Comprehensive Guide to Carpal Instability and Wrist Arthrodesis
Key Takeaway
Carpal instability encompasses a complex spectrum of ligamentous injuries, ranging from scapholunate dissociation to progressive perilunar dislocations. Accurate diagnosis relies on understanding carpal kinematics, recognizing radiographic patterns like DISI and VISI, and performing provocative clinical maneuvers such as the Watson shift test. Surgical management dictates precise anatomical reduction, rigid internal fixation, and robust ligamentous reconstruction to restore carpal alignment and prevent progressive radiocarpal arthrosis.
Total Wrist Arthrodesis: Indications and Surgical Technique
End-stage carpal instability, neglected perilunate dislocations, and advanced radiocarpal arthrosis often necessitate salvage procedures to provide a stable, pain-free wrist. Total wrist arthrodesis remains the gold standard for high-demand patients with pan-carpal arthritis.
Biomechanics and Preoperative Planning
A rigid fusion column must be established through the carpus to the metacarpal, coinciding precisely with plate placement. The fundamental principle is that all joints spanned directly by the plate must be fused; adjacent joints (such as the carpometacarpal joints of the index and middle fingers) can be included if degenerative changes are present.
Surgical Approach and Plate Fixation
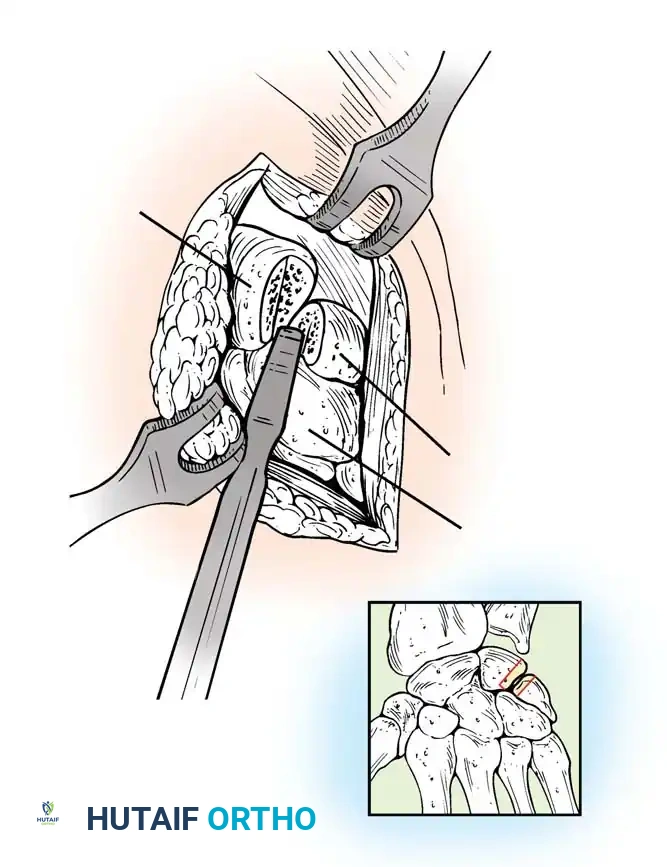
- Positioning and Incision: The patient is positioned supine with the arm on a hand table. A longitudinal dorsal incision is made centered over Lister’s tubercle, extending distally to the base of the third metacarpal.
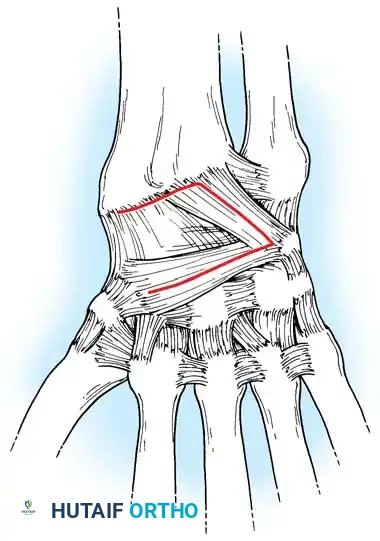
- Exposure: The extensor retinaculum is elevated, and the extensor pollicis longus (EPL) is transposed radially. The dorsal capsule is excised to expose the radiocarpal and midcarpal joints.
- Joint Preparation: The dorsal cartilage of the radiocarpal, intercarpal, and third carpometacarpal joints is meticulously denuded down to bleeding subchondral bone.
