Olecranon Fractures: Epidemiology, Anatomy, Biomechanics & Classification
Key Takeaway
Olecranon fractures are elbow injuries resulting from direct trauma (falls, blows) causing comminuted patterns, or indirect trauma (fall on outstretched hand with elbow flexion) leading to avulsion fractures. They are classified by systems like Mayo (Type I nondisplaced, Type II displaced, Type III fracture-dislocation) and AO/OTA, guiding surgical planning and management.
Introduction & Epidemiology
Olecranon fractures constitute a significant proportion of elbow trauma, accounting for approximately 8% to 10% of all elbow fractures. Understanding the epidemiology, anatomy, and biomechanics of these injuries is fundamental for optimal management.
The incidence of olecranon fractures in the adult population is reported at 11.5 per 100,000 population per year. A distinct bimodal distribution is observed. In younger individuals, olecranon fractures are typically the result of high-energy trauma, such as motor vehicle accidents or direct sports-related impact. These injuries often present with greater comminution and associated soft tissue involvement or other concomitant injuries. Conversely, older individuals commonly sustain an olecranon fracture as a result of a simple fall from standing height. This demographic often presents with osteoporotic bone, which influences fracture patterns and fixation strategies. Given the olecranon's critical role in the extensor mechanism and elbow stability, precise diagnosis and management are paramount to restore function and prevent long-term morbidity.
Surgical Anatomy & Biomechanics
The olecranon, the most proximal aspect of the ulna, forms a critical component of the elbow joint and the forearm's extensor mechanism. Proximally, it articulates with the trochlea of the humerus, forming the humeroulnar joint. This articulation is inherently stable due to its congruent trochlear notch (also known as the greater sigmoid notch).
The coronoid process delineates the distal border of the greater sigmoid notch of the ulna. The trochlear notch, formed by the olecranon proximally and the coronoid distally, engages the trochlea of the humerus. This highly congruent articulation allows motion primarily about the flexion-extension axis, thus providing intrinsic stability to the elbow joint, particularly against valgus and varus stresses. The articular cartilage surface within the trochlear notch is interrupted by a transverse ridge, typically located at the junction of the olecranon and coronoid, known as the "bare area" or the "watershed line." This area is devoid of cartilage and is a crucial anatomical landmark, often corresponding to the site of simple transverse olecranon fractures.
The triceps tendon, a powerful extensor of the elbow, posteriorly envelops the articular capsule before it inserts broadly onto the dorsal and proximal surfaces of the olecranon. This robust tendinous insertion is critical for active elbow extension. A fracture of the olecranon with displacement, especially those involving the metaphyseal-diaphyseal junction or further proximal, represents a functional disruption of the triceps mechanism. This disruption directly results in a loss of active elbow extension, making anatomical reduction and stable fixation essential for restoring this function.
The olecranon has a distinct developmental ossification pattern. Its ossification center typically appears around age 10 years and fuses with the ulnar diaphysis by approximately age 16 years. It is important to note that persistent epiphyseal plates (apophyses) can be observed in adults; these are usually bilateral and demonstrate familial inheritance. Recognition of this variant is crucial to avoid misinterpreting it as a fracture. The subcutaneous position of the olecranon makes it uniquely vulnerable to direct trauma.

Mechanism of Injury
Two common mechanisms are observed, each resulting in a predictable fracture pattern:
- Direct Trauma: A fall directly on the point of the elbow or a direct blow to the olecranon typically results in comminuted or transverse fracture patterns. The fracture configuration is often localized to the olecranon process itself, with varying degrees of articular involvement and comminution depending on the energy of the impact. The fracture line tends to be transverse or short oblique.
- Indirect Trauma: A fall on an outstretched hand with the elbow in flexion generates an axial load combined with a strong eccentric contraction of the triceps muscle. This indirect mechanism results in an avulsion type of fracture, often with a transverse or long oblique fracture pattern. The strong tensile forces exerted by the triceps tend to displace the proximal fragment proximally, and the humerus acts as a fulcrum, potentially impacting the olecranon and leading to fracture. This mechanism can also be associated with elbow dislocation, especially in higher energy settings.
