Lower Back Pain and Disorders of Intervertebral Discs: A Comprehensive Surgical Guide
Key Takeaway
Intervertebral disc disorders and lower back pain represent a profound clinical and socioeconomic challenge in orthopaedics. This comprehensive guide details the pathophysiology, biomechanics, and evidence-based surgical management of disc degeneration and herniation. Emphasizing precise patient selection, it covers diagnostic modalities, nonoperative interventions, and advanced operative techniques—including microdiscectomy and spinal fusion—equipping orthopedic surgeons with the critical knowledge required to optimize patient outcomes and navigate complex spinal pathologies.
Overview of Disc Degeneration and Herniation
By any epidemiological or economic measure, intervertebral disc disorders represent a monumental challenge in modern orthopaedics. Musculoskeletal conditions in the United States incur costs exceeding $254 billion annually. While rarely fatal, these conditions are overwhelmingly chronic, with musculoskeletal injuries remaining the primary driver for physician visits. Axial spine pain—whether cervical, thoracic, or lumbar—is the most frequent musculoskeletal complaint and is frequently, though sometimes erroneously, attributed to disc degeneration.
It is paramount for the practicing orthopedic surgeon to distinguish between age-related disc degeneration, internal disc derangement (IDD), and frank disc herniation. Each of these pathological entities presents with unique clinical findings, biomechanical alterations, and therapeutic indications.
The Genetic and Pathophysiological Basis
The understanding of disc degeneration has undergone a significant transformation, shifting from a purely mechanical "wear-and-tear" model to a complex interplay of genetics, biochemistry, and biomechanics. The genetic influence on disc degeneration is profound, driven by multiple gene loci. Specific variations in the aggrecan gene, matrix metalloproteinase-3 (MMP-3) gene, and genes encoding collagen type IX (alpha 2 and 3 forms) have been definitively associated with disc pathology. These genetic polymorphisms alter the structural integrity of the annulus fibrosus and the hydrophilic properties of the nucleus pulposus, predisposing the functional spinal unit to premature desiccation and mechanical failure.
CLINICAL PEARL:
Do not conflate "disc degeneration" with "degenerative disc disease." Degeneration is a ubiquitous, often asymptomatic physiological process of aging. The term "disease" should be strictly reserved for degeneration that is unequivocally symptomatic and functionally limiting.
Socioeconomic Impact and the Psychosocial Axis
The socioeconomic burden of low back pain is staggering, with total costs in the United States exceeding $100 billion per year. Notably, only one-third of this figure represents direct medical costs; the remainder stems from decreased productivity, lost wages, and absenteeism. A mere 5% of patients account for 75% of these costs.
Return-to-work statistics dictate the urgency of early, effective intervention. Approximately 90% of patients return to work within three months. However, if a patient remains off work for six months, the probability of returning drops to 50%; at one year, it plummets to 25%.
Furthermore, the seminal work by Boos et al. demonstrated that nonanatomical factors—specifically work perception, job dissatisfaction, and psychosocial distress—are intimately intertwined with physical complaints. Socioeconomic factors, low educational attainment, and workers' compensation status are powerful predictors of prolonged disability, highlighting the necessity of a biopsychosocial approach to patient evaluation.
Biomechanics of the Intervertebral Disc
The intervertebral disc is a complex, avascular structure designed to transmit loads and provide flexibility to the spinal column. It consists of three distinct components:
1. Nucleus Pulposus: A gelatinous core rich in proteoglycans and type II collagen, designed to resist compressive forces via hydrostatic pressure.
2. Annulus Fibrosus: Concentric lamellae of type I collagen that resist tensile and torsional forces.
3. Cartilaginous Endplates: Hyaline cartilage layers that anchor the disc to the adjacent vertebral bodies and facilitate the diffusion of nutrients.
In the degenerative cascade (as described by Kirkaldy-Willis), the nucleus loses its proteoglycan content, leading to desiccation and a loss of hydrostatic pressure. Compressive loads are subsequently transferred directly to the annulus fibrosus, causing delamination, annular tears, and eventual herniation of nuclear material. This mechanical shift also overloads the posterior elements, leading to facet joint hypertrophy, ligamentum flavum buckling, and secondary spinal stenosis.
