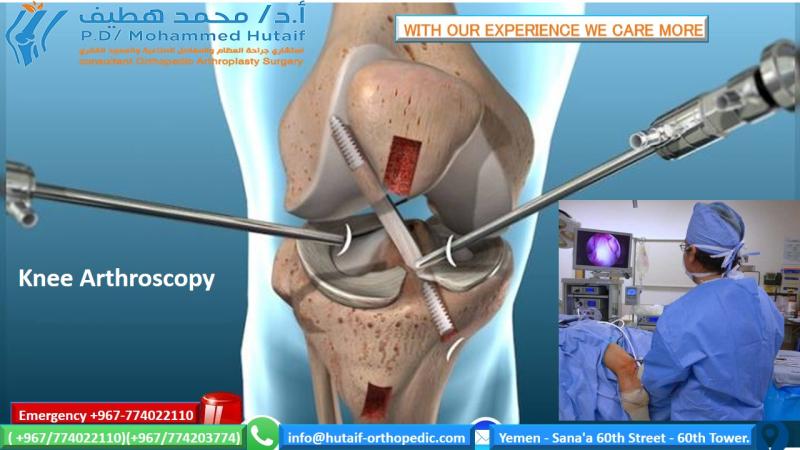
Mastering Arthroscopic Knee Examination and Meniscal Surgery
Key Takeaway
A systematic approach to arthroscopic knee examination is paramount for diagnostic accuracy. This comprehensive guide details the seven-compartment evaluation sequence, optimal portal placement, and the O'Connor classification of meniscal tears. Emphasizing joint preservation, it outlines the biomechanical principles and surgical techniques for partial, subtotal, and total meniscectomies, ensuring orthopedic surgeons achieve optimal functional outcomes and joint stability.
INTRODUCTION TO ARTHROSCOPIC KNEE EXAMINATION
The cornerstone of a successful, accurate, and comprehensive diagnosis of intra-articular knee pathology is the execution of a strictly systematic arthroscopic examination. For the orthopedic surgeon, developing a methodical sequence of visualization is not merely a recommendation; it is an absolute necessity. This sequence must progress logically from one compartment to another, ensuring that no anatomical recess or subtle lesion is overlooked. While the specific order of the sequence may vary based on surgeon preference or institutional protocols, the habit of adhering to a standardized, reproducible routine in every single case is critical. Failure to maintain this discipline significantly compromises diagnostic accuracy, potentially leading to missed pathology, incomplete treatment, and suboptimal patient outcomes.
PREOPERATIVE SETUP AND PATIENT POSITIONING
Optimal patient positioning and meticulous preoperative setup are fundamental to facilitating a seamless arthroscopic procedure. The patient is typically positioned supine on the operating table. A lateral post or a dedicated leg holder is utilized to secure the operative thigh, allowing for the application of valgus and varus stress to open the respective compartments.
The Figure-Four Position
To adequately visualize and instrument the lateral compartment and the posterolateral structures, the "figure-four" position is universally employed.
* Positioning Mechanics: The operative hip is slightly flexed, abducted, and externally rotated. The knee is flexed between 30 and 90 degrees, and the tibia is internally rotated.
* Execution: This position can be achieved by dropping the foot of the table or keeping it extended. If extended, the operative ankle is rested on the contralateral lower leg. In this configuration, the hip naturally falls into external rotation.
* Dynamic Stress: A varus stress can be dynamically applied by the surgeon pushing downward on the flexed knee, effectively opening the lateral joint space and allowing for comprehensive evaluation of the lateral meniscus and popliteal hiatus.
Surgical Warning: Prolonged or excessive force while the knee is in the figure-four position, particularly in older patients or those with pre-existing hip pathology, can lead to iatrogenic hip injury or exacerbation of osteoarthritis. Always apply stress judiciously.
Tourniquet and Local Infiltration
While a proximal thigh tourniquet is routinely applied, it does not necessarily need to be inflated unless troublesome bleeding obscures the visual field. To minimize the need for tourniquet inflation and to enhance postoperative pain control, the planned portal sites should be infiltrated with 4 to 5 mL of a local anesthetic agent mixed with epinephrine (e.g., 1% lidocaine or 0.25% bupivacaine with 1:100,000 epinephrine).
