Scaphoid Fractures: Advanced Clinical Guide to Anatomy, Biomechanics, & Management
Key Takeaway
Scaphoid fractures are problematic due to their unique anatomy and precarious retrograde blood supply, making them prone to nonunion and avascular necrosis (AVN). Their critical role in carpal biomechanics means delayed or inadequate treatment can lead to progressive wrist arthritis (SNAC wrist) and chronic dysfunction.
Introduction & Epidemiology
Scaphoid fractures represent the most common carpal bone fracture, accounting for approximately 70-80% of all carpal injuries and 10-15% of all hand fractures. These injuries predominantly affect young, active males, typically resulting from a fall onto an outstretched hand (FOOSH) with the wrist hyperextended and radially deviated. The unique anatomy and precarious blood supply of the scaphoid predispose it to delayed union, nonunion, and avascular necrosis (AVN), making accurate diagnosis and timely, appropriate management crucial for preventing long-term wrist dysfunction, pain, and degenerative arthritis.
Epidemiological studies indicate a peak incidence in individuals aged 20-30 years. While often subtle in presentation, the clinical sequelae of missed or inadequately treated scaphoid fractures can be severe, leading to significant morbidity. Fracture patterns are typically classified based on their anatomical location:
*
Waist fractures (70-80%):
Most common, often unstable.
*
Proximal pole fractures (15-20%):
Carry the highest risk of AVN due to retrograde blood supply.
*
Distal pole fractures (5-10%):
Generally have a better prognosis.
*
Tubercle fractures (rare):
Usually stable and heal well.
Radiographic assessment often involves standard posteroanterior (PA), lateral, and oblique views, in addition to a dedicated scaphoid view (PA with ulnar deviation). Due to the potential for occult fractures, a high index of suspicion is required, and advanced imaging modalities such as CT or MRI are often utilized for definitive diagnosis, particularly in cases with persistent clinical suspicion despite negative initial radiographs.
Surgical Anatomy & Biomechanics
Surgical Anatomy
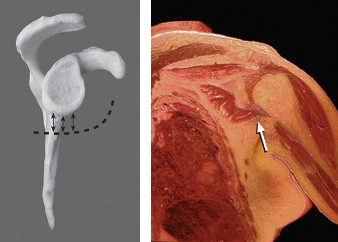
The scaphoid is a boat-shaped carpal bone located in the proximal carpal row, acting as a critical link between the proximal and distal carpal rows. It articulates with five bones: the radius proximally, the lunate medially, the trapezium and trapezoid distally, and the capitate proximodistally.
-
Gross Anatomy:
- Proximal Pole: Articulates with the radial scaphoid fossa and the lunate. Receives its blood supply primarily from distal branches.
- Waist: The narrowest and most commonly fractured part.
- Distal Pole: Articulates with the trapezium and trapezoid. Features the scaphoid tubercle, serving as an attachment point for the flexor retinaculum and abductor pollicis brevis muscle.
-
Ligamentous Attachments:
The scaphoid is extensively covered by cartilage (80%), with limited areas for soft tissue attachment. Key ligaments stabilizing the scaphoid within the carpus include:
- Scapholunate Interosseous Ligament (SLIL): Connects the scaphoid and lunate, crucial for carpal stability. Injury leads to scapholunate dissociation.
- Radioscaphocapitate Ligament (RSC): Arises from the radial styloid, courses volar to the scaphoid, and inserts onto the capitate.
- Scaphotrapezial Ligament: Connects the scaphoid to the trapezium.
- Dorsal Radioscapholunate Ligament (DRSL): Less robust, originates from the dorsal aspect of the radius and inserts on the dorsal scaphoid and lunate.
-
Vascularity:
The scaphoid's blood supply is highly vulnerable and is the primary reason for its high nonunion and AVN rates.
- Dorsal Carpal Artery Branch (Radial Artery): Supplies the majority (70-80%) of the scaphoid via intraosseous branches entering the dorsal ridge. These vessels provide a retrograde blood supply to the proximal pole.
- Palmar Superficial Branch (Radial Artery): Supplies the distal tubercle and a small portion of the distal pole (20-30%) via direct branches.
- Fractures through the scaphoid waist often compromise the retrograde blood supply to the proximal pole, especially if the fracture is displaced. The complete reliance of the proximal pole on this retrograde flow explains its heightened susceptibility to AVN.
Biomechanics
The scaphoid plays a critical role in carpal kinematics, functioning as an "intercalated segment" that bridges the proximal and distal carpal rows. It helps couple the motion of the radius and the distal carpal row (capitate, trapezium, trapezoid).
