Surgical Management of Ulnar Nerve Palsy: Tendon Transfers and Functional Restoration
Key Takeaway
Ulnar nerve palsy results in profound functional deficits, including diminished grip strength, weak key pinch, and characteristic clawing of the ulnar digits. Surgical restoration relies on strategic tendon transfers to rebalance the hand. Low ulnar nerve palsy requires addressing intrinsic minus clawing and adductor pollicis paralysis. High ulnar nerve palsy necessitates additional reconstruction for lost flexor digitorum profundus and flexor carpi ulnaris function to restore terminal digit flexion and wrist stability.
Introduction to Ulnar Nerve Palsy
The ulnar nerve is frequently referred to as the "nerve of fine movements," providing the critical motor innervation required for power grip, key pinch, and synchronized digital kinematics. Ulnar nerve palsy presents a complex reconstructive challenge for the orthopaedic hand surgeon. The resulting imbalance between the intact extrinsic musculature and the paralyzed intrinsic musculature leads to predictable, debilitating deformities.
Surgical management is dictated by the level of the lesion. Low ulnar nerve palsy (distal to the innervation of the flexor digitorum profundus and flexor carpi ulnaris) primarily affects the intrinsic muscles of the hand. High ulnar nerve palsy (proximal to the elbow) involves the loss of both intrinsic and specific extrinsic flexor functions. Successful reconstruction requires a deep understanding of hand biomechanics, meticulous preoperative evaluation, and precise execution of tendon transfers.
Low Ulnar Nerve Palsy
Functional Deficits and Biomechanics
The functional deficits caused by low ulnar nerve palsy are profound and primarily involve the loss of intrinsic muscle function. The hallmark biomechanical failures include:
- Weakness of Pinch: Paralysis of the adductor pollicis and the first dorsal interosseous results in a profound loss of key pinch strength. Patients frequently exhibit Froment’s sign (hyperflexion of the thumb interphalangeal joint driven by the intact flexor pollicis longus to compensate for the loss of the adductor pollicis) and Jeanne’s sign (hyperextension of the thumb metacarpophalangeal joint).
- Weakness of Grip: Paralysis of most of the finger intrinsics (interossei and ulnar two lumbricals) diminishes power grip by up to 50%. The interossei are primary flexors of the metacarpophalangeal (MCP) joints and extensors of the interphalangeal (IP) joints.
- Intrinsic Minus Clawing: Clawing of the ring and little fingers is the most visible deformity. Without the intrinsic muscles to flex the MCP joints and extend the IP joints, the intact extrinsic extensors (extensor digitorum communis) hyperextend the MCP joints, while the intact extrinsic flexors (flexor digitorum profundus and sublimis) hyperflex the IP joints.
Clinical Pearl: The severity of clawing is paradoxically worse in low ulnar nerve palsy compared to high ulnar nerve palsy. In a low lesion, the flexor digitorum profundus (FDP) to the ring and little fingers remains innervated, exacerbating the flexion deformity at the distal interphalangeal (DIP) joints. This phenomenon is known as the Ulnar Paradox.
Preoperative Evaluation
Before proceeding with tendon transfers, the surgeon must ensure that all joints are supple. A fixed flexion contracture at the proximal interphalangeal (PIP) joint will render any tendon transfer ineffective.
The Bouvier Test is critical: the examiner passively blocks the MCP joints in slight flexion. If the patient can then actively extend the PIP and DIP joints using their intact extrinsic extensors, the central slip and lateral bands are functional, and a simple MCP stabilization procedure (anti-claw transfer) will succeed. If the IP joints cannot be extended, the transfer must be routed directly into the lateral bands to actively restore IP extension.
Surgical Restoration: The Omer FDS Transfer
Paralysis of the adductor pollicis results in a major functional loss that should be restored by an appropriate tendon transfer. Furthermore, the clawing of the ulnar digits must be corrected to restore synchronous hand opening and closing.
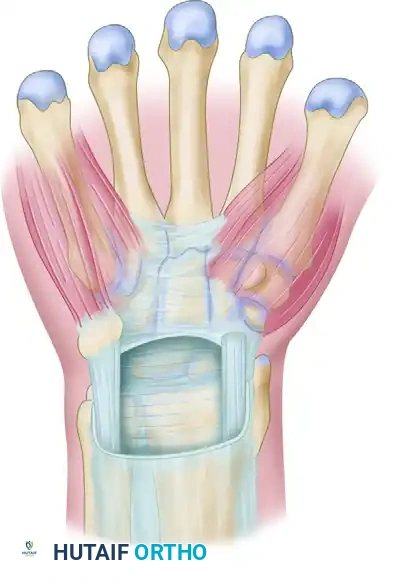
The Omer Transfer utilizes a single flexor digitorum sublimis (FDS) tendon (typically from the middle finger) to simultaneously correct clawing and strengthen thumb-index pinch.
FIGURE 71-30: Single transfer of flexor digitorum sublimis tendon is used to correct clawing and to strengthen thumb-index pinch in isolated ulnar nerve palsy. APB, adductor pollicis brevis; DI and VI, dorsal and volar interossei. The FDS is split into slips to address multiple deficits simultaneously.