Clinical Pearl: Do not exceed 4 to 5 mL of local infiltration per portal site. A larger bolus, particularly in the anterolateral and anteromedial portals, can inadvertently distend the infrapatellar fat pad, pushing it into the joint space and severely obscuring the initial arthroscopic view.
PORTAL PLACEMENT AND SCOPE INSERTION
The precise establishment of arthroscopic portals is the most critical technical step in knee arthroscopy. Improper portal placement restricts instrument maneuverability, damages articular cartilage, and limits the visual field.
Standard Anterior Portals
The standard anterolateral (viewing) and anteromedial (working) portals are located just off the medial and lateral edges of the patellar tendon, adjacent to the broadest portion of the patella. The selection of these sites is crucial; a portal placed too far superiorly will plunge into the fat pad, while one placed too far inferiorly will damage the anterior horn of the meniscus. A 30-degree oblique arthroscope is considered the gold standard for these portals, providing an optimal field of view.
Accessory Far Medial and Lateral Portals
These inferior optional portals are frequently utilized for the triangulation of accessory instruments during complex operative procedures, such as meniscal repairs or osteochondral grafting.
* Location: Approximately 2.5 cm medial or lateral to the standard anteromedial and anterolateral portals. Medially, this portal sits near the anterior edge of the superficial medial collateral ligament (MCL). Laterally, it must be positioned well anterior to the fibular collateral ligament (FCL) and the popliteus tendon.
* Spinal Needle Localization: An excellent, evidence-based technique is to insert an 18-gauge spinal needle through the skin and capsule under direct intra-articular arthroscopic visualization. The needle must enter the joint just above the superior surface of the meniscus.
