Skier's Thumb Case Study: Diagnosing Ulnar Collateral Ligament Rupture & Stener Lesion
Key Takeaway
Diagnosis of Skier's Thumb (UCL rupture) involves a detailed clinical examination, including valgus stress testing that reveals significant instability. A palpable firm mass near the MCP joint strongly suggests a Stener lesion. MRI imaging is crucial for confirming a complete UCL tear and identifying the Stener lesion's displacement, guiding appropriate surgical intervention.
Unraveling Ulnar Collateral Complex Injuries: A Skier's Thumb Case
Patient Presentation & History
A 35-year-old right-hand dominant male presented to the emergency department following a skiing accident. The mechanism of injury involved a fall where his thumb was forcefully abducted and hyperextended by the ski pole strap, leading to immediate pain and swelling localized to the ulnar aspect of his right thumb metacarpophalangeal (MCP) joint. He reported an immediate sensation of instability and a distinct "pop" at the time of injury.
Prior medical history was unremarkable, with no known allergies or significant comorbidities. He denied any previous injuries to the affected hand or wrist. He is an active individual, regularly participating in sports. His social history includes occasional alcohol consumption and no tobacco use. He works as a software engineer, requiring significant fine motor dexterity and repetitive keyboard use, making optimal thumb function critical for his profession.
Upon presentation, the patient described severe pain, rated 8/10 on a visual analog scale, exacerbated by any movement or attempt at grasping objects. He also noted a subjective feeling of weakness in his pinch grip. Ecchymosis developed rapidly over the ulnar aspect of the thumb MCP joint within hours of the injury.
Clinical Examination
Inspection: Significant edema and ecchymosis were observed over the ulnar aspect of the right thumb MCP joint. No gross deformity was evident. The skin integrity was intact. There was no obvious rotational malalignment of the digit.
Palpation: Maximal tenderness was elicited directly over the ulnar collateral ligament (UCL) complex, specifically at its insertion into the base of the proximal phalanx and, to a lesser extent, at its origin on the metacarpal head. A distinct, firm, pea-sized mass was palpable proximally and ulnarly to the MCP joint line, consistent with a potential Stener lesion, indicating displacement of the ruptured UCL superficial to the adductor pollicis aponeurosis. Tenderness was also noted at the adductor pollicis muscle belly. No tenderness was appreciated over the radial collateral ligament, carpometacarpal joint, or surrounding wrist structures.
Range of Motion (ROM):
Active and passive ROM of the right thumb MCP joint was severely painful and restricted due to guarding and swelling.
*
Flexion:
Limited to approximately 30 degrees (normal 50-70 degrees).
*
Extension:
Limited to 0 degrees (normal 0-10 degrees hyperextension).
*
Abduction/Adduction:
Markedly painful and guarded.
Valgus Stress Testing:
This was performed carefully, initially under local anesthetic infiltration, to minimize patient discomfort and allow for an accurate assessment of stability.
*
At 0 degrees MCP flexion:
Demonstrated approximately 20 degrees of valgus angulation compared to the contralateral uninjured thumb's 5 degrees of angulation, with a soft, ill-defined endpoint.
*
At 30 degrees MCP flexion (to isolate the proper UCL):
Revealed approximately 40 degrees of valgus angulation compared to the contralateral side's 10 degrees, again with a distinct soft endpoint and significant gapping perceived by the examiner. This difference of 30 degrees compared to the uninjured side, and a total angulation exceeding 35 degrees, strongly indicated a complete rupture of the proper UCL.
Neurological Assessment: Sensation was intact in the distribution of the radial, median, and ulnar nerves. Specifically, the dorsal digital nerve of the thumb was intact. Motor function of the intrinsic thumb muscles, including the thenar musculature and adductor pollicis, was difficult to assess due to pain but appeared grossly intact.
Vascular Assessment: Capillary refill was brisk in all digits. Radial and ulnar pulses were strong and palpable. No signs of vascular compromise were observed.
Imaging & Diagnostics
Radiographs:
Initial plain radiographs of the right thumb, including AP, lateral, and oblique views, were obtained.
* No obvious fractures of the metacarpal, proximal phalanx, or distal phalanx were identified.
