Surgical Management of Proximal Humerus & Clavicle Malunions
Key Takeaway
Malunions of the proximal humerus and clavicle present complex reconstructive challenges. Disruption of normal anatomy limits shoulder range of motion and strength. Successful management requires a deep understanding of deforming muscle forces, advanced preoperative imaging, and meticulous surgical execution. This guide details the biomechanics, clinical evaluation, and step-by-step surgical techniques—including corrective osteotomy and plate fixation—to restore anatomical alignment and optimize functional outcomes in shoulder girdle malunions.
Pathoanatomy and Biomechanics of Proximal Humerus Malunions
Malunion of a proximal humerus fracture typically results from inadequate operative reduction, secondary loss of fixation, or the nonoperative management of a significantly displaced fracture. The disruption of the normal anatomical relationships between the tuberosities, the humeral head, and the humeral shaft profoundly limits the glenohumeral range of motion and decreases the overall strength of the shoulder girdle.
Bony abnormalities in these scenarios are rarely isolated; they frequently present as a combination of tuberosity displacement, articular surface incongruity, and angular or rotational malalignment of the articular segment. Furthermore, the osseous deformity is almost universally accompanied by severe soft-tissue pathology, including capsular contracture, rotator cuff tearing or retraction, and potential neurological injury.
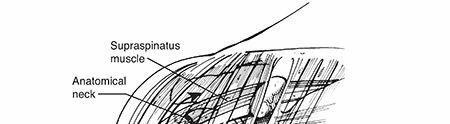
Understanding the predictable patterns of displacement requires a thorough grasp of the deforming muscular forces acting upon the proximal humerus. Each anatomical segment has specific tendinous insertions that dictate its trajectory when fractured:
- The Humeral Shaft: Displaces anteromedially due to the powerful pull of the pectoralis major inserting on the lateral lip of the bicipital groove.
- The Proximal Articular Fragment: Tends to be abducted by the resting tone of the rotator cuff if the tuberosities remain attached.
- The Greater Tuberosity: Displaces posterosuperiorly due to the combined forces of the supraspinatus, infraspinatus, and teres minor muscles.
- The Lesser Tuberosity: Displaces medially, driven by the pull of the subscapularis muscle.
Characteristic Deformity Patterns
Two-Part Surgical Neck Malunions:
These fractures frequently heal in varus and anterior angulation. The shaft is pulled anteromedially by the pectoralis major, while the proximal fragment is abducted. Severe deformities in this plane result in a profound loss of forward flexion and abduction.
Two-Part Greater Tuberosity Malunions:
The tuberosity is drawn posteriorly and superiorly. Healing in this non-anatomical position creates a mechanical block to abduction and external rotation, frequently leading to severe subacromial impingement.
Clinical Pearl: A classic, though not strictly pathognomonic, sign of a greater tuberosity malunion is the complete absence of external rotation when the arm is maximally abducted.
Two-Part Lesser Tuberosity Malunions:
Medial displacement occurs due to the subscapularis. While overall shoulder function may not be catastrophically impaired, the medialized fragment can impinge against the coracoid process, mechanically blocking internal rotation and forward elevation.
Three-Part Malunions:
* Involving the Greater Tuberosity and Surgical Neck: The articular head fragment is internally rotated by the intact subscapularis. The shaft displaces anteromedially, and the greater tuberosity migrates posterosuperiorly. This results in severe functional impairment due to the combined loss of abduction and external rotation.
* Involving the Lesser Tuberosity and Surgical Neck: The articular segment is externally rotated and abducted by the intact posterior rotator cuff. Malunion in this position causes intractable pain and a severe limitation of internal rotation.
Four-Part Malunions and Fracture-Dislocations:
These represent the most formidable reconstructive challenges. They are characterized by severe articular incongruity, dense muscular contractures, intra-articular adhesions, a high incidence of osteonecrosis (AVN) of the humeral head, and frequent concomitant neurological deficits.
Classification of Proximal Humeral Malunions
While no universally adopted classification system exists, the system proposed by Beredjiklian et al. is highly regarded for its clinical utility, categorizing malunions based on specific osseous and soft-tissue parameters:
- Type I: Malposition of the greater or lesser tuberosity by more than 1 cm.
- Type II: Intra-articular incongruity or an articular surface step-off exceeding 5 mm.