* Execution: Once the needle trajectory is confirmed to reach the target pathology without obstruction, the portal incision is made. If the needle cannot reach the desired location, the entry point is adjusted before any incision is made. The margin for error here is minimal; improper placement can lacerate the meniscus, damage the collateral ligaments, or scuff the femoral condyle.
Central Transpatellar Tendon (Gillquist) Portal
The central transpatellar tendon portal is located approximately 1 cm inferior to the lower pole of the patella, directly in the midline of the joint, passing through the substance of the patellar tendon.
* Adjustments: If the patient has patella alta or baja, or if the tendon is laterally subluxated, the portal location must be adjusted accordingly.
* Indications: This portal is highly advantageous in anterior cruciate ligament (ACL) reconstruction procedures, particularly after a bone-patellar tendon-bone (BTB) graft has been harvested, as it utilizes the existing defect. It also provides unparalleled visualization of the posterior compartments when a 70-degree scope is passed through the intercondylar notch.
* Technique: The portal is created with the knee flexed to 90 degrees to maintain tension on the patellar tendon. A 6- to 7-mm vertical incision is made sharply with a No. 11 blade through the skin, subcutaneous tissue, and tendon.
* Limitations: Routine use of the Gillquist portal is not advocated due to the potential for iatrogenic patellar tendon morbidity and postoperative anterior knee pain.
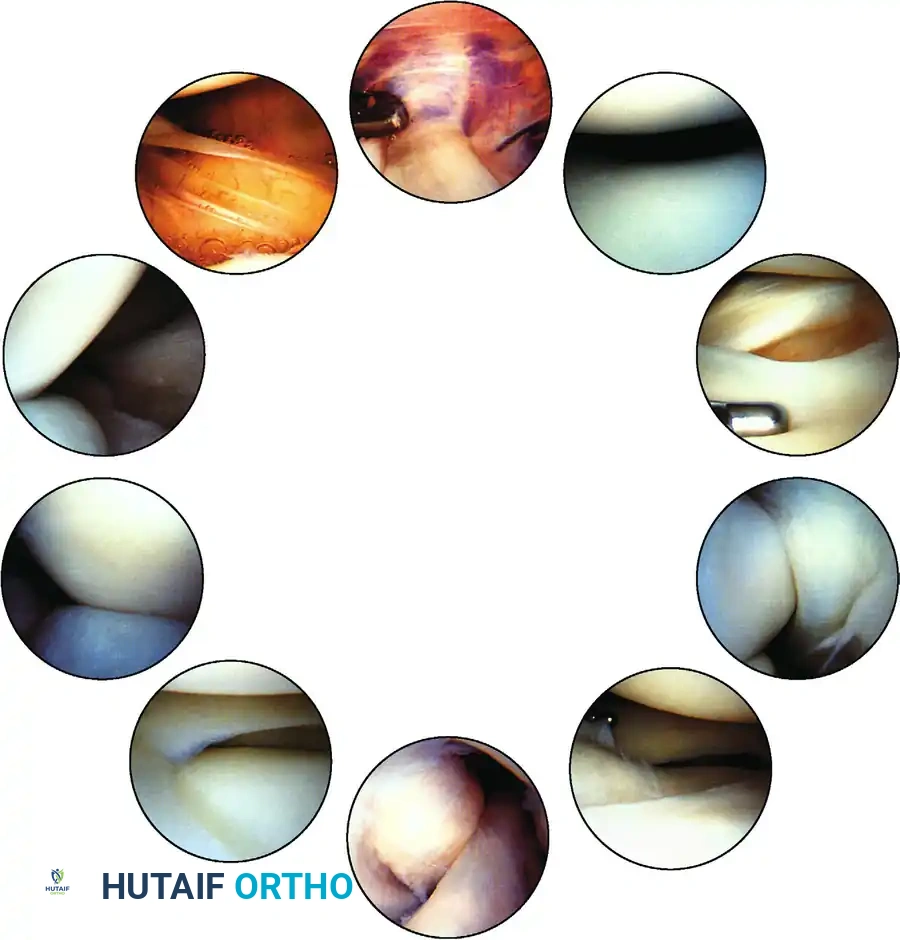
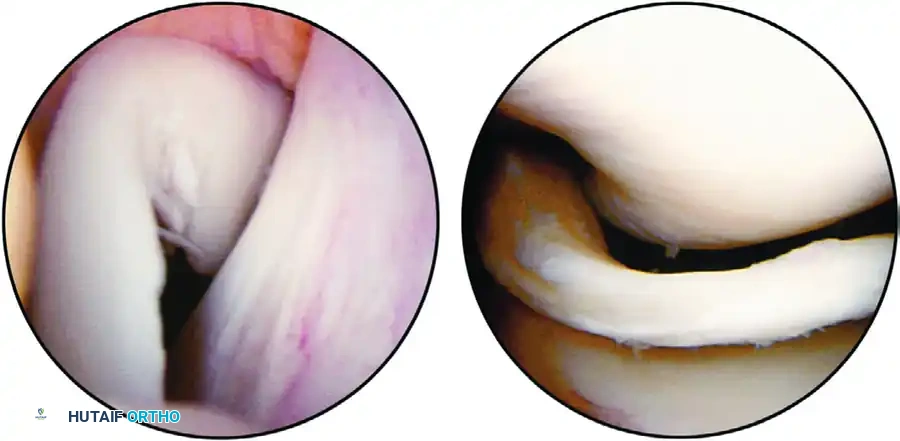
THE SYSTEMATIC SEVEN-COMPARTMENT EXAMINATION
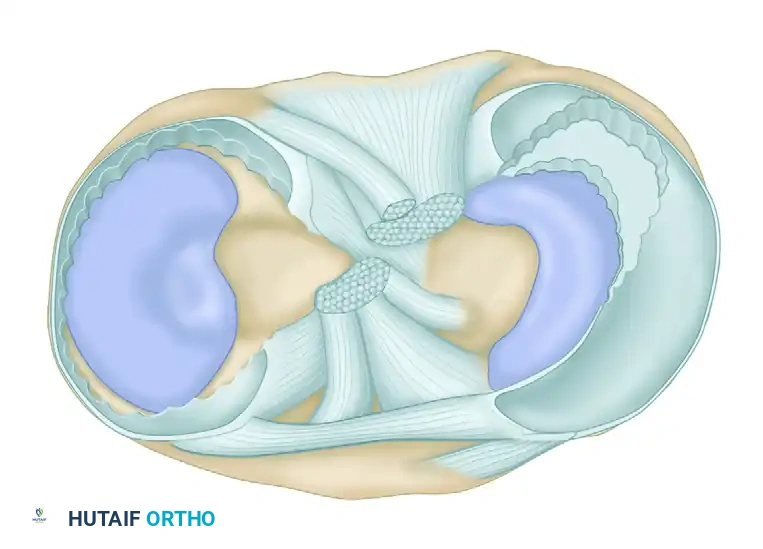
To ensure no pathology is missed, the knee must be routinely divided into seven distinct compartments. The arthroscope should be swept through these regions systematically.