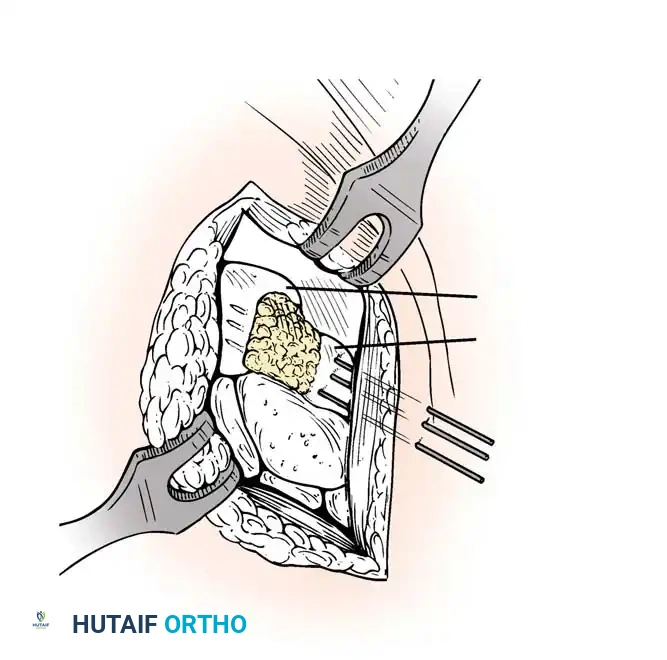
- Bone Grafting: A local distal radial bone graft portal is utilized. Cancellous bone is harvested from the distal radius metaphysis to augment the fusion sites.
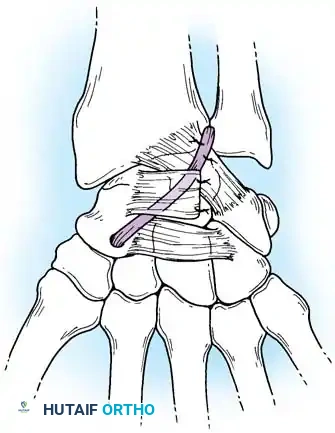
- Plate Application: A 3.5-mm dynamic compression plate (DCP) is applied from distal to proximal. The plate is specifically contoured to provide 10 to 15 degrees of wrist extension. The plate spans the local radial bone graft augmentation, ensuring rigid compression across the fusion mass.
Surgical Warning: Ensure the distal screws engage the dense diaphyseal bone of the third metacarpal without penetrating the palmar cortex, which could tether the flexor tendons. The thickness of the plate distally must be accommodated by adequate soft tissue closure to prevent extensor tendon irritation.
Postoperative Protocol
Protective immobilization in a short-arm volar splint is maintained immediately postoperatively. This is transitioned to a cast or rigid orthosis and discontinued only when solid bone union is demonstrated radiographically, typically at 6 to 8 weeks.
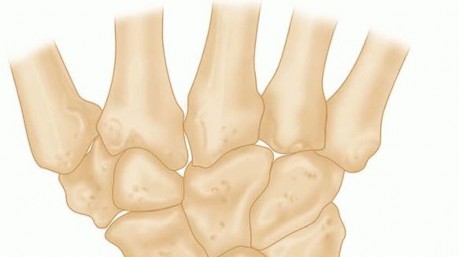
Carpal Ligament Injuries and Instability Patterns
The intricate relationships of the carpal bones rely entirely on capsuloligamentous integrity and articular geometry, as no tendons insert directly onto the proximal carpal row. Abnormalities in these relationships have been recognized since the early 1900s, but the modern understanding of carpal kinematics was revolutionized by Linscheid et al. in 1972.
Kinematics and the Intercalated Segment
The proximal carpal row acts as an intercalated segment between the rigid distal radius and the distal carpal row. The scaphoid has a natural tendency to palmar-flex, while the triquetrum tends to dorsiflex. The lunate, tethered between them by the scapholunate (SL) and lunotriquetral (LT) interosseous ligaments, balances these opposing forces.
Instability in the carpus is classified temporally and kinematically:
* Static Instability: Radiographic intercarpal relationships are abnormal at rest and do not change with motion.
* Dynamic Instability: Resting radiographs appear normal, but intercarpal relationships become abnormal under physiological loads or with specific manipulation.
Radiographic Evaluation of Wrist Collapse
Linscheid et al. emphasized the critical importance of the true lateral radiograph. In a normal wrist, the longitudinal axes of the radius, lunate, capitate, and third metacarpal should be collinear within an approximately 15-degree tolerance.
When ligamentous disruption occurs, predictable collapse patterns emerge:
1. Dorsal Intercalated Segment Instability (DISI): The distal articular surface of the lunate tilts to face dorsally. This is the hallmark of scapholunate dissociation.
2. Volar Intercalated Segment Instability (VISI): The distal articular surface of the lunate tilts toward the palm. This is typically associated with lunotriquetral dissociation.
