Radiographic Evaluation and Surgical Planning for Patellofemoral Disorders

Key Takeaway
The radiographic evaluation of the patellofemoral joint requires a systematic approach utilizing anteroposterior, true lateral, and axial views. Accurate measurement of patellar height indices, such as the Insall-Salvati ratio, and assessment of trochlear dysplasia via Dejour's criteria are paramount. Advanced imaging, including CT for TT-TG distance and MRI for MPFL integrity, dictates the surgical algorithm, guiding interventions like tibial tubercle osteotomy or medial patellofemoral ligament reconstruction in cases of recurrent instability.
Introduction to Patellofemoral Biomechanics and Imaging
The patellofemoral joint is a complex articulation governed by an intricate balance of static and dynamic stabilizers. The patella functions primarily as a biomechanical fulcrum, increasing the moment arm of the quadriceps mechanism and enhancing extension torque. Pathologies of the patellofemoral joint—ranging from anterior knee pain syndromes to recurrent patellar instability and advanced arthropathy—require a meticulous, evidence-based approach to radiographic evaluation.
For the orthopedic surgeon, interpreting these imaging modalities is not merely a diagnostic exercise but the foundational step in preoperative planning. A comprehensive understanding of patellar height, trochlear morphology, and dynamic tracking is essential for determining the appropriate surgical intervention, whether it be a soft-tissue reconstruction or a complex bony realignment.
Standard Radiographic Evaluation
A standard radiographic series for the evaluation of the patellofemoral joint must include an anteroposterior (AP) view, a true lateral view, and an axial (skyline/Merchant) view.
The Anteroposterior (AP) View
While the AP radiograph rarely provides definitive information regarding dynamic patellofemoral tracking problems, it remains a critical baseline study.
* Bipartite Patella: Often seen in the superolateral quadrant, this is a normal variant that must be differentiated from an acute fracture.
* Osteochondral Defects: Occasionally, an osteochondral fracture of the medial patellar edge or the lateral femoral condyle can be visualized following an acute dislocation.
* Loose Bodies: Intra-articular radiopaque loose bodies may be present, necessitating arthroscopic removal.
The True Lateral View
The lateral view of the knee is arguably the most informative plain radiograph for assessing patellar height and trochlear dysplasia. A true lateral radiograph—defined by the perfect superimposition of the posterior femoral condyles—is mandatory.
Assessing Patellar Height
Patella alta (a high-riding patella) is a primary risk factor for patellofemoral instability, as it delays the engagement of the patella into the stabilizing bony confines of the trochlear groove during early flexion.
- Blumensaat’s Line: Originally, Blumensaat demonstrated that with the knee flexed to 30 degrees, a line extending through the intercondylar notch should tangentially touch the inferior pole of the patella. However, contemporary literature has proven this to be an inexact and highly variable index.
- Insall-Salvati Ratio: In a landmark review of normal knees, Insall and Salvati established that the ratio of the length of the patellar tendon (LT) to the diagonal length of the patella (LP) is normally 1.0, with less than 20% variation.
Clinical Pearl: Patella alta is diagnosed when the LT exceeds the LP by more than 20% (an Insall-Salvati ratio of ≥ 1.2). Conversely, patella baja (infera) is present when the ratio is ≤ 0.8.
- Blackburne-Peel Index: To eliminate the variability of the tibial tubercle insertion, Blackburne and Peel described a ratio utilizing the articular surface of the patella. The ratio is calculated by dividing the perpendicular distance from the inferior articular margin of the patella to the tibial plateau by the length of the patellar articular surface. Normal values range between 0.54 and 1.06.
Evaluating Trochlear Dysplasia (Dejour Criteria)
Dejour revolutionized the understanding of patellofemoral instability by defining trochlear dysplasia on a true lateral radiograph taken at 20 degrees of flexion.
* Trochlear Depth: Measured 1 cm proximal to the deepest part of the groove, normal depth should be ≥ 5 mm.
* The Crossing Sign: Pathognomonic for dysplasia, this occurs when the anterior cortical outline of the femoral condyle intersects the floor of the trochlear groove.
* Supratrochlear Spur (Trochlear Bump): A bony prominence where the trochlear floor extends anterior to the anterior femoral cortex, acting as a mechanical block to patellar engagement.
* Double Contour Sign: Indicates a hypoplastic medial facet, where the anterior margin of the lateral condyle is seen anterior to the medial condyle.
The Axial (Skyline) View
The axial view is the most important routine projection for assessing the dynamic relationship of the patellofemoral joint. Several techniques exist (Merchant, Laurin, Sunrise), but standardization is key.
Surgical Warning: The knee must be flexed between 20 and 45 degrees. Flexion beyond 45 degrees drives the patella deep into the trochlear groove, artificially reducing subluxation and masking subtle instability.
For the radiograph to be clinically meaningful:
1. Both knees must be exposed simultaneously for contralateral comparison.
2. The x-ray beam must be perpendicular to the cassette to prevent geometric distortion.
3. The lower extremities must be held vertically to prevent external rotation, which can falsely simulate a hypoplastic lateral femoral condyle.
4. The quadriceps must be completely relaxed.
When evaluating the axial view, the surgeon must assess the congruence angle, lateral patellofemoral angle, and patellar tilt. Normally, the patella is evenly seated within the trochlear sulcus, with symmetric joint space between the medial and lateral facets and the corresponding femoral surfaces.
Abnormalities manifest as lateral patellar tilt, lateral subluxation, or complete dislocation. Progressive lateral tilt causes the median ridge of the patella to superimpose on the lateral facet, ultimately displacing posterior to it in severe cases.
Advanced Cross-Sectional Imaging
While plain radiographs provide the foundation, advanced imaging is mandatory for surgical planning in cases of recurrent instability or complex malalignment.
Computed Tomography (CT)
CT is the gold standard for evaluating bony architecture and rotational alignment.
* Tibial Tubercle-Trochlear Groove (TT-TG) Distance: This measurement quantifies the lateralization of the tibial tubercle relative to the deepest portion of the trochlear groove. Axial slices are superimposed.
* Normal: < 10 mm.
* Borderline: 10 - 15 mm.
* Pathologic: > 20 mm (A strict indication for distal realignment via Tibial Tubercle Osteotomy).
* Rotational Profile: CT allows for the measurement of femoral anteversion and tibial torsion. Excessive femoral anteversion combined with external tibial torsion ("miserable malalignment syndrome") drastically increases the lateral biomechanical vector on the patella.
Magnetic Resonance Imaging (MRI)
MRI is the modality of choice for acute dislocations, particularly in high-level athletes, and for evaluating soft-tissue integrity.
* Medial Patellofemoral Ligament (MPFL): The primary static restraint to lateral patellar translation at 0-30 degrees of flexion. MRI accurately identifies the location of the tear (femoral origin, mid-substance, or patellar insertion), which dictates the surgical approach.
* Bone Bruising Patterns: A classic "kissing contusion" pattern on the anterolateral aspect of the lateral femoral condyle and the inferomedial patella is pathognomonic for a recent transient lateral dislocation.
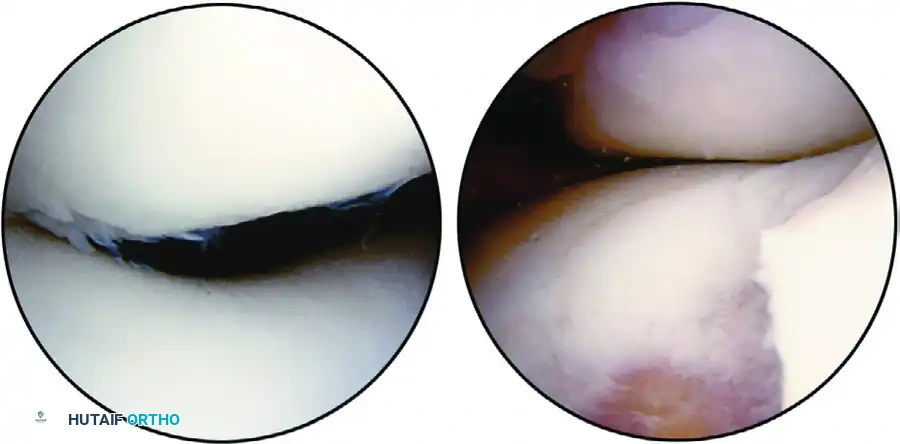
* Chondral Surfaces: High-resolution MRI sequences map the size, depth, and location of osteochondral lesions, guiding the need for concurrent cartilage restoration procedures (e.g., OATS, MACI).
Surgical Decision Making and Operative Approaches
The synthesis of clinical examination and radiographic findings dictates the surgical algorithm. Isolated soft-tissue procedures are doomed to fail if underlying bony malalignment (TT-TG > 20mm, severe patella alta, or high-grade dysplasia) is ignored.
Distal Realignment: Tibial Tubercle Osteotomy (TTO)
Indications: Recurrent patellofemoral instability with a TT-TG distance > 20 mm, patella alta (Insall-Salvati > 1.2), or focal distal/lateral patellar chondral defects requiring offloading.
