Diagnosing SC Joint Osteoarthritis: What You Need to Know
Key Takeaway
This topic focuses on Diagnosing SC Joint Osteoarthritis: What You Need to Know, SC joint osteoarthritis is the most common condition affecting the sternoclavicular joint, often seen in individuals over 60 years old. It involves degenerative changes, which can be asymptomatic or cause pain and a palpable protuberance. Higher risk factors for sc joint osteoarthritis include postmenopausal women, chronic SC joint instability, and manual laborers.
Introduction & Epidemiology
Osteoarthritis (OA) of the sternoclavicular (SC) joint is a relatively common yet often underdiagnosed condition, presenting a significant source of anterior chest wall and shoulder girdle pain. While the SC joint is the only true articulation between the upper extremity and the axial skeleton, its pathologies frequently receive less attention than those of the glenohumeral or acromioclavicular joints. SC joint OA can arise from primary degenerative changes, post-traumatic etiologies, or secondary to repetitive microtrauma, particularly in athletes involved in contact sports, weightlifting, or overhead activities.
The epidemiology of SC joint OA is not as precisely defined as that of more common large joint arthropathies. However, it is generally accepted that its incidence increases with age, analogous to OA in other joints. Studies involving routine chest computed tomography (CT) scans for unrelated conditions have demonstrated radiographic evidence of SC joint degenerative changes in a significant proportion of asymptomatic individuals, suggesting a disconnect between radiographic findings and symptomatic disease. Symptomatic SC joint OA typically manifests in middle-aged to older adults, with a slight predilection for males, likely due to higher rates of trauma or participation in activities associated with joint stress. A history of previous SC joint injury, infection, or inflammatory arthropathy significantly elevates the risk for developing secondary OA. Furthermore, conditions such as hyperparathyroidism and diffuse idiopathic skeletal hyperostosis (DISH) can predispose to SC joint degeneration.
Diagnosis hinges on a thorough history and physical examination, complemented by appropriate imaging. Patients typically report localized pain over the anteromedial aspect of the clavicle, often exacerbated by arm elevation, abduction, or cross-body adduction. A characteristic "clicking," "popping," or grinding sensation may be present, sometimes accompanied by palpable crepitus. Swelling or prominence over the joint can also be observed. Differential diagnoses are broad and include SC joint instability (subluxation/dislocation), clavicular osteolysis, inflammatory arthritis, infection, tumor, Tietze's syndrome, and referred pain from cervical spine pathology or cardiac conditions. A high index of suspicion is crucial for accurate diagnosis.
Surgical Anatomy & Biomechanics
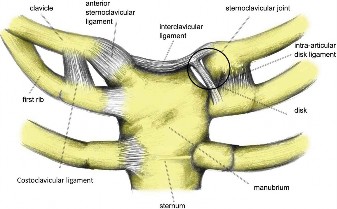
The sternoclavicular joint is a diarthrodial, saddle-type joint, allowing limited motion in three planes: elevation/depression, protraction/retraction, and axial rotation. Despite its small size, it plays a pivotal role in overall shoulder motion and stability. The joint is formed by the medial end of the clavicle, the manubrium of the sternum, and the first costal cartilage. The articular surfaces are incongruent, with the medial clavicle being larger than the sternal facet. This incongruity is compensated for by a complete fibrocartilaginous articular disc, which acts as a shock absorber, improves congruence, and divides the joint into two separate synovial cavities. The disc is firmly attached superiorly to the posterolateral aspect of the clavicle and inferiorly to the junction of the first rib cartilage and the sternum.
The primary stabilizers of the SC joint are its robust ligamentous structures:
*
Anterior and Posterior Sternoclavicular Ligaments:
These are strong capsular thickenings that reinforce the joint anteriorly and posteriorly, preventing anterior and posterior dislocation, respectively. The posterior ligament is generally considered stronger than the anterior.
*
Interclavicular Ligament:
Connecting the superior aspects of the medial clavicles, crossing the jugular notch, this ligament helps prevent superior displacement of the clavicle and reinforces the superior capsule.
