Mastering Wrist Arthroscopy: Essential Preparation and Techniques

Key Takeaway
Looking for accurate information on Mastering Wrist Arthroscopy: Essential Preparation and Techniques? Wrist arthroscopy evolved with advanced preparation and techniques, including midcarpal approaches, driven by anatomic understanding. Initial techniques emphasized dorsal portals (e.g., 1-2, 3-4, 4-5, 6R/6U) due to fewer neurovascular structures. Subsequent midcarpal radial and ulnar portals enable comprehensive joint access and triangulation for treating intracarpal pathology.
Introduction & Epidemiology
Since its inception, wrist arthroscopy has continued to evolve from a purely diagnostic tool to a sophisticated modality for therapeutic intervention. The initial emphasis on viewing the wrist from the dorsal aspect arose from the relative paucity of major neurovascular structures in this region, coupled with the familiarity of most orthopedic surgeons with dorsal approaches to the radiocarpal joint for open procedures. Early applications primarily focused on diagnostic evaluation of chronic wrist pain, assessment of intracarpal fractures, and debridement of synovitis.
Anatomic studies, particularly those elucidating the intricate three-dimensional relationships of interosseous ligaments and the complex kinematics of the carpus, fundamentally advanced our understanding of wrist function and pathology. This deeper insight led directly to the development of midcarpal arthroscopy, expanding the scope of visualization and intervention within the carpal rows. The relentless pursuit of minimally invasive solutions by innovative surgeons has consistently pushed the envelope, leading to the development of novel techniques for treating an ever-broadening spectrum of intracarpal pathologies. This progression has culminated in the description and routine use of a plethora of new accessory portals, enabling access to previously challenging or inaccessible areas of the wrist and distal radioulnar joint (DRUJ).
Epidemiologically, wrist arthroscopy has become an indispensable tool in the modern orthopedic surgeon's armamentarium. Its utility spans from managing chronic wrist pain secondary to ligamentous injuries (e.g., scapholunate or lunotriquetral instability), triangular fibrocartilage complex (TFCC) tears, and inflammatory arthropathies, to acute scenarios such as distal radius fracture management and carpal fracture assessment. The prevalence of these conditions, particularly wrist sprains and traumatic injuries in active populations, underpins the increasing demand for skilled arthroscopic intervention. As the techniques have matured, arthroscopy has demonstrated reduced post-operative morbidity, faster rehabilitation, and improved cosmesis compared to many traditional open procedures, contributing to its widespread adoption and continued refinement within the subspecialty.
Surgical Anatomy & Biomechanics
A thorough understanding of wrist anatomy, particularly the topographical relationships of dorsal extensor compartments and the neurovascular structures, is paramount for safe and effective wrist arthroscopy. The standard portals for wrist arthroscopy are predominantly dorsal ( FIG 1A-C ), a choice dictated by the relative lack of major neurovascular structures dorsally and the initial clinical emphasis on assessing volar radiocarpal ligaments and articular cartilage. These dorsal portals are strategically named in relation to the tendons of the dorsal extensor compartments.
Radiocarpal Portals
The primary radiocarpal portals are:
-
1-2 Portal:
Situated between the first extensor compartment (extensor pollicis brevis (EPB) and abductor pollicis longus (APL)) and the second extensor compartment (extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB)) (
FIG 1D
). This portal offers excellent views of the scaphoid fossa of the radius, the radioscaphocapitate ligament, and the volar capsule. It is utilized as a viewing portal or for instrument insertion for procedures such as scaphoid fracture reduction. Care must be taken to avoid injury to the superficial radial nerve branches.

- 3-4 Portal: Located between the third extensor compartment (extensor pollicis longus (EPL)) and the fourth extensor compartment (extensor digitorum communis (EDC) and extensor indicis proprius (EIP)). This is typically the primary viewing portal for radiocarpal arthroscopy, providing an excellent panoramic view of the lunate fossa, the scapholunate ligament, and the central TFCC.
- 4-5 Portal: Positioned between the fourth extensor compartment (EDC, EIP) and the fifth extensor compartment (extensor digiti minimi (EDM)). This portal is often used for instrument insertion, particularly for procedures involving the lunate, lunotriquetral interval, and ulnar side of the TFCC.
- 6R Portal (Radial 6th Compartment): Located radial to the extensor carpi ulnaris (ECU) tendon (sixth compartment). This portal provides access to the ulnar aspects of the radiocarpal joint, including the radial attachment of the TFCC and the lunotriquetral ligament.
- 6U Portal (Ulnar 6th Compartment): Located ulnar to the ECU tendon. This portal is less commonly used for routine radiocarpal viewing but can be instrumental for direct access to the ulnar aspects of the TFCC and the DRUJ. The dorsal cutaneous branch of the ulnar nerve is at heightened risk with this portal.
Midcarpal Portals
Midcarpal arthroscopy provides visualization of the articulation between the proximal and distal carpal rows.
- Midcarpal Radial (MCR) Portal: Located just distal to the scaphoid tubercle, along the line of the third metacarpal. This portal provides visualization of the radioscaphocapitate and scaphotrapeziotrapezoid joints. It offers good access to the scapholunate interval from the midcarpal side.