Step-by-Step Surgical Technique (Omer FDS Transfer)
- Tendon Harvest: Expose the middle finger sublimis (FDS) tendon through a single incision in the distal palm over the metacarpal heads, or through separate incisions at its insertion on the middle phalanx. Divide the tendon so that the free end of its distal segment lies within its sheath. Withdraw the proximal segment of the tendon through a proximal volar forearm incision.
- Preparation of the Slips: The harvested FDS tendon is split longitudinally into three or four slips, depending on the number of digits requiring intrinsic substitution.
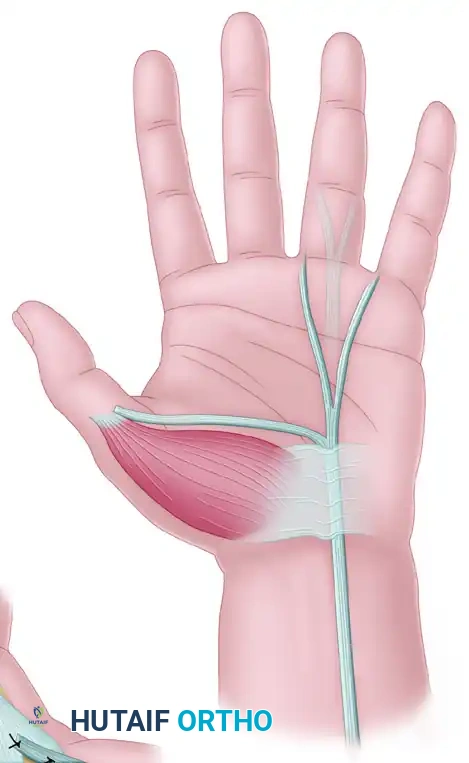
- Routing for Thumb Adduction: One robust slip of the FDS is routed transversely across the palm, deep to the flexor tendons and neurovascular bundles, directed toward the thumb.
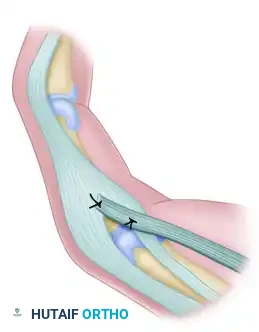
- Anchoring at the Thumb: The slip is anchored securely to the insertion of the adductor pollicis or the adductor pollicis brevis (APB) to restore powerful key pinch.
Anchored at APB insertion: Detail of the FDS slip securely sutured to the adductor/APB insertion to restore key pinch biomechanics.
- Routing for Anti-Claw (Fingers): The remaining slips are routed through the lumbrical canals of the ring and little fingers. They must pass volar to the deep transverse metacarpal ligament to ensure they act as MCP flexors.
- Distal Fixation: Depending on the Bouvier test, the slips are either sutured to the A1/A2 pulleys (Zancolli lasso principle) for simple MCP flexion, or woven into the radial lateral bands of the ring and little fingers to actively extend the PIP joints.
- Tensioning: Tensioning is critical. The thumb slip is tensioned to hold the thumb in slight adduction. The finger slips are tensioned so that with the wrist in neutral, the MCP joints are held in 30 to 40 degrees of flexion.
Surgical Warning: The sublimis tendons of the long and ring fingers must be separated proximally and not crossed over to prevent a scissors-type compression of the median nerve in the distal forearm.
Surgical Pitfall: Differentiating Combined vs. Isolated Palsy Transfers
Historical Note on Literature Discrepancies: Some classic orthopaedic texts inadvertently conflate tendon transfers for radial nerve palsy with those for ulnar nerve palsy when discussing combined nerve injuries. For instance, instructions detailing the perforation of the extensor carpi radialis longus and brevis, or passing the FDS through the interosseous membrane to attach to the common digital extensors and extensor pollicis longus, describe the classic Boyes Transfer for radial nerve palsy.
In an isolated low ulnar nerve palsy, the extrinsic extensors (EDC, EPL) are perfectly intact. Routing flexor tendons through the interosseous membrane to the dorsum of the wrist is contraindicated for isolated ulnar palsy. The surgeon must strictly adhere to volar-based routing (as seen in the Omer or Zancolli procedures) to restore intrinsic flexion at the MCP joints and adduction of the thumb.
High Ulnar Nerve Palsy
Pathoanatomy and Deficits
The functional deficits caused by high ulnar nerve palsy are the same as those described for low ulnar nerve palsy, with the critical addition of lost extrinsic muscle function:
* Flexor Digitorum Profundus (FDP): Paralysis of the FDP to the ring and little fingers results in an inability to actively flex the distal interphalangeal (DIP) joints of these digits.
* Flexor Carpi Ulnaris (FCU): Paralysis of the FCU weakens wrist flexion and leads to radial deviation during active wrist flexion, as the flexor carpi radialis (FCR) is unopposed.
Because the FDP to the ring and little fingers is paralyzed, the severe clawing seen in low ulnar nerve palsy is often blunted (the Ulnar Paradox). However, the functional loss of grip strength is significantly more severe.