Fracture Classification
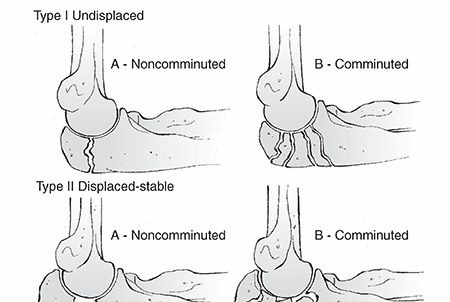
While numerous classification systems exist, a commonly utilized approach involves assessing fracture morphology, displacement, and comminution. The Mayo Classification of Olecranon Fractures is frequently referenced:
*
Type I (Nondisplaced):
Articular congruity maintained, minimal displacement.
*
Type II (Displaced):
*
IIA (Nondisplaced Comminuted):
Significant comminution but fragments remain in acceptable alignment.
*
IIB (Displaced Comminuted):
Displaced and comminuted.
*
Type III (Fracture-Dislocation):
Olecranon fracture associated with elbow dislocation.
The AO/OTA Classification is also used, providing a more detailed descriptive system based on bone region and fracture complexity (e.g., 21-U1, 21-U2). For practical surgical planning, assessment of articular involvement, fragment size, comminution, and bone quality are critical.
Indications & Contraindications
The decision to proceed with operative or non-operative management of an olecranon fracture hinges on several factors, primarily fracture stability, displacement, articular congruity, and patient-specific variables.
Non-Operative Indications
Non-operative management is typically reserved for highly selected cases that meet strict criteria. The fundamental principle is that the fracture must be stable and maintain an acceptable anatomical position throughout the healing process.
- Minimally Displaced Fractures: Fractures with less than 2 mm of displacement and less than 2 mm of articular step-off.
- Stable Fractures: Fractures that demonstrate stability to stress examination (e.g., gravitational stress in various elbow positions) and do not propagate displacement with active elbow flexion or gravity.
- Intact Extensor Mechanism: The patient must be able to actively extend the elbow against gravity, confirming the integrity of the triceps mechanism despite the fracture.
- Comorbidities: Patients with severe medical comorbidities that preclude safe surgical intervention, or those with very low functional demands where the risks of surgery outweigh the potential benefits. In these instances, functional outcomes may be compromised, but non-operative care prioritizes patient safety.
Non-operative treatment generally involves a period of immobilization (typically 2-3 weeks in a long-arm cast or brace with the elbow flexed 45-90 degrees) followed by a carefully progressed rehabilitation protocol. Regular radiographic follow-up is essential to monitor for secondary displacement.
Operative Indications
Operative fixation is the mainstay of treatment for the vast majority of olecranon fractures, given their articular involvement and the critical role of the triceps mechanism. The primary goals are anatomical reduction of the articular surface, stable fixation to allow early motion, and restoration of the extensor mechanism.
- Displaced Fractures: Any fracture with greater than 2 mm of displacement. This displacement translates to a functional loss of the triceps lever arm.
- Articular Incongruity: Any articular step-off greater than 2 mm, which significantly increases the risk of post-traumatic arthritis.
- Loss of Active Elbow Extension: The inability to actively extend the elbow against gravity indicates disruption of the triceps mechanism, necessitating surgical repair.
- Open Fractures: All open olecranon fractures require emergent surgical debridement and stabilization to minimize infection risk and optimize healing.
- Associated Injuries: Fractures associated with elbow instability (e.g., fracture-dislocations, Monteggia-type injuries) or other ipsilateral upper extremity trauma often necessitate operative stabilization to facilitate overall limb rehabilitation.
- Failure of Non-Operative Treatment: Documented secondary displacement during non-operative management.