- Midcarpal Ulnar (MCU) Portal: Positioned just distal to the triquetrum, often in line with the fourth or fifth metacarpal. This is the primary midcarpal viewing portal, offering excellent views of the lunocapitate and triquetrohamate joints, the intrinsic midcarpal ligaments, and the midcarpal aspect of the lunotriquetral interval.
Distal Radioulnar Joint (DRUJ) Portals
Arthroscopy of the DRUJ is performed through specific portals to assess and treat pathologies of the TFCC, articular cartilage, and joint stability.
- DRUJ Dorsal Portal: Typically created directly dorsal to the DRUJ, often through a separate incision from the radiocarpal portals, to allow a clear view of the foveal and stout attachments of the TFCC. Care must be exercised to avoid the dorsal cutaneous branch of the ulnar nerve.
- DRUJ Ulnar Portal: Located just ulnar to the ECU tendon, distal to the ulnar styloid. This portal can provide alternative views or instrument access for DRUJ pathology.
Understanding the relationship of the portals to superficial neurovascular structures is critical. The superficial radial nerve (SRN) and its branches are at risk with radial-sided portals (1-2, 3-4), while the dorsal cutaneous branch of the ulnar nerve (DCBUN) is vulnerable with ulnar-sided portals (4-5, 6R, 6U, DRUJ portals). Tendons of the extensor compartments must be carefully retracted, not violated, during portal creation.

Illustration of dorsal wrist anatomy and common portal placements relative to extensor compartments.

Detailed anatomical overlay depicting neurovascular structures in relation to dorsal arthroscopic portals.
Biomechanics
The wrist is a complex biomechanical unit, linking the forearm to the hand. Its primary articulations are the radiocarpal and midcarpal joints, with the DRUJ facilitating forearm rotation.
*
Radiocarpal Joint:
Primarily allows flexion-extension and radial-ulnar deviation. The distal radius articulates with the scaphoid and lunate. The TFCC, situated between the distal ulna and the carpus, acts as a critical stabilizer, distributing load and allowing smooth rotation of the forearm.
*
Midcarpal Joint:
Connects the proximal carpal row (scaphoid, lunate, triquetrum) to the distal carpal row (trapezium, trapezoid, capitate, hamate). It contributes significantly to overall wrist motion and stability, particularly through the intricate network of intrinsic ligaments (e.g., scapholunate interosseous ligament (SLIL), lunotriquetral interosseous ligament (LTIL)).
*
DRUJ:
A trochoid joint that permits pronation and supination of the forearm. Stability is largely conferred by the TFCC, which comprises articular disc, dorsal and volar radioulnar ligaments, meniscus homologue, ECU subsheath, and the floor of the 6th extensor compartment.
Pathologies such as TFCC tears, scapholunate dissociation, and lunotriquetral instability profoundly disrupt normal wrist kinematics, leading to pain, decreased range of motion, and progressive arthrosis if left untreated. Arthroscopy allows direct visualization and often repair or reconstruction of these critical structures.
Indications & Contraindications
Wrist arthroscopy is indicated for a broad spectrum of wrist pathologies, both diagnostic and therapeutic.
Indications for Wrist Arthroscopy
-
Diagnostic Arthroscopy:
- Unexplained chronic wrist pain unresponsive to conservative management.
- Assessment of subtle ligamentous injuries (e.g., dynamic scapholunate instability not evident on static imaging).
- Evaluation of chondral lesions.
- Biopsy of synovial tissue (e.g., for inflammatory conditions).
-
Therapeutic Arthroscopy:
-
Triangular Fibrocartilage Complex (TFCC) Pathology:
- Debridement of partial tears (Palmer Type 1A, 1B, 1C, 1D if symptomatic).
- Repair of peripheral TFCC tears (Palmer Type 1B) (e.g., using outside-in or all-inside techniques).
- Arthroscopic wafer resection for ulnar impaction syndrome.
-
Ligamentous Instability:
- Diagnostic assessment and confirmation of scapholunate (SLIL) and lunotriquetral (LTIL) ligament tears.
- Assisted repair or reconstruction of SLIL/LTIL injuries (e.g., capsulodesis, tendon graft reconstruction).
- Management of carpal instability non-dissociative (CIND).
-
Intracarpal Fractures:
- Assisted reduction and internal fixation of scaphoid fractures (e.g., percutaneous screw fixation).
- Diagnostic assessment of associated carpal ligament injuries in scaphoid or other carpal fractures.
- Removal of loose bodies or fracture fragments.
-
Distal Radius Fractures:
- Diagnostic assessment of associated intracarpal injuries (TFCC, scapholunate, lunotriquetral tears).
- Articular surface evaluation and impaction fracture reduction assistance.
- Management of intra-articular step-off and gap.
-
Synovitis/Inflammatory Conditions:
- Arthroscopic synovectomy (e.g., rheumatoid arthritis, pigmented villonodular synovitis).
- Removal of loose bodies.
-
Ganglion Cysts:
- Arthroscopic excision of dorsal wrist ganglions (originating from scapholunate ligament or radioscaphoid articulation).
-
Chondral Lesions:
- Debridement of chondral flaps or unstable cartilage.
- Microfracture for focal cartilage defects.
-
Infection:
- Septic arthritis irrigation and debridement.
-
Triangular Fibrocartilage Complex (TFCC) Pathology:
Contraindications
-
Absolute Contraindications:
- Active infection in the surgical field or systemic sepsis.