Surgical Management of High Ulnar Nerve Palsy
The tendon transfers described for low ulnar nerve palsy (to restore thumb adduction and correct MCP hyperextension) are still required. However, critical modifications must be made regarding donor tendon selection and additional procedures must be performed to restore terminal digit flexion.
- Donor Tendon Restrictions: The sublimis (FDS) of the ring finger must not be transferred in a high ulnar nerve palsy. Because the profundus of this finger is paralyzed, harvesting its sublimis would leave the ring finger completely devoid of active flexion, resulting in a useless, flail digit. The middle finger FDS remains the donor of choice.
- Restoration of DIP Flexion (FDP Tenodesis): Flexion of the distal interphalangeal joints of the ring and little fingers can be restored by suturing the paralyzed profundus tendons of these fingers to the intact profundus tendon of the long finger (which is innervated by the anterior interosseous branch of the median nerve). This side-to-side tenodesis synchronizes the flexion of the ulnar three digits.
- Augmentation of Grip Strength: If further power is needed, or if the long finger FDP is deemed too weak to drive all three ulnar digits, an active tendon transfer is indicated. Transfer of the extensor carpi radialis longus (ECRL) into the profundus tendons of the long, ring, and little fingers can be performed.
Anatomic Variation Note: The innervation of the profundus of the long finger is highly variable. It may be totally ulnar at times, and frequently only partially ulnar. Preoperative electromyography (EMG) and careful intraoperative assessment of long finger FDP excursion are mandatory before relying on it as a motor source for the ring and little fingers.
Postoperative Care and Rehabilitation
The success of tendon transfers in ulnar nerve palsy relies as much on meticulous postoperative rehabilitation as it does on surgical execution. The transferred tendons must heal in their new shortened positions before active mobilization begins.
Immobilization Phase (Weeks 0-4)
- Tourniquet Release: Before the transferred tendons are sutured in place, remove the tourniquet and check the interosseous artery and surrounding vascular structures for bleeding. Hemostasis is critical to prevent hematoma-induced adhesions.
- Casting: Immobilization should be implemented for a total of 6 weeks. Usually, a rigid cast or custom thermoplastic splint is maintained on the arm for the first 4 weeks.
- Positioning:
- The metacarpophalangeal (MCP) joints should not be completely extended; they must be held in about 40 degrees of flexion to protect the anti-claw transfers.
- The wrist should be fully extended (approximately 30 to 45 degrees) to relieve tension on the volar transfers.
- The thumb should be immobilized in palmar abduction and extension to protect the adductorplasty.
- The interphalangeal (IP) joints of the fingers should be left in "comfortable" flexion, allowing for gentle passive extension exercises to prevent capsular contracture.
Mobilization Phase (Weeks 4-6 and Beyond)
- Dynamic Splinting: Following the initial 4 weeks of rigid immobilization, the patient is transitioned to a spring-loaded extension splint (or a lumbrical bar splint) for the wrist and fingers for another 1 to 2 weeks. This allows for active flexion while protecting the transfers from sudden passive overstretch.
- Motor Re-education: The patient must undergo extensive hand therapy to achieve cortical remapping. Because an FDS tendon (a native flexor) is often used to restore intrinsic function, synergistic movement patterns are easier to learn than out-of-phase transfers. Therapy focuses on isolating MCP flexion with IP extension, and strengthening the newly restored key pinch.
- Return to Activity: Unrestricted heavy gripping and manual labor are typically restricted until 10 to 12 weeks postoperatively to ensure maximum tensile strength of the tendon weaves.
📚 Medical References
- following rotational osteotomy of congenital radioulnar synostosis, J Pediatr Orthop 7:103, 1987.
- Hansen OH, Andersen NO: Congenital radioulnar synostosis: report of 37 cases, Acta Orthop Scand 41:225, 1970.
- Kanaya F, Ibaraki K: Mobilization of a congenital proximal radioulnar synostosis with use of a free vascularized fascio-fat graft, J Bone Joint Surg 80A:1186, 1998.
- Lin HH, Strecker WB, Manske PR, et al: A surgical technique of radioulnar osteoclasis to correct severe forearm rotation deformities, J Pediatr Orthop 15:53, 1995.
- Murase T, Tada K, Yoshida T, et al: Derotational osteotomy at the shafts of the radius and ulnar for congenital radioular synostosis, J Hand Surg 28A:133, 2003.
- Okrent DH, McFadden JC: Radiologic case study: congenital radio ulnar synostosis, Orthopedics 9:1452, 1986.
- Ramachandran M, Lau K, Jones DH: Rotational osteotomies for congenital radioulnar synostosis, J Bone Joint Surg 87B:1406, 2005.
- Seitz WH Jr, Gordon TL, Konsens RM: Congenital radioulnar synostosis: a new technique for derotational osteotomy, Orthop Rev 19:192, 1990.
- Simmons BP, Southmayd WW, Riseborough EJ: Congenital radioulnar synostosis, J Hand Surg 8A:829, 1983.
- Wilkie DPD: Congenital radio-ulnar synostosis, Br J Surg 1:366, 1913-1914.
You Might Also Like