- Type III: Rotational malalignment of the articular segment by more than 45 degrees in the coronal, sagittal, or axial planes.
Soft-tissue abnormalities are subcategorized into capsular contractures, rotator cuff tears, and mechanical impingement. Notably, in Beredjiklian's series, only 21% of patients presented with an isolated osseous malunion without associated soft-tissue pathology, underscoring the need for comprehensive soft-tissue reconstruction during surgery.
Clinical and Radiographic Evaluation
History and Physical Examination
A meticulous evaluation is paramount. The surgeon must ascertain the original mechanism of injury, the initial treatment modality, and the specific type of hardware utilized (if any) to ensure appropriate extraction equipment is available.
Range of motion (ROM) testing must differentiate between active and passive limits. A severe restriction in passive ROM strongly suggests dense capsular or extracapsular contracture. External rotation must be evaluated both with the arm at the side and at 90 degrees of abduction. Rotator cuff integrity is assessed via external rotation strength testing, the Gerber lift-off test (for subscapularis), and opposed abduction at 90 degrees.
Surgical Warning: Because many patients with proximal humeral malunions harbor subclinical neurological deficits, the function of the axillary, suprascapular, and musculocutaneous nerves must be rigorously documented preoperatively. Electromyography (EMG) and nerve conduction studies (NCS) are highly recommended if a deficit is suspected.
Advanced Imaging
- Standard Radiographs: A complete trauma series (True AP, Scapular Y, and Axillary lateral views) is mandatory. Supplemental internal and external rotation AP views help delineate tuberosity position.
- Computed Tomography (CT): Essential for surgical planning. 3D reconstructions clarify the spatial relationships between the malunited tuberosities, the humeral head, and the shaft. CT is the gold standard for evaluating articular congruity and glenoid version.
- Magnetic Resonance Imaging (MRI): Indicated to assess the integrity of the rotator cuff tendons and to detect early osteonecrosis of the humeral head.
Treatment Strategies for Proximal Humerus Malunions
Nonoperative Management
Conservative care is reserved for low-demand patients with minimal pain who can maintain independence with limited upper extremity function, or for patients whose medical comorbidities preclude complex reconstructive surgery. Modalities include aggressive physical therapy, NSAIDs, and targeted corticosteroid injections.
Operative Management
Surgical intervention is indicated for severe, intractable pain or profound functional loss that has failed conservative management. The choice of procedure depends heavily on the status of the articular cartilage, the viability of the humeral head, and the chronicity of the malunion.
- Joint-Preserving Reconstruction: Includes acromioplasty, lysis of adhesions, and corrective osteotomies of the tuberosities or surgical neck. This is indicated only if the blood supply to the humeral head is intact and the articular surface is preserved. Acromioplasty alone may suffice for greater tuberosity displacement of 1 to 1.5 cm, whereas formal osteotomy and mobilization are required for displacement >1.5 cm.
- Arthroplasty (Hemiarthroplasty or Total Shoulder Arthroplasty): Indicated for extensive articular damage, severe incongruity, or established osteonecrosis. The choice between hemiarthroplasty and TSA depends on the status of the glenoid cartilage and the rotator cuff.
- Arthrodesis: A salvage procedure rarely performed, reserved for cases with profound, irreversible neurological deficits (e.g., complete brachial plexopathy) or chronic, recalcitrant deep infection.
Clinical Pearl: Timing is critical. Delaying operative treatment significantly degrades outcomes. Studies show that 84% of patients treated within 1 year of injury achieve satisfactory outcomes, compared to only 55% of those treated after 1 year, primarily due to the development of irreversible soft-tissue contractures.
Clavicular Malunion: Osteotomy and Plate Fixation Technique
While proximal humerus malunions often require arthroplasty, associated shoulder girdle malunions—particularly of the clavicle—frequently demand extra-articular corrective osteotomy and rigid plate fixation to restore shoulder biomechanics. Severe shortening or angulation of the clavicle alters the resting position of the scapula, leading to scapular dyskinesia, thoracic outlet-type symptoms, and generalized shoulder weakness.
Preoperative Planning
Determine the exact amount of length to be gained both clinically and radiographically.
