Synovial Plicae of the Knee: Comprehensive Diagnosis and Arthroscopic Management
Key Takeaway
Synovial plicae are embryological remnants of synovial membranes within the knee joint. While often asymptomatic, trauma or repetitive microtrauma can lead to pathological thickening, causing impingement, snapping, and secondary chondral damage. This guide provides an evidence-based approach to the clinical evaluation, differential diagnosis, and arthroscopic management of symptomatic synovial plicae, emphasizing complete excision to prevent recurrence and mitigate progressive articular cartilage degeneration.
INTRODUCTION AND EMBRYOLOGY
The knee joint is a complex biomechanical structure that undergoes significant morphological changes during fetal development. Initially, the fetal knee is separated into three distinct compartments (the suprapatellar pouch, the medial compartment, and the lateral compartment) by thin, mesenchymal synovial membranes. At approximately 4 to 5 months of gestation, these internal partitions typically resorb and cavitate to form a single, unified synovial cavity.
When this resorption process is incomplete or partial, residual synovial shelves or bands remain within the joint capsule. These embryological remnants are known as synovial plicae. While the vast majority of plicae remain thin, elastic, and entirely asymptomatic throughout an individual's life, they can become pathological under conditions of chronic irritation, direct trauma, or altered joint mechanics. Understanding the embryology, anatomical variants, and pathomechanics of synovial plicae is essential for the orthopaedic surgeon, as symptomatic plica syndrome is a frequent, yet often misdiagnosed, cause of anterior knee pain and internal derangement.
ANATOMICAL CLASSIFICATION AND PREVALENCE
Synovial plicae of the knee are anatomically categorized based on their location relative to the patella and the tibiofemoral joint. They are commonly described in four distinct variants: suprapatellar, mediopatellar, infrapatellar, and lateral.
1. Infrapatellar Plica (Ligamentum Mucosum)
The infrapatellar plica is widely reported as the most common synovial plica. It originates from the intercondylar notch, runs parallel to the anterior cruciate ligament (ACL), and inserts into the infrapatellar fat pad. In an embryological study of 116 knees, Ogata and Uhthoff found that in fetuses between 11 and 20 weeks of age, an infrapatellar plica was present in 50% of specimens. While highly prevalent, it is rarely symptomatic but can obscure arthroscopic visualization of the ACL if significantly thickened.
2. Mediopatellar Plica (Medial Shelf)
The mediopatellar plica is the most clinically significant variant, frequently implicated in symptomatic plica syndrome. It originates from the medial wall of the joint capsule, courses obliquely downward beneath the medial retinaculum, and inserts into the infrapatellar fat pad. Medial patellar plicae have been reported in 5% to 70% of individuals. In a clinical series of 168 arthroscopic knee examinations of patients presenting with anterior knee pain, Calpur et al. identified 168 mediopatellar plicae, highlighting its strong association with clinical symptoms.
3. Suprapatellar Plica (Plica Synovialis Suprapatellaris)
The suprapatellar plica divides the suprapatellar pouch from the main articular cavity of the knee. It can present as a complete septum (porta) or an incomplete crescent-shaped fold. Ogata and Uhthoff noted its presence in 33% of fetal specimens, while adult prevalence is generally reported at approximately 17%. Calpur et al. found suprapatellar plicae in only 4.7% of their symptomatic cohort.
4. Lateral Plica
The lateral plica is the least common and least discussed variant, located along the lateral parapatellar gutter. Calpur et al. reported an 18% incidence in their symptomatic arthroscopic series, though it rarely causes the classic snapping symptoms associated with its medial counterpart.
PATHOMECHANICS AND BIOMECHANICS
A normal synovial plica is a thin, pliable, and highly elastic structure that glides smoothly over the femoral condyles during knee flexion and extension. However, any condition that produces chronic irritation, direct trauma, or intra-articular scarring can initiate a pathological cascade.
