Mastering the Management of Scaphoid Fractures: Avoid Complications
Key Takeaway
This topic focuses on Mastering the Management of Scaphoid Fractures: Avoid Complications, A scaphoid fracture, commonly from a hyper-dorsiflexed wrist injury, requires careful diagnosis through imaging. Mastering the management involves evaluating treatment options like prolonged immobilization or surgical fixation. Proximal pole fractures have a high non-union rate due to their compromised retrograde blood supply, highlighting the need for precise clinical and therapeutic approaches for optimal healing outcomes.
Introduction & Epidemiology
Scaphoid fractures represent the most common carpal bone fracture, accounting for approximately 60-70% of all carpal injuries and 2-3% of all fractures. The typical mechanism of injury involves a fall onto an outstretched hand (FOOSH) with the wrist in dorsiflexion and radial deviation, compressing the scaphoid against the dorsal rim of the distal radius. This unique injury pattern, coupled with the scaphoid's intricate anatomy and tenuous blood supply, predisposes it to a high incidence of nonunion, malunion, and avascular necrosis (AVN), leading to chronic pain, wrist instability, and ultimately scaphoid nonunion advanced collapse (SNAC) wrist. Early and accurate diagnosis, followed by appropriate management, is therefore paramount to optimize patient outcomes and prevent debilitating long-term complications. The challenges in managing scaphoid fractures lie in their often subtle presentation, radiographic occultation in the acute phase, and the critical importance of achieving anatomic reduction and stable fixation to ensure timely union and preserve carpal kinematics.
Surgical Anatomy & Biomechanics
Gross Anatomy and Morphology
The scaphoid is an irregularly shaped carpal bone, approximately 2-3 cm in length, with a unique 'C' or 'S' shape. It spans both the proximal and distal carpal rows, making it an intercalated segment critical for carpal stability and motion. It articulates proximally with the distal radius and lunate, distally with the trapezium and trapezoid, and medially with the capitate. Functionally, it acts as a mechanical link, transferring loads from the hand to the forearm.
For descriptive purposes, the scaphoid is divided into four main regions:
*
Tubercle:
The most distal and radial aspect, serving as an attachment site for the transverse carpal ligament.
*
Distal Pole:
Distal to the waist, articulating with the trapezium and trapezoid.
*
Waist:
The constricted central portion, where approximately 70-80% of scaphoid fractures occur.
*
Proximal Pole:
Proximal to the waist, articulating with the radius and lunate. This region is particularly susceptible to AVN due to its precarious blood supply.
Vascular Anatomy
The blood supply to the scaphoid is predominantly retrograde, arising primarily from the radial artery.
*
Dorsal Carpal Artery Branch:
The main blood supply (approximately 80%) originates from the dorsal carpal branch of the radial artery. This vessel enters the scaphoid via multiple small branches along the dorsal ridge, supplying the proximal two-thirds of the bone.
*
Palmar Carpal Artery Branch:
The remaining 20% of the blood supply comes from the palmar carpal branch of the radial artery, which enters the scaphoid through the distal pole and tubercle, supplying mainly the distal third.
This retrograde flow pattern means that fractures through the waist or proximal pole can easily compromise the blood supply to the proximal fragment, significantly increasing the risk of AVN. The lack of significant intraosseous collateral circulation further exacerbates this vulnerability.
Ligamentous Attachments
The scaphoid is stabilized by numerous intrinsic and extrinsic ligaments:
*
Intrinsic Ligaments:
The most important is the scapholunate interosseous ligament (SLIL), connecting the scaphoid to the lunate. Injury to this ligament often accompanies scaphoid fractures or contributes to carpal instability.
*
Extrinsic Ligaments:
Key extrinsic ligaments include the radioscaphocapitate ligament (RSC), long radiolunate ligament, and the scaphotrapezio-trapezoidal (STT) ligament complex. These ligaments are crucial for maintaining carpal alignment and stability.
Biomechanics
The scaphoid's unique position and ligamentous attachments make it a critical component of carpal mechanics. It functions as an intercalated segment, bridging the proximal and distal carpal rows.
*
Kinematic Role:
During wrist motion, the scaphoid flexes with the distal carpal row during radial deviation and extends during ulnar deviation. Disruption of the scaphoid's integrity or its ligamentous attachments (e.g., SLIL) can lead to a cascade of abnormal carpal kinematics.
