Arthroscopic Management of Plica Syndrome and Osteochondritis Dissecans of the Knee
Key Takeaway
Arthroscopic management of synovial plica syndrome and osteochondritis dissecans (OCD) requires meticulous surgical staging and precise execution. Pathological plicae necessitate complete saucerization to alleviate patellofemoral impingement. Conversely, OCD treatment algorithms depend heavily on lesion stability, patient skeletal maturity, and fragment viability. Techniques range from retrograde drilling for intact lesions to complex osteochondral grafting and rigid internal fixation for unstable fragments, ensuring optimal joint preservation.
INTRODUCTION TO INTRA-ARTICULAR KNEE PATHOLOGIES
The arthroscopic management of intra-articular knee derangements demands a profound understanding of joint biomechanics, pathoanatomy, and evidence-based surgical algorithms. Among the most frequently encountered, yet distinctly different, pathologies are the pathological synovial plica and osteochondritis dissecans (OCD) of the femoral condyles and patellofemoral joint. While plica syndrome represents a soft-tissue impingement phenomenon derived from embryological remnants, OCD is a complex osteochondral defect driven by subchondral ischemia and mechanical overload.
This comprehensive masterclass delineates the precise surgical techniques, biomechanical considerations, and postoperative protocols required to manage these conditions successfully, ensuring joint preservation and the restoration of optimal kinematic function.
ARTHROSCOPIC RESECTION OF PATHOLOGICAL PLICA
Pathoanatomy and Biomechanics
Synovial plicae are normal embryological remnants of the synovial septae that divide the fetal knee into three distinct compartments. While typically asymptomatic, these structures can become pathological following trauma, repetitive microtrauma, or chronic inflammatory states. The medial patellar plica (often termed the "shelf") is the most frequently implicated in clinical pathology.
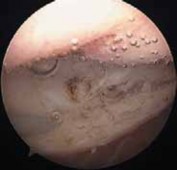
When inflamed, the plica transforms from a thin, translucent, and elastic membrane into a thickened, fibrotic, inelastic, and whitish band. During knee flexion, this fibrotic band bowstrings across the medial femoral condyle, causing mechanical impingement, localized chondromalacia, and anterior knee pain.
Diagnostic Arthroscopy and Indications
Surgical intervention is indicated only after the exhaustion of conservative measures (e.g., physical therapy, NSAIDs, corticosteroid injections) and when mechanical symptoms—such as snapping, catching, or focal medial joint line pain—persist.
A complete and systematic diagnostic arthroscopy must first be performed to rule out other intra-articular pathological conditions, such as meniscal tears or focal chondral defects.
Surgical Pearl: Do not resect a thin, asymptomatic plica incidentally found during arthroscopy for another pathology. Resection is strictly reserved for plicae that are visually thickened, inelastic, rounded, and demonstrate dynamic impingement on the medial femoral condyle during arthroscopic range-of-motion testing.
Step-by-Step Surgical Technique
- Portal Placement and Visualization:
Begin with the 30-degree viewing arthroscope in the standard anterolateral (AL) portal. Perform a comprehensive diagnostic sweep. Examine the medial patellar plica dynamically by taking the knee through a full range of motion, observing for impingement against the medial femoral condyle. - Superior Assessment:
To confirm the pathological nature and full extent of the plica, it is highly recommended to view its superior aspect through a superolateral (SL) portal. This provides a panoramic view of the suprapatellar pouch and the plica's origin. - Instrumentation and Resection:
With the viewing arthroscope maintained in the AL portal, establish a working portal. Scissors or basket forceps can be inserted through the SL portal, or side-biting basket forceps can be utilized through the anteromedial (AM) portal. - Saucerization:
Advance the cutting instrument to the medial side wall. Beginning at the superior aspect of the plica, systematically excise 1 to 2 cm of the fibrotic band. The ultimate goal of the treatment is a complete saucerization of the plica down to the synovial side wall. Simply transecting (cutting) the plica is insufficient and carries a high risk of recurrence and postoperative scarring. - Tension Release:
Often, the initial division of the plica is accompanied by a sudden "snapping apart" of the structure and a wide separation of its cut ends. This phenomenon visually confirms that the plica was under considerable pathological tension. - Debridement and Lavage:
If necessary, insert a motorized shaver or synovial resector through the SL or AM portal to remove the remaining tags of synovium and plica. - Joint Clearance:
Thoroughly lavage and suction the joint to remove any remaining debris, minimizing the risk of postoperative third-body wear or synovitis.
Surgical Warning: Avoid overly aggressive synovial resection beyond the footprint of the plica. Indiscriminate synovectomy significantly increases the risk of severe postoperative hemarthrosis, prolonged synovitis, and arthrofibrosis.