- Kinematic Chain: During wrist motion, the scaphoid flexes with radial deviation and extends with ulnar deviation, maintaining a precise relationship with the lunate and capitate.
- Force Transmission: The scaphoid is a primary load-bearing structure, transmitting axial loads from the radius to the distal carpal row, and subsequently to the metacarpals.
-
Stability:
Proper scaphoid length and alignment are essential for maintaining carpal stability. Disruption of scaphoid integrity or significant shortening / humpback deformity can lead to:
- DISI (Dorsal Intercalated Segment Instability): Often seen with scaphoid nonunion or malunion, characterized by dorsal tilt of the lunate due to loss of the scaphoid's palmar flexion influence.
- SNAC (Scaphoid Nonunion Advanced Collapse) Wrist: A progressive pattern of degenerative arthritis resulting from chronic scaphoid nonunion. It typically begins at the radial styloid-scaphoid articulation, progresses to the capitolunate joint, and spares the radiolunate joint until late stages. The mechanism involves altered carpal mechanics, increased localized loading, and eventual cartilage degeneration.
Understanding these anatomical and biomechanical principles is paramount for both diagnosis and effective surgical planning, aiming to restore not only bone integrity but also the intricate carpal kinematics.
Indications & Contraindications
The decision for operative versus non-operative management of scaphoid fractures is multifactorial, considering fracture characteristics, patient factors, and potential for complications. The primary goal of treatment is to achieve timely union and restore anatomical alignment to prevent long-term sequelae such as nonunion, AVN, and post-traumatic arthritis.
Indications for Operative Management
Surgical intervention is generally indicated for fractures with a high risk of nonunion, significant displacement, or those where early return to function is desired.
- Displaced Fractures: Displacement > 1 mm on any radiographic view, or translation.
- Angulated Fractures: Humpback deformity > 10-15 degrees (scaphoid sagittal angle > 60 degrees, or radioscaphoid angle > 45 degrees on lateral radiographs). This often indicates an unstable fracture pattern and can lead to malunion and altered carpal kinematics.
-
Unstable Fracture Patterns:
- Proximal Pole Fractures: Due to precarious blood supply and high risk of AVN/nonunion.
- Vertical Oblique Fractures: Considered mechanically unstable due to shear forces across the fracture line.
- Comminuted Fractures: Often require internal fixation and potentially bone grafting.
- Scapholunate Angle > 60 degrees or Radiolunate Angle > 15 degrees: Indicative of carpal instability.
- Nonunion or Suspected Nonunion: Established nonunion or delayed union beyond acceptable conservative treatment periods.
- Fracture-Dislocations: Perilunate dislocations involving scaphoid fracture.
- Delayed Presentation: Fractures diagnosed > 3 weeks after injury, especially if displaced or unstable.
- High-Demand Patients: Athletes, manual laborers, or individuals for whom prolonged immobilization is unacceptable due to professional or personal demands. Surgical fixation may allow for earlier mobilization and return to activity.
- Failed Non-Operative Treatment: Persistence of nonunion after an adequate trial of casting/immobilization.
Indications for Non-Operative Management
Conservative management is typically reserved for stable, non-displaced fractures with a high likelihood of union.
-
Non-Displaced, Stable Fractures:
- Distal Tubercle Fractures: Generally heal reliably with short-term immobilization.
- Non-Displaced Distal Pole Fractures: High union rates.
- Non-Displaced Scaphoid Waist Fractures: With no evidence of instability on stress views or dynamic imaging, and reliable patient compliance. Immobilization in a long arm or short arm thumb spica cast is common.
- Patient Preference: When surgery is not desired, and the fracture pattern is amenable to conservative management, with appropriate counseling regarding potential risks (e.g., prolonged immobilization, nonunion).
- Medical Comorbidities: Patients with significant medical contraindications to surgery.
Contraindications for Operative Management
While rare, certain patient and fracture characteristics may contraindicate immediate surgical intervention.
- Active Local or Systemic Infection: Relative contraindication, should be controlled prior to surgery.
- Severe Comorbidities: Patients with unstable medical conditions that significantly increase surgical risk (e.g., uncontrolled cardiac disease, severe coagulopathy).
- Severe Soft Tissue Injury: Open fractures with extensive soft tissue damage may require initial debridement and delayed fixation.
- Non-Compliant Patient: A patient unwilling or unable to adhere to post-operative rehabilitation protocols may have poorer outcomes.
- Irreparable Bone Loss/Severe Comminution: In extreme cases, if the bone is too fragmented to reconstruct, alternative salvage procedures may be considered instead of internal fixation.