*
SNAC Wrist:
A nonunion or malunion of the scaphoid can lead to a compensatory dorsal intercalated segmental instability (DISI) deformity, where the lunate extends dorsally, and the capitate translates proximally. Over time, this abnormal loading pattern results in progressive radioscaphoid and midcarpal arthritis, known as SNAC wrist. The typical progression involves arthritis at the radial styloid-scaphoid articulation, followed by the scaphoid-capitate joint, and eventually the entire radioscaphoid joint, classically sparing the capitolunate joint until late stages. This degenerative pathway highlights the critical importance of anatomic reduction and stable fixation.
Indications & Contraindications
The decision-making process for managing scaphoid fractures hinges on several factors, including fracture location, displacement, stability, patient age, activity level, and associated injuries. While non-operative management can be successful for select stable fractures, operative intervention is increasingly favored for many patterns to improve union rates, reduce immobilization time, and prevent long-term complications.
Non-Operative Indications
- Nondisplaced Distal Tubercle Fractures: These fractures typically have an excellent blood supply and biomechanical stability. They often heal well with short-term immobilization.
- Nondisplaced Distal Pole Fractures: Similar to tubercle fractures, these generally have a favorable prognosis.
- Nondisplaced, Stable Scaphoid Waist Fractures (Herbert Type A): This category remains controversial. While some argue for a trial of non-operative management with strict cast immobilization (thumb spica cast for 6-12 weeks or longer), evidence increasingly supports earlier operative intervention for waist fractures to expedite union and minimize nonunion rates, even if "nondisplaced" by standard X-rays. High-resolution CT scanning is crucial to confirm true nondisplacement.
- Proximal Pole Fractures (Selected Nondisplaced): Extremely rare to manage non-operatively due to high AVN risk. If selected for non-operative management, requires very close monitoring.
Operative Indications
-
Displaced Scaphoid Fractures:
- Any displacement >1 mm (including articular step-off).
- Intrascaphoid angulation >10-15° (humpback deformity).
- Rotational instability.
-
Unstable Fracture Patterns (Herbert Type B):
- Complete fractures of the waist (B1, B2, B3).
- Proximal pole fractures (B4), especially those that are displaced, due to high risk of AVN.
- Vertical oblique fractures.
- Comminuted fractures.
- Scaphoid fracture-dislocations.
-
Scaphoid Nonunion:
- Symptomatic nonunion, especially with signs of collapse or early arthritis.
- Any nonunion in an active individual.
-
Scaphoid Delayed Union:
- Lack of radiographic signs of healing after 3-4 months of appropriate non-operative treatment.
-
Concomitant Carpal Ligamentous Injuries:
- Associated scapholunate instability or other significant carpal ligament tears.
-
Patient Preference:
- Athletes or individuals in professions requiring early return to high-demand activities, who prefer the potentially faster return associated with surgical fixation.
Contraindications
- Absolute Medical Contraindications: Unstable medical comorbidities that preclude surgery (e.g., severe cardiopulmonary disease, uncontrolled diabetes).
- Severe Local Infection: Active infection at the surgical site.
- Non-reconstructible Scaphoid: Extremely comminuted fractures with extensive bone loss or long-standing nonunions with significant collapse and advanced arthritis, where primary reconstruction is not feasible. These cases may necessitate salvage procedures such as proximal row carpectomy (PRC), scaphoid excision and four-corner fusion (4CF), or wrist fusion.
Summary Table: Operative vs. Non-Operative Indications
| Feature / Indication | Non-Operative Management | Operative Management |
|---|---|---|
| Fracture Location | Distal tubercle, select nondisplaced distal pole | Waist, proximal pole, displaced distal pole |
| Displacement | Truly nondisplaced (<1mm, no angulation) by CT confirmation | Displacement >1mm, angulation >10-15°, rotational instability |
| Stability | Stable (e.g., Herbert Type A) | Unstable (e.g., oblique, comminuted, Herbert Type B) |
| Union Status | Acute fractures with high healing potential | Delayed union, established nonunion, AVN |
| Associated Injuries | Isolated scaphoid fracture | Concomitant carpal instability (e.g., SLIL tear) |
| Patient Factors | Low-demand, willing to tolerate prolonged immobilization | High-demand, athletes, desire for early return to activity |
| Imaging Findings (CT) | Absence of significant comminution, articular step-off, or gap | Presence of comminution, step-off, gap, humpback deformity |
| Time to Treatment | Within days of injury | Acute or delayed |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential to anticipate surgical challenges, select the optimal approach, and maximize the chances of successful union while minimizing complications.