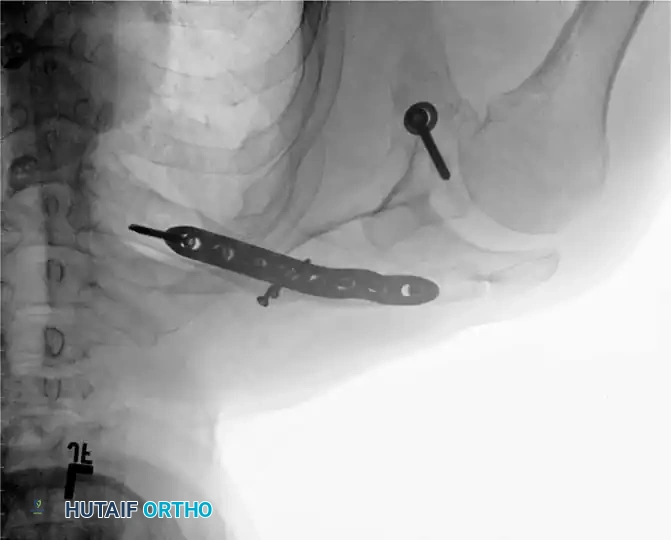
Fig. 55-26A: Midshaft clavicular malunion with significant shortening and inferior displacement.
If the clinical shortening is substantially greater than the observed radiographic shortening, an intercalary structural bone graft (autograft from the iliac crest or allograft) will be required to compensate for the absolute bone loss and restore the native shoulder span.
Patient Positioning and Anesthesia
- Administer general anesthesia.
- Place the patient in a beach-chair (semi-sitting) position.
- Place a small bump or pad behind the ipsilateral scapula to protract the shoulder girdle.
- Tuck the involved upper extremity into the side, allowing it to be draped free for intraoperative manipulation.
- Prep and drape the opposite iliac crest if autogenous structural bone grafting is anticipated.
Surgical Approach and Exposure
-
Incision: Make an oblique incision along the superior surface of the clavicle, following Langer's lines to optimize cosmetic healing.

Fig. 55-25A: Planned oblique incision over the malunion site. -
Flap Elevation: Raise the skin and subcutaneous tissue as a full-thickness flap to identify the underlying platysma and myofascia.
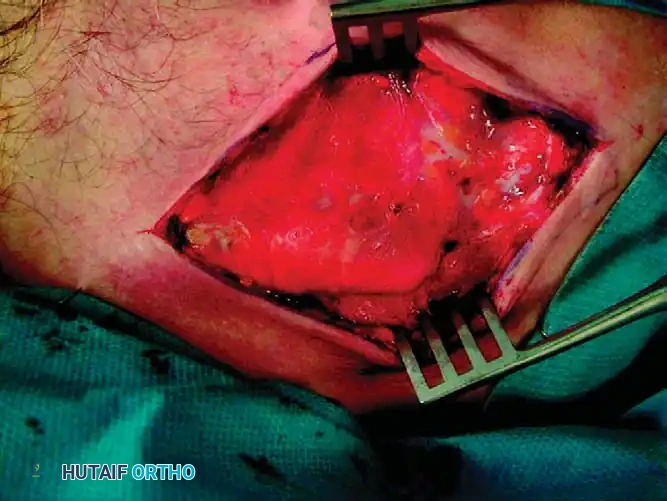
Fig. 55-25B: Subcutaneous flaps raised. -
Myofascial Preservation: Raise the myofascial layer as contiguous flaps. It is critical to preserve this layer so that a robust, two-layered closure can be achieved over the hardware later, minimizing the risk of plate prominence and wound breakdown.
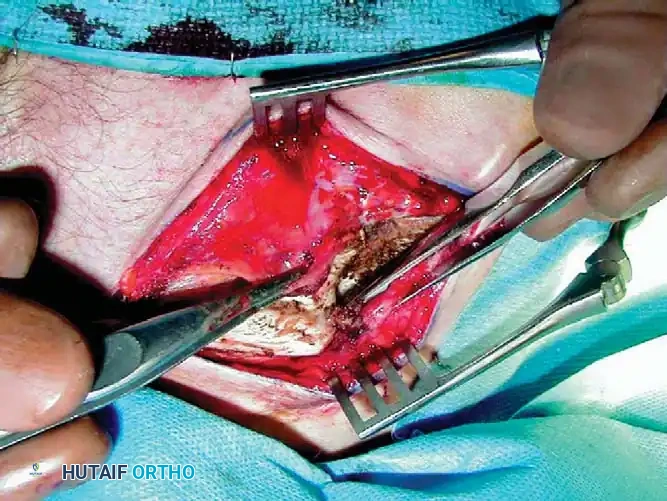
Fig. 55-25C: Identification and preservation of the myofascial layer. -
Identifying the Malunion: Carefully dissect down to the periosteum to identify the malunion site. Plan the corrective osteotomy. In most cases, the original fracture plane can be identified. In extensively remodeled malunions, an oblique sliding osteotomy may be required.