- Suprapatellar Pouch and Patellofemoral Joint: The examination begins superiorly. The undersurface of the articularis genu, the synovial lining, and the patellofemoral tracking are evaluated. The scope is swept medially and laterally to assess the patellar facets and the trochlear groove.
- Medial Gutter: The scope is directed down the medial side of the joint to inspect for loose bodies and assess the medial plica.
- Medial Compartment: A valgus stress is applied. The medial meniscus, medial femoral condyle, and medial tibial plateau are thoroughly inspected. The meniscus must be probed to assess for hidden inferior surface tears.
- Intercondylar Notch: The scope is moved centrally to evaluate the anterior cruciate ligament (ACL), the posterior cruciate ligament (PCL), and the ligament of Humphry or Wrisberg. The synovial covering of the PCL is often noted here.
- Posteromedial Compartment: This can be visualized by passing the arthroscope posteriorly through the intercondylar notch (between the PCL and the medial femoral condyle) or via a separate accessory posteromedial portal if visualization is inadequate.
- Lateral Compartment: The knee is placed in the figure-four position with varus stress. The lateral meniscus, lateral femoral condyle, and lateral tibial plateau are examined.
- Lateral Gutter and Posterolateral Compartment: The scope is swept down the lateral gutter. The popliteal hiatus and the insertion of the popliteus tendon are visualized. If the posterolateral compartment is incompletely viewed from the anterior portal, a direct posterolateral portal must be established.
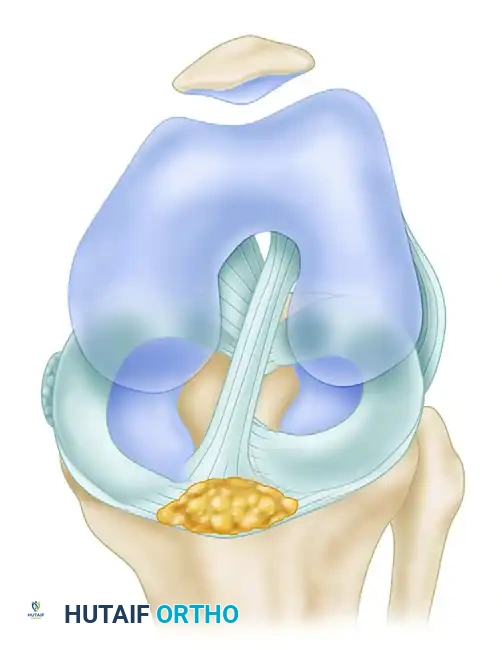
ARTHROSCOPIC SURGERY OF THE MENISCUS: BIOMECHANICS AND CLASSIFICATION
The menisci are vital fibrocartilaginous structures that provide load transmission, shock absorption, joint stability, and proprioception. Recognizing the specific pattern of a meniscal tear during diagnostic arthroscopy is the most critical step in planning subsequent resection or repair.
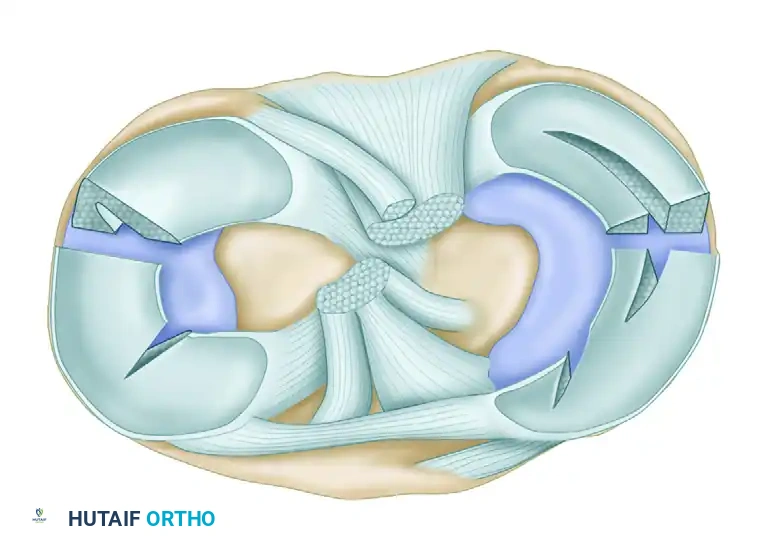
O'Connor's Classification of Meniscal Tears
While numerous classification systems exist, the O'Connor classification remains highly practical and widely utilized in orthopedic surgery. It categorizes tears into five primary patterns: (1) Longitudinal, (2) Horizontal, (3) Oblique, (4) Radial, and (5) Variations (Complex/Degenerative).