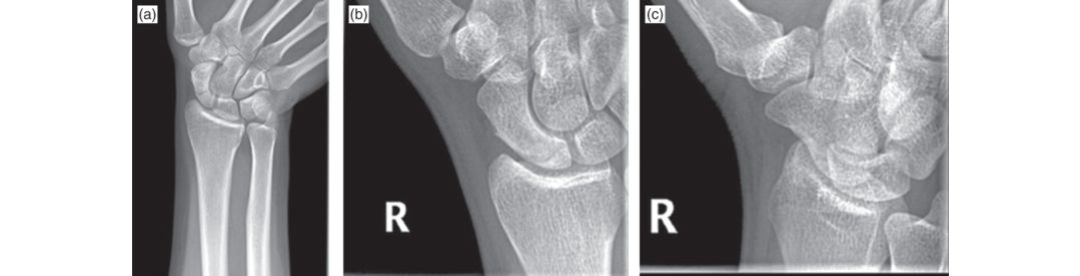
Imaging
- Standard Radiographs: Initial assessment with PA, lateral, oblique, and scaphoid-specific views (e.g., 30° pronated oblique) is mandatory. These films can reveal displacement, angulation, and signs of existing arthritis. However, they often underestimate displacement or miss occult fractures.
-
Computed Tomography (CT) Scan:
A fine-cut CT scan (0.625-1 mm slices) is considered the gold standard for detailed fracture assessment. It provides critical information regarding:
- Precise fracture morphology (simple, oblique, comminuted).
- Degree of displacement, angulation (e.g., intrascaphoid angle, humpback deformity), and rotational malalignment.
- Articular step-off.
- Bone loss or cystic changes in nonunions.
- Evidence of AVN (sclerosis of the proximal pole).
- Aids in choosing the optimal screw length and trajectory.
-
Magnetic Resonance Imaging (MRI):
Highly sensitive for diagnosing occult scaphoid fractures not visible on plain radiographs or CT. It is also invaluable for assessing:
- Early signs of AVN (edema, altered signal intensity).
- Concomitant ligamentous injuries (e.g., scapholunate ligament tear).
- Vascularity of the proximal pole.
- Arthrography / Dynamic Fluoroscopy: Less commonly used but can assess carpal stability and ligamentous integrity in complex cases.
Surgical Planning Considerations
-
Approach Selection:
Based on fracture location, displacement, need for bone graft, and surgeon preference.
- Volar approach: Favored for waist and distal pole fractures, and for reducing a volar flexed proximal pole fragment. Allows easier insertion of a screw across the waist.
- Dorsal approach: Preferred for proximal pole fractures, dorsal comminution, and nonunions requiring dorsal bone grafting. Provides better access to the dorsal aspect of the scaphoid for reduction and graft placement.
- Fixation Choice: Headless cannulated compression screws (e.g., Herbert, Acutrak) are standard. Screw length, diameter, and thread pattern are chosen based on fracture size and quality.
- Bone Grafting: Determine if bone grafting is required (e.g., for nonunions, AVN, significant bone loss). Plan for autograft harvest (distal radius, iliac crest) or consider vascularized bone grafts.
- Reduction Strategy: Plan the sequence of reduction maneuvers (e.g., joystick K-wires, direct manipulation).
- Tourniquet Time: Anticipate the duration of the procedure to allow for appropriate tourniquet management.
Patient Positioning
- Supine Position: The patient is positioned supine on the operating table.
- Arm Table: The affected arm is placed on a dedicated hand table, ensuring ample space for surgical instrumentation and fluoroscopy.
- Padding: All pressure points (e.g., elbow, contralateral arm) are well-padded to prevent nerve compression injuries.
- Tourniquet: A pneumatic tourniquet is applied to the upper arm to provide a bloodless field, typically inflated to 250-300 mmHg.
- Fluoroscopy: The image intensifier (C-arm) is positioned and draped to allow for intraoperative radiographic views (PA, lateral, oblique, and true scaphoid views) without compromising the sterile field. This requires careful pre-operative setup and sometimes adjustments during the procedure. The ability to obtain true lateral views is critical for assessing angulation and screw trajectory.
