Orthopedic Ban Review | Dr Hutaif General Orthopedics R -...
14 Apr 2026
56 min read
82 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Ban Review | Dr Hutaif General Ort...
00:00
Start Quiz
Question 1High Yield
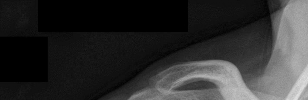
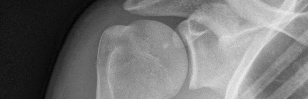
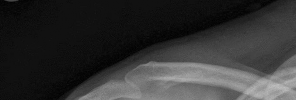
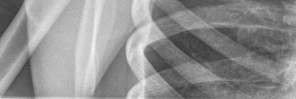
..Figure 19 is the radiograph of a 45-year-old right-hand-dominant man who has had a 2-day history of right shoulder pain, weakness, and a deformity involving the clavicle region after a fall from a scaffold during work activities. He was previously evaluated by his primary care physician and another orthopaedist. He has sought a second opinion regarding his treatment options. What is the most appropriate treatment for his injury?

Explanation
- Open reduction and plate fixation
Question 2High Yield
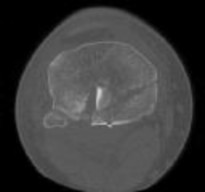
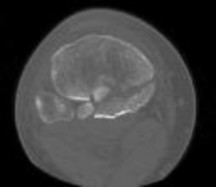
Six months later, the patient’s fracture has healed and a CT scan to further evaluate the physis is performed (Video 85). Based on these findings, how should you advise the family?
Explanation
The hypertrophic zone is the weakest biomechanical zone of the physis and is most likely to fracture. The deep peroneal nerve supplies motor innervation to the ankle and toe
dorsiflexors (anterior compartment) and the first web space, which, in this history, have deficits. The superficial peroneal nerve supplies sensation to the dorsum of the foot and motor to the lateral compartment peroneal musculature (ankle evertors), which also has deficits. The injury must involve both peroneal branches (the common peroneal nerve). Because sensation to the sole of the foot and toe/ankle plantar flexion is intact, the tibial nerve is intact.
Because the nerve was visualized intact, a neuropraxia is the most likely type of nerve injury. This should recover in time and does not necessitate urgent exploration. In pediatric patients, an advancing Tinel sign and partial nerve recovery by 3 months is expected and can be followed clinically. If there is no sign of nerve recovery, an electromyogram should be ordered with consideration for nerve exploration if there is no sign of reinnervation. There is no sign of compartment syndrome because the patient has an unchanged neurologic deficit, is comfortable, and has no pain with passive range of motion.
These injuries are associated with a very high rate of growth arrest (up to 80% in some studies). The CT scan shows an asymmetric growth arrest, which suggests angulation through the distal femur.
dorsiflexors (anterior compartment) and the first web space, which, in this history, have deficits. The superficial peroneal nerve supplies sensation to the dorsum of the foot and motor to the lateral compartment peroneal musculature (ankle evertors), which also has deficits. The injury must involve both peroneal branches (the common peroneal nerve). Because sensation to the sole of the foot and toe/ankle plantar flexion is intact, the tibial nerve is intact.
Because the nerve was visualized intact, a neuropraxia is the most likely type of nerve injury. This should recover in time and does not necessitate urgent exploration. In pediatric patients, an advancing Tinel sign and partial nerve recovery by 3 months is expected and can be followed clinically. If there is no sign of nerve recovery, an electromyogram should be ordered with consideration for nerve exploration if there is no sign of reinnervation. There is no sign of compartment syndrome because the patient has an unchanged neurologic deficit, is comfortable, and has no pain with passive range of motion.
These injuries are associated with a very high rate of growth arrest (up to 80% in some studies). The CT scan shows an asymmetric growth arrest, which suggests angulation through the distal femur.
Question 3High Yield
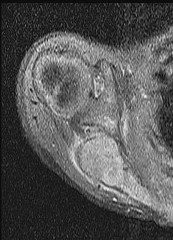
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?
Explanation
The history and MRI findings indicate the presence of anterior tibiotalar osteophytes. This is frequently observed in soccer, rugby, and football athletes who play on grass or turf surfaces and repetitively push off and change directions. Examination may reveal an effusion but no loss of subtalar motion. A positive external rotation (Klieger) test is described as pain at the distal ankle with external rotation of the foot and is observed in patients with syndesmosis sprains. This patient may have an increased anterior drawer because of a history of sprains; however, this finding is not specific for anterior impingement of tibiotalar osteophytes. The most specific finding on physical examination is pain with forced dorsiflexion.
REFERENCES: Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Cannon LB, Hackney RG: Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg 2000;39:383-386.
REFERENCES: Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Cannon LB, Hackney RG: Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg 2000;39:383-386.
Question 4High Yield
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
Patients with chronic ACL-deficient knees typically have lower than normal net quadriceps activity during the middle portion of the stance phase; the net moment about the knee reverses from one that demands quadriceps activity to one that demands increased hamstring activity. This type of gait is termed “quadriceps avoidance.” This avoidance is believed to be a functional adaptation to reduce anterior tibial translation, and it is most prevalent as the knee moves from 45° of flexion toward full extension, the arc of motion through which the ACL is most responsible for stability.
REFERENCES: Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20.
Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Solomonow M, Baratta R, Zhou BH, et al: The synergistic action of the anterior cruciate ligament and thigh muscles in maintaining joint stability. Am J Sports Med 1987;15:207-213.
REFERENCES: Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20.
Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Solomonow M, Baratta R, Zhou BH, et al: The synergistic action of the anterior cruciate ligament and thigh muscles in maintaining joint stability. Am J Sports Med 1987;15:207-213.
Question 5High Yield
When performing an arthroscopic Bankart repair in the lateral decubitus position, a surgeon notes a patulous capsule and a very lax anterior band of the inferior glenohumeral ligament. The surgeon decides that in addition to simply repairing the torn labrum, a capsular shift should be performed. The surgeon instructs the fellow assisting to take a “nice, big bite” of the capsule in this region to tighten the capsule upon repair. Which postoperative complication is most likely a result of this maneuver?
Explanation
The axillary nerve is at most risk in this area of the glenohumeral joint as it passes adjacent to and just inferior to the 6 o’clock position. Although performing capsular shifts within and up to 1 cm from the glenoid rim is generally considered safe, taking large amounts of capsule (>1 cm) in this region in an effort to tighten the capsule can inadvertently damage the nerve as it crosses there.
The musculocutaneous nerve does not cross in this region, although it can be injured during dissection around the coracoid, such as in arthroscopic Latarjet procedures. The musculocutaneous nerve branches to the lateral cutaneous nerve and provides sensory innervation to the lateral aspect of the forearm.
70
The suprascapular nerve crosses superior and posterior to the glenoid and is at greatest risk during transglenoid screw placement in the anteroposterior directions. The suprascapular nerve innervates the supraspinatus and the infraspinatus. The radial nerve courses behind the humeral shaft and can be damaged during bicortical fixation in the anterior to posterior direction in this region. A radial nerve palsy would result in wrist extension weakness.
The musculocutaneous nerve does not cross in this region, although it can be injured during dissection around the coracoid, such as in arthroscopic Latarjet procedures. The musculocutaneous nerve branches to the lateral cutaneous nerve and provides sensory innervation to the lateral aspect of the forearm.
70
The suprascapular nerve crosses superior and posterior to the glenoid and is at greatest risk during transglenoid screw placement in the anteroposterior directions. The suprascapular nerve innervates the supraspinatus and the infraspinatus. The radial nerve courses behind the humeral shaft and can be damaged during bicortical fixation in the anterior to posterior direction in this region. A radial nerve palsy would result in wrist extension weakness.
