Comprehensive Guide to Scaphoid Volar Approach: Anatomy, Indications & Surgical Technique
Key Takeaway
The scaphoid volar approach is a surgical technique for treating scaphoid fractures and nonunions. It provides direct access to the scaphoid, crucially preserving its dorsal blood supply, which is vital for healing and preventing avascular necrosis. It's indicated for various pathologies and offers a more aesthetic scar.
Introduction & Epidemiology
Scaphoid fractures represent the most common carpal bone fracture, accounting for 60-70% of all carpal injuries. Their unique anatomy, precarious blood supply, and complex biomechanical role in wrist kinematics render their management challenging, with a notable propensity for nonunion and avascular necrosis (AVN). The scaphoid acts as an intercalated segment within the carpus, articulating with the radius, lunate, capitate, and trapezium, making it crucial for maintaining carpal stability and motion.
The volar approach to the scaphoid is a well-established surgical technique, offering direct access to the scaphoid tubercle, waist, and distal pole. Its primary advantages include preservation of the critical dorsal blood supply to the proximal pole and a more aesthetically favorable scar. While historically favored for distal pole and waist fractures, its utility has expanded to include challenging nonunions, particularly those involving the volar column, and for placement of long compression screws that traverse the entire scaphoid. Understanding the precise anatomical relationships and meticulous surgical technique is paramount to optimize outcomes and mitigate potential complications.
Surgical Anatomy & Biomechanics
The scaphoid is a boat-shaped carpal bone situated in the distal row of the carpus, acting as a link between the proximal and distal carpal rows. Its unique orientation, lying at approximately a 45-degree angle to the long axis of the forearm, contributes to its vulnerability to injury and the complexity of its surgical exposure.
Vascularity
The scaphoid's blood supply is predominantly retrograde, arising from the radial artery.
*
Dorsal Carpal Branch:
The main blood supply (70-80%) originates from the dorsal carpal branch of the radial artery. This vessel typically enters the scaphoid through multiple foramina along the dorsal ridge, supplying the proximal two-thirds of the bone. Preservation of this dorsal vascularity is a significant advantage of the volar approach.
*
Volar Carpal Branches:
Smaller branches from the volar radial artery supply the scaphoid tubercle and distal pole. While less substantial, these contributions are vital for the viability of the distal scaphoid.
*
Nutrient Foramina:
The density of nutrient foramina is higher distally, diminishing towards the proximal pole, contributing to the higher incidence of AVN in proximal pole fractures.
Neurovascular Structures
The volar wrist anatomy is intricate and requires careful dissection.
*
Radial Artery:
The radial artery runs radially to the flexor carpi radialis (FCR) tendon in the distal forearm and wrist. It lies deep to the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons in the anatomic snuffbox. During the volar approach, it is a primary structure at risk, positioned just radial to the FCR tendon sheath, requiring meticulous retraction.
*
Superficial Radial Nerve (SRN):
While primarily a dorsal risk, branches of the SRN supplying sensation to the radial aspect of the hand and thumb can be inadvertently injured during skin incision or superficial dissection if the incision extends too far radially or proximally.
*
Palmar Cutaneous Branch of the Median Nerve:
This sensory nerve arises from the median nerve approximately 5-7 cm proximal to the wrist crease and traverses superficially, radial to the palmaris longus tendon (if present). It is susceptible to injury during initial skin incision and subcutaneous dissection if an overly radial or oblique incision is utilized.
*
Flexor Carpi Radialis (FCR) Tendon:
This tendon serves as a key landmark. It lies between the radial artery radially and the palmaris longus (if present) ulnarly. The FCR sheath is incised longitudinally to gain access to the underlying structures.
*
Scaphoid Tubercle:
This palpable prominence on the volar aspect of the wrist is a crucial landmark for initiating the incision and for confirming the depth of dissection. It serves as an attachment point for the transverse carpal ligament and part of the thenar musculature.
Biomechanics
The scaphoid plays a critical role in carpal kinematics, functioning as an intercalated segment. It bridges the proximal (scaphoid, lunate, triquetrum) and distal (trapezium, trapezoid, capitate, hamate) carpal rows. Its unique orientation allows for concurrent flexion and extension of both carpal rows, linking radial and ulnar deviation. A disruption of scaphoid integrity, such as a fracture or nonunion, compromises this intricate linkage, leading to altered carpal mechanics, progressive collapse (SNAC wrist - Scaphoid Nonunion Advanced Collapse), and eventual osteoarthritis.