* Specifically, there was no clear evidence of an avulsion fracture at the base of the proximal phalanx, which would indicate a bony UCL insertion avulsion.
* The MCP joint alignment appeared concentric, with no signs of dislocation or subluxation on static views.
* Joint space was preserved.
* Stress radiographs were considered but deemed unnecessary given the clear clinical instability and the palpable Stener lesion, warranting further soft tissue evaluation.
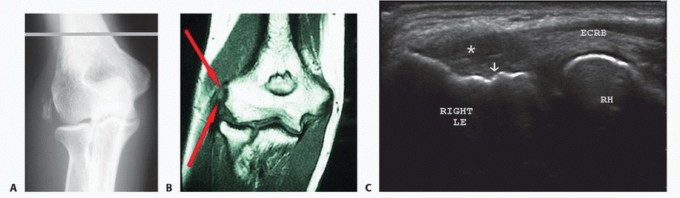
Magnetic Resonance Imaging (MRI):
Due to the strong clinical suspicion of a complete UCL rupture with a Stener lesion, an MRI of the right thumb was ordered.
*
Findings:
The MRI confirmed a complete tear of the proper UCL, characterized by discontinuity of the ligament fibers. The proximal stump of the UCL was identified as having retracted proximally and superficially to the adductor pollicis aponeurosis, consistent with a Stener lesion.
* Significant edema and hemorrhage were noted around the ruptured ligament and within the surrounding soft tissues.
* The accessory UCL and volar plate appeared intact, though some edema was noted in adjacent tissues.
* No significant chondral damage or other osteochondral lesions were identified within the MCP joint.
* No associated bony avulsion fractures were seen.
Computed Tomography (CT): A CT scan was not indicated in this case, as the radiographs adequately ruled out significant bony pathology and the MRI provided superior soft tissue detail crucial for UCL assessment and Stener lesion identification. Templating is not routinely performed for acute UCL repair.
Differential Diagnosis
| Feature | Ulnar Collateral Ligament (UCL) Rupture (Complete) | Radial Collateral Ligament (RCL) Injury (Complete) | Avulsion Fracture (UCL insertion) | Metacarpal Head Fracture |
|---|---|---|---|---|
| Mechanism of Injury | Forced abduction and hyperextension of thumb MCP joint (e.g., ski pole, ball injury) | Forced adduction and hyperextension of thumb MCP joint (less common) | Same as UCL rupture, high-energy impact causing bony avulsion. | Direct axial load or crushing injury, fall on outstretched hand. |
| Pain Location | Ulnar aspect of thumb MCP joint. | Radial aspect of thumb MCP joint. | Ulnar aspect of thumb MCP joint, potentially more diffuse pain if bony involvement. | Localized pain over the metacarpal head, potentially radiating. |
| Swelling/Ecchymosis | Prominent over ulnar aspect. | Prominent over radial aspect. | Over ulnar aspect, often more pronounced due to associated bony injury. | Over the metacarpal head, potentially diffuse depending on soft tissue involvement. |
| Valgus Stress Test | Positive: >15 degrees angulation compared to contralateral side, or >30-35 degrees total angulation at 30° flexion with soft endpoint. | Negative (or stable) on valgus stress. | Positive: Similar to ligamentous rupture, gapping with valgus stress. | May be stable or unstable depending on fracture pattern; stress testing may exacerbate pain. |
| Varus Stress Test | Negative (or stable) on varus stress. | Positive: >15 degrees angulation compared to contralateral side, or >30-35 degrees total angulation at 30° flexion with soft endpoint. | Negative (or stable) on varus stress. | May be stable or unstable; stress testing may exacerbate pain. |
| Palpation for Stener | Positive: Palpable mass (retracted UCL) proximal and ulnar to joint line, indicating interposition of adductor aponeurosis. | Negative. | Negative for classic Stener lesion; palpable bony fragment may be felt if displaced. | Tenderness directly over the metacarpal head; crepitus may be present. |
| Radiographs | Normal or subtle widening of ulnar joint space with stress views. No bony avulsion. | Normal or subtle widening of radial joint space with stress views. No bony avulsion. | Positive: Avulsion fracture from the base of the proximal phalanx (ulnar side). Displacement can vary. | Positive: Fracture line within the metacarpal head; may be comminuted, intra-articular. |
| MRI | Definitive: Confirms UCL rupture, identifies Stener lesion, rules out other soft tissue injury. | Definitive: Confirms RCL rupture, rules out other soft tissue injury. | Confirms bony avulsion and associated ligamentous disruption. Can assess fragment displacement. | Confirms fracture pattern, soft tissue edema, ligamentous integrity. |
| Treatment Implications | Surgical repair indicated for complete tears with Stener lesion or significant instability. Non-operative for partial/stable tears. | Surgical repair indicated for complete tears with significant instability. | Surgical fixation (K-wires, screw, suture anchor) for displaced fragments. Non-operative for non-displaced. | Varies from non-operative (splinting, casting) to operative (ORIF) depending on displacement, intra-articular involvement. |
Surgical Decision Making & Classification
The decision for operative intervention in this patient was based on a confluence of clinical and imaging findings:
1.