Clinical Evaluation and Diagnostic Modalities
Signs and Symptoms
The association of back and leg pain with the sciatic nerve dates back to the 18th century (Cotugno). The clinical examination must meticulously differentiate axial back pain from radiculopathy. The Lasègue sign (straight leg raise), described by Forst in 1881, remains a cornerstone provocative test for lumbar radiculopathy, specifically assessing L4, L5, and S1 nerve root tension.
Diagnostic Imaging
SURGICAL WARNING:
Advanced imaging must always be correlated with clinical findings. Magnetic Resonance Imaging (MRI) reveals significant abnormalities (e.g., disc bulges, protrusions) in up to 76% of completely asymptomatic individuals. Operating on an MRI finding rather than a clinical syndrome is the primary driver of Failed Back Surgery Syndrome (FBSS).
- Radiography: Weight-bearing anteroposterior, lateral, and dynamic flexion-extension views are essential to assess overall alignment, disc height loss, and segmental instability.
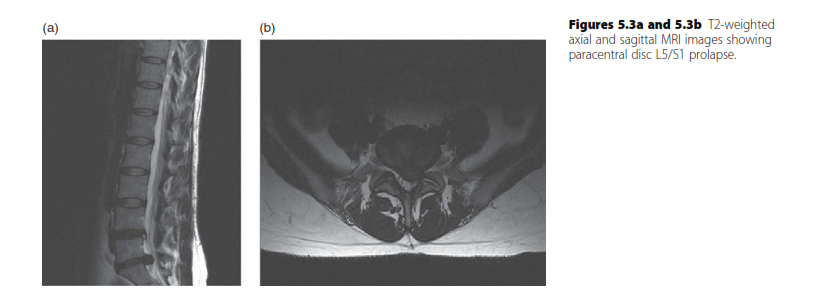
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating soft tissue, neural elements, and disc hydration (T2-weighted sequences).
- Computed Tomography (CT) Myelography: Reserved for patients with contraindications to MRI (e.g., pacemakers) or those with complex revision anatomy where metallic artifact obscures MRI interpretation.
Injection Studies and Discography
When noninvasive imaging is equivocal, diagnostic injections serve as critical adjuncts:
* Epidural Steroid Injections (ESIs): Provide both diagnostic information and therapeutic relief for radicular pain.
* Zygapophyseal (Facet) Joint Injections: Popularized by Mooney and Robertson, these intra-articular injections or medial branch blocks isolate pain originating from the posterior column.
* Discography: A provocative test used to identify internal disc derangement. Concordant pain reproduction upon pressurization of the disc space, coupled with post-discography CT to visualize annular tears, can guide fusion or arthroplasty decisions, though its use remains controversial.
Operative Treatment: Lumbar Microdiscectomy
The standard procedure for disc removal has evolved significantly since Semmes presented the subtotal laminectomy in 1939. Today, microscopic and endoscopic techniques (popularized by Kambin, Onik, and Helms) represent the gold standard for symptomatic lumbar disc herniation.
Indications
- Absolute: Cauda equina syndrome, progressive motor deficit (e.g., foot drop).
- Relative: Intractable radicular pain failing a minimum of 6 weeks of comprehensive conservative management (NSAIDs, physical therapy, ESIs), with concordant MRI findings.
Patient Positioning
Proper positioning is critical to minimize epidural venous bleeding and facilitate exposure.
* The patient is placed prone on a radiolucent spinal frame (e.g., Jackson table, Andrews frame, or Wilson frame).
* The abdomen must hang completely free. Any abdominal compression increases intra-abdominal pressure, which translates to the epidural venous plexus (Batson's plexus), resulting in excessive intraoperative hemorrhage.
* The hips and knees are flexed to reduce lumbar lordosis, opening the posterior interlaminar space.
Surgical Approach: Step-by-Step
- Incision and Exposure: A 2-3 cm midline incision is made centered over the target interspace, confirmed via intraoperative fluoroscopy. The lumbodorsal fascia is incised unilaterally.
- Subperiosteal Dissection: The paraspinal muscles are elevated off the spinous process and lamina using a Cobb elevator. A self-retaining retractor (e.g., Taylor or McCulloch) is placed.
- Laminotomy and Flavectomy: Using a high-speed burr or Kerrison rongeurs, a partial hemilaminotomy is performed. The ligamentum flavum is identified, detached from its bony insertions using a curette, and excised to expose the epidural space.
