Disorders of the Patella: OCD, Dorsal Defects & Bipartite Patella
Key Takeaway
Disorders of the patella, including osteochondritis dissecans, dorsal defects, and bipartite patella, present unique diagnostic and therapeutic challenges. Management ranges from conservative immobilization to advanced surgical interventions like arthroscopic excision, internal fixation, and the Ogata subperiosteal release technique. This guide provides an evidence-based framework for evaluating patellofemoral pathology, optimizing surgical approaches, and ensuring joint preservation in complex patellar anomalies.
INTRODUCTION TO PATELLAR DISORDERS
The patella, the largest sesamoid bone in the human body, plays a critical biomechanical role in the extensor mechanism of the knee. By increasing the moment arm of the quadriceps tendon, it significantly enhances the mechanical advantage of knee extension. However, its unique anatomical position and the tremendous compressive and shear forces it endures make it susceptible to a distinct spectrum of developmental, osteochondral, and traumatic disorders.
This comprehensive guide explores three primary non-traumatic and developmental disorders of the patella: Osteochondritis Dissecans (OCD), Dorsal Defect of the Patella, and Bipartite Patella. Mastery of these conditions is essential for the orthopedic surgeon to differentiate benign developmental anomalies from pathological lesions requiring surgical intervention.
OSTEOCHONDRITIS DISSECANS OF THE PATELLA
Osteochondritis dissecans (OCD) of the patella is a relatively rare entity, occurring far less frequently than OCD of the femoral condyles. Despite its rarity, it typically carries a worse prognosis due to the extreme shear forces generated across the patellofemoral joint during knee flexion and extension.
Pathophysiology and Demographics
Patellar OCD usually manifests in the second and third decades of life. The exact etiology remains multifactorial, involving repetitive microtrauma, localized ischemia, and potential genetic predispositions. The lesion is most frequently located in the lower half of the patella. Notably, involvement is bilateral in up to one-third of patients, necessitating a thorough evaluation of the contralateral knee even in unilateral presentations.
Clinical Pearl: Always distinguish true patellar OCD from a dorsal defect of the patella. OCD typically involves the articular surface and subchondral bone, often leading to fragment instability, whereas a dorsal defect is a benign, usually asymptomatic, subchondral radiolucency.
Clinical Evaluation and Imaging
Patients typically present with anterior knee pain, crepitus, swelling, and mechanical symptoms such as catching or locking if a loose body is present.
Radiographic evaluation is paramount:
* Lateral Radiograph: The lesion is best visualized on a slightly overexposed lateral radiograph, which allows for better penetration of the dense patellar bone.
* Axial ("Skyline" or Merchant) View: This view is critical for determining whether the lesion is located on the medial or lateral facet and for assessing the overall patellofemoral tracking and architecture.
* Magnetic Resonance Imaging (MRI): MRI is the gold standard for assessing the stability of the osteochondral fragment, the viability of the subchondral bone, and the integrity of the overlying articular cartilage.
Surgical Management
Treatment principles for patellar OCD mirror those for the distal femur; however, patellar lesions are frequently associated with extensive chondromalacia that extends considerably beyond the peripheral margins of the avascular bone. Residual disability post-treatment is directly proportional to the size of this chondromalacic area.
Indications for Surgery:
* Failure of conservative management (prolonged immobilization and activity modification).
* Unstable lesions (fluid behind the fragment on MRI).
* Detached loose bodies.
Surgical Options:
1. Fragment Excision and Marrow Stimulation: For small, unsalvageable fragments, excision followed by curettage and drilling (or microfracture) of the base stimulates fibrocartilage formation.
2. Internal Fixation: If the fragment is large and possesses viable articular cartilage, in situ fixation is preferred. This can be achieved using arthroscopic metallic or bioabsorbable screws, or variable-pitch headless compression screws.
3. Cartilage Restoration Techniques: For large, full-thickness defects where the fragment cannot be salvaged, advanced techniques such as Autologous Chondrocyte Implantation (ACI) or Osteochondral Autograft Transfer System (OATS) are indicated.
Surgical Warning: Rarely is chondromalacia so extensive as to require a primary patellectomy. The patella should almost always be preserved during the index procedure to maintain extensor mechanism biomechanics. It can later be excised if severe, intractable disability persists.
DORSAL DEFECT OF THE PATELLA
A dorsal defect of the patella is a benign, circular, well-circumscribed radiolucent lesion, typically measuring approximately 1 cm in diameter. It invariably abuts the articular cartilage and is characteristically located in the superolateral aspect of the patella.
