Total Shoulder Arthroplasty: When Glenohumeral OA Needs Surgery

Key Takeaway
Discover the latest medical recommendations for Total Shoulder Arthroplasty: When Glenohumeral OA Needs Surgery. Total shoulder arthroplasty (TSA) is an operative treatment addressing chronic shoulder pain and disability. It is recommended when conservative measures, including pain medication, physical therapy, and corticosteroid injections, fail to provide lasting relief. Preoperative planning often involves CT scans to assess glenoid bone stock and version for optimal component placement.
Introduction & Epidemiology
Glenohumeral osteoarthritis (GHOA) represents a progressive degenerative joint disease characterized by cartilage loss, subchondral bone sclerosis, osteophyte formation, and joint space narrowing, leading to pain, stiffness, and functional impairment. Total Shoulder Arthroplasty (TSA), first conceptualized by Charles Neer II in the 1950s, has evolved significantly to become a highly effective surgical intervention for advanced, symptomatic GHOA refractory to conservative management. The primary objective of TSA is to alleviate pain and restore functional range of motion by resurfacing both the humeral head and the glenoid fossa.
Epidemiologically, GHOA affects a substantial portion of the adult population, with radiographic evidence present in up to 16% of individuals over 65 years of age. Symptomatic GHOA, however, is less common, affecting approximately 1-2% of adults. The incidence of TSA has steadily increased over the past two decades, driven by an aging population, improved surgical techniques, and expanded indications. While anatomic TSA (aTSA) remains the gold standard for GHOA with an intact and functional rotator cuff, the advent and widespread adoption of reverse Total Shoulder Arthroplasty (RTSA) have broadened the scope of arthroplasty to include cases with rotator cuff deficiency, such as cuff tear arthropathy (CTA) or complex fracture sequelae, which may also develop secondary degenerative changes. Outcomes for both aTSA and RTSA for appropriate indications demonstrate significant improvements in pain relief, patient-reported outcome measures (PROMs), and functional capabilities, with survivorship rates exceeding 90% at 10 years for aTSA in experienced hands.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the shoulder is paramount for successful TSA. The glenohumeral joint is a ball-and-socket articulation, designed for vast mobility at the expense of inherent stability.
The
deltopectoral approach
is the most common anterior approach for TSA, utilizing the interval between the deltoid and pectoralis major muscles.
*
Deltoid:
Innervated by the axillary nerve (C5, C6). Its integrity and function are critical for shoulder elevation and external rotation.
*
Pectoralis Major:
Innervated by the medial and lateral pectoral nerves (C5-T1). Forms the medial border of the surgical interval.
*
Cephalic Vein:
Located within the deltopectoral groove, it serves as a reliable landmark, typically retracted medially with the pectoralis major.
*
Clavipectoral Fascia:
Lies deep to the deltopectoral interval, covering the coracobrachialis, short head of the biceps, and subscapularis. Its incision allows access to the joint capsule.
*
Coracoid Process:
A key anatomical landmark, serving as the origin for the coracobrachialis, short head of the biceps, and pectoralis minor.
*
Neurovascular Structures:
*
Axillary Nerve:
Arises from the posterior cord of the brachial plexus (C5, C6), courses inferiorly and posteriorly, passing inferior to the humeral head and through the quadrangular space (bounded by the teres minor superiorly, teres major inferiorly, long head of triceps medially, and surgical neck of the humerus laterally). It is highly vulnerable during inferior capsular release, humeral head resection, and glenoid exposure. Typically 4-7 cm inferior to the acromion.
*
Musculocutaneous Nerve:
Arises from the lateral cord of the brachial plexus, innervates the coracobrachialis, biceps brachii, and brachialis. Lies medial to the coracoid process.
*
Brachial Plexus:
Located superior and medial to the coracoid.
*
Anterior Circumflex Humeral Artery:
Crosses the surgical neck of the humerus anteriorly, supplying the humeral head. Often encountered during subscapularis tenotomy or lesser tuberosity osteotomy.