Contraindications
Absolute contraindications to operative intervention are rare and primarily revolve around the patient's physiological status (e.g., active infection, uncontrolled systemic illness, severe skin compromise over the surgical site). Relative contraindications include poorly controlled diabetes, severe peripheral vascular disease, or severe osteoporosis where implant purchase may be inadequate. In these cases, a thorough risk-benefit analysis is performed with the patient and family.

Summary of Operative vs. Non-Operative Indications
| Indication Category | Non-Operative Management | Operative Management |
|---|---|---|
| Fracture Type | Minimally displaced (<2mm), stable, articular step-off < 2mm | Displaced (>2mm), unstable, articular step-off > 2mm, comminuted, open |
| Extensor Function | Intact active elbow extension | Loss of active elbow extension |
| Associated Injuries | Isolated, no associated instability | Fracture-dislocation, Monteggia-type, significant soft tissue injury |
| Patient Factors | High anesthetic risk, severe comorbidities, very low functional demand | Healthy, reasonable surgical candidate, desire for full function |
| Radiographic | Stable on stress views | Secondary displacement during non-op treatment |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential for predictable outcomes in olecranon fracture fixation.
Pre-operative Evaluation
- Clinical Assessment: A detailed history regarding the mechanism of injury, hand dominance, and pre-existing elbow function is crucial. A neurovascular assessment, particularly of the ulnar nerve, radial nerve, and median nerve, is mandatory. Inspection for open wounds, compartment syndrome, or signs of associated injuries is also critical.
-
Imaging:
- Standard Radiographs: Anteroposterior (AP) and true lateral views of the elbow are the initial imaging modalities. The lateral view is especially informative for assessing displacement, comminution, and articular step-off. Oblique views may be helpful for complex patterns.
- Computed Tomography (CT) Scan: A CT scan with 3D reconstructions is invaluable for surgical planning, especially in comminuted fractures, articular impaction, or fracture-dislocations. It provides detailed information on fragment orientation, true articular involvement, and helps identify occult associated injuries (e.g., coronoid fractures).
- Templating: For plate fixation, pre-operative templating using radiographs or CT reconstructions can assist in selecting the appropriate plate length, contour, and screw trajectories.
Implant Selection
The choice of implant depends on the fracture pattern, bone quality, and surgeon preference:
*
Tension Band Wiring (TBW):
Ideal for simple transverse or short oblique fractures with good bone stock. It effectively converts tensile forces (from triceps) into compressive forces at the fracture site.
*
Plate Fixation:
Indicated for comminuted fractures, long oblique fractures, osteoporotic bone, fracture-dislocations, or revision cases. Various plates exist, including pre-contoured olecranon-specific plates, one-third tubular plates, or reconstruction plates. Locking plates offer advantages in osteoporotic bone.
*
Intramedullary (IM) Screw:
Less common, typically limited to simple transverse fractures in specific scenarios, often combined with K-wires.
Patient Positioning
The patient is typically positioned supine on the operating table with a sterile tourniquet applied to the upper arm. The arm is then draped to allow full sterile access, including the upper arm, elbow, and forearm. The arm can be placed on a hand table for support or positioned across the patient's chest for easier access to the posterior aspect of the elbow. Some surgeons prefer a lateral decubitus or even prone position for complex cases or to facilitate specific approaches, but supine with the arm draped across the chest is the most common and versatile setup.

Detailed Surgical Approach / Technique
The goal of surgical management is anatomical reduction of the articular surface, stable fixation, and restoration of the triceps extensor mechanism, allowing for early range of motion.
Surgical Approach
- Incision: A posterior midline longitudinal incision is most commonly utilized. This allows for excellent exposure of the olecranon and distal humerus while protecting critical neurovascular structures. The incision should extend sufficiently proximally to allow for triceps access and distally to adequately expose the ulnar shaft if plate fixation is anticipated.
- Skin Flaps: Full-thickness skin flaps are raised medially and laterally to protect the ulnar nerve. Care must be taken to avoid thin skin flaps, which are prone to necrosis, especially given the subcutaneous nature of the olecranon.
