Internal Derangement of the Knee: Biomechanics, Pathoanatomy, and Surgical Management
Key Takeaway
Internal derangement of the knee encompasses a spectrum of intra-articular and extra-articular disturbances that disrupt normal joint mechanics. Originating from William Hey in 1784, the term now demands precise identification of the deranged structure via advanced imaging and arthroscopy. Understanding the complex interplay of tibiofemoral rolling, gliding, and meniscal kinematics is paramount for accurate diagnosis, surgical intervention, and preventing long-term degenerative joint disease following traumatic injury.
Introduction to Internal Derangement
The term "internal derangement" was first introduced into the orthopedic lexicon in 1784 by the English surgeon William Hey. Historically utilized as a catch-all diagnosis for mechanical knee pain, the term is now loosely applied to a variety of intra-articular and extra-articular disturbances—usually of traumatic origin—that interfere with the physiological function of the joint.
In contemporary orthopedic practice, relying solely on "internal derangement" as a definitive diagnosis is insufficient. The specific anatomical structure that is "deranged" must be precisely identified. This requires a keen sense of clinical judgment, comprehensive physical examination, advanced imaging (radiographs, MRI), and, frequently, diagnostic and therapeutic arthroscopy. For accurate diagnosis and rational surgical treatment, a detailed, postgraduate-level understanding of the anatomy, mechanics, and function of the knee joint is absolutely essential.
Functional Anatomy and Tibiofemoral Kinematics
The knee is not a simple hinge joint; it is a complex, polycentric articulation that relies on a sophisticated interplay of osseous geometry, ligamentous restraints, and meniscal interposition to achieve stability through a wide range of motion.
The Rolling and Gliding Mechanism
An accurate plot of the contact points between the femur and tibia reveals that the movement of the femur relative to the tibia during flexion is a complex combination of rolling and gliding. Crucially, the rate of rolling to gliding does not remain constant through all degrees of flexion.
- Early Flexion (0° to 20°): The ratio of rolling to gliding is approximately 1:2.
- Deep Flexion (Towards 120°+): The ratio shifts dramatically to about 1:4 by the end of flexion.
This shifting instant center of rotation represents the true physiological action of the tibiofemoral joint. If the femur only rolled, it would roll off the posterior edge of the tibial plateau. If it only glided, it would impinge against the posterior margin of the tibia. The cruciate ligaments act as the primary mechanical linkages dictating this roll-glide ratio.
Rotary Movements and the Screw-Home Mechanism
The configuration of the osseous structures, combined with the tension of the supporting collateral ligaments, cruciate ligaments, and the menisci, allows virtually no rotary motion in the fully extended position. This obligatory external rotation of the tibia during the terminal degrees of extension is known as the "screw-home mechanism," locking the knee into a stable, energy-efficient position for weight-bearing.
As flexion is initiated, the joint capsule, collateral ligaments, and cruciate ligaments become less tense. This relaxation permits rotary movements that progress increasingly as flexion increases from 0 to 90 degrees.
* Range of Rotation: Rotation ranges from 5 to 25 degrees, subject to individual anatomical variation.
* Directional Dominance: Internal rotation of the tibia on the femur is always quantitatively greater than external rotation.
Femoral Condyle Morphology
The medial and lateral femoral condyles possess distinctly different configurations, which directly influence joint kinematics:
1. Lateral Condyle: Broader in both the anteroposterior and transverse planes compared to the medial condyle.
2. Medial Condyle: Projects distally to a level slightly lower than the lateral condyle. This distal projection is a critical evolutionary adaptation; it helps compensate for the inclination of the mechanical axis and the inherent incongruity between the femoral and tibial articulating surfaces. During rotary movements, the medial condyle describes a smaller arc than the lateral condyle.
Meniscal Anatomy and Kinematics
The menisci are semilunar, fibrocartilaginous structures that serve as critical biomechanical mediators within the knee joint. Located peripherally, they prevent capsular and synovial impingement during flexion-extension movements while deepening the articular surfaces of the tibial plateau.