When traumatized—such as by bumping a flexed knee against a hard object (e.g., a dashboard injury) or through repetitive microtrauma from athletic activities—the plica becomes inflamed. This chronic synovitis leads to edema, cellular infiltration, and eventual fibrosis and hyalinization. The once-elastic tissue transforms into a thickened, rigid, and inelastic fibrotic band.
Surgical Warning: Poorly placed medial arthrotomy incisions or improperly localized anteromedial arthroscopy portals can iatrogenically damage a previously asymptomatic medial plica, causing sufficient scarring to induce postoperative plica syndrome.
The "Bowstring" Effect
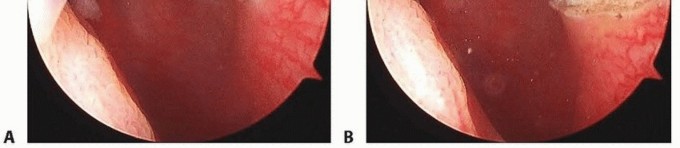
As the knee flexes, a fibrotic mediopatellar plica acts like a rigid bowstring. Strover et al. demonstrated that when viewing through a lateral suprapatellar portal, the suprapatellar and mediopatellar plicae impinge directly on the medial femoral condyle. Specifically, the plica becomes trapped between the quadriceps mechanism and the femoral trochlea when the knee reaches approximately 70 degrees of flexion. This repetitive snapping and mechanical impingement not only causes pain but also leads to progressive abrasive wear on the underlying articular cartilage.
CLINICAL EVALUATION AND DIFFERENTIAL DIAGNOSIS
Diagnosing a pathological plica requires a high index of clinical suspicion and a meticulous physical examination, as its symptoms closely mimic other forms of internal derangement, most notably meniscal tears and patellofemoral pain syndrome.
Patient History and Symptomatology
Patients typically present with:
- Insidious onset of anterior or anteromedial knee pain.
- Mechanical symptoms described as "popping," "catching," or "snapping" as the knee moves through a specific arc of motion.
- Pain exacerbated by prolonged sitting, stair climbing, or kneeling.
- A history of blunt trauma to the anterior knee or a recent increase in repetitive flexion/extension activities (e.g., cycling, running).
Physical Examination
Careful examination is paramount to differentiate the symptoms of a fibrotic, inelastic plica from those of a torn meniscus.
- Meniscal Tear Presentation: Usually causes periodic episodes of giving way, buckling, true joint locking, and pain strictly localized along the joint line. Pain is often increased or reproduced by torsion of the tibia on the femur (e.g., a positive McMurray test).
- Plica Syndrome Presentation: Produces popping and catching by snapping across the patella or medial femoral condyle.
The Plica Stutter Test:
1. Seat the patient on the edge of the examining table with the leg dangling freely.
2. Place your thumb or index finger lightly along the medial border of the patella.
3. Instruct the patient to actively flex and extend the knee.
4. As the knee passes through 45 to 70 degrees of flexion, palpation often localizes the abnormal plica as it flips over the medial femoral condyle, producing a palpable and sometimes audible momentary "stuttering" or snapping of the patella.
IMAGING AND DIAGNOSTIC MODALITIES
While the diagnosis of a pathological plica is primarily clinical and definitively confirmed via arthroscopy, imaging plays a crucial role in ruling out concurrent pathology and assessing secondary cartilage damage.
Radiographic Evaluation
Evaluation of a patient suspected of having a chondral or osteochondral lesion secondary to plica impingement should include:
- Weight-bearing anteroposterior (AP) views.
- 40-degree posteroanterior (PA) flexion views (Rosenberg view).
- Lateral views.
- Patellar (Merchant or sunrise) views to assess patellofemoral tracking and joint space.
- Bilateral standing hip-knee-ankle AP views for mechanical axis alignment.
Magnetic Resonance Imaging (MRI)
Clinical suspicion of an articular cartilage lesion or a thickened plica should prompt evaluation with cartilage-sensitive MRI. MRI is highly effective in determining lesion location, size, and grade (utilizing ICRS classification systems) prior to surgery. A thickened mediopatellar plica may appear as a low-signal band extending from the medial capsule to the fat pad on axial T2-weighted images.