- Ulnar Nerve Identification and Protection: The ulnar nerve lies posterior to the medial epicondyle in the cubital tunnel. It is imperative to identify and protect the ulnar nerve throughout the procedure. Some surgeons routinely decompress or transpose the ulnar nerve, especially if using a bulky plate on the medial side or if pre-existing symptoms are present. However, routine transposition is not universally recommended. The nerve can be gently retracted anteriorly or mobilized and protected during the approach.
Exposure and Reduction
- Fracture Visualization: The hematoma is evacuated to allow for clear visualization of the fracture fragments, articular surface, and triceps insertion.
- Fragment Dissection: The fracture fragments are meticulously dissected from surrounding soft tissues, minimizing further devitalization. The triceps mechanism attached to the proximal fragment should be preserved.
-
Articular Reduction:
This is the most critical step. The articular surface of the olecranon must be perfectly reduced to restore elbow congruity. This is often achieved by applying traction to the forearm while gently manipulating the fragments. A pointed reduction clamp (e.g., Verbrugge clamp) or towel clamp can be used to hold the main fragments provisionally.
- For comminuted articular fragments, these are often reduced first, potentially using small K-wires for provisional fixation.
- The "bare area" or watershed line can serve as a guide for anatomical reduction.
- Fluoroscopic guidance (AP and lateral views) is essential to confirm anatomical reduction, particularly of the articular surface.

Fixation Techniques
1. Tension Band Wiring (TBW)
TBW is a biomechanically sound method for simple transverse or short oblique olecranon fractures with good bone stock. It converts tensile forces from the triceps into compressive forces across the fracture site.
-
Technique:
- K-wire Insertion: Two parallel 1.6-2.0 mm K-wires are inserted from the proximal olecranon tip across the fracture site into the anterior cortex of the ulna. The K-wires should be parallel to each other and perpendicular to the fracture plane. They should engage the anterior cortex to prevent backing out and rotation.
- Transosseous Drill Hole: A transverse drill hole (typically 2.5-3.5 mm) is made approximately 3-4 cm distal to the fracture, through the ulnar cortex.
- Figure-of-Eight Wire Loop: A 1.0-1.25 mm stainless steel wire is passed in a figure-of-eight fashion: through the triceps tendon proximal to the K-wires, then looped around the ends of the K-wires, and finally passed through the transverse drill hole distally.
- Tightening: The wire is carefully tightened, usually by twisting, to achieve compression across the fracture site. The K-wires are then bent at a 180-degree angle and cut short, with the ends buried into the triceps tendon or deep fascia to prevent skin irritation. The figure-of-eight wire knot is also buried.
- Compression Check: Active and passive elbow range of motion is performed to ensure stable compression and absence of gapping at the fracture site.
2. Plate Fixation
Plate fixation is a versatile technique indicated for comminuted fractures, long oblique fractures, osteoporotic bone, and fracture-dislocations. Pre-contoured olecranon-specific plates are generally preferred as they match the complex anatomy of the proximal ulna.
-
Technique:
- Plate Selection and Contouring: A pre-contoured olecranon plate is typically chosen. If not available, a reconstruction plate or one-third tubular plate can be manually contoured to match the posterior surface of the olecranon and proximal ulna. The plate should extend sufficiently proximally to capture the main olecranon fragment and distally to provide adequate screw purchase in the ulnar shaft (typically 6-8 cortices distally).
- Provisional Fixation: After anatomical articular reduction, provisional fixation with K-wires or reduction clamps is secured.
- Plate Application: The contoured plate is then applied to the posterior aspect of the olecranon. The most proximal screw in the olecranon fragment should be directed distally and anteriorly, aiming for optimal purchase without violating the articular surface.
- Compression and Screws: For simple patterns or when using non-locking plates, a lag screw can be placed across the fracture site before plating to achieve interfragmentary compression. Otherwise, the plate can be used to generate compression via eccentric drilling in appropriate plate holes (dynamic compression plating). For comminuted fractures or osteoporotic bone, locking screws are preferred as they provide angular stability and do not rely on plate-bone compression. Screws should be bicortical where possible.