Etiology and Differential Diagnosis
Although the exact cause remains debated, the prevailing consensus among orthopedic authors is that a dorsal defect represents a variant of normal ossification. It is frequently attributed to a traction injury at the insertion site of the vastus lateralis muscle during the active ossification phase of the patella.
In approximately 50% of patients, the lesion is entirely asymptomatic and discovered incidentally. However, when evaluating a lytic lesion in the patella, the differential diagnosis must be exhaustive:
* Osteochondritis dissecans
* Brodie abscess (subacute osteomyelitis)
* Eosinophilic granuloma
* Enchondroma
* Osteoid osteoma
* Metastatic disease (particularly in older individuals)
Management
Given its benign nature, asymptomatic dorsal defects require no intervention. If the patient is symptomatic, conservative management with NSAIDs, activity modification, and physical therapy focusing on vastus medialis obliquus (VMO) strengthening is usually sufficient. Surgical curettage and bone grafting are reserved strictly for refractory cases where all other causes of anterior knee pain have been definitively ruled out.
BIPARTITE PATELLA
A bipartite patella occurs when a secondary ossification center fails to fuse with the primary body of the patella. While often an incidental finding, the synchondrosis between the fragments can become symptomatic due to repetitive microtrauma or acute injury.
Classification and Pathoanatomy
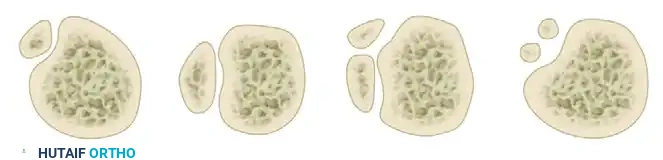
The classification of bipartite patella is based on the anatomical location and the number of fragments. The Oohashi classification provides a comprehensive framework:
Figure: Classification of bipartite patella according to location (superolateral or lateral) and number of fragments (bipartite, tripartite, multipartite).
The superolateral quadrant is by far the most common location. The fragment is connected to the main body of the patella by a fibrocartilaginous synchondrosis. The vastus lateralis inserts directly into this superolateral fragment, creating constant tensile forces that can lead to symptomatic distraction and inflammation.
Diagnostic Evaluation
Diagnosis is primarily radiographic. A skyline view and an AP view will typically reveal a radiolucent line with smooth, sclerotic borders separating the fragment.
Pitfall: Do not rely on bone scintigraphy (bone scans) to dictate treatment. Increased scintigraphic uptake is frequently found in both symptomatic and asymptomatic bipartite patellae, making it an unreliable indicator for surgical intervention.
Conservative Management
The vast majority of symptomatic bipartite patellae respond excellently to non-operative measures.
* Activity Modification: Restricting the specific activities causing the overuse syndrome.
* Pharmacotherapy: Nonsteroidal anti-inflammatory drugs (NSAIDs).
* Physical Therapy: A short-arc exercise program to strengthen the quadriceps without overloading the patellofemoral joint.
* Immobilization: In refractory acute flares, immobilization in a cylinder cast or rigid brace for 3 weeks or more effectively relieves the symptoms of repetitive microtrauma at the synchondrosis.
Surgical Management
Operative treatment is rarely necessary. Fracture and traumatic separation of bipartite patellae have been described in the literature, but these are rare occurrences. When surgery is indicated for chronic, debilitating pain that fails conservative management, several options exist:
- Fragment Excision: Excision of the bipartite fragment, especially in the superolateral quadrant, yields high success rates. Arthroscopic excision is preferred over open excision as it results in significantly less morbidity, faster rehabilitation, and minimal disruption of the extensor retinaculum.
- Caution: Excision of excessively large fragments that bear a significant portion of the articular surface may produce patellofemoral incongruity and subsequent early-onset osteoarthritis.
- Internal Fixation: Open reduction and internal fixation (ORIF) of separated fragments using compression screws has been reported, particularly for large articular fragments, but it currently has limited robust support in the literature.
- Lateral Retinacular Release and Muscle Detachment: Detaching the vastus lateralis muscle insertion reduces the traction force on the loose fragment, producing good pain relief and often leading to spontaneous union of the synchondrosis.
The Ogata Technique: Subperiosteal Release
Ogata described a highly effective, joint-preserving subperiosteal release of the lateral quadriceps mechanism that inserts into the bipartite portion of the patella. This technique relieves the fragment from muscle traction without causing a mediolateral imbalance that would negatively affect patellofemoral tracking.