Dynamic Meniscal Excursion
The menisci are highly dynamic structures. They are described as moving with the femoral condyles during flexion and extension, but moving with the tibia during rotary movements.
* Extension: Both menisci are displaced slightly forward (anteriorly) in full extension.
* Flexion: Both menisci move backward (posteriorly) as flexion proceeds.
Differential Mobility: Medial vs. Lateral
The anchorage of the medial meniscus permits significantly less mobility than that of the lateral meniscus. The medial meniscus is firmly attached to the deep medial collateral ligament (MCL) and the joint capsule. This relative immobility is the primary biomechanical reason why injuries are vastly more common to the medial meniscus than to the lateral meniscus; it cannot easily evade the shearing forces generated by the femoral condyles during sudden, loaded rotation.
Muscular Control of the Menisci
Active muscular retraction plays a vital role in protecting the menisci from entrapment between the advancing articular surfaces during deep knee flexion:
* Lateral Meniscus: The popliteus muscle sends aponeurotic expansions to the posterior horn of the lateral meniscus, actively retracting it posteriorly during flexion and internal rotation.
* Medial Meniscus: The semimembranosus muscle provides a similar dynamic function medially, retracting the posterior horn of the medial meniscus posteriorly.
Clinical Pearl: Failure of the semimembranosus or popliteus to adequately retract the menisci during sudden, explosive flexion (such as deep squatting under load) is a common mechanism for posterior horn longitudinal tears.
Physiological Functions of the Menisci
The menisci are not vestigial remnants; they are indispensable for joint longevity. Their functions include:
1. Load Transmission: They increase the contact area between the femur and tibia, thereby decreasing peak contact stress on the articular cartilage.
2. Joint Lubrication and Nutrition: They help distribute synovial fluid throughout the joint, aiding in the nutrition of the avascular articular cartilage.
3. Stability: They contribute to stability in all planes but are especially important as rotary stabilizers. They are essential for the smooth transition from a pure hinge motion to a gliding or rotary motion as the knee moves from flexion to extension.
Pathomechanics of Internal Derangement
When the structural integrity of the knee is compromised by trauma, a predictable cascade of biomechanical failure ensues. The relationship between mechanical alterations and the biological response is a fundamental concept in orthopedic pathology.
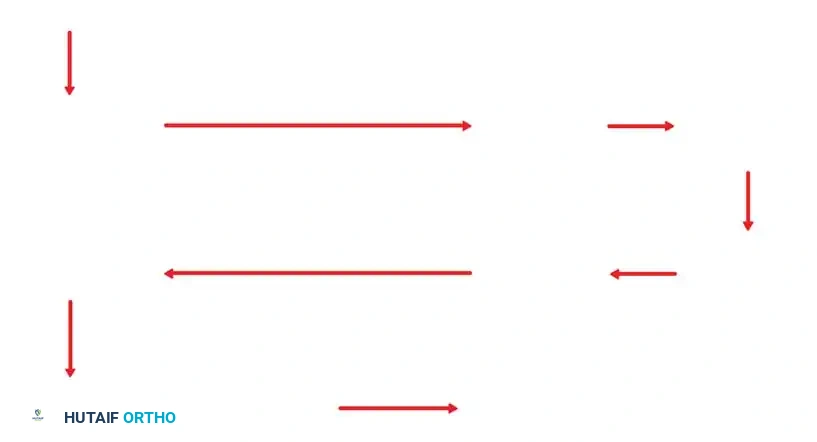
As illustrated in the proposed scheme by Frankel, Burstein, and Brooks, the cascade begins with Trauma, which leads directly to Internal Derangement. This derangement causes a displacement of the centrode (the path of the instant center of rotation), resulting in Abnormal Surface Motion.