- Neural Retraction: The epidural fat is gently mobilized. The traversing nerve root is identified and carefully retracted medially using a Love nerve root retractor.
- Discectomy: The herniated disc fragment is identified. If the fragment is subligamentous, a cruciate annulotomy is performed using a #11 blade. Pituitary rongeurs are used to extract the extruded nucleus pulposus.
- Decompression Confirmation: A Penfield dissector is passed along the nerve root into the neural foramen to ensure complete freedom from compression.
- Closure: The wound is irrigated copiously. The fascia is closed tightly with interrupted sutures to prevent muscle herniation, followed by subcutaneous and subcuticular closure.
PITFALL:
Over-aggressive exploration of the disc space can lead to penetration of the anterior annulus, risking catastrophic injury to the great vessels (aorta, inferior vena cava, or iliac vessels). Instruments should never be advanced blindly beyond the measured depth of the disc space.
Cervical and Thoracic Disc Disease
Cervical Disc Disease
Cervical disc herniations typically present with radiculopathy (e.g., C6 or C7 nerve root distribution) or myelopathy if the spinal cord is compressed.
* Operative Treatment: The Anterior Cervical Discectomy and Fusion (ACDF) remains the workhorse procedure. It allows direct decompression of the neural elements and restoration of disc height and lordosis.
* Cervical Disc Arthroplasty (CDA): In carefully selected patients without significant facet arthropathy or instability, CDA is an excellent alternative to ACDF, designed to preserve segmental motion and theoretically reduce adjacent segment disease.
Thoracic Disc Disease
Thoracic disc herniations are rare but potentially devastating due to the narrow thoracic spinal canal and the tenuous blood supply to the thoracic spinal cord.
* Signs and Symptoms: Axial back pain, band-like radicular chest pain, or progressive myelopathy.
* Operative Treatment: Posterior laminectomy alone is strictly contraindicated for central thoracic disc herniations due to the high risk of spinal cord injury during retraction. Operative approaches must be anterior (transthoracic) or posterolateral (costotransversectomy or transpedicular) to allow ventral decompression without cord manipulation.
Postoperative Protocols and Complications
Postoperative Rehabilitation
Modern spinal surgery emphasizes early mobilization. Patients undergoing microdiscectomy are typically mobilized on the day of surgery.
* Weeks 1-2: Walking program, avoidance of bending, lifting (>10 lbs), and twisting (BLT precautions).
* Weeks 3-6: Initiation of core stabilization exercises and neural mobilization.
* Months 2-3: Gradual return to heavy labor and high-impact sports, contingent upon symptom resolution and functional recovery.
Complications of Disc Excision
- Incidental Durotomy: Dural tears occur in approximately 3-5% of primary lumbar discectomies. They must be recognized intraoperatively and repaired primarily with 4-0 or 5-0 nonabsorbable sutures, often augmented with a dural sealant or free fat graft. Postoperatively, the patient may be kept flat for 24-48 hours to prevent cerebrospinal fluid (CSF) fistula formation.
- Recurrent Disc Herniation: Occurs in 5-10% of patients. Repeat microdiscectomy is often successful, though the presence of epidural fibrosis makes the dissection more hazardous.
- Discitis: Postoperative infection of the disc space is rare (<1%) but presents with severe, unrelenting back pain weeks after surgery. Diagnosis is confirmed via MRI and elevated inflammatory markers (ESR, CRP). Treatment requires prolonged intravenous antibiotics and, occasionally, surgical debridement and fusion.
Failed Spine Surgery and Future Directions
Despite technological advancements, the treatment of disc degeneration with or without herniation remains challenging. "Proper patient selection" is the ultimate determinant of surgical success. Operating on patients with profound psychosocial distress, secondary gain motives, or poorly localized axial pain without clear anatomical correlation inevitably leads to Failed Back Surgery Syndrome (FBSS).
Future advancements must pivot from merely developing new implants to better defining the underlying pathophysiological processes. Biomolecular therapies, stem cell injections, and gene therapy targeting the aggrecan and MMP-3 pathways hold promise for regenerating the intervertebral disc, potentially shifting the paradigm from mechanical salvage to biological restoration. Until reliable criteria for these biological diagnoses are established, the orthopedic surgeon must rely on meticulous clinical evaluation, strict adherence to surgical indications, and flawless operative technique to optimize patient outcomes.
You Might Also Like