Indications & Contraindications
The volar approach is versatile, indicated for a range of scaphoid pathologies.
Indications
The volar approach provides good exposure of the scaphoid bone. It also avoids damaging the dorsal blood supply to the bone’s proximal half, as well as the superficial branch of the radial nerve. It leaves a more cosmetic scar than the dorsal approach, and its uses include the following:
1.
Bone grafting for nonunion of the scaphoid:
Especially for nonunions affecting the waist or distal pole, or those with volar collapse or humpback deformity.
2.
Excision of the proximal third of the scaphoid:
In cases of severe proximal pole avascular necrosis with intact distal fragment viability, or for salvage in specific scaphoid nonunion advanced collapse (SNAC) patterns.
3.
Excision of the radial styloid:
Either alone or combined with one of the above procedures, often performed for associated impingement or osteophytes.
4.
Open reduction and internal fixation of fractures of the scaphoid:
Particularly for distal pole fractures, scaphoid waist fractures with volar displacement or angulation, and for the insertion of long headless compression screws across the entire scaphoid. In such cases this approach frequently is combined with the dorsolateral approach to the scaphoid.
5.
Vascularized bone grafting procedures:
When a volar pedicle (e.g., from the distal radius) is utilized to treat proximal pole AVN, the volar approach facilitates both graft harvest and insertion.
Contraindications
Relative contraindications include:
*
Proximal pole fractures/nonunions with significant dorsal displacement:
The dorsal approach often provides better access for reduction and fixation in these specific scenarios.
*
Severe comminution of the scaphoid:
Making definitive internal fixation challenging via any approach.
*
Pre-existing significant radial artery compromise or anatomical variations:
Requiring careful consideration and potentially an alternative approach.
*
Patients with extreme wrist stiffness or contractures:
Which may limit exposure regardless of approach.
Operative vs. Non-Operative Indications
| Operative Indication (Volar Approach) | Non-Operative Indication |
|---|---|
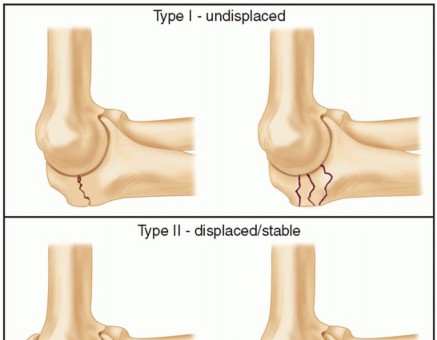
| Displaced or unstable scaphoid fractures (waist, distal pole) | Nondisplaced, stable scaphoid fractures (e.g., distal pole, tubercle) |
| Scaphoid nonunion (especially volar collapse/humpback) | Scaphoid stress reactions without frank fracture |
| Scaphoid nonunion with AVN requiring vascularized bone graft | Asymptomatic scaphoid pseudarthrosis (rarely, in elderly/low-demand patients) |
| Proximal pole excision (specific indications) | Acute scaphoid fractures with high suspicion but negative initial radiographs (serial imaging/CT/MRI) |
| Radial styloidectomy (often combined with scaphoid procedure) |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential for successful scaphoid surgery.
Imaging
- Standard Radiographs: PA, lateral, oblique (pronated 30°, supinated 30°) views of the wrist are crucial. Scaphoid views (ulnar deviation, PA) are often included.
- Computed Tomography (CT) Scans: Gold standard for assessing fracture displacement, comminution, fragment size, angulation (humpback deformity), and nonunion characteristics (sclerosis, cyst formation, gap size). 3D reconstructions are invaluable for understanding complex deformities and planning screw trajectory.
- Magnetic Resonance Imaging (MRI): Useful for assessing vascularity of the proximal pole (avascular necrosis), ligamentous injuries, and occult fractures not visible on plain radiographs or CT.
- Pre-operative Templating: Essential for determining appropriate screw length and diameter, bone graft dimensions, and ensuring adequate fixation.
Patient Preparation
- Anesthesia: Typically general anesthesia or regional anesthesia (e.g., axillary block) provides excellent intraoperative pain control and muscle relaxation.
- Antibiotic Prophylaxis: Administered pre-operatively in accordance with institutional guidelines.
- Patient Positioning: Place the patient supine on the operating table, with the arm lying on an arm board. Supinate the forearm to expose the volar aspect of the wrist, and apply an exsanguinating bandage and tourniquet. The hand and forearm should be prepped and draped to allow full wrist motion and access to potential bone graft donor sites (e.g., distal radius, iliac crest) if necessary. The use of a lead hand or an assistant to maintain forearm supination and wrist extension can be beneficial.