This abnormal motion manifests as a conversion from a complex rolling/gliding articulation to a planar joint, drastically increasing shear forces. This leads to Mechanical Articular Surface Wear. Simultaneously, the joint mounts a Biological Response, characterized by localized synovial hypertrophy and osteophyte formation. Ultimately, both the mechanical wear and the biological response culminate in irreversible Degenerative Joint Disease (DJD).
The Biomechanical Catastrophe of Meniscectomy
Historically, total meniscectomy was a common treatment for meniscal tears. Modern biomechanical understanding has proven this to be highly detrimental. Radiographic changes apparent after meniscectomy include:
* Narrowing of the joint space.
* Flattening of the femoral condyle (due to remodeling from increased focal stress).
* Formation of marginal osteophytes.
Narrowing of the joint space initially is caused by the direct removal of the spacer effect of the meniscus (which accounts for approximately 1 mm of joint space). However, it is further narrowed by a severe reduction in the contact area. When the medial meniscus is removed, the contact area is reduced by approximately 40%. According to Hooke's Law, a 40% reduction in contact area results in a massive, exponential increase in peak contact stresses on the underlying articular cartilage, rapidly accelerating the onset of osteoarthritis.
Surgical Warning: The modern mandate in knee surgery is "Save the Meniscus." Partial meniscectomy should be strictly limited to avascular, unrepairable tissue. Every millimeter of resected meniscus exponentially increases the risk of future degenerative joint disease.
Clinical Evaluation and Diagnostic Protocol
Accurate diagnosis of internal derangement requires a systematic approach.
Clinical Examination
- History: Mechanism of injury (e.g., twisting under axial load), presence of a "pop," delayed vs. immediate effusion, mechanical symptoms (catching, locking, giving way).
- Palpation: Joint line tenderness is highly sensitive for meniscal pathology.
- Provocative Testing:
- McMurray Test: Evaluates for meniscal tears via forced flexion, rotation, and varus/valgus stress.
- Apley Grind Test: Differentiates between ligamentous and meniscal pathology.
- Thessaly Test: Dynamic weight-bearing test at 20° of flexion, highly specific for meniscal tears.
Imaging Modalities
- Radiographs: Standard series must include weight-bearing AP, lateral, Rosenberg (45° flexion PA weight-bearing to assess early joint space narrowing), and Merchant views.
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating internal derangement. It provides high-resolution visualization of the menisci, cruciate ligaments, collateral ligaments, and articular cartilage.
Surgical Management: Arthroscopic Intervention
When conservative management fails, or in the presence of acute, repairable pathology (e.g., bucket-handle meniscal tears causing a locked knee), surgical intervention is indicated. Arthroscopy is the standard of care for addressing internal derangement.
Patient Positioning and Setup
- Anesthesia: General or regional anesthesia.
- Positioning: The patient is placed supine on the operating table. A tourniquet is applied to the proximal thigh.
- Leg Holder vs. Lateral Post: The operative leg is either placed in a circumferential leg holder (allowing for valgus/varus stress to open the joint compartments) or positioned against a lateral post. The contralateral leg is placed in a well-padded lithotomy position or kept flat.
- Preparation: Standard sterile prep and drape. The tourniquet is inflated only if visualization is compromised by bleeding.
Portal Placement
Precise portal placement is critical for accessing the deranged structures without causing iatrogenic damage to the articular cartilage.
* Anterolateral Portal (Viewing): Created first, approximately 1 cm lateral to the patellar tendon and 1 cm superior to the lateral joint line. A #11 blade is used to incise the skin and capsule, aiming toward the intercondylar notch.
* Anteromedial Portal (Working): Created under direct intra-articular visualization using a spinal needle for localization. It is placed 1 cm medial to the patellar tendon, slightly lower than the anterolateral portal to allow instruments to pass parallel to the medial tibial plateau.