Question 6High Yield
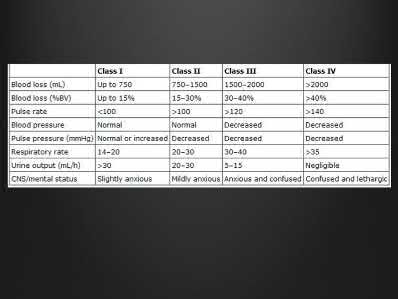
A 17-year-old football player is tackled with an opposing player's helmet hitting him hard in the abdomen. He is knocked backwards and suffers a diaphyseal femur fracture. He denies any loss of consciousness. Vital signs reveal a heart rate of 118, mean arterial pressure (MAP) of 68, and a respiration rate of 32 per minute. A FAST ultrasound study shows trace free fluid in the perisplenic space. A CBC taken prior to bolus IV fluids reveals a hematocrit of 48%, and a blood gas shows a lactate level of 1.8 and a base excess of -2.0. Which of the follow statements regarding the patient's hemodynamic status is correct?
Explanation
Normal lactate levels or base excess indicate adequate tissue perfusion.
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
Answer 1: While an arterial line is often helpful in the setting of
uncompensated hemodynamic shock, it would not be as important as measures of adequate tissue perfusion for ruling out compensated shock. Answer 2: The hematocrit is expected to stay normal for a short time even in the setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage
Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
Answer 1: While an arterial line is often helpful in the setting of
uncompensated hemodynamic shock, it would not be as important as measures of adequate tissue perfusion for ruling out compensated shock. Answer 2: The hematocrit is expected to stay normal for a short time even in the setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage
Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Question 7High Yield
rfl
I "
Figure 59a Figure 59b
A 12-year-old girl with foot pain who has been diagnosed with hereditary motor sensory neuropathy is seen for the foot deformity shown in Figure 59a. A “block test” is performed and shown in Figure 59b. What is the most appropriate management for this patient?
I "
Figure 59a Figure 59b
A 12-year-old girl with foot pain who has been diagnosed with hereditary motor sensory neuropathy is seen for the foot deformity shown in Figure 59a. A “block test” is performed and shown in Figure 59b. What is the most appropriate management for this patient?

Explanation
DISCUSSION: The hindfoot varus in this individual with a cavovarus deformity is nonstructural as shown by the “block test”. Therefore, surgical procedures directed at correcting the hindfoot deformity are not necessary. Observation is not in order and shoe modifications have not been shown to be effective in managing this problem. The patient is symptomatic; therefore, the treatment of choice is plantar release with first metatarsal osteotomy and possible tendon transfers.
REFERENCES: Paulos L, Coleman SS, Samuelson KM: Pes cavovarus: Review of a surgical approach
using selective soft-tissue procedures. J Bone Joint Surg Am 1980;62:942-953.
McCluskey WP, Lovell WW, Cummings RJ: The cavovarus foot deformity: Etiology and management. Clin Orthop Relat Res 1989;247:27-37.
Ward CM, Dolan LA, Bennett DL, et al: Long-term results of reconstruction for treatment of a flexible
cavovarus foot in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 2008;90:2631-2642.
50 • American Academy of Orthopaedic Surgeons
Figure 60a Figure 60b Figure 60c
REFERENCES: Paulos L, Coleman SS, Samuelson KM: Pes cavovarus: Review of a surgical approach
using selective soft-tissue procedures. J Bone Joint Surg Am 1980;62:942-953.
McCluskey WP, Lovell WW, Cummings RJ: The cavovarus foot deformity: Etiology and management. Clin Orthop Relat Res 1989;247:27-37.
Ward CM, Dolan LA, Bennett DL, et al: Long-term results of reconstruction for treatment of a flexible
cavovarus foot in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 2008;90:2631-2642.
50 • American Academy of Orthopaedic Surgeons
Figure 60a Figure 60b Figure 60c
Question 8High Yield
The major blood supply to the cruciate ligaments arises from which of the
following structures?
following structures?
Explanation
The major blood supply to the cruciate ligaments arises from the ligamentous branches of the middle genicular artery. Few terminal branches of the inferior genicular artery contribute to the blood supply. The synovial plexus and sheath covering the cruciate ligaments are also supplied by branches of the middle genicular artery. The blood supply to the cruciate ligaments is predominately of soft-tissue origin. There is no significant osseous vascular contribution to the ligaments.
REFERENCES: Arnoczky SP: Anatomy of the anterior cruciate ligament. Clin Orthop 1983;172:19-25.
Arnoczsky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
REFERENCES: Arnoczky SP: Anatomy of the anterior cruciate ligament. Clin Orthop 1983;172:19-25.
Arnoczsky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
Question 9High Yield
A 60-year-old woman is at the emergency department with a one-week history of thoracic back pain along with fevers >103°F. She notes that her legs are becoming slightly numb over the last 24 hours, but she is able to walk normally and she has a normal lower extremity motor examination. Her medical history is significant for diabetes mellitus. Her WBC is 13x109 cells/liter. She would like to avoid surgery. Her T1-weighted post gadolinium MRI scans are shown in Figures 1 and

Explanation
■
In a retrospective study of patients with epidural abscess from two academic medical centers, a predictive algorithm was developed to help identify which patients will develop a motor deficit. Multivariate analysis allowed points to be assigned to each risk factor. A sensory deficit was associated with 10 points; urinary retention/incontinence, 8 points; fecal incontinence/retention, 5 points; abscess above the conus medullaris, 4 points; diabetes, 2 points; WBC count >12x109 cells/liter, 2 points, and the presence of multiple epidural abscesses, 4 points. Smoking was not found to be predictive of a motor deficit. A dorsally based abscess was found to be protective of having a deficit, but a ventral or circumferential abscess was not. The use of steroids in the setting of infection is not recommended.
In a retrospective study of patients with epidural abscess from two academic medical centers, a predictive algorithm was developed to help identify which patients will develop a motor deficit. Multivariate analysis allowed points to be assigned to each risk factor. A sensory deficit was associated with 10 points; urinary retention/incontinence, 8 points; fecal incontinence/retention, 5 points; abscess above the conus medullaris, 4 points; diabetes, 2 points; WBC count >12x109 cells/liter, 2 points, and the presence of multiple epidural abscesses, 4 points. Smoking was not found to be predictive of a motor deficit. A dorsally based abscess was found to be protective of having a deficit, but a ventral or circumferential abscess was not. The use of steroids in the setting of infection is not recommended.
