High-Pressure Injection Hand Injuries: Pathophysiology, Anatomy, and Preventing DIP Joint Contracture
Key Takeaway
DIP joint contracture after high-pressure hand injuries (HPII) results from chemical irritation, tissue necrosis, and aggressive fibroproliferative responses. Preventing this severe complication requires a thorough understanding of DIP joint surgical anatomy and biomechanics, guiding early intervention to maintain range of motion and preserve critical hand function.
Preventing DIP Joint Contracture After High-Pressure Hand Injury
Introduction & Epidemiology
High-pressure injection injuries (HPII) of the hand represent a devastating and deceptive clinical entity. Despite often presenting with a deceptively small puncture wound, the underlying damage is typically extensive, ranging from localized tissue destruction to widespread chemical cellulitis, acute inflammatory response, and eventual fibrosis leading to severe functional impairment. The distal interphalangeal (DIP) joint is particularly vulnerable to contracture following these injuries due to its complex anatomy, critical role in fine motor control, and the aggressive fibroproliferative response often seen in the surrounding tissues.
Commonly encountered agents include paint, grease, hydraulic fluid, diesel fuel, and various solvents. The pressure at the nozzle typically ranges from 2,000 to 10,000 pounds per square inch (psi), enabling the injected substance to penetrate deep into fascial planes, tendon sheaths, neurovascular bundles, and even joint capsules, often propagating proximally along the path of least resistance. The severity of injury is directly related to the type of injectate, the volume injected, the pressure, the anatomical location, and, critically, the time elapsed between injury and surgical intervention. Non-toxic substances generally cause less severe reactions than toxic ones, with paint and paint thinner mixtures being among the most destructive due to their inflammatory and necrotic properties.
Epidemiologically, HPIIs are relatively uncommon but carry a high rate of morbidity. The hand is involved in approximately 60-80% of cases, with the non-dominant index finger being the most frequently affected digit, followed by the thumb and middle finger. The typical patient is a male industrial worker aged 30-50 years. Delayed presentation, often due to the initial innocuous appearance of the injury, is common and significantly correlates with poorer outcomes, including higher rates of infection, necrosis, amputation, and long-term joint stiffness and contracture. Preventing DIP joint contracture is a primary therapeutic goal, as its development severely compromises the delicate functional integrity of the hand, impacting both pinch and grasp.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the DIP joint and surrounding structures is fundamental to both the surgical management of HPII and the prevention of subsequent contracture.
DIP Joint Anatomy
The DIP joint is a uniaxial hinge joint primarily permitting flexion and extension.
*
Bony Architecture:
Formed by the head of the middle phalanx and the base of the distal phalanx. The articular surfaces are congruent, with the head of the middle phalanx featuring two condyles fitting into reciprocal concavities on the distal phalanx.
*
Joint Capsule:
A thin, fibrous capsule encloses the joint. It is reinforced by various ligamentous structures.
*
Volar Plate:
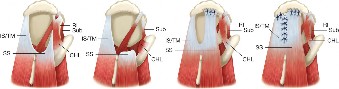
A dense, fibrocartilaginous structure on the palmar aspect of the joint. It acts to prevent hyperextension and is firmly attached to the distal phalanx base, with a looser attachment proximally to the middle phalanx neck, allowing it to fold during flexion. Its integrity is crucial for joint stability and preventing hyperextension deformities. In HPII, it can become infiltrated, scarred, and shortened, leading to flexion contracture.
*
Collateral Ligaments:
Paired true and accessory collateral ligaments provide primary stability, preventing varus/valgus deviation. The true collateral ligaments originate from the middle phalanx condyles and insert on the base of the distal phalanx. They are taut in flexion and relaxed in extension. The accessory collateral ligaments originate more volarly and insert onto the volar plate. Injection material can infiltrate these ligaments, leading to fibrosis and shortening, restricting motion.
*
Extensor Mechanism:
The extensor digitorum communis (EDC) tendon divides into a central slip and two lateral bands. At the DIP joint, the lateral bands converge to form the terminal tendon (also known as the conjoint tendon) which inserts onto the dorsal base of the distal phalanx, mediating DIP joint extension. The oblique retinacular ligament (ORL) runs from the flexor sheath on the proximal phalanx to the terminal extensor tendon, coupling DIP and PIP joint motion. Damage or scarring to the terminal extensor tendon or surrounding soft tissues can result in an extension lag or, conversely, an extension contracture if the dorsal capsule or skin scars.