Clinical Pearl: Articular cartilage lesions are often accompanied by significant hemarthrosis as well as occult subchondral trabecular microfractures (bone bruises or bone blisters). Note that occult subchondral bone bruises are also found in up to 80% of patients with complete ruptures of the anterior cruciate ligament, necessitating a comprehensive review of the MRI to avoid missing concurrent ligamentous instability.
ASSOCIATED CHONDRAL LESIONS
The mechanical friction generated by a fibrotic plica snapping across the medial femoral condyle is a well-documented cause of secondary osteoarthritis and focal chondral defects. Several authors have noted a strong association between the presence of plicae and the development of chondral lesions.
- Christoforakis et al.: In a review of 1,000 knee arthroscopies, 321 patients had classifiable knee plicae. Of these, an overwhelming 95% had cartilage lesions, compared with 81% of patients without plicae. Notably, even though the patients without plicae were older on average (39 years) than those with plicae (33 years), the older cohort had fewer cartilage lesions, underscoring the destructive mechanical nature of the plica.
- Lyu and Hsu: In a massive review of 1,587 knee arthroscopic surgeries, 472 knees (30%) were identified with medial plicae. The incidence was significantly higher (67%) in patients with established osteoarthritis. Degenerative cartilaginous lesions were found on the medial femoral condyle in 97% of knees with medial plicae.
These degenerative changes are directly caused by the pathological medial plica impinging against the underlying femoral condyle during knee motion. Patients with these femoral lesions generally localize pain to the medial or lateral tibiofemoral compartment, which worsens with weight-bearing or high-impact activity.
CONSERVATIVE MANAGEMENT
Treatment of plica syndrome should initially be conservative, particularly in younger patients or those with a short duration of symptoms. Nonoperative treatment focuses on decreasing the mechanical load on the joint and reducing synovial inflammation.
Conservative Protocols Include:
- Activity Modification: Restriction of offending activities (e.g., deep squats, repetitive cycling).
- Pharmacotherapy: Use of oral nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce synovial edema.
- Injections: Intra-articular corticosteroid injections can be highly effective in reducing localized synovitis, allowing the plica to assume a more normal, pliable resiliency.
- Physical Therapy: Institution of a strict isometric exercise program for the quadriceps muscles. Strengthening the dynamic stabilizers alters patellofemoral tracking, often reducing the mechanical impingement of the plica. Weight loss and altering daily activities further decrease joint loads.
If conservative measures successfully reduce edema and synovitis, the plica may cease to produce symptoms. However, if the plica has become permanently fibrotic and hyalinized, conservative measures will inevitably fail, and surgical intervention is warranted.
SURGICAL MANAGEMENT: ARTHROSCOPIC EXCISION
When conservative management fails to relieve a patient's symptoms, surgical excision is the definitive and curative treatment. Abnormal plica is diagnosed best, and treated most effectively, by arthroscopic examination of the knee. While a limited excision can technically be performed through a medial parapatellar arthrotomy, modern standards dictate that excision should be done exclusively via arthroscopic techniques to minimize morbidity and postoperative scarring.
Surgical Pitfall: Simply incising or sectioning (releasing) the plica is strictly NOT recommended. A simple release leaves the fibrotic tissue in situ, and the continuity of the plica will almost certainly be restored by postoperative scar tissue, leading to recurrent symptoms. Complete resection is mandatory.
1. Patient Positioning and Setup
- The patient is placed in the supine position on the operating table.
- A well-padded tourniquet is applied to the proximal thigh.
- The operative leg is placed in a leg holder or over a lateral post to allow for valgus stress and full range of motion during the procedure.
- Standard sterile prep and drape are performed.
2. Portal Placement and Diagnostic Arthroscopy
- Anterolateral Portal: Established first for initial viewing. The arthroscope is introduced into the suprapatellar pouch.
- Note: When a suprapatellar plica is sufficiently prominent, it can present difficulties during arthroscopy as the arthroscope is introduced into the pouch. Careful navigation is required to avoid iatrogenic cartilage scuffing.
