Orthopedic Review | Dr Hutaif General Orthopedics Revie -...
14 Apr 2026
214 min read
57 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Review | Dr Hutaif General Orthope...
00:00
Start Quiz
Question 1High Yield
Based on his radiograph findings, what is the best next step?
Explanation
- Axillary radiograph_
Question 2High Yield
A unilateral "piano key" sign, indicates
Explanation
The piano key sign is a demonstration of instability at the DRUJ, typically seen after healing from a distal radius fracture with an associated ulnar styloid fracture (as in this case) or other wrist injury. The hand is pushed down against a table top, and the distal radius translates dorsally (with the distal ulna apparently moving volarly). In fact, the distal radius is the mobile segment, while the distal ulna is fixed in space. Treatment involves repair or reconstruction of the foveal insertion of the triangular fibrocartilage complex (TFCC) and distal radioulnar ligaments. This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ. Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
Question 3High Yield
Slide 1
A 23-year-old carpenter fell off a roof 4 weeks ago. He has pain in the ankle and a deformity. The lateral radiograph is presented (Slide). Which of the following treatments is most likely to return this patient to work with a functioning foot and ankle:
A 23-year-old carpenter fell off a roof 4 weeks ago. He has pain in the ankle and a deformity. The lateral radiograph is presented (Slide). Which of the following treatments is most likely to return this patient to work with a functioning foot and ankle:
Explanation
The calcaneus fracture is associated with subluxation of the subtalar joint, giving the appearance of injury to the talus and calcaneus. The true extent of the injury cannot be determined without a computed tomography scan; however, the question is not as to the outcome of treatment, but the ability to return this patient to his occupation. At 4 weeks following injury, while open reduction internal fixation of the fracture is possible, anatomic reduction may be difficult. The most likely means of returning this patient to work is with early arthrodesis, which should be combined with an open reduction internal fixation of the calcaneus.
Question 4High Yield
Long strut allografts are not indicated in the initial treatment of reverse obliquity subtrochanteric fractures.
5-Addition of a de-rotation screw would not change the stability of the fixation construct.
A 34-year-old female sustains a proximal third tibia fracture as an isolated injury and elects to undergo operative treatment with intramedullary nailing. Which of the following operative techniques would help to best avoid a procurvatum deformity of the tibia?
5-Addition of a de-rotation screw would not change the stability of the fixation construct.
A 34-year-old female sustains a proximal third tibia fracture as an isolated injury and elects to undergo operative treatment with intramedullary nailing. Which of the following operative techniques would help to best avoid a procurvatum deformity of the tibia?
























































Explanation
The semiextended position for intramedullay nailing of proximal tibia shaft fractures has shown to cause less complications of flexion deformity and malunion. Proximal third tibia fractures are often times difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. The semiextended position helps to eliminate the tendency for
the fracture to flex, due to the avoidance of excessive knee flexion during the reduction. Illustration A is an example of semiextended positioning for tibial nailing. Illustration B shows radiograph utilizing posterior blocking screws to prevent procurvatum deformity.
Tornetta et al looked at the semiextended intramedullary nailing of proximal tibia fractures. Of the 24 patients nailed using this technique, 19 had no anterior angulation, while only 5 had less than 5 degrees of flexion deformity.
In their study, Kubiak et al also advocate the semiextended position for tibial nailing. They note better control of fracture alignment and stabilization especially in the sagittal plane, and better ability to obtain imaging and maintenance of reduction during nail insertion and locking.
Incorrect answers:
would help to avoid valgus deformity. Answer 3 would worsen the flexion deformity.
Answer 4 would worsen the flexion deformity and drive the nail posterior in distal segment.
Answer 5 would not affect flexion deformity.
Which of the following cannulated screw configurations used in the treatment of subcapital femoral neck fractures is optimal?
1) Inverted triangle pattern with the inferior screw posterior to midline and adjacent to the calcar
2) Inverted triangle pattern with the inferior screw anterior to midline and adjacent to the calcar
3) Triangle pattern with the superior screw posterior to midline and adjacent to the calcar
4) Inverted triangle pattern with the inferior screw posterior to midline and central in the femoral neck
5) Inverted triangle pattern with the inferior screw anterior to midline and central in the femoral neck
The strongest portion of the femoral neck is the posterior inferior neck in the region of the femoral calcar. The optimal biomechanical configuration includes an inverted triangle pattern with the single screw in the inferior aspect of the femoral neck adjacent to the calcar.
Booth et al performed a cadaveric study comparing central versus calcar (cortical-adjacent) fixation. The results demonstrated significant improved stability, load, stiffness, and displacement in all tested parameters for the group with calcar-adjacent screw fixation.
Lindequist and Törnkvist performed a Level 4 study of 72 femoral neck fractures. They found that all 5 of their nonunions had screws placed greater than 3mm from the femoral calcar. Additionally, 16 of 18 fractures healed in the group of displaced fractures where both the fixating screws were placed within 3 mm from the femoral neck cortex.
Gurusamy et al performed a Level 4 study of 395 patients undergoing femoral neck fixation. They found a reduced spread of the screws on the lateral view was associated with an increased risk of nonunion of the fracture.
Illustration A depicts the optimal configuration of an inverted triangle with the single screw being inferior and all of the screws being cortical adjacent.
A 63-year-old female sustained a distal radius and associated ulnar styloid fracture 3 months ago after being involved in a motor vehicle collision. Radiographs obtained at the time of injury are shown in Figure A. She underwent open reduction and fixation of the distal radius fracture, and current radiographs are shown in Figure B. At the time of the index operation, there was no distal radioulnar joint instability after plating of the radius. Which of the following is true post-operatively regarding this patient's ulnar styloid fracture?
1) Worse outcomes on the Mayo wrist score are expected without fixation
2) Chronic distal radioulnar joint instability can be expected to occur without fixation
3) Wrist function depends on the level of ulnar styloid fracture and initial displacement
4) Grip strength and wrist range of motion are improved with fixation
5) There is no adverse effect on wrist function or stability without fixation
An accompanying ulnar styloid fracture in patients with stable fixation of a distal radial fracture has no apparent adverse effect on wrist function or stability of the distal radioulnar joint.
Kim et al evaluated 138 patients who underwent surgical treatment of an unstable distal radial fracture, without fixation of an associated ulnar styloid fracture if present. Postoperative evaluation included measurement of grip strength and wrist range of motion; calculation of the modified Mayo wrist score; as well as testing for instability of the distal radioulnar joint at a mean of 19 postoperatively. They did not find a significant relationship between wrist functional outcomes and ulnar styloid fracture level or the amount of displacement.
af Ekenstam et al performed prospective and randomized study of two different treatments of extraarticular Colles' fracture with a fractured ulnar styloid. In one group, the ulnar styloid was left alone, and in the other group it was transfixed and/or the triangular ligament was repaired after closed reduction of the fractured radius. They concluded that repair of the ulnar styloid complex in extraarticular fractures of the distal radius is not better than conventional treatment.
Each of the following are guidelines for management of a domestic violence victim EXCEPT:
1) Socioeconomic status should not preclude evaluation for domestic violence
2) Interview the patient outside the presence of other non-medical personnel
3) Federal law mandates photographs be taken of injuries
4) Document your opinion if the patient’s injuries are not consistent with the offered explanation
5) Physicians should check requirements to see if there is mandatory reporting statute in their state
It is important to fully document the abuse as it has been described to you, however there is no federal law mandating photographic documentation of domestic violence injuries. Photographs may be taken but only with the patient's permission. Disclosure of a diagnosis of abuse to any third party and reporting it to the authorities should be done only with the abused patient’s knowledge and consent, unless there is a mandatory reporting statue in the particular state of practice. Being a female, age 19-29, pregnant, or of a low
socioeconomic status (
An otherwise healthy 34-year-old female undergoes an elective L5-S1 microdiscectomy. At her 4 week followup, she is noted to have drainage from her wound. Labs reveal a CRP of 30 mg/L (normal
1) CRP 20 mg/L, ESR 40 mm/hr
2) CRP 15 mg/L, ESR 20 mm/hr
3) CRP 6 mg/L, ESR 10 mm/hr
4) CRP 1 mg/L, ESR 25 mm/hr
5) CRP 8 mg/L, ESR 5 mm/hr
A normalized C-reactive protein (CRP) value (60 years, smoking, diabetes, previous surgical infection, increased body mass index, and alcohol abuse were all statistically significant preoperative risk factors for developing a post-op wound infection.. The most likely procedure to be complicated by an infection was a combined anterior/posterior spinal fusion performed in a staged manner under separate anesthesia. Infections were primarily monomicrobial and the most common organism cultured from the wounds was Staphylococcus aureus.
Illustration A shows the CRP trends in the study by Khan et al. with postoperative wound infections after spinal surgery treated with IV antibiotics. ER refers to early responder while LR refers to late responder. At the 4-week time point, 16 patients have shown clinical improvement with no fevers, wound drainage, erythema, or need for wound packing. The other 5 patients, referred to as late responders, have shown one or more clinical signs of infection in addition to having an elevated CRP. At 20 weeks, both early and late responders both have shown normalized CRP levels and no clinical evidence of infection. Illustration B shows the ESR trends in the those which demonstrated incomplete normalization of ESR values despite resolution of infection.
Incorrect Answers:
Answer 1, 2, 3, 5: CRP levels > 3 mg/L are elevated and indicate incomplete response to infection
A 25-year-old man is struck by car while crossing the street. His injuries include the closed left tibial shaft fracture shown in Figure A. He is a smoker, but is otherwise healthy. Intramedullary nailing is performed without initial complications. Which of the following puts this patient at greatest risk for tibial nonunion?
1) Use of anti-inflammatories post-operatively
2) Post-operative gapping at the fracture site
3) Presence of an associated fibular fracture
4) History of smoking
5) Mechanism of injury
Post-operative gapping at the fracture site significantly increased the risk of reoperation due to nonunion or malunion.
Bhandari et al performed a retrospective study to identify which prognostic factors were associated with an increased risk of reoperation for nonunion in surgically treated tibial shaft fractures. They examined over 200 fractures, and found the presence of an open fracture wound (RR 4.32), lack of cortical continuity between the fracture ends following fixation (RR 8.33), and the presence of a transverse fracture (RR 20.0) were the three variables most predicitive of reoperation.
Audige et al analyzed 416 patients with operatively treated tibial shaft fractures who were followed for at least 6 months. They found that the greatest risk for delayed healing or nonunion was the presence of an open injury, fractures of the distal 1/3 of the tibia, and postoperative gapping at the
fracture site (The risk of healing problems was doubled for fractures of the distal shaft and for fractures showing a postoperative diastasis).
Figure A is a radiograph of a healthy, independent 51-year-old male. He is treated with immediate open reduction internal fixation to prevent which of the following complications?
1) Fracture non-union
2) Avascular necrosis
3) Skin necrosis
4) Plantar flexion weakness
5) Ankle stiffness
Figure A shows an avulsion fracture of the calcaneal tuberosity. Immediate open reduction and internal fixation is required to prevent wound complications.
Displaced avulsion fractures of the calcaneal tuberosity should be managed urgently to prevent necrosis of the soft tissues overlying the heel. In these injuries, the Achilles tendon is securely attached to the fractured tuberosity. Urgent closed reduction and casting is usually not possible due to the power and proximal pull of the triceps surae. Surgical fixation is required. The best treatment modality is open reduction and bone-to-bone fixation with screws. Closed reduction and percutaneous pinning fixation is not strong enough to provide a stable fixation of the tuberosity.
Lui reported on avulsion fractures of the bony insertion of the Achilles tendon at the calcaneus. He stated that screw fixation alone is not sufficient for repair of these injuries. His technique involved two suture anchors used capture the small bone fragment to the calcaneus. This allowed for the pull of the triceps surae to be neutralized and early physical therapy.
Hess et al. looked at a case series of calcaneal tuberosity avulsion fractures that were treated in a delayed fashion. All three patients with posterior tuberosity calcaneal avulsion fractures developed skin necrosis because of a delay in treatment.
Figure A shows a displaced posterior tuberosity calcaneal avulsion fracture. Illustration A shows skin breakdown overlying the posterior tuberosity calcaneal avulsion fracture.
Incorrect Answers:
Answer 1: The amount of displacement is an indication for fixation, however urgent treatment does not improve union rates with these fractures.
Answer 2: Tuberosity calcaneal avulsion fractures rarely disrupt the blood supply to the avulsion fragment and are not associated with avascular necrosis.
Answer 3: Plantar flexion weakness is a known complication of these injuries despite many treatment options.
Answer 4: Ankle stiffness is most commonly related to surgical fixation methods and post-operative immobilization and delayed rehabilitation.
A 22-year-old male presents 4 weeks following open reduction and internal fixation of his unstable ankle fracture. He has had three days of increasing pain, swelling and the new onset of purulent drainage from the mid-portion of the lateral incision. Laboratory values, including white blood cell count, sedimentation rate, and C-reactive protein are elevated. Current radiographs are seen in Figures A and B. On examination the wound probes deep and likely involves the lateral plate. What is the best step in management at this time?
1) Suppression with broad spectrum oral antibiotics until fracture healing
2) Suppression with broad spectrum intravenous antibiotics until fracture healing
3) Surgical debridement, removal of internal fixation, culture specific antibiotics, casting until fracture healing
4) Surgical debridement, maintenance of internal fixation, culture specific antibiotics until fracture healing
5) Wound culture in the office and suppression with culture specific antibiotics until fracture healing
The patient is presenting with an acute deep infection following open reduction and internal fixation of an unstable ankle fracture. Recent studies have shown that a protocol of early aggressive surgical debridement, maintenance of internal fixation and culture specific antibiotics can be effective at achieving fracture healing.
Management of early postoperative infection following open reduction and internal fixation can be challenging. Effective treatment typically involves a combination of surgical debridement and culture specific antibiotics. Removing internal fixation prior to fracture healing can lead to additional insult to the soft tissue and ongoing inflammation secondary to fracture instability. Recently published protocols have shown effective treatment with maintenance of implants and culture specific antibiotics following early, aggressive surgical debridement.
Berkes et al. performed a multi-center retrospective study of 121 patients with acute postoperative infection (defined as less than 6 weeks from surgery) following internal fracture fixation. The authors demonstrated a 71% rate of success (defined by maintenance of implants until fracture healing) with a protocol of debridement and suppression with culture specific antibiotics. Risk factors for failure of this technique include open fractures and the use of an intramedullary nail for fracture fixation.
Figures A and B show an ankle status post open reduction and internal fixation of a lateral malleolus fracture. There are no signs of loosening of fixation or cortical erosions concerning for osteomyelitis.
Illustrations A and B are weight bearing X-rays that demonstrate the same fracture, now healed, after debridement and culture specific antibiotics.
Illustrations C and D demonstrate the same fracture after elective removal of implants at 10 months following the index procedure. Intraoperative cultures at the time of hardware removal were negative for recurrent infection.
Incorrect answers:
Answers 1 and 2: Broad spectrum antibiotics without surgical debridement would not be effective in dealing with the infection in this clinical scenario with purulence tracking to the level of the plate
Answer 3: Surgical debridement and antibiotics would control the infection adequately, however removal of fracture fixation in an unstable fracture would lead to instability, soft tissue inflammation and likely malunion or nonunion that would require complex revision
Answer 5: Although culture specific antibiotics are an improvement over broad spectrum, again surgical debridement in conjunction with antibiotics is the most appropriate choice in this scenario. Intraoperative deep cultures in a sterile environment are preferred over cultures obtained in the office.
A 28-year-old male sustained an ankle injury 3 months ago, and was treated with closed management and splinting; a current x-ray is shown in Figure A. Which of the following is the most important factor in deciding between a joint sacrificing and a joint preserving operation for this patient at this time?
1) Workers' Compensation involvement
2) Gender
3) Date of injury
4) Degree of tibiotalar arthritis
5) Degree of deformity
This patient presents with malunion after sustaining a bimalleolar ankle fracture. Surgical treatment options consist of osteotomy for deformity correction with internal fixation (joint preserving) versus fusion (joint sacrificing) with the primary determinant being the amount of ankle arthritis present.
When treating ankle malunions, the decision to perform deformity correction and preserve the joint versus fusing the joint is dependent on signs of progressive, advanced tibiotalar arthritis on radiographs.
Yablon and Leach followed 26 patients following corrective fibular osteotomy following malunion and noted excellent results at a mean follow-up of 7 years. All but 3 returned to preinjury level of activity and had desired outcomes following deformity correction.
Reidsma et al. prospectively followed 57 patients with a minimum follow-up of 10 years following corrective osteotomy and fixation for ankle fracture malunions. Good to excellent results were obtained for 85% of the cohort. The authors concluded that those ankle fracture malunions with none to minimal arthritic changes should still receive corrective osteotomy to prevent further progression of arthritis.
Yablon et al. following 53 patients for 6-9 months, reported on the importance of anatomic restoration of the lateral malleolus when fixing bimalleolar ankle fractures. With anatomic reduction and fixation, no progression of arthritis was noted with return to function.
Figure A is an AP radiograph of a right ankle fracture malunion. Incorrect answers:
Answers 1-3, 5: Factors such as age, gender, and degree of deformity are not
as important as the presence of advanced arthritis that may suggest requiring a joint sacrificing fusion procedure. The date of injury may portend a poor outcome (the longer from the date of injury/subsequent malunion), but is not the most important factor in deciding between corrective osteotomy versus fusion.
A 45-year-old male presents after falling off of a ladder. Radiograph is shown in Figure A. Which of the following is the appropriate sequence in management?
1) Closed reduction, splint application, computed tomography (CT) scan, delayed open reduction and internal fixation
2) Closed reduction, cast application, close observation
3) Splint application, CT scan, application external fixator, delayed open reduction and internal fixation
4) Splint application, application external fixator, CT scan, delayed open reduction and internal fixation
5) Splint application, acute open reduction and internal fixation
This patient has sustained a pilon fracture, with severe comminution and impaction at the articular surface.