Figure 1: Patient positioned supine on the operating table with the arm on an arm board, forearm supinated, and hand draped to allow full wrist exposure and potential access to graft sites.
Detailed Surgical Approach / Technique
Landmarks and Incision
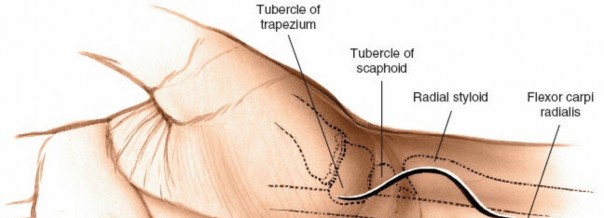
The primary landmark for the volar approach is the palpable scaphoid tubercle . The flexor carpi radialis (FCR) muscle lies radial to the palmaris longus muscle at the level of the wrist. It crosses the scaphoid before inserting into the base of the second and third metacarpals.
A longitudinal incision, approximately 3-4 cm in length, is typically made along the radial border of the FCR tendon. The incision should be centered over the scaphoid waist/tubercle, extending proximally from the distal wrist crease and distally into the thenar eminence towards the first web space if greater exposure of the distal pole and trapezium is required. Some surgeons prefer a slightly oblique incision following a natural skin crease to enhance cosmesis.
Figure 2: Identification of key volar landmarks including the scaphoid tubercle and the course of the flexor carpi radialis (FCR) tendon. The proposed incision line is marked along the radial border of the FCR.
Dissection
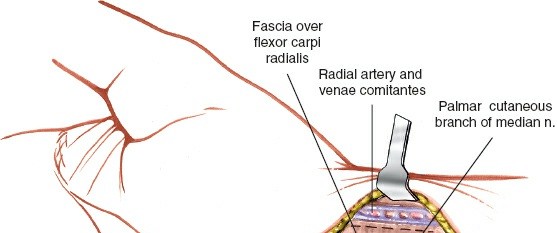
- Skin and Subcutaneous Tissue: Incise the skin and subcutaneous tissue. Meticulous hemostasis is important. Care should be taken to avoid injury to the palmar cutaneous branch of the median nerve, which typically courses radially to the palmaris longus (if present) and can be mistaken for the superficial radial artery if dissection is too far ulnar.
- FCR Sheath Incision: Identify the FCR tendon. A longitudinal incision is made in the retinacular sheath of the FCR tendon, directly along its radial border. The FCR tendon is then retracted ulnarly.

Figure 3: After skin incision, the FCR tendon sheath is incised longitudinally along its radial aspect, allowing for retraction of the FCR tendon ulnarly. The radial artery is visible and carefully protected.
- Radial Artery Identification and Protection: The radial artery lies immediately radial to the FCR tendon. It is crucial to identify and protect this vessel throughout the procedure. It should be carefully mobilized and retracted radially. Small perforating branches from the radial artery to the scaphoid tubercle may be encountered and, if possible, should be preserved. If necessary, a vessel loop can be used for gentle retraction.
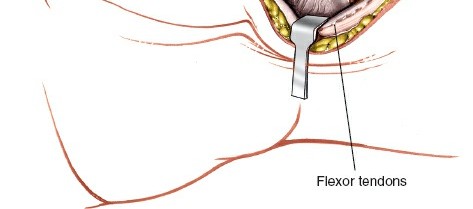
Figure 4: The radial artery has been identified and carefully retracted radially. Deeper structures, including the joint capsule and the exposed scaphoid, are now accessible.
- Capsular Incision and Scaphoid Exposure: Once the radial artery is safely retracted, the anterior capsule of the wrist joint is identified. A longitudinal or oblique capsular incision is made directly over the scaphoid, typically from the radial styloid to the base of the first metacarpal. This exposes the scaphoid tubercle, waist, and distal pole. The capsule can be tagged with sutures for easier repair later.
Procedure-Specific Steps
Bone Grafting for Nonunion
- Debridement of Nonunion Site: The fibrous tissue and sclerotic bone at the nonunion site are meticulously debrided using curettes, osteotomes, and burrs until healthy, bleeding bone is encountered on both fracture fragments. Any avascular necrotic bone (often in the proximal pole) should be removed or decorticated until viable bone is reached.