- Severe, rapidly progressing inflammatory arthritis with profound capsular destruction.
- Significant ankylosis or severely limited range of motion precluding instrumentation.
- Extensive soft tissue injury or open wounds in the portal areas.
-
Relative Contraindications:
- Severe wrist instability (arthroscopy may exacerbate, requiring open stabilization).
- Significant osteophyte formation that restricts visualization or instrument passage.
- History of complex regional pain syndrome (CRPS) in the affected limb (proceed with extreme caution and thorough patient counseling).
- Poor skin quality or scarring in portal regions.
- Unrealistic patient expectations regarding outcome.
Operative vs. Non-Operative Indications
| Condition | Operative (Arthroscopic) Indications | Non-Operative Indications |
|---|---|---|
| Chronic Wrist Pain (Undiagnosed) | Persistent pain >3-6 months unresponsive to conservative care; suspicion of occult ligamentous or chondral injury. | Recent onset of pain; mild, intermittent pain; pain resolving with rest, NSAIDs, activity modification, splinting, corticosteroid injections. |
| TFCC Tears | Symptomatic Palmer Type 1B tears (ulnar avulsion) for repair; symptomatic Palmer Type 1A, 1C, 1D tears for debridement; symptomatic Type 2C/D (degenerative) tears for debridement or wafer resection if associated with ulnar impaction. | Asymptomatic tears; Type 1A, 1C, 1D tears with mild symptoms responding to conservative management (splinting, NSAIDs, injections); Type 2A/B degenerative tears without significant pain or mechanical symptoms. |
| Ligamentous Instability (SLIL, LTIL) | Symptomatic, dynamic instability; acute, repairable tears (e.g., SLIL Geissler Grade III/IV); chronic tears requiring reconstruction. Concurrent TFCC tears requiring management. | Asymptomatic tears; low-grade sprains (Geissler Grade I/II) responding to immobilization and rehabilitation; advanced carpal collapse (SNAC/SLAC wrist) where arthrodesis or other salvage procedure is more appropriate. |
| Distal Radius Fractures | Intra-articular step-off/gap >1-2mm; associated TFCC or carpal ligament injury requiring repair; complex articular fracture patterns requiring direct visualization for reduction; comminution impeding fluoroscopic accuracy. | Nondisplaced or minimally displaced extra-articular fractures; intra-articular fractures with minimal step-off (<1mm) or gap managed adequately with closed reduction and casting; patients with severe comorbidities precluding surgery. |
| Scaphoid Fractures | Displaced or unstable fractures (e.g., >1mm displacement, humpback deformity, large gap); nonunions; associated ligamentous injuries; patients desiring early return to activity. | Nondisplaced or minimally displaced waist fractures (<1mm displacement, no humpback deformity) managed with casting; proximal pole fractures managed with casting if stable. |
| Ganglion Cysts | Symptomatic cysts (pain, mass effect, nerve compression) refractory to aspiration and observation; cosmetic concerns in select patients; recurrent cysts. | Asymptomatic cysts; first-time occurrence of symptoms (often resolves spontaneously); cysts responsive to aspiration (though recurrence rates are high). |
| Synovitis/Loose Bodies | Persistent synovitis refractory to medical management; mechanical symptoms from loose bodies; specific inflammatory diagnoses requiring biopsy/debridement (e.g., PVNS). | Asymptomatic or mildly symptomatic synovitis responding to NSAIDs, activity modification; asymptomatic loose bodies discovered incidentally. |
| DRUJ Pathology | TFCC tears involving the foveal attachment; articular cartilage pathology; instability requiring stabilization (e.g., capsular plication). | Mild DRUJ pain/instability responsive to rest, splinting, NSAIDs, physiotherapy; degenerative changes without significant mechanical symptoms; severe arthrosis requiring open reconstruction or fusion. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are fundamental to the successful execution of wrist arthroscopy, minimizing complications and optimizing surgical access.
Pre-Operative Planning
- Clinical Assessment: A comprehensive history and physical examination are critical. Documentation of range of motion, neurovascular status, specific pain patterns, and provocative tests (e.g., TFCC load test, grind test, Watson scaphoid shift test) is essential.
-
Imaging Review:
- Plain Radiographs: Standard anteroposterior, lateral, oblique, and scaphoid views are mandatory to assess carpal alignment, rule out fractures, and evaluate degenerative changes. Dynamic views may demonstrate instability.
- MRI: Often the cornerstone for evaluating soft tissue pathology, including TFCC tears, intrinsic ligament injuries (SLIL, LTIL), and occult fractures or bone contusions. High-resolution 3T MRI is preferred.
- CT Scan: Indicated for detailed assessment of bony anatomy, particularly in comminuted distal radius or scaphoid fractures, and for evaluating DRUJ congruity. CT arthrography can be useful for subtle ligamentous injuries.
- Arthrogram: Less commonly used with advancements in MRI, but can be helpful for confirming TFCC or intercarpal ligament tears if MRI is inconclusive or contraindicated.
-
Anesthesia Considerations:
- Regional Anesthesia: An interscalene or supraclavicular block (often combined with general anesthesia) provides excellent post-operative pain control and allows for intra-operative patient cooperation if dynamic assessment is required.
- General Anesthesia: Provides patient immobility, which can be advantageous for complex or prolonged cases.