*
Costoclavicular Ligament (Rhomboid Ligament):
This is an extremely strong extra-articular ligament connecting the inferior surface of the medial clavicle to the superior surface of the first rib. It is the primary stabilizer against superior displacement and also restricts excessive protraction and retraction, acting as the primary pivot point for clavicular rotation during shoulder motion.
The capsular attachments are relatively weak superiorly and inferiorly but are significantly reinforced by the sternoclavicular ligaments. The medial physis of the clavicle is the last physis in the body to close, typically around 20-25 years of age, making epiphyseal fractures or Salter-Harris injuries more common in adolescents and young adults than true ligamentous ruptures.
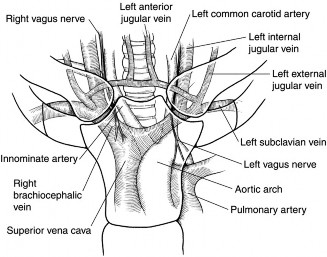
Neurovascular structures in close proximity to the posterior aspect of the SC joint pose significant risks during surgical intervention. These include the brachiocephalic (innominate) artery, subclavian artery and vein, internal jugular vein, vagus nerve, phrenic nerve, recurrent laryngeal nerve, trachea, esophagus, and the thoracic duct on the left side. Understanding these relationships is paramount to avoid catastrophic complications during posterior dissection. The anterior deltoid and pectoralis major muscles overlie the joint anteriorly, with the sternal head of the sternocleidomastoid muscle located medially. The platysma muscle lies subcutaneously.
Biomechanically, the SC joint permits approximately 35-45 degrees of elevation, 10-15 degrees of depression, 15-30 degrees of protraction, and 15-30 degrees of retraction. Additionally, it allows 40-50 degrees of axial rotation of the clavicle, which is critical for full range of motion of the glenohumeral joint, particularly during overhead activities. Degenerative changes, such as osteophytes, articular cartilage wear, and meniscal degeneration, can impinge on these movements, leading to pain and restricted motion. The articular disc, being an intra-articular structure, can also degenerate or tear, contributing to pain and mechanical symptoms.
Indications & Contraindications
The management of SC joint osteoarthritis typically follows a stepwise approach, prioritizing conservative measures before considering surgical intervention. Surgery is generally reserved for patients with persistent, debilitating pain and functional impairment despite an adequate trial of non-operative treatment.
Indications for Surgical Intervention (Medial Clavicle Resection Arthroplasty):
*
Failed Conservative Management:
Persistent, severe pain and functional limitation lasting at least 3-6 months, refractory to comprehensive non-operative treatments. This includes rest, activity modification, NSAIDs, physical therapy focusing on periscapular strengthening and posture correction, corticosteroid injections, and possibly multimodal pain management.
*
Mechanical Symptoms:
Significant grinding, clicking, or crepitus associated with pain and limitation, suggesting intra-articular pathology (e.g., degenerative disc tears, osteophyte impingement).
*
Radiographic Evidence:
Clear radiographic signs of SC joint osteoarthritis (joint space narrowing, osteophytes, subchondral sclerosis, cysts) correlating with clinical symptoms.
*
Positive Diagnostic Injection:
Temporary but significant pain relief (e.g., >50%) after a local anesthetic injection into the SC joint, confirming the joint as the primary pain generator.
Contraindications for Surgical Intervention:
*
Active Infection:
Any local or systemic active infection.
*
Uncontrolled Systemic Disease:
Poorly controlled diabetes, cardiovascular disease, or other comorbidities that significantly increase surgical risk.
*
Unrealistic Patient Expectations:
Inability of the patient to comprehend potential outcomes, risks, or commitment to post-operative rehabilitation.
*
Lack of Conservative Trial:
Insufficient duration or adherence to non-operative treatment protocols.
*
Unconfirmed Diagnosis:
Pain not clearly originating from the SC joint, or confounding pathologies.
*
Symptomatic SC Joint Instability:
While OA can coexist with instability, primary instability may require different surgical approaches (e.g., reconstruction/fusion) rather than simple resection. However, chronic instability leading to secondary OA might be amenable to resection if instability is not the dominant feature.