- Correction of Deformity: If a humpback deformity (volar collapse) is present, gentle distraction and manipulation (e.g., using K-wires as joysticks) are employed to restore the scaphoid's normal length and alignment. This often involves extending the wrist and applying traction. A temporary K-wire may be used to maintain reduction.
-
Bone Graft Harvest:
- Local Distal Radius Graft: A cortical-cancellous wedge or block graft can be harvested from the volar aspect of the distal radius (e.g., from the interval between the FCR and radial artery, or through a separate small incision more proximally). This location provides excellent cancellous bone.
- Iliac Crest Graft: For larger defects or when a more robust graft is needed, an autogenous tricortical iliac crest graft can be harvested.
- Vascularized Bone Graft: In cases of AVN, a vascularized graft (e.g., 1,2 intercompartmental supraretinacular artery (1,2 ICSRA) pedicle graft) may be considered.
- Graft Insertion and Shaping: The harvested bone graft is carefully shaped and impacted into the debrided nonunion site to restore scaphoid length and correct any volar angulation. It should fit snugly, providing structural support and osteoinductive/osteoconductive properties.
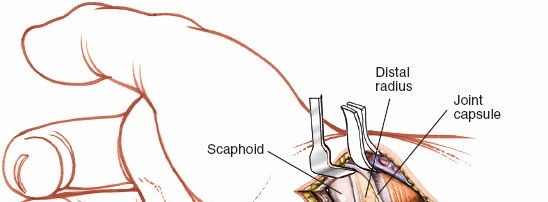
Figure 5: Preparation of a tricortical bone graft, often harvested from the iliac crest or distal radius, precisely contoured to fill the defect at the scaphoid nonunion site and restore anatomical alignment.
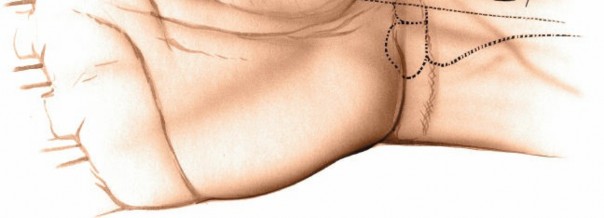
Figure 6: The carefully shaped bone graft is impacted into the debrided nonunion gap, effectively restoring scaphoid length and correcting any collapse deformity.
- Internal Fixation: Following graft placement, fixation is achieved, typically with a headless compression screw (e.g., Herbert, Acutrak, TwinFix). The screw is drilled under fluoroscopic guidance, starting from the distal pole/tubercle and crossing the nonunion site into the proximal pole. Proper trajectory is crucial to ensure optimal compression and stability. Multiple screws or K-wires may be used for specific fracture patterns or to stabilize the graft.
Open Reduction and Internal Fixation (ORIF) for Fractures
- Fracture Exposure: The volar approach allows direct visualization of distal pole and waist fractures.
- Reduction: The fracture fragments are meticulously reduced under direct visualization, often using K-wires as joysticks for manipulation. Careful attention is paid to restoring anatomical alignment and length, correcting any displacement or angulation. Temporary K-wire fixation can be used to hold the reduction.
-
Internal Fixation:
A headless compression screw is typically chosen for fixation.
- Pilot Hole: A guide wire is inserted from the scaphoid tubercle (distal pole) across the fracture site, aiming centrally into the proximal pole under fluoroscopic guidance (PA and lateral views).
- Drilling and Tapping: Over-drilling and tapping are performed according to the screw system's specifications.
- Screw Insertion: The headless compression screw is then inserted, achieving interfragmentary compression. The screw head should be countersunk beneath the articular surface of the scaphoid or within the bone to prevent impingement.
- Confirmatory Imaging: Fluoroscopic images (PA, lateral, oblique) are taken to confirm adequate reduction, screw position, and length.
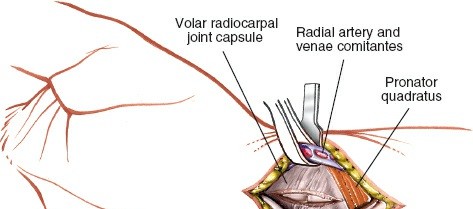
Figure 7: A headless compression screw is inserted from the distal scaphoid pole, across the fracture or nonunion site, and into the proximal pole under fluoroscopic guidance. This provides stable interfragmentary compression.