*
Flexor Mechanism:
The flexor digitorum profundus (FDP) tendon inserts into the volar base of the distal phalanx, providing primary DIP joint flexion. It courses through the fibrous flexor sheath (A5 pulley specifically covers the DIP joint). The integrity of the FDP tendon and its gliding mechanism within the sheath is paramount for DIP joint function. Injected material can track along the tendon sheath, causing chemical tenosynovitis, adhesions, and eventually FDP tendon tethering and severe flexion contracture.
*
Neurovascular Bundles:
The digital nerves and arteries run along the mid-axial lines of the digits, superficial to the flexor sheath, and are highly susceptible to direct injury from the injection or secondary damage from chemical irritation, inflammation, and compartment syndrome.
Biomechanics of Contracture Development
Contracture development after HPII is multifactorial:
1.
Chemical Synovitis and Tenosynovitis:
The injected material, particularly organic solvents and paint, induces a profound inflammatory response, leading to chemical irritation of the synovium, tendon sheaths, and joint capsule. This initiates a fibroproliferative cascade.
2.
Tissue Necrosis and Fibrosis:
Ischemia, direct chemical toxicity, and secondary infection result in tissue necrosis. The subsequent healing involves extensive scar formation. Scar tissue is inherently less elastic and prone to shortening.
3.
Adhesions:
The FDP tendon and extensor mechanism can become adherent to the surrounding soft tissues, joint capsule, and bone, effectively tethering the joint in a fixed position. The flexor sheath is a common site for adhesions, leading to severe flexion contracture.
4.
Capsular Thickening and Shortening:
The joint capsule and collateral ligaments can thicken and contract, restricting normal arthrokinematics.
5.
Ischemia and Compartment Syndrome:
Rapid spread of injected material and subsequent edema can lead to elevated compartmental pressures, compromising microcirculation and exacerbating tissue necrosis.
6.
Delayed Mobilization:
Post-operative pain, wound issues, and fear of injury can lead to prolonged immobilization, further contributing to stiffness and contracture.
The most common DIP joint contracture after HPII is flexion contracture, largely due to FDP tethering and volar plate/collateral ligament scarring. Extension contractures are less common but can occur from dorsal skin and capsular scarring or extensor mechanism tethering.
Indications & Contraindications
Management of HPII is primarily surgical, recognizing the severe and progressive nature of the injury. There are virtually no absolute contraindications to immediate surgical exploration for high-pressure injection injuries themselves. However, indications for specific interventions for contracture prevention or treatment, and relative contraindications, warrant discussion.
Indications for Surgical Intervention
1. Primary Surgical Debridement for HPII (Urgent/Emergent):
*
All suspected or confirmed high-pressure injection injuries:
This is the universal indication. Early surgical intervention (ideally within 6 hours) is critical to mitigate the spread of foreign material, reduce the chemical inflammatory response, and minimize tissue necrosis and subsequent fibrosis, thereby directly impacting the risk of contracture.
*
Presence of pain, swelling, discolouration, crepitus, impaired sensation:
These are signs of advanced injury and mandate immediate intervention.
*
Absence of obvious symptoms:
Even in asymptomatic cases with a clear history of HPII, surgical exploration is indicated due to the deceptive nature of the injury and the high risk of delayed necrosis.
2. Secondary Surgical Interventions for DIP Joint Contracture (Elective/Semi-Elective):
*
Progressive or established DIP joint flexion or extension contracture:
If conservative measures (e.g., intensive hand therapy, splinting, serial casting) fail to restore functional range of motion (typically defined as less than 30 degrees of contracture for the DIP joint to be functional).
*
Persistent functional deficit:
Significant impairment in activities of daily living, pinch strength, or grasp due to limited DIP joint motion.
*
Radiographic evidence of joint fusion or significant degenerative changes:
Arthrodesis or arthroplasty may be considered for salvage.
*
Persistent pain and stiffness:
Due to intractable tendon adhesions or capsular fibrosis despite exhaustive non-operative management.
Contraindications
1. Primary HPII Debridement:
*
No absolute contraindications.
Relative contraindications relate to patient stability.
*
Patient instability:
Severe systemic medical comorbidities precluding anesthesia may necessitate temporizing measures until stabilization, though this is rare given the limb-threatening nature of HPII.
