Master ABOS Orthopedic Board Review: Skeletal Dysplasias, Bone Tumors, & Arthropathy | Part 13

Key Takeaway
Prepare for your ABOS Board Exam with this orthopedic review. It covers critical topics like skeletal dysplasias (achondroplasia, metaphyseal chondrodysplasia), osteoid osteoma, lipomas, stress fractures, hemophilic arthropathy, and CRPS. Master diagnosis and management for board success.
Question 1
A 60-year-old female develops severe pain, swelling, and limited range of motion in her left shoulder, hand, and wrist three months after sustaining a distal radius fracture that required immobilization. She describes her hand as feeling "burning" and appears to have skin atrophy and flexion contractures in her fingers. Which stage of Algodystrophy is most consistent with her current presentation?
View Answer & Explanation
Correct Answer: C
Rationale: The atrophic stage of Algodystrophy is characterized by pain extending proximally on the involved limb, atrophy of the skin, subcutaneous tissue, and general soft tissue, and flexion contractures of the joints. The "hand-shoulder syndrome" is also a known manifestation of upper limb involvement. The acute stage would typically present with warmth, redness, and marked swelling, while the dystrophic stage is transitional. The patient's symptoms of skin atrophy and contractures point to the later, atrophic stage.
Question 2
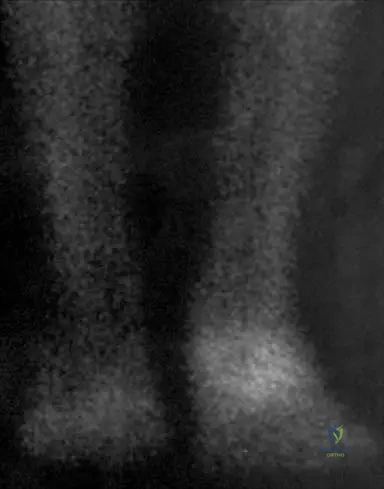
A 55-year-old male presents with a several-week history of severe, burning pain and swelling in his right foot following a minor ankle sprain. Physical examination reveals a warm, erythematous, and exquisitely tender foot. A bone scan is performed.
View Answer & Explanation
Correct Answer: C
Rationale: In the acute stage of Algodystrophy (RSD), a bone scan typically shows increased radioisotope uptake, particularly in the affected bones, such as the tarsal bones in a foot involvement. This reflects the increased metabolic activity and vascular changes occurring in the affected limb. The image (Fig. 4.18) explicitly demonstrates increased radioisotope uptake in the tarsal bones in the acute stage.
Question 3
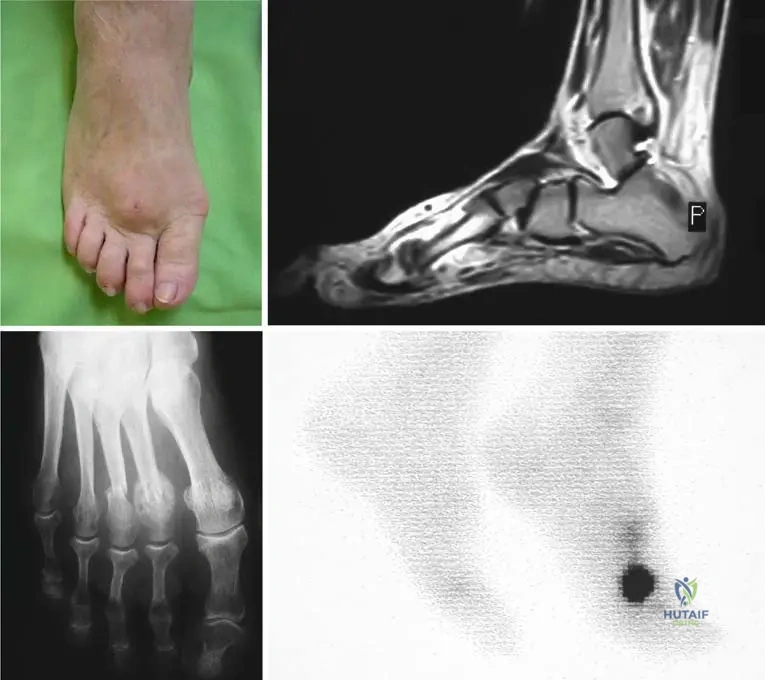
A 22-year-old female ballet dancer presents with insidious onset of forefoot pain that worsens with dancing and improves with rest. Physical examination reveals localized tenderness and mild swelling over the dorsum of her left foot. Radiographs are initially unremarkable, but a follow-up MRI is performed.

View Answer & Explanation
Correct Answer: A
Rationale: In the context of a stress fracture, especially in its early stages where radiographs may be normal, MRI is highly sensitive for detecting bone marrow edema and edema in the surrounding soft tissue, which are characteristic findings. The image (Fig. 5.1c) specifically shows edema in the surrounding soft tissue on an MR picture associated with a metatarsal stress fracture. The other options are less likely given the clinical presentation of a stress fracture.
Question 4
A 19-year-old male army recruit presents with progressive pain in his right shin that began after an increase in marching drills. The pain is worse with activity and relieved by rest. Physical examination reveals localized tenderness over the midshaft of the tibia. Radiographs are initially negative, but a follow-up radiograph two weeks later shows a faint hairline crack and early callus formation.
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of a young adult unaccustomed to sudden physical activity, with pain increasing with activity and decreasing at rest, localized tenderness, and radiographic evidence of a hairline crack and callus formation, is highly characteristic of a stress fracture. Shin splints typically do not show a fracture line or callus. Osteomyelitis would have systemic symptoms and different radiographic features. Ewings sarcoma is a malignant tumor with distinct imaging characteristics. Compartment syndrome presents with acute pain, paresthesias, and muscle tightness, often not relieved by rest.
Question 5
A 25-year-old male marathon runner complains of persistent pain in his left foot. He has been increasing his training intensity significantly. Physical examination reveals swelling above the second and third metatarsal heads. Radiographs show a new subcapital stress fracture in the third metatarsal bone and an old one in the second, surrounded by extensive callus formation.
View Answer & Explanation
Correct Answer: C
Rationale: The patient's history of repetitive stress (marathon runner), localized swelling and pain, and radiographic findings of a subcapital fracture with extensive callus formation are classic signs of a stress fracture. The image (Fig. 5.1b) clearly depicts these radiographic findings. Osteoid osteoma is a benign bone tumor with a characteristic nidus and sclerotic rim, not typically presenting with extensive callus from a fracture. Gout would involve inflammatory arthritis. Plantar fasciitis and Morton's neuroma are soft tissue conditions without bone fracture or callus formation.
Question 6
A 30-year-old female athlete presents with a swollen forefoot and pain that has progressively worsened over several weeks. She denies any specific acute injury but has recently increased her training regimen. CT imaging is performed.

View Answer & Explanation
Correct Answer: B
Rationale: In the context of a stress fracture, particularly in an athlete with repetitive stress, massive callus formation can occur around the diaphysis, sometimes mimicking a tumor on imaging. The CT image (Fig. 5.2c) reveals a fractured bone within such callus. Osteosarcoma would have different imaging characteristics and clinical course. Septic arthritis and Charcot arthropathy have distinct clinical presentations and imaging findings. Avascular necrosis would typically affect joint surfaces and not present with massive diaphyseal callus.
Question 7
A 7-year-old boy presents to the emergency department with acute, spontaneous swelling and severe pain in his right knee. His medical history is significant for an inherited bleeding disorder. Physical examination reveals a tense, warm, and tender knee joint with limited range of motion. There is no history of trauma.

View Answer & Explanation
Correct Answer: C
Rationale: The presentation of acute, spontaneous bleeding into a joint (hemarthrosis) in a patient with a known inherited bleeding disorder, especially without trauma, is highly indicative of severe hemophilia. The image (Fig. 6.1) shows acute spontaneous bleeding into the soft tissues and knee joint in a patient with severe hemophilia. Septic arthritis would typically present with fever and elevated inflammatory markers. Juvenile Idiopathic Arthritis has a more chronic course. Traumatic effusion would require a history of trauma. Osgood-Schlatter disease is an apophysitis of the tibial tubercle, not a joint effusion.
Question 8
A 3-year-old male is diagnosed with an inherited bleeding disorder. His blood clotting activity for Factor VIII is measured at 0.5% of normal. Based on this finding, how would his hemophilia be classified?
View Answer & Explanation
Correct Answer: C
Rationale: According to the provided text, severe hemophilia is classified as having less than 1% of clotting factor activity. A Factor VIII activity of 0.5% falls into this category. Mild hemophilia is 5-25%, and moderate is 2-5%. Von Willebrand's disease is a different clotting disorder, and acquired hemophilia is not inherited.
Question 9
A 10-year-old boy with severe hemophilia A experiences recurrent bleeding into his right ankle joint. This joint has become swollen, painful, and has a limited range of motion. What term is used to describe a joint that displays a tendency towards recurrent bleeding in hemophilia?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly states that "A joint that displays a tendency towards recurrent bleeding is termed a 'target joint.'" This term is crucial in the management and prognosis of hemophilic arthropathy. The image (Fig. 6.2) also refers to hemophilic arthropathy in a target joint.
Question 10
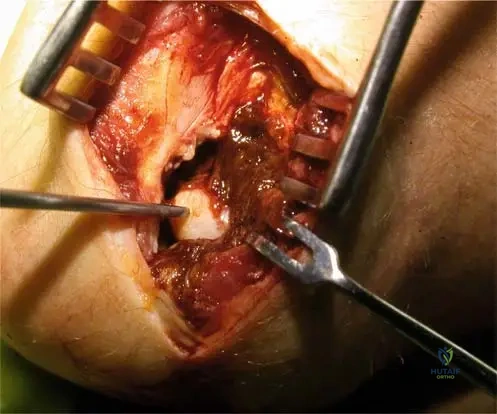
A 15-year-old male with a history of hemophilia presents with chronic pain and stiffness in his elbow. During arthroscopy, the synovium is noted to be hypertrophic and has a characteristic "mahogany brown" appearance.
View Answer & Explanation
Correct Answer: C
Rationale: The characteristic "mahogany brown" synovium seen in hemophilic arthropathy is due to hemosiderin deposition, which results from the breakdown of recurrent intra-articular blood. The image (Fig. 6.5) shows this characteristic appearance. Chronic infection would present differently. Gouty tophi are urate crystal deposits. Rheumatoid pannus is an inflammatory granulation tissue, but the specific color is due to hemosiderin in hemophilia. Amyloidosis is a systemic disorder with different synovial findings.
Question 11
A 20-year-old male with severe hemophilia has developed chronic hemophilic synovitis in his right knee. Which of the following is a primary mechanism leading to this chronic synovitis?
View Answer & Explanation
Correct Answer: C
Rationale: The text states, "When hemarthroses become frequent and/or intense, the synovium may not be able to reabsorb the blood. To compensate for such reabsorptive deficiency, the synovium will become hypertrophic, resulting in what is called chronic hemophilic synovitis." This is the direct mechanism described. The image (Fig. 6.6a) illustrates chronic hemophilic synovitis. The other options are not the primary mechanism for hemophilic synovitis.
Question 12
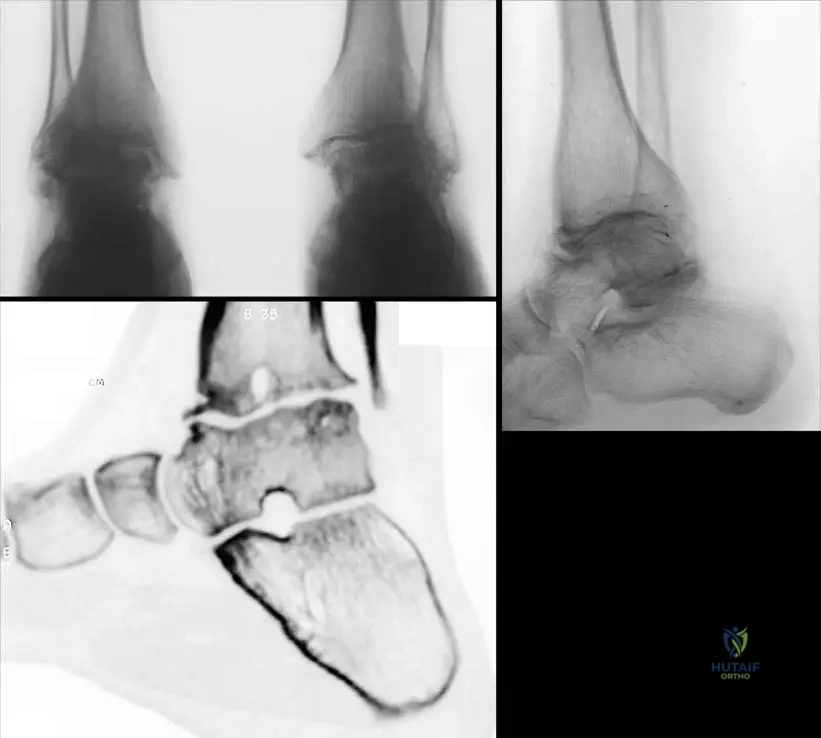
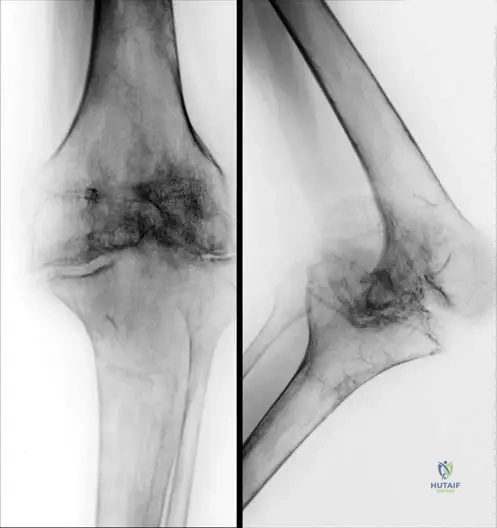
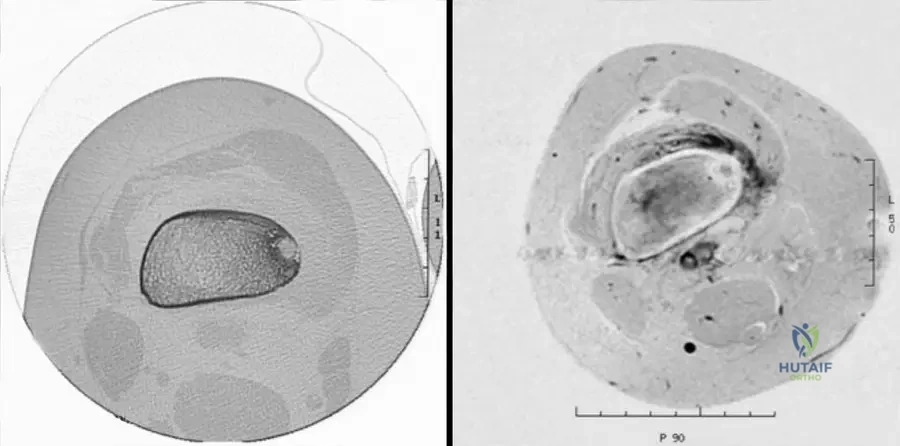
A 12-year-old boy with hemophilia presents with chronic ankle pain and swelling. Radiographs of his ankles are obtained.