- Wrist Position: The wrist is often held in slight extension and ulnar deviation for exposure, or neutrally, depending on the chosen approach and fracture pattern. For specific fracture patterns, distraction may be beneficial via finger traps.
Detailed Surgical Approach / Technique
The goal of surgical management is anatomical reduction, stable internal fixation, and preservation of the scaphoid's vascularity to promote union and restore carpal kinematics.
General Principles
- Anatomic Reduction: This is paramount. Even small amounts of displacement or angulation can lead to malunion and long-term sequelae.
- Stable Fixation: A compression screw provides interfragmentary compression, which is crucial for primary bone healing.
- Preservation of Blood Supply: Meticulous dissection and minimal soft tissue stripping are essential, especially for the precarious proximal pole.
- Fluoroscopic Guidance: Continuous intraoperative fluoroscopy is critical for confirming reduction, guide wire placement, and screw positioning.
1. Volar Approach (Modified Henry's Approach)
This approach is generally preferred for waist and distal pole fractures, as well as for reducing a volar flexed proximal pole fragment.
- Incision: A longitudinal incision approximately 4-6 cm in length is made along the radial border of the flexor carpi radialis (FCR) tendon, centered over the distal scaphoid.
-
Dissection:
- The skin and subcutaneous tissues are incised. Care is taken to identify and protect the palmar cutaneous branch of the median nerve radially and superficial branches of the radial artery ulnarly.
- The FCR tendon sheath is identified and incised longitudinally along its radial side. The FCR tendon is retracted ulnarly.
- Deep to the FCR, the radial artery is identified. It runs obliquely towards the thenar eminence. The radial artery and its branches are carefully protected and retracted radially.
- The interval between the FCR tendon (ulnarly) and the radial artery (radially) is developed. The pronator quadratus muscle lies deep and distal.
- The radioscaphocapitate ligament (RSC) and the volar wrist capsule are encountered. A longitudinal capsulotomy is performed, often extending proximally to the radial styloid and distally over the scaphoid.
-
Exposure:
The volar aspect of the scaphoid waist and distal pole is exposed. For proximal pole fractures, the exposure needs to extend more proximally.

Figure 1: Volar exposure of the scaphoid, demonstrating the interval between the FCR tendon and radial artery. -
Reduction:
- The fracture fragments are identified. Joy-sticking with small K-wires inserted into the fragments can assist in manipulation.
- Manual compression and careful manipulation under fluoroscopic guidance are used to achieve anatomical reduction. A ball-tipped K-wire can be used to hold the reduction temporarily.
- For humpback deformities, dorsal compression or a specialized reduction clamp may be necessary.
-
Fixation:
- Once reduced, a guidewire for the headless compression screw is inserted either antegrade (distal to proximal) or retrograde (proximal to distal) depending on the fracture pattern and surgeon preference. For waist fractures, antegrade insertion from the distal tubercle is common. The guidewire should be centrally placed in both PA and lateral fluoroscopic views, maintaining perpendicularity to the fracture plane.
- Measure screw length. Cannulated drill bit is used to create the appropriate pilot hole.
- The headless compression screw is then inserted over the guidewire. It should be countersunk beneath the articular surface at both ends to prevent impingement. Compression across the fracture site is confirmed fluoroscopically.
- Closure: The capsule is repaired. The FCR sheath may be closed. Subcutaneous tissues and skin are closed in layers.
2. Dorsal Approach
This approach is generally preferred for proximal pole fractures, dorsal comminution, and nonunions requiring dorsal bone grafting.
- Incision: A longitudinal incision, approximately 4-6 cm, is made slightly ulnar to Lister's tubercle, centered over the scaphoid.
-
Dissection:
- Skin and subcutaneous tissues are incised. Care is taken to protect branches of the superficial radial nerve.
- The extensor retinaculum is identified. The interval between the 3rd dorsal compartment (EPL) and the 4th dorsal compartment (EDC, EIP) is developed. Lister's tubercle is identified.
- The EPL tendon is retracted radially.
- The dorsal wrist capsule is identified. A longitudinal capsulotomy is performed directly over the proximal scaphoid.
-
Exposure:
The dorsal aspect of the scaphoid, especially the proximal pole and part of the waist, is exposed.
Figure 2: Dorsal exposure of the scaphoid, highlighting the interval between the third and fourth dorsal compartments and the dorsal blood supply. - Reduction: Similar to the volar approach, reduction is achieved using K-wires or careful manipulation under fluoroscopic guidance.
-
Fixation:
- A guidewire is typically inserted antegrade from the proximal pole into the distal fragment. This allows for optimal compression and minimizes damage to the distal articular cartilage. The guidewire must be centrally placed and perpendicular to the fracture.
- Screw length is measured, and the pilot hole is drilled.
- The headless compression screw is inserted, ensuring it is countersunk.
- Closure: The capsule is repaired. The extensor retinaculum may be partially repaired or left open if tension-free. Subcutaneous tissues and skin are closed.
3. Arthroscopy-Assisted Fixation
- Indications: Minimally displaced fractures, assessment of concomitant ligamentous injuries (e.g., SLIL), or to verify reduction accuracy without extensive capsular exposure.
- Technique: Standard wrist arthroscopy portals are established (e.g., 3-4, 4-5 for visualization; 1-2, 6R for instrumentation). Fractures are reduced under arthroscopic visualization, and guidewires for headless compression screws are inserted percutaneously.
- Advantages: Minimally invasive, reduced soft tissue disruption, direct visualization of articular surfaces and associated pathology.
- Disadvantages: Technically demanding, longer learning curve, limited by severe displacement or comminution.
4. Bone Grafting
- Indications: Required for established nonunions, AVN, or fractures with significant bone loss (e.g., cystic changes).
-
Types of Grafts:
- Non-vascularized Autograft: Most commonly harvested from the distal radius (volar aspect, just distal to Lister's tubercle) or the iliac crest. Provides osteoconductive and osteoinductive properties. The defect is curetted to healthy bleeding bone, and the graft is then impacted into the defect to restore scaphoid length and alignment.
-
Vascularized Autograft:
Indicated for established AVN of the proximal pole or recalcitrant nonunions, particularly when previous non-vascularized grafting has failed. Common sources include:
- 1,2 Intercompartmental Supraretinacular Artery (1,2 ICSRA) Graft: A pedicled graft harvested from the dorsal aspect of the distal radius, based on the 1,2 ICSRA, which is a branch of the radial artery. It provides vascularized bone graft to the dorsal scaphoid.
- Pronator Quadratus Pedicled Graft: A volar-based vascularized graft for volar defects.
- Allograft: Less common, typically used when autograft sites are exhausted or in revision cases, but generally less osteoinductive than autograft.
After bone grafting, stable screw fixation is crucial to hold the graft and fragments under compression.
Complications & Management
Despite meticulous surgical technique, scaphoid fracture management is prone to several complications, primarily due to the bone's unique anatomy and blood supply. Preventing these complications is central to effective treatment.
1. Nonunion
- Incidence: Varies widely, 5-10% even with operative fixation, and significantly higher (up to 30-40%) with non-operative treatment of unstable or displaced fractures.
- Pathogenesis: Inadequate reduction, insufficient fixation stability, compromise of blood supply (especially to the proximal pole), poor patient compliance (e.g., smoking), and delayed diagnosis/treatment.
- Clinical Presentation: Persistent pain, tenderness in the anatomical snuffbox, decreased grip strength, limited range of motion. Radiographs and CT scans show a persistent fracture line, sclerosis, cystic changes, and potentially early signs of carpal collapse.
-
Management:
- Revision Surgery: The mainstay of treatment. Involves débridement of the nonunion site to bleeding bone, stable internal fixation, and almost always bone grafting.
- Bone Grafting: Non-vascularized bone graft (distal radius or iliac crest) is typically used for established nonunions without significant AVN. Vascularized bone grafts (e.g., 1,2 ICSRA or pronator quadratus pedicled graft) are reserved for nonunions with significant AVN, bone loss, or failed previous non-vascularized grafts.
- Salvage Procedures: For long-standing nonunions with advanced SNAC wrist (radiocarpal arthritis), salvage procedures such as proximal row carpectomy (PRC), scaphoid excision and four-corner fusion (4CF), or wrist arthrodesis may be indicated.
2. Avascular Necrosis (AVN)
- Incidence: Highly variable, estimated 10-30% for proximal pole fractures, lower for waist fractures. Directly related to the extent of vascular compromise.
- Pathogenesis: Disruption of the retrograde blood supply to the proximal pole, leading to bone death.
- Clinical Presentation: Can present as delayed union, nonunion, or progressive collapse of the proximal fragment. Radiographs may show increased density (sclerosis) of the proximal pole, fragmentation, or collapse. MRI is the most sensitive diagnostic tool, showing altered signal intensity.
-
Management:
- Early AVN with Union Potential: Vascularized bone grafting (e.g., 1,2 ICSRA) with stable internal fixation to revascularize the fragment and promote union.
- Established AVN with Collapse/Arthritis: If significant collapse or early arthritic changes have occurred, salvage procedures such as PRC or 4CF may be necessary. In rare, early cases without significant collapse, core decompression might be considered.
3. Malunion
- Incidence: Can occur if reduction is not anatomical, leading to persistent angulation (humpback deformity) or rotation.
- Pathogenesis: Inadequate reduction during initial surgery or collapse during prolonged non-operative management.
- Clinical Presentation: Persistent pain, decreased wrist range of motion, altered carpal kinematics, and predisposition to SNAC wrist. Radiographs and CT scans confirm the malalignment.
-
Management:
- Corrective Osteotomy: For symptomatic malunions, a corrective osteotomy with bone grafting (to restore length and correct angulation) and stable internal fixation can be performed. This is a complex procedure.
- Salvage Procedures: If malunion has progressed to significant arthritic changes, PRC or 4CF may be indicated.
4. Infection
- Incidence: Low, typically <1-2% for open reduction and internal fixation.
- Pathogenesis: Contamination during surgery.
- Clinical Presentation: Pain, redness, swelling, warmth, purulent discharge, fever.
-
Management:
- Superficial Infection: Oral antibiotics, local wound care.
- Deep Infection: Surgical débridement, intravenous antibiotics, irrigation, and potentially hardware removal if the infection persists or if the fracture has united.
5. Hardware-Related Complications
- Incidence: Low, but possible.
- Pathogenesis: Incorrect screw placement, screw prominence, screw breakage.
- Clinical Presentation: Pain, tenderness, clicking, limited range of motion, tendon irritation.
-
Management:
- Screw Prominence: If symptomatic (e.g., irritating tendons or articular cartilage), hardware removal may be necessary after union is confirmed.
- Screw Breakage: If the fracture has united, the fragments can be left in place. If nonunion persists, revision surgery with new fixation and bone graft is indicated.
6. Stiffness and Arthritis
- Incidence: Common to some degree after any wrist injury or surgery. Post-traumatic arthritis (SNAC wrist) is a significant long-term complication of nonunion or malunion.
- Pathogenesis: Prolonged immobilization, scar tissue formation, nonunion, malunion leading to altered carpal loading.
- Clinical Presentation: Decreased range of motion, pain, particularly with activity. Radiographs confirm joint space narrowing, osteophytes, and subchondral sclerosis.
-
Management:
- Physiotherapy: Aggressive and prolonged hand therapy is crucial to regain motion and strength.
- Pain Management: NSAIDs, corticosteroid injections (if appropriate).
- Salvage Procedures: For debilitating end-stage arthritis, procedures like PRC, 4CF, or total wrist arthrodesis are considered.
Summary Table: Common Complications & Management
| Complication | Incidence (%) | Pathogenesis | Clinical Presentation | Salvage Strategies |
|---|---|---|---|---|
| Nonunion | 5-40 (operative-conservative) | Inadequate reduction/fixation, vascular compromise, smoking | Persistent pain, snuffbox tenderness, limited ROM, radiographic nonunion | Revision ORIF + bone graft (vascularized if AVN), PRC, 4CF, Wrist Arthrodesis |
| Avascular Necrosis (AVN) | 10-30 (proximal pole) | Disrupted retrograde blood supply | Delayed/nonunion, proximal pole sclerosis/collapse, pain | Vascularized bone graft (early), PRC, 4CF (late) |
| Malunion | Varies (unspecified) | Inadequate reduction/fixation, early weight-bearing | Pain, decreased ROM, altered carpal kinematics, SNAC wrist risk | Corrective osteotomy + bone graft, PRC, 4CF |
| Infection | <1-2 | Surgical contamination | Pain, swelling, erythema, discharge, fever | Débridement, IV antibiotics, hardware removal (if united/persistent) |
| Hardware Complications | Low | Incorrect placement, prominence, breakage | Pain, tendon irritation, impingement, clicking | Hardware removal (if symptomatic), revision fixation |
| Stiffness/Arthritis | Common | Prolonged immobilization, nonunion/malunion, scarring | Decreased ROM, pain with activity, radiographic arthritis | Aggressive PT, pain management, PRC, 4CF, Wrist Arthrodesis |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for achieving optimal functional recovery and minimizing stiffness while ensuring fracture union. Protocols vary based on fracture stability, fixation achieved, and surgeon preference. The general principles involve controlled motion, gradual strengthening, and protection of the healing fracture.
Phase 1: Immobilization and Protection (0-6 weeks)
- Immobilization: A short arm thumb spica cast or a removable splint is typically applied. If highly stable fixation is achieved (e.g., cannulated screw with excellent compression), some surgeons may opt for a shorter period of cast immobilization followed by a removable splint.
- Goals: Protect the surgical site, prevent displacement, reduce pain and swelling.
-
Activities:
- Elevation: Keep the hand elevated above the heart to minimize swelling.
- Ice: Apply ice packs to the wrist (over the cast/dressing) for 15-20 minutes, several times a day.
- Finger ROM: Encourage active range of motion (flexion and extension) of the uninvolved fingers, thumb IP joint, and elbow/shoulder to prevent stiffness.
- Pain Management: Prescribe appropriate analgesics.
- Weight Bearing: No weight bearing or strenuous activity involving the wrist.
- Radiographic Assessment: Initial post-operative X-rays to confirm screw position and reduction. Follow-up X-rays at 2-4 weeks to check for early signs of healing or hardware issues. CT scan may be performed at 6-8 weeks to assess early union.
Phase 2: Controlled Mobilization (6-12 weeks)
- Initiation: Commences once radiographic evidence of early healing (e.g., bridging callus, absence of fracture line widening) is present, and pain is well controlled. This often requires a CT scan to confirm early union.
- Goals: Gradually restore wrist range of motion, improve grip strength, and reduce stiffness.
-
Activities:
- Splinting: Transition to a custom-molded or off-the-shelf removable thumb spica splint for protection during activities, especially outside of therapy. The splint is removed for exercises.
- Gentle Active ROM: Begin with active, pain-free wrist flexion, extension, radial deviation, and ulnar deviation exercises. Avoid excessive force or stress at the fracture site.
- Passive ROM: Gentle passive range of motion exercises may be introduced by a hand therapist.
- Forearm Pronation/Supination: Initiate active and passive forearm rotation.
- Scar Management: Begin scar massage to prevent adhesions.
- Isometric Strengthening: Gentle isometric exercises for the wrist flexors and extensors, and intrinsic hand muscles.
- Light Grip Strengthening: Begin with soft putty or a sponge.
- Weight Bearing: Still no active weight-bearing or heavy lifting.
- Radiographic Assessment: Regular X-rays every 4-6 weeks to monitor union. CT scan at 10-12 weeks if union is still uncertain.
Phase 3: Progressive Strengthening and Return to Activity (12 weeks - 6+ months)
- Initiation: Based on clinical assessment of pain-free range of motion, increasing strength, and definitive radiographic union (often confirmed by CT).
- Goals: Restore full strength and endurance, functional range of motion, and prepare for return to full activities, including sports.
-
Activities:
- Progressive Resistive Exercises: Gradually advance resistance exercises for wrist and hand, including grip strengthening (theraband, hand grippers, weights).
- Proprioceptive Exercises: Balance and coordination activities (e.g., dynamic ball exercises).
- Functional Training: Incorporate activity-specific tasks and simulated work/sport activities.
- Aerobic Conditioning: Maintain general fitness.
- Weight Bearing: Gradual return to weight-bearing activities.
-
Return to Sport/Work:
- Light activities can typically resume around 3-4 months post-operatively if union is solid.
- Heavy lifting, contact sports, or activities involving repetitive wrist loading are generally permitted only after complete, painless union, usually at 4-6 months or even longer, depending on the demands of the activity and individual healing.
- Final clearance for full unrestricted activity should be based on clinical and radiographic evidence of complete union, full pain-free ROM, and adequate strength.
Key considerations:
*
Smoking Cessation:
Crucial for union. Patients should be strongly advised to cease smoking pre- and post-operatively.