Excision of Proximal Third of Scaphoid or Radial Styloidectomy
- Proximal Pole Excision: After exposing the scaphoid, the proximal third is resected using an osteotome or small burr. This is typically followed by a soft tissue interposition arthroplasty (e.g., FCR flap) or conversion to a proximal row carpectomy (PRC) if indicated.
- Radial Styloidectomy: The radial styloid is identified. An osteotome or burr is used to resect the prominent portion of the radial styloid, addressing impingement issues. Care must be taken to protect the radial artery and its branches.
Closure
- Capsular Repair: The anterior wrist capsule is meticulously repaired using absorbable sutures to restore carpal stability and prevent adhesions.
- FCR Sheath Closure: The FCR retinacular sheath is repaired.
- Subcutaneous Tissue and Skin Closure: The subcutaneous layer is closed with absorbable sutures, followed by skin closure with non-absorbable sutures or staples.
- Dressing and Immobilization: A sterile dressing is applied. The wrist is typically immobilized in a short arm thumb spica cast or splint, with the wrist in slight flexion and radial deviation to maintain scaphoid reduction and minimize stress on the repair.
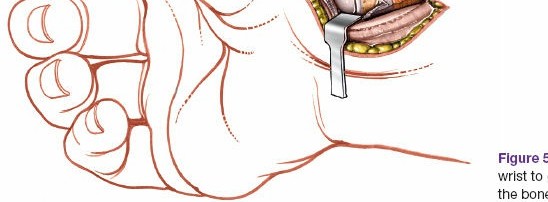
Figure 8: Post-operative radiograph demonstrating successful internal fixation of a scaphoid fracture with a headless compression screw. This confirms proper screw placement and fracture reduction.
Complications & Management
While the volar approach offers several advantages, potential complications must be recognized and managed appropriately.
| Complication | Incidence | Salvage / Management |
|---|---|---|
| Radial Artery Injury | <1-5% (spasm, laceration) | Prevention: Meticulous dissection, gentle retraction. Management: Vasospasm (topical papaverine), laceration (microsurgical repair, vein graft if necessary), ensure adequate distal perfusion. |
| Superficial Radial Nerve Injury | <1-3% (neuropraxia to neurotmesis) | Prevention: Careful skin incision, avoiding excessive radial extension. Management: Neuropraxia (observation, physiotherapy), neurotmesis (nerve repair, neurolysis, or grafting for persistent severe symptoms), desensitization. |
| Persistent Nonunion | 5-15% (varies with initial injury/graft) | Diagnosis: CT scan. Management: Revision surgery (repeat bone grafting, vascularized bone graft, re-fixation), salvage procedures (proximal row carpectomy, scaphoid excision and four-corner fusion, wrist arthrodesis for SNAC stage II/III). |
| Malunion / Deformity | <5% (e.g., persistent humpback) | Diagnosis: CT scan. Management: Corrective osteotomy and re-fixation, or salvage procedures if severe carpal collapse. |
| Infection | <1% (superficial to deep) | Prevention: Strict sterile technique, prophylactic antibiotics. Management: Superficial (oral antibiotics), deep (surgical debridement, IV antibiotics, hardware removal if necessary). |
| Hardware Complications | 5-10% (prominence, migration, breakage) | Prevention: Appropriate screw length/diameter, proper countersinking. Management: Symptomatic hardware removal after bone healing, revision fixation for migration/breakage compromising stability. |
| Flexor Carpi Radialis (FCR) Tenosynovitis | Uncommon | Prevention: Gentle FCR retraction, smooth sheath repair. Management: Rest, NSAIDs, corticosteroid injection, surgical release in refractory cases. |
| Median Nerve Irritation | Rare (palmar cutaneous branch) | Prevention: Careful dissection in the subcutaneous plane, avoiding overly ulnar extension of the incision. Management: Observation, anti-inflammatory agents, rarely nerve exploration. |
| Carpal Tunnel Syndrome | Rare (due to scar tissue or swelling) | Management: Observation, anti-inflammatory agents, rarely carpal tunnel release for persistent symptoms. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is critical for optimizing functional recovery and minimizing complications. Protocols vary based on the stability of fixation, bone quality, type of procedure (fracture vs. nonunion with graft), and surgeon preference.
Phase 1: Immobilization and Protection (0-6/8 weeks)
- Immobilization: Short arm thumb spica cast or splint, typically for 6-8 weeks (or longer for nonunions). The wrist is usually positioned in slight flexion and radial deviation to reduce stress on the scaphoid.