Operative vs. Non-Operative Indications
| Feature / Fracture Type | Operative Indications | Non-Operative Indications |
|---|---|---|
| Displacement | > 1 mm translation or gapping | None |
| Angulation | Humpback deformity > 10-15 degrees (scaphoid sagittal angle > 60°) | None |
| Fracture Location | Proximal pole, Vertical oblique waist, Comminuted waist | Distal tubercle, Non-displaced distal pole |
| Unstable waist fractures (e.g., associated with SL instability) | Non-displaced, stable waist fractures (e.g., Herbert B1) | |
| Delayed Presentation | Diagnosis > 3 weeks post-injury, especially if displaced | Acute, non-displaced, stable (diagnosed within 3 weeks) |
| Associated Injuries | Carpal instability (e.g., SL dissociation), fracture-dislocations | Isolated scaphoid fracture |
| Patient Factors | High-demand patient (athlete, manual laborer) desiring early return to activity | Patient with comorbidities precluding surgery, compliant patient willing for prolonged immobilization |
| Previous Treatment | Failed conservative treatment (nonunion or delayed union) | First-line for stable, non-displaced fractures |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential for optimizing surgical outcomes, minimizing complications, and ensuring efficient execution of the procedure.
Pre-Operative Planning
-
Clinical Assessment:
- Detailed history focusing on injury mechanism, time of injury, prior wrist injuries, and hand dominance.
- Physical examination: Tenderness in the anatomical snuffbox, scaphoid tubercle, pain with axial loading of the thumb, and pain with resisted pronation.
- Assessment of neurovascular status and skin integrity.
-
Imaging Review:
- Plain Radiographs: Standard PA, lateral, oblique, and scaphoid views (PA with ulnar deviation and slight extension) are initial steps. Assess for displacement, angulation, length loss, and carpal alignment (scapholunate angle, radioscaphoid angle).
- Computed Tomography (CT) Scan: The gold standard for assessing fracture displacement, comminution, and fragment orientation, especially in waist and proximal pole fractures. Axial, coronal, and sagittal reconstructions are critical for 3D understanding. It aids in surgical approach selection and screw trajectory planning.
- Magnetic Resonance Imaging (MRI): Useful for diagnosing occult scaphoid fractures not visible on radiographs or CT. It can also detect bone contusion, ligamentous injuries (e.g., SLIL), and assess vascularity (though less reliable for early AVN than clinical progression).
- Bone Scan: Rarely used for acute fractures but can confirm occult fractures by showing increased uptake.
-
Surgical Approach Selection:
Based on fracture location, displacement, and surgeon preference.
- Volar Approach (Henry Approach): Preferred for distal pole and waist fractures, particularly for visualizing humpback deformity and facilitating distal-to-proximal screw insertion. Allows direct visualization of the palmar aspect of the scaphoid.
- Dorsal Approach: Preferred for proximal pole and waist fractures, allowing proximal-to-distal screw insertion, which is often biomechanically advantageous given the retrograde blood supply. Also suitable for bone grafting procedures.
- Percutaneous Fixation: For non-displaced or minimally displaced fractures, often guided by fluoroscopy. Can be performed volarly or dorsally.
-
Hardware Selection & Templating:
- Cannulated Headless Compression Screws: Standard for scaphoid fixation (e.g., Herbert, Acutrak, Twinfix, BaroTraK). Principles include maximal compression and stability across the fracture site.
- Screw Length and Diameter: Determined by templating on CT images. The screw should ideally span 70-80% of the scaphoid length and be centrally placed within the long axis of the bone.
- Bone Grafting: Plan for vascularized or non-vascularized bone grafting if there is significant bone loss, comminution, established nonunion, or suspicion of AVN. Common sources include distal radius (non-vascularized), 2,3-intercompartmental supraretinacular artery (2,3 ICSRA) pedicled graft, or medial femoral condyle (MFC) free vascularized graft.
- Informed Consent: Discuss surgical risks including nonunion, AVN, infection, nerve injury, hardware prominence, malunion, and need for further surgery.
Patient Positioning
- General Anesthesia: Regional nerve block (e.g., supraclavicular or axillary block) can be performed pre-operatively for post-operative pain control, in conjunction with general anesthesia.
- Supine Position: Patient is positioned supine on the operating table.
-
Arm Positioning:
- The affected arm is placed on a radiolucent hand table, allowing for easy access and unobstructed fluoroscopy.
- A tourniquet is applied to the upper arm (typically inflated to 250 mmHg or 100 mmHg above systolic blood pressure).
- Sterile Preparation and Draping: The arm is prepped and draped from the elbow to the fingertips to allow full wrist and digit manipulation.