Operative vs. Non-Operative Indications
| Feature / Treatment Modality | Non-Operative Management | Operative Management (Medial Clavicle Resection) |
|---|---|---|
| Pain Level | Mild to Moderate | Severe, disabling, refractory to conservative care |
| Functional Limitation | Intermittent, manageable | Constant, significantly limits ADLs, work, sport |
| Response to PT/NSAIDs | Positive or partial relief | Minimal or no sustained relief |
| Joint Injections | May provide temporary relief, diagnostic | Diagnostic (confirm pain source), palliative (temporary) |
| Radiographic Severity | Early degenerative changes | Advanced degenerative changes (grade 3-4 OA) |
| Mechanical Symptoms | Absent or mild crepitus | Persistent clicking/grinding with pain, catching |
| Patient Age/Activity | Any, but often preferred for elderly/low demand | Typically younger, active patients with high functional demands, or elderly with severe pain |
| Comorbidities | Significant (high surgical risk) | Minimal or well-controlled |
| Psychosocial Factors | High anxiety, somatization | Stable, motivated, realistic expectations |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is critical to ensure a safe and effective surgical outcome for SC joint osteoarthritis, particularly given the proximity of vital neurovascular structures.
Imaging Review
- Standard Radiographs: Anteroposterior (AP) and Serendipity (40-degree cephalic tilt) views are essential to evaluate joint space narrowing, osteophytes, and subchondral sclerosis. The Serendipity view is particularly useful for assessing superior-inferior displacement or osteophyte formation.
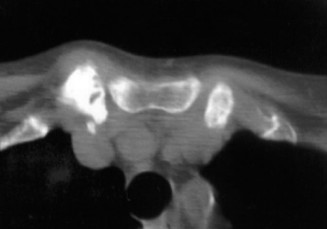
- Computed Tomography (CT) Scan: The gold standard for evaluating bony morphology, extent of osteophytes, joint space narrowing, and articular destruction. A CT scan with fine cuts and 3D reconstructions can precisely delineate the medial clavicle and its relationship to the sternum and first rib, as well as identify posterior osteophytes or involvement of the costoclavicular ligament. This is invaluable for surgical planning, especially when considering the extent of bone resection.
- Magnetic Resonance Imaging (MRI): While less effective for bony detail, MRI can assess soft tissue structures, including the articular disc, joint capsule, surrounding ligaments, and identify concomitant pathologies like disc tears, synovitis, or bone marrow edema, which may contribute to pain. It can also help rule out inflammatory conditions or tumors.
- Diagnostic Injection: A fluoroscopy-guided or ultrasound-guided injection of local anesthetic and corticosteroid into the SC joint is often performed pre-operatively. Significant (e.g., >50%) temporary pain relief confirms the SC joint as the primary pain generator and is a strong predictor of surgical success.
- Neurovascular Assessment: In cases of severe posterior osteophyte formation or previous trauma, a vascular surgeon consultation or pre-operative angiography/CTA may be considered, although this is rare for primary OA.
Patient Education and Consent
Comprehensive discussion with the patient regarding the nature of SC joint OA, the rationale for surgery, expected outcomes, potential complications (including specific neurovascular risks), and the post-operative rehabilitation protocol is mandatory.
Anesthesia
General anesthesia is typically employed. Regional nerve blocks (e.g., superficial cervical plexus block) may be used adjunctively for post-operative pain control, but care must be taken to avoid obscuring potential nerve injury during surgery.
Patient Positioning and Preparation
- Position: Supine position on the operating table.
- Shoulder Roll: A rolled blanket or specialized shoulder bump is placed longitudinally between the scapulae, extending from the occiput to the sacrum. This maneuver helps to retract the shoulders posteriorly, bringing the sternum and SC joints into a more prominent and accessible position. It also aids in preventing posterior translation of the clavicle during the procedure.
- Arm Positioning: The ipsilateral arm is placed on an arm board, allowing for manipulation and range of motion assessment during the procedure if necessary, though this is less critical for medial clavicle resection.
- Draping: Standard sterile preparation and draping to expose the entire shoulder girdle, upper chest, and neck area. Consideration should be given to including the contralateral SC joint in the sterile field for anatomical comparison or potential graft harvest if reconstruction is planned (though less common for OA).