Question 10High Yield
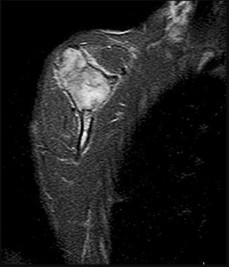
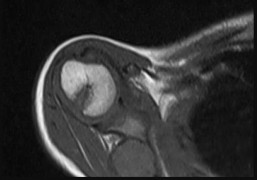
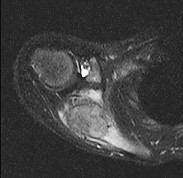
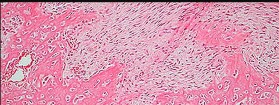
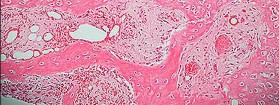
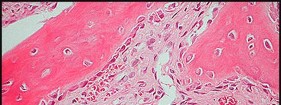
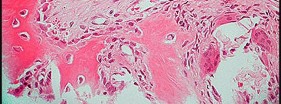
Figure 80a is the radiograph of a 5-year-old girl who has experienced 8 weeks of shoulder pain that is mostly relieved with nonsteroidal anti-inflammatory drugs. Her MR images are shown in Figures 80b through 80f. Histology is shown in Figures 80g through 80i. The most likely diagnosis is


Explanation
The combination of immature woven bone with osteoblastic rimming surrounded by a vascular fibrous bland stroma seen in Figure 80i and scattered giant cells within the lesion seen in Figure 80h should arouse suspicion for osteoblastoma. Osteoblastoma most often is diagnosed in adolescents and young adults, with 75% of patients younger than 25 years of age at diagnosis. Within tubular bones, osteoblastoma most often arises in the metadiaphyseal region, but it is more commonly seen in the spine within the posterior elements and flat bones. The lesion is well defined on radiographs, with lucent to mixed-lucent and blastic areas. MR imaging findings reveal low to intermediate–signal intensity on T1-weighted images and intermediate to high–signal intensity on T2-weighted images. Neoplastic woven bone can be seen in Figure 80g, and osteoclasts are shown in Figures 80h and 80i. Although the bone is expansile in appearance on radiologic studies, there are no large vascular lakes on histology to support the diagnosis of an aneurysmal bone cyst. Although there are areas of woven bone as in fibrous dysplasia, the appearance of osteoblastic rimming rules against this diagnosis. The location and histology of the tumor are inconsistent with giant-cell tumor of bone, the latter being a metaepiphyseal tumor histologically comprising giant cells within a background of stromal cells having nuclei identical to those of the giant cells. Ewing sarcoma would be a diagnostic consideration for a destructive scapular lesion in a 5-year-old, but the histology does not demonstrate the small, round blue-cell morphology of an Ewing sarcoma.
RECOMMENDED READINGS
63. Mirra JB. _Bone Tumors. Clinical, Radiologic, and Pathologic Correlations_. Philadelphia, PA: Lea & Febiger; 1989:391-418.
64. Nielsen GP, Rosenberg AE. _Diagnostic Pathology: Bone_. Manitoba, Canada: Amirsys; 2013:1-27.
RECOMMENDED READINGS
63. Mirra JB. _Bone Tumors. Clinical, Radiologic, and Pathologic Correlations_. Philadelphia, PA: Lea & Febiger; 1989:391-418.
64. Nielsen GP, Rosenberg AE. _Diagnostic Pathology: Bone_. Manitoba, Canada: Amirsys; 2013:1-27.
Question 11High Yield
When performing a radioscapholunate (RSL) fusion for posttraumatic radiocarpal arthritis, excision of the distal pole of the scaphoid will cause a decrease in
Explanation
RSL arthrodesis is a motion-sparing option for posttraumatic radioscaphoid or radiolunate arthritis when the midcarpal joint is preserved. Preserving the midcarpal joint allows the dart-thrower motion to remain. Mühldorfer-Fodor and associates reported that the rates of nonunion for RSL fusion were reduced by excision of the distal pole of the scaphoid. Multiple studies have shown increased radial and ulnar deviation with excision of the distal pole of the scaphoid; excision of the triquetrum further increases the radial-ulnar arc of motion. Bain and associates and Pervaiz and associates reported increased wrist
flexion-extension arcs with distal scaphoid and triquetrum excisions in cadaveric models; other authors _have reported no difference._
flexion-extension arcs with distal scaphoid and triquetrum excisions in cadaveric models; other authors _have reported no difference._
Question 12High Yield
Injuries to what two structures would result in a “floating shoulder"?
Explanation
The superior shoulder suspensory complex (SSSC) is a bone and soft-tissue ring secured to the trunk by superior and inferior bony struts, from which the upper extremity is suspended. The ring is composed of the glenoid process, coracoid process, coracoclavicular ligaments, distal clavicle, acromioclavicular joint, and acromial process. Double lesions of the SSSC are referred to as “floating shoulder” injuries, as in this case in which the injury involves a fractured scapular neck and ipsilateral clavicle fracture. Ipsilateral acromioclavicular dislocation and coracoid fracture is a less common double disruption of the SSSC. Although several case studies have been published on surgical and nonsurgical management of these injuries, no study provides measurable surgical indications beyond the simple presence of the double lesion. This is often referred to as an unstable shoulder girdle.
47
47
Question 13High Yield
While experts disagree whether the postpolio syndrome is caused by a reactivation of the dormant virus or by an attritional aging phenomena of muscles that have been overworked over a period of time, both groups recommend which of the following guidelines for optimizing function in this population?
Explanation
Most leaders in orthopaedic surgery support Jacqueline Perry’s theory that the postpolio syndrome is an attritional degenerative process that is the result of overuse of muscles and joints that are unable to adequately tolerate overload, and have little functional reserve. For that reason, aerobic conditioning and exercise are important. Overload and exhaustion of involved muscles should be avoided.
REFERENCE: Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
REFERENCE: Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
Question 14High Yield
A 15-year-old right-handed pitcher reports shoulder pain after throwing. His symptoms have been present for 3 months and have been getting progressively worse. Clinical examination shows no atrophy of the shoulder muscles, but he has pain with resisted motion of the shoulder, especially internal rotation. Radiographs are shown in Figures 73a and 73b. What is the next step in the evaluation and treatment of his shoulder pain?
Explanation
DISCUSSION: The patient has proximal humeral epiphyseolysis, otherwise known as “Little League shoulder.” This is an overuse injury of the shoulder in the skeletally immature overhead throwing athlete. Most frequently seen in pitchers, it usually develops after an increase in the amount or intensity of throwing activity. Initial treatment involves cessation of throwing activities so the proximal humeral growth plate injury can heal, followed by a gradual return to throwing.
REFERENCES: Chen FS, Diaz VA, Loebenberg M, et al: Shoulder and elbow injuries in the skeletally immature athlete. J Am Acad Orthop Surg 2005;13:172-185.
Keeley DW, Hackett T, Keims M, et al: A biomechanical analysis of youth pitching mechanics. J Pediatr Orthop 2008;28:452-459.
Sabick MB, Kim YK, Torry MR, et al: Biomechanics of the shoulder in youth baseball pitchers:
Implications for the development of proximal humeral epiphysiolysis and humeral retrotorsion. Am J Sports Med 2005;33:1716-1722.
REFERENCES: Chen FS, Diaz VA, Loebenberg M, et al: Shoulder and elbow injuries in the skeletally immature athlete. J Am Acad Orthop Surg 2005;13:172-185.
Keeley DW, Hackett T, Keims M, et al: A biomechanical analysis of youth pitching mechanics. J Pediatr Orthop 2008;28:452-459.
Sabick MB, Kim YK, Torry MR, et al: Biomechanics of the shoulder in youth baseball pitchers:
Implications for the development of proximal humeral epiphysiolysis and humeral retrotorsion. Am J Sports Med 2005;33:1716-1722.
Question 15High Yield
A 25 year-old-male presents with the injury seen in Figure A. Which of the following would be a contraindication to closed management with a functional brace?

Explanation
Closed treatment of humeral shaft fractures with functional bracing is indicated in the vast majority of isolated injuries. An ipsilateral brachial plexus injury, however, is a contraindication to nonoperative management in a functional brace.
Indications for operative management of humeral shaft fractures are limited given the high rates of union and ability of adjacent joints to compensate for deformity. Intact muscular tone is necessary to effect bony apposition in closed treatment with a functional brace. The absence of neurologic and muscle
function in patients with a flail extremity leads to increased rates of nonunion and malunion.
Rutgers and Ring conducted a retrospective review of patients managed with functional bracing of humeral shaft fractures at a single institution. The authors found a 90% overall union rate, with maintenance of shoulder and elbow motion. They caution though, that 29% of their proximal third fractures went on to nonunion.