The correct sequence of management includes (1) immediate splinting, (2) application of an external fixator, (3) restoration of length alignment and rotation with temporizing external fixation, (4) computed tomography, followed by (5) definitive fixation once soft tissues are amenable.
Tornetta and Gorup analyzed the use of preoperative CT scans in comparison to radiographs in preparation for fixing pilon fractures. The authors noted increased recognition of intra-articular fragments, comminution and noted a high percentage of operative planning changes following CT analysis.
Furthermore, the authors recommended CT scans AFTER external fixation, for even better fragment characterization.
Marsh et al. in their instructional course lecture provide tips and tricks in successful management of pilon fractures. One of the highlighted points include staged, delayed treatment of pilon fractures via spanning external fixator as well as highlighting the importance of obtaining the CT after restoring length and alignment.
Figure A exhibits a radiograph of a comminuted, impacted, shortened pilon fracture.
Incorrect answers:
Answer 1: With such a short, impacted fracture, external fixation as a temporizing measure is recommended to help calm the soft tissue envelope. Answer 2: Closed treatment is not accepted in this type of fracture, due to the high incidence of arthritis and malunion.
Answer 3: CT scan should be obtained AFTER external fixation, not before. Answer 5: This high-energy injury likely has severe soft tissue injury, which is not amenable to acute fixation.
A 45-year-old male with long-standing diabetes sustains the injury shown in Figure A. He has a BMI of 38, established peripheral neuropathy, and his most recent HbA1c is 8.8. What is the most appropriate definitive management option of Figures B through F?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
Open reduction and internal fixation (ORIF) remains the mainstay of treatment for ankle fractures in patients with diabetes.
ORIF for ankle fractures in diabetics can be augmented with increased density of fixation to account for notable, pathologic bone. Specifically, multiple quadricortical syndesmotic screws, bicortical medial malleolar screws, and stiffer plates are all viable options. Furthermore, due to delayed healing properties, prolonged immobilization may also be required to avoid fixation failure.
Guo et al. performed a cohort controlled comparison between diabetics and non-diabetic patients with operative ankle fractures. Although they hypothesized that there would be more complications in the diabetic group, there was no statistical differences in fixation failure or complications when adhering to treatment principles for diabetics (including prolonged non-weight bearing for 10-12 weeks and increased density of fixation).
Chaudhary et al. review the notable complications following ankle fracture treatment in patients with diabetes. In reviewing the literature, the authors recommend ORIF with meticulous soft tissue handling, increased density of fixation, and prolonged immobilization as the mainstay of diabetic ankle fracture treatment. External fixation and frames, while treatment options, should be reserved for salvage or infectious clinical scenarios.
Figure A depicts a bimalleolar ankle fracture. Figure B depicts a cam walker.
Figure C depicts a cast. Figure D standard fixation for ankle fracture for a patient without diabetes. Figure E exhibits definitive fixation with additional screws to increase construct stability. Figure F depicts a ring fixator.
Incorrect Answers:
Answers 1,2: Non-operative treatment is not appropriate for this fracture pattern
Answer 3: Figure D, typically used for those without diabetes is less appropriate for this patient/clinical scenario.
Answer 5: While external fixation and a ring fixator may be utilized, ORIF should be attempted first, however, as it provides stiffer fixation.
Distraction bone block arthrodesis alone would most likely help a patient suffering from a painful calcaneus fracture malunion with all of the following except:
1) Low talar declination angle
2) Hindfoot varus alignment
3) Subtalar arthritis
4) Talonavicular subluxation
5) Peroneal impingement
Distraction bone block arthrodesis in isolation would be unlikely to improve pain related to peroneal impingement. Lateral wall exostectomy would likely be needed for this, and should be concomitantly performed in most cases.
Calcaneal fracture malunions demonstrate several common patterns. Patients may manifest pain from anterior tibiotalar impingement (a result of a low talar declination angle), difficulty with shoe wear due to shortening and widening of the hindfoot, painful talonavicular subluxation, subfibular impingement, and post-traumatic subtalar osteoarthritis. The distraction bone block arthrodesis procedure was developed to eliminate the pain of subtalar arthritis while simultaneously normalizing hindfoot height by inserting a contoured structural bone graft into the subtalar joint. The procedure can correct pathologic hindfoot varus/valgus and restore a normal talocalcaneal angle, thereby improving symptomatic post-traumatic pes planus. The procedure alone does not address lateral wall blowout causing subfibular or peroneal impingement, which requires lateral wall exostectomy. Lateral wall exostectomy therefore should be done in addition to address this issue.
Carr et al. first reported the use of subtalar distraction bone block arthrodesis for salvage of post-traumatic subtalar arthritis following calcaneus fractures. In their 16 patient series, distraction of the subtalar joint with insertion of the bone block allowed for correction of talocalcaneal angle, restoration of hindfoot height, and improvement in symptoms related to tibiotalar impingement.
Clare et al. evaluated a treatment protocol for calcaneal malunions based upon the classification of Stephens and Sanders. Type II and III malunions were treated with subtalar bone-block arthrodesis and other concomitant procedures. They found that their treatment protocol was effective for pain relief, re-establishing a plantigrade foot, and improving function. The most difficult component of the case was restoration of calcaneal height.
Braley et al. evaluated isolated lateral decompression in the treatment of symptomatic calcaneal malunions without concomitant subtalar arthrodesis. These 11 patients had persistent lateral sided pain and their malunions did demonstrate subtalar involvement. The authors reported 9 of the 11 patients had a satisfactory outcome with lateral decompression alone. They concluded that a lateral decompression in management of symptomatic malunions with lateral-sided symptoms is an essential consideration.
Incorrect Answers:
Answer 1: Talar declination angle describes the relative plantar- or dorsiflexion of the talus relative to the ground.
Answer 2: Hindfoot alignment can be improved with distraction arthrodesis. Answer 3: Arthrodesis addresses painful subtalar arthritis.
Answer 4: Restoration of the normal talocalcaneal angle can be achieved, which can also normalize the talonavicular relationship.
A 31-year-old patient has had activity related lateral ankle pain for 4 months. She underwent the procedure shown in Figure A approximately 8 months ago. What surgical technique has most likely resulted in this patients pain?
1) Failure to recognize the most distal screw penetrating the joint surface
2) Low posterior plating with prominent distal screw
3) Failure to recognize an associated syndesmosis disruption
4) Fracture malreduction causing shortening of the fibula
5) Failure to use a longer plate with the lag screw positioned outside the plate
Figure A shows a low posterior plate with a prominent screw head in the most distal hole of the plate. This fixation technique is correlated with peroneal pathology, which usually presents months after fixation when the patient increases their activity level.
The two most common fixation techniques of lateral malleolus fractures are (1) lag screw plus lateral neutralizing plating and (2) posterolateral antiglide plating. The disadvantages of the lateral plating includes the risk of intraarticular screws distally, prominent lateral hardware, and poor distal screw fixation. To overcome these complications, posterolateral antiglide plating allows for bicortical distal fixation with no articular perforation. However, low placement of the plate with a prominent screw head in the most distal hole is associated with symptomatic peroneal pathology. If the most distal screw is not prominent, or absent, this is less likely to cause peroneal complications.
Weber et al. examined the effect of antiglide plate and screw positioning on peroneal tendon pathology. They showed that low posterior plating and large screw heads caused significant retromalleolar pain in most patients. To decrease peroneal pathology, they state that the distal end of the plate should stay proximal to the osteosynovial peroneal groove. Radiologically this level
corresponds to the junction of the proximal and middle thirds of the lateral malleolus.
Figure A shows a posterior positioned 5 hole 1/3 tubular plate. There is no articular screw penetration and the fracture is healed in an anatomical position. The distal aspect of the plate is is the distal third of the lateral malleolus.
Incorrect Answers:
Answer 1: The most distal screws rarely penetrates the joint with the use of fibular antiglide plates. In addition, there is no evidence of screw penetration in this patient.
Answer 3: A missed syndesmosis disruption would usually show some radiographic findings. The tibiofibular clear space is usually most sensitive, which is measured radiographically by the distance from the lateral border of the posterior malleolus in the distal tibia to the medial border of the fibula. As a general rule, it is considered normal if the measurement is less than approximately 6 mm on both AP and mortise views.
Answer 4: The fracture reduction looks anatomic. The talocrural angle, 'dime' sign and “Shenton's line” of the ankle all normal.
Answer 5: The construct used to fix this isolated lateral trans-syndesmotic fracture is acceptable. The one-third tubular plate, which is placed posterolaterally on the fibula as an antiglide plate, indirectly reduces the fracture and acts as a buttress to resist the posterior and proximal displacement of the distal fragment. Insertion of a lag screw through the plate is a described technique.
A 35-year-old painter falls from a ladder sustaining an isolated fracture of his left calcaneus. Months later at follow-up, he is noted to have pain and a catching sensation in his medial foot with active flexion of the great toe. What is the most likely initial injury leading to this complication?
1) Displaced calcaneal beak fracture
2) Displaced fracture of the calcaneal tuberosity
3) Comminuted posterior facet fracture
4) Fracture of the sustentaculum tali
5) Lateral wall blowout fracture
A known complication of fractures of the sustentaculum tali is stenosis (delayed) or injury (acute) of the flexor hallucis longus (FHL) tendon. Stenosis
can cause pain and popping with great toe flexion.
Fractures of the calcaneus often occur after falls from height, and in addition, may be associated with vertebral fractures due to the high-impact mechanism. The FHL tendon runs directly underneath the sustentaculum tali on the medial calcaneus and can be injured causing frank tears or delayed stenosis. These fractures may be missed on ankle or foot plain films alone, and advanced imaging should be ordered if clinical suspicion for calcaneus fractures exists given mechanism and location of pain/swelling.
Komiya et al. present a case report of direct impalement of the FHL tendon in the tunnel under the sustentaculum tali. Though this particular complication is quite rare, such a report highlights the relevant anatomy and structures at risk as well as demonstrates the need for a good clinical exam as the injury was not noted on imaging but the concern was raised on physical exam of FHL involvement.
Della Rocca et al. report their 19-patient series on operatively managed isolated sustentaculum tali fractures. They report a high rate of associated ipsilateral foot injuries (14 patients) and describe fixation using a medial approach and retracting the flexor tendons and neurovascular bundle.
Illustration A is an axial CT image from Della Rocca (2009) et al. showing a representative sustentaculum tali fracture
Incorrect Answers:
Answer 1 - beak fractures are posterior, anatomically related to the Achilles tendon insertion, not the FHL tendon.
Answer 2 - FHL tendon is not associated with the tuberosity.
Answer 3 - FHL tendon runs anterior to the posterior facet and would unlikely be involved in that injury.
Answer 5 - FHL tendon runs medially, not laterally.
A 30-year-old male patient involved in a hang-gliding accident sustains a knee dislocation with multiligamentous knee injury and transection of his peroneal nerve. He undergoes multiple reconstructive surgeries. Two years later, he continues to have a foot drop and dynamic tendon transfer is recommended. This treatment most commonly involves transferring a tendon from which native insertion point to which new insertion point?
1) Plantar distal phalanges to medial navicular
2) Medial navicular to dorsal lateral cuneiform
3) Plantar 1st metatarsal to dorsal lateral cuneiform
4) 5th metatarsal base to dorsal medial cuneiform
5) Plantar distal phalanx of the hallux to dorsal distal phalanx of hallux
Dynamic tendon transfer to restore active dorsiflexion of the foot involves transferring the posterior tibial tendon (PTT) insertion on the medial navicular to the dorsal lateral cuneiform.
Common peroneal nerve (CPN) injuries following traumatic knee dislocation are common, with an incidence of 25-40%. CPN palsy is characterized by foot drop
due to loss of ankle dorsiflexors with a steppage gait and eventual development of a supinated equinovarus foot secondary to the unopposed pull of the PTT. Nonsurgical management involves use of an ankle-foot orthosis and physical therapy. Surgical options include acute primary repair, nerve grafting with either autologous sural nerve or nerve conduits and dynamic tendon transfer. The PTT is harvested from its insertion at the navicular, passed through the interosseous membrane (IOM) and anchored to the lateral cuneiform (see Illustration A). The classic bridle procedure involves concomitant anastamosis of the PTT to the tibialis anterior (TA) and peroneus longus (PL) tendons.
Garozzo et al reported a case series of 62 patients with post-traumatic CPN palsy who underwent a one-stage procedure consisting of nerve repair and PTT transfer. Nerve repair combined with PTT transfer improved postoperative outcomes compared to nerve repair alone. At 2-year follow up, neural regeneration was demonstrated in 90% of patients. The authors hypothesized that poor outcomes following nerve repair alone are due to force imbalance between the functioning flexors and paralyzed extensors, which is somewhat equalized by performing a PTT transfer at time of repair.
Niall et al reviewed 55 patients with traumatic knee dislocation and reported a 41% incidence of CPN injury, exclusively associated with dislocations involving disruption of the posterior cruciate ligament (PCL) and posterolateral corner (PLC). Complete neurologic recovery was found in only 21% of patients. The best prognosis was found with lesions in continuity, less than 7cm of nerve involvement, and short conduction block and muscle activity on nerve conduction and EMG studies.
Vigasio et al described a dynamic tendon transfer technique for traumatic complete CPN injury, involving transfer of the PTT to the TA rerouted to a new origin at the lateral cuneiform to restore ankle dorsiflexion and flexor digitorum longus (FDL) to the extensor digitorum longus (EDL) and extensor hallucis longus (EHL) to restore digit dorsiflexion. Rerouting the TA towards the transferred PTT ensures the PTT harvest length is sufficient. This avoids excessive tensioning of the PTT, which may limit tendon excursion and result in a static tenodesis rather than dynamic function, as well as the need for PTT lengthening which may decrease strength of the transfer
Illustration A is a series of intraoperative photographs demonstrating PTT transfer from Garg et al. An incision is made distal to the medial malleolus and the PTT is harvested subperiosteally (A). The PTT is delivered through a second incision ~15cm proximal to the medial malleolus (B-C). The PTT is then passed through the interosseous membrane and out a third incision over the anterior
fibula (D). Lastly, the PTT is passed through a fourth incision over the dorsal midfoot and anchored to the lateral cuneiform (E).
Incorrect Responses:
Answer 1: Transferring the FDL (insertion = plantar distal phalanges) to the medial navicular is used for correction of flexible flatfoot deformity arising from PTT insufficiency. Some surgeons transfer the FDL to the medial navicular at the time of PTT transfer to the dorsum of the foot, to compensate for loss of PTT function and minimize risk of flatfoot development.
Answers 3: Transferring the PL (insertion = plantar 1st metatarsal) is not recommended, as this muscle is innervated by the CPN via the superficial peroneal nerve and therefore would not be functional.
Answer 4: Transferring the peroneus brevis (PB; insertion = 5th metatarsal base) is not recommended, this muscle is innervated by the CPN via the superficial peroneal nerve and therefore would not be functional.
Answer 5: Transferring the flexor hallucis longus (FHL; insertion = plantar distal phalanx of the hallux) to the insertion of the EHL (dorsal distal phalanx of hallux) is recommended for correction of claw toe deformity and would not help restore foot dorsiflexion in this patient.
Which of the following represents the most common complication following operative treatment of the injury shown in Figure A?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
This patient has a displaced talar neck fracture. The most common complication is post-traumatic arthritis.
Complications after treatment of displaced talar neck fractures are common. Both tibiotalar and subtalar arthritis occur, with subtalar arthritis being the most common. Osteonecrosis is also common, but post-traumatic arthritis is the most common.
Lindvall et al. reviewed 26 displaced talar fractures treated with internal fixation and found that post-traumatic arthritis was the most common complication, occurring in 100% of patients. Osteonecrosis was found in 13 of 26 patients (50%).
Vallier et al. reviewed patients presenting with talar neck fractures and found post-traumatic arthritis in 21 of 39 patients (54%). Osteonecrosis was found in 19 of 39 patients (49%).
Figure A shows a displaced talar neck fracture. Figure B shows talar neck nonunion (arrow) and osteonecrosis of the talar body. Figure C is an AP of the same patient shown in Figure B and again shows osteonecrosis of the talar body. Figure D shows subtalar arthritis after internal fixation of a talar neck fracture via medial malleolar osteotomy. Figure E shows a clinical photo of a patient with a varus malunion after talar neck fracture. Figure F shows a wound dehiscence.
Incorrect answers:
Answers 1, 2, 4, 5. These are all known complications of surgical treatment of displaced talar neck fractures but occur less frequently than post-traumatic arthritis.