View Answer & Explanation
Correct Answer: B
Rationale: Hemophilic arthritis, especially in young patients, is characterized by significant joint destruction. The text and image (Fig. 6.7c) describe and show "juxta-articular cysts, destroyed articular surfaces, and diffuse osteoporosis" as key features best evaluated on reconstructive CT pictures, which are also visible on plain radiographs (Fig. 6.7a, b). Joint space narrowing is an indirect sign of cartilage destruction. The other options describe features not typical of hemophilic arthropathy or are incorrect.
Question 13
An adult patient with long-standing severe hemophilia presents with significant functional limitations. Physical examination reveals fixed deformities of his knees and ankles. Which of the following is a common late-stage manifestation of hemophilic arthritis?
View Answer & Explanation
Correct Answer: B
Rationale: The text states that "Late stage of hemophilic arthritis in adult patients: axial deformities, secondary contractures of the knees, hips and equinus of the ankles are frequently seen." These contractures significantly compromise joint function and potential for joint replacement. The image (Fig. 6.8a, b) illustrates these late-stage contractures. Acute inflammatory synovitis is an earlier manifestation. Spontaneous fracture healing is unrelated. Joint pain typically persists, and hyperlaxity is not a feature; rather, contractures lead to stiffness.
Question 14
A 40-year-old male with hemophilia has chronic knee pain and stiffness. Radiographs show significant joint space narrowing, bony erosions, and subchondral cysts. What is the primary reason that recurrent joint bleeding in hemophilia leads to a "vicious cycle" of inflammation and further bleeding?
View Answer & Explanation
Correct Answer: B
Rationale: The text explicitly describes this vicious cycle: "If a joint bleeding is not adequately treated, it tends to recur. The inflamed, swollen synovium bleeds more easily than the normal synovium and causes further swelling and inflammation. This vicious cycle must be broken to prevent the development of arthritis." The image (Fig. 6.9a, b) shows radiological signs of knee arthritis in a hemophilic patient, emphasizing the need to break this cycle. The other options are incorrect mechanisms.
Question 15
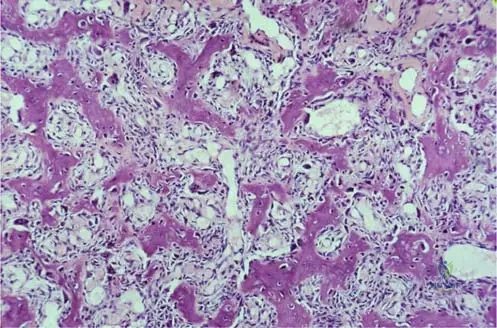
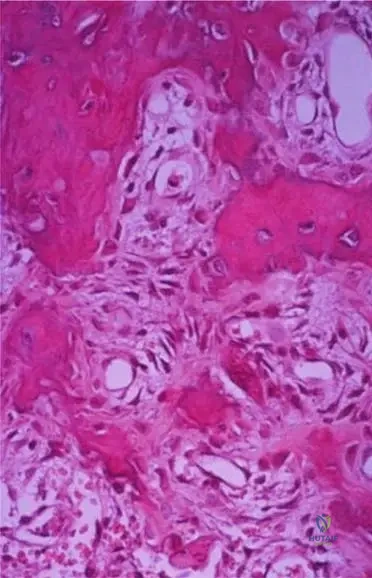
A young hemophilic male undergoes knee arthroscopy for chronic pain and limited motion. The surgeon notes destroyed cartilage surfaces and a pannus creeping over the joint surfaces. Histological examination of the synovium would most likely reveal:

View Answer & Explanation
Correct Answer: B
Rationale: The text describes the pathology of hemophilic arthritis: "Synovium shows marked vascular hyperplasia, hemosiderin deposits. Hemosiderin-stained pannus begins to creep over the joint surfaces." This is a direct consequence of recurrent bleeding and the body's response to blood products within the joint. The image (Fig. 6.10) shows destroyed cartilage surfaces and describes these synovial findings. The other options describe different pathologies.
Question 16
A 28-year-old female presents with chronic, diffuse pain in her left foot, which is worse with activity and improves with rest. She is a recreational runner who recently increased her mileage. Physical examination reveals diffuse swelling and tenderness across the midfoot. A bone scan shows a "hot spot" in the tarsal bones. Which of the following conditions is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: The history of increased activity, pain worse with activity and better with rest, and a "hot spot" on bone scan are classic indicators of a stress fracture. While Algodystrophy can also show increased uptake on bone scan (Fig. 4.18), its clinical presentation typically involves more pronounced vasomotor changes (warmth, redness), hyperesthesia, and often follows a specific trauma or immobilization, rather than just increased activity. The diffuse swelling and tenderness across the midfoot in a runner points more strongly to a stress fracture in the tarsals or metatarsals. Septic arthritis would have more acute inflammatory signs and often systemic symptoms. Gout would have a more acute, episodic presentation. Plantar fasciitis is a soft tissue condition and would not typically cause a "hot spot" on bone scan in the bone itself.
Question 17
A 2-year-old male presents with short stature and a waddling gait. His parents report he has always been smaller than his peers. Physical examination reveals disproportionate short stature with relatively short limbs and genu varum. Radiographs of the knees show widened, irregular, and cupped metaphyses with a broad growth plate. The epiphyses appear relatively normal. Which of the following is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of disproportionate short stature, waddling gait, genu varum, and radiographic findings of widened, irregular, and cupped metaphyses with relatively normal epiphyses are classic for metaphyseal chondrodysplasia, Schmid type. Achondroplasia typically presents with more severe rhizomelic shortening and characteristic skull findings (frontal bossing, midface hypoplasia) and often more pronounced diaphyseal involvement. Spondy
Question 17
A 6-month-old male presents with disproportionate short stature, characterized by short limbs and a relatively normal trunk length. Physical examination reveals rhizomelic shortening of the upper and lower extremities, prominent forehead (frontal bossing), and midface hypoplasia. Radiographs show short, broad long bones with metaphyseal flaring and cupping, as well as a narrow interpedicular distance in the lumbar spine. The foramen magnum appears small. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Achondroplasia is the most common non-lethal skeletal dysplasia, characterized by rhizomelic dwarfism, frontal bossing, midface hypoplasia, and specific radiographic findings including short, broad long bones with metaphyseal flaring, a narrow interpedicular distance in the lumbar spine, and a small foramen magnum. Hypochondroplasia is a milder form, while Schmid type metaphyseal chondrodysplasia typically lacks the craniofacial features and severe spinal changes. Spondyloepiphyseal dysplasia primarily affects the spine and epiphyses, and Cartilage-Hair Hypoplasia has distinct features like sparse hair and immunodeficiency.
Question 17
A 3-year-old boy is diagnosed with achondroplasia. His parents are both of average height and have no family history of skeletal dysplasia. Genetic testing confirms a mutation in the FGFR3 gene. What is the most likely inheritance pattern and origin of this mutation?
View Answer & Explanation
Correct Answer: C
Rationale: Achondroplasia is an autosomal dominant disorder caused by a gain-of-function mutation in the FGFR3 gene. In approximately 80% of cases, it arises from a de novo mutation, meaning neither parent is affected. If a parent were affected, it would be inherited in an autosomal dominant fashion. Autosomal recessive, X-linked, and mitochondrial inheritance patterns are incorrect for achondroplasia.
Question 17
A 9-month-old infant with achondroplasia presents with increasing hypotonia, central apnea episodes, and hyperreflexia. A neurological examination reveals signs of upper motor neuron involvement. What is the most critical orthopedic complication to investigate immediately?
View Answer & Explanation
Correct Answer: C
Rationale: Foramen magnum stenosis is a life-threatening complication in infants with achondroplasia, leading to brainstem compression. Symptoms like hypotonia, apnea, and hyperreflexia are indicative of this compression and require urgent investigation (MRI of the craniocervical junction) and potential surgical decompression. While genu varum, thoracolumbar kyphosis, spinal canal stenosis (more common in older children/adults), and hip dysplasia are known complications, foramen magnum stenosis presents the most immediate neurological threat in an infant with these symptoms.
Question 17
A 45-year-old male with a history of achondroplasia presents with progressive bilateral lower extremity weakness, numbness, and claudication-like symptoms. Physical examination reveals diminished sensation in a stocking-glove distribution and hyperreflexia. Radiographs show severe narrowing of the lumbar spinal canal. What is the most appropriate initial management strategy?
View Answer & Explanation
Correct Answer: D
Rationale: Progressive neurological deficits (weakness, numbness, hyperreflexia) in an adult with achondroplasia and spinal canal stenosis are indications for surgical decompression, typically a laminectomy. The anatomical narrowing of the spinal canal in achondroplasia often leads to severe stenosis that is not amenable to conservative management once neurological symptoms become significant. Physical therapy, NSAIDs, epidural injections, and bracing may provide temporary relief for mild symptoms but are insufficient for progressive neurological compromise.
Question 17
A 5-year-old girl presents with mild short stature and disproportionately short limbs. Her parents note that she is shorter than her peers but does not have the prominent forehead or midface hypoplasia seen in her cousin, who has achondroplasia. Radiographs show mild metaphyseal flaring and short long bones, but the skull and spine are relatively normal. Which diagnosis is most consistent with these findings?
View Answer & Explanation
Correct Answer: B
Rationale: Hypochondroplasia is a milder form of achondroplasia, also caused by a mutation in the FGFR3 gene. It presents with disproportionate short stature and short limbs but typically lacks the severe craniofacial features (frontal bossing, midface hypoplasia) and severe spinal changes (foramen magnum stenosis, severe lumbar stenosis) seen in achondroplasia. Metaphyseal chondrodysplasia, Schmid type, primarily affects metaphyses with less severe limb shortening and no craniofacial features. Spondyloepiphyseal dysplasia primarily affects the spine and epiphyses. Pseudoachondroplasia is a distinct condition with severe short stature, joint laxity, and epiphyseal involvement.
Question 17
A 7-year-old boy presents with a waddling gait and progressive bowing of his lower extremities. His height is below the 5th percentile, but his trunk length appears relatively normal. Physical examination reveals genu varum and mild rhizomelic shortening. There are no craniofacial abnormalities or signs of immunodeficiency. Radiographs show irregular, splayed, and cupped metaphyses, particularly around the knees and hips, with relatively normal epiphyses and spine. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Metaphyseal Chondrodysplasia, Schmid type, is the most common and mildest form of metaphyseal chondrodysplasia. It is characterized by short-limbed dwarfism, genu varum, and a waddling gait, with radiographic findings of irregular, splayed, and cupped metaphyses, especially at the knees and hips. It typically spares the spine and epiphyses and lacks the craniofacial features of achondroplasia or the systemic features (immunodeficiency, sparse hair) of McKusick type. Hypophosphatemic rickets would show similar metaphyseal changes but would also have biochemical abnormalities (low phosphate, normal calcium) and often a family history of rickets, and is not a primary dysplasia.
Question 17
A 6-year-old girl with Metaphyseal Chondrodysplasia, Schmid type, is being evaluated for progressive genu varum. Her parents are concerned about her gait and potential for future arthritis. What is the characteristic radiographic finding in the metaphyses that supports this diagnosis and contributes to the bowing deformity?
View Answer & Explanation
Correct Answer: C
Rationale: Metaphyseal Chondrodysplasia, Schmid type, is characterized by irregular, splayed, and cupped metaphyses due to disorganization of the growth plate, particularly in the zone of provisional calcification. This abnormal growth leads to the characteristic bowing deformities like genu varum. Dense metaphyses are seen in osteopetrosis. Flattened epiphyses are typical of epiphyseal dysplasias. Erlenmeyer flask deformity is characteristic of Pyle disease or Gaucher disease. Premature growth plate fusion is not a primary feature of Schmid type.
Question 17
A 2-year-old boy presents with short-limbed dwarfism, fine, sparse, light-colored hair, and a history of recurrent severe infections. His parents report frequent episodes of diarrhea. Radiographs show metaphyseal irregularities and short long bones. Which additional systemic finding is most commonly associated with this diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of short-limbed dwarfism, sparse hair, and recurrent infections is highly suggestive of Cartilage-Hair Hypoplasia (McKusick type metaphyseal chondrodysplasia). A key systemic feature of this condition is T-cell immunodeficiency, which accounts for the susceptibility to severe infections and can also be associated with Hirschsprung disease (leading to diarrhea). Hypercalcemia and hypophosphatemia are characteristic of Jansen type metaphyseal chondrodysplasia. Intellectual disability, renal tubular acidosis, and craniosynostosis are not primary features of McKusick type.
Question 17
A family is seeking genetic counseling after their child was diagnosed with Cartilage-Hair Hypoplasia (McKusick type metaphyseal chondrodysplasia). The parents are unaffected. What is the most likely inheritance pattern for this condition?