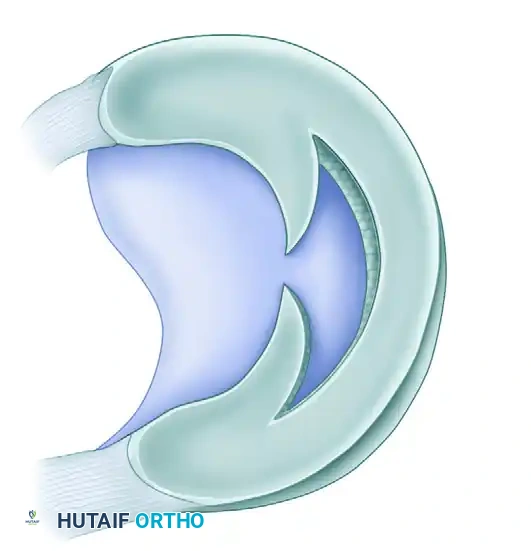
1. Longitudinal Tears and Bucket-Handle Lesions
Longitudinal tears typically result from acute rotational trauma to a previously healthy, biomechanically normal meniscus.
* Morphology: The tear is vertically oriented and runs parallel to the peripheral edge of the meniscus. It may be partial or full-thickness.
* Bucket-Handle Tears: If a complete longitudinal tear propagates extensively, it produces a displaceable inner fragment. When this inner fragment flips and displaces centrally into the intercondylar notch, it is termed a "bucket-handle" tear. This often presents clinically as a locked knee.

Meniscal Vascular Zones
The healing potential of a longitudinal tear is entirely dependent on its proximity to the peripheral blood supply (the perimeniscal capillary plexus).
* Zone I (Red-Red Zone): Tears in the peripheral outer third are highly vascularized and have excellent healing potential. These should almost always be repaired.
* Zone II (Red-White Zone): Tears at the junction of the middle and outer thirds have a variable blood supply. Repair is often indicated, especially in younger patients, sometimes augmented with biological stimulation (e.g., marrow venting).
* Zone III (White-White Zone): Tears in the inner avascular third have virtually no healing potential and are typically treated with partial meniscectomy.



2. Horizontal Tears
Horizontal tears are characterized by a cleavage plane that divides the meniscus into superior and inferior leaves.
* Pathogenesis: These are predominantly degenerative in nature, occurring more frequently in older patients due to chronic shear forces.
* Location: They are most commonly observed in the posterior horn of the medial meniscus or the mid-body of the lateral meniscus. Many complex flap tears originate from an underlying horizontal cleavage component.
3. Oblique Tears
Oblique tears are full-thickness disruptions that run diagonally from the inner free edge of the meniscus outward into the meniscal body.
* Nomenclature: They are classified based on the location of their base. If the base of the tear is posterior, it is a posterior oblique tear; if anterior, it is an anterior oblique tear.
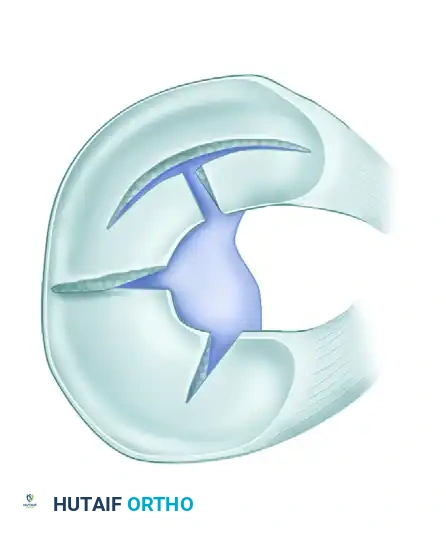
4. Radial Tears
Radial tears are vertically oriented but, unlike longitudinal tears, they extend perpendicularly from the inner free edge toward the periphery.
