Posterior Capsulotomy of the Knee: Comprehensive Surgical Technique and Principles
Key Takeaway
Posterior capsulotomy of the knee is a salvage procedure indicated for severe, recalcitrant flexion contractures that have failed conservative management. This comprehensive guide details the modified Putti technique, encompassing precise patient positioning, neurovascular protection, and stepwise capsular release. By systematically addressing the posterior capsular structures, gastrocnemius heads, and contracted hamstrings, surgeons can safely restore knee extension while minimizing the risk of iatrogenic neurovascular injury.
INTRODUCTION TO POSTERIOR CAPSULOTOMY
Severe flexion contractures of the knee present a formidable challenge to the orthopaedic surgeon. When conservative measures—such as serial casting, dynamic splinting, and aggressive physical therapy—fail to yield functional extension, surgical intervention becomes necessary. The posterior capsulotomy is a powerful, albeit technically demanding, procedure designed to release the tethering posterior structures of the knee joint.
Originally described by Putti and subsequently modified to enhance safety and efficacy, this procedure systematically addresses the posterior joint capsule, the origins of the gastrocnemius, and, when necessary, the hamstring tendons and the posterior cruciate ligament (PCL). This masterclass details the pathoanatomy, preoperative considerations, and the step-by-step surgical execution of the modified Putti posterior capsulotomy, alongside modern supine alternatives.
PATHOANATOMY AND BIOMECHANICS OF KNEE FLEXION CONTRACTURES
A thorough understanding of the posterior knee anatomy is paramount. Flexion contractures rarely involve a single anatomical structure; rather, they represent a synergistic shortening of multiple tissues over time.
The Posterior Capsular Complex
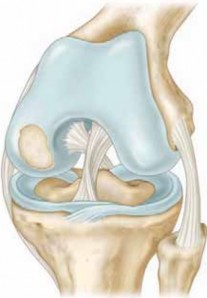
The posterior capsule of the knee is a robust, fibrous structure reinforced by several key ligaments:
* Oblique Popliteal Ligament: An expansion of the semimembranosus tendon that courses superolaterally across the posterior joint.
* Arcuate Ligament Complex: Located posterolaterally, reinforcing the capsule over the popliteus tendon.
* Posterior Cruciate Ligament (PCL): While primarily a central pivot structure, a chronically contracted PCL acts as a secondary restraint to full extension.
Musculotendinous Contractures
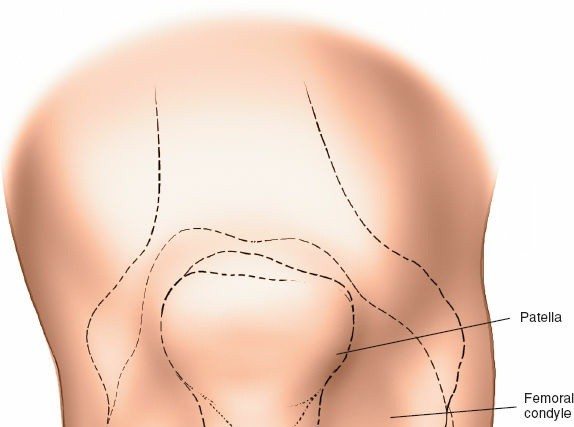
In chronic flexion deformities, the musculotendinous units crossing the posterior knee undergo adaptive shortening. The medial and lateral heads of the gastrocnemius, which originate on the posterior femoral condyles, become primary tethers. Furthermore, the hamstring tendons (biceps femoris laterally; semimembranosus and semitendinosus medially) and the iliotibial band (ITB) exacerbate the deformity and must often be addressed concurrently.
💡 Clinical Pearl: The "Bowstring" Effect
In severe, long-standing flexion contractures, the popliteal neurovascular bundle acts as a bowstring across the popliteal fossa. Acute, forceful correction of the deformity places immense traction on the popliteal artery and the common peroneal nerve, risking intimal arterial tears or profound neuropraxia.
INDICATIONS AND CONTRAINDICATIONS
Indications
- Severe, rigid flexion contractures of the knee (typically >30 degrees) that are recalcitrant to conservative management.
- Contractures secondary to inflammatory arthropathies (e.g., juvenile idiopathic arthritis, rheumatoid arthritis) where joint preservation is still viable.
- Post-traumatic contractures following prolonged immobilization or severe intra-articular fractures.