OSTEOCHONDRITIS DISSECANS (OCD) OF THE KNEE
Etiology and Patient Evaluation
Osteochondritis dissecans (OCD) of the knee is a focal, idiopathic alteration of subchondral bone with risk for instability and disruption of adjacent articular cartilage. While the exact etiology remains debated, it is widely considered a multifactorial process driven by localized subchondral ischemia, precipitated by repetitive microtrauma, infarction, or genetic predisposition.
The condition must be carefully differentiated from true acute osteochondral fractures and normal, irregular ossification centers often seen in the developing femoral condyles of children.
Prognostic Factors
The natural history and prognosis of OCD lesions are heavily dictated by several critical factors:
* Skeletal Maturity: Undisplaced lesions in skeletally immature children (open physes) have a high propensity to heal with conservative management (immobilization and activity modification). Conversely, surgery is almost always indicated for mature or near-mature patients.
* Patient Demographics: Age older than 30 to 45 years, obesity, and smoking negatively impact healing rates and long-term outcomes.
* Joint Mechanics: The condition of the surrounding cartilage, the viability of the meniscus, the stability of the knee ligaments, and the overall coronal/sagittal alignment of the lower extremity weigh heavily on the long-term success of any joint preservation procedure.
Radiographic and Advanced Imaging
Standard radiographic evaluation must include:
* 45-degree posteroanterior (PA) weight-bearing views (Rosenberg view).
* Weight-bearing lateral views.
* Patellofemoral (Merchant or sunrise) views.
* Contralateral knee radiographs (OCD lesions are bilateral in up to 25% of cases).
* Bone age films (e.g., left hand/wrist) to determine actual skeletal maturity.
Radiographically, lesions of the medial femoral condyle (the most common site) are classified by location: central, laterocentral, and inferocentral.
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the size of the lesion, the integrity of the overlying articular cartilage, and the presence of subchondral fluid (a hallmark sign of instability).
ARTHROSCOPIC CLASSIFICATION AND STAGE-SPECIFIC MANAGEMENT
Surgical treatment is dictated by the arthroscopic examination, which remains the ultimate arbiter of lesion stability. Lesions are classified into four distinct groups, each requiring a specific surgical algorithm.
Group 1: Intact Lesions
An intact lesion presents with only a minor irregularity or softening of the articular surface, with absolutely no break in the continuity of the cartilage. Because the surface may appear visually normal, careful tactile palpation and probing are mandatory to identify the softened, "ballotable" defect.
- Surgical Technique (Drilling): The goal is to stimulate angiogenesis and cellular migration into the avascular fragment. This is achieved by drilling multiple holes through the articular surface, penetrating the subchondral fragment, and advancing into the underlying healthy, vascularized cancellous bone.
- Retrograde Drilling: In skeletally immature patients where preservation of the articular surface is paramount, retrograde extra-articular drilling is preferred. Using an image intensifier (fluoroscopy), a guide pin is advanced from the extra-articular cortex, distal to the open physis, directly into the subchondral lesion without breaching the articular cartilage.
Group 2: Lesions Showing Signs of Early Separation
These lesions present with an essentially intact and smooth articular surface, but exhibit greater irregularity than Group 1. Crucially, the articular surface shows a focal break or fissure at the periphery, and the fragment moves significantly when manipulated with an arthroscopic probe.
- Surgical Technique (Fixation): The treatment objective is fragment stabilization to promote bony union. The peripheral break is carefully debrided to remove fibrous interposition. The fragment is then secured using bioabsorbable pins/screws or metallic headless compression screws.
- Implant Selection: Screws offer the distinct biomechanical advantage of active fragment compression, which is highly beneficial for larger lesions. However, metallic screws typically require a secondary surgical procedure for removal once clinical and radiographic healing is achieved.
Group 3: Partially Detached Lesions
A partially detached lesion presents with a gross disruption of the articular surface. Upon probing, the lesion can be displaced or hinged open like a "trapdoor" on one intact edge.
- Surgical Technique (Trapdoor Reconstruction):
- Gently hinge the fragment open to expose the underlying subchondral crater.
- Meticulously debride the crater base using a curette to remove all fibrous tissue down to healthy, bleeding bone (stimulating petechial bleeding).
- If a significant volumetric void exists, pack the crater base with autologous cancellous bone graft (often harvested from the proximal tibia or distal femur).
- Reduce the fragment congruously and secure it with rigid internal fixation (compression screws).
Clinical Pitfall: Failure to adequately debride the fibrous base of a partially detached lesion will result in a non-union, regardless of the rigidity of the fixation applied. Petechial bleeding is the absolute prerequisite for osteointegration.