* Biomechanics: These tears are particularly detrimental because they disrupt the circumferential collagen fibers, severely compromising the meniscus's ability to resist hoop stresses.
* Extent: They can be incomplete or complete. An incomplete radial tear that curves anteriorly or posteriorly is often referred to clinically as a "parrot beak" tear. Tears located posterior to the popliteal tendon may occasionally heal spontaneously or with local abrasion techniques.
5. Complex and Degenerative Variations
- Flap Tears: Similar to oblique tears but usually possess a horizontal cleavage element rather than being purely vertical. They are termed superior or inferior flap tears based on which surface the flap is hinged.
- Complex Tears: These contain elements of multiple tear patterns (e.g., radial, horizontal, and longitudinal). They are typically the end-result of chronic, long-standing altered joint mechanics. The initial tear pattern is often obscured by subsequent planes of tearing.
- Degenerative Tears: A subset of complex tears presenting with marked fraying, irregularity, and multi-planar tearing, predominantly seen in the osteoarthritic knees of older patients.

PRINCIPLES AND TYPES OF MENISCAL EXCISION
The overarching philosophy of modern meniscal surgery is joint preservation. The surgeon must meticulously probe and classify the tear before initiating any resection. Failure to thoroughly explore the extent and hidden planes of a tear often results in the needless sacrifice of healthy, load-bearing meniscal tissue.
Surgical Warning: Never begin a meniscectomy without a complete mental blueprint of the resection. You must visualize the exact tissue to be removed and the final contoured shape of the peripheral rim before making the first cut.
O'Connor categorized meniscal excisions into three distinct types based on the volume of tissue removed.
Partial Meniscectomy
This is the gold standard for non-repairable tears. Only the loose, unstable, and non-functional meniscal fragments are excised.
* Indications: Displaceable inner edges of white-white zone bucket-handle tears, mobile flaps, or the central portion of radial tears.
* Objective: To eliminate the mechanical symptoms (catching/locking) while preserving a stable, balanced, and contoured peripheral rim of healthy meniscal tissue. This maximizes retained load-bearing capacity.
Subtotal Meniscectomy
In a subtotal meniscectomy, the complexity and peripheral extension of the tear necessitate the excision of a portion of the peripheral rim itself.
* Indications: Severe complex or degenerative tears of the posterior horn that extend to the capsule.
* Technique: The resection extends outward to include the peripheral rim in the affected zone. It is termed "subtotal" because the anterior horn and portions of the middle third are preserved. While less desirable than a partial meniscectomy, it is preferable to total removal.
Total Meniscectomy
Total removal of the meniscus is historically associated with rapid progression to unicompartmental osteoarthritis and is now rarely indicated.
* Indications: Reserved strictly for cases where the meniscus is completely detached from its peripheral meniscosynovial junction, and the intrameniscal architecture is so extensively destroyed that it is entirely unsalvageable.
* Alternative: If the body of a peripherally detached meniscus is structurally intact, total meniscectomy is contraindicated, and an aggressive meniscal repair (inside-out or all-inside technique) must be attempted.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative rehabilitation protocol is dictated entirely by the surgical intervention performed.
- Following Partial Meniscectomy: Patients are typically allowed immediate weight-bearing as tolerated. Crutches may be used for 2 to 5 days for comfort. Early range of motion (ROM) exercises, quadriceps activation (straight leg raises), and closed-chain kinetic exercises are initiated immediately to prevent atrophy. Return to sports is generally anticipated between 4 to 6 weeks, provided there is no effusion and full strength is regained.
- Following Meniscal Repair: Rehabilitation is significantly more conservative to protect the healing tissue. Weight-bearing is often restricted or limited to extension for 4 to 6 weeks. Deep flexion (greater than 90 degrees) under weight-bearing loads is strictly prohibited for up to 8 weeks to prevent shear forces from disrupting the sutures. Return to high-impact sports may be delayed for 4 to 6 months.
By adhering to a systematic diagnostic approach, respecting the biomechanical importance of the meniscus, and executing precise, tissue-sparing surgical techniques, orthopedic surgeons can reliably alleviate mechanical symptoms while maximizing the long-term survivorship of the knee joint.
You Might Also Like