Figure A demonstrates an AP radiograph of a comminuted humeral shaft fracture with varus alignment.
Incorrect Answers:
Answer 1: Radial nerve injury is not an indication for operative management as the vast majority of radial nerve injuries recover with conservative management
Answer 2: 1cm of shortening is an acceptable deformity with closed management
Answer 3: 20 degree varus deformity is not an indication for operative management
Answer 5: Fracture comminution is not a contraindication to functional bracing
Indications for operative management of humeral shaft fractures are limited given the high rates of union and ability of adjacent joints to compensate for deformity. Intact muscular tone is necessary to effect bony apposition in closed treatment with a functional brace. The absence of neurologic and muscle
function in patients with a flail extremity leads to increased rates of nonunion and malunion.
Rutgers and Ring conducted a retrospective review of patients managed with functional bracing of humeral shaft fractures at a single institution. The authors found a 90% overall union rate, with maintenance of shoulder and elbow motion. They caution though, that 29% of their proximal third fractures went on to nonunion.
Figure A demonstrates an AP radiograph of a comminuted humeral shaft fracture with varus alignment.
Incorrect Answers:
Answer 1: Radial nerve injury is not an indication for operative management as the vast majority of radial nerve injuries recover with conservative management
Answer 2: 1cm of shortening is an acceptable deformity with closed management
Answer 3: 20 degree varus deformity is not an indication for operative management
Answer 5: Fracture comminution is not a contraindication to functional bracing
Question 16High Yield
The primary advantage of the plantar approach for resection of interdigital neuromas is
Explanation
- better access to the neuroma.
Question 17High Yield
A right-hand-dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made and surgical treatment is chosen. The anatomic relationship of the distal biceps tendon to the median nerve and recurrent radial artery within the antecubital fossa is such that the biceps tendon travels
Explanation
DISCUSSION:
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on
the radial tuberosity.
DISCUSSION:
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on
the radial tuberosity.
Question 18High Yield
What range of motion parameters are required for a patient with posttraumatic elbow stiffness to accomplish all the normal activities of daily living?
Explanation
Activities of daily living such as dressing, eating, and bathing can all be performed with elbow motion through a 100 degrees arc of flexion and extension (30 degrees to 130 degrees) and a 100 degrees arc of forearm rotation (50 degrees pronation, 50 degrees supination). Some patients can accomplish these activities of daily living with 10 degrees less motion at each end point. This is referred to as the functional arc of motion.
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF, Askew LJ, Chao EY: A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63:872-877.
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF, Askew LJ, Chao EY: A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63:872-877.
Question 19High Yield
In an acute closed boutonniere injury, what is the most appropriate splinting technique for the proximal interphalangeal joint?
Explanation
Rupture of the central slip of the extensor mechanism and a varying degree of lateral band volar migration are the pathologic entities in an acute boutonniere injury. Splinting the proximal interphalangeal joint in full extension allows reapproximation of the central slip to the base of the middle phalanx. Distal interphalangeal joint flexion is permitted to allow movement of the lateral bands distally and dorsally, preventing contracture.
REFERENCES: Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Lovet WL, McCalla MA: Management and rehabilitation of extensor tendon injuries. Orthop Clin North Am 1983;14:811-826.
REFERENCES: Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Lovet WL, McCalla MA: Management and rehabilitation of extensor tendon injuries. Orthop Clin North Am 1983;14:811-826.
Question 20High Yield
A newborn infant in the nursery must be seen because of his foot. The dorsum of the foot rests against the tibia. The heel moves up when the forefoot moves down. Power is present in all muscles. The foot has an arch and the leg lengths are equal. The diagnosis is:
Explanation
C alcaneovalgus foot has all of these findings and resolves spontaneously.
Fibular hemimelia typically has less calcaneus attitude and more valgus and shortening. Vertical talus entails loss of an arch and loss of cohesive movement of the foot as a whole. There is no evidence of muscle weakness.
There is no evidence of a neuropathic component.
Fibular hemimelia typically has less calcaneus attitude and more valgus and shortening. Vertical talus entails loss of an arch and loss of cohesive movement of the foot as a whole. There is no evidence of muscle weakness.
There is no evidence of a neuropathic component.
Question 21High Yield
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp
anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus.
The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus.
The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
total knee arthroplasty.
Question 22High Yield
Figures 21a and 21b show the clinical photograph and radiograph of a 15-year-old girl who has a deformity of her feet. Her parents are concerned because there is a family history of Charcot-Marie-Tooth disease. The patient reports some mild instability of the ankle and has noticed mild early callosities; however, she is not having any significant pain. Coleman block testing reveals a forefoot valgus and supple hindfoot. She has weakness to eversion and dorsiflexion. Initial management should consist of
Explanation
Initial management of a young patient with a cavovarus deformity of the foot and a family history of Charcot-Marie-Tooth disease should focus on mobilization and strengthening of the weakening muscular units and an accommodative insert. Surgical intervention should be delayed until progression of the deformity begins to cause symptoms and/or weakness of the muscular units, resulting in contractures of the antagonistic muscle units.
REFERENCES: Pinzur MS: Charcot’s foot. Foot Ankle Clin 2000;5:897-912.
Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
REFERENCES: Pinzur MS: Charcot’s foot. Foot Ankle Clin 2000;5:897-912.
Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 23High Yield
A 57-year-old man has had a 2-week history of neck pain. He has no history of radiating symptoms, and has no complaints of numbness or paresthesias. There was no trauma associated with the onset of the pain. Figure 26 shows the MRI scan initially obtained by his family physician. What should the patient be told regarding the prevalence of the MRI findings in his age group?
Explanation
The MRI findings reveal age-related degenerative changes in the cervical spine, which is a very common finding in the adult population. Boden and associates evaluated cervical spine MRI findings on 63 asymptomatic subjects, and found that the prevalence of having at least one degenerative disk was approximately 57% in those older than age 40 years.
Question 24High Yield
An amputation through the wrist is an indication for attempted replantation.
Explanation
An amputation through the wrist, palm, or forearm is an indication for attempted replantation. The caliber of the vessels and other structures provides a favorable environment for reconstruction.
Question 25High Yield
What are some potential benefits of performing arthroscopiCcompared to open acromioplasty in a patient who develops impingement syndrome following hemiarthroplasty:
Explanation
ArthroscopiCacromioplasty has been used for the treatment of impingement following shoulder arthroplasty. It has the potential benefits of less tissue disruption, more rapid recovery, as well as increased ability to address intra-articular pathology compared to an open procedure.
Question 26High Yield
Which of the following clinical findings is most commonly present in a chronic exertional compartment syndrome of the anterior compartment of the leg?
Explanation
DISCUSSION: Chronic exertional compartment syndrome of the leg is characterized by pain (often burning in nature) of the involved compartment(s) (typically anterior) that worsens with activity and completely subsides within 15 minutes of activity cessation. A high index of suspicion is warranted for this condition. Intracompartmental pressure thresholds considered diagnostic are a 1-minute postexercise pressure of 30 mm Hg and a 5-minute post-exercise pressure of 20 mm Hg. This condition is not associated with the classic findings of an acute compartment syndrome. In this particular example, anterior leg pain with passive dorsiflexion of the toes and sensory loss of the plantar aspect of the foot would not be expected with an exertional compartment syndrome of the anterior compartment.
REFERENCES: Pedowitz RA, Hargens AR, Mubarek SJ, et al: Modified criteria for the objective diagnosis of chronic compartment syndrome of the leg. Am J Sports Med 1990;18:35-40.
Rorabeck CH, Fowler PJ, Nott L: The results of fasciotomy in the management of chronic exertional compartment syndrome. Am J Sports Med 1988;16:224-227.