Group 4: Craters with Loose Bodies
When viewed arthroscopically, these lesions have already progressed to complete detachment, leaving a subchondral crater and a free-floating intra-articular loose body. Treatment depends entirely on the viability of the loose fragment.
- Salvageable Fragments: If the loose body has detached recently (indicated by acute hemorrhage or minimal fibrous encapsulation) and contains viable cartilage with attached subchondral bone, it should be preserved. The crater is reconstructed via curettage and debridement. The fragment is trimmed, the crater is bone-grafted if necessary, and the fragment is congruously reduced and stabilized. Studies (e.g., Magnussen et al.) demonstrate that successfully reattached viable fragments heal in more than 90% of patients.
- Unsalvageable Fragments: If the loose body is fragmented, deformed, or chronically avascular, it must be excised. The remaining crater is then treated based on its size and patient demands:
- Microfracture: Suitable for small lesions (< 2 cm²) in lower-demand patients.
- Osteochondral Autograft Transfer System (OATS): Ideal for small to medium lesions, utilizing cylindrical osteochondral plugs harvested from non-weight-bearing regions of the knee.
- Autologous Chondrocyte Implantation (ACI / MACI): Reserved for large, uncontained defects.
OSTEOCHONDRITIS DISSECANS OF THE PATELLOFEMORAL JOINT
OCD of the patella is less common but presents unique biomechanical challenges. It typically occurs on the medial or lateral facet, the central ridge, or the corresponding aspects of the femoral trochlea.
Surgical Management of Patellar OCD
- First-Line Treatment: For localized, symptomatic lesions, the initial arthroscopic approach involves meticulous debridement of unstable cartilage flaps followed by microfracture of the exposed subchondral bone to stimulate a fibrocartilage healing response.
- Second-Line Treatment (Refractory Cases): For persistent mechanical symptoms, chronic swelling, and pain that fails to respond to microfracture, more aggressive open intervention is required in the skeletally mature individual.
- Biomechanical Offloading: A critical component of treating refractory patellofemoral OCD is altering the joint contact mechanics. An Anterior Medialization of the Tibial Tuberosity (AMZ / Fulkerson Osteotomy) is often indicated to mechanically offload the affected facet.
- Cartilage Restoration: Concurrently with the AMZ, the focal defect is treated with an autogenous osteochondral transplant (OATS) or structural allograft via an open arthrotomy, ensuring a congruous articular surface capable of withstanding patellofemoral shear forces.
POSTOPERATIVE REHABILITATION PROTOCOLS
The success of OCD surgery is inextricably linked to strict adherence to postoperative rehabilitation.
- Weight-Bearing Status: For lesions treated with internal fixation (Groups 2, 3, and salvageable Group 4), strict non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) is mandatory for approximately 6 weeks to protect the fixation and allow initial osteointegration.
- Range of Motion (ROM): Early, protected passive range of motion (often via Continuous Passive Motion [CPM] machines) is encouraged to nourish the articular cartilage and prevent arthrofibrosis, provided the ROM does not place undue shear stress on the specific lesion site.
- Return to Play: Return to high-impact sports is delayed until complete radiographic union is confirmed via MRI or CT, and symmetrical lower extremity strength is achieved, typically requiring 6 to 9 months postoperatively. Plica resections, conversely, follow an accelerated protocol, with immediate weight-bearing and early return to activity as tolerated by pain and swelling.
📚 Medical References
- knee osteochondritis dissecans: a preliminary experience, Am J Sports Med 26:7:1998.
- Patel N, Weiner SD: Osteochondritis dissecans involving the trochlea: report of two patients (three elbows) and review of the literature, J Pediatr Orthop 22:48, 2002.
- Peters TA, McLean ID: Osteochondritis dissecans of the patellofemoral joint, Am J Sports Med 28:63, 2000.
- Peterson RK, Savoie FH, Field LD: Osteochondritis dissecans of the elbow, Instr Course Lect 48:393, 1999.
- Pinar H, Gül Ö, Boya H, et al: Osteochondrosis of the primary ossifi cation center of the patella (Köhler’s disease of the patella): report of three cases, Knee Surg Sports Traumatol Arthrosc 10:141, 2002.
- Ralph BG, Barrett J, Kenyhercz C, et al: Iselin’s disease: a case presentation of nonunion and review of the differential diagnosis, J Foot Ankle Surg 38:409, 1999.
- Rapp IH, Lazerte G: Clinical pathological correlation in OsgoodSchlatter’s disease, South Med J 51:909, 1958.