- LMA (Laryngeal Mask Airway) or Endotracheal Tube: Selection based on duration of surgery and patient comorbidities.
- Equipment Check: Ensure all necessary arthroscopic equipment is available and functional, including various cannula sizes, shaver blades, burrs, suture passers, grasping forceps, and specialized instruments for specific repairs (e.g., TFCC repair kits). A high-definition camera system and monitor are crucial.
Patient Positioning
- Supine Position: The patient is placed supine on the operating table.
- Arm Table/Hand Table: The affected extremity is positioned on a radiolucent arm table or specialized hand table, allowing for full pronation/supination of the forearm.
- Tourniquet: A pneumatic tourniquet is applied high on the upper arm. Exsanguination with an Esmarch bandage and inflation to appropriate pressure (e.g., 250 mmHg) are standard.
-
Traction Tower Application:
A vertical traction tower (e.g., Chinese finger traps for digits 2-5, or specialized traction apparatus for the wrist) is applied to maintain wrist distraction. This typically involves 10-15 lbs (4.5-6.8 kg) of traction applied to the digits (usually index and long fingers, sometimes ring finger for additional distraction) with the elbow flexed 90 degrees and the forearm pronated 70-90 degrees. Traction creates space within the joint, facilitating portal creation and instrument manipulation. Distraction should be maintained throughout the procedure.

Typical patient setup with traction tower for wrist arthroscopy. - Draping: Standard sterile draping ensures a broad sterile field. The tourniquet cuff should be incorporated into the drape.
- Anatomical Landmarks: Prior to inflation of the tourniquet, palpate and mark key anatomical landmarks including the radial styloid, Lister's tubercle, ulnar styloid, extensor compartment tendons, and the anticipated portal sites. This pre-tourniquet marking is essential as landmarks can become obscured or less distinct under traction and after infiltration of local anesthetic/distension fluid.
- Wrist Distension: Prior to portal creation, the radiocarpal joint is distended with 5-10 mL of sterile saline solution injected via a 20-gauge needle dorsal to the extensor carpi ulnaris (ECU) tendon (into the 6R portal area) or directly into the 3-4 portal space. This hydrodistension helps to separate the articular surfaces and posterior capsule from neurovascular structures, making portal entry safer. Confirmation of intra-articular placement is typically achieved by easy injection and visible wrist swelling.
Detailed Surgical Approach / Technique
The execution of wrist arthroscopy requires a systematic approach, beginning with careful portal placement and progressing through diagnostic sweeps to targeted therapeutic interventions.
I. Joint Distension and Initial Portal Creation
- Hydrodistension: With the wrist under traction, inject 5-10 mL of saline into the radiocarpal joint (e.g., via the 3-4 portal interval). This distends the joint capsule and creates a safe working space.
-
3-4 Portal Creation (Primary Viewing Portal):
- Identify the interval between the EPL (3rd compartment) and EDC (4th compartment) tendons. Lister's tubercle is a reliable landmark.
- Infiltrate local anesthetic. Make a small (3-5 mm) skin incision with a #11 blade.
- Carefully advance a sharp arthroscopic trocar and cannula, perpendicular to the skin, aiming toward the scaphoid tubercle. Once through the capsule, the inflow of saline confirms intra-articular position.
- Remove the sharp trocar and insert the blunt trocar. Advance it to ensure no impingement.
- Insert the 2.7 mm or 2.9 mm 30-degree arthroscope, connected to the camera and irrigation pump. Maintain continuous inflow.
II. Diagnostic Radiocarpal Arthroscopy
A systematic diagnostic sweep is crucial to assess all compartments and identify pathology.
- Scaphoid Fossa: Evaluate the radial styloid, scaphoid fossa of the radius, and the articular cartilage of the scaphoid.
- Lunate Fossa: Sweep the arthroscope ulnarly to visualize the lunate fossa, the articular cartilage of the lunate, and the central portion of the TFCC.
-
Scapholunate (SL) Interval:
Examine the SLIL from the radial aspect of the joint. Assess its integrity, tension, and any tears.

Arthroscopic view of the scapholunate interval, assessing ligament integrity. - Lunotriquetral (LT) Interval: Continue sweeping ulnarly to visualize the LTIL and the ulnar structures.
- TFCC Evaluation: A comprehensive evaluation of the TFCC is paramount. Examine its radial attachment to the sigmoid notch, central articular disc (inspecting for tears, fraying), and the foveal and stout attachments to the ulnar head. A probe inserted through an accessory portal is essential for dynamic assessment of TFCC stability and integrity.
- Volar Ligaments: Though dorsal portals offer indirect views, gross tears of volar extrinsic ligaments can sometimes be appreciated.
III. Secondary Portal Creation
Secondary portals are created under direct arthroscopic visualization for safe instrument insertion.
-
2-3 Portal:
Often used for instrument insertion or outflow. Located between the second (ECRL, ECRB) and third (EPL) extensor compartments. Visualize the light from the arthroscope through the skin as a guide. Advance a needle first to confirm safe trajectory, then make a skin incision and insert a blunt trocar and cannula.

Schematic showing common dorsal portal placements, aiding in selection for specific interventions. - 4-5 Portal: Used as an instrument portal for ulnar-sided pathology (TFCC, LTIL). Located between the fourth (EDC, EIP) and fifth (EDM) extensor compartments. Visualize internally, palpate externally, and use a needle for safe entry.