REFERENCES: Pedowitz RA, Hargens AR, Mubarek SJ, et al: Modified criteria for the objective diagnosis of chronic compartment syndrome of the leg. Am J Sports Med 1990;18:35-40.
Rorabeck CH, Fowler PJ, Nott L: The results of fasciotomy in the management of chronic exertional compartment syndrome. Am J Sports Med 1988;16:224-227.
Question 27High Yield
Among patients with adolescent idiopathic scoliosis, a thoracolumbosacral orthosis is most effective for which type of curve?
Explanation
A thoracolumbosacral orthosis is most effective for bracing of curves when the apex is at T7 or below. Bracing is used for patients who are skeletally immature (Risser stage 0, 1, or 2), and it is recommended that the brace be worn 16 to 23 hours per day and continued until skeletal maturity or until the curve progresses to beyond 45 degrees, at which point bracing is no longer considered effective.
RECOMMENDED READINGS
Luhmann SJ, Skaggs DL: Pediatric spine conditions, in Lieberman JR (ed): AAOS Comprehensive Orthopaedic Review. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp 245-265.
[Shaughnessy WJ. Advances in scoliosis brace treatment for adolescent idiopathic scoliosis. Orthop Clin North Am. 2007 Oct;38(4):469-75, v. Review. PubMed PMID: 17945126. ](http://www.ncbi.nlm.nih.gov/pubmed/17945126)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17945126)
RECOMMENDED READINGS
Luhmann SJ, Skaggs DL: Pediatric spine conditions, in Lieberman JR (ed): AAOS Comprehensive Orthopaedic Review. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp 245-265.
[Shaughnessy WJ. Advances in scoliosis brace treatment for adolescent idiopathic scoliosis. Orthop Clin North Am. 2007 Oct;38(4):469-75, v. Review. PubMed PMID: 17945126. ](http://www.ncbi.nlm.nih.gov/pubmed/17945126)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17945126)
Question 28High Yield
A 32-year-old man underwent distal femur resection and endoprosthetic replacement at age 15 for high-grade conventional osteosarcoma. He was treated with neoadjuvant and adjuvant cisplatin, doxorubicin, and methotrexate. There has been no evidence of recurrent osteosarcoma, and he has been otherwise active and well. He is scheduled to undergo exchange of the polyethylene liner and bushings in his prosthesis because of wear that has caused recurrent effusions and a sensation of instability. Which study is most important to assess his perioperative medical risk?
Explanation
This patient was treated with doxorubicin, an anthracycline chemotherapy agent that causes cardiomyopathy in a dose-dependent fashion. Patients with osteosarcoma frequently undergo noninvasive cardiac testing with an echocardiogram or radionuclide angiography prior to anthracycline treatment. Cardiac toxicity is the typical cumulative dose-limiting effect of these agents. Posttreatment cardiac surveillance testing with an echocardiogram or radionuclide angiography is recommended for childhood cancer survivors treated with anthracyclines. Renal toxicity is a common adverse effect of cisplatin but usually manifests acutely. Similarly, methotrexate may cause acute hepatic toxicity that manifests acutely. In contrast, congestive heart failure attributable to doxorubicin cardiotoxicity frequently manifests late, with patients typically experiencing no or minimal symptoms until substantial cardiac dysfunction has occurred. Areflexia and peripheral neuropathy are also common side effects associated with these chemotherapeutic agents.
RECOMMENDED READINGS
65. Armenian SH, Hudson MM, Mulder RL, Chen MH, Constine LS, Dwyer M, Nathan PC, Tissing WJ, Shankar S, Sieswerda E, Skinner R, Steinberger J, van Dalen EC, van der Pal H, Wallace WH, Levitt G, Kremer LC; International Late Effects of Childhood Cancer Guideline Harmonization Group. Recommendations for cardiomyopathy surveillance for survivors of childhood cancer: a report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. 2015 Mar;16(3):e123-36. doi: 10.1016/S1470-2045(14)70409-7. Review. PubMed PMID: 25752563.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25752563)
66. [Longhi A, Ferrari S, Tamburini A, Luksch R, Fagioli F, Bacci G, Ferrari C. Late effects of chemotherapy and radiotherapy in osteosarcoma and Ewing sarcoma patients: the Italian Sarcoma Group Experience (1983-2006). Cancer. 2012 Oct 15;118(20):5050-9. doi: 10.1002/cncr.27493. Epub 2012 Mar 13. PubMed PMID: 22415578.](http://www.ncbi.nlm.nih.gov/pubmed/22415578)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22415578)
RECOMMENDED READINGS
65. Armenian SH, Hudson MM, Mulder RL, Chen MH, Constine LS, Dwyer M, Nathan PC, Tissing WJ, Shankar S, Sieswerda E, Skinner R, Steinberger J, van Dalen EC, van der Pal H, Wallace WH, Levitt G, Kremer LC; International Late Effects of Childhood Cancer Guideline Harmonization Group. Recommendations for cardiomyopathy surveillance for survivors of childhood cancer: a report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. 2015 Mar;16(3):e123-36. doi: 10.1016/S1470-2045(14)70409-7. Review. PubMed PMID: 25752563.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25752563)
66. [Longhi A, Ferrari S, Tamburini A, Luksch R, Fagioli F, Bacci G, Ferrari C. Late effects of chemotherapy and radiotherapy in osteosarcoma and Ewing sarcoma patients: the Italian Sarcoma Group Experience (1983-2006). Cancer. 2012 Oct 15;118(20):5050-9. doi: 10.1002/cncr.27493. Epub 2012 Mar 13. PubMed PMID: 22415578.](http://www.ncbi.nlm.nih.gov/pubmed/22415578)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22415578)
Question 29High Yield
An 8-year-old basketball player jumped up and felt a pop in his knee. He has diffuse anterior swelling and pain, and he is unable to perform a straight-leg raise. A small fleck of bone is seen distal to the patella on his radiograph.
Explanation
- Patellar sleeve fracture
Question 30High Yield
A 3-year-old girl has had pain and swelling in her left thigh for the past 3 weeks. Her mother states she has had a temperature as high as 100.4 degrees F (38 degrees C) and a weight loss of 5 pounds. A CBC shows a WBC count of 11,000/mm3, an erythrocyte sedimentation rate of 13 mm/h, and a C-reactive protein of 0.3. A radiograph is shown in Figure 2. What is the next step in management?
Explanation
The history and laboratory studies indicate that this is not an infection. A lesion in this location and in this age group is likely a Ewing’s sarcoma. The presentation is usually a painful mass. About 20% of patients have a fever. The radiograph shows a typical mottled, permeative lesion with periosteal reaction. An MRI scan should be obtained to further evaluate the soft-tissue mass. Staging of the lesion should take place before biopsy, which should be done by the surgeon who would be performing the next stage of surgical treatment, ideally an orthopaedic oncologist.
REFERENCES: Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Meyer JS, Nadel HR, Marina N, et al: Imaging guidelines for children with Ewing sarcoma and osteosarcoma: A report from the Children’s Oncology Group Bone Tumor Committee. Pediatr Blood Cancer 2008;51:163-170.
T
_AL-Madena Copy_
REFERENCES: Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Meyer JS, Nadel HR, Marina N, et al: Imaging guidelines for children with Ewing sarcoma and osteosarcoma: A report from the Children’s Oncology Group Bone Tumor Committee. Pediatr Blood Cancer 2008;51:163-170.