- Posterior Olecranon Bridge Plate: For highly comminuted fractures, a posterior bridge plate can span the comminution, ensuring axial and rotational stability. Small articular fragments can be fixed to the main fragments with small K-wires or absorbable sutures if bone stock is insufficient for screws.
- Check Articulation: Throughout fixation, the elbow is ranged to ensure hardware does not impinge and that a stable, congruent articulation is achieved.


3. Intramedullary Screw Fixation
This technique is less commonly used and generally reserved for simple, transverse, non-comminuted fractures.
- Technique: A large-diameter cannulated screw is inserted from the olecranon tip, across the fracture, and into the ulnar diaphysis. It is often supplemented with K-wires or a tension band for rotational control. This method can be challenging to achieve stable fixation and maintain anatomical reduction, particularly in older patients with poor bone quality.
4. Fragment Excision and Triceps Advancement
In elderly, low-demand patients with highly comminuted distal olecranon fragments that are too small for stable fixation (typically < 50% of the olecranon), excision of the fragments and reattachment/advancement of the triceps tendon to the remaining ulna may be considered.
- Technique: The comminuted fragments are carefully excised. The triceps tendon is then advanced distally and securely reattached to the ulna, either through drill holes or with suture anchors. The goal is to restore the extensor mechanism. This technique typically results in some loss of extension strength and range of motion but can provide a functional outcome in selected patients.
Wound Closure
After achieving stable fixation and confirming reduction with fluoroscopy and elbow range of motion, the wound is copiously irrigated. The deep fascia is closed, followed by subcutaneous tissue and skin. The ulnar nerve is verified to be in a protected position. A drain may be inserted if there is significant dead space or hemorrhage. A sterile dressing and a well-padded posterior splint (typically in 30-45 degrees of flexion) are applied to provide initial protection.
Complications & Management
Despite meticulous surgical technique, complications following olecranon fracture fixation are relatively common and can significantly impact functional outcomes. Patient education and close follow-up are essential for early detection and management.

Common Complications and Management Strategies
| Complication | Incidence | Salvage Strategies / Management |
|---|---|---|
| Hardware Prominence / Irritation | Up to 80% (TBW) |
Incidence:
Extremely common, particularly with tension band wiring due to K-wire migration or knot prominence. Plate fixation can also cause irritation.
Management: Symptomatic hardware removal (SHR) typically after fracture union (6-12 months post-op). Education pre-operatively about this possibility is crucial. Early removal may risk fracture redisplacement. |
| Nonunion | 2-10% |
Incidence:
Higher in comminuted fractures, osteoporotic bone, inadequate fixation, or infection.
Management: Revision open reduction and internal fixation (ORIF) with bone grafting (autograft or allograft), often converting from tension band to plate fixation. Consider biological augmentation (e.g., bone morphogenetic protein) for recalcitrant cases. |
| Malunion | 5-15% |
Incidence:
Often due to inadequate articular reduction or secondary displacement. Can lead to painful range of motion limitation and post-traumatic arthritis.
Management: Corrective osteotomy and refixation, typically after symptoms develop and imaging confirms deformity. Non-operative management with activity modification if symptoms are mild. |
| Post-traumatic Arthritis | 10-30% |
Incidence:
Direct correlation with articular incongruity, impaction, and severity of initial injury.
Management: Initial conservative management with NSAIDs, injections, activity modification. For severe, symptomatic arthritis, surgical options include arthroscopic debridement, ulnohumeral arthroplasty, or total elbow arthroplasty in older, low-demand patients. |
| Infection (Superficial/Deep) | 1-5% |
Incidence:
Higher in open fractures, immunocompromised patients, or prolonged surgery.
