguished by the presence of hemosiderin and their direct association with hyperparathyroidism. Osteosarcoma (A) and chondrosarcoma (B) are malignant tumors with distinct histological features. Fibrous dysplasia (D) is characterized by immature woven bone within a fibrous stroma.
Question 94
A 70-year-old asymptomatic woman is found to have a serum calcium level of 10.8 mg/dL (normal range 8.5-10.2 mg/dL) and a parathyroid hormone (PTH) level of 95 pg/mL (normal range 10-65 pg/mL). Her 24-hour urine calcium excretion is 350 mg (normal <300 mg). A DEXA scan reveals a T-score of -2.8 at the lumbar spine.
View Answer & Explanation
Correct Answer: D
Rationale: According to current guidelines for primary hyperparathyroidism, a T-score less than -2.5 at any skeletal site (lumbar spine, femoral neck, total hip, or distal 1/3 radius) is a clear indication for parathyroidectomy. While age over 50 (not 65) is a consideration, it's not a standalone indication. Her serum calcium (10.8 mg/dL) is elevated but not >1.0 mg/dL above the upper limit of normal (10.2 + 1.0 = 11.2 mg/dL). She is asymptomatic, so B is not an indication for surgery. There is no mention of nephrolithiasis (E) in the vignette. Therefore, the T-score is the strongest surgical indication presented.
Question 95
A 58-year-old man undergoes successful parathyroidectomy for primary hyperparathyroidism. On post-operative day 2, he develops perioral numbness, tingling in his fingertips, and carpopedal spasms. Laboratory tests reveal a significant drop in serum calcium levels (7.0 mg/dL).
View Answer & Explanation
Correct Answer: B
Rationale: The symptoms of hypocalcemia (perioral numbness, tingling, carpopedal spasms) developing after parathyroidectomy, especially with a significant drop in serum calcium, are characteristic of hungry bone syndrome. This occurs when the sudden removal of excess PTH leads to rapid remineralization of previously demineralized bone, causing a profound and prolonged influx of calcium and phosphate into the bone. While hypomagnesemia (A) can also cause hypocalcemia and similar symptoms, hungry bone syndrome is the primary and most common cause of severe post-parathyroidectomy hypocalcemia. Recurrent laryngeal nerve injury (C) would cause voice changes. Surgical site infection (D) would present with local signs of inflammation and fever. Hyperkalemia (E) has different clinical manifestations.
Question 96
A 50-year-old male with a 15-year history of end-stage renal disease (ESRD) on hemodialysis, who previously had well-controlled secondary hyperparathyroidism, now presents with persistent hypercalcemia (serum calcium 11.5 mg/dL) despite medical management, and markedly elevated parathyroid hormone (PTH) levels (e.g., 1200 pg/mL).
View Answer & Explanation
Correct Answer: C
Rationale: This patient's presentation is classic for tertiary hyperparathyroidism. This condition develops in patients with long-standing secondary hyperparathyroidism (often due to ESRD) where the parathyroid glands become autonomous and continue to secrete excessive PTH even after the underlying stimulus (hypocalcemia) is corrected or in the presence of hypercalcemia. This leads to persistent hypercalcemia and very high PTH levels. Secondary hyperparathyroidism (B) typically presents with hypocalcemia or normal calcium. Primary hyperparathyroidism (A) is not related to ESRD as the initial cause. Parathyroid carcinoma (D) is possible but less common and usually presents with even more extreme hypercalcemia and PTH levels, often with a palpable mass. Familial hypocalciuric hypercalcemia (E) is a genetic disorder not typically associated with ESRD.
Question 97
A 40-year-old man presents with a history of recurrent peptic ulcers, nephrolithiasis, and a recently diagnosed pituitary microadenoma. Laboratory tests reveal hypercalcemia and elevated parathyroid hormone (PTH) levels.
View Answer & Explanation
Correct Answer: C
Rationale: This constellation of findings is highly suggestive of Multiple Endocrine Neoplasia type 1 (MEN1), also known as Wermer syndrome. MEN1 is characterized by the "3 Ps": Parathyroid tumors (causing primary hyperparathyroidism and hypercalcemia, leading to nephrolithiasis), Pituitary tumors (like the microadenoma), and Pancreatic neuroendocrine tumors (such as gastrinomas, which cause recurrent peptic ulcers). MEN2A (A) involves parathyroid hyperplasia, medullary thyroid carcinoma, and pheochromocytoma. MEN2B (B) involves medullary thyroid carcinoma, pheochromocytoma, and mucosal neuromas/marfanoid habitus. Von Hippel-Lindau disease (D) and Neurofibromatosis type 1 (E) are not typically associated with this specific endocrine tumor profile.
Question 98
A 68-year-old woman is diagnosed with primary hyperparathyroidism based on persistent hypercalcemia and elevated PTH. She meets surgical criteria and is scheduled for parathyroidectomy. Her surgeon requests imaging to localize the parathyroid adenoma prior to the procedure.
View Answer & Explanation
Correct Answer: D
Rationale: The Technetium-99m Sestamibi scan (D) is considered the most sensitive and specific imaging modality for localizing a parathyroid adenoma prior to initial surgery. It relies on differential washout kinetics, where parathyroid adenomas retain the tracer longer than thyroid tissue. Ultrasound of the neck (C) is also commonly used as a first-line study due to its accessibility and lack of radiation, but its sensitivity can be lower, especially for ectopic glands or smaller adenomas. CT (A) and MRI (B) can be used for localization, particularly for ectopic or recurrent disease, but are generally less specific than Sestamibi for initial localization. PET scan (E) is not routinely used for parathyroid adenoma localization.
Question 99
A 75-year-old man with known primary hyperparathyroidism presents to the emergency department with altered mental status, severe dehydration, nausea, and vomiting. His serum calcium level is critically elevated at 15.2 mg/dL.
View Answer & Explanation
Correct Answer: C
Rationale: This patient is experiencing a hypercalcemic crisis, a medical emergency. The initial management focuses on rapidly lowering serum calcium and correcting dehydration. The cornerstone of initial therapy is aggressive intravenous hydration with normal saline (to restore intravascular volume and promote calciuresis) followed by loop diuretics (e.g., furosemide) once euvolemia is achieved, to further enhance calcium excretion. Immediate parathyroidectomy (A) is not the initial treatment for an acute crisis. Oral calcitonin (B) has a rapid but mild and transient effect. Oral bisphosphonates (D) take several days to exert their full effect and are not suitable for acute crisis management. Cinacalcet (E) is used for chronic management but not for acute, severe hypercalcemia.
Question 100
A 50-year-old male presents with persistent hypercalcemia. Subsequent laboratory evaluation reveals a suppressed parathyroid hormone (PTH) level.
View Answer & Explanation
Correct Answer: D
Rationale: Hypercalcemia with suppressed PTH is a critical diagnostic clue. When PTH is suppressed, it indicates that the parathyroid glands are appropriately responding to high calcium levels by reducing PTH secretion, meaning the hypercalcemia is not primarily due to parathyroid overactivity. The most common cause of hypercalcemia with suppressed PTH is malignancy-associated hypercalcemia, either through the secretion of parathyroid hormone-related protein (PTHrP) or direct bone metastases. Primary hyperparathyroidism (A) and parathyroid adenoma (C) are characterized by elevated or inappropriately normal PTH levels. Secondary hyperparathyroidism (B) typically presents with hypocalcemia and elevated PTH. Familial hypocalciuric hypercalcemia (E) has inappropriately normal PTH, but not suppressed, and is characterized by low urine calcium excretion.