T
_AL-Madena Copy_
Question 31High Yield
Which of the following describes the inheritance pattern of Duchennes muscular dystrophy:
Explanation
| Autosomal dominant | Autosomal recessive | X-linked dominant | X-linked recessive |
|---|---|---|---|
| Achondroplasia | Sickle cell | Hypophosphatemic rickets | Hemophilia (A, B) |
| SED (congenital) | OI (II, III) | | Duchennes muscular dystrophy |
| MED | Hypophosphatasia | | Hunters syndrome |
| Marfan’s syndrome | Homocystinuria | | SED (tarda) |
| Ehlers-Danlos syndrome | Gaucher’s disease | | Becker’s muscular dystrophy |
Abbreviations: OI (I,IV)=Osteogenesis imperfecta, SED=Spondyloepiphyseal dysplasia, MED=Multiple epiphyseal dysplasia, MHE=Multiple hereditary exostosis
Abbreviations: OI (I,IV)=Osteogenesis imperfecta, SED=Spondyloepiphyseal dysplasia, MED=Multiple epiphyseal dysplasia, MHE=Multiple hereditary exostosis
Question 32High Yield
The mechanism for the osseous destruction is attributable to
Explanation
This scenario is a classic example of the development of Charcot foot. A red, swollen, deformed foot without ulceration suggests neuroarthropathy. Normal inflammatory marker findings, no history of fever or chills, and radiographs demonstrating bone loss support the diagnosis. Limb elevation with dramatic reduction in erythema is also characteristic of this disease process and does not occur with infection. Total-contact casting is the cornerstone of treatment for acute Charcot disease. Hemoglobin A1C is an indicator of glucose averaged over a 3-month period, providing the most reliable indication of a patient's ongoing glucose control. The pathophysiology of bone destruction is believed to be hypervascularity of bone. Infection and Charcot disease may develop simultaneously, but the combination is rare.
RECOMMENDED READINGS
[Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.](http://www.ncbi.nlm.nih.gov/pubmed/23919113)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23919113)
[Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052. ](http://www.ncbi.nlm.nih.gov/pubmed/16701052)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16701052)
RECOMMENDED READINGS
[Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.](http://www.ncbi.nlm.nih.gov/pubmed/23919113)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23919113)
[Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052. ](http://www.ncbi.nlm.nih.gov/pubmed/16701052)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16701052)
Question 33High Yield
An 8-year-old girl with a history of Down syndrome is being evaluated to participate in gym activities. She is otherwise doing well and has appropriate motor developmental milestones. Her neurological exam is normal and cervical spine AP, lateral, flexion and extension radiographs reveal an atlanto-dens interval (ADI) of 7 mm, and normal occipitoatlantal mobility. What is the most appropriate recommendation?
Explanation
■
Down syndrome, with an incidence of 1 in 660 live births, remains the most common human malformation pattern. Individuals with Down syndrome have an increased incidence of congenital heart disease, ophthalmologic disorders, gastrointestinal disorders, thyroid disease, and leukemia.
Musculoskeletal problems commonly occur in Down syndrome and include patellofemoral and hip instability, bunions, severe flatfoot, and instability of cervical spine, which could result in cord compromise and neurological impairment or death.
Increased ADI in the Down syndrome population has not been directly correlated with a concomitant increase in neurologic compromise. The radiographs of the cervical spine in the Down syndrome population must be evaluated by standards specific to that population, and not by traditional standards derived from the radiographs of the cervical spine in the general population. Radiographic evaluation of the cervical spine in the young athlete with Down syndrome is only one component of the preparticipation screening and must be correlated with a pertinent history of physical activity and a detailed physical exam.
When a Down patient presents with an ADI >10 mm and evidence of spinal cord compression, there is little disagreement about the need for surgical intervention. When the ADI is between 4.5 mm and 10 mm in a patient with no decrease in physical activities and no abnormal neurological finding, this may represent hypermobility rather than instability in the Down syndrome population. With an ADI between 4.5 mm and 10 mm, athletes with Down syndrome may participate in most activities but have been advised to avoid high-risk sports such as diving and football.
Down syndrome, with an incidence of 1 in 660 live births, remains the most common human malformation pattern. Individuals with Down syndrome have an increased incidence of congenital heart disease, ophthalmologic disorders, gastrointestinal disorders, thyroid disease, and leukemia.
Musculoskeletal problems commonly occur in Down syndrome and include patellofemoral and hip instability, bunions, severe flatfoot, and instability of cervical spine, which could result in cord compromise and neurological impairment or death.
Increased ADI in the Down syndrome population has not been directly correlated with a concomitant increase in neurologic compromise. The radiographs of the cervical spine in the Down syndrome population must be evaluated by standards specific to that population, and not by traditional standards derived from the radiographs of the cervical spine in the general population. Radiographic evaluation of the cervical spine in the young athlete with Down syndrome is only one component of the preparticipation screening and must be correlated with a pertinent history of physical activity and a detailed physical exam.
When a Down patient presents with an ADI >10 mm and evidence of spinal cord compression, there is little disagreement about the need for surgical intervention. When the ADI is between 4.5 mm and 10 mm in a patient with no decrease in physical activities and no abnormal neurological finding, this may represent hypermobility rather than instability in the Down syndrome population. With an ADI between 4.5 mm and 10 mm, athletes with Down syndrome may participate in most activities but have been advised to avoid high-risk sports such as diving and football.
Question 34High Yield
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right
groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?

Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
Question 35High Yield
If growth arrest is suspected after the fracture shown in the radiographs in Figures 17a through 17c, what is the most appropriate imaging modality to verify the presence of a physeal bar?



Explanation
Premature growth arrest of a physis may occur after fracture, infection, or ischemia. In the setting of fracture this is relatively rare, although certain physes have proven more susceptible than others. In the distal radius, premature growth arrest is more common after wide displacement, redisplacement, or manipulation after a fracture has begun to heal (> 7-10 days after injury). Arrest may take 6 to 12 months to become evident on radiographs and it may take even longer for a patient to experience pain or deformity, depending upon the rate of growth at the time of arrest. Surveillance should take place during the 6- to 12-month time frame with radiographs.
A physeal bar is difficult to rule in or out on radiographs because of natural undulations in the physis or a residual angular deformity after fracture that causes the physis to be less clearly visible. Often, the best clue that indicates physeal arrest after distal radius fracture is clinical prominence of the ulna head or increasing ulna-positive variance. The posteroanterior view of the wrist should be taken with the shoulder abducted to 90 degrees and elbow flexed to 90 degrees. This places the forearm in neutral rotation, and changes in ulnar variance can more accurately be detected. Comparison views of the other side may be warranted.
If a growth arrest is suspected, CT scan and MRI are both effective modalities for imaging the size and location of the bar. The bar is most easily detected on the T1-weighted MR images. Early, unossified cartilaginous bars also may be detected on some MRI sequences. MRI with 3D mapping functions is now used to map the size and location into an easy-to-visualize format, but the computer programs are not yet mainstream. A CT scan can demonstrate the bar but is not as acceptable because of the high dose of radiation (compared to MRI).
The physis has 3 main zones. The zone that is most important and susceptible to injury is the resting zone, where pluripotent chondrocytes reside. This layer is immediately adjacent to the epiphysis. If this layer is disrupted or ischemic, there is permanent growth arrest of that physis section. The central layer is the proliferative zone. The hypertrophic zone is the layer adjacent to the metaphysis and is subdivided into 3 layers: maturation, degeneration, and provisional calcification. The weakest link is the junction between the provisional calcification layer and the metaphysis. Most physeal fractures occur through this layer. Thus, growth arrest after fracture is rare because the level of injury typically is as far as possible from the delicate resting zone.