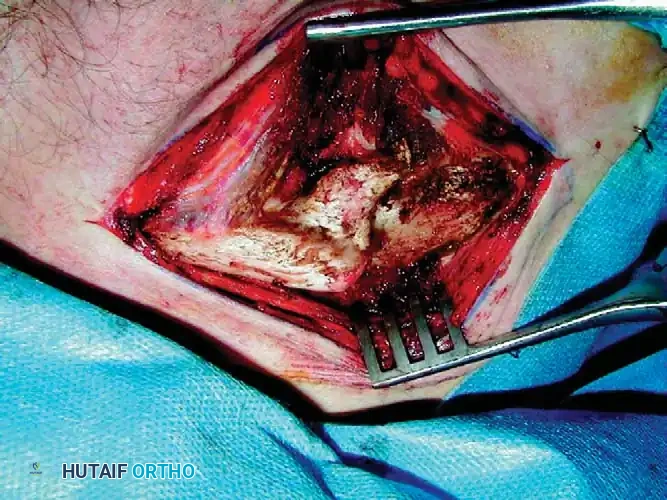
Fig. 55-25D: Exposure of the remodeled clavicular malunion.
Osteotomy and Reduction
-
Executing the Osteotomy: Use a combination of sharp osteotomes and a microsagittal saw to recreate the original fracture line.
Surgical Warning: The saw must be cooled continually with saline irrigation to prevent thermal necrosis of the bone. Place a malleable retractor deep to the clavicle to protect the subclavian vessels and brachial plexus.
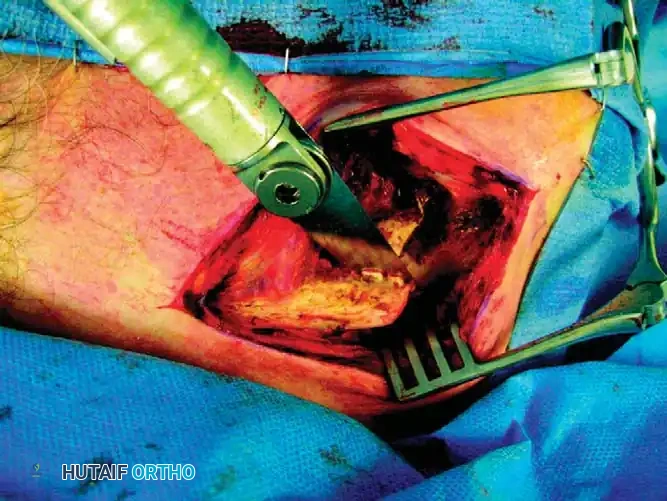
Fig. 55-25E: Osteotomy performed with a microsagittal saw. -
Mobilization: Hold the proximal and distal fragments with reduction forceps (e.g., pointed Weber clamps). Realign the clavicle. Use as little soft-tissue stripping as possible to preserve the periosteal blood supply.

Fig. 55-25F: Initial mobilization of the fragments. -
Canal Preparation: Reestablish the medullary canal using a 3.5-mm drill bit in both the proximal and distal fragments to encourage endosteal bleeding and osteogenesis.

Fig. 55-25G: Realigning the fragments to restore length. -
Correcting Malrotation: Rotate the distal fragment anteriorly so that its flat superior surface faces anteriorly rather than superiorly. Redirect the flat superior surface of the distal fragment to match the proximal segment, creating congruent surfaces.
Pitfall: Make absolutely no attempt to explore or decompress the brachial plexus deep to the clavicle during this maneuver, as the altered anatomy places these structures at high risk of iatrogenic injury.

Fig. 55-25H: Final anatomical reduction achieved.
Plate Fixation and Grafting
- Provisional Fixation: After approximating the fragments, temporarily fix the osteotomy site with a 2.0-mm Kirschner wire.
Associated Surgical & Radiographic Imaging





You Might Also Like