Rotator Cuff:
*
Subscapularis:
Anterior rotator cuff muscle, crucial for internal rotation. Innervated by the upper and lower subscapular nerves. It must be mobilized or released for humeral head and glenoid exposure.
*
Supraspinatus, Infraspinatus, Teres Minor:
Posterior and superior rotator cuff muscles, vital for elevation and external rotation. Innervated by the suprascapular nerve (supraspinatus, infraspinatus) and axillary nerve (teres minor).
Biomechanics:
The native glenohumeral joint is characterized by a high conformity and a concave glenoid surface that articulates with a convex humeral head. The center of rotation (COR) is typically within the glenoid fossa.
*
aTSA:
Aims to restore the native anatomy and biomechanics, including glenoid version, inclination, humeral head height, and version. Proper restoration of the COR is crucial to minimize stresses on the glenoid component, optimize rotator cuff function, and achieve stability. Mismatched version or inclination can lead to impingement, eccentric loading, and component loosening.
*
RTSA:
Fundamentally alters the shoulder biomechanics by medializing and distalizing the COR. This conversion of the glenoid to a convex "glenosphere" and the humerus to a concave "humeral cup" transforms the deltoid into a more efficient elevator and abductor, bypassing the need for a functional rotator cuff. However, this biomechanical alteration places increased stress on the scapula (potential for notching, acromial fractures) and necessitates careful soft tissue balancing.
Indications & Contraindications
The decision for TSA is based on a comprehensive assessment of patient symptoms, functional limitations, radiographic findings, and the patient's overall health and expectations.
Indications for Total Shoulder Arthroplasty (aTSA/RTSA)
-
Primary Glenohumeral Osteoarthritis (GHOA):
- Severe, debilitating pain refractory to non-operative treatment.
- Significant loss of active and passive range of motion.
- Radiographic evidence of severe joint space narrowing, subchondral sclerosis, osteophytes, and sometimes humeral head collapse or glenoid erosion.
- Anatomic TSA: Indicated when the rotator cuff is intact and functional, and there is adequate glenoid bone stock. Concentric glenoid wear is most favorable.
- Reverse TSA: Indicated in specific GHOA patterns, such as severe eccentric posterior glenoid wear with biconcave glenoid, or when associated with irreparable rotator cuff deficiency (cuff tear arthropathy).
-
Post-traumatic Osteoarthritis:
- Sequelae of remote fractures (e.g., proximal humerus fractures, glenoid fractures) leading to painful arthritis, malunion, or nonunion.
-
Inflammatory Arthritis:
- Rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, leading to significant joint destruction and pain.
- Often involves diffuse bone loss and rotator cuff compromise, potentially favoring RTSA.
-
Osteonecrosis of the Humeral Head:
- Advanced stages (e.g., Ficat Stage III or IV) with humeral head collapse and pain.
-
Cuff Tear Arthropathy (CTA):
- Irreparable rotator cuff tear with superior humeral head migration, leading to glenohumeral degeneration and pain. Primarily an indication for RTSA.
-
Failed Previous Shoulder Surgery:
- Unsuccessful arthroscopic debridement, hemiarthroplasty, or prior arthroplasty with implant failure or infection eradication.
Contraindications for Total Shoulder Arthroplasty
-
Absolute Contraindications:
- Active Infection: Absolute contraindication. Infection must be thoroughly eradicated prior to considering arthroplasty.
- Deltoid Paralysis or Irreparable Deltoid Deficiency: Contraindication for RTSA, as deltoid function is critical for its success.
- Irreparable Rotator Cuff Deficiency (for aTSA): Leads to early failure of anatomic implants due to superior migration and eccentric loading.
- Uncontrolled Medical Comorbidities: Severe cardiac, pulmonary, or neurologic conditions that preclude safe anesthesia or surgery.
- Neuropathic Arthropathy (Charcot Joint): High risk of catastrophic failure.