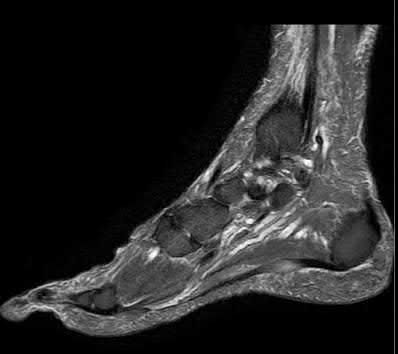
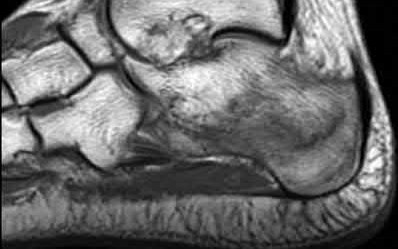
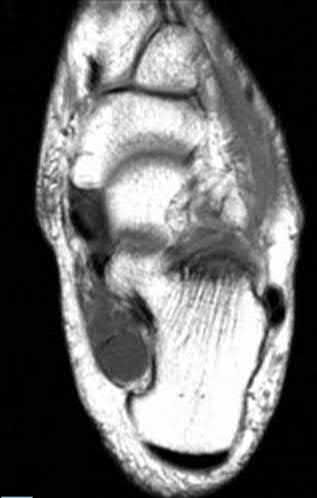
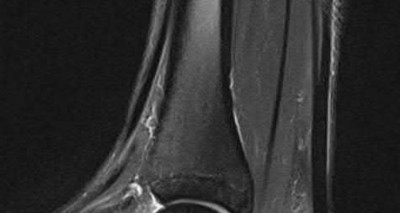
A 25-year-old woman began training for a marathon and she reports a 2-week history of heel pain. She has pain throughout the day that worsens with prolonged weight-bearing. On exam, the location of
maximal tenderness is indicated by the white arrow in Figure A. The patient denies point tenderness at the location of the yellow arrow in Figure A. Which of the following MRI images (Figures B to F) would you expect to find in this patient?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
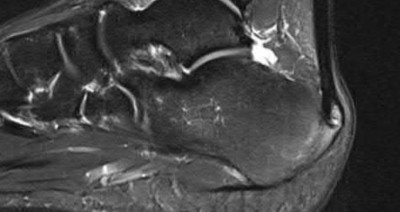
The clinical presentation is consistent with a stress fracture of the calcaneus. The T1 MRI shows a fracture line within the calcaneus which is consistent with
a calcaneal stress fracture.
Calcaneal stress fractures most commonly occur in long-distance runners and military recruits. Usually, they are caused by overload and inability of bone formation to match resorption. Patients usually begin a rapid increase of activity level from a prior sedentary lifestyle. Patients complain of heel pain that persists throughout the day. The pain is located along the medial and lateral walls of the calcaneus. Diagnosis can be made with radiographs 2-3 weeks after symptom onset by the appearance of a sclerotic line. If the diagnosis is uncertain, MRI may be obtained.
Gehrmann et al. performed a review of stress fractures in the foot. They report that most studies of calcaneal stress fractures are from military recruits.
Primary treatment includes rest, avoidance of weight-bearing, and physical therapy. Patients usually return to full duty between 8 and 10 weeks. Recruits with inadequate treatment had a recurrence of symptoms. They conclude that most studies are from the 1940’s and 1950’s and lack any significant detail into specific treatment protocols.
Sormaala et al. performed a retrospective study in which they reviewed MRIs in all military recruits who had exercise-induced heel pain, over an eight-year period. They report that only 15% of injuries were visible on radiographs and a portion of patients had stress fractures of another tarsal bone. They conclude that a majority of calcaneal stress fractures occur in the posterior part of the bone, but some fractures may be found in the middle and anterior parts. They recommend obtaining an MRI if a radiograph is negative in a patient with exercise-induced foot or heel pain.
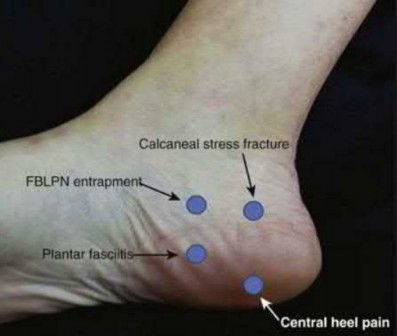
Figure A demonstrates the most common area of tenderness and pain of a calcaneal stress fracture, indicated by the white arrow, while the yellow arrow points to the area of tenderness consistent with plantar fasciitis. Figure B is a sagittal T2-weighted MRI demonstrating plantar fasciitis. Figure C is a sagittal T1-weighted MRI demonstrating a calcaneal stress fracture. Figure D is an axial T1-weighted MRI demonstrating a mass on the medial aspect of the calcaneus consistent with a ganglion cyst. Figure E is a sagittal T1-weighted MRI of the foot demonstrating an intraosseous lipoma within the calcaneus. Figure F is a sagittal T2-weighted MRI demonstrating insertional Achilles tendinopathy.
Illustration A demonstrates the most common etiologies of plantar foot pain.
Incorrect Answers:
Answer 1: Figure B, a sagittal T2-weighted MRI, demonstrates plantar fasciitis. Symptoms of plantar fasciitis are sharp heel pain, usually worse in the morning. Tenderness is usually found on the plantar aspect of the foot.
Answer 3: Figure D, an axial T1-weighted MRI, demonstrates a ganglion cyst in the tarsal tunnel. Symptoms of tarsal tunnel syndrome include sharp burning pains in the foot and parasthesias and numbness in the plantar foot.
Answer 4: Figure E, a sagittal T1-weighted MRI, demonstrates an intraosseous lipoma. Intraosseous lipomas are usually incidental findings.
Answer 5: Figure F, a sagittal T2-weighted MRI, demonstrates insertional Achilles tendinitis. This usually presents with pain over the insertion of the Achilles. It may have a relapsing and remitting course, which worsens with activity.
A 35-year-old male fell and sustained an open talar neck fracture. He underwent operative fixation of his fracture. He presents at 2 months after surgery. He denies any constitutional symptoms and his pain is well controlled. On exam, his wounds are well healed with no erythema. Imaging is shown in Figure A. What can the patient be told about his condition?
1) Hawkins sign is positive. The likelihood of developing osteonecrosis is high
2) Hawkins sign is positive. The likelihood of developing osteonecrosis is low
3) Hawkins sign is negative. The likelihood of developing osteonecrosis is high
4) Hawkins sign is negative. The likelihood of developing osteonecrosis is low
5) He has developed chondrolysis
This patient has a positive Hawkins sign, which signifies that he is unlikely to develop osteonecrosis.
A subchondral radiolucency of the talar dome after a talar neck fracture is known as the Hawkins sign. It is an indication that the talar body is viable. It usually appears by 6-8 weeks after injury and is best seen on the mortise view. If the Hawkins sign is present, it is unlikely that the patient will develop osteonecrosis.
Early writes a review on talus fracture management. He reports that talar neck fractures occur through the extra-articular portion of the talus and represent nearly half of talus fractures. The mechanism of injury is a combined ankle dorsiflexion followed by axial compression of the tibiotalar joint. He concludes that anatomic reduction gives the patient the best chance of a good outcome.
Leduc et al. wrote a review on posttraumatic avascular necrosis of the talus. They note that AVN is diagnosed on plain radiography by the absence of the Hawkins sign. They report that CT can also reveal characteristic talar AVN patterns and can be used to confirm radiographic findings. CT helps to assess subtle depression, collapse, fragmentation, and arthritic changes. MRI remains the most sensitive technique for detecting osteonecrosis of the talus, especially in the early stages. They conclude that although there are many published treatments of AVN of the talus, outcome studies are still lacking.
Tezval et al. performed a retrospective review to determine the prognostic reliability, sensitivity, and specificity of the Hawkins sign. They found that in all patients who developed osteonecrosis, none had the Hawkins sign present. In all patients that exhibited a Hawkins sign, none developed osteonecrosis. They determined the sensitivity of the Hawkins sign to be 100% while the specificity was 57.5%. They conclude that if a full or partial positive Hawkins sign is detected, it is unlikely that AVN will develop.
Figure A demonstrates the Hawkins sign with subchondral radiolucency which is noted by arrows in Illustration A.
Incorrect Answers:
Answers 1, 3, 4: The patient has a positive Hawkins sign, therefore the chance of developing osteonecrosis is low.
Answer 5: Chondrolysis is characterized by rapid destruction of articular cartilage on both sides of the joint which leads to loss of joint space
A 25-year-old male presents to the emergency department after a lawnmower accident with traumatic loss of his great toe. On examination, his wound is grossly contaminated with soil. In addition to a cephalosporin and an aminoglycoside, penicillin is given. Which of the following is true with regards to the organism that penicillin is targeting in this injury?
1) It is an Aerobic, Gram-positive rod
2) It is an Anaerobic, Gram-positive coccus
3) It is an Anaerobic, Gram-negative rod
4) It is Catalase positive
5) It may cause botulism
The organism being covered with penicillin is Clostridia spp. Clostridium botulinum is a Gram Positive Bacilli that is the cause of botulism.
Clostridia spp, is a Gram-positive, obligate anaerobic spore-forming rod that is found in soil and gut flora. It produces gas by the fermentation of glucose and
may cause gas gangrene. Common bacteria of this genus are C. perfringens (most common), C. tetani (causes tetanus), C. difficile, and C. botulinum (causes botulism). If wounds are grossly contaminated with soil, penicillin is given to cover against Clostridia.
Decoster et al. performed a review of traumatic foot wounds. They report that lawnmower injuries to the foot are relatively common. IV antibiotic therapy should be initiated with a broad-spectrum cephalosporin and an aminoglycoside to provide coverage against Gram-negative organisms.
Penicillin should be given to protect against Clostridial infection. They conclude that irrigation and debridement is indicated initially followed by packing of open wounds. Repeat debridements are necessary as nonviable tissue demarcates. If major reconstructive procedures are necessary, they should be delayed as they have a high rate of failure if performed too soon.
Cross et al. wrote a review on treatment principles in the management of open fractures and they note that in open fractures with soil contamination, additional coverage should be added for anaerobic bacteria, typically Clostridia. Another member of the genus Clostridia is C. tetani, the causative agent of tetanus. Vaccine status for tetanus must also be assessed in these situations as well.
Illustration A is a radiograph demonstrating soft tissue swelling and subcutaneous emphysema, consistent with gas gangrene. Illustration B is a clinical photograph of gas gangrene evidenced by edema, discoloration, ecchymosis, and hemorrhagic bullae. Illustration C is a pathology slide of C. perfringens, a Gram-positive rod.
Incorrect Answers:
Answers 1, 2, 3: Clostridia are Gram-positive, obligate anaerobes. Answer 4: Clostridia are catalase negative.
All of the following are ways that a negative pressure dressing is beneficial to wound healing EXCEPT:
1) Accelerated granulation tissue formation
2) Removes excess proteins and electrolytes from wound
3) Reducing anaerobic colonization
4) Causes cells to release vascular endothelial growth factor by mechanical force
5) Causes an increase in capillary afterload
Negative pressure dressings or vacuum-assisted wound closures (VAC) apply a negative pressure to the wound bed which allows a decrease in capillary afterload which produces a better inflow of blood.
VAC dressings exert their positive effects on wound healing in multiple ways. Firstly, they remove interstitial fluids, which have been found to contain inhibitory factors that suppress the formation of fibroblasts, vascular endothelial cells, and keratinocytes. This also eliminates the formation of any superficial purulence or slime which also reduces the potential for anaerobic colonization. Removal of excess fluid also pulls out excess proteins and electrolytes to help maintain and osmotic and oncotic gradient. VACs allow arterioles to dilate which produces a proliferation of granular tissue. Also, there is a decrease in capillary afterload, (the pressure against which the heart must overcome to eject blood), which promotes better inflow of blood. Lastly, applying a mechanical force to the surrounding soft tissues allows the edges of the wound to be drawn towards the center, uniformly. This decreases the size of the wound over time. The micromechanical forces exerted on individual cells causes a release in local growth factors, such as vascular endothelial growth factor (VEGF), which stimulate wound healing.
Herscovici et al. applied VAC dressings to 21 consecutive patients with open, high-energy soft tissue injuries. They found that wounds averaged 4.1 sponge changes and the device was used for an average of 19.3 days. 12 wounds avoided the need for further treatment. Only 9 patients required free tissue transfer. They concluded that the VAC is a viable treatment adjunct for the treatment of open, high-energy injuries.
Clare et al. reported their experience with the VAC dressing in the treatment of non-healing, diabetic and dysvascular wounds. They retrospectively reviewed 17 patients with non-healing wounds of the lower extremity. 9 had diabetes and 8 had severe peripheral vascular disease. The average length of treatment
was 8.2 weeks and 14/17 wounds successfully healed, and only 3 failed VAC treatment. They concluded that the VAC dressing is an acceptable option for wound care of the lower extremity.
Illustration A is a photo of an open wound being treated with a VAC dressing. Incorrect Answers:
Answers 1, 2, 3, and 4 are all ways that VAC dressings are beneficial to wound
healing.
Which of the following is true regarding anterior sternoclavicular joint dislocations?
1) Reduction may result in tracheal injury
2) They are usually stable following closed reduction
3) They require fusion to hold the reduction
4) They are rarely symptomatic when left unreduced
5) They should be treated acutely with medial clavicle excision
From the Bicos article, “Anterior SC joint instability should primarily be treated conservatively. The patients should be informed that there is a high risk of persistent instability with nonoperative or operative care, but that the persistent instability will be well tolerated and have little functional impact in the vast majority. Therefore, operative intervention for anterior SC joint instability is mainly cosmetic in nature."
An otherwise healthy 45-year-old female slips and falls with immediate right ankle pain. Stress examination of the right ankle is shown in Figure A. Which of the following is the most important for achieving a satisfactory outcome following open reduction internal fixation for this injury?
1) Weight-bearing before 3 weeks.
2) Medial clear space >5mm
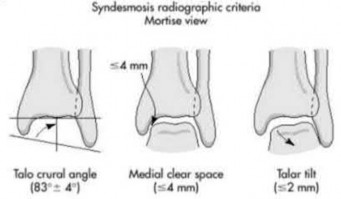
3) Talocrural angle of 83 degrees
4) Tibiofibular clear space of >6mm
5) Talar tilt of >5 degrees
Anatomic reduction of a rotational ankle fracture is considered the most important factor in achieving a satisfactory outcome. A talocrural angle of 83 degrees suggests an anatomic reduction has been achieved.
Unstable rotational ankle fractures should be treated surgically in order to achieve anatomic reduction (if the fracture is not overly comminuted) as well as restore length, rotation, and alignment. Satisfactory outcomes can be best achieved when these surgical goals are achieved. Postoperative protocols
regarding immobilization and weight bearing may be somewhat variable depending on surgeon preference, fracture pattern, modifiable patient factors, and non-modifiable patient factors.
Lin et al. performed a systematic review of randomized studies looking at postoperative immobilization and rehabilitation following ankle fractures. They found that after surgical fixation, starting exercise in a removable brace improved pain, ankle range of motion, and improved activity limitations but led to a higher rate of adverse events. Early weight-bearing improved ankle range of motion as well. They concluded that there is limited evidence to support removable braces, early weight-bearing, and no immobilization following surgical fixation of ankle fractures.
Reidsma et al. retrospectively reviewed 57 malunited ankle fractures treated with revision osteotomy with a minimum of 10 years of follow-up. They found that 85% of patients had good or excellent outcomes and that prolonged time to reconstructive surgery led to a worse outcome. They concluded that reconstructive surgery should be performed early in the setting of a malunited ankle fracture even with early arthritic changes.
Figure A shows a displaced Weber B fibula fracture with medial joint space widening on stress examination. Illustration A shows intraoperative imaging following open reduction internal fixation of the same patient. Illustration B demonstrates the talocrural angle and medial clear space parameters in an anatomically reduced ankle.
Incorrect Answers:
Answer 1: Nonweightbearing for at least 6 weeks is common; however, some studies have shown improved outcomes in range of motion if weight-bearing is started early in the immobilization period.
Answer 2, 4, and 5: Postoperatively the parameters of the medial clear space
Which of the following arteries supplies the surgical flap in the extensile open treatment of the injury shown in Figure A?
1) Lateral calcaneal branch of the anterior tibial artery
2) Lateral calcaneal branch of the peroneal artery
3) Lateral malleolar branch of the peroneal artery
4) Lateral malleolar branch of the dorsalis pedis artery
5) Lateral malleolar branch of the anterior tibial artery
This patient has a displaced calcaneal fracture that is commonly treated through a lateral extensile approach. The flap of the lateral extensile approach is supplied by the lateral calcaneal branch of the peroneal artery.
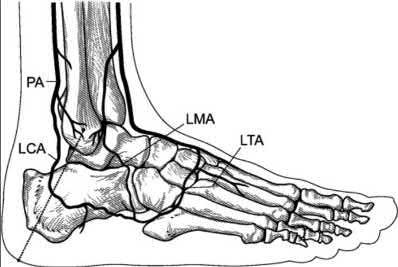
Intraarticular fractures of the calcaneus represent approximately 2% of all fractures and are commonly the result of high-energy trauma such as motor vehicle accidents and falls. Successful operative treatment of these injuries depends on the anatomic reduction of the articular surface; restoration of the alignment, height, and length of the calcaneus; and avoidance of complications. These fractures are usually treated with a lateral extensile approach. The artery which provides blood supply to this flap is the lateral calcaneal branch of the peroneal artery. It is critical to maintain the integrity of this vessel in order to avoid complications.
Borrelli et al. performed a study to describe the arterial blood supply of the subcutaneous tissues of the lateral hindfoot and to define the relationships between these arteries and the lateral extensile incision. The lateral calcaneal artery appeared to be responsible for the blood supply to the corner of the flap.
Figure A demonstrates a displaced fracture of the calcaneus. Illustration A depicts the arteries on the lateral foot (PA: peroneal artery, LCA: lateral calcaneal artery, LMA: lateral malleolar artery, LTA: lateral tarsal artery). Illustration B (Borrelli et al.) is a lateral radiograph of the hindfoot and ankle that demonstrates skin staples placed along the surgical incision and vascular clips placed along the path of each artery. Illustration C is a clinical photograph of the lateral extensile approach.
Incorrect Answers:
Answer 1: The lateral calcaneal artery is a branch of the peroneal artery, not the anterior tibial artery.
Answers 3-5: The lateral malleolar artery is a branch of the anterior tibial artery. It does not supply the flap of the lateral extensile approach.