- Neuromuscular disorders (e.g., cerebral palsy, poliomyelitis) resulting in fixed myostatic contractures.
Contraindications
- Absolute: Active joint infection, severe peripheral vascular disease (which precludes safe stretching of the popliteal artery), and advanced joint destruction where arthrodesis or total knee arthroplasty (TKA) is more appropriate.
- Relative: Poor soft tissue envelope over the popliteal fossa, or a patient unable to comply with rigorous postoperative rehabilitation.
PREOPERATIVE PLANNING
Meticulous preoperative planning is required to mitigate the high risks associated with popliteal surgery.
* Clinical Assessment: Document the exact degree of fixed flexion and the arc of motion. Assess the resting tension of the hamstrings and the ITB.
* Neurovascular Examination: Baseline documentation of distal pulses (dorsalis pedis, posterior tibial) and neurological function (particularly common peroneal nerve distributions) is mandatory.
* Imaging: Weight-bearing anteroposterior, lateral, and skyline radiographs evaluate joint space narrowing and osteophyte formation. Magnetic Resonance Imaging (MRI) may be utilized to assess the integrity of the articular cartilage and the exact thickness of the posterior capsular scar tissue.
SURGICAL TECHNIQUE: THE MODIFIED PUTTI PROCEDURE
The traditional approach to the posterior capsulotomy is performed with the patient in the prone position, allowing direct, unhindered access to the popliteal fossa.
Patient Positioning and Anesthesia
- Anesthesia: General anesthesia with profound muscle relaxation is preferred to eliminate dynamic muscle guarding during the manipulation phase.
- Positioning: Place the patient prone on a radiolucent operating table. Pad all bony prominences meticulously. A high-thigh tourniquet is applied but should be inflated only after exsanguination, keeping in mind that tourniquet time must be strictly monitored.
Incision and Superficial Dissection
- Make a curvilinear (S-shaped or lazy-Z) incision approximately 15 cm long over the popliteal space. The incision should cross the popliteal crease obliquely to prevent postoperative scar contracture.
- Incise the skin and superficial fascia. Raise full-thickness fasciocutaneous flaps to expose the deep popliteal fascia.
⚠️ Surgical Warning: Incision Placement
Never use a straight longitudinal incision across the popliteal crease. A straight scar in this flexion crease will inevitably hypertrophy and contract, causing a secondary iatrogenic flexion contracture.
Lateral Compartment Release
The posterior capsule is approached via two separate windows (medial and lateral) to avoid direct midline dissection through the neurovascular bundle.
- Deep Fascial Incision: Dissect between the subcutaneous tissue and the deep fascia toward the lateral aspect of the popliteal space. Incise the deep fascia longitudinally.
- Nerve Identification: Isolate the common peroneal nerve (CPN) as it courses parallel to the medial border of the biceps femoris tendon. Gently loop the nerve with a vessel loop for continuous identification. Retract the CPN and the biceps femoris tendon laterally.
- Vascular Retraction: Identify the popliteal vessels and the tibial nerve in the midline. Gently retract these structures medially using smooth, blunt retractors (e.g., Army-Navy or malleable retractors).
- Capsular and Muscular Division: Under direct vision, identify the lateral head of the gastrocnemius. Divide its tendinous origin from the lateral femoral condyle. Proceed deep to the gastrocnemius to expose the lateral half of the posterior capsule. Divide the capsule transversely just proximal to the joint line. If the posterior cruciate ligament (PCL) is severely contracted and preventing extension, its femoral attachment may be carefully released at this stage.
Medial Compartment Release
- Medial Dissection: Shift the focus to the medial aspect of the popliteal space. Dissect between the subcutaneous tissue and the deep fascia.
- Muscular Retraction: Incise the deep fascia to expose the lateral aspect of the semimembranosus and semitendinosus muscles. Retract these hamstring muscles medially.
- Neurovascular Protection: Retract the midline popliteal vessels and the tibial nerve laterally.
- Capsular Division: Identify and divide the medial head of the gastrocnemius at its origin on the medial femoral condyle. Expose and divide the medial half of the posterior capsule, ensuring the transverse capsulotomy connects with the lateral release.
Deformity Correction and Manipulation
Once the posterior capsule, gastrocnemius origins, and (if necessary) the PCL have been divided, the knee is ready for extension.
- Gentle Manipulation: Gradually and gently extend the knee. If the hamstring tendons are not severely contracted, the knee may reach full extension.