Clinical Instability:
The valgus stress testing revealed significant instability (40 degrees total angulation at 30 degrees flexion, 30 degrees greater than the contralateral side) with a soft endpoint, indicative of a complete UCL rupture.
2.
Palpable Stener Lesion:
The presence of a palpable mass consistent with a Stener lesion is a direct indication for surgical repair. The Stener lesion represents interposition of the adductor pollicis aponeurosis between the ruptured ends of the UCL, preventing anatomical healing and leading to chronic instability if left untreated.
3.
Functional Demands:
The patient's profession as a software engineer requires excellent fine motor control and strong pinch grip, making restoration of thumb MCP joint stability paramount for his functional recovery and return to work.
Classification:
Based on the MRI findings, this injury would be classified as a
Snyder Type III
UCL injury, which denotes a complete tear with a Stener lesion. This classification system, although based on MRI findings, directly informs surgical necessity due to the mechanical block to healing presented by the Stener lesion. Less formally, it is categorized as a complete UCL rupture with a Stener lesion, which is universally accepted as an indication for surgical repair.
Non-operative management, involving thumb spica casting for 4-6 weeks, is typically reserved for partial UCL tears or complete tears without a Stener lesion where instability is minimal, which was not the case here. Given the clinical and radiographic evidence, non-operative management would lead to chronic instability, pain, and potentially degenerative arthritis of the MCP joint. Therefore, acute surgical repair was deemed the most appropriate course of action to ensure optimal functional outcome.
Surgical Technique / Intervention
Patient Positioning and Anesthesia:
The patient was positioned supine on the operating table. A hand table was utilized to support the right upper extremity. A pneumatic tourniquet was applied to the upper arm. The hand and forearm were prepped and draped in a sterile fashion. Regional anesthesia (axillary block) combined with monitored anesthesia care (MAC) was administered.
Surgical Approach:
A curvilinear incision approximately 3-4 cm in length was made along the dorsal-ulnar aspect of the thumb MCP joint. The incision extended from the metacarpal neck to the mid-portion of the proximal phalanx. Careful dissection was performed through the subcutaneous tissue. The superficial dorsal digital nerves of the thumb were identified and protected to avoid iatrogenic injury. These nerves were gently retracted radially.
The adductor pollicis aponeurosis was identified. Upon incising the aponeurosis longitudinally, the retracted proximal stump of the ruptured UCL was found lying superficial to the aponeurosis, confirming the presence of a Stener lesion. The distal stump of the UCL was identified at its insertion on the ulnar aspect of the proximal phalanx.
Exploration and Debridement:
Hematoma and inflammatory tissue within the joint capsule were debrided. The MCP joint was inspected for any intra-articular damage or loose bodies. The joint surfaces were found to be intact. The ruptured ligament ends were refreshed minimally to expose viable tissue.
Fixation Construct:
Due to the avulsion of the UCL from its insertion at the base of the proximal phalanx, a suture anchor technique was chosen.
1.
Anchor Placement:
A 2.0 mm bioabsorbable suture anchor (e.g., Fiberwire, PEEK) preloaded with two strands of #2 non-absorbable suture was placed into the ulnar cortex at the base of the proximal phalanx, at the anatomical insertion site of the UCL. A drill hole was created perpendicular to the cortical surface, and the anchor was fully deployed.