*
Moribund patient:
Extremely rare context, where the injury is overshadowed by life-threatening systemic issues.
2. Secondary Surgical Interventions for Established Contracture:
*
Active infection:
Must be resolved prior to elective soft tissue release or arthrolysis.
*
Poor general medical health:
Uncontrolled comorbidities that significantly increase surgical risk without substantial anticipated functional gain.
*
Unrealistic patient expectations:
Critical to ensure patient understanding of potential outcomes, which can be limited despite extensive surgery, especially in the context of severe initial injury.
*
Ongoing tissue necrosis or unstable wounds:
Secondary procedures require stable, healed soft tissues.
*
Insufficient commitment to post-operative rehabilitation:
The success of contracture release surgery is heavily reliant on rigorous and prolonged hand therapy.
Operative vs. Non-Operative Indications
| Feature | Operative Indication | Non-Operative Indication |
|---|---|---|
| Initial HPII Management | All suspected or confirmed high-pressure injection injuries. | None. All HPII require immediate surgical exploration. |
| Established Contracture | Failure of intensive non-operative therapy (typically >3-6 months). | Early/mild contracture (<30 deg loss of motion), initial post-op phase, patients unwilling or unfit for surgery. |
| Functional Impact | Significant impairment of pinch, grasp, or ADLs. | Mild or tolerable functional limitation. |
| Pain | Severe, intractable pain associated with stiffness. | Manageable pain with conservative measures. |
| Tissue Status | Stable, healed wounds; no active infection. | Active infection; unstable wounds; ongoing tissue necrosis. |
| Patient Commitment | High commitment to demanding post-operative therapy. | Limited compliance or ability for intense therapy. |
| Specific Procedures | Tenolysis, capsulotomy, arthrolysis, skin grafts/flaps. | Hand therapy, dynamic/static progressive splinting, serial casting, scar management. |
| Goal | Restore functional ROM, reduce pain, improve function. | Prevent progression, maintain existing ROM, manage symptoms. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is paramount for HPII, given its complexity and the potential for devastating outcomes.
Diagnostic Workup
- History: Detailed account of the injury, including type of injectate, pressure, site, and time since injury. Initial symptoms and any treatments received.
- Physical Examination: Assess skin integrity, swelling, discoloration, crepitus, tenderness, neurovascular status (two-point discrimination, capillary refill, motor function), and active/passive range of motion if possible. Document the extent of involvement.
-
Imaging:
- X-rays: Essential to identify injected material (e.g., paint, grease often appear radiopaque), bony involvement (fractures, osteomyelitis), and the presence of gas. Baseline X-rays are crucial for future comparisons.
- MRI: Can delineate soft tissue involvement, tendon sheath tracking, and extent of chemical synovitis or necrosis. May be considered if diagnosis is uncertain or to guide extent of debridement in complex cases, but should not delay urgent surgery.
Patient Assessment & Preparation
- Systemic Evaluation: Address comorbidities. Ensure tetanus prophylaxis is up-to-date.
- Antibiotics: Broad-spectrum intravenous antibiotics (e.g., a cephalosporin plus an aminoglycoside or metronidazole if anaerobic contamination is suspected) should be administered immediately and continued post-operatively, tailored to culture results.
- Informed Consent: Comprehensive discussion with the patient regarding the severity of the injury, potential need for staged procedures, the high risk of infection, necrosis, amputation, long-term stiffness, and the unpredictable functional outcome. Realistic expectations must be set.
- Blood Products: Type and cross-match for potential transfusions, especially if extensive debridement or skin coverage is anticipated.
Anesthesia
- Regional Anesthesia: Axillary or supraclavicular block is often preferred, providing excellent analgesia and sympathetic blockade, which may improve digital perfusion.
- General Anesthesia: May be used, particularly for prolonged cases or if a regional block is not feasible. Ensure muscle relaxation for optimal exposure.
Patient Positioning
- Supine Position: Patient is positioned supine on the operating table.
- Hand Table: The affected upper extremity is placed on a radiolucent hand table.
- Tourniquet: A pneumatic tourniquet is applied to the upper arm. The limb should be exsanguinated (Esmarch bandage) prior to inflation to optimize visualization. Tourniquet time must be strictly monitored, especially with extensive debridement which may necessitate staged operations or longer tourniquet times.
- Magnification: Surgical loupes (2.5x to 4.5x) are mandatory for detailed dissection and visualization of vital structures. A microscope may be helpful for microsurgical repair if nerve or vessel injuries are identified.
- Instrumentation: Standard hand surgery set, fine dissecting instruments, nerve hooks, vessel loops, pulsatile lavage system, electrocautery.
- Sterile Prep and Drape: The entire limb, from mid-humerus to fingertips, should be prepped and draped to allow for wide exposure and potential harvest of local or regional flaps if needed.
Detailed Surgical Approach / Technique
The surgical management of HPII, particularly with the goal of preventing DIP joint contracture, is a multi-staged process primarily focused on early, aggressive debridement. Secondary procedures for contracture release are performed once the acute inflammatory phase has subsided and tissues are stable.
Principles of Primary Surgical Management (Acute Phase)
- Urgency: Debridement within 6 hours of injury significantly improves outcomes.
- Generosity: Extensive debridement of all foreign material and non-viable tissue.
- Decompression: Release of all fascial compartments to prevent ischemia.
- Irrigation: Copious pulsatile lavage.
- Staged Approach: Leave wounds open, perform serial debridements as needed.
Incisions for Initial Debridement
-
Mid-axial Incisions:
The preferred incision for digital HPII. These incisions are made along the non-weight-bearing surfaces of the digits (e.g., ulnar aspect of the index, middle, ring fingers; radial aspect of the small finger). They extend longitudinally across multiple phalanges as needed to adequately expose all involved compartments.
- Advantages: Provide excellent exposure of the neurovascular bundles, flexor tendon sheath, extensor mechanism, and joint capsules. They minimize damage to the volar skin and preserve dorsal lymphatic drainage. They can be extended into the palm or dorsum if the injectate has spread proximally.
- Fish-mouth (racquet) or Zigzag (Brunner) Incisions: While useful for wide exposure in certain hand injuries, they are generally avoided in acute HPII unless extensive skin necrosis dictates their use, due to the increased risk of skin edge necrosis, scarring, and secondary contractures.
- Exploration of all Infiltrated Areas: The small entry wound often belies the widespread distribution of the injected material. Incisions must be extended until all affected tissues are visualized and debrided. This typically involves opening the entire flexor tendon sheath and exploring beyond.
Step-by-Step Debridement for DIP Joint Involvement
- Tourniquet Inflation: Inflate the tourniquet after exsanguination.
- Skin Incision: Make mid-axial incisions. Elevate skin flaps carefully to expose deeper structures.
- Neurovascular Bundle Isolation: Identify and carefully dissect around the digital nerves and arteries. They are often infiltrated or compressed. Release any surrounding constricting tissue.
- Flexor Tendon Sheath Exploration: Open the entire flexor tendon sheath from the proximal phalanx to the DIP joint. This is critical as injectate commonly tracks within this confined space. Meticulously inspect the FDP tendon and its gliding surfaces. Remove all foreign material, chemical synovitis, and necrotic tissue.
-
DIP Joint Capsule and Ligament Inspection:
- Carefully inspect the volar plate, collateral ligaments, and joint capsule. If injected material is found within the joint, the capsule must be incised (capsulotomy) and the joint thoroughly irrigated and debrided.
- Synovectomy of the DIP joint may be necessary if severe chemical synovitis is present.
- In cases of suspected or observed early contracture, consider prophylactic partial release of the accessory collateral ligaments or volar plate during initial debridement, though this is controversial and usually reserved for later stages. The primary goal is debridement.
- Extensor Mechanism Inspection: Inspect the terminal extensor tendon and lateral bands. Remove any injected material or necrotic tissue. The dorsal aspect of the DIP joint capsule may also be affected.
- Muscle and Subcutaneous Tissue Debridement: Remove all non-viable muscle, fat, and subcutaneous tissue. Viability assessment can be challenging and may require repeat inspection after a few days. Non-viable tissue typically appears pale, grey, friable, or lacks bleeding.
- Copious Irrigation: Use pulsatile lavage with several liters of sterile saline to flush out remaining particulate matter and chemical irritants.
-
Wound Management:
Do
not
primarily close the wounds. Leave them open or perform a loose, delayed primary closure.
- Pack wounds lightly with sterile gauze (wet-to-dry dressings are common).