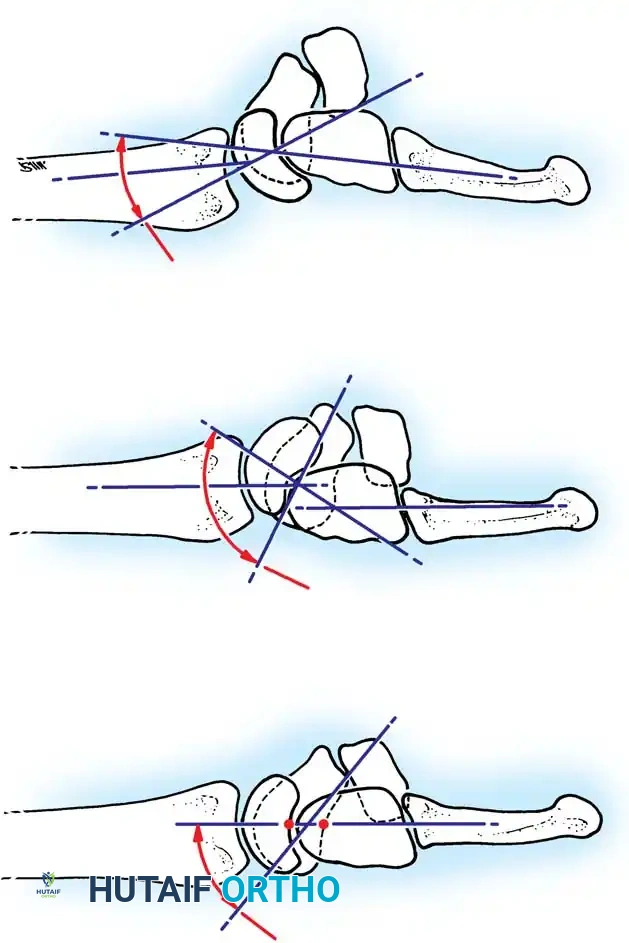
Fig. 66-77 A, Normal scapholunate and capitolunate angles. B, DISI deformity. C, VISI deformity.
Classification of Carpal Instability
The classification of carpal instability has evolved significantly, with the Dobyns and Cooney system providing a comprehensive framework based on location, severity, and radiographic patterns.
I. Carpal Instability Dissociative (CID)
CID involves the disruption of the intrinsic interosseous ligaments between the bones of the same carpal row (usually the proximal row).
* Proximal Carpal Row CID:
* Unstable scaphoid fracture (DISI pattern)
* Scapholunate dissociation (DISI pattern)
* Lunotriquetral dissociation (VISI pattern)
II. Carpal Instability Nondissociative (CIND)
CIND involves the disruption of the extrinsic radiocarpal or midcarpal ligaments, while the intrinsic ligaments between the carpal bones remain intact.
* Radiocarpal CIND: Palmar or dorsal ligament ruptures leading to translation of the entire proximal row.
* Midcarpal CIND: Ulnar or radial midcarpal instability, often presenting with a VISI pattern or a painful "clunk" during ulnar deviation.