Step-by-Step Diagnostic Arthroscopy
A systematic 10-point diagnostic sweep must be performed to ensure no pathology is missed:
1. Suprapatellar Pouch: Inspect for loose bodies, plicae, and synovitis.
2. Patellofemoral Joint: Assess the articular cartilage of the patella and trochlea. Evaluate patellar tracking dynamically.
3. Medial Gutter: Check for loose bodies.
4. Medial Compartment: Introduce the arthroscope into the medial compartment while applying valgus stress and external rotation. Use a probe to systematically palpate the medial meniscus (anterior horn, body, posterior horn) and the medial femoral and tibial articular surfaces.
5. Intercondylar Notch: Evaluate the Anterior Cruciate Ligament (ACL) and Posterior Cruciate Ligament (PCL). Probe the ACL to assess tension and structural integrity.
6. Lateral Compartment: Apply varus stress and internal rotation (the "figure-of-four" position). Probe the lateral meniscus, noting the popliteal hiatus, and assess the lateral articular surfaces.
7. Lateral Gutter: Inspect for loose bodies and evaluate the popliteus tendon.
Surgical Decision Making: Meniscal Repair vs. Resection
If a meniscal tear is identified as the source of the internal derangement, the surgeon must decide between repair and partial resection.
Indications for Meniscal Repair:
* Tears located in the peripheral, vascularized red-red or red-white zones.
* Longitudinal vertical tears (e.g., bucket-handle tears).
* Acute tears in younger patients.
* Tears > 1 cm in length.
Surgical Technique (Repair): Depending on the location, an all-inside (using specialized suture anchors), inside-out (gold standard for body/posterior horn tears), or outside-in technique is utilized. The edges of the tear are rasped to stimulate bleeding and promote a healing response.
Indications for Partial Meniscectomy:
* Complex, degenerative, or radial tears extending into the avascular white-white zone.
* Flap tears causing mechanical catching.
* Failed previous meniscal repairs.
Surgical Technique (Resection): Using arthroscopic biters and shavers, the torn, unstable fragments are resected. The goal is to create a stable, smoothly contoured meniscal rim while preserving as much healthy meniscal tissue as possible to maintain the critical 40% contact area and prevent the rapid onset of degenerative joint disease.
Postoperative Protocols and Rehabilitation
Rehabilitation following surgery for internal derangement is dictated by the specific procedure performed.
Following Partial Meniscectomy
- Weight-Bearing: Weight-bearing as tolerated (WBAT) immediately postoperatively with crutches for support.
- Range of Motion (ROM): Immediate, unrestricted ROM exercises.
- Strengthening: Focus on quadriceps activation (straight leg raises, isometric sets) and closed-kinetic-chain exercises.
- Return to Sport: Typically 4 to 6 weeks, pending resolution of effusion and restoration of full strength.
Following Meniscal Repair
- Weight-Bearing: Restricted. Typically, toe-touch weight-bearing (TTWB) or partial weight-bearing in a hinged knee brace locked in extension for 4 to 6 weeks to protect the repair from shear forces.
- Range of Motion (ROM): ROM is often limited to 0°–90° for the first 4 weeks to prevent the posterior translation of the menisci (driven by the semimembranosus and popliteus) from pulling the repair apart.
- Strengthening: Delayed initiation of loaded flexion exercises.
- Return to Sport: Requires a prolonged biological healing phase, typically 4 to 6 months.
By understanding the intricate biomechanics of the tibiofemoral joint and the devastating consequences of altering its native anatomy, the orthopedic surgeon can effectively diagnose and manage internal derangement, prioritizing joint preservation and long-term functional outcomes.
📚 Medical References
- internal derangement: Part 1. intraosseous entities, AJR Am J Roentgenol 178:589, 2002.
- Stanton RP, Abdel-Mota’al MM: Growth arrest resulting from unicameral bone cyst, J Pediatr Orthop 18:198, 1998.
- Stephenson RB, London MD, Hankin FM, et al: Fibrous dysplasia: an analysis of options for treatment, J Bone Joint Surg 59A:400, 1987.