Management: Superficial infections: Oral antibiotics, wound care. Deep infections: Surgical debridement, intravenous antibiotics tailored to culture results, possible hardware removal (after union) or staged reimplantation. External fixation may be needed in severe cases. |
| Ulnar Nerve Neuropathy | 5-15% |
Incidence:
Due to direct injury during surgery, prolonged retraction, compression from hardware, or scar tissue formation.
Management: Initial observation, NSAIDs, splinting. If symptoms persist or worsen, consider ulnar nerve decompression and/or anterior transposition. |
| Elbow Stiffness / Contracture | 20-50% |
Incidence:
Common sequela, particularly after prolonged immobilization, complex injuries, or heterotopic ossification.
Management: Aggressive post-operative rehabilitation, including physical therapy, dynamic splinting, and sometimes static progressive splinting. For recalcitrant stiffness, surgical options include arthroscopic or open capsular release. |
| Heterotopic Ossification (HO) | 5-15% |
Incidence:
Higher after severe trauma, head injury, or burns.
Management: Prophylaxis with NSAIDs (e.g., Indomethacin) or low-dose radiation in high-risk patients. For established HO causing functional limitation, surgical excision (typically after maturation, 6-12 months) followed by prophylaxis. |
| Implant Failure | Variable |
Incidence:
Fracture patterns, bone quality, and patient compliance influence risk.
Management: Revision surgery with more robust fixation (e.g., longer plate, locking plate, bone graft) and careful assessment of bone quality and surgical technique. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring elbow range of motion and strength while protecting the surgical repair. Protocols are tailored to the specific fracture pattern, fixation stability, bone quality, and patient's compliance.
General Principles
- Early Motion: The primary goal is to initiate early, controlled range of motion to prevent stiffness, improve cartilage nutrition, and optimize healing.
- Protection of Repair: The fixation must be protected from excessive stresses, particularly against the triceps pull in early phases.
- Gradual Progression: Rehabilitation progresses through distinct phases, gradually increasing load and range of motion.
Phased Rehabilitation Protocol
Phase I: Immediate Post-operative (Weeks 0-2)
- Goals: Reduce pain and swelling, protect surgical repair, maintain skin integrity, initiate passive/active-assisted range of motion (AAROM).
- Immobilization: A well-padded posterior splint is typically used for comfort and protection, especially when not performing exercises. Some surgeons prefer a hinged elbow brace.
-
Motion:
- Passive Range of Motion (PROM): Gentle, protected PROM for flexion-extension (typically 30° to 90-100° flexion, avoiding terminal extension initially) and forearm pronation/supination. Therapist-assisted or self-assisted (e.g., using the contralateral hand).
- Active-Assisted Range of Motion (AAROM): Within pain-free limits.
- Weight Bearing: Non-weight bearing for the operated extremity.
- Precautions: Avoid active triceps contraction or resisted extension. Avoid lifting anything heavier than a coffee cup. Ice and elevation for swelling.
Phase II: Early Motion and Protected Strengthening (Weeks 2-6)
- Goals: Gradually increase active range of motion, begin protected strengthening, improve muscular endurance.
- Brace: Progress to a hinged elbow brace, allowing controlled range of motion.
-
Motion:
- Continue PROM/AAROM, gradually increasing the arc towards full flexion and extension as tolerated (avoiding forced end-range extension initially, especially with tension band fixation).
- Initiate active range of motion (AROM) exercises for flexion, extension, pronation, and supination.
-
Strengthening:
- Begin with isometric exercises for biceps and forearm muscles, avoiding triceps.
- Light resistance for wrist and hand.
- Key Precaution: For tension band fixation, active resisted triceps extension is avoided until 6 weeks post-op to prevent disruption of the construct. For plate fixation, light gravity-assisted or gentle active triceps can begin earlier if fixation is robust.
- Weight Bearing: Still minimal weight bearing. Light daily activities are encouraged.
Phase III: Intermediate Strengthening and Functional Return (Weeks 6-12)
- Goals: Restore full range of motion, progressive strengthening of all elbow musculature, prepare for functional activities.