III. Carpal Instability Combined (CIC)
CIC represents complex injuries involving both dissociative and nondissociative elements, such as perilunate dislocations with radiocarpal instability.
IV. Adaptive Carpus
Malposition of the carpus secondary to an extrinsic deformity, such as a distal radius malunion, scaphoid nonunion, or Madelung deformity.
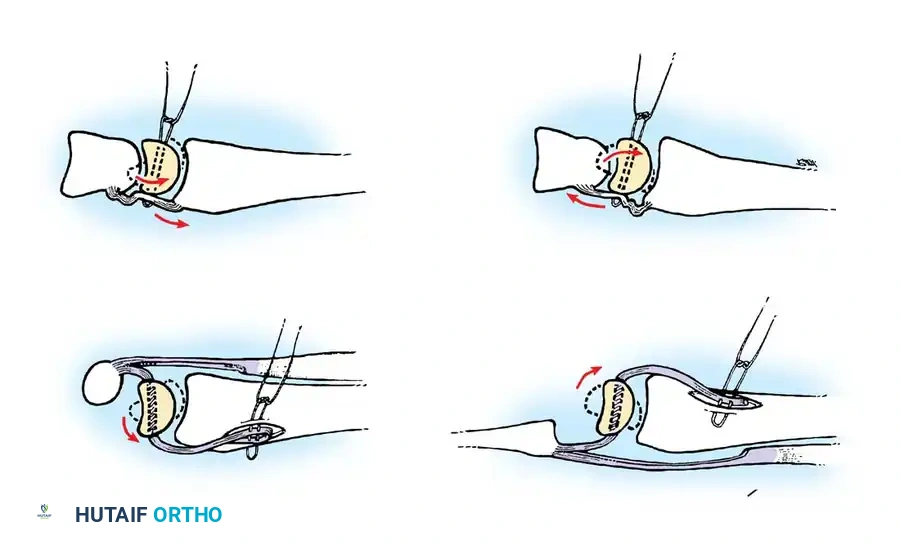
Progressive Perilunar Instability
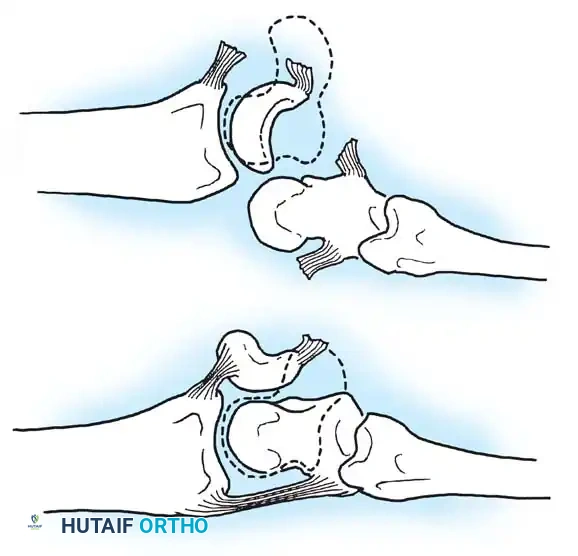
Mayfield, Johnson, and Kilcoyne described the sequential failure of carpal ligaments resulting from forced wrist hyperextension, ulnar deviation, and intercarpal supination. This progressive disruption occurs in four distinct stages around the lunate:
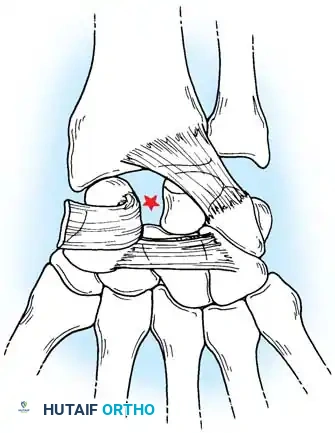
- Stage I (Scapholunate Failure): Disruption of the scapholunate interosseous ligament and volar radioscaphocapitate ligament.
- Stage II (Capitolunate Failure): The force propagates distally, disrupting the space of Poirier (palmar capitolunate joint), allowing the capitate to subluxate dorsally.