- 6R Portal: Radial to the ECU tendon. Valuable for TFCC debridement, repair, and ulnar-sided views.
- 1-2 Portal: Radial to the ECRL. Primarily for scaphoid fracture work or volar capsular assessment. Requires meticulous care due to SRN proximity.
IV. Therapeutic Procedures
A. TFCC Debridement and Repair
- Debridement: For Palmer Type 1A, 1C, or stable degenerative tears, a shaver or radiofrequency ablator is introduced via an instrument portal (e.g., 4-5 or 6R). Unstable, frayed, or torn central portions are carefully debrided to a stable rim.
-
Repair (Palmer Type 1B):
For peripheral avulsions from the distal ulna.
- Outside-In Technique: A spinal needle is passed from outside-in, through the torn TFCC, and retrieved inside the joint via the instrument portal. Suture material is then passed through the needle, grasped inside the joint, and brought out through the other side of the TFCC. This suture is then tied over the capsule after knotting.
- All-Inside Technique: Specialized all-inside suture passers are used to place sutures across the tear and secure them to the capsule or bone.
-
Foveal Reattachment:
For avulsion from the fovea, suture anchors can be placed directly into the fovea and sutures passed through the TFCC. This often requires DRUJ arthroscopy.

Arthroscopic view illustrating a TFCC tear (Palmer Type 1B) undergoing repair with sutures.
B. Ligament Repair/Reconstruction
- SLIL Repair: For acute, repairable tears (Geissler Grade III/IV), various techniques exist. This may involve direct repair with sutures, capsulodesis, or bone-ligament-bone grafts. Arthroscopic-assisted approaches facilitate reduction and precise suture placement. Suture anchors may be used.
- LTIL Repair: Similar principles apply, though less common.
C. Fracture Management
- Distal Radius Fractures: Arthroscopy provides invaluable direct visualization of articular step-offs and gaps in intra-articular distal radius fractures. Under arthroscopic guidance (via 3-4, 4-5 portals), impaction fragments can be elevated, and anatomical reduction confirmed. Provisional K-wire fixation can be performed, and the need for percutaneous or open plating assessed.
- Scaphoid Fractures: Arthroscopic assistance is valuable for reduction and percutaneous screw fixation of scaphoid fractures, especially those with comminution or displacement. The 1-2 portal is often used for instrument insertion, while 3-4 provides the view.
D. Ganglion Excision
- For dorsal wrist ganglions, the stalk connecting the cyst to its intra-articular origin (typically SLIL or radioscaphoid capsule) is identified. A shaver or burr is used to debride the stalk and a portion of the underlying capsule, effectively removing the cyst from its base.
E. Loose Body Removal and Synovectomy
- Loose bodies are identified and grasped with arthroscopic forceps, then removed.
- Synovectomy involves comprehensive debridement of hypertrophic synovium using a shaver, ensuring thorough removal while protecting articular cartilage and ligaments.
V. Midcarpal Arthroscopy
- MCU Portal (Primary Viewing): Located just distal to the triquetrum. Entry is similar to radiocarpal portals but directed towards the space between the lunate and capitate.
- MCR Portal (Instrument): Located distal to the scaphoid tubercle.
- Diagnostic Sweep: Assess the lunocapitate, triquetrohamate, and scaphotrapeziotrapezoid articulations. Evaluate intrinsic midcarpal ligaments, especially the SLIL from the midcarpal side (crucial for assessing SLAC wrist progression).
VI. DRUJ Arthroscopy
- DRUJ Dorsal Portal: Created dorsal to the DRUJ, just distal to the ulnar head. A separate traction setup or careful manipulation of the existing traction may be necessary to open the DRUJ.
-
Diagnostic Sweep:
Evaluate the TFCC attachments to the fovea and ulnar styloid. Assess articular cartilage of the ulnar head and sigmoid notch. Dynamic assessment of DRUJ stability under pronation/supination can be performed.

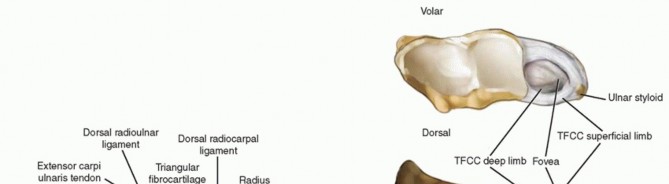
Arthroscopic image showing visualization of the DRUJ, including the TFCC attachment to the fovea.
VII. Closure
- Remove all instruments and the arthroscope.
- Allow excess fluid to egress.
- Portal sites are typically closed with a single skin suture (e.g., 4-0 nylon) or adhesive strips.
- Apply sterile dressings and a soft compressive bandage.
- Immobilization, if indicated, follows (e.g., splint or cast).
Complications & Management
While wrist arthroscopy is generally safe, a clear understanding of potential complications and their management strategies is essential for all practitioners.
I. Nerve Injury
-
Superficial Radial Nerve (SRN):
Most common nerve injury (incidence ~1-10%). Branches are vulnerable during radial-sided portal creation (1-2, 2-3, 3-4, MCR) and instrument manipulation.
- Prevention: Careful blunt dissection, pre-operative marking, adequate joint distension, small skin incisions, and direct arthroscopic visualization of internal structures.
- Management: Most are neurapraxias, resolving spontaneously. Persistent symptoms may warrant nerve conduction studies, EMG, and rarely, neurolysis. CRPS prophylaxis.
-
Dorsal Cutaneous Branch of Ulnar Nerve (DCBUN):
At risk during ulnar-sided portal creation (4-5, 6R, 6U, DRUJ dorsal).
- Prevention: Similar to SRN, ensure portals are centered dorsally in the anatomical interval, avoiding extreme ulnar or volar placement.
- Management: Similar to SRN.
- Other Nerves: Digital nerves (due to traction or direct trauma, rare), posterior interosseous nerve (PIN) during dorsal capsular debridement (very rare).
II. Tendon Injury
-
Extensor Tendons:
Can be lacerated or frayed by trocars, shavers, or burrs if not carefully retracted. Most vulnerable are EPL (3rd compartment) and EDC (4th compartment).
- Prevention: Precise portal placement within extensor compartments, blunt dissection, direct visualization.
- Management: Minor fraying may not require intervention. Significant lacerations may necessitate open repair depending on tendon involved and extent of injury.
III. Chondral Damage / Iatrogenic Articular Injury
-
Direct trauma to articular cartilage by instruments, particularly during initial portal entry or aggressive manipulation.
- Prevention: Always use blunt trocars once the capsule is breached. Maintain adequate joint distension. Avoid excessive force. Use appropriate instrument sizes.
- Management: Minor scuffs or small defects may heal. Larger, symptomatic defects may require microfracture or further arthroscopic debridement. Progressive pain may lead to early arthrosis.
IV. Extravasation / Compartment Syndrome
-
Excessive fluid extravasation into surrounding soft tissues (subcutaneous, muscle compartments) can lead to compartment syndrome or simply impede visualization due to swelling.
- Prevention: Use the lowest effective irrigation pressure. Ensure adequate outflow. Monitor wrist swelling. Limit procedure time.
- Management: Discontinue irrigation. Elevate extremity. If compartment syndrome suspected (rare but critical), immediate fasciotomy. More commonly, simple soft tissue swelling resolves with time.
V. Infection
-
Rare (incidence <1%), but serious. Risk factors include prolonged surgery, multiple portals, immune compromise.
- Prevention: Strict aseptic technique, prophylactic antibiotics.
- Management: Immediate irrigation and debridement, antibiotic therapy (IV and/or intra-articular), culture-directed treatment.
VI. Stiffness / Complex Regional Pain Syndrome (CRPS)
-
Stiffness:
Can result from post-operative pain, inadequate rehabilitation, excessive immobilization, or iatrogenic capsular scarring.
- Prevention: Early mobilization (when appropriate), robust pain management, patient education, diligent physical therapy.
- Management: Aggressive physiotherapy, splinting, NSAIDs, judicious use of steroid injections. Occasionally, arthroscopic capsular release.
-
CRPS:
A devastating potential complication.
- Prevention: Gentle tissue handling, good pain control (regional block), early mobilization, careful post-operative monitoring. Prophylactic Vitamin C may be considered.
- Management: Multidisciplinary approach involving pain specialists, physical therapists, occupational therapists. Pharmacological agents (gabapentin, amitriptyline), sympathetic blocks. Early recognition is key.
VII. Equipment Failure / Breakage
-
Shavers, burrs, or small instruments can break within the joint.
- Prevention: Inspect instruments pre-operatively. Avoid excessive force or bending.
- Management: Retrieve fragments immediately, often requiring extension of portal or conversion to mini-open arthrotomy.
Common Complications & Management Strategies
| Complication | Incidence | Management Strategies |
|---|---|---|
| Nerve Injury (Superficial Radial) | 1-10% | Most are neurapraxias; observe for spontaneous resolution (weeks to months). Educate patient on symptoms. Neuropathic pain management (gabapentin, pregabalin). Nerve conduction studies/EMG if persistent. Rarely, neurolysis. Consider CRPS prophylaxis. |
| Dorsal Cutaneous Ulnar Nerve | <1% | Similar to SRN injury. Conservative management generally effective. |
| Extensor Tendon Laceration/Fraying | <1% | Minor fraying: usually observation. Significant partial or complete laceration: often requires open repair, especially for EPL or EDC. Activity modification. |
| Iatrogenic Chondral Damage | <1% | Minor scuffs: observation, potentially microfracture if symptomatic. Larger defects: specific cartilage repair techniques (e.g., microfracture, OATS, ACI) if symptomatic and localized. Prognosis may worsen regarding future arthrosis. |
| Extravasation (Severe) | Rare (<0.1%) | Immediately cease irrigation. Elevate limb. Monitor for compartment syndrome (rare but emergency). If compartment syndrome diagnosed, immediate forearm fasciotomy. More commonly, resolves with time and elevation. |
| Infection (Septic Arthritis) | <1% | Prompt recognition. Immediate arthroscopic irrigation and debridement. Culture fluid/tissue. IV antibiotics tailored to sensitivities. Prolonged treatment course often required. |
| Joint Stiffness | 5-10% | Aggressive physical and occupational therapy. Dynamic and static splinting. NSAIDs. Oral corticosteroids in selected cases. Intra-articular steroid injection. Rarely, arthroscopic capsular release or manipulation under anesthesia. |
| Complex Regional Pain Syndrome | <1% (variable) | Early diagnosis and multidisciplinary management: pain specialists, physical therapy, occupational therapy, psychological support. Medications (NSAIDs, gabapentinoids, tricyclic antidepressants). Sympathetic nerve blocks. Aggressive pain control with regional anesthesia is a crucial preventative measure. |
| Instrument Breakage | Very rare | Immediate cessation of procedure. Attempt arthroscopic retrieval with specialized grasping forceps. If unsuccessful, convert to mini-open or open arthrotomy for removal. Document incident thoroughly. |
| Inadequate Visualization | Variable | Optimize traction, irrigation flow, and outflow. Reposition arthroscope or instruments. Clear hypertrophic synovium or hemorrhage with shaver. Consider additional or alternative portals. Re-distend joint. Patient with significant fibrosis/adhesions may require more aggressive debridement or open approach. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical determinant of functional outcome after wrist arthroscopy, demanding a structured, phased approach tailored to the specific procedure performed. The overarching goals are to reduce pain and swelling, restore range of motion (ROM), improve strength, and facilitate a safe return to activity.
General Principles
- Pain and Edema Control: Elevation, cryotherapy, and analgesics are initiated immediately post-operatively.
- Early Mobilization (for diagnostic or debridement procedures): For procedures not requiring prolonged immobilization, early, controlled active and passive ROM exercises are encouraged to prevent stiffness and promote synovial fluid circulation.
- Protection (for repairs/reconstructions): For procedures involving repair or reconstruction of ligaments (e.g., TFCC, SLIL), controlled protection through immobilization is paramount during the initial healing phases to allow soft tissue integration.
- Progression: Rehabilitation progresses from passive to active-assisted, then active ROM, followed by strengthening and proprioceptive exercises. The timeline for progression is dependent on tissue healing and surgeon's preference.
Phased Rehabilitation Protocols
Phase I: Immobilization and Protection (0-4/6 Weeks Post-Op)
- Applicable Procedures: TFCC repair, SLIL/LTIL repair/reconstruction, unstable fracture fixation, significant synovectomy.
- Goals: Protect healing tissues, control pain and swelling, prevent joint stiffness in adjacent un-operated joints.
-
Immobilization:
- TFCC Repair: Forearm-based sugar tong or long arm cast (pronated for dorsal tears, supinated for volar tears, neutral for central) for 4-6 weeks, often followed by a removable splint.
- Ligament Repair/Reconstruction: Forearm-based thumb spica cast or splint (for SLIL) or ulnar gutter cast (for LTIL) for 4-6 weeks.
- Fracture Fixation: Based on fracture stability and surgeon preference, typically 4-6 weeks in a cast or splint.
- Exercises (Adjacent Joints): Gentle active ROM for shoulder, elbow, and digits (MCP, PIP, DIP joints) several times daily to prevent stiffness.
- Pain Management: Continue analgesics, cryotherapy, elevation.
Phase II: Early Motion and Light Strengthening (4/6-12 Weeks Post-Op)
- Applicable Procedures: All procedures after initial immobilization (if any), or immediately for diagnostic/debridement procedures.
- Goals: Restore full, pain-free ROM, initiate muscle re-education, reduce swelling.
-
Mobilization:
- Active-Assisted ROM: Gentle flexion, extension, radial and ulnar deviation. Forearm rotation (pronation/supination) introduced gradually, especially cautiously after TFCC repair.
- Passive ROM: Gentle stretching by therapist or self-stretches as tolerated, avoiding forceful manipulation.
- Joint Mobilization: Soft tissue mobilization and joint glides by a therapist to improve capsular mobility.
-
Light Strengthening:
- Isometric Exercises: Gentle isometric contractions for wrist flexors, extensors, and forearm rotators (e.g., against resistance from the opposite hand).
- Theraband Exercises: Very light resistance for wrist flexion/extension.
- Grip Strengthening: Beginning with soft putty or sponge.
- Edema Control: Continue elevation, compression garments if needed.
- Modalities: Therapeutic modalities (ultrasound, electrical stimulation) as indicated by therapist for pain and healing.
Phase III: Progressive Strengthening and Functional Training (12 Weeks - 6 Months Post-Op)
- Applicable Procedures: All procedures as healing progresses.
- Goals: Achieve full functional strength, endurance, and dexterity. Prepare for return to specific activities.
-
Strengthening:
- Progressive Resistance Exercises: Gradual increase in resistance for wrist flexion/extension, radial/ulnar deviation, and forearm pronation/supination using weights, resistance bands, and specialized equipment.
- Forearm Strengthening: Exercises targeting brachioradialis, biceps, triceps.
- Grip and Pinch Strengthening: Using various tools and objects.
-
Proprioceptive and Dexterity Training:
- Balance Board/Weight-Bearing Exercises: Gradually introduce light weight-bearing through the wrist (e.g., tabletop pushes, wall pushes).
- Functional Activities: Incorporate tasks relevant to daily living and occupational needs (e.g., typing, lifting, tool use).
- Sport/Activity Specific Training: Gradually reintroduce sport-specific drills, ensuring proper technique and progressive loading.
- Cardiovascular Fitness: Maintain overall fitness.