Surgical Positioning and Preparation:
* The patient is placed supine on the operating table.
* A well-padded high thigh tourniquet is applied.
* The operative leg is prepped and draped in a standard sterile fashion. The knee is flexed to 30 degrees to place mild tension on the extensor mechanism.
Step 1: Surgical Approach
An oblique skin incision is made over the distal portion of the vastus lateralis tendon. The incision extends just distal to the midportion of the separated area of the patella, allowing adequate exposure of the superolateral pole.
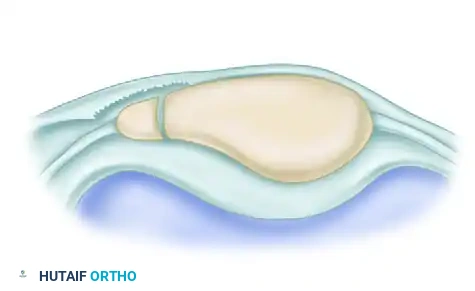
Figure: Ogata technique for bipartite patella. Oblique skin incision is made over the distal portion of the vastus lateralis tendon.
Step 2: Tendon Splitting and Subperiosteal Detachment
The vastus lateralis tendon is identified and split longitudinally along the direction of its middle fibers. Using a scalpel and a periosteal elevator, the insertion of the vastus lateralis onto the painful bipartite patellar fragment is carefully detached subperiosteally.
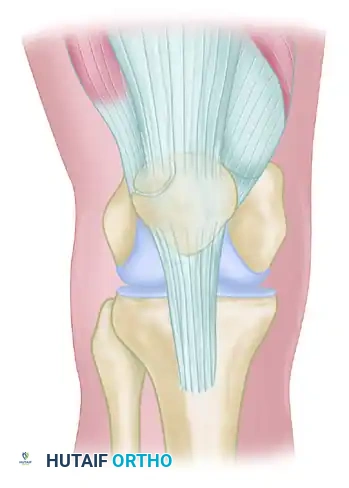
Figure: The vastus lateralis tendon is split along its middle fibers, and the insertion to the painful patellar fragment is detached subperiosteally.
Step 3: Preservation of Tracking and Closure
It is critical that the continuity of the tendon-periosteum complex to the main portion of the patella is meticulously preserved. By doing so, the bipartite fragment is relieved from the constant, painful muscle traction, yet the overall mediolateral balance of the extensor mechanism remains intact, preventing iatrogenic patellar maltracking.
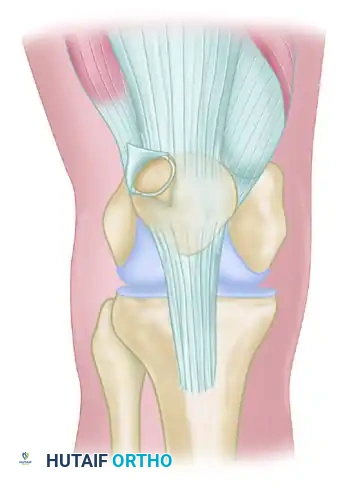
Figure: The fragment is relieved from muscle traction without causing mediolateral imbalance. Care must be taken not to injure the synovial capsule to preserve the blood supply to the fragment.
Surgical Pearl: During the subperiosteal elevation, extreme care should be taken not to violate or injure the underlying synovial capsule. Preserving the capsule ensures that some residual blood supply to the bipartite fragment is maintained, which aids in potential spontaneous fusion and prevents avascular necrosis of the fragment.
Postoperative Protocol for the Ogata Technique:
* Phase 1 (Weeks 0-2): The knee is placed in a hinged knee brace locked in extension for ambulation. Weight-bearing as tolerated is permitted. Isometric quadriceps exercises (quad sets) and straight leg raises are initiated immediately.
* Phase 2 (Weeks 2-6): The brace is unlocked to allow progressive range of motion (ROM). Active-assisted and passive ROM exercises are advanced. Short-arc quadriceps exercises are introduced.
* Phase 3 (Weeks 6-12): Progression to full, unrestricted ROM. Strengthening focuses on closed kinetic chain exercises (e.g., leg presses, wall slides) to minimize patellofemoral shear forces. Return to sports is typically permitted between 3 to 4 months postoperatively, contingent upon the restoration of full quadriceps strength and absence of pain.
You Might Also Like