- Stage III (Triquetrolunate Failure): Disruption of the lunotriquetral interosseous ligament. The entire carpus separates from the lunate, resulting in a dorsal perilunate dislocation.
- Stage IV (Lunate Dislocation): The dorsal radiocarpal ligament fails. The capitate is driven proximally, forcing the lunate to extrude anteriorly into the carpal tunnel.
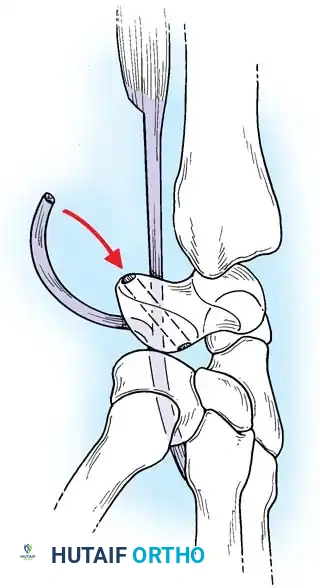
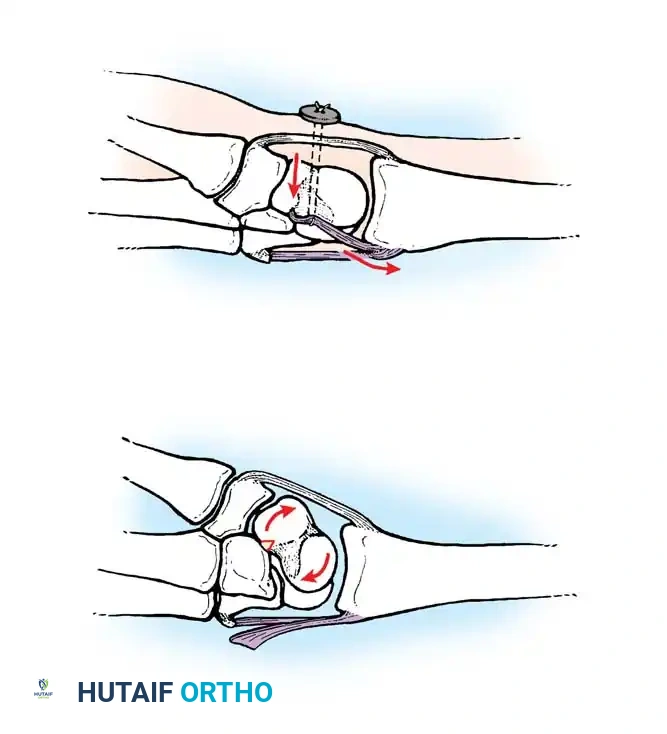
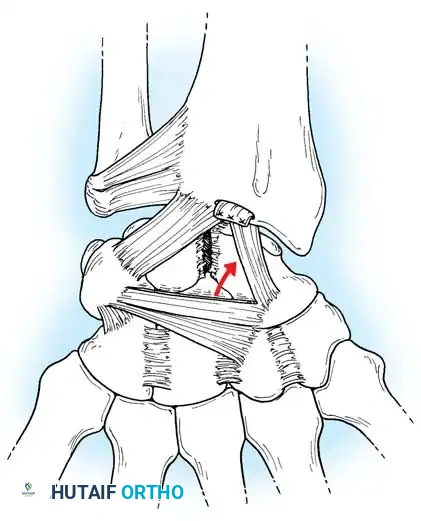
Rotary Subluxation of the Scaphoid
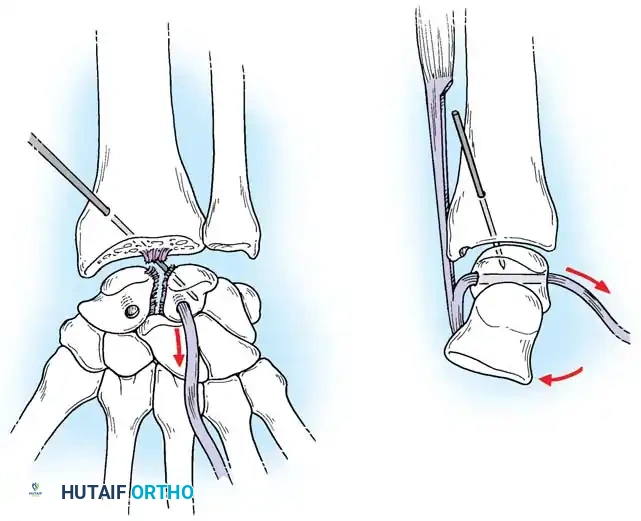
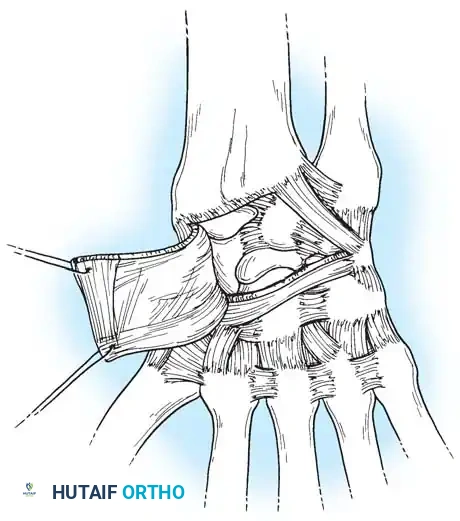
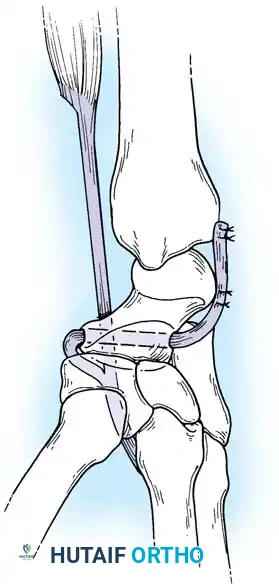
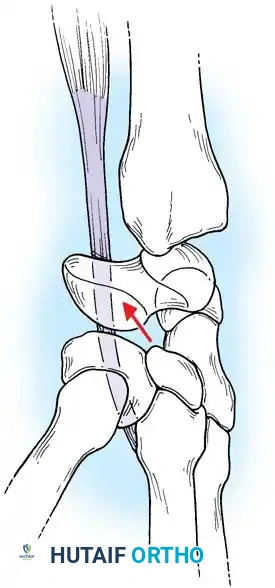
Scapholunate (SL) dissociation is the most common and clinically significant carpal instability. It results from injuries to the dorsal and volar portions of the scapholunate interosseous ligament, the long radiolunate ligament, and the radioscaphocapitate ligament.
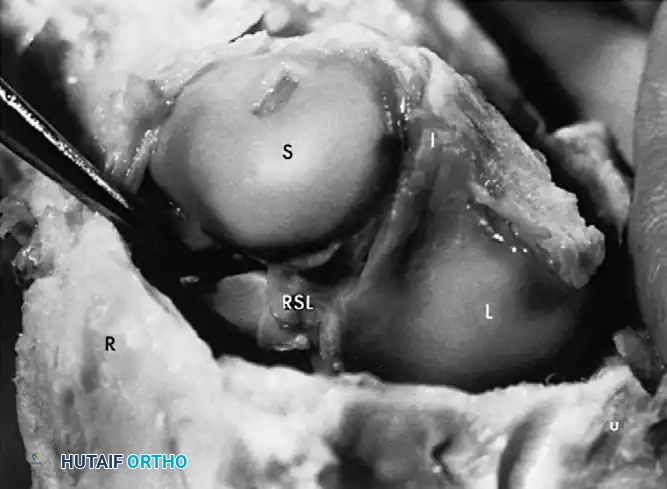
Fig. 66-76 Radioscaphoid ligament (RSL) and surrounding capsular anatomy.