- Audible Rupture: During this slow extension, the surgeon may hear or feel the audible rupture of deep intra-articular fibrous adhesions. This is normal, but force must be strictly controlled.
🛑 Pitfall: The Danger of Excessive Force
Do not use the tibia as a long lever arm to forcefully crack the knee into extension. Excessive force can lead to distal femoral physeal fractures (in pediatric patients), supracondylar fractures, or catastrophic rupture of the popliteal artery. If the knee does not extend with gentle pressure, look for residual tethering structures.
Adjunctive Soft Tissue Procedures
In cases of long-standing deformity, releasing the capsule alone is insufficient.
* Hamstring Lengthening: If the biceps femoris, semitendinosus, and semimembranosus are severely contracted, perform a fractional lengthening or a formal Z-plasty of these tendons.
* Yount’s Procedure: If the iliotibial band (ITB) is a deforming force (often contributing to external tibial torsion and valgus), divide the ITB and the lateral intermuscular septum just proximal to the lateral femoral condyle, as described by Yount.
ALTERNATIVE APPROACH: THE SUPINE DUAL-INCISION TECHNIQUE
While the prone position offers excellent exposure of the popliteal fossa, it precludes simultaneous access to the anterior compartment of the knee. Modern orthopaedic practice frequently utilizes a supine approach with limited medial and lateral incisions.
Advantages of the Supine Approach
- Allows the patient to remain supine throughout the operation.
- Facilitates concurrent anterior procedures, such as arthroscopic lysis of adhesions, anterior compartment synovectomy, or patellar realignment.
- Permits easier assessment of overall limb alignment and patellar tracking during the correction.
Technique Execution
- Medial Incision: A longitudinal incision is made anterior to the medial hamstring tendons. The medial capsule and medial gastrocnemius are accessed by retracting the hamstrings posteriorly and the medial collateral ligament (MCL) anteriorly.
- Lateral Incision: A longitudinal incision is made anterior to the biceps femoris. The common peroneal nerve is identified and protected. The lateral capsule and lateral gastrocnemius are accessed by retracting the biceps posteriorly and the ITB anteriorly.
- Capsulotomy: The capsule is elevated off the posterior femur using periosteal elevators (e.g., Cobb elevators) from both the medial and lateral sides until the dissection meets in the midline, effectively stripping the posterior capsule away from the bone.
COMPLICATIONS AND RISK MANAGEMENT
Posterior capsulotomy is a high-stakes procedure with a narrow margin for error. Surgeons must be vigilant regarding the following complications:
- Common Peroneal Nerve Palsy: The CPN is highly sensitive to stretch. If the preoperative flexion contracture exceeds 45 degrees, acute correction to 0 degrees is contraindicated. The nerve will suffer traction neuropraxia. In such cases, correct the knee to 15-20 degrees of flexion intraoperatively and achieve the remaining extension postoperatively via serial casting.
- Popliteal Artery Injury: The popliteal artery is tethered by the superior and inferior genicular arteries. Acute extension can cause intimal tearing, leading to delayed thrombosis and limb ischemia. Always deflate the tourniquet prior to wound closure to confirm robust distal perfusion with the knee in its newly extended position.
- Wound Dehiscence and Skin Necrosis: The posterior skin, accustomed to a flexed posture, may blanch and become ischemic when the knee is fully extended. If skin tension is excessive, the knee must be splinted in slight flexion to allow the skin to accommodate over time.
- Recurrence of Contracture: Fibroblastic proliferation in the popliteal space is aggressive. Without rigorous postoperative bracing and physical therapy, the contracture will inevitably recur.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of a posterior capsulotomy relies as much on postoperative care as it does on surgical execution.
Immediate Postoperative Phase (Days 0-7)
- Immobilization: The knee is immobilized in a well-padded posterior splint or a bivalved cast in maximum safe extension (determined intraoperatively based on skin tension and neurovascular status).
- Neurovascular Monitoring: Hourly checks of pedal pulses, capillary refill, and CPN function (extensor hallucis longus strength and first webspace sensation) are mandatory for the first 24-48 hours.
- Pain Management: Adequate analgesia, often utilizing regional nerve blocks (e.g., adductor canal block) or epidural anesthesia, is critical to prevent reflex muscle spasm.