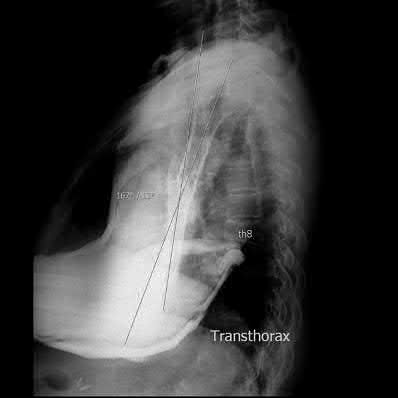
A 25-year-old male presents following a motor vehicle collision with a Glasgow Coma Scale of 7. Subsequent imaging in the trauma bay demonstrates a bifrontal cerebral contusion, an L4 burst fracture, multiple rib fractures, an LC-1 type pelvic ring injury, a femoral shaft fracture, and an open ipsilateral tibial shaft fracture. He is intubated and an intracranial pressure monitor is placed which consistently measures 30mm Hg. He is normotensive with a lactate of 1.5 after 2 liters of crystalloid and 1 unit of packed red blood cells. Which of his injuries would most dictate a temporizing approach with external
fixation of his femoral shaft fracture instead of reamed intramedullary nailing?
1) L4 burst fracture
2) Bifrontal cerebral contusion
3) Open ipsilateral tibia fracture
4) LC1 pelvic ring injury
5) Rib fractures
In the setting of a severe closed head injury such as a bifrontal cerebral contusion with elevated intracranial pressures, external fixation of a femoral shaft fracture is indicated to limit the risk of intraoperative hypotension and decreased cerebral perfusion pressure.
Immediate reamed nailing remains the standard treatment for the vast majority of femoral shaft fractures, however patients with multiple injuries with incomplete resuscitation and patients with severe intracranial trauma may benefit from a damage control approach with external fixation.
Anglen et al retrospectively reviewed the intracranial pressure (ICP) and cerebral perfusion pressure (CPP) in patients undergoing femoral nailing. The authors found a significant decrease in intraoperative CPP, especially in those patient undergoing femoral nailing in the first 24 hours, however they were unable to demonstrate a link between the decreased CPP and poor patient outcomes.
Pietropaoli et al examined the effects of intraoperative hypotension on patients with blunt head trauma. The authors found that 32% of patients experienced intraoperative hypotension (systolic blood pressure less than 90mm Hg) and those patients with a hypotensive episode had an 82% mortality and significantly worse outcomes on the Glasgow Outcomes Scale.
McKee et al conducted a retrospective cohort study comparing matched groups of patients with femoral shaft fractures with and without a closed head injury. In contrast to previous studies, the authors found no significant difference in outcome between the groups including mortality, hospital length of stay or neuropsychologic testing.
Illustration A shows a femoral shaft fracture treated with external fixation. Incorrect Answers:
Answer 1, 3-5: Immediate reamed nailing would not change the outcome of any of these injuries
A 22-year-old left hand dominant laborer sustains the injury shown in Figures A and B as the result of a fall from a ladder. Which of the following has been shown to be true regarding operative versus nonoperative treatment of this injury?
1) Decreased chance of nonunion with nonoperative treatment
2) Improved Constant and DASH scores with operative treatment at all time points
3) Increased symptomatic malunion rate with operative treatment
4) No change in shoulder abduction strength
5) Increased time to union with operative treatment
Surgical management of displaced, shortened clavicle fractures is associated with a decreased rate of nonunion and malunion. General recommendations for surgical treatment include shortening of greater than 2 centimeters.
Kim et al. review clavicle fracture treatment history and current indications. They report that although previous thought was that nearly all clavicle fractures should be treated nonoperatively, outcomes can be improved with fixation of certain clavicle fracture patterns.
COTS et al. performed a multicenter, randomized controlled trial of 132 patients with a displaced midshaft fracture of the clavicle. They found that Constant and DASH scores were improved in the operative fixation group at all points in time, with union time being 28 weeks in the nonoperative group and
16 weeks in the operative group. Malunion was higher in the nonoperative group as well.
McKee et al. reviewed 30 patients who underwent closed treatment of a displaced midshaft clavicle fracture. They found that range of motion of the shoulder was maintained but the strength of the shoulder was decreased to 81% for flexion, 82% for maximum abduction, 81% for maximum external rotation, and 85% for maximum internal rotation. Endurance for these movements was also significantly decreased as compared to the contralateral side.
Figure A shows a clinical photo of a patient with a clavicle fracture. Figure B shows a displaced, comminuted clavicle fracture.
Incorrect Answers:
Answer 1: Operative treatment increases the union rate.
Answer 3: Operative treatment decreases the rate of symptomatic malunion. Answer 4: Operative treatment increases shoulder abduction strength.
Answer 5: Time to union is decreased with operative treatment.
A 45-year-old female presents to the office wearing a right upper arm splint with radiographs shown in Figure A and B. She sustained an isolated closed injury to the right arm 9 days ago. Her soft-tissues and neurological examination are normal. What would be the most appropriate treatment for this injury?
1) Continue current splint for 6 weeks
2) Continue current splint for 3 weeks and transition to hanging arm sling for additional 3 weeks
3) Transition to functional brace for additional 6-8 weeks
4) Open reduction internal fixation with compression plating
5) Staged procedure with humeral external fixator, then open reduction internal fixation with compression plating
Figures A and B show radiographs on a minimally displaced humeral shaft fracture. The most appropriate treatment for this injury would be functional bracing (Sarmiento) for an additional 6-8 weeks or until healed.
Commonly accepted parameters for closed treatment include less than 30 degrees of varus angulation, 20 degrees of anterior/posterior angulation, and 3 cm of shortening. Functional bracing has become the gold standard for humeral shaft fractures as it consistently shows excellent healing results as well as preventing the complication of shoulder +/- elbow stiffness associated with joint spanning splints or slings.
Sarmiento et al. treated 922 patients with humeral diaphysis fractures with a prefabricated brace. They found a 97% rate of union with the use of the brace. In addition, only 2% of the patients had lost more than 25 degrees of shoulder motion at the time of brace removal.
Koch et al. reviewed 67 humeral shaft fractures that were treated by Sarmiento bracing in a 15-year period. Fifty-eight cases (87%) had healed clinically at a mean of 10 weeks. Among 9 patients with delayed or nonunion leading to operative intervention, there were 6 cases with transverse fractures
Figures A and B show a moderately displaced right humeral shaft fracture with 13 degrees of AP angulation, 10 degrees of varus/valgus angulation and no shortening, treated in a coaptation splint. A nondisplaced proximal humeral fracture is also seen. Illustration A shows an image taken of a patient wearing the sarmiento brace.
Incorrect Answers:
Answer 1,2: Joint spanning splints or slings have not shown to be superior to functional bracing. They are associated with joint stiffness post removal.
Answer 4: Operative indications are: associated vascular injuries, bilateral humeral shaft fractures, polytrauma patient (including paraplegia), injury to the brachial plexus, pathological fractures, floating elbow, and floating shoulder.
Answer 5: Staged operative procedure would be indicated in open fractures or significant deformity with soft-tissue swelling.
Which of the following is an appropriate initial step in the management of a multiply injured patient with an unstable pelvic ring fracture and hemodynamic instability?
1) Application of an external fixator
2) Pelvic angiography
3) Pelvic packing
4) Application of a pelvic binder
5) Percutaneous Iliosacral screws
Patients with multiple injuries including a pelvic ring fracture who present with hemodynamic instability should have a pelvic binder or circumferential pelvic sheet placed as part of their initial resuscitation.
A systematic approach to search for sources of bleeding and control ongoing hemorrhage is necessary for patients who present with hemodynamic changes in the setting of a pelvic ring fracture. Management of continued hypotension after pelvic binder placement is controversial and varies among trauma centers.
Krieg et al. prospectively evaluated 16 patients with unstable pelvic ring injuries initially managed with a novel circumferential compression device. The authors found substantial reduction in pelvic width with the use of this
compressive device in patients with volume expanding pelvic ring fractures.
Croce et al. retrospectively compared patients with unstable pelvic ring injuries who were treated with either emergent pelvic fixation (EPF) or a pelvic orthotic device (POD). The authors found that those patients treated with POD had decreased transfusion requirements and shorter length of hospital stay.
Routt et al describe their technique for circumferential pelvic antishock sheeting (CPAS). The authors provide an illustrative case and discuss the potential advantages of sheet application versus other techniques of pelvic stabilization.
Illustration A is the initial AP radiograph of a patient with a pelvic fracture and hemodynamic instability. The pelvic binder was placed in the field prior to arrival. Illustration B demonstrates the same patient in the angiography suite after removal of the pelvic binder. Note the increased widening of bilateral SI joints, greater on the left than the right.
Incorrect Answers:
Answer 1: External fixation of pelvic ring fractures can be used to assist with resuscitation but pelvic binder application should be attempted first
Answer 2: The use of pelvic angiography is controversial and institution specific however some centers utilize pelvic angiography as part of the algorithm for management of ongoing hemorrhage.
Answer 3: Pelvic packing is utilized in some centers to control ongoing pelvic hemorrhage however it is not used as initial management of patients with hemodynamic instability
Answer 5: Percutaneous iliosacral screws can also be utilized as a form of resuscitation however they should not be used as as first line of management
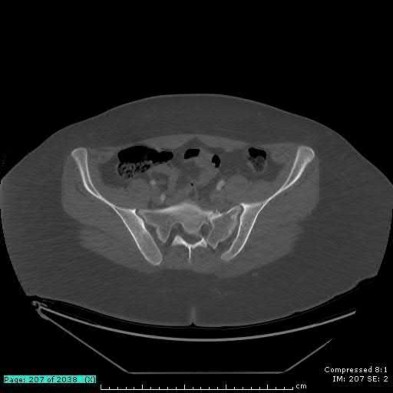
A 19-year-old female sustains the injury shown in Figures A thru C as the result of a motor vehicle collision. Which of the following is the most common cause of death with this type of pelvic injury pattern?
1) Hypovolemic shock
2) Spinal injury
3) Solid organ rupture
4) Acute respiratory distress syndrome
5) Closed head injury
The injury pattern described in the question and images is a lateral compression pelvic ring injury. Of the choices provided, the most common associated cause of death is a closed head injury.
Pelvic ring disruptions are the result of high energy blunt trauma and are associated with other significant injuries in greater than 50% of the cases. These injuries may involve neurovascular structures and other organ systems.
Burgess et al. retrospectively reviewed their pelvic ring injuries and reported their classification system based upon the vector of force involved and the quantification of disruption from that force, i.e., lateral compression, anteroposterior compression, vertical shear, and combined mechanical injury. Overall blood replacement was highest in anterior-posterior patterns. Mortality was also highest in anteroposterior patterns. The most common identifiable cause of death in patients with lateral compression fractures is closed head injury. In contrast, the identifiable cause of death in patients with anteroposterior compression injuries is combined pelvic and visceral injury.
Watnik et al. reviewed lower urinary tract injuries and noted that they occur in as much as 25% of patients with pelvic ring disruptions. They also report that early repair of bladder injury can facilitate the placement anterior pelvic fixation, in efforts to minimize infection.
Smith et al. reviewed hemodynamically unstable pelvic ring fracture patients and found that there is a positive association of blood replacement requirements and mortality. They also reported that death within the first 24 hours after admission was most often a result of acute blood loss while death after the first day was most often caused by multi-organ failure.
Figure A shows an AP pelvic radiograph with evident anterior pelvic ring fractures. Figure B and C are axial CT cuts showing the posterior and anterior ring fractures, respectively. This fracture pattern is consistent with a lateracl compression mechanism.
Incorrect Answers:
Answer 1-4: These options are less commonly reported as causes of death than closed head injury in a lateral pelvic ring injury mechanism.
A 67-year-old male is involved in a motor vehicle accident and presents with the closed orthopedic injuries shown in Figures A and B. He is also noted to have a grade 1 splenic laceration and lung contusion. He is cleared by the trauma team, and undergoes early total care with reamed femoral and tibial nailing. A tourniquet is used for the tibial nailing portion of the case, and the tibial isthmus is over reamed to accept a larger nail. The use of a tourniquet in this case has been most clearly shown to be associated with which of the following?
1) Tibia shaft necrosis post-operatively
2) Increased pulmonary morbidity post-operatively
3) Increased cortical bone temperature during reaming
4) Increased nonunion rates
5) Decreased pain post-operatively
In patients with multitrauma, combining reamed femoral nailing with fracture fixation (ie. tibial shaft) under tourniquet control has been shown to increase pulmonary morbidity.
Limb reperfusion after tourniquet ischemia causes pulmonary microvascular injury. Similarly, microembolization, like that associated with reamed femoral nailing, can induce pulmonary microvascular injury. Both processes result in increased pulmonary capillary membrane permeability and edema, and ultimately increased pulmonary morbidity.
Karunakar et al showed in a canine model that there is no significant difference in the heat generated during reaming with and without a tourniquet. The factor that made the most difference was related to the size of the reamer used compared with the diameter of the isthmus. They concluded that the risk of
thermal necrosis appears to be related more to the process of intramedullary reaming than to the tourniquet.
Giannoudis and associates performed a prospective randomized trial on 34 patients to measure the rise of temperature during reaming of the tibia before intramedullary nailing with and without the use of a tourniquet. The factor that generated the most heat was using large reamers (11 mm to 12 mm) in a patient with a small isthmus (8 mm to 9 mm). Use of a tourniquet, steroid use, and knee flexion during reaming were not shown to be associated with diaphyseal necrosis after reamed tibial nailing.
Pollak et al evaluated the association between femoral nailing followed by tourniquet ischemia and clinical lung injury. They reviewed 72 patients with femoral shaft fractures and tibial or ankle fractures requiring internal fixation over a six year period. All femoral shaft fractures were treated with reamed intramedullary nails, and the patients were divided into groups, based on whether the tibial or ankle injury was managed surgically with or without a tourniquet. They noted increased pulmonary morbidity in the group where a tourniquet was used.
Figure A shows a femoral shaft fracture at the junction of the middle and proximal one-third of the femoral shaft. Figure B shows a contralateral tibial shaft fracture.
Incorrect Answers:
1-Tourniquet use has not been shown to lead to thermal necrosis of the bone during reaming of the tibial shaft.
the fracture to flex, due to the avoidance of excessive knee flexion during the reduction. Illustration A is an example of semiextended positioning for tibial nailing. Illustration B shows radiograph utilizing posterior blocking screws to prevent procurvatum deformity.
Tornetta et al looked at the semiextended intramedullary nailing of proximal tibia fractures. Of the 24 patients nailed using this technique, 19 had no anterior angulation, while only 5 had less than 5 degrees of flexion deformity.
In their study, Kubiak et al also advocate the semiextended position for tibial nailing. They note better control of fracture alignment and stabilization especially in the sagittal plane, and better ability to obtain imaging and maintenance of reduction during nail insertion and locking.
Incorrect answers:
would help to avoid valgus deformity. Answer 3 would worsen the flexion deformity.
Answer 4 would worsen the flexion deformity and drive the nail posterior in distal segment.
Answer 5 would not affect flexion deformity.
Which of the following cannulated screw configurations used in the treatment of subcapital femoral neck fractures is optimal?
1) Inverted triangle pattern with the inferior screw posterior to midline and adjacent to the calcar
2) Inverted triangle pattern with the inferior screw anterior to midline and adjacent to the calcar
3) Triangle pattern with the superior screw posterior to midline and adjacent to the calcar
4) Inverted triangle pattern with the inferior screw posterior to midline and central in the femoral neck
5) Inverted triangle pattern with the inferior screw anterior to midline and central in the femoral neck
The strongest portion of the femoral neck is the posterior inferior neck in the region of the femoral calcar. The optimal biomechanical configuration includes an inverted triangle pattern with the single screw in the inferior aspect of the femoral neck adjacent to the calcar.
Booth et al performed a cadaveric study comparing central versus calcar (cortical-adjacent) fixation. The results demonstrated significant improved stability, load, stiffness, and displacement in all tested parameters for the group with calcar-adjacent screw fixation.
Lindequist and Törnkvist performed a Level 4 study of 72 femoral neck fractures. They found that all 5 of their nonunions had screws placed greater than 3mm from the femoral calcar. Additionally, 16 of 18 fractures healed in the group of displaced fractures where both the fixating screws were placed within 3 mm from the femoral neck cortex.
Gurusamy et al performed a Level 4 study of 395 patients undergoing femoral neck fixation. They found a reduced spread of the screws on the lateral view was associated with an increased risk of nonunion of the fracture.
Illustration A depicts the optimal configuration of an inverted triangle with the single screw being inferior and all of the screws being cortical adjacent.
A 63-year-old female sustained a distal radius and associated ulnar styloid fracture 3 months ago after being involved in a motor vehicle collision. Radiographs obtained at the time of injury are shown in Figure A. She underwent open reduction and fixation of the distal radius fracture, and current radiographs are shown in Figure B. At the time of the index operation, there was no distal radioulnar joint instability after plating of the radius. Which of the following is true post-operatively regarding this patient's ulnar styloid fracture?
1) Worse outcomes on the Mayo wrist score are expected without fixation
2) Chronic distal radioulnar joint instability can be expected to occur without fixation
3) Wrist function depends on the level of ulnar styloid fracture and initial displacement
4) Grip strength and wrist range of motion are improved with fixation
5) There is no adverse effect on wrist function or stability without fixation
An accompanying ulnar styloid fracture in patients with stable fixation of a distal radial fracture has no apparent adverse effect on wrist function or stability of the distal radioulnar joint.
Kim et al evaluated 138 patients who underwent surgical treatment of an unstable distal radial fracture, without fixation of an associated ulnar styloid fracture if present. Postoperative evaluation included measurement of grip strength and wrist range of motion; calculation of the modified Mayo wrist score; as well as testing for instability of the distal radioulnar joint at a mean of 19 postoperatively. They did not find a significant relationship between wrist functional outcomes and ulnar styloid fracture level or the amount of displacement.
af Ekenstam et al performed prospective and randomized study of two different treatments of extraarticular Colles' fracture with a fractured ulnar styloid. In one group, the ulnar styloid was left alone, and in the other group it was transfixed and/or the triangular ligament was repaired after closed reduction of the fractured radius. They concluded that repair of the ulnar styloid complex in extraarticular fractures of the distal radius is not better than conventional treatment.