- Anteromedial Portal: Established under direct visualization for instrumentation.
- A systematic diagnostic sweep of the knee is performed. Careful assessment of the width, thickness, and texture of the plica by viewing and probing is critical.

3. Dynamic Evaluation
With the arthroscope in the lateral portal, the knee is slowly taken through a range of motion from full extension to 90 degrees of flexion. The surgeon must directly observe the mediopatellar plica to confirm if it snaps over the medial femoral condyle or becomes trapped between the quadriceps mechanism and the trochlea at 70 degrees of flexion.
4. Excision Technique
- Instrumentation: A motorized oscillating shaver (4.0 mm or 4.5 mm) and an arthroscopic basket punch or radiofrequency (RF) ablation wand are utilized.
- Resection: Beginning at the free edge of the plica, the tissue is systematically resected. The resection must be carried down to the normal synovial base at the medial capsule.
- Suprapatellar Plicae: If a complete suprapatellar septum is present, the central portion is resected to widely communicate the suprapatellar pouch with the main joint cavity.
- Hemostasis: The medial capsular base is highly vascular. An RF wand should be used to achieve meticulous hemostasis, preventing postoperative hemarthrosis which can lead to arthrofibrosis.
5. Management of Concurrent Chondral Lesions
If full-thickness articular cartilage lesions (ICRS grade III or IV) are identified on the medial femoral condyle secondary to plica impingement, they must be addressed concurrently. Depending on the lesion's size and the patient's age, treatment may include chondroplasty (debridement of unstable cartilage flaps), microfracture, or preparation for future cartilage restoration procedures.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The primary goal of postoperative rehabilitation following arthroscopic plica excision is the prevention of intra-articular adhesions and the restoration of normal quadriceps function.
Phase 1: Immediate Postoperative (Weeks 0-2)
- Weight-Bearing: Weight-bearing as tolerated (WBAT) with crutches. Crutches are typically weaned within the first 3 to 5 days as quad control returns.
- Range of Motion (ROM): Immediate initiation of active and passive ROM is critical. The patient should achieve full extension and at least 90 degrees of flexion by the end of week one to prevent the medial capsule from scarring down.
- Strengthening: Isometric quadriceps sets, straight leg raises (SLR), and ankle pumps.
- Edema Control: Cryotherapy and compression dressings.
Phase 2: Intermediate Rehabilitation (Weeks 2-6)
- Progression to full, symmetric ROM.
- Closed kinetic chain exercises (e.g., mini-squats, leg presses) are introduced, keeping flexion angles within a pain-free range.
- Stationary cycling is highly encouraged to promote synovial fluid circulation and maintain capsular mobility.
Phase 3: Return to Activity (Weeks 6-12)
- Progression to sport-specific or work-specific functional activities.
- Patients can generally return to high-impact activities and full sports participation between 6 to 8 weeks postoperatively, provided they have achieved full ROM, no effusion, and symmetric quadriceps strength.
CONCLUSION
Synovial plicae are common embryological remnants that, while usually benign, can transform into a significant source of anterior knee pain and articular cartilage degradation when subjected to trauma or chronic inflammation. A meticulous clinical examination, highlighted by the plica stutter test and differentiated from meniscal pathology, is essential for accurate diagnosis. When conservative measures such as NSAIDs, injections, and physical therapy fail, arthroscopic evaluation and complete surgical excision provide a highly successful, curative outcome. Surgeons must ensure complete resection of the fibrotic band to the synovial base to prevent recurrence and halt the progression of secondary chondral damage to the medial femoral condyle.
📚 Medical References
- synovial plicae of the knee: pathological signifi cance, diagnosis, and treatment by arthroscopic surgery, Ir Med J 78:279, 1985.
- Boyd CR, Eakin C, Matheson GO: Infrapatellar plica as a cause of anterior knee pain, Clin J Sport Med 15:98, 2005.
- Calpur OU, Tan L, Gurbuz H, et al: Arthroscopic mediopatellar plicaectomy and
You Might Also Like