Phase IV: Return to Activity (6 Months + Post-Op)
- Goals: Full, unrestricted return to all activities, including sports and heavy labor, as tolerated and approved by the surgeon.
-
Criteria for Return:
- Full, pain-free ROM comparable to the contralateral side.
- Strength at least 80-90% of the contralateral side.
- Absence of swelling, pain, or instability with activity.
- Successful completion of sport/activity-specific functional tests.
- Ongoing Conditioning: Continue a home exercise program to maintain strength and flexibility.
Important Considerations:
* Rehabilitation is highly individualized and must be guided by the patient's specific pathology, surgical findings, and progress.
* Close communication between the surgeon, therapist, and patient is essential.
* Patient adherence to the protocol is paramount for optimal outcomes.
* For advanced degenerative conditions, complete pain relief may not be achievable, and the focus shifts to functional improvement and pain management.
Summary of Key Literature / Guidelines
The body of literature supporting wrist arthroscopy has grown exponentially, establishing it as a primary diagnostic and therapeutic modality for a wide array of wrist pathologies. Contemporary guidelines emphasize evidence-based decision-making, patient selection, and meticulous surgical technique.
1. Diagnostic Efficacy:
Early literature, such as that by
Chen (1979)
, initially described the technique, primarily for diagnostic purposes. Subsequent studies by
Lichtman et al. (1986)
and
Slater et al. (1998)
highlighted its superiority over conventional imaging for diagnosing subtle intra-articular pathologies, particularly in cases of chronic wrist pain where plain radiographs, MRI, or CT failed to provide a definitive diagnosis. It remains the "gold standard" for direct visualization and dynamic assessment of intercarpal ligaments and articular cartilage.
2. TFCC Pathology:
Palmer (1981)
revolutionized our understanding of TFCC tears, classifying them into traumatic (Class 1) and degenerative (Class 2). Arthroscopic debridement of central tears (1A) and arthroscopic repair of peripheral tears (1B) are well-established. Studies by
Cooney et al. (1994)
and
Bednar et al. (1998)
demonstrated favorable outcomes with arthroscopic TFCC debridement for central tears. For peripheral tears,
Whipple et al. (1991)
pioneered arthroscopic repair, and meta-analyses by
Chang et al. (2014)
have shown comparable or superior results to open repair with potentially lower morbidity. Arthroscopic wafer resection for ulnar impaction syndrome, as described by
Paley and McMurtry (1992)
, is another effective, minimally invasive treatment option.
3. Ligamentous Instability:
Arthroscopy plays a crucial role in assessing and managing intercarpal ligamentous injuries, especially scapholunate (SLIL) and lunotriquetral (LTIL) instability.
Geissler et al. (1996)
developed an arthroscopic grading system for SLIL tears, which guides treatment decisions. For acute, repairable SLIL tears, arthroscopic-assisted repair or capsulodesis has been explored by
Rosenwasser et al. (2001)
and others, with emphasis on early intervention to prevent progressive carpal collapse (SNAC wrist). The literature supports arthroscopy for precise assessment, but chronic, high-grade instabilities often require open reconstruction or salvage procedures.
4. Fracture Management:
The utility of wrist arthroscopy in acute fracture management, particularly for distal radius and scaphoid fractures, has gained widespread acceptance.
Culp et al. (1994)
and
Graham (2001)
championed arthroscopy for assessing articular congruity, identifying concomitant ligamentous injuries (TFCC, SLIL) in distal radius fractures, and assisting in fragment reduction and fixation. For scaphoid fractures, arthroscopic-assisted percutaneous screw fixation, as described by
Haddad et al. (1999)
and
Slade and Dodds (2007)
, offers advantages such as direct visualization of the fracture site, reduction of associated soft tissue stripping, and accurate screw placement, potentially leading to faster union rates and reduced complications compared to blind percutaneous fixation.
5. Other Applications:
Arthroscopic ganglion excision, advocated by
Osterman et al. (1995)
, demonstrates lower recurrence rates than aspiration alone and avoids an open scar. Synovectomy for inflammatory or infectious conditions, debridement of chondral lesions, and removal of loose bodies are also well-documented and effective arthroscopic procedures.
6. Learning Curve and Training:
The intricate anatomy and technical demands of wrist arthroscopy necessitate a significant learning curve.
Trumble and Clarke (2002)
emphasized the importance of cadaveric training and mentorship. Modern educational guidelines stress the progressive acquisition of skills, starting with diagnostic arthroscopy and basic debridement before advancing to complex repairs or reconstructions. Simulation models are also increasingly utilized for skill development.
7. Future Directions:
Ongoing research focuses on advanced arthroscopic techniques for complex ligament reconstruction (e.g., all-arthroscopic SLIL reconstruction), biologic augmentation strategies for cartilage repair, and the application of smaller-diameter arthroscopes for highly confined spaces. The integration of advanced imaging modalities pre-operatively with real-time navigation during arthroscopy also holds promise for enhanced precision and safety.
In conclusion, wrist arthroscopy has evolved from a niche diagnostic procedure to a cornerstone of modern hand and wrist surgery. Its efficacy and safety are supported by extensive literature, provided that appropriate indications, meticulous technique, and comprehensive post-operative rehabilitation are employed.
Clinical & Radiographic Imaging


You Might Also Like