If growth arrest occurs after distal radius fracture, surgical intervention is tailored to the situation. If the child is young, an attempt at bar resection and interposition of fat or bone wax is appropriate. If a teenage child is asymptomatic and ulna variance is a few millimeters positive, simple ulna epiphysiodesis is appropriate. If there is deformity of the distal radius, corrective osteotomy may be best.
RECOMMENDED READINGS
6. [Abzug JM, Little K, Kozin SH. Physeal arrest of the distal radius. J Am Acad Orthop Surg. 2014 Jun;22(6):381-9. doi: 10.5435/JAAOS-22-06-381. Review. PubMed PMID: 24860134. ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860134)
7. [Craig JG, Cramer KE, Cody DD, Hearshen DO, Ceulemans RY, van Holsbeeck MT, Eyler WR. Premature partial closure and other deformities of the growth plate: MR imaging and three-dimensional modeling. Radiology. 1999 Mar;210(3):835-43. PubMed PMID: 10207489. ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10207489)
8. [Ecklund K, Jaramillo D. Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol. 2002 Apr;178(4):967-72. PubMed PMID: 11906884. ](http://www.ncbi.nlm.nih.gov/pubmed/11906884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11906884)
A physeal bar is difficult to rule in or out on radiographs because of natural undulations in the physis or a residual angular deformity after fracture that causes the physis to be less clearly visible. Often, the best clue that indicates physeal arrest after distal radius fracture is clinical prominence of the ulna head or increasing ulna-positive variance. The posteroanterior view of the wrist should be taken with the shoulder abducted to 90 degrees and elbow flexed to 90 degrees. This places the forearm in neutral rotation, and changes in ulnar variance can more accurately be detected. Comparison views of the other side may be warranted.
If a growth arrest is suspected, CT scan and MRI are both effective modalities for imaging the size and location of the bar. The bar is most easily detected on the T1-weighted MR images. Early, unossified cartilaginous bars also may be detected on some MRI sequences. MRI with 3D mapping functions is now used to map the size and location into an easy-to-visualize format, but the computer programs are not yet mainstream. A CT scan can demonstrate the bar but is not as acceptable because of the high dose of radiation (compared to MRI).
The physis has 3 main zones. The zone that is most important and susceptible to injury is the resting zone, where pluripotent chondrocytes reside. This layer is immediately adjacent to the epiphysis. If this layer is disrupted or ischemic, there is permanent growth arrest of that physis section. The central layer is the proliferative zone. The hypertrophic zone is the layer adjacent to the metaphysis and is subdivided into 3 layers: maturation, degeneration, and provisional calcification. The weakest link is the junction between the provisional calcification layer and the metaphysis. Most physeal fractures occur through this layer. Thus, growth arrest after fracture is rare because the level of injury typically is as far as possible from the delicate resting zone.
If growth arrest occurs after distal radius fracture, surgical intervention is tailored to the situation. If the child is young, an attempt at bar resection and interposition of fat or bone wax is appropriate. If a teenage child is asymptomatic and ulna variance is a few millimeters positive, simple ulna epiphysiodesis is appropriate. If there is deformity of the distal radius, corrective osteotomy may be best.
RECOMMENDED READINGS
6. [Abzug JM, Little K, Kozin SH. Physeal arrest of the distal radius. J Am Acad Orthop Surg. 2014 Jun;22(6):381-9. doi: 10.5435/JAAOS-22-06-381. Review. PubMed PMID: 24860134. ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860134)
7. [Craig JG, Cramer KE, Cody DD, Hearshen DO, Ceulemans RY, van Holsbeeck MT, Eyler WR. Premature partial closure and other deformities of the growth plate: MR imaging and three-dimensional modeling. Radiology. 1999 Mar;210(3):835-43. PubMed PMID: 10207489. ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10207489)
8. [Ecklund K, Jaramillo D. Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol. 2002 Apr;178(4):967-72. PubMed PMID: 11906884. ](http://www.ncbi.nlm.nih.gov/pubmed/11906884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11906884)
Question 36High Yield
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
The patient has an acute peroneal tendon dislocation. The evaluation for syndesmotic injury and lateral ankle instability is negative. The cortical avulsion off the distal tip of the lateral malleolus, a rim fracture, is characteristic of peroneal tendon dislocations. The sensation of apprehension or frank subluxation of the peroneal tendons with active dorsiflexion of the foot while the foot is held in plantar flexion confirms the diagnosis. Based on these findings, initial management should consist of cast immobilization and protected weight bearing. If a recurrent or chronic condition develops, surgery is the most reliable treatment option.
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
REFERENCES: Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Marti R: Dislocation of the peroneal tendons. Am J Sports Med 1977;5:19-22.
Question 37High Yield
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Initial treatment should consist of
Explanation
DISCUSSION:
This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. (Note: It may be necessary to splint the elbow in pronation if the medial collateral ligament [MCL] is intact and the lateral collateral ligament [LCL] is disrupted, or in supination if the LCL is intact but the MCL disrupted.) Surgical reconstruction of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If unstable after reconstruction,
application of a hinged external fixator may be considered.
DISCUSSION:
This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. (Note: It may be necessary to splint the elbow in pronation if the medial collateral ligament [MCL] is intact and the lateral collateral ligament [LCL] is disrupted, or in supination if the LCL is intact but the MCL disrupted.) Surgical reconstruction of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If unstable after reconstruction,
application of a hinged external fixator may be considered.
Question 38High Yield
What complication following total elbow arthroplasty poses more risk for a 60-year-old man with osteoarthritis than for a man of the same age with rheumatoid arthritis?
Explanation
Patients with primary elbow osteoarthritis tend to be active and are often involved in manual occupations that place greater demands on a total elbow implant. Such patients are most often treated with nonprosthetic options because of concerns about prosthetic longevity. As a result, few cases of primary osteoarthritis are included in published studies. However, complications such as stem fracture and aseptic loosening appear to be more common in this population than in any other subgroup, including revision patients. The poor soft-tissue quality associated with rheumatoid arthritis leads to a high-risk ligamentous attenuation and is a general contraindication to use of an unlinked implant. The same poor soft tissue leads to a higher rate of triceps insufficiency and wound dehiscence.
Question 39High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 3 through 8 are the axial and sagittal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 3 through 8 are the axial and sagittal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---








Explanation
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the
femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 40High Yield
Figures 1 and 2 are the most recent radiographs of an 18-year-old high school student who sustains an anterior shoulder dislocation playing recreational football. He has a low Beighton score on physical examination. He was closed reduced and underwent a course of physical therapy but had a second dislocation playing recreational basketball. What is the most appropriate course of treatment, with the lowest complication rate, to prevent further dislocation?


Explanation
The patient has recurrent instability and is at a high rate of further dislocations due to his young age. Therefore, therapy and bracing are unlikely to decrease his dislocation rate. The radiographs are normal, and there is no Hill-Sachs lesion or bony Bankart lesion. His instability severity index score is 3, and; therefore, a bony procedure such as Latarjet is not necessary. Furthermore, the rate of complication following a Latarjet procedure, especially nerve
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
Question 41High Yield
Figure 1 is the radiograph of a 54-year-old man who has increasing weakness and numbness in his lateral arm. No prior surgery or injury is reported. What is the most appropriate next diagnostic test?
Explanation
22
The radiograph reveals a Charcot neuropathic shoulder. The atraumatic destruction of the humeral head is concerning for a neuropathic etiology and warrants MR imaging of the cervical spine to evaluate for the presence of a syrinx. Shoulder arthroplasty in the setting of a neuropathic joint is challenging given the local bone and soft-tissue loss, in addition to the loss of protective sensation. The scant literature on the use of shoulder arthroplasty in these challenging patients reports an improvement in pain but only modest improvements in shoulder function.