Intermediate Phase (Weeks 1-6)
- Continuous Passive Motion (CPM): If wound healing is satisfactory, CPM may be initiated to prevent intra-articular adhesion formation.
- Dynamic Splinting: Transition to a dynamic extension splint (e.g., Dynasplint or JAS brace) to provide a low-load, prolonged stretch to the posterior structures.
- Physical Therapy: Aggressive active and active-assisted range of motion exercises are instituted. Quadriceps strengthening is vital, as a strong extensor mechanism is required to maintain the surgical correction.
Long-Term Management
- Night Splinting: Patients should continue to wear an extension splint at night for 6 to 12 months postoperatively to prevent nocturnal flexion posturing and recurrence of the contracture.
- Weight-Bearing: Weight-bearing is generally allowed as tolerated in an extension brace, which further assists in maintaining the correction through the mechanical force of gravity and body weight.
CONCLUSION
The posterior capsulotomy remains an indispensable technique in the orthopaedic armamentarium for addressing severe knee flexion contractures. Whether utilizing the classic prone modified Putti technique or the modern supine dual-incision approach, success hinges on a profound understanding of popliteal anatomy, meticulous surgical dissection, and a disciplined, phased approach to deformity correction. By respecting the neurovascular constraints and committing to rigorous postoperative rehabilitation, surgeons can safely restore limb alignment and significantly improve patient function.
📚 Medical References
- posterior capsulotomy, and quadri- ceps mechanism shortening, Dev Med Child Neurol 43:802, 2001.
- Drummond DS, Rogala E, Templeton J, et al: Proximal hamstring release for knee fl exion and crouched posture in cerebral palsy, J Bone Joint Surg 56A:1598, 1974.
- Eggers GWN: Surgical division of the patellar retinacula to improve extension of the knee joint in cerebral spastic paralysis, J Bone Joint Surg 32A:80, 1950.
- Eggers GWN: Transplantation of hamstring tendons to femoral condyles in order to improve hip extension and to decrease knee fl exion in cerebral spastic paralysis, J Bone Joint Surg 34A:827, 1952.
- Evans EB: The status of surgery of the lower extremities in cerebral palsy, Clin Orthop Relat Res 47:127, 1966.
- Evans EB: Cerebral palsy, III: knee fl exion deformity in cerebral palsy, Instr Course Lect 20:42, 1971.
- Evans EB, Julian JD: Modifi cations of the hamstring transfer, Dev Med Child Neurol 8:539, 1966.
- Gage JR: Surgical treatment of knee dysfunction in cerebral palsy, Clin Orthop Relat Res 253:45, 1990.
- Gage JR, Perry J, Hicks R, et al: Rectus femoris transfer as a means of improving knee fl exion in cerebral palsy, Dev Med Child Neurol 28(suppl 53):5, 1986 (abstract). Grant AD, Small RD, Lehman WB: Correction of fl exion deformity of the knee by supracondylar osteotomy, Bull Hosp Jt Dis 42:28, 1982.
- Grogan DP, Lundy MS, Ogden JA: A method for early postoperative mobilization of the cerebral palsy patient using a removable abduction bar, J Pediatr Orthop 7:338, 1987.
- Kay RM, Rethlefsen SA, Hale JM, et al: Comparison of proximal and distal rotational femoral osteotomy in children with cerebral palsy, J Pediatr Orthop 23:150, 2003.
- Kay RM, Rethlefsen SA, Skaggs D, et al: Outcome of medial versus combined medial and lateral hamstring lengthening surgery in cerebral palsy, J Pediatr Orthop 22:169, 2002.
- Keenan MAE, Ure K, Smith CW, et al: Hamstring release for knee fl exion contracture in spastic adults, Clin Orthop Relat Res 236:221, 1988.
- Lloyd-Roberts GC, Jackson AM, Albert JS: Avulsion of the distal pole of the patella in cerebral palsy: a cause of deteriorating gait, J Bone Joint Surg 67B:252, 1985.
- Mann RL, Root L: Long-term follow-up of distal hamstring releases in cerebral palsy, Dev Med Child Neurol 28(suppl 53):6, 1986 (abstract). McCarroll HR: Surgical treatment of spastic paralysis, Instr Course Lect 6:134, 1949.
- Moreau N, Tinsley S, Li L: Progression of knee joint kinematics in children with cerebral palsy with and without rectus femoris transfers: a long-term follow up, Gait Posture 22:132, 2005.