2.
Suture Configuration:
Each limb of the suture was then passed through the substance of the distal stump of the avulsed UCL in a mattress or figure-of-eight fashion, ensuring a wide purchase of healthy ligamentous tissue.
3.
Repair and Tensioning:
The MCP joint was flexed to approximately 30 degrees and held in slight adduction to relax the ligament. The sutures were then tied securely, bringing the avulsed UCL stump anatomically back to its insertion site on the proximal phalanx. The repair was meticulously tightened to ensure appropriate tension, avoiding both overtensioning and laxity.
4.
Capsular Repair:
The joint capsule and any torn portions of the adductor pollicis aponeurosis were repaired over the UCL repair using fine absorbable sutures (e.g., 3-0 Vicryl) to reinforce the repair and restore anatomical layers.
5.
Assessment of Stability:
Following the repair, valgus stress testing was re-performed. The MCP joint demonstrated excellent stability with a firm endpoint, comparable to the contralateral uninjured thumb. No residual gapping or instability was noted.
6.
Wound Closure:
The subcutaneous tissues were closed with absorbable sutures (e.g., 4-0 Vicryl). The skin was closed with non-absorbable monofilament sutures (e.g., 4-0 Nylon) in an interrupted fashion. A sterile dressing was applied, followed by a well-padded thumb spica splint maintaining the thumb MCP joint in slight flexion (20-30 degrees) and slight adduction.
Post-Operative Protocol & Rehabilitation
The post-operative protocol is critical for optimal healing and functional recovery, balancing protection of the repair with timely mobilization.
Phase 1: Immobilization and Protection (Weeks 0-4)
*
Immobilization:
The thumb MCP joint will be immobilized in a rigid custom-molded thermoplastic thumb spica splint, maintaining the MCP joint in 20-30 degrees of flexion and slight adduction. The interphalangeal (IP) joint of the thumb is left free for active range of motion, and the wrist is typically included to prevent unwanted thumb motion.
*
Wound Care:
Regular wound checks. Sutures will be removed at 10-14 days post-op.
*
Activity Restrictions:
No active or passive thumb MCP motion. No lifting, grasping, or pinching activities with the affected hand. Avoid any valgus stress to the thumb.
*
Adjunctive Care:
Elevation of the hand to minimize swelling. Ice application. Pain management as needed. Active range of motion for the wrist, elbow, and shoulder is encouraged to prevent stiffness in uninvolved joints. Gentle active and passive range of motion of the unaffected fingers.
Phase 2: Controlled Active Motion (Weeks 4-8)
*
Splint Weaning:
At 4 weeks post-op, the thumb spica splint will be discontinued. A removable custom-molded thumb spica orthosis or soft thumb brace will be provided for use during activities and for protection.
*
Initiate Thumb MCP ROM:
Gentle, pain-free active range of motion (AROM) exercises for the thumb MCP joint are initiated. Passive range of motion (PROM) may be cautiously introduced by a hand therapist, ensuring no valgus stress.
*
Strengthening:
Gentle isometric exercises for the thumb (e.g., light opposition, adduction) can begin.
*
Functional Activities:
Light functional activities involving the hand are permitted, avoiding any heavy gripping, lifting, or activities that place valgus stress on the thumb.
*
Therapist Visits:
Weekly hand therapy sessions to monitor progress, ensure proper technique, and adjust exercises.
Phase 3: Progressive Strengthening and Functional Return (Weeks 8-12)
*
Increased ROM:
Continue to progress AROM and PROM, aiming for full pain-free motion.
*
Progressive Strengthening:
Increase the intensity of strengthening exercises. This includes resistance exercises with therapy putty, light weights, and resistance bands for all thumb movements (flexion, extension, abduction, adduction, opposition). Focus on pinch strength and grip strength.
*
Scar Management:
Scar massage and desensitization techniques as needed.
*
Return to Work:
Gradual return to work duties, with modifications as necessary, depending on the physical demands.
*
Activity Restrictions:
Continued avoidance of high-impact activities or direct valgus stress.
Phase 4: Return to Sport and Unrestricted Activity (Weeks 12-24+)
*
Sport-Specific Training:
For athletes, sport-specific drills and progressive return to activity protocols are initiated.