*
Compliance:
Patient adherence to the rehabilitation program is critical for successful outcomes.
*
Customization:
Rehabilitation protocols should be individualized based on the patient's progress, fracture characteristics, and any developing complications.
Summary of Key Literature / Guidelines
The management of scaphoid fractures has evolved significantly over the past decades, driven by advancements in imaging, surgical techniques, and a deeper understanding of scaphoid biomechanics and vascularity. Key literature and guidelines generally emphasize accurate diagnosis, early intervention for unstable fractures, and meticulous surgical technique to prevent complications.
Diagnostic Evolution
-
CT Scan as Gold Standard:
Modern literature consistently highlights the superiority of fine-cut CT scanning over plain radiographs for precise diagnosis of displacement, angulation, comminution, and early signs of nonunion or AVN. This diagnostic accuracy directly impacts surgical planning.
- Reference: Gelberman et al. (1981) detailed the vascularity of the scaphoid, providing the anatomical basis for understanding AVN.
- Role of MRI: MRI remains critical for occult fractures and for detailed assessment of AVN and associated ligamentous injuries, complementing CT findings.
Surgical vs. Non-operative Management
-
Shift Towards Earlier Surgery:
There is a growing consensus in the literature, particularly from large systematic reviews and meta-analyses, that operative fixation of displaced or unstable scaphoid waist fractures leads to higher union rates, faster union, and an earlier return to work/activity compared to prolonged cast immobilization. While non-operative treatment can be successful for truly nondisplaced fractures, the threshold for surgery has lowered.
- Reference: Herbert and Fisher (1984) introduced the Herbert screw and a classification system, significantly influencing surgical management. Many subsequent studies have evaluated the effectiveness of headless compression screws.
- Nondisplaced Waist Fractures: The management of truly nondisplaced scaphoid waist fractures remains an area of ongoing debate. While some studies suggest comparable union rates between operative and non-operative groups, operative fixation consistently demonstrates shorter time to union and reduced duration of immobilization.
Surgical Techniques and Fixation
- Headless Compression Screws: Headless cannulated compression screws have become the standard of care for scaphoid fixation, providing interfragmentary compression and allowing for buried hardware.
- Volar vs. Dorsal Approach: The choice of approach (volar or dorsal) is guided by fracture location, displacement pattern, and need for bone grafting. Current literature supports the tailored use of each approach based on these factors.
-
Bone Grafting:
Non-vascularized bone grafts remain the primary option for nonunions without significant AVN. Vascularized bone grafts, notably the 1,2 ICSRA graft, have demonstrated superior outcomes for established AVN of the proximal pole or recalcitrant nonunions.
- Reference: Many studies by Slade, Mathoulin, and others have refined and reported on vascularized bone grafting techniques.
- Arthroscopy-Assisted Surgery: Growing evidence supports the utility of arthroscopy-assisted reduction and fixation, particularly for minimally displaced fractures, allowing for direct visualization of articular surfaces and concomitant ligamentous injuries, potentially reducing morbidity.
Prevention of Complications
- Anatomic Reduction: The literature consistently emphasizes that achieving and maintaining anatomic reduction is the most critical factor in preventing malunion and subsequent SNAC wrist.
- Stable Fixation: Biomechanical studies and clinical outcomes underscore the importance of stable fixation to allow for early mobilization and promote union.
- Smoking Cessation: Numerous studies confirm that smoking significantly impairs bone healing and increases nonunion rates. Aggressive patient education and counseling on smoking cessation are vital.
Guidelines
Major orthopedic societies, such as the American Academy of Orthopaedic Surgeons (AAOS), provide clinical practice guidelines that often reflect these general principles, advocating for accurate diagnosis (including advanced imaging), considering early surgical intervention for displaced or unstable fractures, and emphasizing the importance of specialized hand therapy.
In conclusion, mastering the management of scaphoid fractures requires a comprehensive understanding of its complex anatomy, meticulous pre-operative planning utilizing advanced imaging, precise surgical execution focused on anatomical reduction and stable fixation, and structured post-operative rehabilitation. The overarching goal is to avoid the devastating long-term complications of nonunion, malunion, and carpal collapse, thereby preserving wrist function and quality of life for the patient. Continuous engagement with evolving literature and adherence to evidence-based practices are essential for optimal outcomes.
You Might Also Like