-
Fluoroscopy Setup:
The C-arm fluoroscope should be positioned for easy access to obtain true lateral, PA, and scaphoid views without repositioning the patient or the arm.
- Crucial for confirming reduction and guiding K-wire/screw placement.
- Lateral view: Superimposition of the pisiform over the distal pole of the scaphoid.
- PA view: Superimposition of the distal radius and ulna.
- Scaphoid view: Slight wrist extension and ulnar deviation.
- Hand Position: For volar approaches, the forearm is typically supinated. For dorsal approaches, the forearm is pronated.
Detailed Surgical Approach / Technique
The goal of scaphoid fracture fixation is anatomical reduction and rigid internal fixation, promoting primary bone healing and minimizing the risks of nonunion and AVN. Cannulated headless compression screws are the standard fixation device.
General Principles of Fixation
- Anatomic Reduction: Crucial for restoring carpal kinematics and preventing malunion.
- Central Screw Placement: The screw should ideally be placed in the geometric center of the scaphoid in all planes to maximize compression and prevent eccentric load bearing, which can lead to fatigue failure.
- Adequate Screw Length: The screw should engage both the proximal and distal fragments, crossing the fracture site perpendicular to the fracture plane if possible, to achieve maximal compression. It should occupy at least 70-80% of the scaphoid length but remain entirely intraosseous.
- Avoid Prominence: The screw head should be countersunk beneath the bone surface to prevent impingement on articular cartilage or soft tissues.
Volar (Henry) Approach
This approach is preferred for distal pole and waist fractures, particularly those with a volar angulation (humpback deformity) or where direct visualization of the volar aspect of the scaphoid is required.
- Incision: A curvilinear incision approximately 4-6 cm long is made along the radial border of the flexor carpi radialis (FCR) tendon, centered over the distal wrist crease. The incision may extend proximally across the crease and distally into the thenar eminence.
-
Deep Dissection:
- The subcutaneous tissue is carefully incised. The radial sensory nerve branches and the palmar cutaneous branch of the median nerve should be identified and protected.
- The FCR tendon sheath is opened longitudinally along its radial border. The FCR tendon is retracted ulnarly.
- Deep to the FCR, the radial artery is identified. It runs between the FCR and the flexor pollicis longus (FPL). The radial artery is carefully retracted radially, often with the FPL. Alternatively, the FPL can be retracted radially. The important interval is between the FCR and the FPL/Radial Artery.
- The radioscaphocapitate ligament (RSC) and the volar wrist capsule are now visible.
- Capsulotomy: A longitudinal or L-shaped capsulotomy is performed directly over the volar aspect of the scaphoid. Care is taken to avoid excessive stripping of the soft tissues supplying the scaphoid.
-
Fracture Exposure & Reduction:
- The fracture site is identified. Traction on the thumb and wrist extension can facilitate exposure and reduction.
- Direct Reduction: Using small periosteal elevators, dental picks, or K-wires as joysticks, the fracture fragments are anatomically reduced. Fluoroscopy is used to confirm reduction in PA, lateral, and scaphoid views.
- Correction of Humpback Deformity: If a humpback deformity is present, a small bone graft (wedge or structural) may be required volarly to restore scaphoid length and alignment, especially in established nonunions.
-
K-wire Placement:
- A 0.045" or 0.062" K-wire is inserted from the distal pole into the proximal fragment, aiming for the center of the scaphoid. The trajectory should be perpendicular to the fracture plane.
- Fluoroscopy is essential to confirm appropriate K-wire position (central in both PA and lateral views, crossing the fracture without distraction). A second K-wire may be placed for anti-rotation if necessary.
-
Screw Insertion:
- The K-wire is overdrilled with the appropriate cannulated drill bit according to the screw system.
- Depth measurement is performed.
- A headless compression screw is inserted over the K-wire. The goal is to bury the screw head just beneath the cortical surface to prevent articular impingement.
- The K-wire is removed.
-
Closure:
- The capsule is closed, if possible, but often left open to prevent overtightening.
- The FCR tendon sheath is closed.
- Subcutaneous tissues and skin are closed in layers.
Dorsal Approach
This approach is preferred for proximal pole fractures, waist fractures that are dorsally displaced, or for proximal-to-distal screw insertion, which is biomechanically advantageous as it often allows better purchase in the vascularized distal fragment.
- Incision: A 4-6 cm longitudinal incision is made along the radial aspect of the dorsal wrist, typically just ulnar to Lister's tubercle.
-
Deep Dissection:
- The subcutaneous tissue is incised. The radial sensory nerve branches should be identified and protected.