View Answer & Explanation
Correct Answer: B
Rationale: Cartilage-Hair Hypoplasia (McKusick type metaphyseal chondrodysplasia) is inherited in an autosomal recessive pattern. It is caused by mutations in the RMRP gene. This means that both parents must be carriers of the mutated gene, even if they do not show symptoms themselves. Autosomal dominant inheritance (like achondroplasia) would typically mean at least one parent is affected or it's a de novo mutation. X-linked and mitochondrial inheritance patterns are incorrect for this condition.
Question 17
A newborn presents with severe short-limbed dwarfism, profound metaphyseal irregularities, and hypercalcemia with hypophosphatemia. Radiographs show extremely short, broad long bones with severe metaphyseal cupping and fraying, resembling rickets but without vitamin D deficiency. This constellation of findings is most characteristic of which skeletal dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: Metaphyseal Chondrodysplasia, Jansen type, is a rare and severe form characterized by profound short-limbed dwarfism, severe metaphyseal abnormalities, and a unique biochemical profile of hypercalcemia and hypophosphatemia, often mimicking hyperparathyroidism. Achondroplasia and Schmid type are generally milder and lack these specific biochemical abnormalities. McKusick type has immunodeficiency and sparse hair. Hypophosphatemic rickets would present with hypophosphatemia but typically normal or low calcium, and is a metabolic disorder rather than a primary dysplasia.
Question 17
A 10-year-old boy is evaluated for mild short stature and a history of frequent fractures. Physical examination reveals a relatively normal skull and facial features. Radiographs of the long bones show marked widening of the metaphyses, giving them an "Erlenmeyer flask" appearance, particularly in the distal femurs. The bone density appears normal. Which condition is most consistent with these findings?
View Answer & Explanation
Correct Answer: C
Rationale: Pyle disease, also known as metaphyseal dysplasia, is characterized by marked widening (splaying) of the metaphyses of long bones, leading to the classic "Erlenmeyer flask" deformity, particularly in the distal femurs. Unlike osteopetrosis, bone density is typically normal or reduced, and there are no significant skull abnormalities. Craniometaphyseal dysplasia involves both skull thickening and metaphyseal flaring. Hypophosphatemic rickets causes metaphyseal cupping and fraying but not typically the Erlenmeyer flask deformity. Achondroplasia has short, broad metaphyses but not the severe flaring of Pyle disease.
Question 17
A 4-year-old child presents with progressive frontal bossing, hypertelorism, and a broad nasal bridge. Radiographs of the skull show diffuse thickening and sclerosis, particularly of the frontal and occipital bones. Long bone radiographs reveal metaphyseal flaring and widening, but without significant short stature. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Craniometaphyseal dysplasia is characterized by a combination of craniofacial abnormalities (frontal bossing, hypertelorism, broad nasal bridge) due to skull thickening and sclerosis, along with metaphyseal flaring and widening of long bones. Pyle disease primarily affects metaphyses without significant skull involvement. Achondroplasia has frontal bossing but also severe short stature and different metaphyseal changes. Osteopetrosis involves generalized increased bone density and can have metaphyseal changes but typically presents with more severe bone fragility and hematological issues. Fibrous dysplasia is a localized bone disorder, not a generalized dysplasia.
Question 17
Mutations in the Fibroblast Growth Factor Receptor 3 (FGFR3) gene are responsible for several skeletal dysplasias with metaphyseal involvement. Which of the following conditions is *not* typically associated with an activating mutation in the FGFR3 gene?
View Answer & Explanation
Correct Answer: D
Rationale: Achondroplasia, hypochondroplasia, thanatophoric dysplasia, and SADDAN are all caused by activating mutations in the FGFR3 gene, representing a spectrum of severity. Spondyloepiphyseal Dysplasia Tarda (SEDT) is typically caused by mutations in the TRAPPC2 gene (formerly SEDL) and is X-linked recessive, not associated with FGFR3 mutations. It primarily affects the spine and epiphyses, with less prominent metaphyseal involvement compared to the FGFR3-related conditions.
Question 17
In skeletal dysplasias with predominant metaphyseal involvement, the primary defect often lies in the process of endochondral ossification. Which specific zone of the growth plate is most commonly disrupted, leading to the characteristic metaphyseal abnormalities?
View Answer & Explanation
Correct Answer: D
Rationale: In many metaphyseal dysplasias, the primary defect is in the orderly maturation and calcification of cartilage in the hypertrophic zone and the subsequent removal of cartilage and deposition of bone in the zone of provisional calcification. This leads to disorganized cartilage columns, inadequate calcification, and defective remodeling, resulting in the characteristic splaying, cupping, and irregularity of the metaphyses. While the proliferative and hypertrophic zones are also affected in conditions like achondroplasia (FGFR3 signaling), the *visible* metaphyseal changes are a direct consequence of the failure of proper provisional calcification and subsequent ossification.
Question 17
A 1-year-old infant presents with bowing of the legs and widening of the wrists and ankles. Radiographs show prominent metaphyseal cupping and fraying. Biochemical tests reveal low serum phosphate, normal serum calcium, and elevated alkaline phosphatase. Which condition is the most important differential diagnosis to consider alongside genetic metaphyseal chondrodysplasias?
View Answer & Explanation
Correct Answer: C
Rationale: The combination of metaphyseal cupping/fraying, bowing of legs, and specific biochemical findings (low serum phosphate, normal calcium, elevated alkaline phosphatase) is highly suggestive of hypophosphatemic rickets. This metabolic bone disorder causes significant metaphyseal changes that can mimic genetic metaphyseal chondrodysplasias. Achondroplasia, osteopetrosis, spondyloepiphyseal dysplasia, and craniometaphyseal dysplasia are genetic dysplasias with different primary features and biochemical profiles.
Question 17
A 12-year-old boy with a metaphyseal chondrodysplasia presents with significant bilateral genu varum (bowlegs) causing functional limitations and pain. His growth plates are still open. What is the most appropriate surgical intervention to address the angular deformity?
View Answer & Explanation
Correct Answer: B
Rationale: For angular deformities like genu varum in growing children with open physes, hemiepiphysiodesis (guided growth) is often the preferred method. By temporarily arresting growth on the convex side of the deformity (medial side for genu varum), the remaining growth on the concave side allows for gradual correction. Corrective osteotomy is an option for more severe deformities or in skeletally mature patients. External fixation is typically used for complex deformities, limb lengthening, or nonunions. Total knee arthroplasty and amputation are not appropriate for this age and condition.
Question 17
A couple is expecting their second child, and their first child was diagnosed with a severe form of metaphyseal chondrodysplasia. They are concerned about the recurrence risk and potential prenatal diagnosis. What is the most important initial step for the orthopedic surgeon to recommend regarding their concerns?
View Answer & Explanation
Correct Answer: C
Rationale: The most important initial step is to refer the couple to a genetic counselor. Genetic counselors can take a detailed family history, explain the specific inheritance pattern of the diagnosed metaphyseal chondrodysplasia (which varies widely), discuss recurrence risks, and outline available options for genetic testing (for parents and potentially prenatal diagnosis for future pregnancies). Prenatal ultrasound might be recommended by the genetic counselor, but it's not the first step for the orthopedic surgeon. Advising against more children is premature and inappropriate without genetic counseling. Nutritional supplements are irrelevant to genetic dysplasias. An orthopedic consultation for the newborn is important but does not address the parents' genetic concerns.
Question 17
Which of the following skeletal dysplasias, characterized by predominant metaphyseal involvement, is considered the most common non-lethal form?
View Answer & Explanation
Correct Answer: C
Rationale: Achondroplasia is by far the most common non-lethal skeletal dysplasia, with an incidence of approximately 1 in 20,000 to 30,000 live births. While it affects endochondral ossification throughout the skeleton, its impact on long bone growth plates leads to characteristic metaphyseal changes. Jansen type is very rare and severe. McKusick type is also rare. Spondyloepiphyseal dysplasia congenita and diastrophic dysplasia are less common than achondroplasia.
Question 17
A 3-year-old child presents with short stature and bowing of the lower extremities. Radiographs show widened, irregular, and cupped metaphyses. To differentiate between a genetic metaphyseal chondrodysplasia and nutritional rickets, which of the following laboratory tests would be most crucial?
View Answer & Explanation
Correct Answer: B
Rationale: Nutritional rickets (due to vitamin D deficiency) and hypophosphatemic rickets are metabolic conditions that cause significant metaphyseal changes resembling those seen in genetic metaphyseal chondrodysplasias. Measuring serum calcium, phosphate, alkaline phosphatase, and vitamin D levels is crucial to distinguish between these conditions. Rickets will show characteristic biochemical abnormalities (e.g., low vitamin D, low calcium/phosphate, high alkaline phosphatase), whereas genetic dysplasias typically have normal or specific, non-rickets-related biochemical profiles (e.g., hypercalcemia in Jansen type). The
Question 18
A 6-month-old male presents with disproportionate short stature, characterized by short limbs and a relatively normal trunk length. Physical examination reveals rhizomelic shortening of the upper and lower extremities, prominent forehead (frontal bossing), and midface hypoplasia. Radiographs show short, broad long bones with metaphyseal flaring and cupping, as well as a narrow interpedicular distance in the lumbar spine. The foramen magnum appears small. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Achondroplasia is the most common non-lethal skeletal dysplasia, characterized by rhizomelic dwarfism, frontal bossing, midface hypoplasia, and specific radiographic findings including short, broad long bones with metaphyseal flaring, a narrow interpedicular distance in the lumbar spine, and a small foramen magnum. Hypochondroplasia is a milder form, while Schmid type metaphyseal chondrodysplasia typically lacks the craniofacial features and severe spinal changes. Spondyloepiphyseal dysplasia primarily affects the spine and epiphyses, and Cartilage-Hair Hypoplasia has distinct features like sparse hair and immunodeficiency.
Question 19
A 3-year-old boy is diagnosed with achondroplasia. His parents are both of average height and have no family history of skeletal dysplasia. Genetic testing confirms a mutation in the FGFR3 gene. What is the most likely inheritance pattern and origin of this mutation?
View Answer & Explanation
Correct Answer: C
Rationale: Achondroplasia is an autosomal dominant disorder caused by a gain-of-function mutation in the FGFR3 gene. In approximately 80% of cases, it arises from a de novo mutation, meaning neither parent is affected. If a parent were affected, it would be inherited in an autosomal dominant fashion. Autosomal recessive, X-linked, and mitochondrial inheritance patterns are incorrect for achondroplasia.
Question 20
A 9-month-old infant with achondroplasia presents with increasing hypotonia, central apnea episodes, and hyperreflexia. A neurological examination reveals signs of upper motor neuron involvement. What is the most critical orthopedic complication to investigate immediately?
View Answer & Explanation
Correct Answer: C
Rationale: Foramen magnum stenosis is a life-threatening complication in infants with achondroplasia, leading to brainstem compression. Symptoms like hypotonia, apnea, and hyperreflexia are indicative of this compression and require urgent investigation (MRI of the craniocervical junction) and potential surgical decompression. While genu varum, thoracolumbar kyphosis, spinal canal stenosis (more common in older children/adults), and hip dysplasia are known complications, foramen magnum stenosis presents the most immediate neurological threat in an infant with these symptoms.
Question 21
A 45-year-old male with a history of achondroplasia presents with progressive bilateral lower extremity weakness, numbness, and claudication-like symptoms. Physical examination reveals diminished sensation in a stocking-glove distribution and hyperreflexia. Radiographs show severe narrowing of the lumbar spinal canal. What is the most appropriate initial management strategy?
View Answer & Explanation
Correct Answer: D
Rationale: Progressive neurological deficits (weakness, numbness, hyperreflexia) in an adult with achondroplasia and spinal canal stenosis are indications for surgical decompression, typically a laminectomy. The anatomical narrowing of the spinal canal in achondroplasia often leads to severe stenosis that is not amenable to conservative management once neurological symptoms become significant. Physical therapy, NSAIDs, epidural injections, and bracing may provide temporary relief for mild symptoms but are insufficient for progressive neurological compromise.
Question 22
A 5-year-old girl presents with mild short stature and disproportionately short limbs. Her parents note that she is shorter than her peers but does not have the prominent forehead or midface hypoplasia seen in her cousin, who has achondroplasia. Radiographs show mild metaphyseal flaring and short long bones, but the skull and spine are relatively normal. Which diagnosis is most consistent with these findings?
View Answer & Explanation
Correct Answer: B
Rationale: Hypochondroplasia is a milder form of achondroplasia, also caused by a mutation in the FGFR3 gene. It presents with disproportionate short stature and short limbs but typically lacks the severe craniofacial features (frontal bossing, midface hypoplasia) and severe spinal changes (foramen magnum stenosis, severe lumbar stenosis) seen in achondroplasia. Metaphyseal chondrodysplasia, Schmid type, primarily affects metaphyses with less severe limb shortening and no craniofacial features. Spondyloepiphyseal dysplasia primarily affects the spine and epiphyses. Pseudoachondroplasia is a distinct condition with severe short stature, joint laxity, and epiphyseal involvement.
Question 23
A 7-year-old boy presents with a waddling gait and progressive bowing of his lower extremities. His height is below the 5th percentile, but his trunk length appears relatively normal. Physical examination reveals genu varum and mild rhizomelic shortening. There are no craniofacial abnormalities or signs of immunodeficiency. Radiographs show irregular, splayed, and cupped metaphyses, particularly around the knees and hips, with relatively normal epiphyses and spine. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Metaphyseal Chondrodysplasia, Schmid type, is the most common and mildest form of metaphyseal chondrodysplasia. It is characterized by short-limbed dwarfism, genu varum, and a waddling gait, with radiographic findings of irregular, splayed, and cupped metaphyses, especially at the knees and hips. It typically spares the spine and epiphyses and lacks the craniofacial features of achondroplasia or the systemic features (immunodeficiency, sparse hair) of McKusick type. Hypophosphatemic rickets would show similar metaphyseal changes but would also have biochemical abnormalities (low phosphate, normal calcium) and often a family history of rickets, and is not a primary dysplasia.
Question 24
A 6-year-old girl with Metaphyseal Chondrodysplasia, Schmid type, is being evaluated for progressive genu varum. Her parents are concerned about her gait and potential for future arthritis. What is the characteristic radiographic finding in the metaphyses that supports this diagnosis and contributes to the bowing deformity?
