Master ABOS Orthopedic Board Review: Musculoskeletal Pathology & Dysplasias | Part 16
Key Takeaway
This ABOS review covers key musculoskeletal pathologies including synovial chondromatosis, lipoma arborescens, and soft tissue sarcomas. It also provides a detailed examination of various skeletal dysplasias like osteopetrosis, osteogenesis imperfecta, and achondroplasia, focusing on their clinical presentation, imaging, and management for board exam preparation.
Question 1
A 42-year-old patient presents with a 9-month history of left knee pain, stiffness, and occasional locking. Radiographs show multiple intra-articular calcified bodies. What is the most common joint affected by synovial chondromatosis?
View Answer & Explanation
Correct Answer: D
Rationale: The text explicitly states that synovial chondromatosis "most commonly affects the knee, hip, and elbow." Among the options provided, the knee is listed as the most common site. While other joints can be affected, they are less common than the knee, hip, and elbow.
Question 2
A 50-year-old male presents with chronic right hip pain and mechanical symptoms. Radiographs show an enlarged joint capsule filled with numerous calcified cartilaginous bodies. A biopsy is performed. What degree of cytologic atypia might be observed in the cartilaginous nodules?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Microscopically, nodules of hyaline cartilage are seen. There may be some degree of cytologic atypia." This is an important point for pathologists to recognize, as some atypia can be present even in this benign condition and should not automatically be interpreted as malignancy. Severe atypia would be more concerning for malignancy. No atypia is incorrect as some can be present. Atypia is not exclusive to malignant transformation, and it is generally less severe than that seen in a true chondrosarcoma.
Question 3
A 35-year-old female presents with progressive pain and stiffness in her right hip. She reports a sensation of something "catching" in the joint. Plain radiographs show intra-articular calcifications and an enlarged joint capsule. What is the most appropriate initial imaging modality to further characterize the extent of the disease and the nature of the loose bodies?
View Answer & Explanation
Correct Answer: C
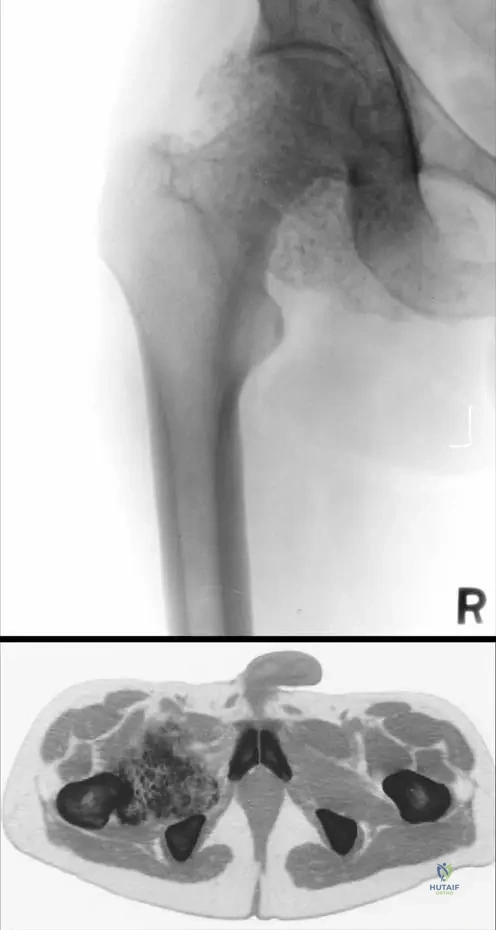
Rationale: The provided clinical context and images (Fig. 10.1 a, b) specifically highlight the utility of CT scans for synovial chondromatosis, stating "Plain radiographs (a) and CT scan (b) of synovial chondromatosis of the hip. Note the enlarged joint capsule filled by large mass of intra-articular calcified cartilaginous free bodies." While MRI can show soft tissue detail, CT is superior for characterizing calcified bodies and their extent within the joint capsule, especially when plain radiographs already show calcifications. Ultrasound can detect effusions and some superficial loose bodies but is less comprehensive for deep joints like the hip. Bone scintigraphy is for metabolic activity, and arthrography is less commonly used for initial characterization of calcified loose bodies.
Question 4
A 47-year-old male presents with chronic left hip pain, stiffness, and a decreased range of motion. Radiographs show multiple calcified intra-articular bodies. Which of the following is NOT a typical clinical symptom of synovial chondromatosis?
View Answer & Explanation
Correct Answer: D
Rationale: The text describes typical symptoms as "intermittent swelling, effusions, and progressive pain in the involved joint. Mechanical symptoms such as stiffness, joint locking, or catching may be present. Over time, patients may lose mobility and develop contractures." Acute onset, severe, burning neuropathic pain is not characteristic of synovial chondromatosis, which typically presents with mechanical and inflammatory symptoms related to the intra-articular bodies and synovial proliferation.
Question 5
A 58-year-old patient with a long history of synovial chondromatosis in the knee presents with significant joint contractures. This is a direct consequence of which aspect of the disease?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Over time, patients may lose mobility and develop contractures." This indicates that the chronic pain, stiffness, and mechanical symptoms associated with synovial chondromatosis lead to decreased use and range of motion, eventually resulting in contractures. It is not due to a systemic inflammatory response, direct nerve impingement, or primary bone involvement. Malignant transformation is a rare complication, not a direct cause of contractures.
Question 6
A 41-year-old patient presents with chronic right hip pain and mechanical symptoms. Radiographs show intra-articular calcifications. The CT scan reveals an enlarged joint capsule filled with numerous calcified cartilaginous free bodies. What is the most likely appearance of the surrounding synovium on microscopic examination?
View Answer & Explanation
Correct Answer: B
Rationale: The text states, "Microscopically... Surrounding synovium is hyperplastic." This hyperplasia is part of the proliferative nature of synovial chondromatosis, where the synovium undergoes metaplastic changes to form cartilage. Atrophic or necrotic synovium is not characteristic. While malignant transformation is rare, the typical finding is hyperplasia, not malignant infiltration. The synovium is actively involved, so it would not be normal.
Question 7
A 33-year-old female presents with chronic left knee pain and recurrent effusions. Radiographs show multiple intra-articular calcifications. The condition is described as a "benign proliferation of cartilaginous tissue." What does "benign" imply about this condition?
View Answer & Explanation
Correct Answer: C
Rationale: In medical terminology, "benign" primarily means that a tumor or growth is not cancerous, does not invade surrounding tissue, and does not typically metastasize (spread) to distant sites. While synovial chondromatosis is benign, it can recur, and there is a rare potential for malignant transformation. It does not always resolve spontaneously and can cause significant long-term functional impairment and secondary osteoarthritis. Therefore, the core meaning of benign is its non-cancerous nature and lack of metastatic potential.
Question 8
A 50-year-old patient presents with chronic right hip pain and mechanical symptoms. Plain radiographs show intra-articular calcifications. A CT scan confirms an enlarged joint capsule filled with numerous calcified cartilaginous free bodies. What is the most accurate description of the radiographic appearance of the intra-articular bodies?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "Radiographs show intra- and periarticular soft tissue masses with varying amounts of calcification." This accurately describes the appearance of the cartilaginous bodies, which can range from purely cartilaginous (radiolucent) to heavily calcified or even ossified. The image also shows varying densities. Radiolucent bodies would not be seen on plain radiographs unless they were very large and caused joint widening. Uniformly dense ossified bodies are possible but "varying amounts of calcification" is more comprehensive. Punctate/linear calcifications are not typical, and diffuse amorphous calcification is also not the most precise description.
Question 9
A 44-year-old male presents with chronic left elbow pain and stiffness. He reports occasional catching. Radiographs show multiple calcified intra-articular bodies. If these bodies were to be removed, what is the most likely long-term complication if the underlying synovial pathology is not addressed?
View Answer & Explanation
Correct Answer: C
Rationale: Synovial chondromatosis is a proliferative process of the synovium. If only the loose bodies are removed (chondrectomy) without addressing the abnormal synovium (synovectomy), the metaplastic process can continue, leading to the formation of new cartilaginous nodules and subsequent recurrence of the condition. Septic arthritis and avascular necrosis are not direct complications of incomplete treatment. Malignant transformation to osteosarcoma is incorrect as the origin is cartilage, not bone, and it's a rare event. Spontaneous fusion is not a typical outcome.
Question 10
A 39-year-old female presents with chronic right hip pain and mechanical symptoms. Radiographs show an enlarged joint capsule filled with numerous calcified cartilaginous free bodies. The patient is concerned about the nature of the condition. Which of the following statements best describes synovial chondromatosis?
View Answer & Explanation
Correct Answer: C
Rationale: The text defines synovial chondromatosis as "a benign proliferation of cartilaginous tissue arising in the synovium." This describes a metaplastic process where the synovium transforms into cartilage-producing tissue. It is not a congenital anomaly, an inflammatory autoimmune disease, or a primary malignant tumor. While it can cause inflammation, it's not primarily an autoimmune disease. It is also not a metabolic disorder leading to crystal deposition, which would describe conditions like gout or pseudogout.
Question 11
A 62-year-old patient with a long history of synovial chondromatosis in the hip presents with severe pain and significant loss of joint function. Radiographs show advanced secondary osteoarthritic changes. What is the most likely cause of these secondary changes?
View Answer & Explanation
Correct Answer: C
Rationale: The presence of numerous intra-articular loose bodies, often calcified, and the hyperplastic synovium in synovial chondromatosis lead to chronic mechanical irritation, friction, and abnormal loading within the joint. This persistent mechanical stress and inflammation contribute to the progressive degeneration of articular cartilage, ultimately resulting in secondary osteoarthritic changes. It is not primarily due to systemic inflammation, infection, autoimmune destruction, or primary bone necrosis.
Question 12
A 6-month-old male infant presents with recurrent fractures, poor feeding, and lethargy. Physical examination reveals pallor, hepatosplenomegaly, and nystagmus. Radiographs show diffuse osteosclerosis, particularly dense metaphyses, and a "bone-within-a-bone" appearance in the vertebral bodies. Laboratory studies indicate pancytopenia.
View Answer & Explanation
Correct Answer: C
Rationale: Infantile malignant osteopetrosis is characterized by severe osteosclerosis, leading to bone marrow failure (pancytopenia), nerve compression (nystagmus, optic atrophy), and hepatosplenomegaly due to extramedullary hematopoiesis. The "bone-within-a-bone" appearance is pathognomonic. Osteogenesis Imperfecta Type II presents with severe fractures but decreased bone density. Hypophosphatasia involves poor mineralization, not increased density. Pycnodysostosis has osteosclerosis but typically presents later with short stature and open fontanelles, without severe marrow failure in infancy. Craniometaphyseal dysplasia involves cranial hyperostosis and metaphyseal flaring, but not diffuse osteosclerosis or marrow failure.
Question 13
A 4-year-old girl is brought to the clinic due to multiple long bone fractures since infancy. She has blue sclera, hearing loss, and dental abnormalities. Physical examination reveals short stature and bowing of the long bones. Radiographs demonstrate diffuse osteopenia, multiple healed and healing fractures, and wormian bones in the skull.
View Answer & Explanation
Correct Answer: B
Rationale: The constellation of recurrent fractures, blue sclera, hearing loss, dental abnormalities (dentinogenesis imperfecta), and osteopenia is classic for Osteogenesis Imperfecta (OI), specifically Type I which is the mildest and most common form. Achondroplasia is a dwarfism with normal bone density. Rickets involves poor mineralization but typically lacks blue sclera or hearing loss. Hypophosphatasia also involves poor mineralization but is characterized by low alkaline phosphatase and rickets-like changes, not blue sclera. Marfan syndrome involves connective tissue abnormalities, tall stature, and joint laxity, not osteopenia or blue sclera.
Question 14
A 3-year-old boy presents with bowing of the legs, delayed motor milestones, and poor weight gain. Physical examination reveals widened growth plates and costochondral junctions. Laboratory studies show markedly low serum alkaline phosphatase, elevated pyridoxal 5'-phosphate (PLP), and hypercalcemia. Radiographs demonstrate metaphyseal irregularities, poor mineralization of the growth plates, and generalized osteopenia.
View Answer & Explanation
Correct Answer: C
Rationale: The key diagnostic features are the rickets-like presentation (bowing, widened growth plates), generalized osteopenia, and critically, the markedly low serum alkaline phosphatase with elevated PLP. This triad is pathognomonic for Hypophosphatasia, an inherited disorder of bone mineralization. Vitamin D-resistant rickets would have normal or elevated alkaline phosphatase. Osteopetrosis involves increased bone density. Scurvy presents with subperiosteal hemorrhages and metaphyseal changes but not low alkaline phosphatase. Fibrous dysplasia is a localized bone lesion, not a systemic mineralization disorder.