- The extensor retinaculum is identified. The interval between the third dorsal compartment (extensor pollicis longus, EPL) and the second dorsal compartment (extensor carpi radialis longus and brevis, ECRL/ECRB) is developed. Lister's tubercle is a key landmark.
- The EPL tendon is retracted ulnarly, exposing the floor of the fourth compartment (extensor digitorum communis and extensor indicis proprius). The second compartment tendons (ECRL/ECRB) are retracted radially.
- The dorsal wrist capsule is exposed.
- Capsulotomy: An L-shaped or longitudinal capsulotomy is performed, often through the dorsal radioscapholunate ligament (DRSL) and dorsal intercarpal ligament. Care must be taken to minimize capsular stripping of the dorsal scaphoid, as it carries critical vascular supply.
-
Fracture Exposure & Reduction:
- The fracture site, particularly the proximal pole, is identified.
- Reduction is achieved using gentle traction, manipulation with K-wires, or small elevators. Fluoroscopy confirms anatomical alignment.
- For established nonunions, a dorsal wedge osteotomy or bone grafting may be necessary to restore scaphoid length and correct carpal collapse.
-
K-wire Placement:
- A K-wire is inserted from the proximal pole (dorsal aspect) distally, aiming for the central axis of the scaphoid.
- Careful trajectory is needed to ensure the K-wire does not penetrate the articular surfaces and is central in PA and lateral views.
- A second K-wire can be used as a joystick for reduction or as an anti-rotational wire.
-
Screw Insertion:
- The K-wire is overdrilled, depth measured.
- A headless compression screw is inserted over the K-wire, ensuring the screw head is countersunk.
- The K-wire is removed.
-
Closure:
- Capsule closure (if feasible without tension).
- Extensor retinaculum repair.
- Subcutaneous tissues and skin are closed in layers.
Percutaneous Fixation
This minimally invasive technique is suitable for non-displaced or minimally displaced scaphoid waist fractures, offering potentially faster recovery and reduced soft tissue dissection.
- Preparation: Patient positioning and draping as described above. Accurate fluoroscopic views (PA, lateral, scaphoid view) are paramount.
-
Entry Point:
- Volar Percutaneous: A small incision (1-2 cm) is made on the volar aspect of the wrist, aiming at the scaphoid tubercle. The FCR tendon and radial artery are identified and protected. The K-wire is inserted from the distal pole.
- Dorsal Percutaneous: A small incision is made just ulnar to Lister's tubercle. The K-wire is inserted from the proximal pole.
-
K-wire Insertion:
- Under continuous fluoroscopic guidance, a K-wire is carefully advanced across the fracture site. Multiple attempts may be needed to achieve optimal central placement.
- The wire should be centered in the scaphoid in both PA and lateral views, parallel to the long axis of the scaphoid, and engage both fragments without distraction.
- Screw Insertion: The technique proceeds as with open fixation: overdrilling, depth measurement, and headless compression screw insertion over the K-wire.
- Closure: The small skin incision is closed.
Regardless of the approach, intraoperative fluoroscopy is used throughout the procedure to confirm reduction, K-wire placement, screw length, and final screw position in multiple planes. Post-fixation, a final set of high-quality fluoroscopic images or intraoperative radiographs should be obtained.
Complications & Management
Despite meticulous surgical technique, scaphoid fracture fixation is associated with a range of potential complications, which can significantly impact patient outcomes. Vigilant post-operative monitoring and a well-defined management strategy are crucial.
Common Complications
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Nonunion | 5-15% (acute fixation), Up to 50%+ (non-displaced treated conservatively), 80-90%+ (established nonunion) | Revision internal fixation, non-vascularized bone grafting (e.g., iliac crest, distal radius), vascularized bone grafting (e.g., 2,3-ICSRA, MFC free flap) for AVN or challenging nonunions. For SNAC wrist: Scaphoidectomy and four-corner arthrodesis (4CA), proximal row carpectomy (PRC). Partial or total wrist arthrodesis in advanced cases. |
| Avascular Necrosis (AVN) | 10-30% (proximal pole), Lower in waist fractures | For early AVN without collapse: Vascularized bone graft (e.g., 2,3-ICSRA, MFC free flap) with fixation. For established collapse/degeneration: Proximal row carpectomy (PRC), scaphoidectomy and 4CA, total wrist arthrodesis. |
| Malunion | 5-10% | Corrective osteotomy and bone grafting (e.g., volar wedge graft) to restore scaphoid length and carpal alignment. For established SNAC changes: PRC, scaphoidectomy and 4CA, total wrist arthrodesis. |
| Hardware Complications | 2-5% | Screw prominence: Removal of symptomatic screw. Screw breakage: Removal of symptomatic fragments, revision fixation if fracture still ununited. Loosening/Migration: Revision fixation. Usually requires removal and revision surgery with longer/larger screw or bone grafting. |
| Infection | <1-2% | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics, hardware removal if infection persists or bone involvement. May require delayed reconstruction. |
| Nerve Injury | <1% | Radial Sensory Nerve: Most common. Neuropraxia often resolves. Neuroma (rare) may require excision and nerve capping. Palmar Cutaneous Branch of Median Nerve: Less common, usually resolves. Motor Nerves: Extremely rare (e.g., median nerve, radial nerve motor branches) due to direct trauma or traction, may require neurolysis. |
| Wrist Stiffness | 5-15% | Intensive hand therapy, stretching, mobilization exercises. For recalcitrant stiffness: Capsulotomy, tenolysis. Rarely requires surgical intervention if no underlying bony pathology. |
| Post-traumatic Arthritis (SNAC Wrist) | Progressive with nonunion/malunion | Prevention is key via anatomical reduction and stable fixation. For established arthritis: Scaphoidectomy and four-corner arthrodesis (4CA), proximal row carpectomy (PRC), total wrist arthrodesis. Partial fusions are considered for localized arthritis. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Early diagnosis and multi-modal treatment: physical therapy, pain management (gabapentin, tricyclic antidepressants), regional blocks, psychological support. Referral to pain specialist. |
| Secondary Displacement | 2-5% | Re-reduction and revision fixation. May require additional bone grafting or a different fixation strategy. |
Management Principles
- Early Recognition: Many complications can be mitigated by early identification through regular clinical and radiographic follow-up.
-
Nonunion:
- Diagnosis: Persistent pain, tenderness, and lack of radiographic healing (sclerosis, cystic changes, persistent fracture line) after 3-4 months post-operatively. CT scan is essential for confirmation and detailed assessment of bone loss/fragment viability.
-
Management:
- Without AVN/Collapse: Revision internal fixation, often with non-vascularized bone grafting (e.g., distal radius, iliac crest).
- With AVN of Proximal Pole: Vascularized bone grafting (e.g., 2,3-ICSRA pedicled graft, free MFC flap) is often preferred to enhance revascularization.
- With Carpal Collapse (SNAC Wrist): Salvage procedures such as scaphoidectomy and four-corner arthrodesis (4CA), or proximal row carpectomy (PRC) are considered depending on the extent of arthritis. Total wrist arthrodesis for end-stage pan-carpal arthritis.
-
Avascular Necrosis:
- Diagnosis: Radiographic findings include increased density (sclerosis) of the proximal pole, fragmentation, and collapse. MRI can show absence of marrow edema signal on T2, but is less reliable for definitive diagnosis.
- Management: Varies based on stage. Early: vascularized bone grafting. Late (collapse/arthritis): salvage procedures (PRC, 4CA, arthrodesis).
-
Malunion:
- Diagnosis: Persistent humpback deformity, loss of scaphoid length, or altered carpal angles on lateral radiographs. CT is key.
- Management: Corrective osteotomy and bone grafting for symptomatic malunion without significant arthritis. If arthritis is present, management parallels SNAC wrist.
- Hardware Issues: Symptomatic hardware requires removal. If the fracture is ununited, revision fixation is required. Asymptomatic buried hardware is usually left in situ.
- Infection: Prompt treatment with antibiotics and surgical debridement is crucial. Deep infections involving bone or hardware may necessitate hardware removal and potentially a staged reconstruction.
- Neurovascular Injuries: Most nerve injuries are neuropraxias and resolve spontaneously. Persistent or severe symptoms may warrant nerve exploration and neurolysis.
Successful management of scaphoid fracture complications requires a comprehensive understanding of carpal anatomy, biomechanics, and a range of surgical techniques, often with a multidisciplinary approach involving hand therapists and pain specialists.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional recovery and minimizing stiffness while ensuring fracture healing. Protocols vary based on the stability of fixation, fracture type, and surgeon preference. The general principle is to balance adequate protection for bone healing with early, controlled motion to prevent stiffness.
Phase 1: Immobilization & Protection (Weeks 0-6/8)
Goal: Protect fixation, promote bone healing, manage pain and swelling.
-
Immobilization:
-
Stable Fixation (non-displaced/minimally displaced, single screw):
- Short arm thumb spica splint or cast for 4-6 weeks. Some surgeons may opt for a removable splint with immediate gentle range of motion (ROM) if fixation is exceptionally rigid and patient compliance is high.
- For percutaneous fixation, a removable splint or short arm thumb spica cast is common for 4-6 weeks.
-
Less Stable Fixation (comminution, bone graft, revision surgery):
- Long arm thumb spica cast for the initial 2-4 weeks, then conversion to a short arm thumb spica cast for an additional 4-6 weeks.
- Duration: Immobilization typically continues until initial radiographic signs of healing are evident, usually 6-8 weeks for acute fractures and longer (10-12+ weeks) for nonunions or grafts.
-
Stable Fixation (non-displaced/minimally displaced, single screw):
-
Early Mobilization (Non-Immobilized Joints):
- Fingers and Elbow: Encourage full active and passive ROM of all non-immobilized joints (shoulder, elbow, fingers, metacarpophalangeal joints) several times daily to prevent stiffness and reduce swelling.
- Thumb IP Joint: If the thumb IP joint is immobilized, ensure gentle passive ROM can be performed if splint allows or during splint changes.
-
Pain & Swelling Management:
- Elevation of the hand above the heart.
- Ice application (carefully, especially with cast).
- Prescribed analgesics.
- Weight-Bearing: No weight-bearing through the wrist.
- Activity: Avoid any gripping, lifting, or twisting activities. No driving if in a cast.
Phase 2: Controlled Active Range of Motion (Weeks 6/8-12)
Goal: Restore pain-free active wrist motion, prevent stiffness, maintain fracture protection.
- Imaging: Repeat radiographs (and potentially CT scan) at 6-8 weeks to confirm signs of fracture healing. If healing is sufficient, progress to active ROM.
- Immobilization: Discontinue full-time cast immobilization. A removable wrist splint (short arm thumb spica) may be worn for support during activity or sleep for another 2-4 weeks, or as needed for comfort.
-
Active Range of Motion (AROM):
- Begin gentle, pain-free active wrist flexion, extension, radial and ulnar deviation.
- Continue full AROM for fingers, thumb, and elbow.
- Gentle forearm pronation/supination.
- Passive Range of Motion (PROM): Initiate gentle, pain-free passive wrist ROM as tolerated, if AROM is limited.
- Soft Tissue Mobilization: Scar massage, desensitization of incision site.
- Activity: Light daily activities. Avoid heavy lifting, pushing, pulling, or gripping.
Phase 3: Strengthening & Advanced Mobility (Weeks 12+)
Goal: Improve wrist strength, endurance, and prepare for return to full activity.
- Imaging: Further radiographs/CT scan may be performed at 12-16 weeks to confirm complete union.
-
Strengthening:
- Begin with isometric exercises for wrist flexors, extensors, radial and ulnar deviators.
- Progress to isotonic exercises with light resistance bands, putty, or small weights.
- Gradually increase resistance and repetitions.
- Forearm strengthening (pronation/supination).
- Grip strengthening exercises.
-
Proprioception and Coordination:
- Exercises using wobble boards or dynamic activities to improve wrist stability and coordination.
-
Activity:
- Gradual return to heavier lifting and functional activities.
- Sport-specific or work-specific activities are introduced gradually.
-
Return to Play/Work:
- Typically not before 4-6 months, and only after complete radiographic union is confirmed, full pain-free ROM is achieved, and adequate strength is regained.
- Contact sports or activities involving heavy impact may require longer recovery.
Important Considerations:
- Patient Compliance: Essential for adherence to protocols and avoiding premature stress on the healing fracture.
- Pain as a Guide: Activities should remain pain-free. Any increase in pain warrants reconsideration of activity level.
- Individualized Protocol: Protocols should be tailored to the individual patient, considering fracture stability, healing progress, and functional demands.
- Complication Monitoring: Ongoing vigilance for signs of nonunion, AVN, or other complications.
- Physician and Therapist Communication: Close collaboration between the surgeon and hand therapist is paramount for effective rehabilitation progression.
For nonunions treated with bone grafting, particularly vascularized grafts, the immobilization period may be extended, and the progression through rehabilitation phases may be slower to ensure robust graft incorporation and healing.
Summary of Key Literature / Guidelines
The management of scaphoid fractures has evolved considerably over decades, with a substantial body of literature informing current best practices. Key areas of ongoing research and consensus development include optimal imaging for diagnosis, indications for surgery, choice of surgical approach and fixation, and management of complications.
Diagnostic Algorithms
-
Initial Presentation:
For suspected scaphoid fractures with negative initial radiographs, the literature supports various approaches:
- Immobilization and Repeat Radiographs: A common strategy involves immobilizing the wrist in a thumb spica splint for 7-10 days, followed by repeat scaphoid views. This approach detects fractures that become apparent with early bone resorption.
- Advanced Imaging: Increasingly, CT or MRI is recommended for acute presentations with high clinical suspicion despite negative radiographs. MRI is highly sensitive for occult fractures and bone contusions, while CT offers superior detail for fracture geometry, displacement, and comminution, which is critical for surgical planning.
- Meta-analyses have demonstrated the superior diagnostic accuracy of MRI over plain radiographs and bone scans for occult scaphoid fractures.
Operative vs. Non-Operative Treatment
- Non-displaced Waist Fractures: While traditionally managed non-operatively with prolonged casting (10-12 weeks), recent literature, including randomized controlled trials (RCTs) and systematic reviews , suggests that surgical fixation with a headless compression screw can lead to earlier return to work/sport and potentially lower rates of nonunion in some patient groups. The Cochrane Review on interventions for treating scaphoid fractures highlights that surgery may lead to faster union and earlier return to function, but with potential for surgical complications.
- Displaced Fractures (any location): There is broad consensus in the literature that displaced scaphoid fractures (>1mm displacement or >10-15° angulation) benefit from surgical fixation to achieve anatomical reduction, stable internal fixation, and minimize the risk of nonunion and subsequent degenerative arthritis (SNAC wrist).
- Proximal Pole Fractures: Due to their high risk of AVN and nonunion, even minimally displaced proximal pole fractures are often managed operatively. Studies by Hage et al. and others emphasize the challenging nature of these fractures.
Surgical Techniques
-
Approach:
- Volar vs. Dorsal: The choice of approach is dictated by fracture location, displacement, and surgeon preference. Haddad et al. and other studies discuss the advantages and disadvantages of each. Volar approach is generally favored for distal and waist fractures with volar angulation, while dorsal approach is better for proximal pole fractures or to facilitate proximal-to-distal screw placement.
- Percutaneous vs. Open: Percutaneous fixation is a viable option for non-displaced or minimally displaced waist fractures, offering potentially smaller incisions, less soft tissue disruption, and faster recovery. However, it requires significant fluoroscopic expertise and carries a risk of inadequate reduction or eccentric screw placement if not performed meticulously. Bond et al. demonstrated good results with percutaneous fixation.
- Fixation: Cannulated headless compression screws are the gold standard. Optimal screw placement (central, perpendicular to fracture line, subchondral) is emphasized in numerous biomechanical and clinical studies.
Management of Nonunion and AVN
-
Nonunion:
The management strategy for scaphoid nonunion is complex and depends on factors such as fracture location, stability, presence of AVN, carpal collapse, and arthritic changes.
- Bone Grafting: Non-vascularized bone grafting (e.g., autogenous iliac crest or distal radius) with screw fixation is effective for stable nonunions without significant AVN or bone loss.
- Vascularized Bone Grafts: For cases with established AVN of the proximal pole or recalcitrant nonunions, vascularized bone grafts (e.g., 2,3-ICSRA pedicled graft, free medial femoral condyle flap) have shown superior union rates by providing a direct blood supply. Key proponents include Zaidemberg et al. (2,3-ICSRA) and Mathoulin et al. (MFC).
- SNAC Wrist: For advanced stages of post-traumatic arthritis secondary to scaphoid nonunion, salvage procedures such as scaphoidectomy and four-corner arthrodesis (4CA) or proximal row carpectomy (PRC) are well-established. Watson et al. originally described the concept of SNAC wrist and the role of 4CA.
Rehabilitation
- The trend in rehabilitation is towards earlier, controlled motion, especially after stable surgical fixation. However, the duration of immobilization and the rate of progression remain controversial and depend on evidence of healing. Most protocols emphasize protection until radiographic union is confirmed, followed by progressive ROM and strengthening.
Key Guidelines and Consensus Statements
- American Academy of Orthopaedic Surgeons (AAOS): While there isn't a specific comprehensive guideline solely on scaphoid fractures from AAOS, their general guidelines on acute fracture management and hand/wrist injuries indirectly apply.
- International Consensus: Expert panels and specialized hand societies (e.g., European Wrist Arthroscopy Society - EWAS) often publish consensus statements or "white papers" that synthesize current evidence and provide recommendations, though these are not always universally adopted as formal guidelines.
- Evidence-Based Reviews: Ongoing systematic reviews and meta-analyses published in journals like the Journal of Bone and Joint Surgery (JBJS), Hand Clinics, and the Journal of Hand Surgery provide updated evidence synthesis for clinical decision-making.
In summary, the literature underscores the importance of prompt and accurate diagnosis, individualized treatment planning based on fracture characteristics and patient factors, meticulous surgical technique when indicated, and structured post-operative rehabilitation to achieve optimal outcomes for scaphoid fractures. Ongoing research continues to refine diagnostic and therapeutic strategies.
You Might Also Like