View Answer & Explanation
Correct Answer: C
Rationale: Metaphyseal Chondrodysplasia, Schmid type, is characterized by irregular, splayed, and cupped metaphyses due to disorganization of the growth plate, particularly in the zone of provisional calcification. This abnormal growth leads to the characteristic bowing deformities like genu varum. Dense metaphyses are seen in osteopetrosis. Flattened epiphyses are typical of epiphyseal dysplasias. Erlenmeyer flask deformity is characteristic of Pyle disease or Gaucher disease. Premature growth plate fusion is not a primary feature of Schmid type.
Question 25
A 2-year-old boy presents with short-limbed dwarfism, fine, sparse, light-colored hair, and a history of recurrent severe infections. His parents report frequent episodes of diarrhea. Radiographs show metaphyseal irregularities and short long bones. Which additional systemic finding is most commonly associated with this diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation of short-limbed dwarfism, sparse hair, and recurrent infections is highly suggestive of Cartilage-Hair Hypoplasia (McKusick type metaphyseal chondrodysplasia). A key systemic feature of this condition is T-cell immunodeficiency, which accounts for the susceptibility to severe infections and can also be associated with Hirschsprung disease (leading to diarrhea). Hypercalcemia and hypophosphatemia are characteristic of Jansen type metaphyseal chondrodysplasia. Intellectual disability, renal tubular acidosis, and craniosynostosis are not primary features of McKusick type.
Question 26
A family is seeking genetic counseling after their child was diagnosed with Cartilage-Hair Hypoplasia (McKusick type metaphyseal chondrodysplasia). The parents are unaffected. What is the most likely inheritance pattern for this condition?
View Answer & Explanation
Correct Answer: B
Rationale: Cartilage-Hair Hypoplasia (McKusick type metaphyseal chondrodysplasia) is inherited in an autosomal recessive pattern. It is caused by mutations in the RMRP gene. This means that both parents must be carriers of the mutated gene, even if they do not show symptoms themselves. Autosomal dominant inheritance (like achondroplasia) would typically mean at least one parent is affected or it's a de novo mutation. X-linked and mitochondrial inheritance patterns are incorrect for this condition.
Question 27
A newborn presents with severe short-limbed dwarfism, profound metaphyseal irregularities, and hypercalcemia with hypophosphatemia. Radiographs show extremely short, broad long bones with severe metaphyseal cupping and fraying, resembling rickets but without vitamin D deficiency. This constellation of findings is most characteristic of which skeletal dysplasia?
View Answer & Explanation
Correct Answer: C
Rationale: Metaphyseal Chondrodysplasia, Jansen type, is a rare and severe form characterized by profound short-limbed dwarfism, severe metaphyseal abnormalities, and a unique biochemical profile of hypercalcemia and hypophosphatemia, often mimicking hyperparathyroidism. Achondroplasia and Schmid type are generally milder and lack these specific biochemical abnormalities. McKusick type has immunodeficiency and sparse hair. Hypophosphatemic rickets would present with hypophosphatemia but typically normal or low calcium, and is a metabolic disorder rather than a primary dysplasia.
Question 28
A 10-year-old boy is evaluated for mild short stature and a history of frequent fractures. Physical examination reveals a relatively normal skull and facial features. Radiographs of the long bones show marked widening of the metaphyses, giving them an "Erlenmeyer flask" appearance, particularly in the distal femurs. The bone density appears normal. Which condition is most consistent with these findings?
View Answer & Explanation
Correct Answer: C
Rationale: Pyle disease, also known as metaphyseal dysplasia, is characterized by marked widening (splaying) of the metaphyses of long bones, leading to the classic "Erlenmeyer flask" deformity, particularly in the distal femurs. Unlike osteopetrosis, bone density is typically normal or reduced, and there are no significant skull abnormalities. Craniometaphyseal dysplasia involves both skull thickening and metaphyseal flaring. Hypophosphatemic rickets causes metaphyseal cupping and fraying but not typically the Erlenmeyer flask deformity. Achondroplasia has short, broad metaphyses but not the severe flaring of Pyle disease.
Question 29
A 4-year-old child presents with progressive frontal bossing, hypertelorism, and a broad nasal bridge. Radiographs of the skull show diffuse thickening and sclerosis, particularly of the frontal and occipital bones. Long bone radiographs reveal metaphyseal flaring and widening, but without significant short stature. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: C
Rationale: Craniometaphyseal dysplasia is characterized by a combination of craniofacial abnormalities (frontal bossing, hypertelorism, broad nasal bridge) due to skull thickening and sclerosis, along with metaphyseal flaring and widening of long bones. Pyle disease primarily affects metaphyses without significant skull involvement. Achondroplasia has frontal bossing but also severe short stature and different metaphyseal changes. Osteopetrosis involves generalized increased bone density and can have metaphyseal changes but typically presents with more severe bone fragility and hematological issues. Fibrous dysplasia is a localized bone disorder, not a generalized dysplasia.
Question 30
Mutations in the Fibroblast Growth Factor Receptor 3 (FGFR3) gene are responsible for several skeletal dysplasias with metaphyseal involvement. Which of the following conditions is *not* typically associated with an activating mutation in the FGFR3 gene?
View Answer & Explanation
Correct Answer: D
Rationale: Achondroplasia, hypochondroplasia, thanatophoric dysplasia, and SADDAN are all caused by activating mutations in the FGFR3 gene, representing a spectrum of severity. Spondyloepiphyseal Dysplasia Tarda (SEDT) is typically caused by mutations in the TRAPPC2 gene (formerly SEDL) and is X-linked recessive, not associated with FGFR3 mutations. It primarily affects the spine and epiphyses, with less prominent metaphyseal involvement compared to the FGFR3-related conditions.
Question 31
In skeletal dysplasias with predominant metaphyseal involvement, the primary defect often lies in the process of endochondral ossification. Which specific zone of the growth plate is most commonly disrupted, leading to the characteristic metaphyseal abnormalities?
View Answer & Explanation
Correct Answer: D
Rationale: In many metaphyseal dysplasias, the primary defect is in the orderly maturation and calcification of cartilage in the hypertrophic zone and the subsequent removal of cartilage and deposition of bone in the zone of provisional calcification. This leads to disorganized cartilage columns, inadequate calcification, and defective remodeling, resulting in the characteristic splaying, cupping, and irregularity of the metaphyses. While the proliferative and hypertrophic zones are also affected in conditions like achondroplasia (FGFR3 signaling), the *visible* metaphyseal changes are a direct consequence of the failure of proper provisional calcification and subsequent ossification.
Question 32
A 1-year-old infant presents with bowing of the legs and widening of the wrists and ankles. Radiographs show prominent metaphyseal cupping and fraying. Biochemical tests reveal low serum phosphate, normal serum calcium, and elevated alkaline phosphatase. Which condition is the most important differential diagnosis to consider alongside genetic metaphyseal chondrodysplasias?
View Answer & Explanation
Correct Answer: C
Rationale: The combination of metaphyseal cupping/fraying, bowing of legs, and specific biochemical findings (low serum phosphate, normal calcium, elevated alkaline phosphatase) is highly suggestive of hypophosphatemic rickets. This metabolic bone disorder causes significant metaphyseal changes that can mimic genetic metaphyseal chondrodysplasias. Achondroplasia, osteopetrosis, spondyloepiphyseal dysplasia, and craniometaphyseal dysplasia are genetic dysplasias with different primary features and biochemical profiles.
Question 33
A 12-year-old boy with a metaphyseal chondrodysplasia presents with significant bilateral genu varum (bowlegs) causing functional limitations and pain. His growth plates are still open. What is the most appropriate surgical intervention to address the angular deformity?
View Answer & Explanation
Correct Answer: B
Rationale: For angular deformities like genu varum in growing children with open physes, hemiepiphysiodesis (guided growth) is often the preferred method. By temporarily arresting growth on the convex side of the deformity (medial side for genu varum), the remaining growth on the concave side allows for gradual correction. Corrective osteotomy is an option for more severe deformities or in skeletally mature patients. External fixation is typically used for complex deformities, limb lengthening, or nonunions. Total knee arthroplasty and amputation are not appropriate for this age and condition.
Question 34
A couple is expecting their second child, and their first child was diagnosed with a severe form of metaphyseal chondrodysplasia. They are concerned about the recurrence risk and potential prenatal diagnosis. What is the most important initial step for the orthopedic surgeon to recommend regarding their concerns?
View Answer & Explanation
Correct Answer: C
Rationale: The most important initial step is to refer the couple to a genetic counselor. Genetic counselors can take a detailed family history, explain the specific inheritance pattern of the diagnosed metaphyseal chondrodysplasia (which varies widely), discuss recurrence risks, and outline available options for genetic testing (for parents and potentially prenatal diagnosis for future pregnancies). Prenatal ultrasound might be recommended by the genetic counselor, but it's not the first step for the orthopedic surgeon. Advising against more children is premature and inappropriate without genetic counseling. Nutritional supplements are irrelevant to genetic dysplasias. An orthopedic consultation for the newborn is important but does not address the parents' genetic concerns.
Question 35
Which of the following skeletal dysplasias, characterized by predominant metaphyseal involvement, is considered the most common non-lethal form?
View Answer & Explanation
Correct Answer: C
Rationale: Achondroplasia is by far the most common non-lethal skeletal dysplasia, with an incidence of approximately 1 in 20,000 to 30,000 live births. While it affects endochondral ossification throughout the skeleton, its impact on long bone growth plates leads to characteristic metaphyseal changes. Jansen type is very rare and severe. McKusick type is also rare. Spondyloepiphyseal dysplasia congenita and diastrophic dysplasia are less common than achondroplasia.
Question 36
A 14-year-old male presents with a 6-month history of localized, throbbing pain in his distal tibia. The pain is consistently worse at night and is significantly relieved by over-the-counter ibuprofen. Physical examination reveals minimal swelling but no tenderness to palpation. Radiographs show a small, sclerotic lesion with a central lucency.
View Answer & Explanation
Correct Answer: A
Rationale: The classic presentation of an osteoid osteoma includes intense, throbbing, night pain that is largely relieved by nonsteroidal anti-inflammatory medicines, typically occurring in adolescents, especially males. The radiographic findings of a small sclerotic lesion with a central lucency (nidus) are also characteristic. Osteoblastoma can have similar histology but typically presents with a larger nidus and less dramatic NSAID response. Ewing sarcoma and osteosarcoma are malignant and would have a more aggressive clinical and radiographic presentation. Chondroblastoma typically affects epiphyses and has different pain characteristics.
Question 37
A 16-year-old boy complains of persistent pain in his left proximal femur for several months. He describes the pain as deep and aching, particularly bothersome at night, often waking him from sleep. He finds significant relief after taking naproxen. On examination, there is no obvious deformity or warmth, but mild tenderness is elicited over the greater trochanter. Imaging reveals a small, well-circumscribed lesion within the femoral cortex.
View Answer & Explanation
Correct Answer: A
Rationale: The clinical vignette describes the classic symptoms of an osteoid osteoma: intense, throbbing, night pain that is largely relieved by nonsteroidal anti-inflammatory medicines. This is a hallmark feature distinguishing it from many other bone lesions. Options B, C, D, and E describe symptoms less characteristic of an osteoid osteoma and more suggestive of other conditions like stress fractures, arthritis, infection, or acute trauma, respectively.
Question 38
A 15-year-old male presents with a several-month history of localized pain in his right tibia. The pain is worse at night and improves significantly with ibuprofen. Radiographs show a small, sclerotic lesion in the tibial diaphysis. A diagnosis of osteoid osteoma is suspected.
View Answer & Explanation
Correct Answer: A
Rationale: Osteoid osteomas most commonly occur during adolescence, and males are affected more commonly than females. The patient's age and gender in the vignette perfectly match this demographic profile. The other options represent age and gender groups less commonly associated with osteoid osteomas.
Question 39
A 13-year-old male presents with chronic, localized pain in his left thigh, which is worse at night and partially relieved by NSAIDs. Physical examination is unremarkable. Radiographs show a small, dense lesion with a lucent center in the proximal femur.
View Answer & Explanation
Correct Answer: A
Rationale: The text states that most osteoid osteomas occur in the meta- or diaphysis of the long bones, specifically mentioning the proximal femur and tibia as common locations. The proximal femur is a classic site for this lesion. While osteoid osteomas can occur in other bones, the proximal femur is a highly prevalent location.
Question 40
A 12-year-old girl is evaluated for progressive back pain and a newly developing scoliotic curve. Her pain is worse at night and shows some improvement with ibuprofen. Imaging studies reveal a small, sclerotic lesion within a lumbar vertebral body, consistent with an osteoid osteoma.
View Answer & Explanation
Correct Answer: A
Rationale: The provided text explicitly states that "spinal lesions can lead to painful scoliosis" in the context of osteoid osteoma. This presentation, with back pain and scoliosis, is a well-recognized manifestation of an osteoid osteoma located in the spine. Other locations listed are less likely to cause scoliosis.
Question 41
A 17-year-old male presents with chronic knee pain, particularly at night, which is relieved by aspirin. MRI shows significant associated edema and adjacent periostitis around the distal femur, suggestive of an osteoid osteoma. The lesion is found to be located within the joint capsule.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states that "Ten per cent has an intraarticular location." This makes intraarticular osteoid osteomas a less common, but recognized, presentation. The other percentages are incorrect according to the provided information.
Question 42
A 14-year-old male presents with localized pain in his distal femur, worse at night and relieved by NSAIDs. A CT scan is performed to further characterize the lesion.
View Answer & Explanation
Correct Answer: A
Rationale: Figure 8.6a, an axial CT image, clearly shows "typical surrounding medullary sclerosis" associated with a juxtacortical osteoid osteoma of the distal femur. This reactive sclerosis around the lucent nidus is a classic CT finding for osteoid osteoma. Cortical thinning, pathologic fracture, and large soft tissue masses are not typical CT features of an osteoid osteoma, and joint effusion is a secondary finding, not a primary bone change.
Question 43
A 16-year-old female presents with chronic knee pain, particularly at night, which is partially relieved by over-the-counter pain medication. An MRI is performed to evaluate the distal femur for a suspected bone lesion.