- Fluoroscopy: Intraoperative fluoroscopy may be available, though often not strictly necessary for medial clavicle resection unless complex osteotomy or hardware placement is anticipated.
- Identification of Landmarks: Palpate and mark the sternal notch, medial clavicle, and sternoclavicular joint line.
Detailed Surgical Approach / Technique
The most common surgical intervention for symptomatic SC joint osteoarthritis is medial clavicle resection arthroplasty. This procedure aims to decompress the joint and remove degenerative bone that is causing pain and impingement. For severe instability leading to secondary OA, or when instability is the primary driver, other techniques such as reconstruction or fusion may be considered, but resection is typically the first line for primary OA.
Medial Clavicle Resection Arthroplasty
-
Incision:
- A transverse incision approximately 4-6 cm in length is made directly over the SC joint. This curvilinear incision should ideally follow Langer's lines to optimize cosmetic outcome.
- Alternatively, an oblique incision parallel to the medial border of the clavicle can be used.
- The incision extends through the skin and subcutaneous tissue.
- Care is taken to identify and preserve branches of the supraclavicular nerve.
-
Platysma and Fascia Dissection:
- The platysma muscle, if present in the field, is carefully incised transversely or separated vertically in line with its fibers.
- The superficial fascia is then incised.
-
Exposure of SC Joint:
- The sternal head of the sternocleidomastoid (SCM) muscle is identified. It may need to be retracted superiorly and medially to expose the superior and anterior aspects of the medial clavicle. While some advocate for partial detachment of the SCM, often gentle retraction suffices.
- The fibers of the pectoralis major muscle attach inferiorly and anteriorly to the medial clavicle and may also require retraction.
- The anterior capsule of the SC joint is identified.
-
Capsular Incision and Joint Inspection:
- A transverse or longitudinal incision is made in the anterior capsule of the SC joint, carefully staying close to the clavicular side to avoid injury to the sternal attachment of the articular disc or posterior structures.
- The joint is opened, and the articular surfaces of the medial clavicle, sternum, and the articular disc are inspected. Degenerative changes, osteophytes, and disc pathology are confirmed.
-
Medial Clavicle Resection:
- The amount of clavicle to be resected is typically 1.5 to 2.0 cm. Resection of less than 1.5 cm may not adequately decompress the joint, while excessive resection can lead to instability.
- Using a fine-tipped electrocautery or small periosteal elevator, the posterior capsule and periosteum are carefully elevated from the posterior aspect of the medial clavicle. This step is critical to protect the underlying neurovascular structures. A blunt instrument (e.g., Doyen elevator or bent malleable retractor) is often inserted posteriorly to shield these structures during the osteotomy.
- Oscillating Saw: An oscillating saw with a narrow blade is used to make the osteotomy cuts. The first cut is typically made perpendicular to the long axis of the clavicle, approximately 1.5-2.0 cm lateral to the medial end.
- Second Cut: A second cut is made obliquely or parallel to the sternal facet, removing a wedge or block of bone. The goal is to remove the diseased articular surface and underlying subchondral bone, ensuring adequate space is created between the remaining clavicular stump and the sternum.
- Smoothing and Debridement: After the bone is resected, a high-speed burr or rongeur is used to smooth any sharp edges of the remaining clavicle. All osteophytes from the sternum and first rib should also be carefully removed to prevent impingement.
- Soft Tissue Interposition (Optional): Some surgeons advocate for interposition of soft tissue (e.g., local fascia, sternocleidomastoid flap, or synthetic material) into the resection gap to prevent bony regrowth and further impingement. This remains controversial, and many achieve good results without interposition.
-
Hemostasis and Closure:
- Thorough hemostasis is achieved using electrocautery or ligatures.
- The deep fascia is closed, often including the anterior capsule, loosely to allow for the new joint space.
- The platysma (if incised) is repaired.
- Subcutaneous layers are closed, followed by skin closure with sutures or staples.
- A sterile dressing is applied.
Arthroscopic Medial Clavicle Resection
While open medial clavicle resection is the traditional approach, arthroscopic techniques have been described. These may offer advantages in terms of smaller incisions, less soft tissue disruption, and potentially faster recovery. However, arthroscopy of the SC joint is technically demanding due to its tight confines and the proximity of neurovascular structures. It typically requires specialized instrumentation and experience.