*
Protection:
Continued use of protective taping or a custom brace during sports or high-risk activities may be recommended for several months.
*
Full Activity:
Full return to unrestricted activities, including contact sports, typically occurs between 4-6 months, provided stability and strength are fully restored, and the patient is pain-free. Final assessment includes comparison of pinch and grip strength to the contralateral side.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- Mechanism of Injury: Always elicit a detailed history of the injury mechanism. Forced abduction and hyperextension of the thumb MCP joint is pathognomonic for UCL injury.
- Clinical Assessment is Key: A thorough clinical examination, particularly focused valgus stress testing, is paramount. Perform stress testing at both 0 degrees (tests volar plate, proper, and accessory ligaments) and 30 degrees of MCP flexion (isolates the proper UCL). Compare to the contralateral side. A difference of >15 degrees or total angulation >30-35 degrees at 30 degrees flexion is indicative of complete rupture.
- Palpable Stener Lesion: The ability to palpate a firm mass (the retracted UCL stump) proximal and ulnar to the MCP joint line is a critical diagnostic pearl, strongly indicating a Stener lesion and thus the need for surgical intervention.
- MRI for Confirmation: While clinical suspicion is high, MRI is the gold standard for confirming UCL rupture, identifying a Stener lesion, and ruling out other soft tissue or occult bony injuries. It guides surgical planning.
- Acute Surgical Repair: For complete tears with a Stener lesion or significant instability, acute surgical repair within 3 weeks (ideally 7-10 days) yields superior outcomes compared to delayed reconstruction. Direct repair of the ligament to its bony insertion (often with suture anchors) is the preferred technique.
- Nerve Protection: Meticulous dissection to identify and protect the dorsal digital branches of the radial nerve is crucial during the surgical approach to prevent iatrogenic neuromas or sensory deficits.
- Appropriate Tensioning: During repair, ensure the ligament is re-tensioned anatomically. The MCP joint should be gently flexed (20-30 degrees) and slightly adducted to relax the repair during suture tying, preventing overtensioning which can lead to stiffness, or undertensioning which can result in persistent instability.
- Controlled Rehabilitation: A structured, progressive rehabilitation protocol is essential. Initial immobilization is followed by controlled, gentle range of motion, then gradual strengthening. Premature or aggressive mobilization can compromise the repair.
Pitfalls:
- Missed Stener Lesion: Failure to recognize or adequately assess for a Stener lesion is a significant pitfall. If a Stener lesion is present, non-operative management will inevitably lead to chronic instability and poor functional outcomes due to the mechanical block to healing.
- Inadequate Stress Testing: Rushing or performing stress tests without adequate pain control can lead to patient guarding and inaccurate assessment of instability, resulting in misdiagnosis of a partial tear when a complete tear exists. Failure to test at 30 degrees flexion may mask a proper UCL tear.
- Over-reliance on X-rays: Plain radiographs primarily assess bone. A ligamentous injury can be severe even with normal radiographs. Over-reliance on X-rays can lead to underestimation of soft tissue injury severity.
- Failure to Address Avulsion Fractures: While this case involved a pure ligamentous tear, UCL injuries can be associated with small avulsion fractures from the base of the proximal phalanx. If displaced, these fragments must be anatomically reduced and fixed to restore stability.
- Iatrogenic Nerve Injury: The superficial radial nerve branches are vulnerable during the dorsal-ulnar approach. Inadequate identification and protection can lead to painful neuromas or persistent sensory loss.
- Premature Rehabilitation: Advancing rehabilitation too quickly, especially initiating valgus stress or heavy gripping activities, can disrupt the healing ligament and lead to re-rupture or chronic laxity.
- Chronic Instability and Arthritis: Undiagnosed or inadequately treated UCL injuries can lead to chronic pain, persistent instability, weakened pinch grip, and eventually degenerative arthritis of the thumb MCP joint, severely impacting function and quality of life.
- Underestimating Patient Functional Demands: For patients with high demands on their hands (e.g., surgeons, musicians, athletes, those requiring fine motor skills for work), even seemingly minor instability can be debilitating, necessitating a robust treatment plan.
You Might Also Like