View Answer & Explanation
Correct Answer: A
Rationale: Figure 8.6b, a T2-weighted MRI, demonstrates "significant associated edema and adjacent periostitis" around the juxtacortical osteoid osteoma. These inflammatory changes in the surrounding soft tissues and bone are characteristic MRI findings, often more prominent than the nidus itself. Extensive cortical destruction, large soft tissue components, metastatic lesions, or degenerative changes are not typical MRI features of an osteoid osteoma.
Question 44
During surgical excision of a suspected osteoid osteoma from a 15-year-old patient, the nidus is identified and removed. The surgeon notes its distinct appearance.

View Answer & Explanation
Correct Answer: A
Rationale: Figure 8.9, a gross pathologic image, explicitly states that "The nidus is typically 'cherry-red' on gross examination." This distinct color is a key identifying feature during surgical removal and gross pathological assessment. The other descriptions do not match the characteristic appearance of an osteoid osteoma nidus.
Question 45
A biopsy is performed on a bone lesion from a 14-year-old male presenting with classic symptoms of an osteoid osteoma. Microscopic evaluation is undertaken to confirm the diagnosis.
View Answer & Explanation
Correct Answer: A
Rationale: Figure 8.10, a microscopic evaluation image, clearly shows "Thin, irregular osteoid trabeculae are evident on microscopic evaluation." This is a characteristic histological feature of the nidus of an osteoid osteoma. Broad lamellar bone is mature bone, a cartilaginous cap is seen in osteochondromas, spindle cell proliferation with pleomorphism suggests malignancy, and numerous giant cells are characteristic of giant cell tumors.
Question 46
Microscopic examination of a resected osteoid osteoma nidus from a 16-year-old patient reveals the characteristic bone formation. The pathologist also notes the nature of the intervening tissue.
View Answer & Explanation
Correct Answer: A
Rationale: Figure 8.10, a microscopic evaluation image, states that "There is loose fibrovascular connective tissue between the trabeculae." This loose, vascularized connective tissue is an integral component of the osteoid osteoma nidus, supporting the osteoid trabeculae. The other options describe different types of connective tissue not characteristic of an osteoid osteoma.
Question 47
A high-power microscopic examination of an osteoid osteoma nidus is performed to assess the cellular characteristics of the lesion.
View Answer & Explanation
Correct Answer: A
Rationale: Figure 8.11, a higher power microscopic examination image, explicitly states that it "shows osteoid with uniform osteoblasts without nuclear atypia." This lack of atypia and the uniform appearance of the osteoblasts are crucial features confirming the benign nature of the lesion. Pleomorphic osteoblasts with atypia would suggest malignancy (e.g., osteosarcoma). The other options describe cells characteristic of different tumor types.
Question 48
A 14-year-old male presents with classic symptoms of an osteoid osteoma in the distal tibia. His pain is worse at night and relieved by NSAIDs. He denies any recent trauma or fever.
View Answer & Explanation
Correct Answer: A
Rationale: The text states that "Patients have minimal findings on clinical examination." While some may have swelling, muscle atrophy, or spasm, the overall clinical examination is often unremarkable, especially compared to the intensity of the pain. Significant joint instability, a pulsatile mass, skin discoloration, or a pathologic fracture are not typical primary findings for an osteoid osteoma.
Question 49
A 16-year-old female is diagnosed with an osteoid osteoma in the proximal femur after presenting with chronic, NSAID-responsive night pain. Her physical examination is mostly unremarkable, but the physician notes a subtle change in the affected limb.
View Answer & Explanation
Correct Answer: A
Rationale: The text mentions that "some [patients] will have swelling, muscle atrophy, or spasm" as associated clinical findings, despite generally having minimal findings on examination. These are localized reactions to the lesion. High-grade fever, weight loss, lymphadenopathy, or skin rash are systemic symptoms not typically associated with a benign osteoid osteoma.
Question 50
A benign bone lesion is identified in a patient presenting with localized pain. The lesion exhibits characteristic features of an osteoid osteoma on imaging and biopsy.
View Answer & Explanation
Correct Answer: A
Rationale: The text explicitly states that "Osteoid osteomas are uniquely painful benign lesions that most commonly occur during adolescence." This makes adolescence the most prevalent age group for this condition. The other age groups are less commonly affected.
Question 51
A 15-year-old patient presents with classic symptoms of an osteoid osteoma, including intense night pain relieved by NSAIDs. Imaging confirms the diagnosis.
- A) Males
- B) Females
-
Question 51
A 14-year-old male presents with a 6-month history of worsening right distal thigh pain, particularly at night, which is significantly relieved by ibuprofen. Physical examination reveals mild tenderness over the distal femur. Radiographs show cortical thickening, and a subsequent CT scan confirms a small lucent nidus with surrounding medullary sclerosis in the distal femoral diaphysis.
View Answer & Explanation
Correct Answer: A
Rationale: For osteoid osteomas, especially in cases with classic symptoms well-controlled by NSAIDs, initial management often involves observation with continued NSAID use. While surgical or interventional options exist, many patients can manage their symptoms effectively with conservative measures, and some lesions may even spontaneously resolve over time. Open surgical excision is a definitive treatment but is more invasive than other options and not always the first choice if symptoms are well-controlled. Radiation and chemotherapy are not indicated for benign osteoid osteoma. Intralesional curettage with bone grafting is a surgical option but not the primary conservative approach.
Question 51
A 16-year-old male presents with a 9-month history of left proximal tibia pain, worse at night and partially relieved by over-the-counter analgesics. MRI shows significant associated edema and adjacent periostitis in the proximal tibia. A CT scan confirms a small cortical lesion with a central lucent nidus. The patient desires a more definitive treatment than continuous NSAID use due to side effects and incomplete pain relief.
View Answer & Explanation
Correct Answer: B
Rationale: Percutaneous radiofrequency ablation (RFA) is a highly effective and minimally invasive treatment for osteoid osteomas, offering excellent pain relief with low complication rates. It is often preferred over open surgery when conservative management fails or is not desired. Systemic corticosteroids are not a primary treatment for osteoid osteoma. External beam radiation is not indicated for this benign lesion. Wide en bloc resection is an overly aggressive procedure for a benign osteoid osteoma. Long-term opioid therapy is inappropriate given the availability of definitive treatments.
Question 51
A 12-year-old female presents with progressive scoliosis and chronic low back pain. Imaging reveals a small, lucent lesion with surrounding sclerosis in a lumbar vertebral pedicle. The pain is worse at night and partially responsive to NSAIDs. Given the location of the lesion, what is the most likely specific complication directly attributable to this osteoid osteoma?
View Answer & Explanation
Correct Answer: C
Rationale: Spinal lesions, particularly osteoid osteomas, can lead to painful scoliosis due to muscle spasm and asymmetric growth stimulation. The case text explicitly states, "spinal lesions can lead to painful scoliosis." While other complications can occur in the spine, painful scoliosis is a classic presentation for osteoid osteoma in this location. Pathologic fracture is rare for osteoid osteoma. Spinal cord compression is less common unless the lesion is very large or in a critical location. Malignant transformation is exceedingly rare for osteoid osteoma. Vertebral body collapse is not a typical complication of osteoid osteoma.
Question 51
A 10-year-old boy presents with chronic right knee pain, swelling, and a limp. Physical examination reveals a warm, swollen knee with a mild effusion. Radiographs are initially unremarkable, but an MRI shows synovitis and significant edema within the distal femur, adjacent to the joint. A subsequent CT scan identifies a small osteoid osteoma in the juxta-articular region of the distal femur. What is the most likely reason for the joint-related symptoms?
View Answer & Explanation
Correct Answer: B
Rationale: Osteoid osteomas, especially those in an intra-articular or juxta-articular location, can release prostaglandins and other inflammatory mediators, leading to synovitis, joint effusion, and associated joint pain. The case text mentions that 10% of lesions have an intraarticular location. Direct invasion of the joint capsule is not the primary mechanism for synovitis. Associated meniscal tear or ligamentous laxity are not directly caused by osteoid osteoma. Concurrent septic arthritis is a separate condition and not directly related to the osteoid osteoma itself.
Question 51
A 15-year-old male presents with a several-month history of progressive right thigh pain, worse at night and partially relieved by NSAIDs. Initial radiographs show subtle cortical thickening. An MRI is performed to evaluate the extent of soft tissue involvement and periostitis. Which of the following imaging features would be most characteristic of an osteoid osteoma on T2-weighted MRI?
View Answer & Explanation
Correct Answer: B
Rationale: The provided clinical context for Fig. 8.6 states, "The MRI shows significant associated edema and adjacent periostitis." This is a classic MRI finding for osteoid osteoma, reflecting the inflammatory reaction around the nidus. Extensive fat suppression with central calcification is not the most specific T2-weighted MRI finding. Large soft tissue mass with heterogeneous enhancement, multiple fluid-fluid levels, and well-defined lobulated mass with low signal intensity are more characteristic of other bone tumors (e.g., sarcoma, aneurysmal bone cyst, fibroma, respectively).
Question 51
A 13-year-old female presents with chronic left index finger swelling and pain, particularly at night. Physical examination reveals localized swelling and tenderness over the proximal phalanx. Radiographs show cortical thickening and a small lucent lesion. What is the most appropriate imaging modality to definitively characterize the nidus and its relationship to the surrounding bone?
View Answer & Explanation
Correct Answer: C
Rationale: Computed Tomography (CT) is considered the gold standard for definitively characterizing the nidus of an osteoid osteoma, demonstrating its size, location, and the characteristic surrounding medullary sclerosis with high detail. While plain radiographs may show cortical thickening, they often miss the nidus. Ultrasound is not suitable for bone lesions. MRI is excellent for soft tissue edema and periostitis but may be less precise than CT for the nidus itself. Bone scintigraphy shows increased uptake but is not specific for diagnosis or detailed characterization.
Question 51
During surgical excision of an osteoid osteoma from the proximal femur of a 17-year-old male, the surgeon identifies the nidus. What gross appearance is typically expected for the nidus of an osteoid osteoma?

View Answer & Explanation
Correct Answer: C
Rationale: The provided clinical context for Fig. 8.9 explicitly states, "The nidus is typically 'cherry-red' on gross examination." This distinct color is due to its high vascularity. White, gritty, and sclerotic describes reactive bone. Soft, gelatinous, and yellowish, dark brown with hemorrhage, or cystic with clear fluid are not characteristic of an osteoid osteoma nidus.
Question 51
A biopsy is performed on a 14-year-old male with a suspected osteoid osteoma in the distal tibia. Microscopic evaluation of the nidus is crucial for diagnosis. Which of the following features is characteristic of an osteoid osteoma on microscopic examination?
View Answer & Explanation
Correct Answer: C
Rationale: The provided clinical context for Fig. 8.10 states, "Thin, irregular osteoid trabeculae are evident on microscopic evaluation. There is loose fibrovascular connective tissue between the trabeculae." This is the hallmark microscopic appearance of an osteoid osteoma. Sheets of atypical chondrocytes suggest chondrosarcoma. Spindle cells with nuclear pleomorphism suggest sarcoma. Large, multinucleated giant cells within a hemorrhagic stroma suggest giant cell tumor or aneurysmal bone cyst. Nests of epithelioid cells with clear cytoplasm are not characteristic of osteoid osteoma.
Question 51
A 16-year-old female undergoes biopsy for a suspected osteoid osteoma. Histopathological examination of the nidus is performed. What specific characteristic of the osteoblasts within the nidus helps distinguish it from more aggressive bone lesions?
View Answer & Explanation
Correct Answer: B
Rationale: The provided clinical context for Fig. 8.11 states, "Higher power examination shows osteoid with uniform osteoblasts without nuclear atypia." This benign cellular appearance is crucial for distinguishing osteoid osteoma from malignant bone tumors like osteosarcoma, which would show significant atypia and mitotic activity. Prominent nuclear atypia and mitotic activity would suggest malignancy. Spindle-shaped osteoblasts forming woven bone is too general. Osteoblasts exhibiting chondroid differentiation is not typical. Multinucleated osteoblasts are not a defining feature.
Question 51
A 13-year-old male presents with a 4-month history of worsening right proximal femur pain, particularly at night, which is only partially relieved by high doses of NSAIDs. Radiographs show cortical thickening, and a CT scan reveals a 1.2 cm lucent nidus with surrounding sclerosis. The patient's parents are concerned about the long-term use of NSAIDs. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: B
Rationale: Given the classic symptoms, imaging findings consistent with osteoid osteoma, and the patient's desire for more definitive treatment due to inadequate pain relief and concerns about long-term NSAID use, percutaneous radiofrequency ablation (RFA) is the most appropriate next step. It is a minimally invasive and highly effective treatment. Increasing NSAID dosage is not ideal given the concerns. An open biopsy is generally not needed if imaging is classic for osteoid osteoma. Immobilization is not a treatment for osteoid osteoma. While spontaneous resolution can occur, it can take years, and the patient is seeking more immediate relief.
Question 51
A 10-year-old boy presents with a 6-month history of progressive right leg length discrepancy and a painful limp. He reports chronic right hip pain, worse at night, which improves with ibuprofen. Radiographs show mild cortical thickening in the proximal femur. What is the most likely underlying cause of the leg length discrepancy in this patient?
View Answer & Explanation
Correct Answer: B
Rationale: Osteoid osteomas, particularly those located near growth plates, can cause chronic inflammation and hyperemia, which can stimulate local bone growth, leading to leg length discrepancy. This is a known, albeit less common, complication. Direct tumor invasion of the growth plate is not the primary mechanism. Muscle atrophy can occur but does not directly cause leg length discrepancy. Pathologic fracture is rare. Associated congenital anomaly is less likely given the classic pain pattern and response to NSAIDs.
Question 51
A 14-year-old male presents with a 5-month history of severe, throbbing pain in his left distal tibia, particularly at night. The pain is almost completely relieved by a single dose of naproxen. Physical examination is largely unremarkable, with only mild localized tenderness. What is the most likely mediator responsible for the characteristic pain associated with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The characteristic pain of osteoid osteoma, especially its nocturnal exacerbation and dramatic relief with NSAIDs, is primarily mediated by prostaglandins (PGE2) produced within the highly vascularized nidus. NSAIDs inhibit prostaglandin synthesis, thus alleviating the pain. While other mediators play roles in pain, prostaglandins are the key mediators targeted by NSAIDs in this context. Bradykinin, Substance P, Histamine, and Serotonin are general pain mediators but not as specifically implicated in the NSAID-responsive pain of osteoid osteoma.