Each of the following are guidelines for management of a domestic violence victim EXCEPT:
1) Socioeconomic status should not preclude evaluation for domestic violence
2) Interview the patient outside the presence of other non-medical personnel
3) Federal law mandates photographs be taken of injuries
4) Document your opinion if the patient’s injuries are not consistent with the offered explanation
5) Physicians should check requirements to see if there is mandatory reporting statute in their state
It is important to fully document the abuse as it has been described to you, however there is no federal law mandating photographic documentation of domestic violence injuries. Photographs may be taken but only with the patient's permission. Disclosure of a diagnosis of abuse to any third party and reporting it to the authorities should be done only with the abused patient’s knowledge and consent, unless there is a mandatory reporting statue in the particular state of practice. Being a female, age 19-29, pregnant, or of a low
socioeconomic status (
An otherwise healthy 34-year-old female undergoes an elective L5-S1 microdiscectomy. At her 4 week followup, she is noted to have drainage from her wound. Labs reveal a CRP of 30 mg/L (normal
1) CRP 20 mg/L, ESR 40 mm/hr
2) CRP 15 mg/L, ESR 20 mm/hr
3) CRP 6 mg/L, ESR 10 mm/hr
4) CRP 1 mg/L, ESR 25 mm/hr
5) CRP 8 mg/L, ESR 5 mm/hr
A normalized C-reactive protein (CRP) value (60 years, smoking, diabetes, previous surgical infection, increased body mass index, and alcohol abuse were all statistically significant preoperative risk factors for developing a post-op wound infection.. The most likely procedure to be complicated by an infection was a combined anterior/posterior spinal fusion performed in a staged manner under separate anesthesia. Infections were primarily monomicrobial and the most common organism cultured from the wounds was Staphylococcus aureus.
Illustration A shows the CRP trends in the study by Khan et al. with postoperative wound infections after spinal surgery treated with IV antibiotics. ER refers to early responder while LR refers to late responder. At the 4-week time point, 16 patients have shown clinical improvement with no fevers, wound drainage, erythema, or need for wound packing. The other 5 patients, referred to as late responders, have shown one or more clinical signs of infection in addition to having an elevated CRP. At 20 weeks, both early and late responders both have shown normalized CRP levels and no clinical evidence of infection. Illustration B shows the ESR trends in the those which demonstrated incomplete normalization of ESR values despite resolution of infection.
Incorrect Answers:
Answer 1, 2, 3, 5: CRP levels > 3 mg/L are elevated and indicate incomplete response to infection
A 25-year-old man is struck by car while crossing the street. His injuries include the closed left tibial shaft fracture shown in Figure A. He is a smoker, but is otherwise healthy. Intramedullary nailing is performed without initial complications. Which of the following puts this patient at greatest risk for tibial nonunion?
1) Use of anti-inflammatories post-operatively
2) Post-operative gapping at the fracture site
3) Presence of an associated fibular fracture
4) History of smoking
5) Mechanism of injury
Post-operative gapping at the fracture site significantly increased the risk of reoperation due to nonunion or malunion.
Bhandari et al performed a retrospective study to identify which prognostic factors were associated with an increased risk of reoperation for nonunion in surgically treated tibial shaft fractures. They examined over 200 fractures, and found the presence of an open fracture wound (RR 4.32), lack of cortical continuity between the fracture ends following fixation (RR 8.33), and the presence of a transverse fracture (RR 20.0) were the three variables most predicitive of reoperation.
Audige et al analyzed 416 patients with operatively treated tibial shaft fractures who were followed for at least 6 months. They found that the greatest risk for delayed healing or nonunion was the presence of an open injury, fractures of the distal 1/3 of the tibia, and postoperative gapping at the
fracture site (The risk of healing problems was doubled for fractures of the distal shaft and for fractures showing a postoperative diastasis).
Figure A is a radiograph of a healthy, independent 51-year-old male. He is treated with immediate open reduction internal fixation to prevent which of the following complications?
1) Fracture non-union
2) Avascular necrosis
3) Skin necrosis
4) Plantar flexion weakness
5) Ankle stiffness
Figure A shows an avulsion fracture of the calcaneal tuberosity. Immediate open reduction and internal fixation is required to prevent wound complications.
Displaced avulsion fractures of the calcaneal tuberosity should be managed urgently to prevent necrosis of the soft tissues overlying the heel. In these injuries, the Achilles tendon is securely attached to the fractured tuberosity. Urgent closed reduction and casting is usually not possible due to the power and proximal pull of the triceps surae. Surgical fixation is required. The best treatment modality is open reduction and bone-to-bone fixation with screws. Closed reduction and percutaneous pinning fixation is not strong enough to provide a stable fixation of the tuberosity.
Lui reported on avulsion fractures of the bony insertion of the Achilles tendon at the calcaneus. He stated that screw fixation alone is not sufficient for repair of these injuries. His technique involved two suture anchors used capture the small bone fragment to the calcaneus. This allowed for the pull of the triceps surae to be neutralized and early physical therapy.
Hess et al. looked at a case series of calcaneal tuberosity avulsion fractures that were treated in a delayed fashion. All three patients with posterior tuberosity calcaneal avulsion fractures developed skin necrosis because of a delay in treatment.
Figure A shows a displaced posterior tuberosity calcaneal avulsion fracture. Illustration A shows skin breakdown overlying the posterior tuberosity calcaneal avulsion fracture.
Incorrect Answers:
Answer 1: The amount of displacement is an indication for fixation, however urgent treatment does not improve union rates with these fractures.
Answer 2: Tuberosity calcaneal avulsion fractures rarely disrupt the blood supply to the avulsion fragment and are not associated with avascular necrosis.
Answer 3: Plantar flexion weakness is a known complication of these injuries despite many treatment options.
Answer 4: Ankle stiffness is most commonly related to surgical fixation methods and post-operative immobilization and delayed rehabilitation.
A 22-year-old male presents 4 weeks following open reduction and internal fixation of his unstable ankle fracture. He has had three days of increasing pain, swelling and the new onset of purulent drainage from the mid-portion of the lateral incision. Laboratory values, including white blood cell count, sedimentation rate, and C-reactive protein are elevated. Current radiographs are seen in Figures A and B. On examination the wound probes deep and likely involves the lateral plate. What is the best step in management at this time?
1) Suppression with broad spectrum oral antibiotics until fracture healing
2) Suppression with broad spectrum intravenous antibiotics until fracture healing
3) Surgical debridement, removal of internal fixation, culture specific antibiotics, casting until fracture healing
4) Surgical debridement, maintenance of internal fixation, culture specific antibiotics until fracture healing
5) Wound culture in the office and suppression with culture specific antibiotics until fracture healing
The patient is presenting with an acute deep infection following open reduction and internal fixation of an unstable ankle fracture. Recent studies have shown that a protocol of early aggressive surgical debridement, maintenance of internal fixation and culture specific antibiotics can be effective at achieving fracture healing.
Management of early postoperative infection following open reduction and internal fixation can be challenging. Effective treatment typically involves a combination of surgical debridement and culture specific antibiotics. Removing internal fixation prior to fracture healing can lead to additional insult to the soft tissue and ongoing inflammation secondary to fracture instability. Recently published protocols have shown effective treatment with maintenance of implants and culture specific antibiotics following early, aggressive surgical debridement.
Berkes et al. performed a multi-center retrospective study of 121 patients with acute postoperative infection (defined as less than 6 weeks from surgery) following internal fracture fixation. The authors demonstrated a 71% rate of success (defined by maintenance of implants until fracture healing) with a protocol of debridement and suppression with culture specific antibiotics. Risk factors for failure of this technique include open fractures and the use of an intramedullary nail for fracture fixation.
Figures A and B show an ankle status post open reduction and internal fixation of a lateral malleolus fracture. There are no signs of loosening of fixation or cortical erosions concerning for osteomyelitis.
Illustrations A and B are weight bearing X-rays that demonstrate the same fracture, now healed, after debridement and culture specific antibiotics.
Illustrations C and D demonstrate the same fracture after elective removal of implants at 10 months following the index procedure. Intraoperative cultures at the time of hardware removal were negative for recurrent infection.
Incorrect answers:
Answers 1 and 2: Broad spectrum antibiotics without surgical debridement would not be effective in dealing with the infection in this clinical scenario with purulence tracking to the level of the plate
Answer 3: Surgical debridement and antibiotics would control the infection adequately, however removal of fracture fixation in an unstable fracture would lead to instability, soft tissue inflammation and likely malunion or nonunion that would require complex revision
Answer 5: Although culture specific antibiotics are an improvement over broad spectrum, again surgical debridement in conjunction with antibiotics is the most appropriate choice in this scenario. Intraoperative deep cultures in a sterile environment are preferred over cultures obtained in the office.
A 28-year-old male sustained an ankle injury 3 months ago, and was treated with closed management and splinting; a current x-ray is shown in Figure A. Which of the following is the most important factor in deciding between a joint sacrificing and a joint preserving operation for this patient at this time?
1) Workers' Compensation involvement
2) Gender
3) Date of injury
4) Degree of tibiotalar arthritis
5) Degree of deformity
This patient presents with malunion after sustaining a bimalleolar ankle fracture. Surgical treatment options consist of osteotomy for deformity correction with internal fixation (joint preserving) versus fusion (joint sacrificing) with the primary determinant being the amount of ankle arthritis present.
When treating ankle malunions, the decision to perform deformity correction and preserve the joint versus fusing the joint is dependent on signs of progressive, advanced tibiotalar arthritis on radiographs.
Yablon and Leach followed 26 patients following corrective fibular osteotomy following malunion and noted excellent results at a mean follow-up of 7 years. All but 3 returned to preinjury level of activity and had desired outcomes following deformity correction.
Reidsma et al. prospectively followed 57 patients with a minimum follow-up of 10 years following corrective osteotomy and fixation for ankle fracture malunions. Good to excellent results were obtained for 85% of the cohort. The authors concluded that those ankle fracture malunions with none to minimal arthritic changes should still receive corrective osteotomy to prevent further progression of arthritis.
Yablon et al. following 53 patients for 6-9 months, reported on the importance of anatomic restoration of the lateral malleolus when fixing bimalleolar ankle fractures. With anatomic reduction and fixation, no progression of arthritis was noted with return to function.
Figure A is an AP radiograph of a right ankle fracture malunion. Incorrect answers:
Answers 1-3, 5: Factors such as age, gender, and degree of deformity are not
as important as the presence of advanced arthritis that may suggest requiring a joint sacrificing fusion procedure. The date of injury may portend a poor outcome (the longer from the date of injury/subsequent malunion), but is not the most important factor in deciding between corrective osteotomy versus fusion.
A 45-year-old male presents after falling off of a ladder. Radiograph is shown in Figure A. Which of the following is the appropriate sequence in management?
1) Closed reduction, splint application, computed tomography (CT) scan, delayed open reduction and internal fixation
2) Closed reduction, cast application, close observation
3) Splint application, CT scan, application external fixator, delayed open reduction and internal fixation
4) Splint application, application external fixator, CT scan, delayed open reduction and internal fixation
5) Splint application, acute open reduction and internal fixation
This patient has sustained a pilon fracture, with severe comminution and impaction at the articular surface.
The correct sequence of management includes (1) immediate splinting, (2) application of an external fixator, (3) restoration of length alignment and rotation with temporizing external fixation, (4) computed tomography, followed by (5) definitive fixation once soft tissues are amenable.
Tornetta and Gorup analyzed the use of preoperative CT scans in comparison to radiographs in preparation for fixing pilon fractures. The authors noted increased recognition of intra-articular fragments, comminution and noted a high percentage of operative planning changes following CT analysis.
Furthermore, the authors recommended CT scans AFTER external fixation, for even better fragment characterization.
Marsh et al. in their instructional course lecture provide tips and tricks in successful management of pilon fractures. One of the highlighted points include staged, delayed treatment of pilon fractures via spanning external fixator as well as highlighting the importance of obtaining the CT after restoring length and alignment.
Figure A exhibits a radiograph of a comminuted, impacted, shortened pilon fracture.
Incorrect answers:
Answer 1: With such a short, impacted fracture, external fixation as a temporizing measure is recommended to help calm the soft tissue envelope. Answer 2: Closed treatment is not accepted in this type of fracture, due to the high incidence of arthritis and malunion.
Answer 3: CT scan should be obtained AFTER external fixation, not before. Answer 5: This high-energy injury likely has severe soft tissue injury, which is not amenable to acute fixation.
A 45-year-old male with long-standing diabetes sustains the injury shown in Figure A. He has a BMI of 38, established peripheral neuropathy, and his most recent HbA1c is 8.8. What is the most appropriate definitive management option of Figures B through F?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
Open reduction and internal fixation (ORIF) remains the mainstay of treatment for ankle fractures in patients with diabetes.
ORIF for ankle fractures in diabetics can be augmented with increased density of fixation to account for notable, pathologic bone. Specifically, multiple quadricortical syndesmotic screws, bicortical medial malleolar screws, and stiffer plates are all viable options. Furthermore, due to delayed healing properties, prolonged immobilization may also be required to avoid fixation failure.
Guo et al. performed a cohort controlled comparison between diabetics and non-diabetic patients with operative ankle fractures. Although they hypothesized that there would be more complications in the diabetic group, there was no statistical differences in fixation failure or complications when adhering to treatment principles for diabetics (including prolonged non-weight bearing for 10-12 weeks and increased density of fixation).
Chaudhary et al. review the notable complications following ankle fracture treatment in patients with diabetes. In reviewing the literature, the authors recommend ORIF with meticulous soft tissue handling, increased density of fixation, and prolonged immobilization as the mainstay of diabetic ankle fracture treatment. External fixation and frames, while treatment options, should be reserved for salvage or infectious clinical scenarios.
Figure A depicts a bimalleolar ankle fracture. Figure B depicts a cam walker.
Figure C depicts a cast. Figure D standard fixation for ankle fracture for a patient without diabetes. Figure E exhibits definitive fixation with additional screws to increase construct stability. Figure F depicts a ring fixator.
Incorrect Answers:
Answers 1,2: Non-operative treatment is not appropriate for this fracture pattern
Answer 3: Figure D, typically used for those without diabetes is less appropriate for this patient/clinical scenario.
Answer 5: While external fixation and a ring fixator may be utilized, ORIF should be attempted first, however, as it provides stiffer fixation.
Distraction bone block arthrodesis alone would most likely help a patient suffering from a painful calcaneus fracture malunion with all of the following except:
1) Low talar declination angle
2) Hindfoot varus alignment
3) Subtalar arthritis
4) Talonavicular subluxation
5) Peroneal impingement
Distraction bone block arthrodesis in isolation would be unlikely to improve pain related to peroneal impingement. Lateral wall exostectomy would likely be needed for this, and should be concomitantly performed in most cases.
Calcaneal fracture malunions demonstrate several common patterns. Patients may manifest pain from anterior tibiotalar impingement (a result of a low talar declination angle), difficulty with shoe wear due to shortening and widening of the hindfoot, painful talonavicular subluxation, subfibular impingement, and post-traumatic subtalar osteoarthritis. The distraction bone block arthrodesis procedure was developed to eliminate the pain of subtalar arthritis while simultaneously normalizing hindfoot height by inserting a contoured structural bone graft into the subtalar joint. The procedure can correct pathologic hindfoot varus/valgus and restore a normal talocalcaneal angle, thereby improving symptomatic post-traumatic pes planus. The procedure alone does not address lateral wall blowout causing subfibular or peroneal impingement, which requires lateral wall exostectomy. Lateral wall exostectomy therefore should be done in addition to address this issue.
Carr et al. first reported the use of subtalar distraction bone block arthrodesis for salvage of post-traumatic subtalar arthritis following calcaneus fractures. In their 16 patient series, distraction of the subtalar joint with insertion of the bone block allowed for correction of talocalcaneal angle, restoration of hindfoot height, and improvement in symptoms related to tibiotalar impingement.
Clare et al. evaluated a treatment protocol for calcaneal malunions based upon the classification of Stephens and Sanders. Type II and III malunions were treated with subtalar bone-block arthrodesis and other concomitant procedures. They found that their treatment protocol was effective for pain relief, re-establishing a plantigrade foot, and improving function. The most difficult component of the case was restoration of calcaneal height.
Braley et al. evaluated isolated lateral decompression in the treatment of symptomatic calcaneal malunions without concomitant subtalar arthrodesis. These 11 patients had persistent lateral sided pain and their malunions did demonstrate subtalar involvement. The authors reported 9 of the 11 patients had a satisfactory outcome with lateral decompression alone. They concluded that a lateral decompression in management of symptomatic malunions with lateral-sided symptoms is an essential consideration.
Incorrect Answers:
Answer 1: Talar declination angle describes the relative plantar- or dorsiflexion of the talus relative to the ground.
Answer 2: Hindfoot alignment can be improved with distraction arthrodesis. Answer 3: Arthrodesis addresses painful subtalar arthritis.
Answer 4: Restoration of the normal talocalcaneal angle can be achieved, which can also normalize the talonavicular relationship.
A 31-year-old patient has had activity related lateral ankle pain for 4 months. She underwent the procedure shown in Figure A approximately 8 months ago. What surgical technique has most likely resulted in this patients pain?
1) Failure to recognize the most distal screw penetrating the joint surface
2) Low posterior plating with prominent distal screw
3) Failure to recognize an associated syndesmosis disruption
4) Fracture malreduction causing shortening of the fibula
5) Failure to use a longer plate with the lag screw positioned outside the plate
Figure A shows a low posterior plate with a prominent screw head in the most distal hole of the plate. This fixation technique is correlated with peroneal pathology, which usually presents months after fixation when the patient increases their activity level.