Pathoanatomy and Clinical Presentation
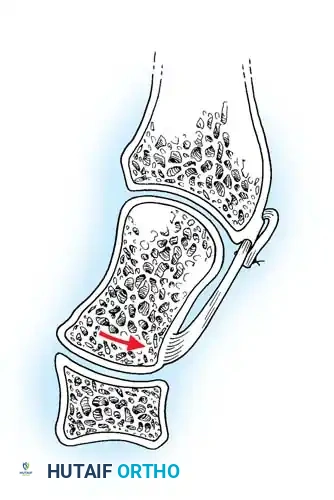
Without the tethering effect of the lunate, the proximal pole of the scaphoid rotates dorsally, assuming a more vertical orientation. Eventually, the scaphoid separates entirely from the lunate.
Patients typically present after a fall on an extended wrist. The initial injury is frequently dismissed as an uncomplicated wrist sprain. Over time, patients report activity-related pain, weakness, and aching localized to the dorsal radiocarpal articulation.
Clinical Pearl: Always maintain a high index of suspicion for SL dissociation in patients presenting with chronic dorsal radial wrist pain and a history of trauma. Missed SL tears inevitably progress to Scapholunate Advanced Collapse (SLAC) arthritis.
Provocative Clinical Maneuvers
- Watson Scaphoid Shift Test: The examiner places four fingers on the dorsum of the radius and the thumb on the scaphoid tuberosity. The wrist is moved from ulnar deviation (where the scaphoid