- Severe Bone Loss: Inability to achieve stable component fixation (absolute for both, though RTSA can often manage more severe glenoid bone loss than aTSA).
-
Relative Contraindications:
- Poor Patient Compliance: Unwillingness or inability to adhere to rehabilitation protocols.
- Psychiatric Disorders: Uncontrolled mental health issues.
- Younger Patients: Given the finite lifespan of implants, aTSA is generally reserved for patients typically over 55-60 years of age, though individualized decisions are made.
- Progressive Neurological Disease: May compromise long-term outcomes.
- Prior Radiation Therapy: May affect bone quality and soft tissue healing.
- Active Smoking: Significantly increases infection risk and impairs healing. Should be optimized pre-operatively.
Table 1: Operative vs. Non-Operative Indications for Glenohumeral Osteoarthritis
| Feature/Intervention | Non-Operative Management | Operative Management (TSA) |
|---|---|---|
| Pain | Mild to moderate, intermittent | Severe, constant, debilitating, affecting sleep |
| Function | Acceptable, manageable limitations | Significant loss of ADLs, profound stiffness |
| Radiographs | Early to moderate joint space narrowing, minimal osteophytes | Advanced joint space narrowing, subchondral sclerosis, large osteophytes, subluxation, cyst formation, bone loss |
| Response to Conservative Rx | Responsive to NSAIDs, PT, injections | Failure of 3-6 months of structured non-operative care |
| Rotator Cuff | Intact, functional | Intact & functional (aTSA); Irreparable deficiency (RTSA) |
| Patient Age | Generally younger, or older with less severe symptoms | Generally >55-60 years for aTSA, indications broader for RTSA |
| Comorbidities | High surgical risk, multiple uncontrolled medical issues | Optimized for surgery, manageable medical comorbidities |
| Goals | Symptom control, maintain function | Pain relief, restore motion & function, improve QoL |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical to optimizing outcomes and minimizing complications in TSA.
Pre-Operative Planning
- Clinical Assessment: Detailed history (pain, duration, aggravating/alleviating factors, functional limitations, previous treatments, patient expectations). Physical examination (range of motion, strength testing, neurovascular status, rotator cuff integrity, deltoid function).
-
Imaging Studies:
- Standard Radiographs: AP (true glenoid view), axillary, and scapular Y views are essential to assess joint space, osteophytes, glenoid version/inclination, humeral head sphericity, and superior migration.
- Computed Tomography (CT) Scan: With 3D reconstruction, this is paramount for detailed assessment of glenoid bone loss, retroversion, and erosion patterns (e.g., Walch classification for GHOA, particularly B2/B3 glenoids often require RTSA or augmented glenoid components). It is also vital for templating glenoid component size, position, and assessing humeral canal morphology.
- Magnetic Resonance Imaging (MRI): While not routinely required for primary GHOA, it can be useful if rotator cuff integrity is questionable (e.g., suspected associated tears) or to rule out other pathologies.
-
[Example of pre-operative imaging demonstrating severe glenohumeral osteoarthritis with joint space narrowing and osteophyte formation.]
-
Templating:
- Humeral Component: Size, stem length, fit (cemented vs. press-fit), head diameter, offset, and retroversion. Aim for restoration of native anatomy.
- Glenoid Component: Size, peg/keel design, version, and inclination. For RTSA, glenosphere size, lateralization, and inferior overhang. Patient-specific instrumentation (PSI) or 3D printed guides are increasingly used for complex glenoid deformities to optimize component placement and minimize bone removal.
- Patient Optimization: Medical clearance, cessation of smoking, optimization of nutritional status, and control of co-morbidities (e.g., diabetes). Discussion of potential risks and benefits, expected outcomes, and alternative treatments. Antibiotic prophylaxis, usually a first or second-generation cephalosporin, administered within 60 minutes of incision.
Patient Positioning
The
beach chair position
is the most common and preferred position for TSA.
*
Setup:
Patient is semi-recumbent, torso elevated approximately 60-70 degrees from horizontal. The head is secured in a well-padded headrest, ensuring the neck is neutral and avoiding excessive rotation or lateral flexion to prevent brachial plexus neuropraxia.
*
Padding:
All pressure points (heels, sacrum, elbows) are meticulously padded.
*
Arm Preparation:
The operative arm is prepped and draped freely to allow full manipulation and assessment of range of motion during the procedure. A sterile stockinette covers the hand and forearm.
*
Traction:
A traction tower may be used to apply gentle, intermittent traction, aiding in joint distraction and exposure, particularly for RTSA.
*
Fluoroscopy:
The C-arm image intensifier is positioned to allow AP and axillary views of the shoulder, critical for accurate guide pin placement and component positioning, especially for the glenoid.
Detailed Surgical Approach / Technique
The deltopectoral approach is the workhorse for both aTSA and RTSA, offering excellent exposure while preserving deltoid function and the axillary nerve.
Deltopectoral Approach
- Incision: A curvilinear incision is made from the posterior aspect of the acromion, extending inferiorly and medially towards the coracoid process, then gently curving down the deltopectoral groove for approximately 10-15 cm.
- Deltopectoral Interval Dissection: The interval between the deltoid (lateral) and pectoralis major (medial) is identified. The cephalic vein typically lies within this interval and is carefully mobilized and retracted medially with the pectoralis major. The underlying clavipectoral fascia is incised longitudinally.
- Coracoid & Conjoined Tendon: The coracoid process and its attached conjoined tendon (coracobrachialis and short head of biceps) are identified and serve as a medial reference.
-
Subscapularis Management:
The anterior capsule is exposed. The subscapularis tendon, a critical anterior stabilizer, must be addressed.
- Subscapularis Tenotomy: The tendon is sharply released from its insertion on the lesser tuberosity. This is the most common method, requiring meticulous repair at the end of the case.
- Lesser Tuberosity Osteotomy: A small wafer of bone with the subscapularis insertion is osteotomized. This offers a larger bony footprint for repair, potentially stronger, but may increase risks of non-union or avulsion. This is often preferred in revision cases or when significant soft tissue balance is required.
- Note: In RTSA, the subscapularis is not repaired to allow for the medialized COR and altered biomechanics, but full mobilization and release of the muscle are still required.
- Capsular Release: After subscapularis management, the anterior capsule is released from the glenoid rim. Inferior capsular release is performed cautiously to protect the axillary nerve. A blunt Hohmann retractor can be carefully placed inferiorly to tent the capsule and protect the nerve during release.
Humeral Preparation (for aTSA and RTSA)
- Humeral Head Dislocation: The arm is externally rotated and extended to dislocate the humeral head anteriorly.
-
Humeral Head Resection:
The humeral head is resected using an oscillating saw. The cut is typically made at the anatomical neck, approximately 8-10 mm above the superior aspect of the pectoralis major insertion. The amount of retroversion (typically 20-40 degrees relative to the epicondylar axis) and inclination (often 130-135 degrees) must be carefully controlled using a cutting guide or jig to match native anatomy or templated parameters.
-
[Intraoperative view showing humeral head resection in preparation for stem insertion.]
-
-
Humeral Canal Preparation:
Sequential reaming and broaching of the humeral canal are performed to prepare for the humeral stem.
- Stem Type: Can be cemented (standard, often for osteoporotic bone) or press-fit (often for good bone quality). Short stems and stemless implants are increasingly popular, aiming for bone preservation.
- Trial Reduction: Trial components are inserted on both the humeral and glenoid sides to assess stability, range of motion, and soft tissue tension.
Glenoid Preparation (for aTSA)
- Glenoid Exposure: The remaining soft tissues and labrum are carefully debrided from the glenoid rim. The glenoid is exposed using retractors, ensuring adequate visualization of the entire glenoid surface.
- Reaming: The glenoid surface is prepared by reaming, removing only enough bone to achieve a flat, concentric surface that matches the posterior tilt (version) and superior-inferior inclination (typically 0-10 degrees retroversion and 0-5 degrees superior tilt) dictated by the native glenoid or corrected according to preoperative planning. Over-reaming can lead to significant bone loss.
- Keel/Peg Preparation: Drilling holes or creating a keel slot for the glenoid component's fixation elements.
-
Glenoid Component Implantation:
The final glenoid component is cemented into place, ensuring optimal version and inclination. It's crucial to vent the glenoid bone to prevent cement pressurization and potential fat emboli.
-
[Intraoperative view showing glenoid reaming and preparation for component implantation during anatomic TSA.]
-
Glenoid Preparation (for RTSA)
- Glenoid Exposure: Similar to aTSA, but often requires more aggressive inferior capsular release and careful protection of the axillary nerve.
-
Baseplate Implantation:
The glenoid is reamed to accept a central post and peripheral screws for the glenoid baseplate. The baseplate is typically secured with locking screws. Careful attention is paid to central position and avoiding inferior overhang to prevent scapular notching.
- Augmented baseplates or bone grafting may be used to address severe glenoid bone loss or excessive retroversion.
- Glenosphere Attachment: The glenosphere (the convex component) is then attached to the baseplate. The size and lateralization of the glenosphere impact deltoid tension and impingement.
Final Humeral Component Implantation
- Cemented Stem: The humeral canal is cleaned and dried, cement is injected, and the definitive stem is inserted with the trial head.
- Press-Fit Stem: The definitive press-fit stem is impacted, and the trial head is placed.
- Final Components & Reduction: The definitive humeral head (for aTSA) or humeral cup (for RTSA) is placed onto the stem. The joint is then reduced.
Closure
- Subscapularis Repair (for aTSA): The subscapularis tendon is meticulously repaired to its insertion site on the lesser tuberosity using strong non-absorbable sutures (e.g., Krackow stitch). This is a critical step for stability and function.
- Deltopectoral Interval: The clavipectoral fascia is approximated, and the deltopectoral interval is closed if desired.
-
Layered Closure:
Subcutaneous tissues and skin are closed. A drain may be placed.
-
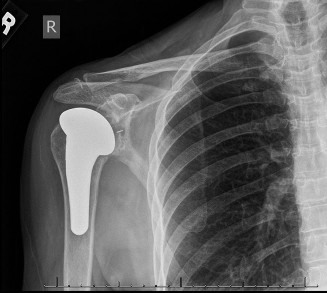[Post-operative radiograph demonstrating well-fixed total shoulder arthroplasty components.]
-
Complications & Management
Despite high success rates, TSA is associated with a range of potential complications, requiring thorough understanding for prevention and effective management.
Table 2: Common Complications of Total Shoulder Arthroplasty
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Infection | 0.5-2% | Debridement, antibiotics, implant retention (DAIR) if acute; two-stage revision arthroplasty if chronic; resection arthroplasty/fusion for intractable cases. |
| Instability/Dislocation | 1-5% (higher in RTSA) | Closed reduction, activity modification, bracing; open revision for recurrent instability (component malposition, soft tissue imbalance). |
| Glenoid Loosening (aTSA) | 5-15% (radiographic), 1-2% (symptomatic) | Glenoid revision (bone graft, augmented glenoid, RTSA conversion), conservative management if asymptomatic. |
| Humeral Loosening | <1% | Humeral component revision. |
| Periprosthetic Fracture | 0.5-3% | Non-operative (sling, activity restriction); ORIF with cable/plate fixation; revision arthroplasty (cemented stem, long stem) depending on fracture type and implant stability. |
| Axillary Nerve Injury | 0.5-2% (neuropraxia) | Observation, neurolysis if persistent deficit (rare). |
| Brachial Plexus Injury | <0.5% | Observation, supportive care, nerve grafting (rare). |
| Rotator Cuff Failure (aTSA) | 1-3% | Conservative management; revision to RTSA for symptomatic irreparable tears. |
| Stiffness/Arthrofibrosis | 5-10% | Intensive physical therapy, manipulation under anesthesia (MUA), arthroscopic capsular release (rare). |
| Scapular Notching (RTSA) | Up to 50% (radiographic), 5-10% (symptomatic) | Non-operative if asymptomatic; lateralization/distalization of COR, inferior overhang in primary surgery; revision with augmented glenoid, bone graft, or lateralizing implants if symptomatic. |
| Acromial/Scapular Spine Fracture (RTSA) | 1-10% (can be higher with lateralized COR) | Non-operative (sling, activity restriction); ORIF for displaced fractures (rare); may necessitate revision or failure. |
Management Principles:
*
Prevention:
Meticulous surgical technique, proper templating, appropriate component selection, meticulous soft tissue handling, and patient optimization.