The two most common fixation techniques of lateral malleolus fractures are (1) lag screw plus lateral neutralizing plating and (2) posterolateral antiglide plating. The disadvantages of the lateral plating includes the risk of intraarticular screws distally, prominent lateral hardware, and poor distal screw fixation. To overcome these complications, posterolateral antiglide plating allows for bicortical distal fixation with no articular perforation. However, low placement of the plate with a prominent screw head in the most distal hole is associated with symptomatic peroneal pathology. If the most distal screw is not prominent, or absent, this is less likely to cause peroneal complications.
Weber et al. examined the effect of antiglide plate and screw positioning on peroneal tendon pathology. They showed that low posterior plating and large screw heads caused significant retromalleolar pain in most patients. To decrease peroneal pathology, they state that the distal end of the plate should stay proximal to the osteosynovial peroneal groove. Radiologically this level
corresponds to the junction of the proximal and middle thirds of the lateral malleolus.
Figure A shows a posterior positioned 5 hole 1/3 tubular plate. There is no articular screw penetration and the fracture is healed in an anatomical position. The distal aspect of the plate is is the distal third of the lateral malleolus.
Incorrect Answers:
Answer 1: The most distal screws rarely penetrates the joint with the use of fibular antiglide plates. In addition, there is no evidence of screw penetration in this patient.
Answer 3: A missed syndesmosis disruption would usually show some radiographic findings. The tibiofibular clear space is usually most sensitive, which is measured radiographically by the distance from the lateral border of the posterior malleolus in the distal tibia to the medial border of the fibula. As a general rule, it is considered normal if the measurement is less than approximately 6 mm on both AP and mortise views.
Answer 4: The fracture reduction looks anatomic. The talocrural angle, 'dime' sign and “Shenton's line” of the ankle all normal.
Answer 5: The construct used to fix this isolated lateral trans-syndesmotic fracture is acceptable. The one-third tubular plate, which is placed posterolaterally on the fibula as an antiglide plate, indirectly reduces the fracture and acts as a buttress to resist the posterior and proximal displacement of the distal fragment. Insertion of a lag screw through the plate is a described technique.
A 35-year-old painter falls from a ladder sustaining an isolated fracture of his left calcaneus. Months later at follow-up, he is noted to have pain and a catching sensation in his medial foot with active flexion of the great toe. What is the most likely initial injury leading to this complication?
1) Displaced calcaneal beak fracture
2) Displaced fracture of the calcaneal tuberosity
3) Comminuted posterior facet fracture
4) Fracture of the sustentaculum tali
5) Lateral wall blowout fracture
A known complication of fractures of the sustentaculum tali is stenosis (delayed) or injury (acute) of the flexor hallucis longus (FHL) tendon. Stenosis
can cause pain and popping with great toe flexion.
Fractures of the calcaneus often occur after falls from height, and in addition, may be associated with vertebral fractures due to the high-impact mechanism. The FHL tendon runs directly underneath the sustentaculum tali on the medial calcaneus and can be injured causing frank tears or delayed stenosis. These fractures may be missed on ankle or foot plain films alone, and advanced imaging should be ordered if clinical suspicion for calcaneus fractures exists given mechanism and location of pain/swelling.
Komiya et al. present a case report of direct impalement of the FHL tendon in the tunnel under the sustentaculum tali. Though this particular complication is quite rare, such a report highlights the relevant anatomy and structures at risk as well as demonstrates the need for a good clinical exam as the injury was not noted on imaging but the concern was raised on physical exam of FHL involvement.
Della Rocca et al. report their 19-patient series on operatively managed isolated sustentaculum tali fractures. They report a high rate of associated ipsilateral foot injuries (14 patients) and describe fixation using a medial approach and retracting the flexor tendons and neurovascular bundle.
Illustration A is an axial CT image from Della Rocca (2009) et al. showing a representative sustentaculum tali fracture
Incorrect Answers:
Answer 1 - beak fractures are posterior, anatomically related to the Achilles tendon insertion, not the FHL tendon.
Answer 2 - FHL tendon is not associated with the tuberosity.
Answer 3 - FHL tendon runs anterior to the posterior facet and would unlikely be involved in that injury.
Answer 5 - FHL tendon runs medially, not laterally.
A 30-year-old male patient involved in a hang-gliding accident sustains a knee dislocation with multiligamentous knee injury and transection of his peroneal nerve. He undergoes multiple reconstructive surgeries. Two years later, he continues to have a foot drop and dynamic tendon transfer is recommended. This treatment most commonly involves transferring a tendon from which native insertion point to which new insertion point?
1) Plantar distal phalanges to medial navicular
2) Medial navicular to dorsal lateral cuneiform
3) Plantar 1st metatarsal to dorsal lateral cuneiform
4) 5th metatarsal base to dorsal medial cuneiform
5) Plantar distal phalanx of the hallux to dorsal distal phalanx of hallux
Dynamic tendon transfer to restore active dorsiflexion of the foot involves transferring the posterior tibial tendon (PTT) insertion on the medial navicular to the dorsal lateral cuneiform.
Common peroneal nerve (CPN) injuries following traumatic knee dislocation are common, with an incidence of 25-40%. CPN palsy is characterized by foot drop
due to loss of ankle dorsiflexors with a steppage gait and eventual development of a supinated equinovarus foot secondary to the unopposed pull of the PTT. Nonsurgical management involves use of an ankle-foot orthosis and physical therapy. Surgical options include acute primary repair, nerve grafting with either autologous sural nerve or nerve conduits and dynamic tendon transfer. The PTT is harvested from its insertion at the navicular, passed through the interosseous membrane (IOM) and anchored to the lateral cuneiform (see Illustration A). The classic bridle procedure involves concomitant anastamosis of the PTT to the tibialis anterior (TA) and peroneus longus (PL) tendons.
Garozzo et al reported a case series of 62 patients with post-traumatic CPN palsy who underwent a one-stage procedure consisting of nerve repair and PTT transfer. Nerve repair combined with PTT transfer improved postoperative outcomes compared to nerve repair alone. At 2-year follow up, neural regeneration was demonstrated in 90% of patients. The authors hypothesized that poor outcomes following nerve repair alone are due to force imbalance between the functioning flexors and paralyzed extensors, which is somewhat equalized by performing a PTT transfer at time of repair.
Niall et al reviewed 55 patients with traumatic knee dislocation and reported a 41% incidence of CPN injury, exclusively associated with dislocations involving disruption of the posterior cruciate ligament (PCL) and posterolateral corner (PLC). Complete neurologic recovery was found in only 21% of patients. The best prognosis was found with lesions in continuity, less than 7cm of nerve involvement, and short conduction block and muscle activity on nerve conduction and EMG studies.
Vigasio et al described a dynamic tendon transfer technique for traumatic complete CPN injury, involving transfer of the PTT to the TA rerouted to a new origin at the lateral cuneiform to restore ankle dorsiflexion and flexor digitorum longus (FDL) to the extensor digitorum longus (EDL) and extensor hallucis longus (EHL) to restore digit dorsiflexion. Rerouting the TA towards the transferred PTT ensures the PTT harvest length is sufficient. This avoids excessive tensioning of the PTT, which may limit tendon excursion and result in a static tenodesis rather than dynamic function, as well as the need for PTT lengthening which may decrease strength of the transfer
Illustration A is a series of intraoperative photographs demonstrating PTT transfer from Garg et al. An incision is made distal to the medial malleolus and the PTT is harvested subperiosteally (A). The PTT is delivered through a second incision ~15cm proximal to the medial malleolus (B-C). The PTT is then passed through the interosseous membrane and out a third incision over the anterior
fibula (D). Lastly, the PTT is passed through a fourth incision over the dorsal midfoot and anchored to the lateral cuneiform (E).
Incorrect Responses:
Answer 1: Transferring the FDL (insertion = plantar distal phalanges) to the medial navicular is used for correction of flexible flatfoot deformity arising from PTT insufficiency. Some surgeons transfer the FDL to the medial navicular at the time of PTT transfer to the dorsum of the foot, to compensate for loss of PTT function and minimize risk of flatfoot development.
Answers 3: Transferring the PL (insertion = plantar 1st metatarsal) is not recommended, as this muscle is innervated by the CPN via the superficial peroneal nerve and therefore would not be functional.
Answer 4: Transferring the peroneus brevis (PB; insertion = 5th metatarsal base) is not recommended, this muscle is innervated by the CPN via the superficial peroneal nerve and therefore would not be functional.
Answer 5: Transferring the flexor hallucis longus (FHL; insertion = plantar distal phalanx of the hallux) to the insertion of the EHL (dorsal distal phalanx of hallux) is recommended for correction of claw toe deformity and would not help restore foot dorsiflexion in this patient.
Which of the following represents the most common complication following operative treatment of the injury shown in Figure A?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
This patient has a displaced talar neck fracture. The most common complication is post-traumatic arthritis.
Complications after treatment of displaced talar neck fractures are common. Both tibiotalar and subtalar arthritis occur, with subtalar arthritis being the most common. Osteonecrosis is also common, but post-traumatic arthritis is the most common.
Lindvall et al. reviewed 26 displaced talar fractures treated with internal fixation and found that post-traumatic arthritis was the most common complication, occurring in 100% of patients. Osteonecrosis was found in 13 of 26 patients (50%).
Vallier et al. reviewed patients presenting with talar neck fractures and found post-traumatic arthritis in 21 of 39 patients (54%). Osteonecrosis was found in 19 of 39 patients (49%).
Figure A shows a displaced talar neck fracture. Figure B shows talar neck nonunion (arrow) and osteonecrosis of the talar body. Figure C is an AP of the same patient shown in Figure B and again shows osteonecrosis of the talar body. Figure D shows subtalar arthritis after internal fixation of a talar neck fracture via medial malleolar osteotomy. Figure E shows a clinical photo of a patient with a varus malunion after talar neck fracture. Figure F shows a wound dehiscence.
Incorrect answers:
Answers 1, 2, 4, 5. These are all known complications of surgical treatment of displaced talar neck fractures but occur less frequently than post-traumatic arthritis.
A 25-year-old woman began training for a marathon and she reports a 2-week history of heel pain. She has pain throughout the day that worsens with prolonged weight-bearing. On exam, the location of
maximal tenderness is indicated by the white arrow in Figure A. The patient denies point tenderness at the location of the yellow arrow in Figure A. Which of the following MRI images (Figures B to F) would you expect to find in this patient?
1) Figure B
2) Figure C
3) Figure D
4) Figure E
5) Figure F
The clinical presentation is consistent with a stress fracture of the calcaneus. The T1 MRI shows a fracture line within the calcaneus which is consistent with
a calcaneal stress fracture.
Calcaneal stress fractures most commonly occur in long-distance runners and military recruits. Usually, they are caused by overload and inability of bone formation to match resorption. Patients usually begin a rapid increase of activity level from a prior sedentary lifestyle. Patients complain of heel pain that persists throughout the day. The pain is located along the medial and lateral walls of the calcaneus. Diagnosis can be made with radiographs 2-3 weeks after symptom onset by the appearance of a sclerotic line. If the diagnosis is uncertain, MRI may be obtained.
Gehrmann et al. performed a review of stress fractures in the foot. They report that most studies of calcaneal stress fractures are from military recruits.
Primary treatment includes rest, avoidance of weight-bearing, and physical therapy. Patients usually return to full duty between 8 and 10 weeks. Recruits with inadequate treatment had a recurrence of symptoms. They conclude that most studies are from the 1940’s and 1950’s and lack any significant detail into specific treatment protocols.
Sormaala et al. performed a retrospective study in which they reviewed MRIs in all military recruits who had exercise-induced heel pain, over an eight-year period. They report that only 15% of injuries were visible on radiographs and a portion of patients had stress fractures of another tarsal bone. They conclude that a majority of calcaneal stress fractures occur in the posterior part of the bone, but some fractures may be found in the middle and anterior parts. They recommend obtaining an MRI if a radiograph is negative in a patient with exercise-induced foot or heel pain.
Figure A demonstrates the most common area of tenderness and pain of a calcaneal stress fracture, indicated by the white arrow, while the yellow arrow points to the area of tenderness consistent with plantar fasciitis. Figure B is a sagittal T2-weighted MRI demonstrating plantar fasciitis. Figure C is a sagittal T1-weighted MRI demonstrating a calcaneal stress fracture. Figure D is an axial T1-weighted MRI demonstrating a mass on the medial aspect of the calcaneus consistent with a ganglion cyst. Figure E is a sagittal T1-weighted MRI of the foot demonstrating an intraosseous lipoma within the calcaneus. Figure F is a sagittal T2-weighted MRI demonstrating insertional Achilles tendinopathy.
Illustration A demonstrates the most common etiologies of plantar foot pain.
Incorrect Answers:
Answer 1: Figure B, a sagittal T2-weighted MRI, demonstrates plantar fasciitis. Symptoms of plantar fasciitis are sharp heel pain, usually worse in the morning. Tenderness is usually found on the plantar aspect of the foot.
Answer 3: Figure D, an axial T1-weighted MRI, demonstrates a ganglion cyst in the tarsal tunnel. Symptoms of tarsal tunnel syndrome include sharp burning pains in the foot and parasthesias and numbness in the plantar foot.
Answer 4: Figure E, a sagittal T1-weighted MRI, demonstrates an intraosseous lipoma. Intraosseous lipomas are usually incidental findings.
Answer 5: Figure F, a sagittal T2-weighted MRI, demonstrates insertional Achilles tendinitis. This usually presents with pain over the insertion of the Achilles. It may have a relapsing and remitting course, which worsens with activity.
A 35-year-old male fell and sustained an open talar neck fracture. He underwent operative fixation of his fracture. He presents at 2 months after surgery. He denies any constitutional symptoms and his pain is well controlled. On exam, his wounds are well healed with no erythema. Imaging is shown in Figure A. What can the patient be told about his condition?
1) Hawkins sign is positive. The likelihood of developing osteonecrosis is high
2) Hawkins sign is positive. The likelihood of developing osteonecrosis is low
3) Hawkins sign is negative. The likelihood of developing osteonecrosis is high
4) Hawkins sign is negative. The likelihood of developing osteonecrosis is low
5) He has developed chondrolysis
This patient has a positive Hawkins sign, which signifies that he is unlikely to develop osteonecrosis.
A subchondral radiolucency of the talar dome after a talar neck fracture is known as the Hawkins sign. It is an indication that the talar body is viable. It usually appears by 6-8 weeks after injury and is best seen on the mortise view. If the Hawkins sign is present, it is unlikely that the patient will develop osteonecrosis.
Early writes a review on talus fracture management. He reports that talar neck fractures occur through the extra-articular portion of the talus and represent nearly half of talus fractures. The mechanism of injury is a combined ankle dorsiflexion followed by axial compression of the tibiotalar joint. He concludes that anatomic reduction gives the patient the best chance of a good outcome.
Leduc et al. wrote a review on posttraumatic avascular necrosis of the talus. They note that AVN is diagnosed on plain radiography by the absence of the Hawkins sign. They report that CT can also reveal characteristic talar AVN patterns and can be used to confirm radiographic findings. CT helps to assess subtle depression, collapse, fragmentation, and arthritic changes. MRI remains the most sensitive technique for detecting osteonecrosis of the talus, especially in the early stages. They conclude that although there are many published treatments of AVN of the talus, outcome studies are still lacking.
Tezval et al. performed a retrospective review to determine the prognostic reliability, sensitivity, and specificity of the Hawkins sign. They found that in all patients who developed osteonecrosis, none had the Hawkins sign present. In all patients that exhibited a Hawkins sign, none developed osteonecrosis. They determined the sensitivity of the Hawkins sign to be 100% while the specificity was 57.5%. They conclude that if a full or partial positive Hawkins sign is detected, it is unlikely that AVN will develop.
Figure A demonstrates the Hawkins sign with subchondral radiolucency which is noted by arrows in Illustration A.
Incorrect Answers:
Answers 1, 3, 4: The patient has a positive Hawkins sign, therefore the chance of developing osteonecrosis is low.
Answer 5: Chondrolysis is characterized by rapid destruction of articular cartilage on both sides of the joint which leads to loss of joint space
A 25-year-old male presents to the emergency department after a lawnmower accident with traumatic loss of his great toe. On examination, his wound is grossly contaminated with soil. In addition to a cephalosporin and an aminoglycoside, penicillin is given. Which of the following is true with regards to the organism that penicillin is targeting in this injury?
1) It is an Aerobic, Gram-positive rod
2) It is an Anaerobic, Gram-positive coccus
3) It is an Anaerobic, Gram-negative rod
4) It is Catalase positive
5) It may cause botulism
The organism being covered with penicillin is Clostridia spp. Clostridium botulinum is a Gram Positive Bacilli that is the cause of botulism.
Clostridia spp, is a Gram-positive, obligate anaerobic spore-forming rod that is found in soil and gut flora. It produces gas by the fermentation of glucose and
may cause gas gangrene. Common bacteria of this genus are C. perfringens (most common), C. tetani (causes tetanus), C. difficile, and C. botulinum (causes botulism). If wounds are grossly contaminated with soil, penicillin is given to cover against Clostridia.
Decoster et al. performed a review of traumatic foot wounds. They report that lawnmower injuries to the foot are relatively common. IV antibiotic therapy should be initiated with a broad-spectrum cephalosporin and an aminoglycoside to provide coverage against Gram-negative organisms.
Penicillin should be given to protect against Clostridial infection. They conclude that irrigation and debridement is indicated initially followed by packing of open wounds. Repeat debridements are necessary as nonviable tissue demarcates. If major reconstructive procedures are necessary, they should be delayed as they have a high rate of failure if performed too soon.
Cross et al. wrote a review on treatment principles in the management of open fractures and they note that in open fractures with soil contamination, additional coverage should be added for anaerobic bacteria, typically Clostridia. Another member of the genus Clostridia is C. tetani, the causative agent of tetanus. Vaccine status for tetanus must also be assessed in these situations as well.