is extended) to radial deviation (where the scaphoid normally flexes). Thumb pressure resists scaphoid flexion. If the SL ligament is incompetent, the proximal pole of the scaphoid is driven dorsally out of the elliptical radial fossa, producing pain and a palpable subluxation.
- Catch-Up Clunk: As the loaded wrist moves from radial to ulnar deviation, an unstable lunate remains in a volar-flexed position until sufficient pressure forces it to suddenly shift and "catch up" with the scaphoid, producing a palpable clunk.
Radiographic Diagnosis
While dynamic instability requires stress views or fluoroscopy, static rotary subluxation is evident on standard radiographs:
1. Terry Thomas Sign: A gap of >2 mm between the scaphoid and lunate on the AP view (accentuated with a clenched-fist view).
2. Cortical Ring Sign: The axially rotated scaphoid presents its distal pole end-on, creating a dense circular outline on the AP view.
3. Scaphoid Shortening: The scaphoid appears abnormally short due to its vertical orientation.
4. DISI Deformity: On the lateral view, the normal scapholunate angle is 30° to 60° (mean 47°), and the capitolunate angle is <20°. In a DISI deformity, the scapholunate angle exceeds 60° (often >80°), and the capitolunate angle exceeds 20°.
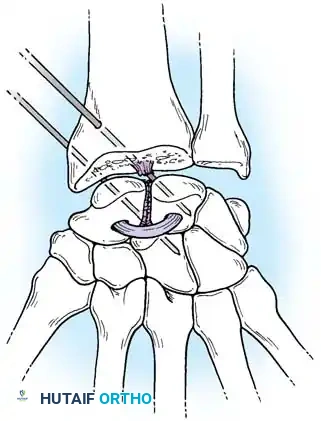
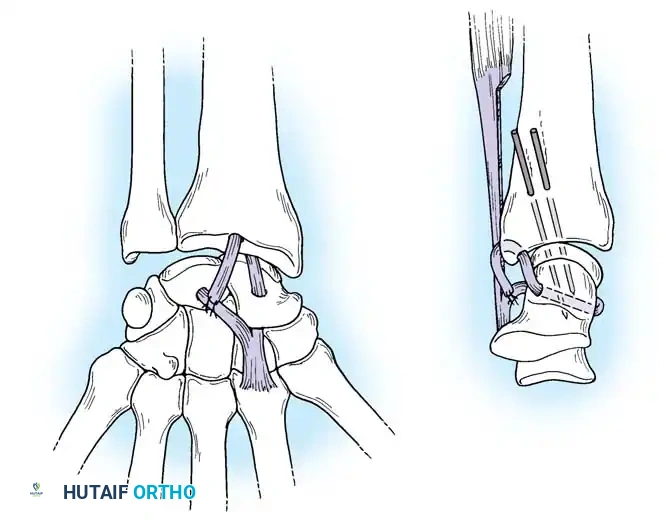
Surgical Management of Scapholunate Dissociation
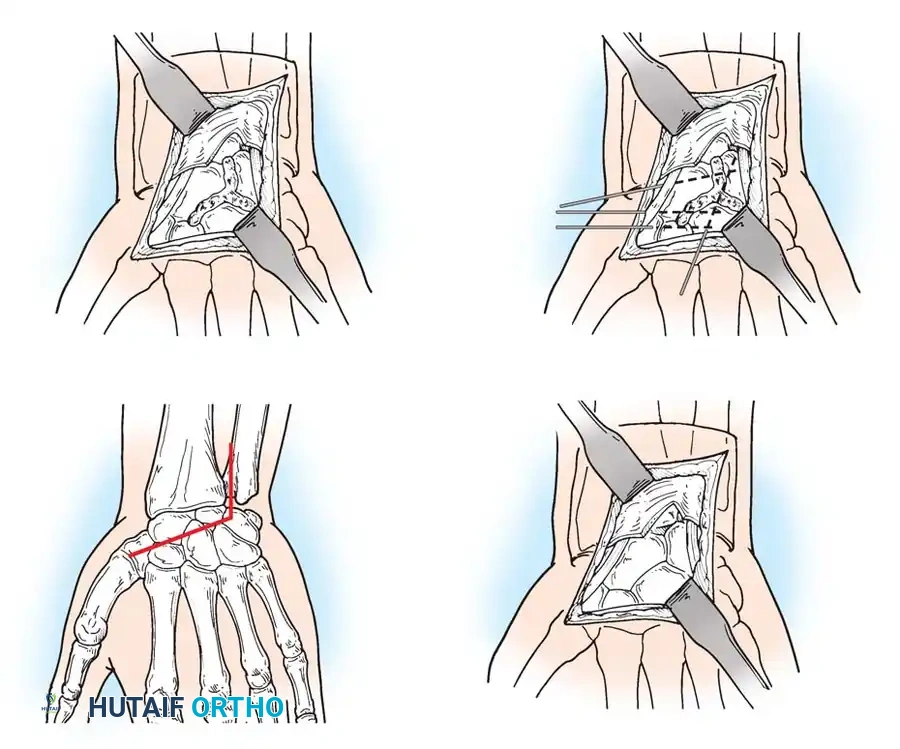
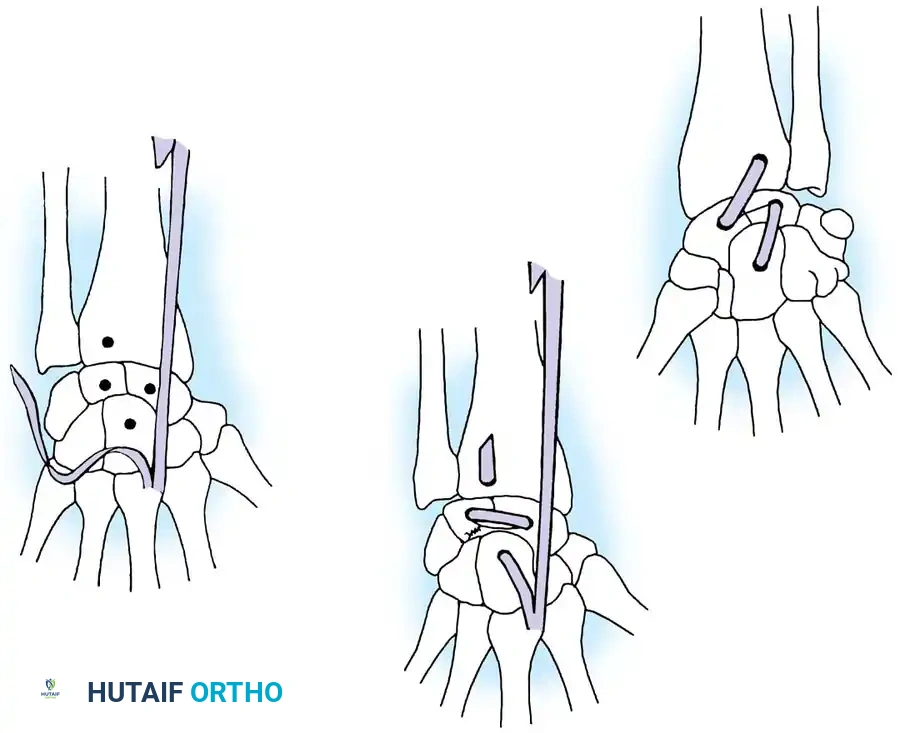
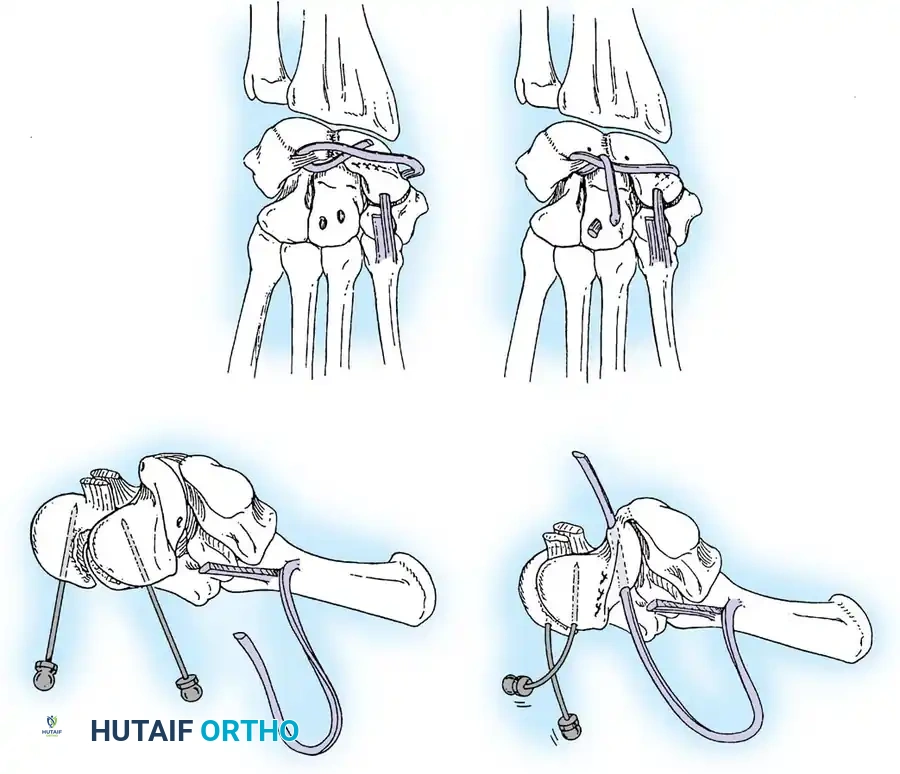
Acute Injuries (<4 weeks):
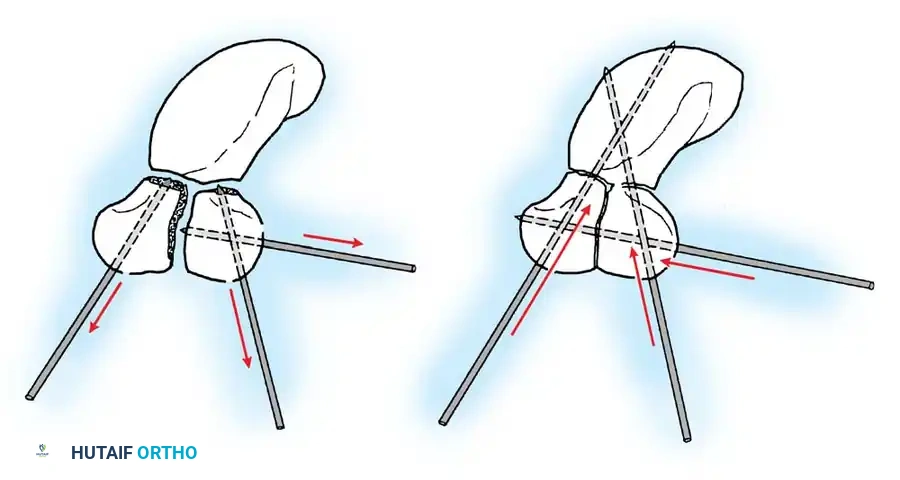
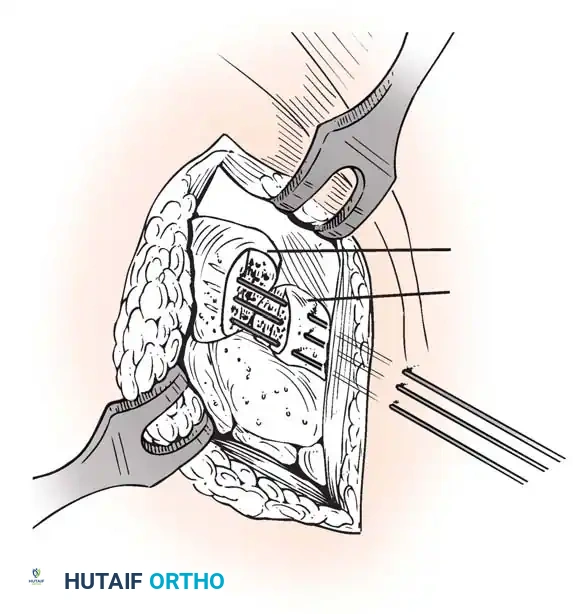
Closed reduction with percutaneous pinning (placing 0.045-inch K-wires from the scaphoid to the capitate and lunate) can be attempted. However, open reduction through a dorsal approach is generally preferred. This allows direct closure of the scapholunate gap, K-wire fixation, and primary repair of the dorsal SL interosseous ligament using suture anchors.

You Might Also Like