*
Early Recognition:
Vigilant post-operative monitoring for signs of complications.
*
Tailored Treatment:
Management depends on the specific complication, its severity, timing, and patient factors. A multidisciplinary approach may be required.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as crucial as the surgery itself for optimizing outcomes after TSA. Protocols vary based on surgeon preference, implant type (aTSA vs. RTSA), soft tissue repair (e.g., subscapularis repair), and patient factors. The general principles involve protection, early controlled motion, and progressive strengthening.
Phase I: Protection & Early Controlled Motion (0-6 weeks)
- Immobilization: Arm is typically immobilized in a sling for 4-6 weeks. The sling may be removed for hygiene and specific exercises. For aTSA with subscapularis repair, external rotation is restricted (often to neutral or slight internal rotation) to protect the repair. For RTSA, internal rotation and combined adduction/internal rotation may be restricted to prevent dislocation.
- Goals: Protect surgical repair, minimize pain and swelling, prevent stiffness, begin passive range of motion.
-
Exercises (Daily):
- Passive Range of Motion (PROM): Pendulum exercises, supine passive flexion (up to 90-120 degrees depending on protocol), passive external rotation (restricted as per subscapularis repair), passive internal rotation (restricted as per RTSA protocol).
- Scapular Mobilization: Gentle scapular glides.
- Elbow, Wrist, Hand Exercises: To prevent stiffness and maintain circulation.
- Patient Education: Teach proper body mechanics, sling use, precautions, and signs of complications.
Phase II: Active-Assisted & Active Motion (6-12 weeks)
- Goals: Gradually increase active range of motion (AROM), improve muscular control, begin light strengthening.
-
Exercises:
- Active-Assisted Range of Motion (AAROM): With assistance from the contralateral arm or therapist, progress flexion, abduction, and rotation within pain-free limits.
- Active Range of Motion (AROM): Begin active elevation, abduction, and rotation, often starting in gravity-eliminated planes.
- Isometric Strengthening: Begin gentle isometric contractions for rotator cuff and deltoid, initiated gradually as per surgeon comfort. For RTSA, deltoid strengthening is emphasized.
- Scapular Stabilization: Progress scapular strengthening exercises.
Phase III: Progressive Strengthening & Advanced Function (12 weeks - 6 months)
- Goals: Restore full range of motion, maximize strength, improve endurance, return to light activities.
-
Exercises:
- Progressive Resistance Exercises: Gradual introduction of elastic bands, light weights for rotator cuff, deltoid, and scapular musculature. Focus on functional movement patterns.
- Proprioception and Neuromuscular Control: Exercises to improve joint position sense and stability.
- Endurance Training: Light cardiovascular exercises.
- Activity Progression: Gradual return to light daily activities, driving. Avoid overhead lifting, pushing, pulling heavy objects.
Phase IV: Return to Activity & Maintenance (6 months onwards)
- Goals: Maximize strength and endurance, return to recreational and occupational activities, maintain long-term shoulder health.
- Exercises: Continued strengthening, stretching, and functional training.
- Activity Restrictions (Long-term): Patients are generally advised to avoid repetitive heavy lifting, contact sports, and activities that involve high-impact or sudden jerking movements. For RTSA, weight-bearing or pushing/pulling limits may be advised to protect the glenoid fixation.
Regular follow-up with the surgeon and physical therapist is essential to monitor progress and adjust the rehabilitation program as needed.
Summary of Key Literature / Guidelines
The landscape of shoulder arthroplasty is continually evolving, with robust literature guiding clinical practice.
Anatomic Total Shoulder Arthroplasty (aTSA):
*
Outcomes:
Long-term studies consistently report excellent pain relief and functional improvement, with prosthesis survival rates exceeding 90% at 10 years and 80% at 15-20 years. Glenoid component loosening remains the most common mode of failure for aTSA, particularly with polyethylene pegged components.
*
Glenoid Bone Loss:
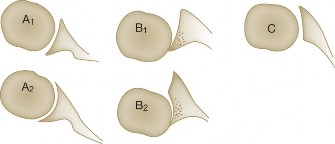
The Walch classification (A1, A2, B1, B2, B3, C) is widely used to categorize glenoid morphology and guide treatment. Walch B2 and B3 glenoids with significant retroversion and posterior bone loss pose challenges for aTSA, often requiring augmented glenoid components (e.g., posterior wedge) or conversion to RTSA to address glenoid wear. CT is crucial for pre-operative assessment.
*
Humeral Component:
Both cemented and uncemented humeral stems provide good results. Short stems and stemless designs are gaining traction, demonstrating comparable early-to-mid-term results with potential benefits in bone preservation and easier revision, though long-term data are still accumulating.
*
Subscapularis Repair:
A critical determinant of anterior stability and internal rotation strength. Meticulous repair is paramount.
Reverse Total Shoulder Arthroplasty (RTSA):
*
Outcomes:
RTSA has revolutionized the treatment of cuff tear arthropathy and complex proximal humerus fractures in older patients. It provides reliable pain relief and often better elevation and abduction than aTSA in cases of rotator cuff deficiency.
*
Indications Expansion:
While initially developed for CTA, indications have expanded to include severe GHOA with glenoid bone loss (e.g., Walch B2/B3 glenoids), revision shoulder arthroplasty, and certain fracture sequelae.
*
Complications Unique to RTSA:
Scapular notching, acromial stress fractures, and instability remain significant concerns. Surgical techniques aimed at lateralizing and/or distalizing the glenosphere (e.g., lateralizing glenosphere, augmented baseplates, bone grafting) have been developed to mitigate notching and improve range of motion.
*
Deltoid Function:
A functional deltoid is paramount for RTSA success.
General Guidelines and Trends:
*
Patient-Reported Outcome Measures (PROMs):
Scores such as the American Shoulder and Elbow Surgeons (ASES) score, Constant-Murley score, and Shoulder Pain and Disability Index (SPADI) are widely used to assess clinical outcomes.
*
Pre-operative Planning:
The increasing use of 3D CT templating and patient-specific instrumentation (PSI) is improving accuracy of component placement, especially for complex glenoid deformities.
*
Evidenced-Based Practice:
Current guidelines emphasize the importance of shared decision-making, patient education, and careful consideration of patient expectations.
*
Risk Mitigation:
Strategies such as anti-coagulation protocols, antibiotic prophylaxis, and peri-operative pain management are standardized to improve safety and patient experience.
*
Future Directions:
Continued advancements in implant design (e.g., improved glenoid fixation, modularity), robotic assistance, and biological solutions for cuff repair are areas of active research.
In conclusion, TSA, encompassing both anatomic and reverse designs, offers predictable and durable solutions for advanced glenohumeral osteoarthritis and related pathologies. Mastery of surgical technique, comprehensive pre-operative planning, appropriate patient selection, and rigorous post-operative rehabilitation are essential for optimal patient outcomes.
Clinical & Radiographic Imaging

You Might Also Like