- Olney BW, Williams PF, Menelaus MB: Treatment of spastic equinus by aponeurosis lengthening, J Pediatr Orthop 8:422, 1988.
- Ounpuu S, Muik E, Davis RB III, et al: Rectus femoris surgery in children with cerebral palsy, I: the effect of rectus femoris transfer location on knee motion, J Pediatr Orthop 13:325, 1993.
- Ounpuu S, Muik E, Davis RB III, et al: Rectus femoris surgery in children with cerebral palsy, II: a comparison between the effect of transfer and release of the distal rectus femoris on knee motion, J Pediatr Orthop 13:331, 1993.
- Patrick JH: Techniques of psoas tenotomy and rectus femoris transfer: “new” operations for cerebral palsy diplegia—a description, J Pediatr Orthop 5B:242, 1996.
- Perry J: Distal rectus femoris transfer, Dev Med Child Neurol 29:153, 1987.
- Perry J, Hoffer MM, Antonelli D, et al: Electromyography before and after surgery for hip deformity in children with cerebral palsy, J Bone Joint Surg 58A:201, 1976.
- Reimers J: Contracture of the hamstrings in spastic cerebral palsy: a study of three methods of operative correction, J Bone Joint Surg 56B:102, 1974.
- Rethlefsen S, Tolo VT, Reynolds RA, et al: Outcome of hamstring lengthening and distal rectus femoris transfer surgery, J Pediatr Orthop 8B:75, 1999.
- Root L, Angel D, Weiner L: Distal release or transfer of the rectus femoris muscle in cerebral palsy patients, Orthop Trans 12:561, 1988 (abstract). Senaran H, Holden C, Dabney KW, et al: Anterior knee pain in children with cerebral palsy, J Pediatr Orthop 27:12, 2007.
- Simon SR, Deutsch SD, Nuzzo RM, et al: Genu recurvatum in spastic cerebral palsy: report on fi ndings by gait analysis, J Bone Joint Surg 60:882, 1978.
- Sutherland DH, Larsen LJ, Mann R: Rectus femoris release in selected patients with cerebral palsy: a preliminary report, Dev Med Child Neurol 17:26, 1975.
- Sutherland DH, Santi M, Abel MF: Treatment of stiff-knee gait in cerebral palsy: a comparison by gait analysis of distal rectus femoris transfer versus proximal rectus release, J Pediatr Orthop 104:433, 1990.
- Sutherland DH, Schottstaedt ER, Larsen LJ, et al: Clinical and electromyographic study of seven spastic children with internal rotation gait, J Bone Joint Surg 51A:1070, 1969.
- Terjesen T, Lie GD, Hyldmo AA, et al: Adductor tenotomy in spastic cerebral palsy: a long-term follow-up study of 78 patients, Acta Orthop 76:128, 2005.
- Thometz J, Simon S, Rosenthal R: The effect on gait of lengthening of the medial hamstring in cerebral palsy, J Bone Joint Surg 71A:345, 1989.
- Topoleski TA, Kurtz CA, Grogan DP: Radiographic abnormalities and clinical symptoms associated with patella alta in ambulatory children with cerebral palsy, J Pediatr Orthop 20:636, 2000.
- van der Linden ML, Aitchison AM, Hazlewood ME, et al: Effects of surgical lengthening of the hamstrings without a concomitant distal rectus femoris transfer in ambulant patients with cerebral palsy, J Pediatr Orthop 23:308, 2003.
- Foot and Ankle Adler N, Bleck EE, Rinsky LA: Gait electromyograms and surgical decisions for paralytic deformities of the foot, Dev Med Child Neurol 31:287, 1989.
- Baker LD: Triceps surae syndrome in cerebral palsy, Arch Surg 68:216, 1954.
- Baker LD: A rational approach to the surgical needs of the cerebral palsy patient, J Bone Joint Surg 38A:313, 1956.
- Baker LD, Hill LM: Foot alignment in the cerebral palsy patient, J Bone Joint Surg 46A:1, 1964.
- Banks HH: Equinus and cerebral palsy: its management, Foot Ankle 4:149, 1983.
- Banks HH, Green WT: The correction of equinus deformity in cerebral palsy, J Bone Joint Surg 40A:1359, 1958.
- Barnes MJ, Herring JA: Combined split anterior tibial-tendon transfer and intramuscular lengthening of the
You Might Also Like