- Elevation: Continuous elevation of the hand above heart level to reduce swelling.
- Finger and Elbow ROM: Patients are encouraged to perform active range of motion (ROM) exercises for the fingers, thumb interphalangeal joint, and elbow to prevent stiffness.
- Weight-Bearing Restrictions: Strict non-weight-bearing for the affected limb.
- Monitoring: Regular wound checks, assessment of neurovascular status, and radiographic evaluation (typically at 2, 4, and 8 weeks) to monitor healing.
Phase 2: Controlled Mobilization (6/8 - 12 weeks)
- Cast/Splint Removal (based on radiographic evidence of healing): If radiographic union is progressing well, the cast may be removed, and a removable splint initiated.
- Gentle Active ROM: Initiation of gentle active wrist flexion, extension, radial, and ulnar deviation. Avoid passive stretching initially.
- Forearm Pronation/Supination: Initiate active forearm rotation.
- Gradual Strengthening: Begin isometric exercises for wrist and forearm muscles. Avoid heavy gripping or lifting.
- Scar Management: Initiate scar massage and desensitization techniques.
- Progression Criteria: Full, pain-free active wrist ROM and good radiographic evidence of union.
Phase 3: Strengthening and Functional Return (12 weeks onwards)
- Progressive Strengthening: Advance strengthening exercises with increased resistance, including grip strengthening, wrist curls, and forearm exercises.
- Proprioception and Dexterity: Incorporate activities to improve fine motor control and proprioception.
- Return to Activity: Gradual return to light activities of daily living and work-specific tasks. Sports-specific training is introduced in a progressive manner, typically avoiding impact or heavy loading until 4-6 months post-surgery.
- Monitoring: Continued radiographic assessment to confirm complete union before allowing unrestricted activities. A CT scan may be indicated to confirm complete bony bridging, especially in high-demand individuals or if concerns persist.
The total rehabilitation period can range from 3-6 months for uncomplicated fractures to 6-12 months or longer for complex nonunions, especially those with associated AVN. Patient compliance with rehabilitation protocols is paramount for achieving optimal long-term outcomes.
Summary of Key Literature / Guidelines
The volar approach remains a cornerstone in scaphoid surgery, with extensive literature supporting its efficacy for specific indications. Key themes in the literature include:
- Vascularity Preservation: Numerous studies highlight the advantage of the volar approach in preserving the dorsal carpal branch of the radial artery, which is the dominant blood supply to the proximal pole. This is a critical consideration in preventing or treating avascular necrosis, particularly in nonunions.
- Indications: The volar approach is consistently recommended for fractures and nonunions of the scaphoid waist and distal pole, especially those with volar displacement or a humpback deformity requiring correction. It is also favored for long compression screw placement traversing the entire scaphoid.
- Comparative Studies (Volar vs. Dorsal): While some studies indicate comparable union rates between volar and dorsal approaches for acute scaphoid waist fractures, the choice often depends on fracture pattern, surgeon preference, and the need to address specific deformities. The dorsal approach is generally preferred for proximal pole fractures or nonunions with significant dorsal displacement. For complex nonunions, often a combined approach or a single approach offering best access to the pathology is chosen.
- Bone Grafting Techniques: The literature widely supports the use of autogenous bone grafting (cancellous or cortical-cancellous) for scaphoid nonunions. Vascularized bone grafts, often harvested locally from the distal radius, have demonstrated superior results in cases complicated by established avascular necrosis of the proximal pole.
- Fixation Modalities: Headless compression screws are the gold standard for internal fixation, providing interfragmentary compression and allowing for early mobilization in stable constructs. Screw placement along the central axis of the scaphoid is critical for optimal biomechanical stability.
- Outcomes: Reported union rates for scaphoid fractures treated via the volar approach with internal fixation generally range from 90-98%. For scaphoid nonunions with bone grafting, union rates vary more widely (70-95%) depending on factors such as AVN presence, chronicity, and initial deformity. Long-term outcomes often emphasize the prevention of SNAC wrist and restoration of functional wrist motion and strength.
- Consensus: Current guidelines emphasize the importance of meticulous surgical technique, careful anatomical reduction, stable internal fixation, and individualized post-operative rehabilitation to achieve predictable and favorable outcomes following the volar approach to the scaphoid. Continued advancements in imaging, instrumentation, and biological augmentation strategies (e.g., bone morphogenetic proteins, platelet-rich plasma) are areas of ongoing research.
Clinical & Radiographic Imaging
You Might Also Like