- Portals: Usually involves an anterosuperior portal for the arthroscope and an anteroinferior working portal, or an anteromedial and anterolateral portal.
- Procedure: A small shaver and burr are used to resect the medial clavicle and debride the joint.
- Challenges: Limited visualization, restricted working space, and the persistent risk of neurovascular injury require extreme caution. Arthroscopic guidance for needle placement for posterior protection can be particularly useful.
The choice between open and arthroscopic approach often depends on surgeon preference, experience, and the specific patient's anatomy and pathology. For complex cases or revision surgery, an open approach may offer better control and visualization.
Complications & Management
Surgical intervention at the sternoclavicular joint, while often effective, carries a distinct set of potential complications, largely due to its intricate anatomy and proximity to vital neurovascular structures. Meticulous surgical technique, thorough pre-operative planning, and an understanding of potential pitfalls are paramount for minimizing these risks.
Common Complications and Management Strategies
| Complication | Incidence (Approximate) | Management Strategies |
|---|---|---|
| Neurovascular Injury | <1% (but potentially catastrophic) | Prevention is key. Meticulous dissection with blunt posterior retraction/shielding (Doyen, malleable retractor) during osteotomy. Use of oscillating saw with controlled passes. Careful hemostasis. Management: Immediate vascular surgery consultation for vessel injury; neurosurgery/thoracic surgery for nerve/pleural injury. Resuscitation and operative repair. |
| Pneumothorax | <1% | Prevention: Avoid deep posterior penetration. Management: Immediate recognition, chest tube insertion, respiratory support. |
| Infection (Superficial/Deep) | 1-5% (similar to other clean orthopaedic surgeries) | Prevention: Standard aseptic technique, prophylactic antibiotics. Management: Superficial: wound care, oral antibiotics. Deep: surgical debridement, IV antibiotics, removal of any foreign material (if present from other procedures like fixation). |
| Hematoma/Seroma | 5-10% | Prevention: Meticulous hemostasis, consider drain placement in selected cases. Management: Small hematomas often resolve spontaneously. Large/symptomatic: aspiration, re-exploration, or surgical evacuation. |
| Recurrence of Pain/Impingement | 5-15% (can vary with resection amount) | Prevention: Adequate initial resection (1.5-2.0 cm), complete removal of osteophytes. Management: Conservative management (PT, injections). If persistent and debilitating, revision surgery for further resection or soft tissue interposition may be considered. |
| Instability (Post-Resection) | Rare for appropriate resection | Prevention: Adequate resection size (not too much), preservation of costoclavicular ligament. Management: Mostly conservative. For severe symptomatic instability, reconstruction (e.g., using sternocleidomastoid tendon or synthetic grafts) or fusion may be required, although this is unusual after medial clavicle resection for OA. |
| Prominent Scar | Variable | Prevention: Transverse incision following Langer's lines, meticulous skin closure, gentle tissue handling. Management: Silicone sheeting, massage, topical steroids, or scar revision in severe cases. |
| Nonunion/Malunion (if Fusion) | 5-10% (for fusion procedures) | Prevention: Robust internal fixation, adequate decortication, bone grafting, protected weight-bearing. Management: Non-symptomatic nonunion may be observed. Symptomatic: revision surgery with debridement, fresh bone graft, and potentially more stable fixation. |
| Symptomatic Hardware (if Fixation) | 5-10% | Prevention: Use low-profile hardware, careful placement. Management: Hardware removal after bony union, typically 12-18 months post-operatively, if symptomatic. |
| Post-Operative Stiffness/Adhesions | 5-10% | Prevention: Early, controlled range of motion exercises as per rehabilitation protocol. Management: Aggressive physical therapy, stretching, possibly manipulation under anesthesia in refractory cases. |

Key Considerations for Salvage Strategies
- Careful Evaluation: For recurrent pain or instability, a thorough workup including repeat imaging (CT, MRI) and diagnostic injections is essential to identify the exact cause.
- Multidisciplinary Approach: In complex cases, collaboration with vascular, thoracic, or pain management specialists may be beneficial.
- Patient Expectations: Manage patient expectations regarding the complexity of revision surgery and the potential for residual symptoms.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following medial clavicle resection arthroplasty for SC joint osteoarthritis is crucial for optimizing functional outcomes and minimizing complications. The protocol aims to protect the surgical site while gradually restoring range of motion, strength, and function. While specific protocols may vary slightly based on surgeon preference and intraoperative findings (e.g., amount of resection, interpositional graft), a phased approach is generally followed.
Phase I: Immediate Post-Operative (Weeks 0-2)
- Goals: Pain control, protect surgical site, minimize swelling, initiate gentle motion.
- Immobilization: The arm is typically placed in a sling for comfort and protection, especially during sleep and in crowded environments. The sling is typically removed for exercises and personal hygiene.
- Pain Management: Oral analgesics, NSAIDs, and cryotherapy.
-
Activity Restrictions:
- No active shoulder flexion or abduction beyond 90 degrees.
- No heavy lifting or carrying.
- Avoid direct pressure on the surgical site.
- No pushing, pulling, or reaching overhead.
-
Exercises:
- Elbow, Wrist, Hand Range of Motion (ROM): Actively perform multiple times daily to prevent stiffness.
- Pendulum Exercises: Gentle, pain-free pendulum swings of the ipsilateral arm.
- Scapular Mobility: Gentle scapular retraction and protraction exercises.
- Posture Awareness: Maintain good posture to support shoulder girdle mechanics.
Phase II: Early Motion and Strengthening (Weeks 2-6)
- Goals: Restore full passive and active-assisted ROM, begin gentle active ROM, protect healing tissues.
- Sling Use: Gradually discontinue sling use as comfort allows, typically by the end of this phase.
- Activity Restrictions: Continue to avoid heavy lifting, pushing, pulling, and impact activities.
-
Exercises:
- Passive Range of Motion (PROM): Progress to full passive shoulder flexion, abduction, and external rotation, respecting pain.
- Active-Assisted Range of Motion (AAROM): Use a wand or the contralateral arm to assist in full ROM exercises.
- Gentle Active Range of Motion (AROM): Begin active shoulder flexion, abduction, internal and external rotation within pain-free limits.
- Isometric Strengthening: Initiate gentle isometric exercises for the rotator cuff and periscapular muscles (e.g., against a wall).
- Thoracic Mobility: Continue with thoracic spine extension and rotation exercises.
Phase III: Progressive Strengthening (Weeks 6-12)
- Goals: Restore full active ROM, improve strength, endurance, and proprioception.
- Activity Restrictions: Gradual return to light functional activities. Continue to avoid heavy overhead lifting and contact sports.
-
Exercises:
- Progressive Resistive Exercises (PREs): Using light weights, resistance bands, or body weight for rotator cuff and scapular stabilizer muscles (e.g., rows, external rotation, internal rotation, shoulder presses below 90 degrees).
- Core Strengthening: Essential for overall stability and kinetic chain involvement.
- Proprioception and Neuromuscular Control: Exercises using balance boards or unstable surfaces (if appropriate).
- Increased Duration and Intensity: Gradually increase repetitions and sets as tolerated.
Phase IV: Advanced Strengthening and Return to Activity (Weeks 12+)
- Goals: Maximize strength, power, and endurance; prepare for return to specific activities or sports.
- Activity Restrictions: Gradual and progressive return to sport-specific or work-specific activities. Supervision and guidance from the physical therapist are crucial.
-
Exercises:
- Sport-Specific Training: Incorporate activities that mimic demands of the patient's sport or occupation.
- Plyometric Exercises: For throwing or overhead athletes, introduce plyometrics as appropriate.
- Heavy Resistance Training: Gradually increase weight and resistance, including overhead activities if tolerated and necessary.
- Maintenance Program: Patients should be educated on a long-term home exercise program to maintain strength and flexibility.
Important Considerations:
*
Individualization:
Rehabilitation protocols must be tailored to the individual patient's progress, pain level, and functional goals.
*
Pain as a Guide:
Exercises should always be performed within a pain-free range.
*
Communication:
Regular communication between the surgeon, physical therapist, and patient is vital for successful outcomes.
*
Potential for Protracted Recovery:
Some patients may experience residual stiffness or discomfort for several months, requiring patience and continued adherence to the rehabilitation program. Full recovery can take 6-12 months.
Summary of Key Literature / Guidelines
The understanding and management of SC joint osteoarthritis, particularly surgical interventions, are supported by a body of literature that has evolved over time. While not as extensively studied as larger joints, key principles and outcomes have been established.
- Diagnosis and Imaging: Current consensus emphasizes the role of plain radiographs (AP, Serendipity views) as initial screening, with CT scans being the definitive imaging modality for bony detail and assessment of degenerative changes. MRI provides valuable information on soft tissue pathology (e.g., disc tears, synovitis) and can help differentiate other conditions. Diagnostic anesthetic injections are considered highly valuable for confirming the SC joint as the pain generator.
- Conservative Management: The literature consistently supports a trial of non-operative management as the first line of treatment. This includes activity modification, NSAIDs, physical therapy focusing on periscapular and core strengthening, and corticosteroid injections. Success rates for conservative care vary, but surgical intervention is generally reserved for those failing a comprehensive trial.
-
Surgical Outcomes for Medial Clavicle Resection Arthroplasty:
Numerous case series and retrospective studies have demonstrated favorable outcomes for medial clavicle resection arthroplasty in alleviating pain and improving function in patients with symptomatic SC joint OA resistant to conservative treatment.
- Pain Relief: Patients typically report significant reduction in pain scores post-operatively.
- Functional Improvement: Improvements in shoulder range of motion and ADL scores are commonly observed.
- Complication Rates: While overall complication rates are generally low, the potential for severe neurovascular injury is a critical consideration. Studies highlight the importance of meticulous surgical technique and careful posterior protection. Recurrence of impingement or pain can occur if inadequate bone is resected.
- Amount of Resection: The optimal amount of medial clavicle resection is generally quoted as 1.5 to 2.0 cm. Resection of less than 1.5 cm may lead to persistent impingement, while resection exceeding 2.0-2.5 cm carries a theoretical risk of iatrogenic instability, though this is less commonly reported in the OA literature compared to instability-specific procedures.
- Arthroscopic vs. Open Approaches: While open medial clavicle resection remains the gold standard due to superior visualization and control, arthroscopic techniques have gained traction. Comparative studies are limited, but arthroscopy may offer benefits in terms of smaller incisions and potentially reduced post-operative pain. However, the technical difficulty and inherent risks associated with arthroscopic access to this confined space require specialized training and expertise.
- Role of Soft Tissue Interposition: The use of interpositional soft tissue (e.g., local capsule, muscle, fascia) to fill the resection gap and prevent bony regrowth is a debated topic. Some surgeons advocate for it, believing it improves outcomes, while others achieve good results without it. Current literature does not definitively prove a superior outcome with routine interposition.
- Rehabilitation: Post-operative protocols emphasize early controlled motion to prevent stiffness, followed by progressive strengthening of the shoulder girdle and core musculature. Adherence to a structured rehabilitation program is crucial for achieving optimal long-term results.
Key Guidelines and Recommendations:
*
Patient Selection:
Strict adherence to surgical indications, including failed conservative management and objective evidence of SC joint pathology correlating with symptoms, is paramount.
*
Pre-operative Imaging:
Comprehensive imaging, particularly CT scans, is essential for surgical planning and identifying potential anatomical variants or risks.
*
Surgical Technique:
Emphasis on precise resection, adequate bone removal, and meticulous protection of posterior neurovascular structures is critical.
*
Informed Consent:
Thorough discussion of risks, benefits, and alternatives, including specific details regarding potential neurovascular complications, is mandatory.
In conclusion, the management of SC joint osteoarthritis, especially when considering surgical intervention, requires a thorough diagnostic workup, a clear understanding of the complex anatomy, and meticulous surgical execution. Medial clavicle resection arthroplasty remains a reliable procedure for providing pain relief and functional improvement in appropriately selected patients. Continued research into novel techniques, long-term outcomes, and specific patient populations will further refine management strategies for this challenging joint.
Clinical & Radiographic Imaging
You Might Also Like