Illustration A is a radiograph demonstrating soft tissue swelling and subcutaneous emphysema, consistent with gas gangrene. Illustration B is a clinical photograph of gas gangrene evidenced by edema, discoloration, ecchymosis, and hemorrhagic bullae. Illustration C is a pathology slide of C. perfringens, a Gram-positive rod.
Incorrect Answers:
Answers 1, 2, 3: Clostridia are Gram-positive, obligate anaerobes. Answer 4: Clostridia are catalase negative.
All of the following are ways that a negative pressure dressing is beneficial to wound healing EXCEPT:
1) Accelerated granulation tissue formation
2) Removes excess proteins and electrolytes from wound
3) Reducing anaerobic colonization
4) Causes cells to release vascular endothelial growth factor by mechanical force
5) Causes an increase in capillary afterload
Negative pressure dressings or vacuum-assisted wound closures (VAC) apply a negative pressure to the wound bed which allows a decrease in capillary afterload which produces a better inflow of blood.
VAC dressings exert their positive effects on wound healing in multiple ways. Firstly, they remove interstitial fluids, which have been found to contain inhibitory factors that suppress the formation of fibroblasts, vascular endothelial cells, and keratinocytes. This also eliminates the formation of any superficial purulence or slime which also reduces the potential for anaerobic colonization. Removal of excess fluid also pulls out excess proteins and electrolytes to help maintain and osmotic and oncotic gradient. VACs allow arterioles to dilate which produces a proliferation of granular tissue. Also, there is a decrease in capillary afterload, (the pressure against which the heart must overcome to eject blood), which promotes better inflow of blood. Lastly, applying a mechanical force to the surrounding soft tissues allows the edges of the wound to be drawn towards the center, uniformly. This decreases the size of the wound over time. The micromechanical forces exerted on individual cells causes a release in local growth factors, such as vascular endothelial growth factor (VEGF), which stimulate wound healing.
Herscovici et al. applied VAC dressings to 21 consecutive patients with open, high-energy soft tissue injuries. They found that wounds averaged 4.1 sponge changes and the device was used for an average of 19.3 days. 12 wounds avoided the need for further treatment. Only 9 patients required free tissue transfer. They concluded that the VAC is a viable treatment adjunct for the treatment of open, high-energy injuries.
Clare et al. reported their experience with the VAC dressing in the treatment of non-healing, diabetic and dysvascular wounds. They retrospectively reviewed 17 patients with non-healing wounds of the lower extremity. 9 had diabetes and 8 had severe peripheral vascular disease. The average length of treatment
was 8.2 weeks and 14/17 wounds successfully healed, and only 3 failed VAC treatment. They concluded that the VAC dressing is an acceptable option for wound care of the lower extremity.
Illustration A is a photo of an open wound being treated with a VAC dressing. Incorrect Answers:
Answers 1, 2, 3, and 4 are all ways that VAC dressings are beneficial to wound
healing.
Which of the following is true regarding anterior sternoclavicular joint dislocations?
1) Reduction may result in tracheal injury
2) They are usually stable following closed reduction
3) They require fusion to hold the reduction
4) They are rarely symptomatic when left unreduced
5) They should be treated acutely with medial clavicle excision
From the Bicos article, “Anterior SC joint instability should primarily be treated conservatively. The patients should be informed that there is a high risk of persistent instability with nonoperative or operative care, but that the persistent instability will be well tolerated and have little functional impact in the vast majority. Therefore, operative intervention for anterior SC joint instability is mainly cosmetic in nature."
An otherwise healthy 45-year-old female slips and falls with immediate right ankle pain. Stress examination of the right ankle is shown in Figure A. Which of the following is the most important for achieving a satisfactory outcome following open reduction internal fixation for this injury?
1) Weight-bearing before 3 weeks.
2) Medial clear space >5mm
3) Talocrural angle of 83 degrees
4) Tibiofibular clear space of >6mm
5) Talar tilt of >5 degrees
Anatomic reduction of a rotational ankle fracture is considered the most important factor in achieving a satisfactory outcome. A talocrural angle of 83 degrees suggests an anatomic reduction has been achieved.
Unstable rotational ankle fractures should be treated surgically in order to achieve anatomic reduction (if the fracture is not overly comminuted) as well as restore length, rotation, and alignment. Satisfactory outcomes can be best achieved when these surgical goals are achieved. Postoperative protocols
regarding immobilization and weight bearing may be somewhat variable depending on surgeon preference, fracture pattern, modifiable patient factors, and non-modifiable patient factors.
Lin et al. performed a systematic review of randomized studies looking at postoperative immobilization and rehabilitation following ankle fractures. They found that after surgical fixation, starting exercise in a removable brace improved pain, ankle range of motion, and improved activity limitations but led to a higher rate of adverse events. Early weight-bearing improved ankle range of motion as well. They concluded that there is limited evidence to support removable braces, early weight-bearing, and no immobilization following surgical fixation of ankle fractures.
Reidsma et al. retrospectively reviewed 57 malunited ankle fractures treated with revision osteotomy with a minimum of 10 years of follow-up. They found that 85% of patients had good or excellent outcomes and that prolonged time to reconstructive surgery led to a worse outcome. They concluded that reconstructive surgery should be performed early in the setting of a malunited ankle fracture even with early arthritic changes.
Figure A shows a displaced Weber B fibula fracture with medial joint space widening on stress examination. Illustration A shows intraoperative imaging following open reduction internal fixation of the same patient. Illustration B demonstrates the talocrural angle and medial clear space parameters in an anatomically reduced ankle.
Incorrect Answers:
Answer 1: Nonweightbearing for at least 6 weeks is common; however, some studies have shown improved outcomes in range of motion if weight-bearing is started early in the immobilization period.
Answer 2, 4, and 5: Postoperatively the parameters of the medial clear space
Which of the following arteries supplies the surgical flap in the extensile open treatment of the injury shown in Figure A?
1) Lateral calcaneal branch of the anterior tibial artery
2) Lateral calcaneal branch of the peroneal artery
3) Lateral malleolar branch of the peroneal artery
4) Lateral malleolar branch of the dorsalis pedis artery
5) Lateral malleolar branch of the anterior tibial artery
This patient has a displaced calcaneal fracture that is commonly treated through a lateral extensile approach. The flap of the lateral extensile approach is supplied by the lateral calcaneal branch of the peroneal artery.
Intraarticular fractures of the calcaneus represent approximately 2% of all fractures and are commonly the result of high-energy trauma such as motor vehicle accidents and falls. Successful operative treatment of these injuries depends on the anatomic reduction of the articular surface; restoration of the alignment, height, and length of the calcaneus; and avoidance of complications. These fractures are usually treated with a lateral extensile approach. The artery which provides blood supply to this flap is the lateral calcaneal branch of the peroneal artery. It is critical to maintain the integrity of this vessel in order to avoid complications.
Borrelli et al. performed a study to describe the arterial blood supply of the subcutaneous tissues of the lateral hindfoot and to define the relationships between these arteries and the lateral extensile incision. The lateral calcaneal artery appeared to be responsible for the blood supply to the corner of the flap.
Figure A demonstrates a displaced fracture of the calcaneus. Illustration A depicts the arteries on the lateral foot (PA: peroneal artery, LCA: lateral calcaneal artery, LMA: lateral malleolar artery, LTA: lateral tarsal artery). Illustration B (Borrelli et al.) is a lateral radiograph of the hindfoot and ankle that demonstrates skin staples placed along the surgical incision and vascular clips placed along the path of each artery. Illustration C is a clinical photograph of the lateral extensile approach.
Incorrect Answers:
Answer 1: The lateral calcaneal artery is a branch of the peroneal artery, not the anterior tibial artery.
Answers 3-5: The lateral malleolar artery is a branch of the anterior tibial artery. It does not supply the flap of the lateral extensile approach.
A 25-year-old male presents following a motor vehicle collision with a Glasgow Coma Scale of 7. Subsequent imaging in the trauma bay demonstrates a bifrontal cerebral contusion, an L4 burst fracture, multiple rib fractures, an LC-1 type pelvic ring injury, a femoral shaft fracture, and an open ipsilateral tibial shaft fracture. He is intubated and an intracranial pressure monitor is placed which consistently measures 30mm Hg. He is normotensive with a lactate of 1.5 after 2 liters of crystalloid and 1 unit of packed red blood cells. Which of his injuries would most dictate a temporizing approach with external
fixation of his femoral shaft fracture instead of reamed intramedullary nailing?
1) L4 burst fracture
2) Bifrontal cerebral contusion
3) Open ipsilateral tibia fracture
4) LC1 pelvic ring injury
5) Rib fractures
In the setting of a severe closed head injury such as a bifrontal cerebral contusion with elevated intracranial pressures, external fixation of a femoral shaft fracture is indicated to limit the risk of intraoperative hypotension and decreased cerebral perfusion pressure.
Immediate reamed nailing remains the standard treatment for the vast majority of femoral shaft fractures, however patients with multiple injuries with incomplete resuscitation and patients with severe intracranial trauma may benefit from a damage control approach with external fixation.
Anglen et al retrospectively reviewed the intracranial pressure (ICP) and cerebral perfusion pressure (CPP) in patients undergoing femoral nailing. The authors found a significant decrease in intraoperative CPP, especially in those patient undergoing femoral nailing in the first 24 hours, however they were unable to demonstrate a link between the decreased CPP and poor patient outcomes.
Pietropaoli et al examined the effects of intraoperative hypotension on patients with blunt head trauma. The authors found that 32% of patients experienced intraoperative hypotension (systolic blood pressure less than 90mm Hg) and those patients with a hypotensive episode had an 82% mortality and significantly worse outcomes on the Glasgow Outcomes Scale.
McKee et al conducted a retrospective cohort study comparing matched groups of patients with femoral shaft fractures with and without a closed head injury. In contrast to previous studies, the authors found no significant difference in outcome between the groups including mortality, hospital length of stay or neuropsychologic testing.
Illustration A shows a femoral shaft fracture treated with external fixation. Incorrect Answers:
Answer 1, 3-5: Immediate reamed nailing would not change the outcome of any of these injuries
A 22-year-old left hand dominant laborer sustains the injury shown in Figures A and B as the result of a fall from a ladder. Which of the following has been shown to be true regarding operative versus nonoperative treatment of this injury?
1) Decreased chance of nonunion with nonoperative treatment
2) Improved Constant and DASH scores with operative treatment at all time points
3) Increased symptomatic malunion rate with operative treatment
4) No change in shoulder abduction strength
5) Increased time to union with operative treatment
Surgical management of displaced, shortened clavicle fractures is associated with a decreased rate of nonunion and malunion. General recommendations for surgical treatment include shortening of greater than 2 centimeters.
Kim et al. review clavicle fracture treatment history and current indications. They report that although previous thought was that nearly all clavicle fractures should be treated nonoperatively, outcomes can be improved with fixation of certain clavicle fracture patterns.
COTS et al. performed a multicenter, randomized controlled trial of 132 patients with a displaced midshaft fracture of the clavicle. They found that Constant and DASH scores were improved in the operative fixation group at all points in time, with union time being 28 weeks in the nonoperative group and
16 weeks in the operative group. Malunion was higher in the nonoperative group as well.
McKee et al. reviewed 30 patients who underwent closed treatment of a displaced midshaft clavicle fracture. They found that range of motion of the shoulder was maintained but the strength of the shoulder was decreased to 81% for flexion, 82% for maximum abduction, 81% for maximum external rotation, and 85% for maximum internal rotation. Endurance for these movements was also significantly decreased as compared to the contralateral side.
Figure A shows a clinical photo of a patient with a clavicle fracture. Figure B shows a displaced, comminuted clavicle fracture.
Incorrect Answers:
Answer 1: Operative treatment increases the union rate.
Answer 3: Operative treatment decreases the rate of symptomatic malunion. Answer 4: Operative treatment increases shoulder abduction strength.
Answer 5: Time to union is decreased with operative treatment.
A 45-year-old female presents to the office wearing a right upper arm splint with radiographs shown in Figure A and B. She sustained an isolated closed injury to the right arm 9 days ago. Her soft-tissues and neurological examination are normal. What would be the most appropriate treatment for this injury?
1) Continue current splint for 6 weeks
2) Continue current splint for 3 weeks and transition to hanging arm sling for additional 3 weeks
3) Transition to functional brace for additional 6-8 weeks
4) Open reduction internal fixation with compression plating
5) Staged procedure with humeral external fixator, then open reduction internal fixation with compression plating
Figures A and B show radiographs on a minimally displaced humeral shaft fracture. The most appropriate treatment for this injury would be functional bracing (Sarmiento) for an additional 6-8 weeks or until healed.
Commonly accepted parameters for closed treatment include less than 30 degrees of varus angulation, 20 degrees of anterior/posterior angulation, and 3 cm of shortening. Functional bracing has become the gold standard for humeral shaft fractures as it consistently shows excellent healing results as well as preventing the complication of shoulder +/- elbow stiffness associated with joint spanning splints or slings.
Sarmiento et al. treated 922 patients with humeral diaphysis fractures with a prefabricated brace. They found a 97% rate of union with the use of the brace. In addition, only 2% of the patients had lost more than 25 degrees of shoulder motion at the time of brace removal.
Koch et al. reviewed 67 humeral shaft fractures that were treated by Sarmiento bracing in a 15-year period. Fifty-eight cases (87%) had healed clinically at a mean of 10 weeks. Among 9 patients with delayed or nonunion leading to operative intervention, there were 6 cases with transverse fractures
Figures A and B show a moderately displaced right humeral shaft fracture with 13 degrees of AP angulation, 10 degrees of varus/valgus angulation and no shortening, treated in a coaptation splint. A nondisplaced proximal humeral fracture is also seen. Illustration A shows an image taken of a patient wearing the sarmiento brace.
Incorrect Answers:
Answer 1,2: Joint spanning splints or slings have not shown to be superior to functional bracing. They are associated with joint stiffness post removal.
Answer 4: Operative indications are: associated vascular injuries, bilateral humeral shaft fractures, polytrauma patient (including paraplegia), injury to the brachial plexus, pathological fractures, floating elbow, and floating shoulder.
Answer 5: Staged operative procedure would be indicated in open fractures or significant deformity with soft-tissue swelling.
Which of the following is an appropriate initial step in the management of a multiply injured patient with an unstable pelvic ring fracture and hemodynamic instability?
1) Application of an external fixator
2) Pelvic angiography
3) Pelvic packing
4) Application of a pelvic binder
5) Percutaneous Iliosacral screws
Patients with multiple injuries including a pelvic ring fracture who present with hemodynamic instability should have a pelvic binder or circumferential pelvic sheet placed as part of their initial resuscitation.
A systematic approach to search for sources of bleeding and control ongoing hemorrhage is necessary for patients who present with hemodynamic changes in the setting of a pelvic ring fracture. Management of continued hypotension after pelvic binder placement is controversial and varies among trauma centers.
Krieg et al. prospectively evaluated 16 patients with unstable pelvic ring injuries initially managed with a novel circumferential compression device. The authors found substantial reduction in pelvic width with the use of this
compressive device in patients with volume expanding pelvic ring fractures.
Croce et al. retrospectively compared patients with unstable pelvic ring injuries who were treated with either emergent pelvic fixation (EPF) or a pelvic orthotic device (POD). The authors found that those patients treated with POD had decreased transfusion requirements and shorter length of hospital stay.
Routt et al describe their technique for circumferential pelvic antishock sheeting (CPAS). The authors provide an illustrative case and discuss the potential advantages of sheet application versus other techniques of pelvic stabilization.
Illustration A is the initial AP radiograph of a patient with a pelvic fracture and hemodynamic instability. The pelvic binder was placed in the field prior to arrival. Illustration B demonstrates the same patient in the angiography suite after removal of the pelvic binder. Note the increased widening of bilateral SI joints, greater on the left than the right.
Incorrect Answers:
Answer 1: External fixation of pelvic ring fractures can be used to assist with resuscitation but pelvic binder application should be attempted first
Answer 2: The use of pelvic angiography is controversial and institution specific however some centers utilize pelvic angiography as part of the algorithm for management of ongoing hemorrhage.
Answer 3: Pelvic packing is utilized in some centers to control ongoing pelvic hemorrhage however it is not used as initial management of patients with hemodynamic instability
Answer 5: Percutaneous iliosacral screws can also be utilized as a form of resuscitation however they should not be used as as first line of management
A 19-year-old female sustains the injury shown in Figures A thru C as the result of a motor vehicle collision. Which of the following is the most common cause of death with this type of pelvic injury pattern?
1) Hypovolemic shock
2) Spinal injury
3) Solid organ rupture
4) Acute respiratory distress syndrome
5) Closed head injury
The injury pattern described in the question and images is a lateral compression pelvic ring injury. Of the choices provided, the most common associated cause of death is a closed head injury.
Pelvic ring disruptions are the result of high energy blunt trauma and are associated with other significant injuries in greater than 50% of the cases. These injuries may involve neurovascular structures and other organ systems.
Burgess et al. retrospectively reviewed their pelvic ring injuries and reported their classification system based upon the vector of force involved and the quantification of disruption from that force, i.e., lateral compression, anteroposterior compression, vertical shear, and combined mechanical injury. Overall blood replacement was highest in anterior-posterior patterns. Mortality was also highest in anteroposterior patterns. The most common identifiable cause of death in patients with lateral compression fractures is closed head injury. In contrast, the identifiable cause of death in patients with anteroposterior compression injuries is combined pelvic and visceral injury.
Watnik et al. reviewed lower urinary tract injuries and noted that they occur in as much as 25% of patients with pelvic ring disruptions. They also report that early repair of bladder injury can facilitate the placement anterior pelvic fixation, in efforts to minimize infection.
Smith et al. reviewed hemodynamically unstable pelvic ring fracture patients and found that there is a positive association of blood replacement requirements and mortality. They also reported that death within the first 24 hours after admission was most often a result of acute blood loss while death after the first day was most often caused by multi-organ failure.