Question 15
A 10-year-old boy presents with short stature, disproportionately short limbs (rhizomelia), and a large head with a prominent forehead. Physical examination reveals lumbar lordosis and limited elbow extension. Radiographs show short, broad long bones with metaphyseal flaring, a narrow interpedicular distance in the lumbar spine, and a small foramen magnum.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of disproportionate short stature with rhizomelia, macrocephaly, prominent forehead, lumbar lordosis, and characteristic radiographic findings (short broad long bones, metaphyseal flaring, narrow interpedicular distance, small foramen magnum) is classic for Achondroplasia. Hypochondroplasia is a milder form with less severe features. Spondyloepiphyseal dysplasia primarily affects the spine and epiphyses, leading to short trunk dwarfism. Multiple epiphyseal dysplasia causes joint pain and epiphyseal irregularities. Diastrophic dysplasia involves clubfoot, hitchhiker thumb, and ear anomalies.
Question 16
A 12-year-old girl presents with short stature, a large head, and persistent open fontanelles. She has a history of recurrent fractures and dental crowding. Physical examination reveals a flattened midface and short distal phalanges with nail hypoplasia. Radiographs show diffuse osteosclerosis, particularly of the skull and vertebral bodies, and acro-osteolysis of the distal phalanges.
View Answer & Explanation
Correct Answer: C
Rationale: The combination of short stature, diffuse osteosclerosis, persistent open fontanelles, acro-osteolysis of the distal phalanges, and recurrent fractures is characteristic of Pycnodysostosis. This condition is caused by a defect in cathepsin K. Osteopetrosis also has osteosclerosis but typically presents with more severe complications like marrow failure or nerve compression, and lacks acro-osteolysis. Cleidocranial dysplasia involves open fontanelles and dental issues but is characterized by absent clavicles and normal bone density. Craniometaphyseal dysplasia has cranial hyperostosis but not diffuse osteosclerosis or acro-osteolysis. Osteogenesis Imperfecta involves decreased bone density.
Question 17
A 7-year-old boy is evaluated for a history of delayed tooth eruption and abnormal facial features. Physical examination reveals a large head, prominent forehead, and widely spaced eyes. He is able to approximate his shoulders in front of his chest. Radiographs show hypoplastic or absent clavicles, persistent wide cranial sutures, and multiple unerupted supernumerary teeth.
View Answer & Explanation
Correct Answer: B
Rationale: The classic triad of hypoplastic or absent clavicles (allowing approximation of shoulders), persistent wide cranial sutures/open fontanelles, and dental anomalies (delayed eruption, supernumerary teeth) is diagnostic for Cleidocranial Dysplasia. Achondroplasia involves rhizomelia and normal clavicles. Pycnodysostosis has open fontanelles but also osteosclerosis and acro-osteolysis. Craniometaphyseal dysplasia involves cranial hyperostosis and metaphyseal flaring. Osteogenesis Imperfecta involves osteopenia and fractures.
Question 18
A 5-year-old boy presents with progressive hearing loss, visual impairment, and a "leonine facies." His parents note his head appears unusually large and dense. Radiographs show marked hyperostosis of the skull base and facial bones, with sclerosis extending into the metaphyses of long bones, giving a "club-shaped" appearance.
View Answer & Explanation
Correct Answer: C
Rationale: The combination of progressive cranial hyperostosis (leading to nerve compression and "leonine facies"), and metaphyseal flaring ("club-shaped" long bones) is characteristic of Craniometaphyseal Dysplasia. Osteopetrosis has diffuse osteosclerosis and marrow failure. Pycnodysostosis has osteosclerosis and acro-osteolysis. Camurati-Engelmann disease involves diaphyseal hyperostosis and muscle weakness, not primarily cranial hyperostosis or metaphyseal flaring. Fibrous dysplasia is a localized lesion.
Question 19
A 14-year-old male presents with chronic hip and knee pain, worse with activity. He has a history of mild short stature. Physical examination reveals limited range of motion in multiple large joints. Radiographs show flattened and irregular epiphyses, particularly in the femoral heads and knees, with early degenerative changes.
View Answer & Explanation
Correct Answer: C
Rationale: The presentation of chronic joint pain, mild short stature, and characteristic radiographic findings of flattened and irregular epiphyses with early osteoarthritis is classic for Multiple Epiphyseal Dysplasia (MED). Achondroplasia primarily affects metaphyses and has rhizomelia. Spondyloepiphyseal Dysplasia Congenita involves significant spinal involvement and short trunk dwarfism. Pseudochondroplasia is a severe epiphyseal dysplasia with more pronounced short stature. Diastrophic dysplasia has specific limb and ear anomalies.
Question 20
A 2-year-old girl presents with severe short stature, bilateral clubfeet, and a "hitchhiker's thumb" deformity. Physical examination reveals a cleft palate and cauliflower-like ears due to calcification. Radiographs show short, broad long bones, severe clubfoot deformities, and characteristic short, oval first metacarpals.
View Answer & Explanation
Correct Answer: D
Rationale: The combination of severe short stature, bilateral clubfeet, "hitchhiker's thumb" (abducted thumb), cleft palate, and calcified/cauliflower ears is pathognomonic for Diastrophic Dysplasia. Achondroplasia has rhizomelia but lacks these specific hand/foot/ear anomalies. Spondyloepiphyseal dysplasia primarily affects the spine and epiphyses. Multiple epiphyseal dysplasia causes joint pain and epiphyseal irregularities. Hypochondroplasia is a milder form of achondroplasia.
Question 21
A 6-month-old infant is diagnosed with Infantile Malignant Osteopetrosis. Which of the following is the most effective definitive treatment to prevent progressive neurological complications and bone marrow failure?
View Answer & Explanation
Correct Answer: C
Rationale: Infantile malignant osteopetrosis is caused by defective osteoclast function. Hematopoietic Stem Cell Transplantation (HSCT) can introduce functional osteoclast precursors, leading to the development of normal osteoclasts that can resorb bone, thereby alleviating marrow compression and nerve impingement. Bisphosphonates inhibit osteoclast activity, which would worsen osteopetrosis. Vitamin D and calcitonin are not definitive treatments for the underlying osteoclast defect. Growth hormone therapy is irrelevant to the pathophysiology of osteopetrosis.
Question 22
A 1-year-old boy with Osteogenesis Imperfecta Type III presents with severe bowing of the femurs and tibias, making ambulation impossible. He has already sustained multiple fractures. Which of the following surgical interventions is most appropriate to improve his mobility and prevent further fractures?
View Answer & Explanation
Correct Answer: C
Rationale: For severe bowing and recurrent fractures in Osteogenesis Imperfecta, particularly Type III, intramedullary rodding (e.g., with Fassier-Duval telescoping rods) combined with corrective osteotomies is the gold standard. This provides internal stabilization, corrects deformity, and reduces fracture risk. External fixation carries higher risks of infection and pin tract complications in these fragile bones. Serial casting and bracing are insufficient for severe bowing and recurrent fractures. Arthrodesis is too drastic and would eliminate joint function. Amputation is not indicated unless limb salvage is impossible due to severe, untreatable complications.
Question 23
A 3-month-old infant is diagnosed with Achondroplasia. The parents are concerned about potential neurological complications. Which of the following is the most critical area to monitor for potential neurological compromise in infancy?
View Answer & Explanation
Correct Answer: C
Rationale: Foramen magnum stenosis is the most critical neurological complication in infants with achondroplasia. It can lead to brainstem compression, hydrocephalus, central apnea, and sudden death. Lumbar spinal canal stenosis is more common in older children and adults. Cervical instability is less common than foramen magnum stenosis in infancy. While hydrocephalus can occur, it is often secondary to foramen magnum stenosis. Peripheral nerve entrapment is rare in infancy.
Question 24
A 25-year-old man with a known history of Achondroplasia presents with progressive lower extremity weakness, numbness, and claudication-like symptoms. Physical examination reveals hyperreflexia and a positive Babinski sign. Radiographs of the spine show severe narrowing of the lumbar spinal canal. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: D
Rationale: The patient's symptoms (progressive weakness, numbness, claudication-like pain) combined with neurological signs (hyperreflexia, Babinski) and radiographic evidence of severe lumbar spinal canal stenosis indicate myelopathy. Surgical decompression (laminectomy) is the definitive treatment for symptomatic spinal stenosis in achondroplasia. Conservative measures like physical therapy, corticosteroids, injections, or bracing are generally ineffective for progressive neurological deficits due to severe structural compression.
Question 25
A 6-year-old boy with Osteogenesis Imperfecta Type IV is being managed with intravenous bisphosphonates. Which of the following is a potential serious complication of long-term bisphosphonate therapy in children?
View Answer & Explanation
Correct Answer: B
Rationale: Atypical femoral fractures (AFFs) are a recognized, albeit rare, complication of long-term bisphosphonate use in both adults and children. These fractures typically occur in the subtrochanteric or diaphyseal region of the femur with minimal or no trauma. Bisphosphonates do not increase the risk of osteosarcoma, cause hypercalcemia (they typically lower calcium), or directly cause renal failure (though some forms require renal dose adjustment). Blue sclera is a feature of OI itself and is not worsened by bisphosphonates.
Question 26
A 1-month-old infant presents with severe respiratory distress and a bell-shaped chest. Radiographs show extremely short, broad long bones, platyspondyly, and very small iliac wings. The parents report a family history of similar findings, with affected individuals dying shortly after birth. This presentation is most consistent with a lethal skeletal dysplasia. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: The severe short-limbed dwarfism, bell-shaped chest leading to respiratory distress, platyspondyly, and small iliac wings, with a lethal outcome, are characteristic features of Thanatophoric Dysplasia. Achondroplasia and Hypochondroplasia are non-lethal. Spondyloepiphyseal Dysplasia Congenita is also non-lethal and primarily affects the spine and epiphyses, leading to short trunk dwarfism. Diastrophic dysplasia is non-lethal and has specific limb and ear anomalies.
Question 27
A 4-year-old boy with a history of recurrent fractures and osteopenia is found to have a mutation in the COL1A1 gene. This genetic finding is most consistent with which of the following conditions?
View Answer & Explanation
Correct Answer: C
Rationale: Mutations in COL1A1 or COL1A2 genes, which encode for type I collagen, are the primary genetic cause of Osteogenesis Imperfecta (OI). Achondroplasia is caused by mutations in FGFR3. Osteopetrosis has various genetic causes, often involving genes related to osteoclast function (e.g., TCIRG1, CLCN7). Hypophosphatasia is caused by mutations in ALPL. Pycnodysostosis is caused by mutations in CTSK (cathepsin K).
Question 28
A 15-year-old girl with Spondyloepiphyseal Dysplasia Congenita (SEDC) presents with progressive kyphoscoliosis and neck pain. Physical examination reveals a short trunk, waddling gait, and hyperlaxity of the cervical spine. Radiographs show platyspondyly, odontoid hypoplasia, and significant atlantoaxial instability. What is the most critical management consideration for this patient?
View Answer & Explanation
Correct Answer: C
Rationale: Odontoid hypoplasia and atlantoaxial instability are common and potentially life-threatening complications in SEDC due to the risk of spinal cord compression. Given the progressive symptoms and radiographic evidence of significant instability, surgical stabilization of the cervical spine is the most critical management consideration to prevent neurological injury. Bracing may help with kyphoscoliosis but does not address severe cervical instability. Physical therapy and NSAIDs are insufficient for structural instability. Growth hormone therapy is not indicated for this complication.
Question 29
A 7-year-old boy presents with progressive muscle weakness, bone pain, and hyperostosis of the long bone diaphyses. Radiographs show symmetrical cortical thickening and sclerosis of the diaphyses of the femurs, tibias, and humeri, with relative sparing of the epiphyses and metaphyses. This presentation is most consistent with which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The key features are progressive muscle weakness, bone pain, and symmetrical diaphyseal hyperostosis (cortical thickening and sclerosis of the diaphyses of long bones), which are characteristic of Camurati-Engelmann Disease (Progressive Diaphyseal Dysplasia). Osteopetrosis involves diffuse osteosclerosis affecting all parts of the bone. Craniometaphyseal dysplasia primarily affects the skull and metaphyses. Melorheostosis is a localized, "flowing candle wax" hyperostosis, typically asymmetrical. Fibrous dysplasia is a localized lesion with a "ground glass" appearance.
Question 30
A 5-year-old boy with a history of multiple fractures and blue sclera is being evaluated for a new fracture. His parents are concerned about the inheritance pattern. Genetic testing confirms a dominant negative mutation in the COL1A1 gene. What is the most likely inheritance pattern for this child's condition?
View Answer & Explanation
Correct Answer: C
Rationale: The most common forms of Osteogenesis Imperfecta (Types I, II, III, IV), which are caused by mutations in COL1A1 or COL1A2 genes, are inherited in an autosomal dominant pattern. A dominant negative mutation means that the abnormal protein product interferes with the function of the normal protein, even if only one copy of the gene is affected. Autosomal recessive and X-linked patterns are seen in rarer forms of OI or other skeletal dysplasias, but not typically with COL1A1 mutations.
Question 31
A 1-year-old infant presents with short stature, a short trunk, and a waddling gait. Radiographs show severe platyspondyly, pear-shaped vertebral bodies, and delayed ossification of the epiphyses, particularly in the hips and knees. The long bones appear relatively normal in length. This constellation of findings is most consistent with which of the following?
View Answer & Explanation
Correct Answer: C
Rationale: The key features of short trunk dwarfism, severe platyspondyly (flattened vertebral bodies), pear-shaped vertebral bodies, and delayed/dysplastic epiphyseal ossification (especially hip and knee) with relatively normal long bone length are characteristic of Spondyloepiphyseal Dysplasia Congenita (SEDC). Achondroplasia and Hypochondroplasia are short-limbed dwarfisms with normal spinal length. Multiple Epiphyseal Dysplasia primarily affects epiphyses but typically has less severe spinal involvement and normal trunk length. Metaphyseal Chondrodysplasia affects the metaphyses, not primarily the spine or epiphyses in this manner.
Question 32
A neonate is born with severe micromelia, multiple intrauterine fractures, and pulmonary hypoplasia. Radiographs reveal extremely short, broad long bones with crumpled appearance and poor skull ossification. The infant succumbs shortly after birth due to respiratory insufficiency.
View Answer & Explanation
Correct Answer: B
Rationale: The clinical presentation of severe micromelia, multiple intrauterine fractures, pulmonary hypoplasia, and poor skull ossification leading to neonatal death is classic for Osteogenesis Imperfecta (OI) Type II, which is the perinatal lethal form. This type is characterized by severe bone fragility and often results in stillbirth or death shortly after birth due to respiratory compromise from rib fractures and pulmonary hypoplasia. The main distractor, Hypophosphatasia, perinatal lethal form (D), also presents with severe skeletal mineralization defects and respiratory distress, but radiographs typically show absent or severely deficient mineralization, particularly of the skull and long bones, rather than the crumpled, broad bones seen in OI Type II.
Question 33
An 8-month-old infant presents with progressive macrocephaly, nystagmus, and failure to thrive. Physical examination reveals hepatosplenomegaly and optic atrophy. Laboratory studies show pancytopenia. Radiographs demonstrate diffuse osteosclerosis, particularly prominent in the skull base and vertebral endplates, with a "bone-within-a-bone" appearance in the vertebrae and long bones.
View Answer & Explanation
Correct Answer: C
Rationale: The constellation of diffuse osteosclerosis, macrocephaly, optic atrophy, pancytopenia, hepatosplenomegaly, and the characteristic "bone-within-a-bone" radiographic appearance in an infant is pathognomonic for Infantile Malignant Osteopetrosis (also known as Autosomal Recessive Osteopetrosis). This severe form is caused by defective osteoclast function, leading to impaired bone resorption and accumulation of dense, brittle bone. The increased bone density encroaches on marrow spaces (causing pancytopenia) and cranial nerve foramina (causing optic atrophy and hearing loss). Pyknodysostosis (B) also presents with dense bones and open fontanelles, but typically includes short stature, acro-osteolysis, and multiple fractures, without the severe cranial nerve compression or pancytopenia seen in malignant osteopetrosis.
Question 34
A 3-day-old neonate presents with severe respiratory distress and hypotonia. Physical examination reveals a soft skull, short limbs, and a bell-shaped chest. Radiographs show severe undermineralization of the entire skeleton, with almost complete absence of ossification of the calvarium and marked metaphyseal lucencies in the long bones. Laboratory tests reveal extremely low serum alkaline phosphatase levels.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical picture of severe undermineralization, particularly of the skull, short limbs, respiratory distress, and extremely low serum alkaline phosphatase in a neonate is characteristic of the perinatal lethal form of Hypophosphatasia. This condition is caused by mutations in the ALPL gene, leading to a deficiency of tissue-nonspecific alkaline phosphatase, which is crucial for bone mineralization. Osteogenesis Imperfecta Type II (A) also presents with severe skeletal abnormalities and is lethal, but it is characterized by multiple fractures and crumpled bones due to defective collagen, not primarily by severe undermineralization and low alkaline phosphatase.
Question 35
A 10-year-old boy presents with short stature, frequent fractures, and a large head with persistent open fontanelles. Physical examination reveals a small jaw, dental malocclusion, and short, broad hands with nail dysplasia. Radiographs show generalized osteosclerosis, particularly of the skull and vertebral bodies, along with acro-osteolysis of the distal phalanges and absence of the mandibular angle.
View Answer & Explanation
Correct Answer: B
Rationale: The combination of short stature, frequent fractures, open fontanelles, small jaw, acro-osteolysis, and generalized osteosclerosis is highly suggestive of Pyknodysostosis. This autosomal recessive disorder is caused by a deficiency of cathepsin K, an enzyme involved in bone resorption. The dense, brittle bones are prone to fracture, and the characteristic craniofacial features (open fontanelles, small jaw) and acro-osteolysis are key diagnostic clues. Infantile Malignant Osteopetrosis (C) also causes dense bones but typically presents in infancy with more severe complications like pancytopenia and cranial nerve compression, and lacks the acro-osteolysis and specific facial features of pyknodysostosis.
Question 36
A 7-year-old girl presents with a history of 5 long bone fractures since toddlerhood, typically from minor trauma. Her parents note her sclerae have always appeared bluish. She has normal stature for her age, and a recent audiogram shows mild conductive hearing loss. Radiographs show generalized osteopenia with slender long bones and evidence of healed fractures.
View Answer & Explanation
Correct Answer: A
Rationale: This clinical presentation is classic for Osteogenesis Imperfecta (OI) Type I, the mildest and most common form. Key features include recurrent fractures from minimal trauma, blue sclerae, normal or near-normal stature, and often early-onset hearing loss. It is an autosomal dominant condition caused by quantitative defects in Type I collagen. OI Type IV (D) also presents with recurrent fractures and normal sclerae, but typically involves moderate short stature and greater bone deformity than Type I.
Question 37
A 5-year-old boy is referred for progressive facial dysmorphism and hearing loss. His parents describe a widening of his jaw and forehead. Radiographs reveal progressive sclerosis and thickening of the skull, particularly the cranial base and facial bones, along with metaphyseal flaring of the long bones, giving them an "Erlenmeyer flask" appearance. Bone density in the diaphyses is normal.
View Answer & Explanation
Correct Answer: B
Rationale: The combination of progressive facial dysmorphism, hearing loss (due to cranial nerve compression from skull sclerosis), and metaphyseal flaring (Erlenmeyer flask deformity) with normal diaphyseal bone density is characteristic of Craniometaphyseal Dysplasia (CMD). This condition involves abnormal bone modeling, particularly affecting the skull and metaphyses. Pyle Disease (A) also presents with severe metaphyseal flaring (Erlenmeyer flask deformity) but typically lacks the significant cranial sclerosis and facial dysmorphism seen in CMD.
Question 38
An 18-year-old male presents with progressive facial enlargement, particularly of the mandible, and a history of syndactyly of the second and third fingers. He is notably tall for his age. Radiographs show extreme generalized osteosclerosis, especially marked in the skull and long bone cortices, with obliteration of the medullary canals. Bone biopsy reveals markedly increased bone formation.
View Answer & Explanation
Correct Answer: B
Rationale: The key features of progressive facial enlargement (mandibular overgrowth), syndactyly, gigantism, and severe generalized osteosclerosis due to increased bone formation are pathognomonic for Sclerosteosis. This rare autosomal recessive disorder is caused by mutations in the SOST gene, leading to a deficiency of sclerostin, a negative regulator of bone formation. Van Buchem Disease (A) is a milder autosomal recessive disorder also involving increased bone density due to LRP5 mutations, but it typically lacks the syndactyly and gigantism seen in sclerosteosis, and the bone overgrowth is generally less severe.
Question 39
A 35-year-old man presents with a history of progressive thickening of his jaw and forehead, leading to facial asymmetry. He denies any history of fractures or significant pain. Physical examination is otherwise unremarkable, with no syndactyly or gigantism. Radiographs show generalized cortical thickening and increased bone density, particularly in the skull, mandible, and diaphyses of long bones, but without obliteration of the medullary canal.
View Answer & Explanation
Correct Answer: C
Rationale: The presentation of progressive cortical thickening and increased bone density, especially in the skull and mandible, without syndactyly or gigantism, is characteristic of Van Buchem Disease. This autosomal recessive disorder is caused by a deletion downstream of the SOST gene, leading to increased Wnt signaling and enhanced bone formation. It is a milder form of high bone mass disorder compared to sclerosteosis. Sclerosteosis (A) is a more severe condition with similar bone overgrowth but typically includes syndactyly and gigantism, which are absent in this patient.
Question 40
A 6-year-old girl is diagnosed with Osteogenesis Imperfecta Type III. Her condition is characterized by severe bone fragility, progressive deformities, and short stature. Which of the following is the primary underlying genetic defect responsible for most forms of Osteogenesis Imperfecta?
View Answer & Explanation
Correct Answer: B
Rationale: The vast majority of Osteogenesis Imperfecta (OI) cases, including Type III, are caused by mutations in the COL1A1 or COL1A2 genes, which encode the alpha-1 and alpha-2 chains of Type I collagen, respectively. These mutations lead to either a quantitative deficiency or a structural defect in Type I collagen, resulting in brittle bones and other connective tissue abnormalities. Deficiency in tissue-nonspecific alkaline phosphatase (A) is the cause of Hypophosphatasia, while impaired osteoclast function (C) is the hallmark of Osteopetrosis. Mutations in the SOST gene (D) cause Sclerosteosis, and deficiency in cathepsin K (E) causes Pyknodysostosis.
Question 41
A 4-month-old infant is diagnosed with Infantile Malignant Osteopetrosis, presenting with severe anemia, thrombocytopenia, and progressive vision loss due to optic nerve compression. The parents are seeking information on the most effective definitive treatment for this condition.
View Answer & Explanation
Correct Answer: C
Rationale: The definitive treatment for Infantile Malignant Osteopetrosis is hematopoietic stem cell transplantation (HSCT). This procedure aims to replace the defective osteoclasts (derived from hematopoietic stem cells) with functional ones, thereby restoring normal bone resorption and reversing the disease progression, including the hematologic and neurologic complications. While interferon gamma-1b (B) can be used as an adjunct to stimulate osteoclast activity, and surgical decompression (E) may be necessary for acute cranial nerve compression, neither is a definitive cure. Corticosteroids (A) and bisphosphonates (D) are not primary treatments for this condition.
Question 42
A 2-year-old child is diagnosed with childhood-onset Hypophosphatasia, characterized by rickets, premature tooth loss, and low serum alkaline phosphatase. Genetic testing is recommended to confirm the diagnosis and for family counseling. Which gene is typically implicated in Hypophosphatasia?
View Answer & Explanation
Correct Answer: B
Rationale: Hypophosphatasia is caused by mutations in the ALPL gene, which encodes the tissue-nonspecific alkaline phosphatase (TNSALP) enzyme. A deficiency in TNSALP leads to impaired mineralization of bone and teeth. COL1A1 (A) is associated with Osteogenesis Imperfecta. SOST (C) is associated with Sclerosteosis. LRP5 (D) is associated with high bone mass disorders like Van Buchem disease and some forms of osteoporosis. CTSK (E) is associated with Pyknodysostosis.
Question 43
A 6-month-old infant presents with symptoms consistent with osteopetrosis. The underlying pathophysiology of osteopetrosis involves a primary defect in which of the following cellular processes?
View Answer & Explanation
Correct Answer: C
Rationale: Osteopetrosis, regardless of its specific genetic cause, is characterized by a primary defect in osteoclast-mediated bone resorption. Osteoclasts are responsible for breaking down old bone, and when their function is impaired, bone accumulates, leading to increased bone density, obliteration of marrow spaces, and brittle bones. Increased osteoblast activity (A) is seen in conditions like sclerosteosis and Van Buchem disease. Defective collagen synthesis (D) is the hallmark of Osteogenesis Imperfecta. Abnormal mineralization of osteoid (E) is seen in rickets and osteomalacia, and specifically in hypophosphatasia.
Question 44
A 4-year-old child presents with genu valgum and a waddling gait. Radiographs of the lower extremities reveal marked widening and flaring of the metaphyses of the long bones, particularly the distal femurs, resembling an "Erlenmeyer flask." Bone density appears normal. Which of the following skeletal dysplasias is most commonly associated with this specific radiographic finding?
View Answer & Explanation
Correct Answer: C
Rationale: The "Erlenmeyer flask" deformity, characterized by marked metaphyseal flaring of long bones, is a classic radiographic finding in Pyle Disease (Familial Metaphyseal Dysplasia). This condition is a rare autosomal recessive disorder of bone modeling, where the metaphyses fail to undergo normal tubulation. While other conditions like Gaucher disease, Niemann-Pick disease, and some forms of osteopetrosis can also show this finding, Pyle disease is a primary skeletal dysplasia defined by this modeling defect. Osteogenesis Imperfecta (A) is characterized by osteopenia and fractures. Infantile Malignant Osteopetrosis (B) shows diffuse osteosclerosis. Hypophosphatasia (D) presents with undermineralization and rickets. Achondroplasia (E) involves short limbs with rhizomelic shortening and specific metaphyseal changes, but not typically the classic Erlenmeyer flask deformity.
Question 45
A 9-year-old boy has a history of multiple fractures, moderate short stature, and mild bowing of the long bones. His sclerae are noted to be normal (white), and he has no significant hearing impairment. Dental examination reveals dentinogenesis imperfecta. Based on these findings, which type of Osteogenesis Imperfecta is most likely?
View Answer & Explanation
Correct Answer: D
Rationale: Osteogenesis Imperfecta Type IV is characterized by recurrent fractures, moderate short stature, and normal (white) sclerae. Dentinogenesis imperfecta is a common feature. This distinguishes it from Type I (blue sclerae, normal stature) and Type III (severe progressive deformity, very short stature, often blue/grey sclerae). Type II is perinatal lethal, and Type V has specific features like calcification of interosseous membranes and hyperplastic callus formation. The absence of blue sclerae rules out Type I, and the moderate severity with normal sclerae points to Type IV over the more severe Type III.
Question 46
A 45-year-old woman presents with chronic foot pain and a history of recurrent stress fractures in her lower extremities. She also reports premature loss of her adult teeth in her 30s. Laboratory tests reveal persistently low serum alkaline phosphatase levels, with elevated pyridoxal 5'-phosphate (PLP) and phosphoethanolamine (PEA) in her urine. Bone density scan shows osteopenia.
View Answer & Explanation
Correct Answer: C
Rationale: The combination of recurrent stress fractures, premature adult tooth loss, osteopenia, and persistently low serum alkaline phosphatase with elevated PLP and PEA is diagnostic of adult Hypophosphatasia. This form is typically milder than the childhood or perinatal forms but still results from a deficiency in tissue-nonspecific alkaline phosphatase, leading to impaired mineralization. Osteoporosis (A) involves osteopenia and fractures but typically has normal alkaline phosphatase. Osteomalacia (D) also involves impaired mineralization but is usually due to vitamin D deficiency and presents with low or normal alkaline phosphatase, but not typically the specific biochemical markers of hypophosphatasia or premature tooth loss.
Question 47
A 6-year-old boy presents with severe facial dysmorphism, including hypertelorism and a broad nasal bridge. He has progressive hearing loss and visual impairment due to cranial nerve compression. Radiographs show marked sclerosis and thickening of the skull, especially the cranial base, along with significant widening and sclerosis of the diaphyses of the long bones, resembling a "club-like" appearance. The metaphyses are also affected but less severely than the diaphyses.
View Answer & Explanation
Correct Answer: B
Rationale: The severe facial dysmorphism, cranial nerve compression, and particularly the marked diaphyseal widening and sclerosis of long bones, along with skull sclerosis, are characteristic of Craniodiaphyseal Dysplasia. This condition is distinct from Craniometaphyseal Dysplasia (A) by its predominant involvement of the diaphyses, leading to a "club-like" appearance of the long bones, in addition to the cranial abnormalities. Craniometaphyseal Dysplasia (A) primarily affects the skull and metaphyses, with less severe or absent diaphyseal involvement. Pyle Disease (C) primarily affects metaphyses with flaring but no significant sclerosis or cranial involvement.
Question 48
A genetic counselor is discussing different forms of osteopetrosis with the parents of a newborn diagnosed with the condition. They are particularly concerned about the prognosis and severity. Which genetic inheritance pattern is typically associated with the most severe, life-threatening form of osteopetrosis that presents in infancy?
View Answer & Explanation
Correct Answer: B
Rationale: The most severe, life-threatening form of osteopetrosis, known as Infantile Malignant Osteopetrosis, is typically inherited in an autosomal recessive pattern. This form presents in infancy with severe complications such as pancytopenia, cranial nerve compression, and failure to thrive, often leading to early mortality without treatment. Autosomal dominant (A) forms of osteopetrosis (e.g., Albers-Schönberg disease) are generally milder, presenting later in life with fewer complications and a better prognosis.
Question 49
A 58-year-old male presents with a 3-year history of recurrent, painless swelling of his left knee, often accompanied by a feeling of fullness and occasional stiffness. Physical examination reveals a moderate knee effusion, no warmth or erythema, and full range of motion with mild crepitus. Plain radiographs show mild degenerative changes in the patellofemoral joint but no loose bodies. MRI of the knee demonstrates diffuse, frond-like synovial proliferation within the suprapatellar pouch, exhibiting signal intensity identical to subcutaneous fat on all sequences, including fat-suppressed images.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical presentation of chronic, painless knee effusion with the pathognomonic MRI finding of frond-like synovial proliferation exhibiting fat signal intensity on all sequences, including fat-suppressed images, is diagnostic for Lipoma Arborescens. PVNS typically shows low signal intensity on T1 and T2 due to hemosiderin deposition. Synovial chondromatosis would show chondral loose bodies. Rheumatoid arthritis would present with inflammatory signs and specific serological markers, and synovial hemangioma would show vascular characteristics on MRI.
Question 50
A 62-year-old female complains of chronic, progressive knee pain and swelling for the past 18 months. She reports intermittent catching sensations but no true locking. Physical examination reveals a large, soft, non-tender effusion in the right knee. Radiographs show mild tricompartmental osteoarthritis. An MRI is ordered to further evaluate the synovial changes. Which of the following MRI characteristics is most indicative of Lipoma Arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The hallmark MRI finding for Lipoma Arborescens is villous or frond-like synovial proliferation with signal intensity identical to subcutaneous fat on all sequences, including fat-suppressed images. This fat signal is key to distinguishing it from other synovial pathologies. Low signal intensity on T1 and T2 (A) is characteristic of PVNS. Multiple calcified loose bodies (B) suggest synovial chondromatosis. Extensive synovial enhancement (D) is seen in inflammatory synovitis or PVNS. Prominent flow voids (E) would suggest a vascular lesion like a hemangioma.
Question 51
A 48-year-old male presents with a 1-year history of left knee swelling and discomfort. He denies any specific trauma but notes the swelling is persistent. Physical examination reveals a palpable, doughy suprapatellar mass and a moderate effusion. Arthrocentesis yields straw-colored fluid. An MRI is performed, showing extensive frond-like synovial proliferation with high signal on T1 and T2, which completely suppresses on fat-saturated sequences. What is the most appropriate definitive treatment for this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The MRI findings are classic for Lipoma Arborescens. While conservative measures like NSAIDs, injections, and aspirations may provide temporary relief, they do not address the underlying pathology. Arthroscopic synovectomy, which involves surgical excision of the hypertrophied synovial tissue, is considered the definitive treatment for Lipoma Arborescens and typically results in excellent long-term outcomes. Radiation therapy is not indicated for this benign condition.
Question 52
A 52-year-old female presents with chronic, insidious onset of right knee pain and swelling. She has a history of mild osteoarthritis in the same knee. Physical examination reveals a moderate effusion and mild tenderness along the joint line. Plain radiographs show joint space narrowing and osteophytes consistent with osteoarthritis. An MRI is ordered to investigate the persistent effusion. The MRI report describes villous synovial proliferation with signal characteristics identical to mature adipose tissue. Which of the following conditions is the most important differential diagnosis to exclude based on MRI findings?
View Answer & Explanation
Correct Answer: B
Rationale: Given the MRI findings suggestive of Lipoma Arborescens, Pigmented Villonodular Synovitis (PVNS) is the most critical differential diagnosis to exclude. Both conditions present with synovial proliferation and chronic effusion. However, PVNS is characterized by hemosiderin deposition, which results in low signal intensity on T1 and T2-weighted MRI sequences, often with "blooming" on gradient echo images, distinctly different from the fat signal seen in Lipoma Arborescens. Gout, septic arthritis, osteochondritis dissecans, and meniscal tears have different clinical presentations and distinct MRI features.
Question 53
A 68-year-old male undergoes arthroscopic synovectomy for a diagnosis of Lipoma Arborescens in his left knee. During the procedure, the surgeon notes diffuse, yellowish, frond-like synovial tissue. What is the expected histological finding upon pathological examination of the resected tissue?
View Answer & Explanation
Correct Answer: B
Rationale: Lipoma Arborescens is histologically characterized by a villous proliferation of mature adipocytes (fat cells) within the subsynovial connective tissue, often accompanied by chronic inflammatory changes. This explains the yellowish appearance observed arthroscopically and the fat signal on MRI. Hemosiderin-laden macrophages (A) are characteristic of PVNS. Cartilaginous metaplasia (C) is seen in synovial chondromatosis. Granulomatous inflammation (D) is associated with conditions like tuberculosis or sarcoidosis. Atypical spindle cells (E) would raise concern for malignancy.
Question 54
A 50-year-old female presents with a 6-month history of intermittent swelling and mild pain in her right shoulder. She reports a limited range of motion, particularly with overhead activities. Physical examination reveals a mild effusion and tenderness in the glenohumeral joint. Radiographs are unremarkable. An MRI shows diffuse, frond-like synovial proliferation within the joint, demonstrating signal intensity consistent with fat. While most commonly found in the knee, Lipoma Arborescens can occur in other joints. Which of the following is the most frequently affected joint?
View Answer & Explanation
Correct Answer: D
Rationale: Lipoma Arborescens is overwhelmingly most common in the knee, particularly affecting the suprapatellar pouch. While it can occur in other joints such as the hip, shoulder, ankle, and elbow, these are much rarer presentations. The question describes a shoulder presentation, but asks for the most frequently affected joint overall.
Question 55
A 70-year-old male with a long-standing history of osteoarthritis presents with worsening knee pain and a persistent, large effusion that has been refractory to conservative management, including multiple aspirations and corticosteroid injections. An MRI confirms the diagnosis of Lipoma Arborescens. What is the typical long-term prognosis following complete arthroscopic synovectomy for Lipoma Arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma Arborescens is a benign condition, and complete arthroscopic synovectomy typically provides an excellent long-term prognosis with rare recurrence. The condition does not lead to progressive joint destruction beyond what might be associated with underlying osteoarthritis, nor does it carry a risk of malignant transformation. Surgical intervention is usually highly effective in resolving symptoms.
Question 56
A 59-year-old female presents with a 2-year history of intermittent, non-traumatic swelling of her right knee. She reports no significant pain but notes a feeling of "fullness" and occasional stiffness. Physical examination reveals a moderate effusion. Plain radiographs are normal. An MRI is performed, showing diffuse synovial proliferation with signal intensity identical to fat. Which of the following conditions is most frequently associated with Lipoma Arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma Arborescens is frequently associated with underlying osteoarthritis, as well as chronic joint effusions or trauma. While its exact etiology is unknown, it is often considered a reactive process. It is not typically associated with inflammatory arthropathies like rheumatoid arthritis, psoriatic arthritis, gout, or systemic lupus erythematosus, which have distinct pathological mechanisms and clinical presentations.
Question 57
A 65-year-old male presents with chronic left hip pain and stiffness that has been worsening over the past year. He denies any history of trauma. Physical examination reveals a painful limited range of motion, particularly with internal rotation. Plain radiographs show mild degenerative changes in the hip joint. Due to persistent symptoms and suspicion of intra-articular pathology, an MRI is performed. The MRI reveals extensive villous synovial proliferation within the hip joint capsule, demonstrating signal characteristics consistent with mature fat. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The MRI findings of extensive villous synovial proliferation with signal characteristics consistent with mature fat are pathognomonic for Lipoma Arborescens. While less common in the hip than the knee, the imaging features are definitive. Synovial chondromatosis would show chondral loose bodies. PVNS would show low signal intensity due to hemosiderin. Avascular necrosis would show characteristic changes in the femoral head. Septic arthritis would present acutely with systemic signs and specific fluid analysis.
Question 58
A 53-year-old female presents with a 9-month history of intermittent right knee swelling and a feeling of "giving way." She denies any acute injury. Physical examination reveals a moderate effusion and mild tenderness along the medial joint line. Plain radiographs of the knee are obtained. What are the typical findings on plain radiographs in a patient with Lipoma Arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: Plain radiographs in Lipoma Arborescens are often normal or may show non-specific findings such as joint effusion or soft tissue prominence. Given its frequent association with osteoarthritis, signs of degenerative changes (joint space narrowing, osteophytes) may also be present. Radiopaque loose bodies (A) are characteristic of synovial chondromatosis. Diffuse osteopenia and joint space narrowing (B) are common in inflammatory arthritis. Subchondral cysts and erosions (D) can be seen in various arthropathies, including PVNS or inflammatory arthritis. Periosteal reaction and bone destruction (E) would suggest infection or malignancy.
Question 59
A 60-year-old male presents with chronic left knee pain and swelling. An MRI reveals extensive synovial proliferation with signal intensity identical to fat, confirming Lipoma Arborescens. The patient is scheduled for arthroscopic synovectomy. Which of the following is a potential intraoperative challenge or consideration during arthroscopic management of Lipoma Arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The diffuse, frond-like, and often extensive nature of Lipoma Arborescens can make complete arthroscopic resection challenging, especially in areas difficult to access. Incomplete resection can lead to persistent symptoms. The lesion is typically yellowish and distinct from normal synovium (A). It is not highly vascularized (B) like a hemangioma, and bleeding is usually manageable. The tissue is soft, not hard or calcified (D). While very extensive cases might require an open approach, arthroscopy is generally preferred and feasible (E).
Question 60
A 55-year-old female presents with a 1-year history of recurrent, non-traumatic knee effusion. Physical examination reveals a large, soft effusion in the suprapatellar pouch. An ultrasound of the knee is performed, which shows hyperechoic, villous projections within the joint fluid. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Ultrasound findings of hyperechoic, villous projections within a joint effusion are characteristic of Lipoma Arborescens, reflecting the fatty synovial proliferation. While MRI is the gold standard, ultrasound can be a useful initial imaging modality. Septic arthritis would show hypoechoic fluid with debris and possibly synovial thickening. Gout would show characteristic crystal deposits (double contour sign). Rheumatoid arthritis would show synovial hypertrophy with increased vascularity on Doppler. Osteochondritis dissecans is a cartilage lesion, not primarily a synovial condition.
Question 61
A 63-year-old male presents with chronic right knee pain and swelling. He has a history of mild osteoarthritis. An MRI confirms Lipoma Arborescens. The patient asks about the underlying cause of his symptoms. What is the primary mechanism responsible for the pain and swelling in Lipoma Arborescens?
View Answer & Explanation
Correct Answer: B
Rationale: The primary mechanism for symptoms in Lipoma Arborescens is mechanical irritation and chronic inflammation caused by the hypertrophied, villous synovial tissue within the joint. This leads to recurrent effusions, pain, stiffness, and sometimes mechanical symptoms like catching. It is not due to nerve compression (A), ischemic necrosis (C), malignant transformation (D - it's benign), or autoimmune destruction (E - not an autoimmune disease).
Question 62
A 57-year-old female presents with a 1-year history of left knee swelling and discomfort. She reports no specific trauma. Physical examination reveals a moderate effusion and mild tenderness. An MRI is performed. The radiologist notes diffuse synovial proliferation with high signal intensity on T1 and T2-weighted images, which completely suppresses on fat-saturated sequences. This finding is crucial for diagnosis. What is the primary purpose of using fat-saturated sequences in the MRI evaluation of suspected Lipoma Arborescens?
View Answer & Explanation
Correct Answer: C
Rationale: The primary purpose of fat-saturated sequences (e.g., STIR or fat-suppressed T2) in the MRI evaluation of Lipoma Arborescens is to confirm the presence of fat within the synovial proliferation. Fat signal will be high on T1 and T2, but will completely suppress on fat-saturated sequences, which is a pathognomonic feature distinguishing it from other synovial lesions. Hemosiderin (A) would be low signal on all sequences. Cartilage defects (B) are better seen on specific cartilage sequences. Bone marrow edema (D) is evaluated on T2 fat-saturated sequences, but the focus here is the synovium. Vascularity (E) is assessed with contrast enhancement.
Question 63
A 61-year-old male presents with a 2-year history of intermittent right knee swelling and a dull ache. He has tried NSAIDs and activity modification without significant relief. Physical examination reveals a moderate effusion and a slightly doughy feel to the suprapatellar pouch. An MRI confirms Lipoma Arborescens. Considering the natural history of this condition, which of the following statements is most accurate?
Correct Answer: C
Rationale: Lipoma Arborescens is a benign, slowly progressive condition characterized by chronic synovial hypertrophy. It typically does not resolve spontaneously (A) and often requires surgical intervention for definitive relief of symptoms. It is not rapidly progressive or destructive (B), nor does it undergo malignant transformation (D). It is not a self-limiting inflammatory process (E), but rather a reactive or idiopathic synovial proliferation.
Question 64
A 45-year-old male presents with chronic, non-traumatic swelling of his right elbow for 1 year. He experiences occasional stiffness and a feeling of fullness. Physical examination reveals a moderate elbow effusion. Plain radiographs are unremarkable. An MRI shows diffuse, frond-like synovial proliferation within the joint, with signal intensity identical to subcutaneous fat on all sequences. What is the most appropriate initial management strategy for this patient?
View Answer & Explanation
Correct Answer: C
Rationale: Given the definitive MRI diagnosis of Lipoma Arborescens and the patient's chronic symptoms, arthroscopic synovectomy is the most appropriate initial management strategy. While observation (A) or injections (B) might be considered for very mild or asymptomatic cases, or as temporary measures, they are generally ineffective in providing long-term relief for symptomatic Lipoma Arborescens. Systemic immunosuppressive therapy (D) is not indicated for this benign, non-inflammatory condition. Aspiration (E) might provide temporary relief but does not address the underlying synovial proliferation.
Question 65
A 68-year-old female undergoes arthroscopic synovectomy for Lipoma Arborescens in her knee. The procedure is successful, with complete removal of the hypertrophied synovial tissue. What is the most important aspect of post-operative rehabilitation following this procedure?
View Answer & Explanation
Correct Answer: B
Rationale: Following arthroscopic synovectomy for Lipoma Arborescens, early range of motion and strengthening exercises are crucial to prevent stiffness, restore joint function, and facilitate recovery. Strict immobilization (A) is generally avoided as it can lead to arthrofibrosis. Long-term anti-inflammatory medications (C) or steroid injections (D) are not typically needed after successful surgical removal. Weight-bearing restrictions (E) are usually not necessary unless there are concomitant procedures or specific cartilage concerns.
Question 66
A 50-year-old male presents with a 2-year history of chronic, non-traumatic left knee swelling and pain. Physical examination reveals a large, soft effusion. MRI confirms Lipoma Arborescens, showing extensive involvement of the entire synovial lining, including the posterior compartments and difficult-to-access areas. Given the extent of the disease, which surgical approach might be considered if arthroscopic synovectomy is deemed insufficient?
View Answer & Explanation
Correct Answer: B
Rationale: While arthroscopic synovectomy is the preferred approach for Lipoma Arborescens, in cases of very extensive disease involving difficult-to-access areas or when complete arthroscopic resection is not feasible, an open synovectomy may be considered to ensure complete removal of the hypertrophied synovium. Diagnostic arthroscopy
Question 66
A 55-year-old male presents with chronic knee swelling and pain. Physical examination reveals a boggy effusion. MRI reveals villous, frond-like synovial proliferation with fat signal intensity in the suprapatellar pouch.
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is characterized by villous lipomatous proliferation of the synovium, which appears as fat signal intensity on MRI (hyperintense on T1 and T2, suppressed on fat-saturated sequences). PVNS typically shows hemosiderin deposition (low signal on T1 and T2, blooming on gradient echo). Synovial chondromatosis involves cartilaginous or osteocartilaginous loose bodies. Rheumatoid arthritis is an inflammatory synovitis with pannus formation, and septic arthritis involves purulent effusion and synovial inflammation.
Question 66
A 62-year-old female complains of recurrent knee effusions and a "boggy" feeling in her knee for several years. Physical exam shows a moderate effusion with full range of motion. Radiographs show mild degenerative changes.
View Answer & Explanation
Correct Answer: E
Rationale: The knee joint, particularly the suprapatellar pouch, is by far the most common location for lipoma arborescens. While it can occur in other joints, the vast majority of cases are reported in the knee. The other joints listed are less commonly affected.
Question 66
A 48-year-old male presents with a 2-year history of progressive knee pain and swelling. Physical exam reveals a palpable, soft, non-tender mass in the suprapatellar region. MRI images demonstrate a frond-like synovial proliferation that is hyperintense on T1-weighted images and completely suppresses on fat-saturated sequences.
View Answer & Explanation
Correct Answer: C
Rationale: The MRI findings of a frond-like synovial proliferation that is hyperintense on T1-weighted images and completely suppresses on fat-saturated sequences are pathognomonic for lipoma arborescens, indicating the presence of mature fat within the synovium. PVNS would show low signal intensity on T1 and T2 due to hemosiderin. Synovial chondromatosis would show cartilaginous or ossified nodules. Synovial hemangioma would show vascular characteristics, and rheumatoid arthritis would show inflammatory pannus without fat signal suppression.
Question 66
A 58-year-old female presents with a 3-year history of intermittent, painless knee swelling and a feeling of "fullness." Physical exam shows a moderate effusion and a soft, doughy feel to the joint. She denies any locking or instability. Radiographs show no acute findings.
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens typically presents with chronic, often painless, joint swelling and effusion. The fatty proliferation can lead to a "boggy" or "doughy" feel on examination. Acute severe pain, rapidly progressive joint destruction, and systemic inflammatory symptoms are not characteristic of this benign condition. While mechanical symptoms like locking can occur, chronic painless effusion is more common.
Question 66
A 68-year-old male with a long history of osteoarthritis in his right knee develops persistent knee swelling and a "squishy" feeling. Physical exam reveals crepitus and limited range of motion. MRI confirms lipoma arborescens.
View Answer & Explanation
Correct Answer: D
Rationale: Lipoma arborescens is frequently associated with underlying degenerative joint disease, particularly osteoarthritis. It is often considered a reactive process secondary to chronic irritation or inflammation within the joint. While it can occur in isolation, its association with osteoarthritis is well-documented. The other conditions listed are less commonly associated.
Question 66
A 52-year-old patient is diagnosed with lipoma arborescens of the knee after MRI. Conservative management with NSAIDs and aspiration has failed to provide lasting relief from swelling and discomfort. Physical exam shows persistent effusion and mild tenderness.
View Answer & Explanation
Correct Answer: D
Rationale: For symptomatic lipoma arborescens that fails conservative management, synovectomy (either arthroscopic or open) is the definitive treatment. This involves surgical removal of the proliferative synovial tissue. Arthroscopic debridement is too general; synovectomy specifically targets the diseased synovium. Total knee arthroplasty is reserved for end-stage arthritis, not primarily for lipoma arborescens. Corticosteroid injections and physical therapy are conservative measures that have already failed.
Question 66
A 35-year-old male presents with recurrent knee swelling and pain. Physical exam reveals a diffuse, boggy synovitis. MRI shows synovial proliferation. The radiologist notes that the signal characteristics are crucial to differentiate between two common conditions: lipoma arborescens and pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: D
Rationale: The key differentiating feature on MRI between lipoma arborescens and PVNS is the signal intensity on fat-suppressed sequences. Lipoma arborescens, being composed of fat, will show complete signal suppression on fat-saturated sequences. PVNS, due to hemosiderin deposition, will not suppress and often demonstrates low signal intensity on T1 and T2, with characteristic "blooming" on gradient echo sequences. While both can have joint effusions and be located in the suprapatellar pouch, and PVNS can cause bone erosions, the fat suppression is the most specific differentiator.
Question 66
A 60-year-old female undergoes arthroscopic synovectomy for chronic knee swelling. Physical exam prior to surgery showed a large, soft effusion. Histopathological examination of the resected tissue is performed.
View Answer & Explanation
Correct Answer: C
Rationale: The characteristic histopathological finding in lipoma arborescens is the villous proliferation of mature adipocytes (fat cells) within the synovial membrane. This fatty infiltration gives the synovium its characteristic frond-like appearance. Hemosiderin deposition is characteristic of PVNS. Chondroid metaplasia is seen in synovial chondromatosis. Granulomatous inflammation is associated with conditions like tuberculosis or sarcoidosis, and necrotic debris is non-specific.
Question 66
A 50-year-old patient underwent a complete arthroscopic synovectomy for lipoma arborescens of the knee due to persistent pain and swelling. The surgeon reported complete removal of the affected synovium. The patient is now asking about the likelihood of the condition returning.
View Answer & Explanation
Correct Answer: C
Rationale: The recurrence rate after a complete synovectomy for lipoma arborescens is generally very low, typically less than 10%. This is because it is a benign condition, and complete surgical excision of the affected synovium is usually curative. Incomplete resection, however, may lead to persistent symptoms or recurrence.
Question 66
A 59-year-old male presents with chronic knee pain and swelling. Physical exam reveals a large, soft effusion. Initial radiographs are obtained to evaluate for underlying bony pathology.
View Answer & Explanation
Correct Answer: D
Rationale: Plain radiographs in patients with lipoma arborescens are often normal or show only non-specific findings such as soft tissue swelling or joint effusion. If associated with osteoarthritis, signs of degenerative changes may be present. Extensive calcification or multiple loose bodies are characteristic of synovial chondromatosis. Significant joint space narrowing and subchondral sclerosis are signs of advanced osteoarthritis, which may coexist but are not direct findings of lipoma arborescens itself. Periosteal reaction is not typical.
Question 66
A patient is diagnosed with lipoma arborescens of the knee after presenting with chronic, unexplained knee swelling. The physician is counseling the patient on the typical demographic profile of this condition.
View Answer & Explanation
Correct Answer: D
Rationale: Lipoma arborescens typically affects individuals in the middle-aged to elderly population, often coinciding with the prevalence of degenerative joint conditions like osteoarthritis. While rare cases have been reported in younger individuals, it is not common in pediatric, adolescent, or young adult populations.
Question 66
A 45-year-old male with no history of trauma or inflammatory conditions develops lipoma arborescens in his knee, confirmed by MRI. The pathology is being discussed in terms of its underlying nature.
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is generally considered a reactive or degenerative process, often associated with chronic irritation, trauma, or underlying osteoarthritis. While it involves a proliferation of fat cells, it is not considered a true neoplasm in the sense of a tumor, but rather a hyperplastic response of the synovium. It is benign and does not metastasize. It is not infectious or autoimmune in nature.
Question 66
A 60-year-old female with mild symptoms from lipoma arborescens of the knee, confirmed by MRI, prefers to avoid surgery if possible. Physical exam shows a small to moderate effusion and mild discomfort with activity.
View Answer & Explanation
Correct Answer: C
Rationale: For patients with mild symptoms or those who wish to avoid surgery, conservative management options include NSAIDs, physical therapy, and joint aspiration. Joint aspiration can provide temporary symptomatic relief by reducing the volume of the effusion. The other options are inappropriate for this benign condition: chemotherapy and radiation are for malignancy, antibiotics for infection, and total joint replacement for end-stage arthritis.
Question 66
A 55-year-old male presents with chronic knee swelling. Physical exam reveals a palpable mass. MRI reveals a characteristic villous fatty proliferation predominantly located in the suprapatellar pouch.
View Answer & Explanation
Correct Answer: C
Rationale: The suprapatellar pouch is the most common site for lipoma arborescens due to its relatively large synovial surface area, which provides ample space for the villous fatty proliferation to develop and expand. While other factors might play a minor role, the extensive synovial lining is the primary reason for its predilection for this location. Its communication with the popliteal fossa (Baker's cyst) is a separate issue, and its proximity to menisci or role in patellar tracking are not directly related to the pathology's location preference.
Question 66
A 63-year-old female presents with chronic knee pain and swelling. Physical exam shows a moderate effusion. MRI is performed to evaluate the cause of the symptoms.
View Answer & Explanation
Correct Answer: C
Rationale: On T1-weighted MRI sequences, lipoma arborescens typically appears hyperintense. This is due to the high fat content within the proliferating synovial villi. Fat is inherently bright on T1-weighted images. Hypointense signals are usually associated with fluid, fibrous tissue, or hemosiderin. Isointense signals are similar to surrounding tissues, and signal voids are seen with cortical bone or rapidly flowing blood.
Question 66
A 40-year-old male presents with knee pain, swelling, and occasional mechanical symptoms. Physical exam reveals crepitus and a palpable effusion. MRI shows synovial proliferation. The radiologist is considering lipoma arborescens versus synovial chondromatosis.
View Answer & Explanation
Correct Answer: C
Rationale: The key differentiating feature on MRI between lipoma arborescens and synovial chondromatosis is the signal intensity of the synovial proliferation. Lipoma arborescens shows fat signal (hyperintense on T1, suppressed on fat-sat). Synovial chondromatosis, on the other hand, involves cartilaginous or osteocartilaginous nodules, which typically appear intermediate to low signal on T1 and high signal on T2, often with calcifications visible on plain radiographs or CT. Both can cause effusion and mechanical symptoms.
Question 66
A 70-year-old patient with long-standing, untreated lipoma arborescens in the knee presents with worsening pain and limited range of motion. Physical exam shows significant crepitus and a fixed flexion deformity.
View Answer & Explanation
Correct Answer: C
Rationale: While lipoma arborescens is benign, chronic untreated cases can lead to progressive articular cartilage damage. The persistent effusion,
Question 67
A 55-year-old male presents with chronic knee swelling and pain. Physical examination reveals a boggy effusion. MRI reveals villous, frond-like synovial proliferation with fat signal intensity in the suprapatellar pouch.
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is characterized by villous lipomatous proliferation of the synovium, which appears as fat signal intensity on MRI (hyperintense on T1 and T2, suppressed on fat-saturated sequences). PVNS typically shows hemosiderin deposition (low signal on T1 and T2, blooming on gradient echo). Synovial chondromatosis involves cartilaginous or osteocartilaginous loose bodies. Rheumatoid arthritis is an inflammatory synovitis with pannus formation, and septic arthritis involves purulent effusion and synovial inflammation.
Question 68
A 62-year-old female complains of recurrent knee effusions and a "boggy" feeling in her knee for several years. Physical exam shows a moderate effusion with full range of motion. Radiographs show mild degenerative changes.
View Answer & Explanation
Correct Answer: E
Rationale: The knee joint, particularly the suprapatellar pouch, is by far the most common location for lipoma arborescens. While it can occur in other joints, the vast majority of cases are reported in the knee. The other joints listed are less commonly affected.
Question 69
A 48-year-old male presents with a 2-year history of progressive knee pain and swelling. Physical exam reveals a palpable, soft, non-tender mass in the suprapatellar region. MRI images demonstrate a frond-like synovial proliferation that is hyperintense on T1-weighted images and completely suppresses on fat-saturated sequences.
View Answer & Explanation
Correct Answer: C
Rationale: The MRI findings of a frond-like synovial proliferation that is hyperintense on T1-weighted images and completely suppresses on fat-saturated sequences are pathognomonic for lipoma arborescens, indicating the presence of mature fat within the synovium. PVNS would show low signal intensity on T1 and T2 due to hemosiderin. Synovial chondromatosis would show cartilaginous or ossified nodules. Synovial hemangioma would show vascular characteristics, and rheumatoid arthritis would show inflammatory pannus without fat signal suppression.
Question 70
A 58-year-old female presents with a 3-year history of intermittent, painless knee swelling and a feeling of "fullness." Physical exam shows a moderate effusion and a soft, doughy feel to the joint. She denies any locking or instability. Radiographs show no acute findings.
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens typically presents with chronic, often painless, joint swelling and effusion. The fatty proliferation can lead to a "boggy" or "doughy" feel on examination. Acute severe pain, rapidly progressive joint destruction, and systemic inflammatory symptoms are not characteristic of this benign condition. While mechanical symptoms like locking can occur, chronic painless effusion is more common.
Question 71
A 68-year-old male with a long history of osteoarthritis in his right knee develops persistent knee swelling and a "squishy" feeling. Physical exam reveals crepitus and limited range of motion. MRI confirms lipoma arborescens.
View Answer & Explanation
Correct Answer: D
Rationale: Lipoma arborescens is frequently associated with underlying degenerative joint disease, particularly osteoarthritis. It is often considered a reactive process secondary to chronic irritation or inflammation within the joint. While it can occur in isolation, its association with osteoarthritis is well-documented. The other conditions listed are less commonly associated.
Question 72
A 52-year-old patient is diagnosed with lipoma arborescens of the knee after MRI. Conservative management with NSAIDs and aspiration has failed to provide lasting relief from swelling and discomfort. Physical exam shows persistent effusion and mild tenderness.
View Answer & Explanation
Correct Answer: D
Rationale: For symptomatic lipoma arborescens that fails conservative management, synovectomy (either arthroscopic or open) is the definitive treatment. This involves surgical removal of the proliferative synovial tissue. Arthroscopic debridement is too general; synovectomy specifically targets the diseased synovium. Total knee arthroplasty is reserved for end-stage arthritis, not primarily for lipoma arborescens. Corticosteroid injections and physical therapy are conservative measures that have already failed.
Question 73
A 35-year-old male presents with recurrent knee swelling and pain. Physical exam reveals a diffuse, boggy synovitis. MRI shows synovial proliferation. The radiologist notes that the signal characteristics are crucial to differentiate between two common conditions: lipoma arborescens and pigmented villonodular synovitis (PVNS).
View Answer & Explanation
Correct Answer: D
Rationale: The key differentiating feature on MRI between lipoma arborescens and PVNS is the signal intensity on fat-suppressed sequences. Lipoma arborescens, being composed of fat, will show complete signal suppression on fat-saturated sequences. PVNS, due to hemosiderin deposition, will not suppress and often demonstrates low signal intensity on T1 and T2, with characteristic "blooming" on gradient echo sequences. While both can have joint effusions and be located in the suprapatellar pouch, and PVNS can cause bone erosions, the fat suppression is the most specific differentiator.
Question 74
A 60-year-old female undergoes arthroscopic synovectomy for chronic knee swelling. Physical exam prior to surgery showed a large, soft effusion. Histopathological examination of the resected tissue is performed.
View Answer & Explanation
Correct Answer: C
Rationale: The characteristic histopathological finding in lipoma arborescens is the villous proliferation of mature adipocytes (fat cells) within the synovial membrane. This fatty infiltration gives the synovium its characteristic frond-like appearance. Hemosiderin deposition is characteristic of PVNS. Chondroid metaplasia is seen in synovial chondromatosis. Granulomatous inflammation is associated with conditions like tuberculosis or sarcoidosis, and necrotic debris is non-specific.
Question 75
A 50-year-old patient underwent a complete arthroscopic synovectomy for lipoma arborescens of the knee due to persistent pain and swelling. The surgeon reported complete removal of the affected synovium. The patient is now asking about the likelihood of the condition returning.
View Answer & Explanation
Correct Answer: C
Rationale: The recurrence rate after a complete synovectomy for lipoma arborescens is generally very low, typically less than 10%. This is because it is a benign condition, and complete surgical excision of the affected synovium is usually curative. Incomplete resection, however, may lead to persistent symptoms or recurrence.
Question 76
A 59-year-old male presents with chronic knee pain and swelling. Physical exam reveals a large, soft effusion. Initial radiographs are obtained to evaluate for underlying bony pathology.
View Answer & Explanation
Correct Answer: D
Rationale: Plain radiographs in patients with lipoma arborescens are often normal or show only non-specific findings such as soft tissue swelling or joint effusion. If associated with osteoarthritis, signs of degenerative changes may be present. Extensive calcification or multiple loose bodies are characteristic of synovial chondromatosis. Significant joint space narrowing and subchondral sclerosis are signs of advanced osteoarthritis, which may coexist but are not direct findings of lipoma arborescens itself. Periosteal reaction is not typical.
Question 77
A patient is diagnosed with lipoma arborescens of the knee after presenting with chronic, unexplained knee swelling. The physician is counseling the patient on the typical demographic profile of this condition.
View Answer & Explanation
Correct Answer: D
Rationale: Lipoma arborescens typically affects individuals in the middle-aged to elderly population, often coinciding with the prevalence of degenerative joint conditions like osteoarthritis. While rare cases have been reported in younger individuals, it is not common in pediatric, adolescent, or young adult populations.
Question 78
A 45-year-old male with no history of trauma or inflammatory conditions develops lipoma arborescens in his knee, confirmed by MRI. The pathology is being discussed in terms of its underlying nature.
View Answer & Explanation
Correct Answer: C
Rationale: Lipoma arborescens is generally considered a reactive or degenerative process, often associated with chronic irritation, trauma, or underlying osteoarthritis. While it involves a proliferation of fat cells, it is not considered a true neoplasm in the sense of a tumor, but rather a hyperplastic response of the synovium. It is benign and does not metastasize. It is not infectious or autoimmune in nature.
Question 79
A 60-year-old female with mild symptoms from lipoma arborescens of the knee, confirmed by MRI, prefers to avoid surgery if possible. Physical exam shows a small to moderate effusion and mild discomfort with activity.
View Answer & Explanation
Correct Answer: C
Rationale: For patients with mild symptoms or those who wish to avoid surgery, conservative management options include NSAIDs, physical therapy, and joint aspiration. Joint aspiration can provide temporary symptomatic relief by reducing the volume of the effusion. The other options are inappropriate for this benign condition: chemotherapy and radiation are for malignancy, antibiotics for infection, and total joint replacement for end-stage arthritis.
Question 80
A 55-year-old male presents with chronic knee swelling. Physical exam reveals a palpable mass. MRI reveals a characteristic villous fatty proliferation predominantly located in the suprapatellar pouch.
View Answer & Explanation
Correct Answer: C
Rationale: The suprapatellar pouch is the most common site for lipoma arborescens due to its relatively large synovial surface area, which provides ample space for the villous fatty proliferation to develop and expand. While other factors might play a minor role, the extensive synovial lining is the primary reason for its predilection for this location. Its communication with the popliteal fossa (Baker's cyst) is a separate issue, and its proximity to menisci or role in patellar tracking are not directly related to the pathology's location preference.
Question 81
A 63-year-old female presents with chronic knee pain and swelling. Physical exam shows a moderate effusion. MRI is performed to evaluate the cause of the symptoms.
View Answer & Explanation
Correct Answer: C
Rationale: On T1-weighted MRI sequences, lipoma arborescens typically appears hyperintense. This is due to the high fat content within the proliferating synovial villi. Fat is inherently bright on T1-weighted images. Hypointense signals are usually associated with fluid, fibrous tissue, or hemosiderin. Isointense signals are similar to surrounding tissues, and signal voids are seen with cortical bone or rapidly flowing blood.
Question 82
A 40-year-old male presents with knee pain, swelling, and occasional mechanical symptoms. Physical exam reveals crepitus and a palpable effusion. MRI shows synovial proliferation. The radiologist is considering lipoma arborescens versus synovial chondromatosis.
View Answer & Explanation
Correct Answer: C
Rationale: The key differentiating feature on MRI between lipoma arborescens and synovial chondromatosis is the signal intensity of the synovial proliferation. Lipoma arborescens shows fat signal (hyperintense on T1, suppressed on fat-sat). Synovial chondromatosis, on the other hand, involves cartilaginous or osteocartilaginous nodules, which typically appear intermediate to low signal on T1 and high signal on T2, often with calcifications visible on plain radiographs or CT. Both can cause effusion and mechanical symptoms.
Question 83
A 55-year-old male presents with a firm, non-tender mass on his posterior thigh that he noticed approximately 6 months ago. He reports no pain or functional limitations, but states the mass has slowly increased in size. Physical examination reveals a palpable, firm, immobile mass deep to the fascia. Plain radiographs of the thigh are unremarkable, showing only soft tissue fullness.
View Answer & Explanation
Correct Answer: C
Rationale: Soft tissue sarcomas are uncommon soft tissue malignancies that most often occur in adults. The clinical presentation described is classic for a soft tissue sarcoma. Option A is incorrect because while lipomas are common, a firm, deep, growing mass in an adult warrants suspicion for sarcoma. Option B is incorrect as sarcomas are primarily adult diseases. Option D is incorrect as these lesions are usually asymptomatic. Option E is incorrect as while some may change size over a short time, "several months" is a more typical duration, and rapid growth over days is less common.
Question 84
A 62-year-old female presents with a palpable, firm mass in her proximal forearm. She reports noticing the mass about 4 months ago, and it has slowly enlarged. She denies pain, numbness, or weakness. On examination, the mass is firm, non-tender, and appears to be located subcutaneously, but abuts the myofascial plane. Plain radiographs are negative for osseous involvement.
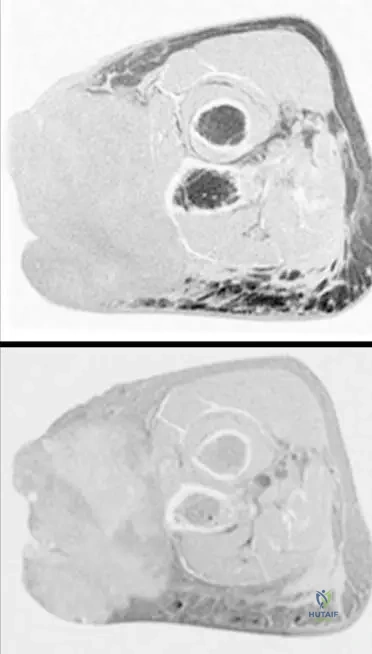
View Answer & Explanation
Correct Answer: B
Rationale: While most soft tissue sarcomas occur in a deep, subfascial location, approximately one in three soft tissue sarcomas occurs in the subcutaneous tissues. Therefore, a subcutaneous location does not rule out malignancy. Option A is incorrect as deep locations are more common. Option C is incorrect as subcutaneous lesions do occur. Option D is incorrect as subcutaneous location does not preclude malignancy. Option E is incorrect as soft tissue sarcomas are usually asymptomatic.
Question 85
A 48-year-old male presents with a slowly growing, firm mass on the lateral aspect of his leg. He has noticed it for about 5 months. He denies any pain or other symptoms. Physical examination reveals a 4 cm, firm, non-tender mass that is mobile over the deep fascia but fixed to the subcutaneous tissue. Plain radiographs are normal.
View Answer & Explanation
Correct Answer: C
Rationale: Patients will note a firm mass that usually has been present for several months. Occasionally, patients will note a change in size over a fairly short time. Lesions are usually asymptomatic. Option A is incorrect as lesions are usually asymptomatic. Option B is incorrect as they are typically present for several months. Option D is incorrect as they are described as firm. Option E is incorrect as systemic symptoms are not typically associated with the initial presentation of soft tissue sarcomas.
Question 86
A 70-year-old female presents with a 7 cm, firm, non-tender mass in her gluteal region. She reports it has been present for approximately 9 months and has slowly increased in size. She denies any pain, numbness, or weakness. Plain radiographs show a non-specific soft tissue fullness. An MRI is ordered.
View Answer & Explanation
Correct Answer: C
Rationale: Many soft tissue sarcomas have non-specific signal characteristics on MRI, with low to intermediate signal intensity on T1, heterogeneous primarily high signal intensity on T2, and variable enhancement with gadolinium. Option B is incorrect because heterogeneity is a key feature, especially in larger lesions. Options A and D are incorrect as T2 is typically high signal and T1 is low to intermediate. Option E is incorrect as variable enhancement is typical.
Question 87
A 58-year-old male presents with a 6 cm, firm, non-tender mass in his posterior calf. He has noticed it for about 7 months. He denies any pain or other symptoms. Physical examination reveals a palpable, firm mass deep to the gastrocnemius fascia. Plain radiographs are normal. An MRI is performed.
View Answer & Explanation
Correct Answer: B
Rationale: Most soft tissue sarcomas have non-specific signal characteristics on MRI, with low to intermediate signal intensity on T1, often described as isointense with muscle. Option A is incorrect as T1 signal is typically not high. Option C is incorrect as there is signal. Option D is incorrect as heterogeneity is more characteristic of T2 images and post-gadolinium T1 images. Option E is incorrect as they are solid masses.
Question 88
A 65-year-old female presents with a 5 cm, firm, non-tender mass near her elbow that has been slowly growing over the past 8 months. On examination, the mass is fungating through the skin. Plain radiographs are unremarkable. An MRI is performed.

View Answer & Explanation
Correct Answer: C
Rationale: The image (Fig. 9.14) shows a subcutaneous soft tissue sarcoma fungating through the skin. This is an aggressive presentation of a malignancy, not a benign process. Option A and B are incorrect as fungating lesions are highly suspicious for malignancy. Option D is incorrect as sarcomas can occur in any location. Option E is incorrect as the lesion is described as a soft tissue mass.
Question 89
A 50-year-old male presents with a 4 cm, firm, non-tender mass in his proximal forearm. He reports it has been present for several months. Physical examination reveals a palpable mass that appears to be predominantly in the subcutaneous tissues, but abuts the adjacent myofascial plane. Plain radiographs are normal. An MRI is performed, as shown.
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 9.15 b, an axial T2-weighted image with gadolinium and fat saturation, shows a heterogeneous soft tissue sarcoma with predominantly high signal intensity. The image also confirms its location predominantly in the subcutaneous tissues abutting the adjacent myofascial plane. Option A is incorrect as the lesion is heterogeneous and high signal on T2. Option C is incorrect as it's a solid mass. Option D is incorrect as it's predominantly subcutaneous. Option E is incorrect as calcification is not mentioned or typically seen as a primary feature.
Question 90
A 60-year-old female presents with a 7 cm, firm, non-tender mass in her distal thigh. She reports it has been present for approximately 6 months and has slowly increased in size. She denies any pain or other symptoms. Plain radiographs show only soft tissue fullness. An MRI is performed, revealing typical features of a soft tissue sarcoma.
View Answer & Explanation
Correct Answer: C
Rationale: Most soft tissue sarcomas are isodense with the adjacent muscle on CT scans. Option A and B are incorrect as isodensity is characteristic. Option D is incorrect as extensive calcification is not a typical feature. Option E is incorrect as only specific types like liposarcoma might show fat density, but "most" sarcomas are isodense with muscle.
Question 91
A 52-year-old male presents with a 6 cm, firm, non-tender mass in his proximal forearm. He reports it has been present for several months. Physical examination reveals a palpable mass that appears to be predominantly in the subcutaneous tissues, but abuts the adjacent myofascial plane. Plain radiographs are normal. An MRI is performed, as shown.
View Answer & Explanation
Correct Answer: B
Rationale: Fig. 9.15 a, b shows axial T1 (a) and T2-weighted (b) images. Soft tissue sarcomas typically show low to intermediate signal intensity on T1-weighted images. Option A is incorrect. Option C is incorrect as T2 images typically show heterogeneous high signal. Option D is incorrect as variable enhancement with gadolinium is expected. Option E is incorrect as they are often infiltrative and may abut or involve adjacent structures.
Question 92
A 68-year-old male presents with a 9 cm, firm, non-tender mass in his posterior thigh. He reports it has been present for approximately 10 months and has slowly increased in size. He denies any pain or other symptoms. Plain radiographs show only soft tissue fullness. An MRI is performed, revealing a large, heterogeneous mass with variable enhancement.
View Answer & Explanation
Correct Answer: C
Rationale: Areas of necrosis and/or hemorrhage are common in large soft tissue sarcomas, contributing to their heterogeneous appearance and variable enhancement patterns on MRI. Option A is incorrect as calcification is not a primary cause of heterogeneity. Option B is incorrect as only liposarcomas would have significant fat. Option D is incorrect as sarcomas are solid masses. Option E is incorrect as the mass is growing, not resolving.
Question 93
A 59-year-old female presents with a 5 cm, firm, non-tender mass in her distal leg. She reports it has been present for several months. Physical examination reveals a palpable mass intimately associated with the fibula. Plain radiographs are normal. An MRI is performed, as shown.

View Answer & Explanation
Correct Answer: B
Rationale: Fig. 9.17 a, b (Proton density and T2 images) clearly demonstrates the heterogeneity of the lesion and its intimate association with the fibula. This intimate association is a concerning feature for potential involvement or origin. Option A is incorrect as the lesion is heterogeneous and associated with the fibula. Option C is incorrect as it's a solid soft tissue mass. Option D is incorrect as signal characteristics are distinct from normal muscle, especially on T2. Option E is incorrect as heterogeneity and intimate bone association are concerning for malignancy.
Question 94
A 63-year-old male undergoes resection of a 10 cm soft tissue mass from his proximal leg, which was intimately associated with the fibula. The pathology report confirms a liposarcoma. The resected specimen is shown.

View Answer & Explanation
Correct Answer: B
Rationale: Fig. 9.18 explicitly states "Resected proximal fibula with adjacent liposarcoma." This image demonstrates the surgical specimen, including the bone that was involved or intimately associated with the tumor. Option A is incorrect as it's a sarcoma, not a benign lipoma, and bone is involved. Option C is incorrect as it's a soft tissue sarcoma (liposarcoma) adjacent to the fibula, not a primary bone tumor. Option D is incorrect as the fibula is resected with the tumor. Option E is incorrect as the fibula was resected due to its intimate association, implying it was not easily separable.
Question 95
A 57-year-old female presents with a 8 cm, firm, non-tender mass in her deep thigh. She reports it has been present for approximately 7 months and has slowly increased in size. She denies any pain or other symptoms. Plain radiographs show only soft tissue fullness. An MRI is performed, as shown.
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 9.19 a, b shows typical MRI features of a soft tissue sarcoma with intermediate signal intensity on T1 (isointense with muscle) and markedly heterogeneous predominantly high signal intensity on T2. It also notes the tumor originates within the deep muscular compartment and delineates its relationship with neurovascular structures. Option A is incorrect as it originates in the deep muscular compartment. Option B is incorrect as T2 signal is high. Option D is incorrect as the MRI is used to delineate the relationship, implying potential proximity or involvement. Option E is incorrect as it's a sarcoma, not a pure lipoma.
Question 96
A 61-year-old male undergoes surgical resection of a large soft tissue sarcoma from his thigh. The gross specimen is shown. The lesion was noted to encompass the superficial femoral vascular bundle.
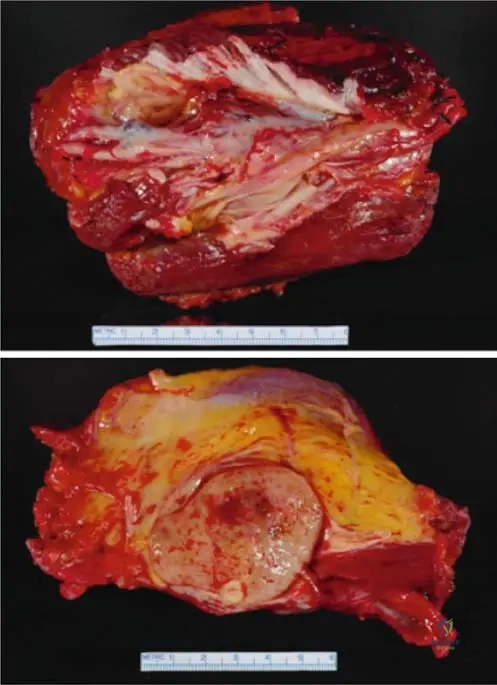
View Answer & Explanation
Correct Answer: C
Rationale: Fig. 9.20 a, b shows a gross specimen where the lesion encompassed the superficial femoral vascular bundle. This highlights the aggressive nature and potential for neurovascular involvement in soft tissue sarcomas. Option A is incorrect as it's a sarcoma. Option B is incorrect as it encompassed the vascular bundle. Option D is incorrect as encompassing neurovascular structures is evidence of local invasion. Option E is incorrect as such a lesion would require wide or radical excision, not intralesional.
Question 97
A 45-year-old female presents with a 3 cm, firm, non-tender mass in her anterior thigh. She reports it has been present for 3 months and has not changed significantly in size. Physical examination reveals a palpable, firm mass that is mobile within the subcutaneous tissue. Plain radiographs are normal. Given the clinical context of soft tissue sarcomas, what characteristic of this mass would be LEAST concerning for malignancy?
View Answer & Explanation
Correct Answer: E
Rationale: While none of these features definitively rule out malignancy, a mobile mass is generally less concerning than a fixed mass. Soft tissue sarcomas are typically firm (A), present for several months (B), and usually asymptomatic (C). Approximately one-third of sarcomas occur in the subcutaneous tissues (D), so this location alone does not make it less concerning. A fixed mass, especially to deep structures, is a more concerning sign for malignancy.
Question 98
A 72-year-old male presents with a 12 cm, firm, non-tender mass in his medial thigh. He reports it has been present for over a year and has slowly increased in size. He denies any pain or other symptoms. Plain radiographs show only soft tissue fullness. An MRI is performed, which shows a large, heterogeneous mass with areas of necrosis and hemorrhage.
View Answer & Explanation
Correct Answer: B
Rationale: Areas of necrosis and/or hemorrhage are common in large soft tissue sarcomas, contributing to their heterogeneous appearance on imaging. Option A is incorrect as these are features of aggressive malignancies. Option C is incorrect as while inflammation can cause necrosis, in the context of a growing mass, it points to malignancy. Option D is incorrect as primary sarcomas can exhibit these features. Option E is incorrect as the mass has been present for over a year and is growing, not resolving.
Question 99
A 60-year-old female presents with a 6 cm, firm, non-tender mass in her posterior calf. She reports it has been present for 8 months and has slowly increased in size. She denies any pain or other symptoms. Plain radiographs are normal. An MRI is performed, showing a lesion with low to intermediate signal on T1 and heterogeneous high signal on T2, with variable enhancement. Which of the following is a common histological type of soft tissue sarcoma?
View Answer & Explanation
Correct Answer: C
Rationale: The provided text lists "malignant fibrous histiocytoma (MFH), liposarcoma, etc." as examples of soft tissue sarcomas. Options A, B, D are benign soft tissue tumors. Option E, a desmoid tumor, is locally aggressive but generally considered intermediate rather than fully malignant in the same category as MFH or liposarcoma. MFH is a common type of high-grade sarcoma.
Question 100
A 50-year-old male presents with a 5 cm, firm, non-tender mass in his deep thigh. He reports it has been present for 6 months and has slowly increased in size. He denies any pain or other symptoms. Plain radiographs are normal. An MRI is performed, showing a lesion with intermediate signal intensity on T1 (isointense with muscle) and markedly heterogeneous predominantly high signal intensity on T2, with variable enhancement. The MRI also delineates the relationship between the mass and the adjacent neurovascular structures.
View Answer & Explanation
Correct Answer: C
Rationale: MRI is the imaging modality of choice for local staging of soft tissue sarcomas. It provides excellent soft tissue contrast, allowing for precise delineation of tumor size, depth (subcutaneous vs. deep/subfascial), and its relationship to critical neurovascular structures and bone, which is essential for surgical planning. Option A is incorrect as the features are concerning for malignancy. Option B is incorrect as CT chest/abdomen/pelvis is typically used for distant metastases. Option D is incorrect as MRI is highly
Question 100
A 58-year-old male presents to the clinic complaining of a firm mass in his posterior thigh. He states it has been present for approximately six months and has recently increased slightly in size. He denies any pain, numbness, or weakness associated with the mass.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that patients with soft tissue sarcomas will note a firm mass that usually has been present for several months and that lesions are usually asymptomatic. Severe pain, rapid onset, systemic symptoms, or neurological deficits are less common initial presentations. Main Distractor: B) Severe, localized pain. Soft tissue sarcomas are typically asymptomatic, making severe pain an unlikely initial presentation.
Question 100
A 45-year-old female presents with a palpable, firm, non-tender mass located just beneath the skin in her proximal forearm. She is concerned about its nature.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that "although most often these lesions will occur in a deep, subfascial location, approximately one in three soft tissue sarcomas occurs in the subcutaneous tissues." Main Distractor: C) Approximately one in two. While a significant proportion, the text specifically states "one in three" for subcutaneous locations, with the majority being deep.
Question 100
A 62-year-old male presents with a slowly enlarging, firm mass in his medial thigh. Plain radiographs of the thigh are obtained as part of the initial workup.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that "radiographs are frequently negative, but may show a masslike area of soft tissue fullness." Cortical destruction or periosteal reaction are more typical of primary bone tumors or aggressive infections. Main Distractor: B) Cortical destruction of the adjacent bone. While possible in advanced cases, plain radiographs are frequently negative for soft tissue sarcomas, and cortical destruction is not the most common initial finding.
Question 100
A 50-year-old female presents with a firm, deep-seated mass in her calf. An MRI is performed to further characterize the lesion. On T1-weighted images, the mass appears similar in signal intensity to the surrounding muscle.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that "Most soft tissue sarcomas are isodense with the adjacent muscle. Many soft tissue sarcomas have nonspecific signal characteristics on MRI, with low to intermediate signal intensity on T1." Main Distractor: B) Markedly high signal intensity, brighter than fat. This is incorrect; fat would be high signal on T1, and sarcomas are typically low to intermediate, isointense with muscle.
Question 100
A 68-year-old male presents with a large, firm mass in his proximal thigh. An MRI is performed, and on T2-weighted images, the lesion shows varying bright areas within it.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text describes MRI characteristics of soft tissue sarcomas as having "heterogeneous primarily high signal intensity on T2." Main Distractor: B) Homogeneous low signal intensity. This is incorrect; sarcomas typically show high signal on T2, and often with heterogeneity, not homogeneous low signal.
Question 100
A 55-year-old female undergoes an MRI with gadolinium for a suspected soft tissue sarcoma in her gluteal region. The radiologist notes that the mass shows areas of enhancement but it is not uniform throughout the lesion.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that soft tissue sarcomas exhibit "variable enhancement with gadolinium." Main Distractor: B) No enhancement with gadolinium. Malignant lesions typically enhance due to increased vascularity and capillary permeability, so no enhancement would be atypical for a sarcoma.
Question 100
A 70-year-old male presents with a rapidly growing, large mass in his popliteal fossa. MRI reveals a large, complex lesion with internal areas of fluid signal and signal voids.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical text states that "Areas of necrosis and/or hemorrhage are common in large lesions." These features contribute to the heterogeneous appearance on MRI. Main Distractor: B) Extensive calcification. While some sarcomas can calcify, the text specifically highlights necrosis and hemorrhage as common features in large lesions, which would correspond to fluid signal and signal voids.
Question 100
A 65-year-old patient presents with a mass near the elbow that has broken through the skin, appearing as an ulcerated, exophytic lesion.
View Answer & Explanation
Correct Answer: A
Rationale: Fig. 9.14 is described as "Subcutaneous soft tissue sarcoma fungating through the skin near the elbow." This directly matches the description of the image and the clinical presentation. Main Distractor: B) Deep intramuscular location with intact overlying skin. The image clearly shows a superficial lesion that has breached the skin, contradicting a deep intramuscular location with intact skin.
Question 100
A 52-year-old male presents with a firm mass in his proximal forearm. An MRI is performed to evaluate the extent and characteristics of the lesion.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.15 states: "Axial T1(a) and T2-weighted image with gadolinium and fat saturation (b) showing a heterogeneous soft tissue sarcoma in the proximal forearm that is predominantly in the subcutaneous tissues abutting the adjacent myofascial plane." Main Distractor: B) Entirely within the deep muscular compartment. The image context explicitly states the lesion is "predominantly in the subcutaneous tissues," which contradicts a purely deep muscular location.
Question 100
A 60-year-old female presents with a growing mass in her proximal forearm. MRI images are obtained to characterize the lesion.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.15 describes the lesion as a "heterogeneous soft tissue sarcoma." Heterogeneity is a common feature of sarcomas due to varying cellularity, necrosis, and hemorrhage. Main Distractor: B) Uniform signal intensity throughout the mass. This is incorrect, as the text explicitly describes the sarcoma in this image as "heterogeneous."
Question 100
A 48-year-old male presents with a firm mass in his lower leg. MRI is performed to assess the lesion's relationship to surrounding structures.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.17 states: "Proton density (a), T2 (b), images of the lesion. Note the heterogeneity and intimate association with the fibula." Main Distractor: B) Tibia. While the tibia is in the lower leg, the text specifically mentions the "intimate association with the fibula" for this particular image.
Question 100
A 59-year-old patient underwent surgical resection of a mass in the lower leg, which included a portion of the proximal fibula due to its close proximity to the tumor. The resected specimen is shown.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.18 explicitly states: "Resected proximal fibula with adjacent liposarcoma." Main Distractor: B) Malignant fibrous histiocytoma (MFH). While MFH is a type of soft tissue sarcoma mentioned in the general text, the specific image context identifies the tumor as a liposarcoma.
Question 100
A 63-year-old male presents with a deep-seated mass in his thigh. An MRI is performed to characterize the lesion. The axial T1-weighted image is shown.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.19 states: "Axial T1(a) and axial T2-weighted MRI with fat saturation (b) showing typical MRI features of a soft tissue sarcoma with intermediate signal intensity on T1 (isointense with muscle)." Main Distractor: B) Markedly high signal intensity, brighter than fat. This is incorrect; T1 signal for STS is typically intermediate, isointense with muscle, not markedly high like fat.
Question 100
A 63-year-old male presents with a deep-seated mass in his thigh. An MRI is performed to characterize the lesion. The axial T2-weighted MRI with fat saturation is shown.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.19 states: "Axial T1(a) and axial T2-weighted MRI with fat saturation (b) showing typical MRI features of a soft tissue sarcoma with intermediate signal intensity on T1 (isointense with muscle) and markedly heterogeneous predominantly high signal intensity on T2." Main Distractor: B) Homogeneous low signal intensity. This is incorrect; sarcomas typically show high signal on T2, and often with heterogeneity, not homogeneous low signal.
Question 100
A 63-year-old male presents with a deep-seated mass in his thigh. An MRI is performed to characterize the lesion and its anatomical origin.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical context for Fig. 9.19 states: "Note that the tumor originates within the deep muscular compartment of the thigh." Main Distractor: B) Subcutaneous compartment. While some sarcomas are subcutaneous, the text specifically states this particular tumor (Fig 9.19) originates in the "deep muscular compartment."
Question 100
A 72-year-old patient underwent surgical resection of a large soft tissue sarcoma in the thigh. The gross specimen is shown, demonstrating the extensive nature of the tumor.
<ul class="