Question 51
A 17-year-old male presents with a 7-month history of increasing right hip pain, worse with activity and at night, but only partially relieved by NSAIDs. Radiographs show subtle cortical thickening in the femoral neck. An MRI is ordered to evaluate for an osteoid osteoma. What is a potential pitfall in diagnosing an osteoid osteoma in an intra-articular location, such as the femoral neck?
View Answer & Explanation
Correct Answer: C
Rationale: Osteoid osteomas in an intra-articular location (e.g., femoral neck, talus) can present with joint pain, swelling, and synovitis, mimicking inflammatory arthritis or other joint pathologies, leading to delayed diagnosis. The case text mentions 10% have an intraarticular location. While surrounding sclerosis may be less pronounced in intra-articular lesions, a nidus is still present. A nidus is typically visible on MRI, though CT is better for characterization. Rapid malignant transformation is not a feature of osteoid osteoma. Biopsy is generally feasible, though challenging, in most locations.
Question 51
A 15-year-old male presents with chronic right distal femur pain, worse at night and relieved by NSAIDs. A CT scan confirms a juxtacortical osteoid osteoma with typical surrounding medullary sclerosis. The patient is considering treatment options. What is the typical size range of the nidus in an osteoid osteoma?
View Answer & Explanation
Correct Answer: A
Rationale: Osteoid osteomas are typically small lesions, with the nidus usually measuring less than 1.5-2 cm in diameter. This small size is a key distinguishing feature from osteoblastoma, which is generally larger (>2 cm). Options B, C, and D describe sizes more typical of osteoblastomas or other larger tumors. While variable, the defining characteristic is its small size, making "less than 2 cm" the most accurate description.
Question 51
A 12-year-old female presents with a 3-month history of left proximal tibia pain, worse at night and partially relieved by ibuprofen. Physical examination reveals mild localized swelling and tenderness. Radiographs show cortical thickening. What is the most common anatomical location for osteoid osteomas?
View Answer & Explanation
Correct Answer: C
Rationale: The case text states, "Most lesions occur in the meta- or diaphysis of the long bones (proximal femur and tibia)." This makes the meta- or diaphysis of long bones the most common anatomical location. While they can occur in other locations (e.g., spine, small bones), these are less common than the long bones.
Question 51
A 16-year-old male presents with a 6-month history of right distal femur pain, worse at night and relieved by NSAIDs. A CT scan shows a typical osteoid osteoma. The patient is concerned about the long-term prognosis if left untreated. What is the natural history of an untreated osteoid osteoma?
View Answer & Explanation
Correct Answer: B
Rationale: While symptoms can be debilitating, osteoid osteomas are benign lesions that can spontaneously resolve over several years, though this process can be prolonged. Therefore, observation with NSAIDs is a valid initial management strategy. They do not invariably progress to malignancy, continuously grow to cause pathologic fracture, transform into osteoblastoma, or cause chronic osteomyelitis.
Question 51
A 14-year-old male presents with a 7-month history of left proximal tibia pain, worse at night and relieved by NSAIDs. Physical examination reveals mild muscle atrophy in the left thigh. Radiographs show cortical thickening, and a CT scan confirms an osteoid osteoma. What is the most likely cause of the muscle atrophy in this patient?
View Answer & Explanation
Correct Answer: B
Rationale: The case text mentions that patients with osteoid osteoma can have "muscle atrophy, or spasm." This is typically a result of disuse atrophy due to chronic pain and guarding, where the patient subconsciously or consciously limits the use of the affected limb to avoid pain. Direct tumor invasion, neurological compression, systemic inflammation, or vascular compromise are not typical mechanisms for muscle atrophy in osteoid osteoma.
Question 51
A 12-year-old male presents with a 5-month history of right distal femur pain, worse at night and significantly relieved by ibuprofen. Radiographs show cortical thickening. A CT scan reveals a small lucent nidus with surrounding sclerosis. The patient's parents are concerned about the recurrence rate after treatment. Which treatment modality for osteoid osteoma is associated with the lowest recurrence rate?
View Answer & Explanation
Correct Answer: C
Rationale: Complete surgical excision of the nidus, when feasible, is associated with the lowest recurrence rate because it ensures the entire lesion is removed. Incomplete removal of the nidus, as might occur with curettage without complete nidus removal, is the primary reason for recurrence. While RFA and cryoablation are highly effective, complete surgical excision historically has the lowest recurrence if the nidus is fully removed. Intralesional steroid injection is not a definitive treatment. Observation with NSAIDs is not a definitive treatment and does not remove the lesion.
Question 51
A 15-year-old male presents with a 6-month history of right proximal tibia pain, worse at night and relieved by NSAIDs. Physical examination reveals mild localized swelling. Radiographs show cortical thickening. What is the most common age group affected by osteoid osteomas?
View Answer & Explanation
Correct Answer: C
Rationale: The case text explicitly states, "Osteoid osteomas are uniquely painful benign lesions that most commonly occur during adolescence." This makes adolescence (typically 10-20 years) the most common age group. While they can occur outside this range, it is less frequent.
Question 51
A 13-year-old male presents with a 4-month history of left distal femur pain, worse at night and significantly relieved by ibuprofen. Physical examination is unremarkable. Radiographs show cortical thickening. A CT scan confirms a small lucent nidus with surrounding medullary sclerosis. What is the typical gender predilection for osteoid osteomas?
View Answer & Explanation
Correct Answer: B
Rationale: The case text explicitly states, "Males are affected more commonly than females." This is a consistent epidemiological finding for osteoid osteomas. Therefore, males have a higher incidence than females. The other options are incorrect based on the provided text and general knowledge of osteoid osteoma epidemiology.
Question 52
A 14-year-old male presents with a 6-month history of worsening right distal thigh pain, particularly at night, which is significantly relieved by ibuprofen. Physical examination reveals mild tenderness over the distal femur. Radiographs show cortical thickening, and a subsequent CT scan confirms a small lucent nidus with surrounding medullary sclerosis in the distal femoral diaphysis.
View Answer & Explanation
Correct Answer: A
Rationale: For osteoid osteomas, especially in cases with classic symptoms well-controlled by NSAIDs, initial management often involves observation with continued NSAID use. While surgical or interventional options exist, many patients can manage their symptoms effectively with conservative measures, and some lesions may even spontaneously resolve over time. Open surgical excision is a definitive treatment but is more invasive than other options and not always the first choice if symptoms are well-controlled. Radiation and chemotherapy are not indicated for benign osteoid osteoma. Intralesional curettage with bone grafting is a surgical option but not the primary conservative approach.
Question 53
A 16-year-old male presents with a 9-month history of left proximal tibia pain, worse at night and partially relieved by over-the-counter analgesics. MRI shows significant associated edema and adjacent periostitis in the proximal tibia. A CT scan confirms a small cortical lesion with a central lucent nidus. The patient desires a more definitive treatment than continuous NSAID use due to side effects and incomplete pain relief.
View Answer & Explanation
Correct Answer: B
Rationale: Percutaneous radiofrequency ablation (RFA) is a highly effective and minimally invasive treatment for osteoid osteomas, offering excellent pain relief with low complication rates. It is often preferred over open surgery when conservative management fails or is not desired. Systemic corticosteroids are not a primary treatment for osteoid osteoma. External beam radiation is not indicated for this benign lesion. Wide en bloc resection is an overly aggressive procedure for a benign osteoid osteoma. Long-term opioid therapy is inappropriate given the availability of definitive treatments.
Question 54
A 12-year-old female presents with progressive scoliosis and chronic low back pain. Imaging reveals a small, lucent lesion with surrounding sclerosis in a lumbar vertebral pedicle. The pain is worse at night and partially responsive to NSAIDs. Given the location of the lesion, what is the most likely specific complication directly attributable to this osteoid osteoma?
View Answer & Explanation
Correct Answer: C
Rationale: Spinal lesions, particularly osteoid osteomas, can lead to painful scoliosis due to muscle spasm and asymmetric growth stimulation. The case text explicitly states, "spinal lesions can lead to painful scoliosis." While other complications can occur in the spine, painful scoliosis is a classic presentation for osteoid osteoma in this location. Pathologic fracture is rare for osteoid osteoma. Spinal cord compression is less common unless the lesion is very large or in a critical location. Malignant transformation is exceedingly rare for osteoid osteoma. Vertebral body collapse is not a typical complication of osteoid osteoma.
Question 55
A 10-year-old boy presents with chronic right knee pain, swelling, and a limp. Physical examination reveals a warm, swollen knee with a mild effusion. Radiographs are initially unremarkable, but an MRI shows synovitis and significant edema within the distal femur, adjacent to the joint. A subsequent CT scan identifies a small osteoid osteoma in the juxta-articular region of the distal femur. What is the most likely reason for the joint-related symptoms?
View Answer & Explanation
Correct Answer: B
Rationale: Osteoid osteomas, especially those in an intra-articular or juxta-articular location, can release prostaglandins and other inflammatory mediators, leading to synovitis, joint effusion, and associated joint pain. The case text mentions that 10% of lesions have an intraarticular location. Direct invasion of the joint capsule is not the primary mechanism for synovitis. Associated meniscal tear or ligamentous laxity are not directly caused by osteoid osteoma. Concurrent septic arthritis is a separate condition and not directly related to the osteoid osteoma itself.
Question 56
A 15-year-old male presents with a several-month history of progressive right thigh pain, worse at night and partially relieved by NSAIDs. Initial radiographs show subtle cortical thickening. An MRI is performed to evaluate the extent of soft tissue involvement and periostitis. Which of the following imaging features would be most characteristic of an osteoid osteoma on T2-weighted MRI?
View Answer & Explanation
Correct Answer: B
Rationale: The provided clinical context for Fig. 8.6 states, "The MRI shows significant associated edema and adjacent periostitis." This is a classic MRI finding for osteoid osteoma, reflecting the inflammatory reaction around the nidus. Extensive fat suppression with central calcification is not the most specific T2-weighted MRI finding. Large soft tissue mass with heterogeneous enhancement, multiple fluid-fluid levels, and well-defined lobulated mass with low signal intensity are more characteristic of other bone tumors (e.g., sarcoma, aneurysmal bone cyst, fibroma, respectively).
Question 57
A 13-year-old female presents with chronic left index finger swelling and pain, particularly at night. Physical examination reveals localized swelling and tenderness over the proximal phalanx. Radiographs show cortical thickening and a small lucent lesion. What is the most appropriate imaging modality to definitively characterize the nidus and its relationship to the surrounding bone?
View Answer & Explanation
Correct Answer: C
Rationale: Computed Tomography (CT) is considered the gold standard for definitively characterizing the nidus of an osteoid osteoma, demonstrating its size, location, and the characteristic surrounding medullary sclerosis with high detail. While plain radiographs may show cortical thickening, they often miss the nidus. Ultrasound is not suitable for bone lesions. MRI is excellent for soft tissue edema and periostitis but may be less precise than CT for the nidus itself. Bone scintigraphy shows increased uptake but is not specific for diagnosis or detailed characterization.
Question 58
During surgical excision of an osteoid osteoma from the proximal femur of a 17-year-old male, the surgeon identifies the nidus. What gross appearance is typically expected for the nidus of an osteoid osteoma?
View Answer & Explanation
Correct Answer: C
Rationale: The provided clinical context for Fig. 8.9 explicitly states, "The nidus is typically 'cherry-red' on gross examination." This distinct color is due to its high vascularity. White, gritty, and sclerotic describes reactive bone. Soft, gelatinous, and yellowish, dark brown with hemorrhage, or cystic with clear fluid are not characteristic of an osteoid osteoma nidus.
Question 59
A biopsy is performed on a 14-year-old male with a suspected osteoid osteoma in the distal tibia. Microscopic evaluation of the nidus is crucial for diagnosis. Which of the following features is characteristic of an osteoid osteoma on microscopic examination?
View Answer & Explanation
Correct Answer: C
Rationale: The provided clinical context for Fig. 8.10 states, "Thin, irregular osteoid trabeculae are evident on microscopic evaluation. There is loose fibrovascular connective tissue between the trabeculae." This is the hallmark microscopic appearance of an osteoid osteoma. Sheets of atypical chondrocytes suggest chondrosarcoma. Spindle cells with nuclear pleomorphism suggest sarcoma. Large, multinucleated giant cells within a hemorrhagic stroma suggest giant cell tumor or aneurysmal bone cyst. Nests of epithelioid cells with clear cytoplasm are not characteristic of osteoid osteoma.
Question 60
A 16-year-old female undergoes biopsy for a suspected osteoid osteoma. Histopathological examination of the nidus is performed. What specific characteristic of the osteoblasts within the nidus helps distinguish it from more aggressive bone lesions?
View Answer & Explanation
Correct Answer: B
Rationale: The provided clinical context for Fig. 8.11 states, "Higher power examination shows osteoid with uniform osteoblasts without nuclear atypia." This benign cellular appearance is crucial for distinguishing osteoid osteoma from malignant bone tumors like osteosarcoma, which would show significant atypia and mitotic activity. Prominent nuclear atypia and mitotic activity would suggest malignancy. Spindle-shaped osteoblasts forming woven bone is too general. Osteoblasts exhibiting chondroid differentiation is not typical. Multinucleated osteoblasts are not a defining feature.
Question 61
A 13-year-old male presents with a 4-month history of worsening right proximal femur pain, particularly at night, which is only partially relieved by high doses of NSAIDs. Radiographs show cortical thickening, and a CT scan reveals a 1.2 cm lucent nidus with surrounding sclerosis. The patient's parents are concerned about the long-term use of NSAIDs. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: B
Rationale: Given the classic symptoms, imaging findings consistent with osteoid osteoma, and the patient's desire for more definitive treatment due to inadequate pain relief and concerns about long-term NSAID use, percutaneous radiofrequency ablation (RFA) is the most appropriate next step. It is a minimally invasive and highly effective treatment. Increasing NSAID dosage is not ideal given the concerns. An open biopsy is generally not needed if imaging is classic for osteoid osteoma. Immobilization is not a treatment for osteoid osteoma. While spontaneous resolution can occur, it can take years, and the patient is seeking more immediate relief.
Question 62
A 10-year-old boy presents with a 6-month history of progressive right leg length discrepancy and a painful limp. He reports chronic right hip pain, worse at night, which improves with ibuprofen. Radiographs show mild cortical thickening in the proximal femur. What is the most likely underlying cause of the leg length discrepancy in this patient?
View Answer & Explanation
Correct Answer: B
Rationale: Osteoid osteomas, particularly those located near growth plates, can cause chronic inflammation and hyperemia, which can stimulate local bone growth, leading to leg length discrepancy. This is a known, albeit less common, complication. Direct tumor invasion of the growth plate is not the primary mechanism. Muscle atrophy can occur but does not directly cause leg length discrepancy. Pathologic fracture is rare. Associated congenital anomaly is less likely given the classic pain pattern and response to NSAIDs.
Question 63
A 14-year-old male presents with a 5-month history of severe, throbbing pain in his left distal tibia, particularly at night. The pain is almost completely relieved by a single dose of naproxen. Physical examination is largely unremarkable, with only mild localized tenderness. What is the most likely mediator responsible for the characteristic pain associated with this condition?
View Answer & Explanation
Correct Answer: C
Rationale: The characteristic pain of osteoid osteoma, especially its nocturnal exacerbation and dramatic relief with NSAIDs, is primarily mediated by prostaglandins (PGE2) produced within the highly vascularized nidus. NSAIDs inhibit prostaglandin synthesis, thus alleviating the pain. While other mediators play roles in pain, prostaglandins are the key mediators targeted by NSAIDs in this context. Bradykinin, Substance P, Histamine, and Serotonin are general pain mediators but not as specifically implicated in the NSAID-responsive pain of osteoid osteoma.
Question 64
A 17-year-old male presents with a 7-month history of increasing right hip pain, worse with activity and at night, but only partially relieved by NSAIDs. Radiographs show subtle cortical thickening in the femoral neck. An MRI is ordered to evaluate for an osteoid osteoma. What is a potential pitfall in diagnosing an osteoid osteoma in an intra-articular location, such as the femoral neck?
View Answer & Explanation
Correct Answer: C
Rationale: Osteoid osteomas in an intra-articular location (e.g., femoral neck, talus) can present with joint pain, swelling, and synovitis, mimicking inflammatory arthritis or other joint pathologies, leading to delayed diagnosis. The case text mentions 10% have an intraarticular location. While surrounding sclerosis may be less pronounced in intra-articular lesions, a nidus is still present. A nidus is typically visible on MRI, though CT is better for characterization. Rapid malignant transformation is not a feature of osteoid osteoma. Biopsy is generally feasible, though challenging, in most locations.
Question 65
A 15-year-old male presents with chronic right distal femur pain, worse at night and relieved by NSAIDs. A CT scan confirms a juxtacortical osteoid osteoma with typical surrounding medullary sclerosis. The patient is considering treatment options. What is the typical size range of the nidus in an osteoid osteoma?
View Answer & Explanation
Correct Answer: A
Rationale: Osteoid osteomas are typically small lesions, with the nidus usually measuring less than 1.5-2 cm in diameter. This small size is a key distinguishing feature from osteoblastoma, which is generally larger (>2 cm). Options B, C, and D describe sizes more typical of osteoblastomas or other larger tumors. While variable, the defining characteristic is its small size, making "less than 2 cm" the most accurate description.
Question 66
A 12-year-old female presents with a 3-month history of left proximal tibia pain, worse at night and partially relieved by ibuprofen. Physical examination reveals mild localized swelling and tenderness. Radiographs show cortical thickening. What is the most common anatomical location for osteoid osteomas?
View Answer & Explanation
Correct Answer: C
Rationale: The case text states, "Most lesions occur in the meta- or diaphysis of the long bones (proximal femur and tibia)." This makes the meta- or diaphysis of long bones the most common anatomical location. While they can occur in other locations (e.g., spine, small bones), these are less common than the long bones.
Question 67
A 16-year-old male presents with a 6-month history of right distal femur pain, worse at night and relieved by NSAIDs. A CT scan shows a typical osteoid osteoma. The patient is concerned about the long-term prognosis if left untreated. What is the natural history of an untreated osteoid osteoma?
View Answer & Explanation
Correct Answer: B
Rationale: While symptoms can be debilitating, osteoid osteomas are benign lesions that can spontaneously resolve over several years, though this process can be prolonged. Therefore, observation with NSAIDs is a valid initial management strategy. They do not invariably progress to malignancy, continuously grow to cause pathologic fracture, transform into osteoblastoma, or cause chronic osteomyelitis.
Question 68
A 14-year-old male presents with a 7-month history of left proximal tibia pain, worse at night and relieved by NSAIDs. Physical examination reveals mild muscle atrophy in the left thigh. Radiographs show cortical thickening, and a CT scan confirms an osteoid osteoma. What is the most likely cause of the muscle atrophy in this patient?
View Answer & Explanation
Correct Answer: B
Rationale: The case text mentions that patients with osteoid osteoma can have "muscle atrophy, or spasm." This is typically a result of disuse atrophy due to chronic pain and guarding, where the patient subconsciously or consciously limits the use of the affected limb to avoid pain. Direct tumor invasion, neurological compression, systemic inflammation, or vascular compromise are not typical mechanisms for muscle atrophy in osteoid osteoma.
Question 69
A 12-year-old male presents with a 5-month history of right distal femur pain, worse at night and significantly relieved by ibuprofen. Radiographs show cortical thickening. A CT scan reveals a small lucent nidus with surrounding sclerosis. The patient's parents are concerned about the recurrence rate after treatment. Which treatment modality for osteoid osteoma is associated with the lowest recurrence rate?
View Answer & Explanation
Correct Answer: C
Rationale: Complete surgical excision of the nidus, when feasible, is associated with the lowest recurrence rate because it ensures the entire lesion is removed. Incomplete removal of the nidus, as might occur with curettage without complete nidus removal, is the primary reason for recurrence. While RFA and cryoablation are highly effective, complete surgical excision historically has the lowest recurrence if the nidus is fully removed. Intralesional steroid injection is not a definitive treatment. Observation with NSAIDs is not a definitive treatment and does not remove the lesion.
Question 70
A 15-year-old male presents with a 6-month history of right proximal tibia pain, worse at night and relieved by NSAIDs. Physical examination reveals mild localized swelling. Radiographs show cortical thickening. What is the most common age group affected by osteoid osteomas?
View Answer & Explanation
Correct Answer: C
Rationale: The case text explicitly states, "Osteoid osteomas are uniquely painful benign lesions that most commonly occur during adolescence." This makes adolescence (typically 10-20 years) the most common age group. While they can occur outside this range, it is less frequent.
Question 71
A 45-year-old male presents with a slowly growing, painless, soft, mobile mass on his posterior neck for the past 3 years. On examination, the mass is subcutaneous, non-tender, and feels rubbery. There are no overlying skin changes. Radiographs are unremarkable. MRI shows a well-circumscribed lesion with signal intensity identical to subcutaneous fat on all sequences, which suppresses with fat-saturation techniques.
View Answer & Explanation
Correct Answer: D
Rationale: The clinical presentation of a slowly growing, painless, soft, mobile, subcutaneous mass, combined with MRI findings of a well-circumscribed lesion with signal intensity identical to subcutaneous fat that suppresses with fat-saturation, is classic for a lipoma. Lipomas are benign tumors composed of mature adipocytes. The main distractor, liposarcoma, typically presents with more rapid growth, deep location, larger size (>5 cm), and often heterogeneous signal on MRI with non-fat components.
Question 72
A 62-year-old female presents with a 7 cm, soft, non-tender mass in her right thigh that has been present for several years. It is mobile relative to deep structures. She is concerned about its cosmetic appearance. What is the most common histological finding in this lesion?
View Answer & Explanation
Correct Answer: C
Rationale: Lipomas are benign tumors composed of mature fat cells (adipocytes) that are histologically indistinguishable from normal fat, except for being encapsulated. The nuclei are typically uniform and small. Atypical lipoblasts with hyperchromatic nuclei (A) are characteristic of liposarcoma, which is the main distractor and represents a malignant lesion.
Question 73
A 38-year-old male presents with a 4 cm, soft, mobile mass on his left forearm that has been present for 2 years. It is painless and causes no functional limitations. He is otherwise healthy. What is the most appropriate initial management for this lesion?
View Answer & Explanation
Correct Answer: C
Rationale: For a classic presentation of a lipoma (painless, soft, mobile, subcutaneous, small size) in a benign location, observation and reassurance are often the most appropriate initial management. Surgical excision is typically reserved for symptomatic lesions, cosmetic concerns, or if there is diagnostic uncertainty. Immediate surgical excision (A) is generally not indicated for asymptomatic, classic lipomas, making it the main distractor.
Question 74
A 55-year-old female presents with a 6 cm, firm, slightly tender mass located deep within the musculature of her right posterior thigh. It has grown noticeably over the past 6 months. MRI shows a heterogeneous mass with some fat signal, but also non-fat components and areas of enhancement. What is the most appropriate next step in management?
View Answer & Explanation
Correct Answer: C
Rationale: The clinical presentation (deep, firm, growing, tender, >5 cm) and MRI findings (heterogeneous, non-fat components, enhancement) are concerning for a malignant lesion, such as a liposarcoma, despite some fat signal. In such cases, a core needle biopsy is essential to establish a definitive diagnosis before definitive surgical planning. Reassurance and observation (A) would be inappropriate given the concerning features, making it the main distractor.
Question 75
Which of the following is NOT a typical characteristic of a benign lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: Benign lipomas typically exhibit slow growth over years, or remain stable in size. Rapid growth over weeks to months is a red flag that suggests a more aggressive lesion, such as a liposarcoma, and warrants further investigation. The other options (soft consistency, mobility, well-circumscribed, painless) are all characteristic features of benign lipomas.
Question 76
A 70-year-old male presents with multiple, painful, subcutaneous nodules distributed symmetrically on his trunk and extremities. He reports a family history of similar lesions. Physical examination reveals numerous tender, mobile masses ranging from 1 to 5 cm. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Dercum's disease, also known as adiposis dolorosa, is characterized by multiple, painful lipomas, often symmetrically distributed, and can have a familial component. Multiple symmetric lipomatosis (D) involves large, unencapsulated fat masses, typically in the head, neck, and shoulders, but is usually painless. Familial multiple lipomatosis (E) involves multiple, painless lipomas. The presence of pain is key here, making Dercum's disease the most likely. Neurofibromatosis Type 1 (A) involves neurofibromas, not primarily lipomas. Gardner's syndrome (C) involves osteomas, colon polyps, and desmoid tumors, not typically painful lipomas.
Question 77
A 50-year-old male undergoes excision of a 3 cm subcutaneous mass from his back. Histopathological examination reveals mature adipocytes with a prominent vascular component, including numerous thin-walled, branching capillaries. What is the most likely variant of lipoma?
View Answer & Explanation
Correct Answer: A
Rationale: Angiolipoma is a variant of lipoma characterized by the presence of mature adipocytes and a significant vascular component, typically composed of numerous small blood vessels. These are often painful. Spindle cell lipoma (B) contains spindle-shaped cells in a myxoid stroma. Pleomorphic lipoma (C) contains bizarre, hyperchromatic giant cells. Myxolipoma (D) has a prominent myxoid stroma. Hibernoma (E) is a tumor of brown fat.
Question 78
A 40-year-old female presents with a 5 cm, soft, mobile mass on her anterior thigh. She is concerned about its cosmetic appearance. What is the most common complication associated with surgical excision of a lipoma?
View Answer & Explanation
Correct Answer: D
Rationale: Hematoma and seroma formation are the most common complications following surgical excision of lipomas, especially larger ones, due to the potential for dead space and disruption of small vessels. While infection (C) and nerve injury (B) can occur, they are less frequent. Recurrence (E) is rare if the lipoma is completely excised. Malignant transformation (A) of a benign lipoma is exceedingly rare and controversial.
Question 79
A 58-year-old male has a 10 cm, deep-seated, firm mass in his gluteal region. MRI shows a large, predominantly fatty mass with several thick septa and a few nodular, non-fatty components that enhance after contrast. What is the most appropriate diagnostic procedure?
View Answer & Explanation
Correct Answer: D
Rationale: The size (>5 cm), deep location, firmness, and MRI features (thick septa, non-fatty enhancing components) are highly suspicious for a well-differentiated liposarcoma. A core needle biopsy is the preferred diagnostic procedure for such lesions as it provides sufficient tissue for accurate histological diagnosis and grading, which is crucial for treatment planning. FNA (A) often yields insufficient tissue for definitive diagnosis of sarcomas. Incisional (B) or excisional (C) biopsies are generally avoided for large, deep, potentially malignant lesions due to the risk of tumor seeding and complicating future definitive surgery. Observation (E) is inappropriate given the concerning features.
Question 80
Which of the following features on MRI is most concerning for a liposarcoma rather than a benign lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: The presence of thick septa (>2 mm), nodular non-fatty components, and prominent enhancement are MRI features that strongly suggest a liposarcoma, particularly a well-differentiated liposarcoma, rather than a benign lipoma. Well-circumscribed margins (A), signal intensity identical to subcutaneous fat (B), and subcutaneous location (E) are typical of benign lipomas. Absence of internal vascularity (D) would be less concerning for malignancy.
Question 81
A 25-year-old male presents with a 2 cm, firm, non-tender mass on his posterior neck. It is mobile and appears to be within the subcutaneous tissue. He is concerned about its nature. Which of the following is the least likely differential diagnosis for this lesion?
View Answer & Explanation
Correct Answer: E
Rationale: Basal cell carcinoma is a skin cancer that typically presents as a pearly nodule with rolled borders, often with telangiectasias, and is usually superficial, not a mobile subcutaneous mass. While it's a skin lesion, its typical presentation is distinct from a mobile subcutaneous mass. Epidermoid cysts (A), dermatofibromas (B), lipomas (C), and even an enlarged lymph node (D) could present as a firm, mobile subcutaneous mass, making them more plausible differential diagnoses.
Question 82
A 48-year-old female has a 3 cm, soft, mobile mass on her shoulder. She reports that it occasionally feels "heavy" or "pulling" when she moves her arm in certain ways, but it is not painful at rest. She requests removal. What is the primary indication for surgical excision in this case?
View Answer & Explanation
Correct Answer: C
Rationale: For a classic lipoma, the primary indications for surgical excision are cosmetic concerns, mild symptoms (such as the "heavy" or "pulling" sensation described), or if there is diagnostic uncertainty. Risk of malignant transformation (A) is exceedingly rare for benign lipomas. Rapid growth (B) would be a red flag for malignancy, not a benign lipoma. Deep location (D) would raise suspicion for malignancy and warrant biopsy, not just excision for symptoms. Uncertainty of diagnosis (E) is a valid indication, but the vignette implies a classic lipoma with mild symptoms/cosmetic concern.
Question 83
Which of the following statements regarding lipomas is FALSE?
View Answer & Explanation
Correct Answer: D
Rationale: Lipomas are benign tumors and do not metastasize. Metastasis is a characteristic of malignant tumors. The other statements are true: lipomas are the most common benign soft tissue tumors (A), are typically encapsulated (B), can occur anywhere fat is present (C), and are composed of mature adipocytes (E).
Question 84
A 60-year-old male presents with a 5 cm, soft, mobile mass on his back. He has a history of multiple similar lesions. He is concerned about the possibility of malignancy. Which of the following factors is LEAST likely to suggest malignancy in this patient?
View Answer & Explanation
Correct Answer: D
Rationale: A soft, mobile consistency is characteristic of a benign lipoma and is generally reassuring. Conversely, rapid increase in size (A), deep location (B), pain or tenderness (C), and firm or hard consistency (E) are all "red flags" that should raise suspicion for malignancy (e.g., liposarcoma) and warrant further investigation. Therefore, soft, mobile consistency is the least likely to suggest malignancy.
Question 85
A 35-year-old female has a 3 cm, painless, subcutaneous mass on her posterior arm. Ultrasound shows a well-defined, ovoid, hyperechoic lesion with posterior acoustic enhancement, consistent with a lipoma. She is anxious and requests removal. What is the most important principle for surgical excision of a lipoma?
View Answer & Explanation
Correct Answer: B
Rationale: For a benign, well-circumscribed lipoma, the most important principle for surgical excision is complete enucleation of the encapsulated mass, often through a small incision, to minimize scarring and complications. Wide margins (A) are reserved for malignant tumors. Adjuvant radiation (C), lymph node dissection (D), and preoperative chemotherapy (E) are treatments for malignant tumors and are not indicated for benign lipomas.
Question 86
A 52-year-old male presents with a 4 cm, soft, mobile mass on his anterior chest wall. He has a history of obesity and hyperlipidemia. What is the most common location for a lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: The vast majority of lipomas (approximately 95%) are subcutaneous, meaning they are located just beneath the skin. While lipomas can occur in deeper locations such as intramuscular (A), retroperitoneal (B), intraosseous (D), or mediastinal (E), these are far less common.
Question 87
A 40-year-old male presents with a 3 cm, firm, non-tender mass on his back. Histology after excision shows mature adipocytes mixed with spindle cells and ropey collagen. What is the most likely diagnosis?
View Answer & Explanation
Correct Answer: B
Rationale: Spindle cell lipoma is a benign variant characterized by a mixture of mature adipocytes, spindle cells, and ropey collagen bundles, often with a myxoid background. It typically occurs in the posterior neck, shoulder, or back of older men. Conventional lipoma (A) would primarily show mature adipocytes. Pleomorphic lipoma (C) would show bizarre giant cells. Liposarcoma (D) would show atypical lipoblasts. Fibrolipoma (E) is a lipoma with a significant fibrous component, but not typically spindle cells.
Question 88
A 65-year-old female presents with a 2 cm, soft, mobile mass on her anterior forearm. She is concerned about its nature. Which imaging modality is generally NOT required for the diagnosis of a typical subcutaneous lipoma?
View Answer & Explanation
Correct Answer: D
Rationale: For a typical, superficial, soft, mobile lipoma, a CT scan is generally not required and exposes the patient to unnecessary radiation. Clinical examination alone (E) is often sufficient for diagnosis. Ultrasound (B) can confirm the fatty nature and rule out cystic lesions. MRI (C) is useful for larger, deeper, or atypical lesions to differentiate from liposarcoma, but not typically for small, superficial, classic lipomas. Plain radiographs (A) are usually unremarkable for soft tissue lesions but may be done to rule out bony involvement.
Question 89
A 42-year-old male presents with a 6 cm, soft, mobile mass on his left upper arm. He states it has been present for "many years" and has not changed significantly in size. He is concerned about its potential to become cancerous. What is the approximate risk of malignant transformation of a benign lipoma?
View Answer & Explanation
Correct Answer: D
Rationale: The malignant transformation of a benign lipoma into a liposarcoma is exceedingly rare, with an estimated risk of less than 0.1%, and some experts even question if it truly occurs or if the initial diagnosis was simply incorrect (i.e., it was a well-differentiated liposarcoma from the start). The other options represent significantly higher risks that are not applicable to benign lipomas.
Question 90
A 55-year-old female presents with a 7 cm, soft, mobile mass on her posterior thigh. She is otherwise healthy. Which of the following conditions is NOT typically associated with multiple lipomas?
View Answer & Explanation
Correct Answer: E
Rationale: Tuberous Sclerosis is a genetic disorder characterized by the growth of benign tumors in the brain, kidneys, heart, eyes, lungs, and skin (e.g., angiofibromas, shagreen patches), but it is not typically associated with multiple lipomas. Familial multiple lipomatosis (A), Dercum's disease (B), and Madelung's disease (C) are all conditions specifically characterized by the presence of multiple lipomas. Neurofibromatosis Type 1 (D) is associated with neurofibromas, but lipomas can also occur more frequently in these patients than in the general population, though not as a primary feature of the syndrome.
Question 91
A 48-year-old male presents with a slowly growing, soft tissue mass on his posterior neck that he noticed approximately 2 years ago. He denies any pain, tenderness, or functional limitation. On physical examination, the mass is subcutaneous, soft, mobile, and non-tender to palpation.
View Answer & Explanation
Correct Answer: E
Rationale: Lipomas are benign tumors of mature adipocytes, and their most characteristic clinical presentation is a painless, soft, mobile, and non-tender subcutaneous mass. Rapid growth, firmness, fixation, pain, or pulsatility are atypical for a simple lipoma and should raise suspicion for other diagnoses, including malignancy. The main distractor, "A) Rapidly growing," is incorrect because lipomas typically grow slowly over years. Rapid growth is a red flag for potential malignancy.
Question 92
A 55-year-old female presents with a 4 cm subcutaneous mass on her anterior thigh. She reports it has been present for several years and is asymptomatic. On physical examination, the mass is palpable, soft, and easily moves beneath the skin but not with the underlying muscle. When pressed, it tends to slip out from under the examining fingers.
View Answer & Explanation
Correct Answer: C
Rationale: The "slip sign" (or "gliding sign") is a classic physical examination finding for a lipoma, where the mass easily slips away from the examining fingers due to its soft, mobile nature and lack of adherence to deeper structures. Fixedness, tenderness, discoloration, warmth, or erythema are not typical for a simple lipoma and may suggest other pathologies. The main distractor, "A) Fixed to underlying fascia," is incorrect as lipomas are typically mobile and not fixed to deeper structures. Fixation would be concerning for malignancy or a different type of tumor.
Question 93
A 62-year-old male presents with a 6 cm, soft, mobile, non-tender mass in his upper arm. The clinical diagnosis of lipoma is suspected, but the patient requests imaging for confirmation and surgical planning. Which imaging modality is generally considered the most appropriate initial study for evaluating a suspected lipoma, especially for surgical planning or if there is diagnostic uncertainty?
View Answer & Explanation
Correct Answer: D
Rationale: Ultrasound is often the most appropriate initial imaging modality for a suspected superficial lipoma. It is readily available, inexpensive, non-ionizing, and can confirm the fatty nature of the mass (hyperechoic, compressible, often with linear echogenic striations), differentiate it from cysts or solid tumors, and assess its relationship to adjacent structures. While MRI provides excellent soft tissue detail, ultrasound is often sufficient for initial evaluation of typical superficial lipomas. MRI is preferred for deep-seated or large masses, or when malignancy is suspected. The main distractor, "C) Magnetic Resonance Imaging (MRI)," is also a good option for soft tissue masses, especially for deep or large ones. However, for a typical superficial lipoma, ultrasound is often sufficient as a first-line imaging study due to its cost-effectiveness and ability to confirm the diagnosis without radiation.
Question 94
A 50-year-old female undergoes an MRI for a suspected lipoma in her posterior thigh. The radiologist describes a well-circumscribed mass with signal characteristics identical to subcutaneous fat. Which of the following MRI findings is most characteristic of a simple lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: A simple lipoma typically appears hyperintense (bright) on T1-weighted MRI images, reflecting its fatty composition. Crucially, this signal will suppress (become dark) on fat-saturated sequences (e.g., STIR or fat-suppressed T2-weighted images), confirming its fatty nature. Lack of significant enhancement and homogeneity are also characteristic. The main distractor, "B) Hyperintense on T2-weighted images with fat suppression," is incorrect because if it's a simple lipoma, the fat signal should suppress on fat-saturated sequences, meaning it would appear hypointense (dark) on such images, not hyperintense.
Question 95
A 38-year-old male presents with a 7 cm, deep-seated, soft tissue mass in his gluteal region. While a lipoma is suspected, the size and depth raise concern. Which of the following is the most critical differential diagnosis to consider and exclude when evaluating a deep-seated fatty mass?
View Answer & Explanation
Correct Answer: D
Rationale: The most critical differential diagnosis for any fatty soft tissue mass, especially one that is large (>5 cm) or deep-seated, is liposarcoma. Liposarcomas are malignant tumors that can mimic lipomas clinically and radiographically, particularly well-differentiated liposarcomas. Distinguishing between them often requires imaging (MRI with contrast) and biopsy. The main distractor, "A) Sebaceous cyst," is incorrect because sebaceous cysts are typically superficial, epidermal lesions with different imaging characteristics and are easily distinguished from deep-seated fatty masses.
Question 96
A 68-year-old patient has a known 5 cm lipoma on their back. It has been stable for years, but recently the patient reports it has started to grow noticeably and is causing some discomfort when leaning against a chair. Which of the following is the primary indication for surgical excision of a lipoma?
View Answer & Explanation
Correct Answer: C
Rationale: While cosmetic concern, patient request, and size can be reasons for excision, the primary indication that raises clinical concern and necessitates intervention is rapid growth, pain, or any change in the character of the mass (e.g., firmness, fixation). These features may suggest a diagnosis other than a simple lipoma, such as a liposarcoma, and warrant further investigation and often excision. The main distractor, "A) Cosmetic concern," is a common reason for excision but not the primary medical indication that mandates intervention due to potential pathology.
Question 97
A 42-year-old male undergoes excision of a 3 cm subcutaneous mass from his shoulder. Histopathological examination is performed. Which of the following is the characteristic microscopic finding of a simple lipoma?
View Answer & Explanation
Correct Answer: B
Rationale: A simple lipoma is histologically characterized by a proliferation of mature, univacuolated adipocytes that are indistinguishable from normal fat cells, typically surrounded by a thin fibrous capsule. The nuclei are uniform and small, pushed to the periphery by the large lipid vacuole. The main distractor, "C) Pleomorphic lipoblasts with hyperchromatic nuclei," describes features characteristic of a liposarcoma, specifically pleomorphic liposarcoma, which indicates malignancy.
Question 98
A 35-year-old female presents with a small, tender, subcutaneous nodule on her forearm that has been present for several months. Unlike typical lipomas, this mass is consistently painful, especially with pressure. Imaging confirms a fatty lesion. Which specific variant of lipoma is most commonly associated with pain?
View Answer & Explanation
Correct Answer: C
Rationale: Angiolipoma is a distinct variant of lipoma characterized by the presence of mature adipocytes mixed with numerous small blood vessels. These lesions are often painful or tender, which is a key distinguishing feature from typical lipomas. The pain is thought to be due to the vascular proliferation and potential thrombosis within the vessels. The main distractor, "A) Spindle cell lipoma," is incorrect. Spindle cell lipomas are typically painless and often found in the posterior neck, shoulder, or back of older men.
Question 99
A 58-year-old male has an MRI of a 9 cm, deep-seated fatty mass in his thigh. The report describes the mass as predominantly fatty but notes the presence of thick internal septations, a few non-fatty nodules, and areas of contrast enhancement. Which of these MRI features is most concerning for differentiating a lipoma from a well-differentiated liposarcoma?
View Answer & Explanation
Correct Answer: C
Rationale: While large size (>5 cm) and deep location are risk factors for malignancy, the most specific MRI features that help differentiate a well-differentiated liposarcoma from a benign lipoma are the presence of thick internal septations (>2mm), nodular non-fatty components, and areas of contrast enhancement within these non-fatty components. Simple lipomas are typically homogeneous, thin-septated (if at all), and do not enhance significantly. The main distractor, "A) Size greater than 5 cm," is a risk factor for malignancy and warrants further investigation, but it is not as specific as the internal architectural features (thick septations, non-fatty nodules, enhancement) for differentiating between a benign lipoma and a well-differentiated liposarcoma.
Question 100
A 40-year-old patient undergoes surgical excision of a lipoma from the back. Six months later, the patient notices a new, similar-appearing mass developing at the site of the previous excision. What is the most common reason for recurrence of a lipoma after surgical removal?
View Answer & Explanation
Correct Answer: B
Rationale: The most common reason for recurrence of a lipoma after excision is incomplete removal of the original lesion. While lipomas are typically well-encapsulated, especially intramuscular or infiltrating lipomas can have ill-defined borders, making complete excision challenging. True malignant transformation of a benign lipoma is exceedingly rare. The main distractor, "A) Malignant transformation of residual cells," is incorrect. Malignant transformation of a benign lipoma is extremely rare. Recurrence is almost always due to residual benign tissue.