- Roberts JM: Fractures and separations of the knee. In Rockwood CA Jr, Wilkins KE, King RE, eds: Fractures in children, 3rd ed, Philadelphia, 1991, Lippincott. Robertsen K, Krsitensen O, Sommer J: Pseudoarthrosis between a patellar tendon ossicle and the tibial tuberosity in OsgoodSchlatter’s disease, Scand J Med Sci Sports 6:57, 1996.
- Ruch DS, Cory JW, Poehling GG: The arthroscopic management of osteochondritis dissecans of the adolescent elbow, Arthroscopy 14:797, 1998.
- Safran MR, McDonough P, Seeger L, et al: Dorsal defect of the patella, J Pediatr Orthop 14:603, 1994.
- Schenck RC, Goodnight JM: Current concepts review: osteochondritis dissecans, J Bone Joint Surg 78A:439, 1996.
- Slawski DP: High tibial osteotomy in the treatment of adult osteochondritis dissecans, Clin Orthop Relat Res 341:155, 1997.
- Smillie IS: Freiberg’s infraction (Köhler’s second disease), J Bone Joint Surg 39B:580, 1957.
- Sueyoshi Y, Shimozaki E, Matsumoto T, et al: Two cases of dorsal defect of the patella with arthroscopically visible cartilage surface perforations, Arthroscopy 9:164, 1993.
- Takahara M, Ogino T, Fukushima S, et al: Nonoperative treatment of osteochondritis dissecans of the humeral capitellum, Am J Sports Med 27:728, 1999.
- Takahara M, Ogino T, Sasaki I, et al: Long-term outcome of osteochondritis dissecans of the humeral capitellum, Clin Orthop Relat Res 363:108, 1999.
- Takahara M, Ogino T, Takagi M, et al: Natural progression of osteochondritis dissecans of the humeral capitellum: initial observations, Radiology 216:207, 2000 . Takeda H, Watarai K, Matsushita T, et al: A surgical treatment for unstable osteochondritis dissecans lesions of the humeral capitellum in adolescent baseball players, Am J Sports Med 30:713, 2002.
- Taranow WS, Bisignani GA, Towers JD, et al: Retrograde drilling of osteochondral lesions of the medial talar dome, Foot Ankle Int 20:474, 1999.
- Thomee R, Augustsson J, Karlsson J: Patellofemoral pain syndrome: a review of current issues, Sports Med 28:245, 1999.
- Thompson MS, Dickinson PH: Osgood-Schlatter’s disease in the army, Int Surg 23:170, 1955.
- Thomson JEM: Operative treatment of osteochondritis of the tibial tubercle, J Bone Joint Surg 38A:142, 1956.
- Tol JL, Struijs PAA, Bossuyt PMM, et al: Treatment strategies in osteochondral defects of the talar dome: a systematic review, Foot Ankle 21:120, 2000.
- Trial IA: Tibial sequestrectomy in the management of OsgoodSchlatter disease, J Pediatr Orthop 8:554, 1988.
- Tullos JS, King JW: Lesions of the pitching arm in adolescents, JAMA 220:264, 1972.
- Tuompo P, Arvela V, Partio EK, et al: Osteochondritis dissecans of the knee fi xed with biodegradable self-reinforced polyglycolide and polylactide rods in 24 patients, Int Orthop 21:355, 1997.
- Tyler W, McCarthy EF: Osteochondrosis of the superior pole of the patella: two cases with histologic correlation, Iowa Orthop J 22:86, 2002.
- Victoroff BM, Marcus RE, Deutsch A: Arthroscopic bone peg fi xation in the treatment of osteochondritis dissecans in the knee, Arthroscopy 12:506, 1996.
- Waugh W: The ossifi cation and vascularization of the tarsal navicular and their relation to Köhler’s disease, J Bone Joint Surg 40B:765, 1958.
- Wood JB, Klassen RA, Peterson HA: Osteochondritis dissecans of the femoral head in children and adolescents: a report of 17 cases, J Pediatr Orthop 15:313, 1995.
- Woodward AH, Bianco AJ Jr: Osteochondritis dissecans of the elbow, Clin Orthop Relat Res 110:35, 1975.
- Yashar A, Loder RT, Hensinger RN: Determination of skeletal age in children with Osgood-Schlatter disease by using radiographs of the knee, J Pediatr Orthop 15:298, 1995.
- Yoshida S, Ikata T, Takai H, et al: Osteochondritis dissecans of the femoral condyle in the growth stage, Clin Orthop Relat Res 346:162, 1998.
- Young MC, Fornasier VL, Cameron HU: Osteochondral disruption of the second metatarsal: a variant of Freiberg’s infraction? Foot Ankle Int 8:103, 1987.
- Zimbler S, Menkow S: Genu recurvatum: a possible complication after Osgood-Schlatter’s disease, J Bone Joint Surg 66A:1129, 1984.
You Might Also Like