- Sugiura I: Tibial periosteal hemangioma, Clin Orthop Relat Res 106:242, 1975.
- Sung MS, Kim YS, Resnick D: Epithelioid hemangioma of bone, Skeletal Radiol 29:530, 2000.
- Suzuki M, Satoh T, Nishida J, et al: Solid variant of aneurysmal bone cyst of the cervical spine, Spine 29:E3776, 2004.
- Szendröi M, Cser I, Konya A, et al: Aneurysmal bone cyst: a review of 52 primary and 16 secondary cases, Arch Orthop Trauma Surg 111:318, 1992.
- Taconis WK, Schütte HE, van der Heul RO: Desmoplastic fi broma of bone: a report of 18 cases, Skeletal Radiol 23:283, 1994.
- Thomas IH, Chow CW, Cole WG: Case report: giant cell reparative granuloma of the humerus, J Pediatr Orthop 8:596, 1988.
- Unni KK, ed: Dahlin’s bone tumors, 5th ed, Philadelphia, 1996, Lippincott-Raven. Vanhoenacker FM, Hauben E, De Beuckeler LH, et al: Desmoplastic fi broma of bone: MRI features, Skeletal Radiol 29:171, 2000.
- Van Royen BJ, Baayen JC, Pijpers R, et al: Osteoid osteoma of the spine: a novel technique using combined computer-assisted and gamma probe-guided high-speed intralesional drill excision, Spine 30:369, 2005.
- [Vigorita VJ, ed: Orthopaedic pathology, Philadelphia, 1999, Lippincott Williams & Wilkins.
Waddell WR, Gerner RE: Indomethacin and ascorbate inhibit desmoid tumors, J Surg Oncol 15:85, 1980.](https://pubmed.ncbi.nlm.nih.gov/?term=Vigorita%20VJ%2C%20ed%3A%20Orthopaedic%20pathology%2C%20Philadelphia%2C%201999%2C%20Lippincott%20Williams%20%26%20Wilkins.%0A%0AWaddell%20WR%2C%20Gerner%20RE%3A%20Indomethacin%20and%20ascorbate%20inhibit%20desmoid%20tumors%2C%20J%20Surg%20Oncol%2015%3A85%2C%201980.)
- Walker LG, Meals RA: Painless osteoid osteoma of the phalanx, Orthopedics 12:776, 1989.
- Ward WG, Eckardt JJ, Shayestehfar S, et al: Osteoid osteoma diagnosis and management with low morbidity, Clin Orthop Relat Res 291:229, 1993.
- Weiner SD: Enchondroma and chondrosarcoma of bone: clinical, radiologic, and histologic differentiation, Instr Course Lect 53:645, 2004.
- Wenger DE, Wold LE: Benign vascular lesions of bone: radiologic and pathologic features, Skeletal Radiol 29:63, 2000.
- Wilkins RM: Unicameral bone cysts, J Am Acad Orthop Surg 8:217, 2000.
- Yabut SM Jr, Kenan S, Sissons HA, et al: Malignant transformation of fi brous dysplasia: a case report and review of the literature, Clin Orthop Relat Res 228:281, 1988.
- Yamamoto T, Kurosaka M, Mizuno K: Juxta-articular hemangioma of long bone, Skeletal Radiol 29:535, 2000.
- Yamamoto T, Mauri T, Akisue T, et al: Solid aneurysmal bone cyst in the humerus, Skeletal Radiol 29:470, 2000.
- Yu J, Chang S-S, Suratwala S, et al: Zoledronate induces apoptiosis in cells from fi bro-cellular membrane of unicameral bone cyst (UBC), J Orthop Res 23:1004, 2005.
- Zmurko MG, Mott MP, Lucas DR, et al: Multicentric osteoid osteoma, Orthopedics 27:1294, 2004.
You Might Also Like