Positioning and Setup:
1. The patient is positioned supine on a radiolucent operating table.
2. A high thigh tourniquet is applied.
3. A lateral post or sandbag is placed to control hip rotation, allowing the knee to flex freely to 90 degrees.
Step-by-Step Surgical Approach (Fulkerson Anteromedialization):
1. Incision: A longitudinal incision is made just lateral to the tibial crest, extending from the distal pole of the patella to 5-7 cm distal to the tibial tubercle.
2. Exposure: The anterior compartment musculature (tibialis anterior) is elevated off the lateral aspect of the tibia. A retractor is carefully placed to protect the deep peroneal nerve and anterior tibial artery.
3. Osteotomy Design: Using an oscillating saw, an oblique osteotomy is performed. The angle of the cut determines the ratio of anteriorization to medialization. A steeper angle (e.g., 60 degrees to the coronal plane) provides more anteriorization (offloading), while a shallower angle provides more medialization (instability correction).
4. Translation: The osteotomized bone block (at least 5-7 cm in length to prevent fracture) is translated medially and/or anteriorly based on preoperative TT-TG calculations.
5. Fixation: The tubercle is temporarily pinned with K-wires. Fixation is achieved using two or three 4.5 mm fully threaded cortical lag screws directed from anterior to posterior, engaging the posterior tibial cortex.
6. Closure: The wound is closed in layers over a suction drain to prevent hematoma formation.
Proximal Realignment: MPFL Reconstruction
Indications: Recurrent lateral patellar instability with a normal TT-TG distance (< 15 mm), normal patellar height, and MRI-confirmed MPFL incompetence.
Step-by-Step Surgical Approach:
1. Graft Harvest: A semitendinosus or gracilis autograft is harvested and prepared. Alternatively, an allograft may be utilized to decrease donor-site morbidity.
2. Patellar Fixation: A small incision is made over the superomedial border of the patella. The graft is secured to the upper half of the medial patella using suture anchors or transosseous tunnels.
3. Femoral Isometric Point (Schöttle’s Point): Fluoroscopy is utilized to identify the anatomic femoral origin of the MPFL. On a true lateral radiograph, this point is located 1 mm anterior to the posterior cortical line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to the level of the posterior point of Blumensaat’s line.
4. Graft Passage: The graft is passed extra-articularly but deep to the medial retinaculum, from the patella to the femoral footprint.
5. Tensioning and Fixation:
> Surgical Pitfall: Over-tensioning the MPFL graft is the most common cause of failure, leading to medial compartment overload, severe pain, and iatrogenic medial subluxation.
The graft must be tensioned with the knee at 30 degrees of flexion. It should act as a check-rein, not a tight medializing force. Fixation is typically achieved with an interference screw in the femoral tunnel.
Postoperative Protocols and Rehabilitation
Successful outcomes in patellofemoral surgery rely heavily on strict adherence to phased, evidence-based rehabilitation protocols.
Phase I: Maximum Protection (Weeks 0-2)
- Weight Bearing: Weight-bearing as tolerated (WBAT) with the knee locked in full extension in a hinged knee brace.
- Range of Motion (ROM): ROM is restricted to 0-30 degrees to protect the MPFL graft and/or the TTO fixation.
- Therapeutic Exercise: Isometric quadriceps sets, straight leg raises (in the brace), and ankle pumps to prevent deep vein thrombosis.
Phase II: Moderate Protection (Weeks 2-6)
- Weight Bearing: Continue WBAT in the locked brace for ambulation.
- ROM: Gradual progression of flexion. Goal is 90 degrees by week 4, and 120 degrees by week 6.
- Therapeutic Exercise: Initiate closed kinetic chain exercises (e.g., mini-squats, leg press) within the pain-free and protected ROM arc. Open kinetic chain knee extension is strictly avoided to prevent shear stress on the patellofemoral joint and osteotomy site.
Phase III: Early Return to Function (Weeks 6-12)
- Bracing: The hinged knee brace is gradually weaned as quadriceps control normalizes (absence of extensor lag).
- Imaging: For TTO patients, AP and lateral radiographs are obtained at 6 weeks to confirm bony union before progressing to heavy resistance training.
- Therapeutic Exercise: Advance closed chain strengthening, initiate proprioceptive training (BOSU ball, balance board), and begin stationary cycling with progressive resistance.
Phase IV: Return to Sport (Months 3-6+)
- Criteria for Progression: Full, painless ROM; radiographic union of osteotomies; quadriceps strength > 85% of the contralateral limb; and no effusion.
- Therapeutic Exercise: Plyometric training, sport-specific agility drills, and cutting maneuvers. Return to competitive play is typically cleared between 5 to 7 months postoperatively, contingent upon passing functional hop testing and psychological readiness assessments.
You Might Also Like