The radiograph reveals a Charcot neuropathic shoulder. The atraumatic destruction of the humeral head is concerning for a neuropathic etiology and warrants MR imaging of the cervical spine to evaluate for the presence of a syrinx. Shoulder arthroplasty in the setting of a neuropathic joint is challenging given the local bone and soft-tissue loss, in addition to the loss of protective sensation. The scant literature on the use of shoulder arthroplasty in these challenging patients reports an improvement in pain but only modest improvements in shoulder function.
Question 42High Yield
Figure 54 is the lateral radiograph of a 55-year-old man who is evaluated for a 2-year history of pain and stiffness of his right metatarsophalangeal (MTP) joint. Upon examination he has dorsal bossing, severe crepitation, and pain
with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?
with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?



Explanation
The radiograph reveals end-stage degenerative changes of the first MTP joint with a dorsal loose body. MTP arthritis and decreased joint dorsiflexion is referred to as hallux rigidus. A chevron bunionectomy is used to correct hallux valgus deformity without arthritis. The cheilectomy is used in lesser degrees of joint destruction. Resection of the proximal phalanx results in a floppy toe and is generally not recommended.
RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23386758)
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2022661564)
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.
A B
RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23386758)
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2022661564)
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.
A B
Question 43High Yield
A 12-year-old patient with osteogenic sarcoma metastatic to the spine is noted to have new onset of weakness of both lower extremities. Magnetic resonance imaging shows a mass expanding posteriorly and encroaching on the spinal cord. The recommended initial step is:
Explanation
Radiation therapy combined with steroids should be tried first to try to halt progression of the tumor. Unfortunately, the prognosis for this child is extremely poor.
Increasing the dose of chemotherapy is not likely to work because the metastasis has already progressed despite initial treatment.
Surgical resection must be tried if radiation does not produce improvement. Steroids are an adjunct to treatment but not sufficient alone.
The patient is likely to have progressive paraparesis and loss of bowel function. In order to improve the quality of life remaining, surgical resection should be offered to the patient.
Increasing the dose of chemotherapy is not likely to work because the metastasis has already progressed despite initial treatment.
Surgical resection must be tried if radiation does not produce improvement. Steroids are an adjunct to treatment but not sufficient alone.
The patient is likely to have progressive paraparesis and loss of bowel function. In order to improve the quality of life remaining, surgical resection should be offered to the patient.
Question 44High Yield
What is the most likely diagnosis based on the MRI findings shown in Figures 87a and 87b?
Explanation
DISCUSSION: The MRI scans reveal increased signal in the medial facet of the patella and the anterior aspect of the lateral femoral condyle. This pattern is typically seen in patients with acute patellar dislocations. In patients with ACL tears, the bone bruise of the lateral femoral condyle is usually seen in the central portion at the sulcus terminalis and the posterior half of the lateral tibial plateau and is not usually seen in the patella. This pattern of bone bruising is not seen with patellar tendon ruptures, LCL tears, and PCL tears.
REFERENCES: Elias DA, White LM, Fithian DA: Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002;225:736-743.
Virolainen H, Visuri T, Kuusela T: Acute dislocation of the patella: MR findings. Radiology 1993;189:243-246.
REFERENCES: Elias DA, White LM, Fithian DA: Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002;225:736-743.
Virolainen H, Visuri T, Kuusela T: Acute dislocation of the patella: MR findings. Radiology 1993;189:243-246.
Question 45High Yield
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?
Explanation
Tillaux and triplane fractures occur in adolescents as the result of an external rotation injury of the ankle. As seen on the CT scan, the growth plate starts to close during adolescence; therefore, growth arrest resulting in limb-length discrepancy or angulation is less of a concern in this age group than achieving joint congruity. The joint should be surgically reduced if displacement is greater than 2 mm to minimize the chances of late arthrosis.
REFERENCES: Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment.
J Am Acad Orthop Surg 2001;9:268-278.
Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Duchesneau S, Fallat LM: The Tillaux fracture. J Foot Ankle Surg 1996;35:127-133.
REFERENCES: Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment.
J Am Acad Orthop Surg 2001;9:268-278.
Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Duchesneau S, Fallat LM: The Tillaux fracture. J Foot Ankle Surg 1996;35:127-133.
Question 46High Yield
Which of the following types of bone behaves in an isotropiCmanner when loaded in different directions:
Explanation
Woven bone is immature bone that is found in newborns, fracture callus, and the metaphyses of growing bone. In woven bone, the collagen fibers are oriented in a completely random fashion. When woven bone is loaded, it performs in an isotropiCmanner. The other types of bone (lamellar, cortical, cancellous, and plexiform) contain collagen that is oriented along the long axis of the bone and cause the bone to perform anisotropically.
Question 47High Yield
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include
Explanation
The displaced talar neck fracture should be treated with open reduction and internal fixation using screws. Closed reduction and casting will not maintain position, and percutaneous pinning is not able to maintain reduction to allow union. External fixation and amputation are not necessary for this injury unless there is severe soft-tissue loss.
REFERENCE: Adelaar RS: Fractures of the talus. Instr Course Lect 1990;39:147-156.
REFERENCE: Adelaar RS: Fractures of the talus. Instr Course Lect 1990;39:147-156.
Question 48High Yield
Figures 1 and 2 show the intraoperative photographs obtained during surgical treatment for de Quervain tendonitis. For orientation purposes, dorsal is at the top. Figure 1 is obtained just after the initial first extensor compartment release, and Figure 2 shows the floor of the first extensor compartment. If the structure marked by the black dot is not addressed, the most common postoperative problem would be

Explanation
The black dot identifies an accessory compartment of the extensor pollicis brevis (EPB) tendon. The incidence of accessory EPB compartment in patients undergoing surgical treatment for de Quervain syndrome ranges from 46% to 60%. Failure to release this compartment at the time of initial surgery can cause persistent postoperative pain. The patient would not experience altered sensation if this compartment were not released. Altered sensation would most commonly occur following injury to the dorsal radial sensory nerve branch during surgery. EPB tendon subluxation also would not occur should the accessory compartment not be released. For EPB tendon subluxation to occur, its own compartment would need to be released first. Finally, EPB tendon rupture would be an extremely uncommon complication of failure to release the accessory compartment.
Question 49High Yield
A surgeon recommends an interscalene regional block to a patient undergoing shoulder arthroscopy. When asked about potential complications, which of the following is most likely to occur?
Explanation
**
Sensory neuropathy is the most common complication seen with interscalene regional block.
Sensory neuropathy is the most common complication seen with interscalene regional block.
Question 50High Yield
Slide 1
A 76-year-old man has experienced aching in the anterior aspect of his ankle for 6 months. He felt a sudden onset of soreness 6 months ago. Since then, he has noted weakness of the foot. He walks with a limp, and the foot hits the ground during the heel contact phase of gait. On examination there is a mobile subcutaneous mass in the anterior ankle. The patientâs magnetic resonance image (MRI) is presented (Slide). Which of the following is the most accurate diagnosis:
A 76-year-old man has experienced aching in the anterior aspect of his ankle for 6 months. He felt a sudden onset of soreness 6 months ago. Since then, he has noted weakness of the foot. He walks with a limp, and the foot hits the ground during the heel contact phase of gait. On examination there is a mobile subcutaneous mass in the anterior ankle. The patientâs magnetic resonance image (MRI) is presented (Slide). Which of the following is the most accurate diagnosis:
Explanation
This MRI presents the typical appearance of an anterior tibial tendon rupture. There is no continuity of the tendon distally, and the retracted tendon end has formed a scar palpable as a subcutaneous mass. The clinical history of the weakness associated with a drop foot gait is characteristic of the tendon rupture.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon