Volar Wrist Ganglion: Epidemiology, Surgical Anatomy, & Management Guide
Key Takeaway
Volar wrist ganglions are benign cysts, the second most common wrist soft tissue tumor, often causing cosmetic issues, pain, or functional limitations. They arise from the anterior wrist capsule, frequently near the scapholunate or radioscaphocapitate ligaments. Etiology involves synovial herniation or microtrauma, requiring careful attention to critical neurovascular structures like the radial artery during management.
Introduction & Epidemiology
Volar wrist ganglions represent the second most prevalent soft tissue tumor of the wrist, superseded only by their dorsal counterparts. While universally benign, these cysts frequently present with cosmetic concerns, palpable masses, and, in a subset of patients, pain or functional limitations. They typically arise from the anterior aspect of the wrist capsule, most commonly associated with the scapholunate (SL) ligament or the radioscaphocapitate (RSC) ligament complex.
Epidemiologically, wrist ganglions affect individuals across all age groups but exhibit a peak incidence in young to middle-aged adults, commonly within the second to fourth decades of life. A slight female predominance is consistently observed in most series. The precise etiology remains a subject of ongoing debate; however, prevailing theories suggest a multifactorial origin involving synovial herniation through a capsular defect, repetitive microtrauma, or mucoid degeneration of underlying capsular or ligamentous structures. Histologically, these lesions are characterized by a fibrous capsule containing a viscous, clear, gelatinous fluid rich in hyaluronic acid, and are invariably connected to the underlying joint capsule by a discrete stalk, most frequently originating from the radiocarpal joint. Volar ganglions account for approximately 15-20% of all wrist ganglions, with those located radially being the most common volar presentation.
Surgical Anatomy & Biomechanics
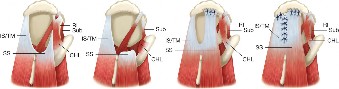
A profound understanding of the intricate anatomy of the volar wrist is paramount for the safe and effective surgical excision of volar wrist ganglions. The proximity of critical neurovascular structures mandates meticulous identification and protection throughout the procedure.
Anatomical Landmarks & Structures to Protect:
- Radial Artery: This represents the single most critical structure to identify and meticulously protect during volar wrist ganglion excision. Volar ganglions commonly present on the radial side of the palmar wrist, frequently lying directly adjacent to, or occasionally even superficial to, the radial artery. The artery typically courses between the flexor carpi radialis (FCR) tendon and the brachioradialis muscle distally, subsequently crossing the radial aspect of the wrist capsule. Pre-operative and intra-operative pulsed identification and direct visualization of the radial artery are imperative. A large ganglion may cause significant displacement of the artery, or the artery may be intimately draped over the ganglion's surface.
- Flexor Carpi Radialis (FCR) Tendon: The FCR tendon serves as a crucial and consistent anatomical landmark. Volar ganglions most commonly emerge between the FCR tendon and the radial artery. This tendon provides a reliable guide to the underlying wrist capsule and assists in localizing the ganglion’s deep stalk.
- Palmar Cutaneous Branch of the Median Nerve: This sensory nerve typically originates from the radial side of the median nerve in the distal forearm, approximately 5-7 cm proximal to the wrist crease. It then courses superficially, often crossing over the flexor retinaculum, to provide sensation to the radial palm. Due to its superficial course and variable anatomy, it is highly susceptible to iatrogenic injury during skin incision and initial subcutaneous dissection, potentially leading to painful neuroma formation or chronic dysesthesia within its sensory distribution.
- Superficial Radial Nerve (SRN) Branches: While less commonly directly involved in volar wrist ganglion excision compared to dorsal approaches, distal branches of the SRN can be at risk, particularly if the surgical field extends excessively radially or distally, or if incisions are not precisely planned. These branches are responsible for providing sensation to the radial dorsum of the hand and thumb.
- Median Nerve Proper: The main trunk of the median nerve lies deep to the palmaris longus tendon (when present) and the FCR tendon, situated directly beneath the flexor retinaculum. Although typically not in direct contiguity with a volar ganglion, careful and precise dissection around the FCR tendon is essential to avoid inadvertent injury to the median nerve itself.
- Palmaris Longus Tendon: Present in approximately 85% of individuals, the palmaris longus tendon offers another useful superficial anatomical landmark, typically positioned just ulnar to the FCR tendon. It overlies and provides some protection to the median nerve.
- Scapholunate (SL) Ligament & Radioscaphocapitate (RSC) Ligament: These are the most frequent points of origin for the ganglion stalk. The stalk represents the crucial anatomical connection between the ganglion and the underlying wrist joint capsule. A definitive surgical excision mandates thorough resection of this stalk along with a small cuff of the surrounding capsule to minimize the risk of recurrence. Volar ganglions most frequently arise from the volar aspect of the SL ligament or the RSC ligament, often extending towards the radial styloid.
Biomechanics:
The pathogenesis of volar wrist ganglions is hypothesized to be related to areas of capsular weakness or chronic repetitive stress. The characteristic viscous fluid within the ganglion is produced by synovial cells that generate hyaluronic acid. The "one-way valve" theory postulates that synovial fluid is extruded from the joint through a capsular defect during specific wrist motions but is subsequently unable to freely flow back into the joint, leading to gradual accumulation and progressive cyst expansion. Activities involving repetitive wrist flexion and extension may exacerbate this proposed mechanism. Biomechanically, these areas of capsular vulnerability are frequently located near the confluence of multiple wrist ligaments, particularly around the radiocarpal joint.
Indications & Contraindications
The therapeutic decision-making process for volar wrist ganglions involves a careful consideration of patient symptoms, functional impact, and the inherent potential for spontaneous resolution versus the risks and benefits of surgical intervention.
Non-Operative Indications:
- Asymptomatic mass: A significant proportion of ganglions are discovered incidentally and cause no pain, functional limitation, or cosmetic concern. In such instances, observation with reassurance is the primary recommendation.
- Mild, intermittent pain: Patients experiencing minimal discomfort, particularly if activity-related and manageable with activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), or over-the-counter analgesics.
- First-line treatment strategy: Initial management typically involves a period of observation, often combined with a trial of splinting or activity modification, given the natural history of potential spontaneous resolution.
- Diagnostic uncertainty (initial phase): If the precise nature of the mass is not definitively a benign ganglion, but immediate surgical exploration is not warranted, initial observation with serial imaging may be appropriate.
- Patient preference: For patients who express a strong desire to avoid surgery or are not significantly bothered by the mass, conservative management is appropriate.
- Aspiration and injection: While known to have a higher recurrence rate compared to surgical excision, aspiration of the ganglion (often followed by corticosteroid injection) can be considered, particularly for smaller, symptomatic cysts. It can offer temporary symptomatic relief and serves to confirm the cystic nature of the mass. Success rates for aspiration alone typically range from 30-70%.
Operative Indications:
- Persistent or severe pain: When pain is debilitating, unremitting, unresponsive to adequate non-operative measures, or significantly impacts daily activities, occupational function, or sleep quality.
- Neurological symptoms: Documented compression of adjacent peripheral nerves (e.g., palmar cutaneous branch of median nerve) leading to paresthesias, dysesthesia, numbness, or motor weakness (though nerve compression causing motor weakness is exceedingly rare for volar ganglions).
- Vascular compromise: Although extremely rare, exceptionally large ganglions may theoretically compress the radial artery, potentially leading to distal ischemic symptoms. A positive pre-operative Allen's test in conjunction with clinical symptoms supports this indication.
- Functional limitation: Physical impingement during wrist motion, quantifiable reduction in grip strength, or interference with the wearing of gloves, braces, or occupational equipment.
- Cosmetic concern: Significant aesthetic distress to the patient, particularly if the mass is prominent or perceived as disfiguring.
- Recurrence after aspiration: Documented recurrence following one or more attempts at non-operative aspiration.
- Uncertain diagnosis: If clinical examination and advanced imaging (ultrasound, MRI) do not definitively confirm a benign ganglion, and there is suspicion of alternative soft tissue tumors (e.g., lipoma, giant cell tumor of tendon sheath, hemangioma, schwannoma) or malignancy, diagnostic excision is indicated.
Contraindications:
- Active local infection: Surgical intervention should be absolutely deferred until any active local infection is completely resolved to prevent wound complications, deep space infection, and potential systemic sequelae.
- Uncontrolled systemic comorbidities: Patients with poorly controlled systemic conditions such as diabetes mellitus, significant cardiovascular disease, or unmanaged coagulopathies present increased surgical risks. These conditions must be optimally managed and stabilized pre-operatively.
- Patient unwillingness: Absolute refusal of surgical intervention by an adequately informed patient.
- Unrealistic expectations: Patients must possess a clear and realistic understanding of the potential benefits, inherent risks (recurrence, nerve injury, radial artery injury, scar sensitivity, infection, stiffness), and expected recovery timeline.
- Spontaneous resolution: Given that a significant percentage of ganglions (up to 50%) can resolve spontaneously without intervention, initial observation is often a prudent strategy, particularly for asymptomatic or minimally symptomatic lesions.
Summary of Operative vs. Non-Operative Indications:
| Indication Type | Non-Operative Management | Operative Management |
|---|---|---|
| Symptoms | Asymptomatic mass | Persistent or severe pain |
| Mild, intermittent pain | Neurological symptoms (paresthesias, dysesthesia, numbness) | |
| Vascular compression (rare, with objective signs of ischemia) | ||
| Functional Impairment | No functional limitation | Functional impairment (e.g., restricted ROM, reduced grip strength) |
| Treatment History | Initial presentation, no prior interventions | Recurrence after aspiration/previous non-operative failures |
| Cosmetic Concern | Minor or no cosmetic concern | Significant cosmetic distress impacting quality of life |
| Diagnostic Clarity | Clear diagnosis of benign ganglion, no atypical features | Diagnostic uncertainty, suspicion of other tumor types/malignancy |
| Patient Health | Presence of active infection, uncontrolled systemic comorbidities (temporarily contraindicates surgery) | Patient is fit for surgery, comorbidities optimized |
| Patient Desire | Reluctance for surgery, high anxiety regarding surgical risks | Informed consent, realistic expectations, strong desire for definitive treatment |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is indispensable to optimize surgical outcomes, minimize potential complications, and ensure patient safety during volar wrist ganglion excision.
Pre-Operative Planning:
-
Clinical Assessment:
- History: A comprehensive history is critical, detailing the onset, duration, any perceived changes in size (fluctuation), precise characteristics of pain (severity, aggravating/alleviating factors), presence of neurological symptoms (e.g., paresthesias, dysesthesias, weakness), and any prior attempts at treatment (e.g., aspiration, splinting).
-
Physical Examination:
- Palpation: Accurately confirm the presence, size, consistency (typically firm and rubbery, but can be soft or boggy), mobility relative to underlying structures, and tenderness of the mass. Crucially, assess its relationship to the FCR tendon and the radial artery.
- Transillumination: A classic diagnostic test; true ganglions typically transilluminate due to their fluid content.
- Allen's Test: This is an absolutely mandatory assessment for all volar wrist masses, particularly those located on the radial side. It evaluates the patency of the ulnar artery and the collateral circulation to the hand. A positive Allen's test (indicating an absent or sluggish return of blood flow with ulnar artery occlusion) identifies patients with a dominant radial artery supply or anomalous arterial anatomy, where temporary compression or iatrogenic injury to the radial artery during surgery could result in severe ischemic consequences. The findings of the Allen's test must be documented pre-operatively.
- Range of Motion (ROM): Assess active and passive wrist motion, noting any limitations, crepitus, or pain through the arc of motion.
- Neurovascular Status: Perform a thorough sensory examination of the median, ulnar, and radial nerve distributions, and assess motor strength in the intrinsic and extrinsic hand muscles.
-
Imaging:
- Ultrasound (US): Often the first-line and most valuable imaging modality. US readily confirms the cystic nature of the mass, effectively differentiates it from solid tumors, precisely delineates its size and its critical relationship to adjacent neurovascular structures (especially the radial artery), and can often visualize the stalk originating from the joint capsule. This information is invaluable for pre-operative surgical mapping and planning.
- Magnetic Resonance Imaging (MRI): Generally reserved for cases presenting with diagnostic uncertainty, very large or deeply seated ganglions, or when there is suspicion of intraosseous pathology, complex intra-articular involvement, or alternative soft tissue tumors. MRI offers superior soft tissue contrast, allowing for precise definition of the lesion's extent and its relationship to osseous structures, tendons, nerves, and vessels. T2-weighted images typically demonstrate high signal intensity characteristic of fluid-filled cysts.
- Plain Radiographs: While not directly diagnostic for ganglions themselves, plain radiographs (e.g., PA, lateral, oblique views of the wrist) are useful to exclude underlying osseous pathology such as carpal instability, degenerative arthritis, occult fractures, or primary/secondary bone tumors.
- Informed Consent: A comprehensive discussion with the patient is essential. This must cover the nature of the condition, the proposed surgical procedure, the anticipated benefits (e.g., pain relief, cosmetic improvement), and the full spectrum of potential risks. Specific risks to be highlighted include recurrence, nerve injury (palmar cutaneous branch of the median nerve, superficial radial nerve), radial artery injury (including potential for ischemia), scar sensitivity, infection, stiffness, and Complex Regional Pain Syndrome (CRPS). Expected recovery timeline and alternative treatment options should also be thoroughly reviewed.
Patient Positioning & Anesthesia:
-
Anesthesia:
- Regional Anesthesia: An axillary or supraclavicular brachial plexus block is frequently the preferred anesthetic technique. It provides excellent intraoperative anesthesia, allows for comfortable tourniquet use without the need for general anesthesia, and confers superior post-operative pain control.
- General Anesthesia: An acceptable alternative, particularly if regional blockade is contraindicated, fails, or if patient preference dictates.
-
Patient Positioning:
- Supine Position: The patient is positioned supine on the operating table.
- Arm on Hand Table: The affected upper extremity is abducted and securely placed on a specialized hand table. This ensures unimpeded, stable access to the volar aspect of the wrist.
- Tourniquet Application: A pneumatic tourniquet is applied to the upper arm. The limb is exsanguinated (typically using an Esmarch bandage) prior to inflation to a pressure of 250-300 mmHg or approximately 100 mmHg above the patient's systolic blood pressure. A bloodless surgical field is absolutely critical for precise identification and protection of delicate neurovascular structures.
- Arm Support: The hand should be positioned with the wrist in slight extension, which can facilitate optimal exposure of the volar wrist capsule. This can be achieved using a rolled towel or specialized hand table attachments.
- Sterile Preparation and Drape: The entire hand, wrist, and distal forearm are meticulously prepared with an antiseptic solution and draped in a sterile fashion, ensuring ample exposure for the planned incision and providing flexibility for potential incision extension if deemed necessary intraoperatively.
Detailed Surgical Approach / Technique
Complete surgical excision of a volar wrist ganglion is a technically demanding procedure that requires meticulous surgical technique, precise anatomical knowledge, and diligent dissection to prevent iatrogenic neurovascular injury and minimize the risk of recurrence. The primary surgical objective is the complete excision of the entire cyst, including its stalk, back to its point of origin from the underlying joint capsule.
Incision Planning:
- Incision Type: A transverse or slightly curvilinear incision (aligned with Langer's lines) is generally preferred over a longitudinal incision for volar wrist approaches. This minimizes the risk of hypertrophic scarring, scar contracture, and potential nerve cross-over injuries. The incision should be centered over the most prominent or palpable portion of the ganglion.
- Location Considerations: For typical radial volar ganglions, the incision should be meticulously planned to allow for sufficient exposure of both the radial artery and the FCR tendon. It is imperative to avoid placing the incision directly over the radial artery or the main course of the palmar cutaneous branch of the median nerve. Pre-operative marking of the radial artery pulse and the ganglion's outline using a surgical pen can significantly aid precise incision placement.
Step-by-Step Dissection:
-
Skin Incision:
- Using a #15 scalpel, make a careful and controlled incision through the skin.
- Critical First Step: Immediately upon incising the skin and subcutaneous tissue, proactively identify and protect the palmar cutaneous branch of the median nerve . This nerve often courses superficially and can be inadvertently incised or mistaken for fibrous tissue if not specifically anticipated. It typically lies ulnar to the FCR tendon but can have variable courses. Once identified, it should be carefully isolated and gently retracted, usually in an ulnar direction, throughout the remainder of the procedure.
-
Subcutaneous Dissection & Exposure:
- Incise the subcutaneous fat and the superficial investing fascia. Employ a combination of fine dissecting scissors (Metzenbaum or tenotomy scissors) and a scalpel, utilizing both sharp and careful blunt dissection techniques.
- The ganglion typically resides within the subcutaneous tissue or just deep to the fascia.
- Identify the Radial Artery: This is the paramount structure requiring immediate identification. It usually lies radial and deep to the ganglion. Meticulously dissect the radial artery free from the ganglion capsule using fine instruments. Once isolated, gently retract it radially, ideally by carefully passing two vessel loops around it to sling and protect it throughout the entire procedure. Caution: Preserve a thin layer of adventitial tissue around the radial artery if the ganglion is densely adherent, rather than risking direct injury to the vessel wall.
- Identify the Flexor Carpi Radialis (FCR) Tendon: This tendon lies consistently ulnar to the ganglion in most common presentations. It serves as a reliable anatomical landmark. Gently retract the FCR tendon in an ulnar direction.
-
Ganglion Isolation:
- With the radial artery safely protected and the FCR tendon retracted, the ganglion capsule should be clearly visualized. It commonly appears as a pearly white or translucent, thin-walled sac.
- Carefully dissect circumferentially around the entire ganglion using a combination of blunt and sharp dissection. The goal is to isolate the ganglion completely from its surrounding soft tissue attachments.
- Avoid Premature Rupture: While not a catastrophic event, try to avoid rupturing the ganglion prematurely. A ruptured ganglion can collapse, making complete identification and excision of its capsule and stalk significantly more challenging due due to obscuration of tissue planes. If rupture occurs, aspirate the mucinous content and meticulously proceed with complete capsule removal.
-
Stalk Identification and Excision:
- Systematically trace the ganglion inferiorly and deeply to its point of origin, which is the "stalk." This stalk invariably arises from the volar wrist capsule, most commonly from the scapholunate (SL) or radioscaphocapitate (RSC) ligament regions.
- The stalk is often a narrow, fibrous pedicle directly connecting the ganglion to the underlying joint.
- Key to Preventing Recurrence: The definitive step for minimizing recurrence is the complete excision of the stalk along with a small, elliptical cuff of the surrounding joint capsule from which it originates. Use fine, curved scissors or a #15 scalpel to excise this capsular defect precisely. The resulting defect in the joint capsule is typically small and rarely requires direct repair, as it usually heals spontaneously without adverse sequelae.
- Thoroughly inspect the base of the excision site for any remaining fragments of synovial tissue or smaller, accessory loculations of the ganglion, ensuring complete removal.
-
Hemostasis:
- Once the entire ganglion and its stalk have been completely removed, meticulous hemostasis is paramount. Employ fine bipolar cautery for any small bleeding vessels. Exercise extreme caution and avoid excessive cautery near vital structures such as the radial artery or any nerves.
-
Wound Closure:
- Capsular/Fascial Closure: The capsular defect created by the excision is generally left open to heal by secondary intention. If the deep fascia has been opened, a loose re-approximation may be performed using fine absorbable sutures (e.g., 3-0 or 4-0 absorbable) to provide a degree of soft tissue coverage.
- Subcutaneous Layer: Close the subcutaneous layer with interrupted absorbable sutures (e.g., 4-0 absorbable or 5-0 absorbable) to approximate the skin edges and reduce tension on the final skin closure.
- Skin Closure: Close the skin with fine non-absorbable sutures (e.g., 5-0 or 6-0 nylon) or an absorbable subcuticular suture for optimal cosmetic outcome.
- Dressing: Apply a sterile, non-adherent dressing directly to the wound, followed by a soft compressive wrap or a volar wrist splint. This provides immediate comfort, gentle immobilization, and helps control post-operative swelling for the initial 7-10 days.
Internervous Planes / Critical Relationships:
- The primary internervous plane of consideration in this approach is defined by the relationship between the FCR tendon, the radial artery, and the palmar cutaneous branch of the median nerve. The ganglion most commonly resides within the fascial plane bordered by the FCR tendon (ulnarly) and the radial artery (radially).
- Understanding the highly superficial course and variable anatomy of the palmar cutaneous branch of the median nerve is absolutely paramount during the initial skin incision and subcutaneous dissection to prevent iatrogenic injury.
- The radial artery is consistently located radial to the FCR tendon and must be identified early in the dissection and carefully protected throughout the entire procedure.
Complications & Management
While generally considered a safe procedure, surgical excision of a volar wrist ganglion is associated with potential complications. Comprehensive awareness of these risks, coupled with robust prevention and management strategies, is critical for all orthopedic surgeons.
Common Complications, Incidence, and Salvage Strategies:
| Complication | Incidence | Description | Prevention Strategies | Salvage Strategies / Management |
|---|---|---|---|---|
| Recurrence | 5-15% | Re-formation of the ganglion at or adjacent to the surgical site. Higher risk if the stalk and a sufficient cuff of adjacent capsule are not fully excised. | Complete excision of the entire ganglion and its stalk, including a generous cuff of the underlying joint capsule. Careful identification and removal of all loculations. | Initial conservative management (observation, aspiration). If symptomatic and persistent, re-excision may be considered after detailed imaging (US/MRI) for precise localization and planning. Consider referral to a specialist for potentially complex revision surgery. |
| Nerve Injury | <5% | Palmar cutaneous branch of median nerve: Most common nerve injured, leading to numbness, paresthesias, or painful neuroma formation in the radial palm. Superficial radial nerve: Less common but possible with extensive radial dissection, leading to dorsal hand sensory deficits. | Meticulous and unhurried dissection. Employ a transverse or curvilinear incision. Early identification and careful retraction of the palmar cutaneous branch of the median nerve. Avoid aggressive electrocautery near identified neural structures. | Mild symptoms: Observation, nerve gliding exercises, neuropathic pain medications (e.g., gabapentin, pregabalin). Persistent, severe pain or documented neuroma: Surgical exploration for neurolysis, neurectomy with nerve burial, or stump capping. Consider referral to a peripheral nerve specialist. |
| Radial Artery Injury | <1% | Laceration, transection, or post-operative thrombosis of the radial artery. Potentially leads to hand ischemia in cases of dominant radial artery supply (identified by a positive Allen's test). | Mandatory pre-operative Allen's test. Meticulous identification, careful blunt dissection, and gentle retraction (using vessel loops) of the radial artery throughout the procedure. Avoid direct grasping, clamping, or aggressive retraction of the artery. | Immediate Intraoperative: Primary repair if small laceration. Transection/Thrombosis: Microvascular repair or interpositional vein grafting by a surgeon experienced in microsurgery if there is a significant risk of hand ischemia (positive Allen's test). Post-operative anticoagulation may be necessary. |
| Wound Complications | <5% | Post-operative infection, hematoma formation, seroma development, or surgical wound dehiscence. Can lead to prolonged recovery, increased pain, and adverse cosmetic scarring. | Adherence to strict aseptic technique, meticulous intraoperative hemostasis, careful multi-layer wound closure, and appropriate sterile post-operative dressing. Proper tourniquet technique. | Infection: Systemic antibiotics (empiric, then culture-directed), wound debridement as indicated. Hematoma/Seroma: Aspiration if small and symptomatic, or incision and drainage. Dehiscence: Meticulous wound care, potential secondary closure if appropriate. |
| Scar Tenderness / Hypersensitivity | Varies | Painful, hyperesthetic, or aesthetically unpleasing scar (e.g., hypertrophic or keloid scarring) possibly due to subtle nerve irritation or abnormal wound healing. | Optimal incision placement (following Langer's lines), careful atraumatic soft tissue handling, precise skin edge approximation. Encourage early mobilization and scar massage. | Scar massage, silicone gel sheeting, topical emollients. Desensitization exercises. Local corticosteroid injections for hypertrophic scars. Rarely, surgical scar revision or targeted nerve treatment if neuroma is suspected. |
| Wrist Stiffness / Decreased ROM | <5% | Post-operative pain, edema, or prolonged immobilization leading to restricted wrist motion. | Early, controlled active and passive range of motion exercises initiated as per rehabilitation protocol. Minimize excessive soft tissue trauma during surgery. | Aggressive referral to and management by a certified hand therapist. Active and passive range of motion exercises. Dynamic or static progressive splinting may be beneficial. Rarely, surgical lysis of adhesions if severe and refractory. |
| Complex Regional Pain Syndrome (CRPS) | Rare (<1%) | A severe, chronic pain condition characterized by disproportionate pain, swelling, allodynia, hyperalgesia, sudomotor dysfunction, and trophic changes. | Employ atraumatic surgical technique, ensure adequate post-operative pain control, and encourage early controlled mobilization. Early recognition and prompt multidisciplinary treatment of emerging symptoms. | Aggressive multi-modal pain management strategies (physical therapy, occupational therapy, neuropathic medications, regional nerve blocks, psychological support). Early diagnosis and specialist referral to a pain management clinic are paramount for optimal outcomes. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following volar wrist ganglion excision is designed to restore full wrist function, minimize the development of stiffness, and effectively manage any potential complications, all while ensuring appropriate tissue healing. Rehabilitation protocols may require slight adjustments based on the extent of intraoperative dissection, individual patient factors, and the presence of specific complications.
Immediate Post-Operative Period (Day 0-7):
-
Immobilization:
- A bulky soft compressive dressing is typically applied in the operating room to provide gentle pressure, minimize swelling, and protect the surgical site.
- A custom or prefabricated volar wrist splint, or a sugar-tong splint, is commonly applied for approximately 1 week. This provides comfort, protection, and gentle immobilization of the wrist, usually in a position of slight extension (0-15 degrees).
- Elevation: Strict elevation of the hand above heart level (e.g., using pillows or a sling while ambulating) is crucial to minimize post-operative swelling and edema.
- Pain Management: Prescribe appropriate oral analgesics to ensure adequate pain control.
- Finger ROM: Encourage immediate, gentle active range of motion (AROM) exercises for the fingers and thumb. This helps prevent stiffness in the digits, maintains tendon gliding, and promotes lymphatic drainage.
- Wound Care: Maintain meticulous wound hygiene. Keep the wound dressing clean and dry. Initial dressing changes are typically performed by the surgeon or nursing staff at 2-3 days post-op.
Early Rehabilitation Phase (Weeks 1-3):
- Splint Removal & Suture Removal: The surgical dressing and splint are generally removed at the 7- to 10-day post-operative visit. Skin sutures are also typically removed at this time.
- Gentle Active Range of Motion (AROM): Initiate gentle, pain-free active wrist flexion, extension, radial deviation, and ulnar deviation exercises. These movements should be performed slowly and within the patient's comfortable range.
- Forearm Pronation/Supination: Begin active forearm rotation exercises (pronation and supination) to maintain mobility of the radioulnar joints.
- Scar Management: Once the surgical wound is completely closed and dry, begin gentle scar massage. This technique helps to improve scar pliability, reduce sensitivity, and prevent adherence to deeper tissues. Silicone gel sheets or scar creams can also be initiated to prevent hypertrophic scarring or keloid formation.
- Edema Control: Continue to emphasize limb elevation and encourage gentle hand pumping exercises to facilitate fluid drainage and minimize residual swelling.
- Progressive Strengthening (Optional for some): For uncomplicated cases with minimal pain, very light isometric gripping exercises (e.g., squeezing a soft ball) may be introduced cautiously towards the end of this phase, provided pain allows.
Intermediate Rehabilitation Phase (Weeks 3-6):
- Progressive AROM and Passive Range of Motion (PROM): Gradually increase the intensity and arc of wrist motion exercises. If wrist stiffness persists, gentle passive stretching can be carefully initiated, often under the guidance of a hand therapist.
-
Strengthening:
- Initiate progressive strengthening exercises for the wrist flexors, extensors, and intrinsic/extrinsic grip musculature. Start with light resistance (e.g., therapeutic putty, light hand weights, elastic bands).
- Focus on exercises that incorporate functional movements relevant to the patient's daily activities.
- Proprioception and Coordination: Begin exercises aimed at improving wrist stability, balance, and fine motor coordination (e.g., controlled movements, light object manipulation).
- Desensitization: If scar tenderness, hyperesthesia, or neuropathic irritation is present, continue with specific desensitization techniques as guided by a therapist.
Advanced Rehabilitation Phase (Weeks 6-12 and beyond):
- Return to Activity: Patients should gradually and progressively return to sport-specific or work-specific activities. High-impact activities, heavy lifting, or activities requiring repetitive forceful gripping should be avoided until full strength, pain-free motion, and confidence are achieved.
- Continued Strengthening: Implement advanced resistance exercises tailored to the patient's specific occupational demands, recreational activities, and overall fitness goals.
- Endurance Training: For patients requiring return to demanding physical activities, incorporate endurance training for the wrist and forearm musculature.
- Monitoring for Complications: Continue diligent monitoring for any signs of ganglion recurrence, persistent nerve irritation, or the development of Complex Regional Pain Syndrome (CRPS).
Special Considerations:
- Persistent Pain/Stiffness: If significant pain or stiffness persists despite adherence to the protocol, a formal referral for hand therapy evaluation and treatment is strongly recommended. Modalities such as therapeutic ultrasound, heat/cold therapy, and advanced manual therapy techniques may be beneficial.
- Neuropathic Symptoms: Should nerve irritation or neuropathic pain persist, referral to a hand therapist for specialized nerve gliding exercises and a pain specialist for comprehensive neuropathic pain management strategies may be necessary.
- Recurrence: In the event of documented ganglion recurrence, a thorough re-evaluation with advanced imaging (US, MRI) is warranted. Options may include repeat aspiration, or considering surgical revision after a period of observation, as deemed appropriate based on patient symptoms and imaging findings.
Summary of Key Literature / Guidelines
Current literature on volar wrist ganglions largely advocates for a systematic, graduated approach to management, prioritizing non-operative modalities as the initial course of action and reserving surgical excision for symptomatic, persistent, or recurrent lesions. Recurrence rates, complication profiles, and optimal surgical techniques have been extensively investigated and reported in the orthopedic literature.
Key Findings & Consensus:
- Diagnosis: High-resolution ultrasound (US) has emerged as an exceptionally effective first-line imaging modality for confirming the cystic nature of volar wrist masses. It is superior in differentiating benign ganglions from solid soft tissue tumors and is invaluable for precisely mapping their intricate relationship to critical neurovascular structures, most notably the radial artery. This detailed anatomical information significantly enhances pre-operative surgical planning. Magnetic Resonance Imaging (MRI) is generally reserved for cases presenting with diagnostic ambiguity, very large or deeply situated ganglions, or when there is a suspicion of complex intra-articular pathology or alternative tumor types.
-
Non-Operative Management:
- Observation: A notable proportion of wrist ganglions (reported as high as 50% in some series) can undergo spontaneous resolution. Therefore, observation with reassurance is considered a valid and often preferred initial strategy for asymptomatic or minimally symptomatic lesions.
- Aspiration: While effective in confirming the diagnosis by yielding characteristic mucinous fluid and providing temporary symptomatic relief, aspiration (whether standalone or combined with corticosteroid injection) demonstrates significantly higher recurrence rates (ranging from 30% to 70%) compared to definitive surgical excision. Despite this, it remains a low-risk, minimally invasive intervention and is a reasonable first-line treatment option for symptomatic patients who wish to defer or avoid surgery.
-
Surgical Excision:
- Indications: The primary indications for surgical intervention include persistent, debilitating pain, significant functional impairment, documented neurological symptoms (e.g., nerve compression), profound cosmetic distress impacting the patient's quality of life, or diagnostic uncertainty where malignancy cannot be definitively excluded.
- Technique: Complete open surgical excision, which explicitly includes the entirety of the ganglion cyst, its stalk, and a small, circumferential cuff of the underlying joint capsule from which it originates, remains the gold standard for achieving the lowest recurrence rates. Meticulous and unhurried dissection, with particular emphasis on early identification and diligent protection of the radial artery and the palmar cutaneous branch of the median nerve, is absolutely paramount to prevent iatrogenic injury.
- Recurrence Rates: Recurrence rates following carefully performed open surgical excision of volar wrist ganglions typically range from 5% to 15%. Incomplete excision of the capsular stalk or failure to remove all accessory loculations is widely considered the predominant cause of recurrence.
- Complications: Nerve injury, predominantly involving the palmar cutaneous branch of the median nerve, is the most frequently reported iatrogenic complication. Although rare, radial artery injury represents a potentially severe complication. Other recognized complications include scar hypersensitivity, post-operative wrist stiffness, and wound-related issues (e.g., infection, hematoma).
-
Arthroscopic Excision:
- For dorsal wrist ganglions, arthroscopic excision has gained considerable popularity, offering recurrence rates comparable to open excision with potentially faster recovery and improved cosmesis.
- However, for volar wrist ganglions , arthroscopic techniques are significantly more technically challenging. This is primarily due to the anatomically confined operative space, the close proximity of vital neurovascular structures (especially the radial artery), and the inherent difficulty in achieving direct intra-articular visualization and thorough excision of the volar capsule and stalk from within the joint. While some specialized arthroscopic approaches have been described, they are considerably less common than open excision for volar lesions and are typically reserved for experienced arthroscopic wrist surgeons. The supporting literature for arthroscopic excision of volar ganglions is less robust and mature compared to that for dorsal lesions.
- Post-Operative Care: Current guidelines generally recommend early, controlled mobilization of the wrist post-operatively to prevent stiffness, followed by progressive strengthening exercises as tolerated and guided by patient comfort and tissue healing.
The long-term outcomes following surgical excision of volar wrist ganglions are generally excellent, with high rates of patient satisfaction, provided that appropriate patient selection criteria are applied and meticulous surgical technique is executed. Continued research endeavors aim to further elucidate ganglion pathogenesis and refine minimally invasive surgical strategies.
You Might Also Like