- Brace: Often discontinued if range of motion and stability are satisfactory.
- Motion: Continue to work towards full flexion and extension. Dynamic or static progressive splinting may be used for persistent stiffness.
-
Strengthening:
- Gradually introduce progressive resistance exercises for biceps, triceps, and forearm.
- Concentration on eccentric and concentric strengthening.
- Increase weight-bearing activities as tolerated.
- Activity: Begin functional activities, light lifting, and self-care tasks.
Phase IV: Advanced Strengthening and Return to Sport/Work (Weeks 12+)
- Goals: Maximize strength, power, and endurance; return to full activities, including sport or work-specific tasks.
- Strengthening: Advanced resistance training, plyometrics (if appropriate for sport), sport-specific drills.
- Activity: Gradual return to desired activities. High-impact or heavy resistance activities are introduced cautiously.
- Hardware Removal: If hardware prominence or irritation is significant, hardware removal may be considered after complete fracture union (typically 6-12 months post-op). A brief period of rest (2-4 weeks) is often recommended after hardware removal before returning to full activities.
It is imperative that the rehabilitation program is closely monitored by the orthopedic surgeon and a skilled physical therapist, with frequent reassessments to adjust the protocol based on fracture healing and patient progress.
Summary of Key Literature / Guidelines
Olecranon fractures have been extensively studied, leading to evolving best practices. Key principles are rooted in restoring articular congruity and extensor mechanism integrity.
- AO Principles: The fundamental AO principles of stable anatomical reduction and internal fixation allowing early mobilization remain the cornerstone of olecranon fracture management. The AO/OTA classification provides a universally recognized system for categorizing these injuries.
- Tension Band Wiring (TBW): While highly effective for simple transverse fractures, long-term studies and systematic reviews often report a high rate of symptomatic hardware requiring removal (up to 80%). However, functional outcomes are generally good in well-selected cases. TBW remains a valid and cost-effective option for simple patterns.
- Plate Fixation: A growing body of evidence supports plate fixation, particularly pre-contoured locking plates, for comminuted fractures, osteoporotic bone, and fracture-dislocations. Studies comparing plate fixation to TBW for complex patterns often show superior biomechanical stability and potentially better functional outcomes, though hardware removal rates can still be significant (around 20-40%). Locking plates have demonstrated advantages in maintaining reduction in comminuted and osteoporotic fractures by providing angular stability.
- Articular Reconstruction: The importance of anatomical articular reduction cannot be overstated. Numerous studies have linked residual articular step-off (even >2 mm) to increased rates of post-traumatic arthritis and poorer long-term functional outcomes. CT imaging is increasingly recognized as critical for pre-operative planning, especially for assessing articular involvement and comminution.
- Ulnar Nerve Management: The optimal management of the ulnar nerve (in-situ decompression vs. anterior transposition) during olecranon fracture fixation remains a topic of debate. Most literature suggests that routine prophylactic transposition is not necessary unless there are pre-existing symptoms or concerns about hardware impingement. Careful intraoperative identification and protection are paramount.
- Rehabilitation: Consensus guidelines emphasize early, controlled range of motion. Prolonged immobilization is associated with increased stiffness and poorer functional results. The rehabilitation protocol must be individualized, considering the stability of fixation and bone quality. For example, active triceps resistance is delayed longer in TBW constructs compared to robust plate fixation.
- Complication Rates: While successful outcomes are frequent, a notable rate of complications, particularly hardware irritation necessitating removal and post-traumatic stiffness, is consistently reported across various studies. This underscores the need for thorough pre-operative counseling and vigilant post-operative care.
In conclusion, the management of olecranon fractures has evolved towards increasingly stable internal fixation techniques that prioritize anatomical articular reduction and allow for early rehabilitation. The choice of surgical technique is guided by fracture morphology, patient factors, and surgeon experience, aiming to restore the intricate biomechanics of the elbow and optimize long-term patient function.
You Might Also Like