- Consider vacuum-assisted closure (VAC) if extensive tissue loss or difficulty with dressing changes is anticipated.
- Often, a "second look" operation within 24-48 hours is mandatory to reassess tissue viability and perform further debridement.
Secondary Surgical Management (for Established Contracture)
These procedures are performed after all acute inflammatory processes have resolved, wounds are healed, and intensive hand therapy has failed to improve range of motion.
-
Flexion Contracture:
- Tenolysis of FDP: If the FDP tendon is adherent, an extensive tenolysis is performed through mid-axial incisions, releasing all scar tissue tethering the tendon within its sheath and to surrounding structures. Care is taken to preserve any remaining A pulleys that are functional.
- Volar Plate Release/Capsulotomy: If the volar plate and joint capsule are scarred and shortened, a volar plate release (often requiring resection of a portion) and anterior capsulotomy are performed to restore extension.
- Collateral Ligament Release: Release of the accessory or true collateral ligaments (collaterectomy) may be necessary for severe contractures.
-
Extension Contracture:
- Dorsal Capsulotomy: Release of a scarred and tightened dorsal joint capsule.
- Extensor Tenolysis: Release of adhesions involving the terminal extensor tendon.
- Skin Contracture: If overlying skin scarring is contributing, Z-plasty, local flaps, or skin grafting may be required.
- K-wire Fixation (Post-release): After a successful contracture release (tenolysis, capsulotomy), a temporary Kirschner wire can be used to maintain the corrected position (e.g., full extension for a flexion contracture) for 2-3 weeks, followed immediately by aggressive therapy. However, fixation can also lead to joint stiffness if not managed carefully, and dynamic splinting is often preferred.
- Arthrodesis/Arthroplasty: For severe, intractable contractures with significant joint destruction or pain, DIP joint arthrodesis in a functional position (typically 10-20 degrees of flexion) or, less commonly, arthroplasty (for specific indications) may be considered as a salvage procedure.
Complications & Management
HPII carries a notoriously high complication rate, ranging from minor stiffness to limb-threatening necrosis and amputation. Proactive management and a high index of suspicion are crucial.
Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Salvage / Management Strategy |
|---|---|---|
| Infection | Highly variable, 20-70%, depending on injectate & delay. | Prevention: Early, aggressive debridement; broad-spectrum IV antibiotics; open wound management; serial debridements. Treatment: Culture-directed antibiotics; repeat debridement; removal of foreign bodies; wound cultures; irrigation; local wound care (e.g., VAC); potentially IV-antibiotic beads (rare). |
| Tissue Necrosis / Amputation | 10-60%, depending on injectate (paint highest). | Prevention: Urgent, extensive debridement; decompression of fascial compartments; preservation of viable tissue; avoidance of primary closure; aggressive management of infection. Treatment: Staged debridement of non-viable tissue; revascularization attempts (if vascular compromise is the cause, rare); hyperbaric oxygen therapy (controversial); eventual definitive wound coverage (skin graft, local/regional flap); primary or secondary amputation for unsalvageable digits. |
| DIP Joint Contracture | Very high, 50-90% for significant injuries. | Prevention: Early, aggressive hand therapy; active/passive ROM; dynamic/static progressive splinting; serial casting; scar management. Treatment: Intensive, supervised hand therapy; custom splinting (e.g., Capener splints); serial casting; if refractory: surgical tenolysis, capsulotomy, collateral ligament release; if joint destruction: arthrodesis or arthroplasty (rare). |
| Neuropathy / Sensory Loss | Up to 30%, direct injury or secondary to compression/fibrosis. | Prevention: Careful dissection; meticulous release of neurovascular bundles during debridement. Treatment: Nerve decompression for entrapment; nerve grafting for transection (rare in acute phase); desensitization therapy; patient education regarding protective sensation. |
| Tendon Adhesion / Rupture | High (adhesion), Rupture (less common, but severe). | Prevention: Meticulous debridement of tendon sheath; early, protected active motion. Treatment: Intensive tendon gliding exercises; blocking exercises; if refractory: surgical tenolysis; tendon grafting or transfer for severe rupture (complex). |
| Complex Regional Pain Syndrome (CRPS) | 5-20%. | Prevention: Aggressive pain management; early mobilization; gentle, non-painful therapy; psychological support. Treatment: Multidisciplinary approach: physical/occupational therapy; pain medication (gabapentin, tricyclics, NSAIDs); sympathetic nerve blocks; psychological support; spinal cord stimulator (refractory cases). |
| Chronic Pain | Common, can be debilitating. | Prevention: Optimal early management; aggressive pain control; early rehabilitation. Treatment: Multimodal pain management; nerve blocks; desensitization; physical therapy; psychological counseling; sometimes surgical intervention for specific pain generators (e.g., neuroma excision). |
| Osteomyelitis / Avascular Necrosis | <5-10% (more common with bone involvement or delayed treatment). | Prevention: Thorough debridement of bone, meticulous irrigation, appropriate antibiotics. Treatment: Long-term culture-directed antibiotics; repeat surgical debridement of necrotic bone; possibly bone grafting; amputation for intractable cases. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a cornerstone of preventing DIP joint contracture and restoring function after HPII. It is an intensive, prolonged, and often challenging process that requires close collaboration between the surgeon, hand therapist, and patient. Early, protected motion is key.
Immediate Post-Operative Phase (Days 0-2 weeks)
- Wound Management: Meticulous wound care, often with open dressings changed frequently. Elevation of the hand above the heart to minimize edema.
- Pain Management: Aggressive pain control to facilitate early motion and prevent CRPS.
- Edema Control: Compression gloves/wraps, elevation, gentle retrograde massage.
-
Initial Mobilization:
- Adjacent Joints: Active range of motion (AROM) of uninvolved joints (wrist, MCPs, other digits) begins immediately.
- Affected DIP Joint: If wounds permit and there is no active infection or unstable fixation, very gentle, protected active DIP joint flexion and extension may be initiated within the first few days. This is crucial for preventing tendon adhesions and maintaining joint lubrication. The key is active , not passive, to promote tendon gliding.
- Splinting: Static splinting in a position of safety (wrist extension, MCP flexion, DIP extension) may be used for night wear or for short protective periods, but prolonged immobilization must be avoided. Dynamic extension splinting (e.g., Capener splint) may be initiated early for existing or developing flexion contractures if the wounds are stable.
Intermediate Phase (Weeks 2-6)
- Increased AROM: Progress active DIP flexion and extension, focusing on full excursion.
- Passive Range of Motion (PROM): Gentle, pain-free PROM may be introduced cautiously. Avoid forceful manipulation which can cause re-injury or trigger CRPS.
- Tendon Gliding Exercises: Specific exercises to promote differential gliding of FDP and extensor tendons.
- Blocking Exercises: Isolate DIP joint motion by stabilizing the PIP joint.
-
Progressive Splinting:
- Dynamic Splinting: Continue dynamic extension splinting for flexion contractures, with adjustable outriggers to apply gentle, constant stretch.
- Static Progressive Splinting: Utilize splints that allow for gradual, incremental adjustments to increase the stretch on the contracted structures. These are often worn for prolonged periods, especially at night.
- Serial Casting: For significant, refractory contractures, serial casting involves applying a cast that holds the joint in a maximally corrected position, which is then removed and reapplied every few days or weeks to progressively gain range.
- Scar Management: Deep tissue massage, silicone gel sheeting, and compression garments to soften scar tissue and prevent hypertrophic scarring.
- Strengthening: Gentle intrinsic muscle strengthening as tolerated.
Advanced Phase (Weeks 6-beyond)
- Progressive Resistive Exercises: Gradually increase resistance for strengthening of grip, pinch, and individual finger motions.
- Functional Activities: Incorporate occupation-specific or daily living activities to integrate improved range of motion and strength into functional tasks.
- Desensitization: For patients with nerve injuries or hypersensitivity, desensitization techniques are employed.
- Continued Splinting: Night splinting and use of dynamic/static progressive splints during periods of rest often continue for many months to prevent contracture recurrence.
- Return to Work/Sport: Gradual return, guided by functional assessments.
Key Principles for DIP Joint Contracture Prevention
- Early Mobilization: The single most important factor. Active, protected motion of the DIP joint should be initiated as soon as surgical stability and wound healing permit.
- Specific Joint Isolation: Blocking exercises are essential to ensure the DIP joint is actively moving, rather than compensating from more proximal joints.
- Sustained Low-Load Stretch: Dynamic and static progressive splinting applies a prolonged, gentle stretch to contracted tissues, which is more effective than forceful, brief stretches in remodeling scar tissue.
- Patient Adherence: The success of rehabilitation is highly dependent on the patient's commitment to a rigorous home exercise program and splint wear.
- Multi-Modal Approach: Combining exercises, splinting, scar management, and pain control is crucial.
Rehabilitation can last for many months, often extending to a year or more. Realistic expectations regarding functional recovery, even with optimal therapy, must be maintained.
Summary of Key Literature / Guidelines
The literature on high-pressure injection injuries consistently emphasizes the critical importance of early and aggressive surgical intervention to mitigate tissue damage and prevent long-term sequelae, including DIP joint contracture.
1. Early Surgical Debridement:
*
Consensus:
There is overwhelming consensus across hand surgery literature that all HPIIs are surgical emergencies requiring prompt and thorough debridement. Numerous studies (e.g., Pinto et al., 1999; Hogan & Ruland, 2006; Lewis et al., 1999) highlight a direct correlation between delay to surgery (especially >6-10 hours) and increased rates of infection, necrosis, amputation, and poor functional outcomes. The chemical nature of the injury mandates washout and removal of the foreign substance.
*
Extent of Debridement:
While aggressive debridement is essential, the debate centers on its maximal extent. Some advocate for prophylactic wide debridement of all potentially involved tissue (even if viable appearing), while others prefer a more targeted approach with serial re-evaluation. However, for substances like paint, aggressive debridement is generally preferred due to their high toxicity and inflammatory potential. The goal is to remove all injected material and non-viable tissue while preserving vital structures.
2. Type of Injectate:
* Literature consistently demonstrates that paint and paint thinner mixtures are the most damaging, leading to the highest rates of amputation and contracture. Water, air, and some solvents cause less severe reactions but still require prompt intervention. The chemical properties of the injectate directly influence the severity of the inflammatory response, tissue necrosis, and subsequent fibrosis, which are direct precursors to contracture.
3. Role of Adjunctive Therapies:
*
Corticosteroids:
The use of corticosteroids (oral or local) remains controversial. Some studies suggest they may attenuate the inflammatory response and reduce fibrosis, particularly in non-infectious cases with agents like paint. Others warn against their use due to potential immunosuppression and masking of infection. Current guidelines generally do not recommend routine prophylactic corticosteroids, but they may be considered on a case-by-case basis by experienced surgeons.
*
Hyperbaric Oxygen Therapy (HBO):
HBO is theorized to improve tissue oxygenation, reduce edema, and enhance wound healing. While some case reports and small series suggest benefit in HPII, particularly for tissue salvage, large-scale randomized controlled trials are lacking. Its use is not universally recommended and should be considered an adjunct, not a substitute, for surgery.
*
Antibiotics:
Prophylactic broad-spectrum antibiotics are universally recommended due to the high risk of infection, often started pre-operatively and continued post-operatively, guided by culture results.
4. Post-Operative Rehabilitation:
* The literature strongly supports intensive and prolonged hand therapy as critical for preventing contracture and optimizing function. Studies by Brand and Hollister (1999), and later authors, emphasize the importance of early, protected active motion, dynamic splinting, and serial casting for contracture management. Prolonged immobilization is cited as a major contributor to stiffness and contracture development. Patient adherence to therapy protocols is a significant predictor of functional outcome.
5. Contracture Management:
* For established DIP joint contractures, surgical interventions such as tenolysis, capsulotomy, and collateral ligament release are described as effective but require meticulous technique and are typically performed after a period of failed conservative management. The timing of these secondary procedures is crucial, often deferred until the acute inflammatory phase has completely subsided and tissues are quiescent, typically several weeks to months post-injury. The outcomes of these procedures are directly linked to the intensity of post-operative therapy.
6. Amputation Rates:
* Amputation rates vary widely (10-60%) depending on the injectate, delay to treatment, and severity of initial injury. Paint injuries consistently show higher amputation rates. This highlights the severity and destructive nature of these injuries.
Future Directions: Research continues to focus on improving tissue viability assessment during debridement, developing more effective anti-fibrotic agents, and refining rehabilitation protocols. Advances in imaging may allow for earlier and more precise delineation of the injectate spread, guiding more targeted surgical interventions. However, the fundamental principles of rapid diagnosis, urgent, aggressive surgical debridement, and intensive rehabilitation remain the cornerstones of management for HPII and the prevention of disabling DIP joint contractures.
You Might Also Like