Figure A shows an AP pelvic radiograph with evident anterior pelvic ring fractures. Figure B and C are axial CT cuts showing the posterior and anterior ring fractures, respectively. This fracture pattern is consistent with a lateracl compression mechanism.
Incorrect Answers:
Answer 1-4: These options are less commonly reported as causes of death than closed head injury in a lateral pelvic ring injury mechanism.
A 67-year-old male is involved in a motor vehicle accident and presents with the closed orthopedic injuries shown in Figures A and B. He is also noted to have a grade 1 splenic laceration and lung contusion. He is cleared by the trauma team, and undergoes early total care with reamed femoral and tibial nailing. A tourniquet is used for the tibial nailing portion of the case, and the tibial isthmus is over reamed to accept a larger nail. The use of a tourniquet in this case has been most clearly shown to be associated with which of the following?
1) Tibia shaft necrosis post-operatively
2) Increased pulmonary morbidity post-operatively
3) Increased cortical bone temperature during reaming
4) Increased nonunion rates
5) Decreased pain post-operatively
In patients with multitrauma, combining reamed femoral nailing with fracture fixation (ie. tibial shaft) under tourniquet control has been shown to increase pulmonary morbidity.
Limb reperfusion after tourniquet ischemia causes pulmonary microvascular injury. Similarly, microembolization, like that associated with reamed femoral nailing, can induce pulmonary microvascular injury. Both processes result in increased pulmonary capillary membrane permeability and edema, and ultimately increased pulmonary morbidity.
Karunakar et al showed in a canine model that there is no significant difference in the heat generated during reaming with and without a tourniquet. The factor that made the most difference was related to the size of the reamer used compared with the diameter of the isthmus. They concluded that the risk of
thermal necrosis appears to be related more to the process of intramedullary reaming than to the tourniquet.
Giannoudis and associates performed a prospective randomized trial on 34 patients to measure the rise of temperature during reaming of the tibia before intramedullary nailing with and without the use of a tourniquet. The factor that generated the most heat was using large reamers (11 mm to 12 mm) in a patient with a small isthmus (8 mm to 9 mm). Use of a tourniquet, steroid use, and knee flexion during reaming were not shown to be associated with diaphyseal necrosis after reamed tibial nailing.
Pollak et al evaluated the association between femoral nailing followed by tourniquet ischemia and clinical lung injury. They reviewed 72 patients with femoral shaft fractures and tibial or ankle fractures requiring internal fixation over a six year period. All femoral shaft fractures were treated with reamed intramedullary nails, and the patients were divided into groups, based on whether the tibial or ankle injury was managed surgically with or without a tourniquet. They noted increased pulmonary morbidity in the group where a tourniquet was used.
Figure A shows a femoral shaft fracture at the junction of the middle and proximal one-third of the femoral shaft. Figure B shows a contralateral tibial shaft fracture.
Incorrect Answers:
1-Tourniquet use has not been shown to lead to thermal necrosis of the bone during reaming of the tibial shaft.
Question 5High Yield
**ONLINE ORTHOPEDIC MCQS SPINE0 9**
**1**. Which is the best initial study for the diagnostic evaluation of diskogenic low back pain?
**1**. Which is the best initial study for the diagnostic evaluation of diskogenic low back pain?
Explanation
Radiography is the best initial study for the evaluation of diskogenic low back pain. The normal degenerative process can be evaluated. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain should also be evaluated. The other tests may be beneficial but represent later imaging options.**
**REFERENCE: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 319-329.**
**2****. A patient who is an observant Jehovah’s Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?
1- Transfusion of whole blood
2- Transfusion of packed red blood cells
3- A cell saver with continuity maintained in a “closed circuit”
4- Transfusion of plasma
5- Transfusion of platelets
PREFERRED RESPONSE: 3**
**DISCUSSION: Jehovah’s Witnesses will not accept the transfusion of blood or blood products such as packed red or white cells, platelets, or plasma. However, many Jehovah’s Witnesses will accept the use of a cell saver in a “closed circuit.”**
**
**REFERENCE: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 319-329.**
**2****. A patient who is an observant Jehovah’s Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?
1- Transfusion of whole blood
2- Transfusion of packed red blood cells
3- A cell saver with continuity maintained in a “closed circuit”
4- Transfusion of plasma
5- Transfusion of platelets
PREFERRED RESPONSE: 3**
**DISCUSSION: Jehovah’s Witnesses will not accept the transfusion of blood or blood products such as packed red or white cells, platelets, or plasma. However, many Jehovah’s Witnesses will accept the use of a cell saver in a “closed circuit.”**
**
Scientific References
- : Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.**
**www.watchtower.org. Official Web Site of Jehovah’s Witnesses. Link verified as active as of August 8, 2008.**
**3****. Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy?
1- Space available for the cord of less than 8 mm
2- Ossification of the posterior longitudinal ligament
3- Fixed cervical kyphosis
4- Previous posterior surgery
5- Concomitant cervical radiculopathy
PREFERRED RESPONSE: 3**
**DISCUSSION: Laminoplasty or any posterior decompressive procedure is contraindicated in patients with cervical spondylotic myelopathy and cervical kyphosis. The residual kyphotic posture of the cervical spine results in persistent spinal cord compression. The other choices are not contraindications for laminoplasty. Concomitant cervical radiculopathy can be addressed at the time of laminoplasty with a keyhole foraminotomy.**
**REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.**
**Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-247.**
**4****. A 44-year-old man reports persistent left leg pain following a L5-S1 hemilaminotomy and partial diskectomy. Examination shows a grade 4 weakness of the left extensor hallucis longus and a positive left straight leg raise. A radiograph is shown in Figure 1a, and sagittal and axial MRI scans are shown in Figures 1b and 1c. Nonsurgical management consisting of medication, physical therapy, and injections has failed to provide relief. Surgical management should consist of
1- revision L5-S1 hemilaminotomy.
2- L5-S1 total disk arthroplasty.
3- L5 Gill laminectomy.
4- posterior foraminal decompression and fusion at L5-S1 with instrumentation and bone graft.
5- stand-alone posterior lumbar interbody fusion.
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a grade I isthmic spondylolisthesis at L5-S1. He has an L5 radiculopathy with foraminal stenosis. Any further treatment needs to include an arthrodesis and foraminal decompression. Isolated interbody fusion is contraindicated in patients with spondylolisthesis, as is total disk arthroplasty. Therefore, the best procedure is a posterior fusion with instrumentation and bone graft along with a foraminal decompression.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 311-317.**
**Moller H, Hedlund R: Instrumented and noninstrumented posterolateral fusion in adult spondylolisthesis: A prospective randomized study: Part 2. Spine 2000;25:1716-1721.**
**5****. Bisphosphonates are indicated in the treatment of osteoporosis in patients who have a DEXA T-score of
1- between 0 and 1.
2- between 0 and -1.
3- -3.5 and are already on teriparatide.
4- within one standard deviation from the mean.
5- less than -1.
PREFERRED RESPONSE: 5**
**DISCUSSION: Bisphosphonates are indicated in the treatment of osteoporosis. They have been shown to reduce the incidence of vertebral and extremity fractures in patients with a T-score of less than -1.**
**REFERENCE: Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.**
**6****. A 45-year-old man reports that he awoke 2 weeks ago with severe pain in his right arm. Examination reveals weakness in the biceps, brachialis, and wrist extensors. There is decreased sensation in the thumb and index finger and a diminished brachioradialis reflex. Assuming this patient has a posterolateral herniated nucleus pulposus, what level is involved?
1- C2-3
2- C3-4
3- C4-5
4- C5-6
5- C6-7
PREFERRED RESPONSE: 4**
**DISCUSSION: This is a classic C6 nerve injury, and it is most likely the result of a herniated nucleus pulposus at C5-6. The C5 nerve root controls the elbow flexors, shoulder abductors, and external rotators. The C7 nerve root controls the elbow extensors, wrist pronators, and the triceps reflex.**
**REFERENCES: Standaert CJ: The patient history and physical examination: Cervical, thoracic and lumbar, in Herkowitz HN, Garfin SR, Eismont FJ, et al (eds): Rothman-Simeone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, vol 1, pp 171-186.**
**Bates B: A Guide to Physical Examination and History Taking, ed 5. Philadelphia, PA,
JB Lippincott, 1991.**
**7****. A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent clinical result with complete resolution of leg pain. Three months later she now reports increasing back pain and weakness in her legs. Examination reveals weakness in the quadriceps and tibialis anterior. Radiographs show no interval changes in the position of the hardware. MRI scans are shown in Figures 2a through 2c. What is the next most appropriate step in management?
1- Observation
2- Oral antibiotics only
3- IV antibiotics only
4- Irrigation and debridement of the surgical site
5- Irrigation and debridement of the surgical site with hardware removal
PREFERRED RESPONSE: 4**
**DISCUSSION: The MRI scans reveal a postoperative infection. Observation and antibiotics are not appropriate choices. There is a large fluid collection and this requires decompression because the patient has neurologic changes. There is considerable debate regarding the removal of hardware. Many contend that biofilm on the implants can harbor the infection. However, these complications usually can be treated with serial irrigations, debridements, and IV antibiotics. The incidence of infection has been widely studied with varying rates in fusions with instrumentation. Rates appear to be increased with instrumentation, yet these infections usually can be managed without hardware removal.**
**REFERENCES: Glassman SD, Dimar JR, Puno RM, et al: Salvage of instrumental lumbar fusions complicated by surgical wound infection. Spine 1996;21:2163-2169.**
**Fang A, Hu SS, Endres N, et al: Risk factors for infection after spinal surgery. Spine 2005;30:1460-1465.**
**8****. What is the primary reason for including the ilium in the distal fixation of long instrumentation constructs in adult scoliosis?
1- Better coronal balance
2- Better pelvic balance
3- Reduced fretting and corrosion
4- Improved curve correction
5- Improved fusion success
PREFERRED RESPONSE: 5**
**DISCUSSION: Studies have shown that when compared with fixation to the sacrum alone, the success rate of fusion across the lumbosacral junction increases when both the sacrum and ilium are included in the posterolateral construct. Curve correction, coronal balance, and pelvic balance are all attended to within the thoracolumbar spine and are not directly related to the pelvic fixation. Fretting and corrosion are a byproduct of metal-to-metal connections.**
**REFERENCES: Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.**
**Emami A, Deviren V, Berven S, et al: Outcome and complications of long fusions to the sacrum in adult spine deformity: Luque-Galveston, combined iliac and sacral screws, and sacral fixation. Spine 2002;27:776-786.**
**9****. A 60-year-old man is evaluated in the ICU after a rollover motor vehicle accident 3 days ago. He has multiple upper and lower extremity trauma and was found unresponsive at the accident scene. Surgery is planned for the extremity trauma once the patient is medically stable. He remains intubated and the cervical spine is immobilized in a semi-rigid collar. Examination reveals mild erythema in the posterior occipital cervical region. Initial AP and lateral radiographs of the cervical spine have not revealed any obvious fracture. What is the most appropriate treatment option at this time?
1- Continued semi-rigid immobilization until the extremity surgeries are completed
2- Halo skeletal fixation prior to the extremity surgery
3- Definitive clearance of the cervical spine with CT and/or MRI
4- Removal of the semi-rigid collar and physical examination when the patient is responsive
5- Soft collar immobilization and local wound care
PREFERRED RESPONSE: 3**
**DISCUSSION: Ackland and associates demonstrated that the failure to achieve early spinal clearance in an unconscious blunt trauma patient predisposed the patient to increased morbidity secondary to the prolonged used of cervical immobilization. They demonstrated that the four significant predictors of collar-related ulcers were ICU admission, mechanical ventilation, the necessity for cervical MRI, and the time to cervical spine clearance and collar removal. The risk of pressure-related ulceration increased by 66% for every 1-day increase in Philadelphia collar time and this highlights the need for definitive C-spine clearance.**
**REFERENCES: Ackland HM, Cooper DJ, Malham GM, et al: Factors predicting cervical collar-related decubitus ulceration in major trauma patients. Spine 2007;32:423-428.**
**Hewitt S: Skin necrosis caused by semi-rigid cervical collar in a ventilated patient with multiple injuries. Injury 1994;25:323-324.**
**10****. A 46-year-old woman who was involved in a motor vehicle accident reports a 4-month history of right-sided lower back pain and pain radiating into the right thigh. The patient underwent an extensive 3-month course of physical therapy and now is dependent on narcotic medication for pain control. Epidural injection therapy has failed to improve her symptoms. Examination is significant for weakness of hip flexion in the seated position and for decreased sensation to light touch in the medial anterior thigh region. Straight leg raise is negative, but the femoral stretch test reproduces anterior thigh pain. A CT myelogram image, at L3-L4, is shown in Figure 3. What is the most appropriate management at this time?
1- Repeat epidural steroid injections
2- Wide lumbar laminectomy
3- Microdiskectomy from either a midline approach or far lateral approach
4- Referral to pain management
5- Minimally invasive posterior lumbar interbody fusion
PREFERRED RESPONSE: 3**
**DISCUSSION: The CT scan reveals a right-sided lateral disk protrusion at L3-4 that has been symptomatic for more than 4 months despite appropriate nonsurgical management. Relative surgical indications include persistent radiculopathy despite an adequate trial of nonsurgical management, recurrent episodes of sciatica, persistent motor deficit with tension signs and pain, and pseudoclaudication caused by underlying stenosis. Whereas studies have shown improvement in patients with sciatica from a lumbar disk herniation treated either nonsurgically or surgically, those undergoing surgical treatment had an overall greater improvement of symptoms.**
**REFERENCES: Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.**
**Yorimitsu E, Chiba K, Toyama Y, et al: Long-term outcomes of standard discectomy for lumbar disc herniation: A follow-up study of more than 10 years. Spine 2001;26:652-657.**
**11****. A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time?
1- Lumbar laminectomy with synovial cyst excision
2- Repeat epidural steroid injection
3- Microdiskectomy at L4-5
4- Nonsteroidal medication and outpatient physical therapy
5- Left-sided facet blocks at L4-5 and L5-S1
PREFERRED RESPONSE: 1**
**DISCUSSION: Lumbar spinal stenosis with lumbar radiculopathy can be commonly caused by a synovial cyst arising from the facet joints. Lyons and associates reported on the surgical treatment of synovial cysts in 194 patients. Of the 147 with follow-up data, 91% reported good pain relief and 82% had improvement of their motor deficits. Epstein reported a 58% to 63% incidence of good/excellent results and a 38 to 42 point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis.**
**REFERENCES: Lyons MK, Atkinson JL, Wharen RE, et al: Surgical evaluation and management of lumbar synovial cysts: The Mayo Clinic Experience. J Neurosurg
2000;93:53-57.**
**Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.**
**Epstein NE: Lumbar laminectomy for the resection of synovial cysts and coexisting lumbar spinal stenosis or degenerative spondylolisthesis: An outcome study. Spine 2004;29:1049-1055.**
**12****. Osteoporotic vertebral compression fractures are associated with
1- neurologic deterioration in 33% of patients.
2- osteomalacia in 50% of patients.
3- a further fracture risk rate of 20%.
4- chronic pain in 75% of patients.
5- a 2-year mortality rate that is less than that associated with hip fractures.
PREFERRED RESPONSE: 3**
**DISCUSSION: Osteoporotic vertebral compression fractures are associated with neurologic complications in less than 1% of patients. After the initial fracture however, patients have a 20% risk of further fractures. The mortality rate of patients with vertebral fractures exceeds that of patients with hip fractures when they are followed beyond 6 months.**
**REFERENCES: Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.**
**Lindsay R, Silverman SL, Cooper C, et al: Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285:320-323.**
**Kado DM, Duong T, Stone KL, et al: Incident vertebral fractures and mortality in older women: A prospective study. Osteoporos Int 2003;14:589-594.**
**13****. When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively?
1- 1 month
2- 2 months
3- 4 months
4- 6 months
5- 12 months
PREFERRED RESPONSE: 4**
**DISCUSSION: The effects of cigarette smoking and smoking cessation on spinal fusion have been studied extensively. Although permanent smoking cessation is ideal, significant improvements in fusion rates are seen in patients who avoid smoking for greater than 6 months postoperatively.**
**REFERENCE: Glassman SD, Anagnost SC, Parker A, et al: The effect of cigarette smoking and smoking cessation on spinal fusion. Spine 2000;25:2608-2615.**
**14****. A 19-year-old woman reports persistent neck pain for 2 years. Pain is relieved with aspirin. A bone scan shows intense uptake in the superior, posterior portion of the C3 vertebral body. A sagittal CT reconstruction is shown in Figure 5. Treatment should consist of
1- radiation therapy.
2- en bloc excision.
3- posterior fusion at C2-C3 with instrumentation.
4- CT-guided aspiration followed by IV antibiotics.
5- radiofrequency ablation.
PREFERRED RESPONSE: 2**
**DISCUSSION: The CT scan shows an osteoblastic nidus pathognomic for an osteoid osteoma. Surgical treatment should include an en bloc excision of the lesion. Surgical treatment is not mandatory because the lesion often becomes asymptomatic over time. This lesion is not amenable to radiofrequency ablation due to its proximity to the spinal cord. A complete corpectomy is not necessary to adequately resect the lesion, as only the nidus needs to be removed. Radiation therapy and antibiotics are not appropriate treatments for an osteoid osteoma. Posterior C2-C3 fusion will not address the pathology.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.**
**Hadjipavlou AG, Lander PH, Marchesi D, et al: Minimally invasive surgery for ablation of osteoid osteoma of the spine. Spine 2003;28:E472-E477.**
**15****. A 56-year-old man with a history of chronic lower back pain from lumbar spondylosis reports a 2-day history of acute incapacitating back pain. He denies any history of acute trauma, although he reports the pain starting after a coughing spell. He also reports difficulty urinating and some fecal incontinence. Examination reveals generalized lower extremity weakness, saddle paresthesia, hyporeflexia in the lower extremities, and loss of rectal tone. What is the most appropriate management at this time?
1- Immediate MRI of the lumbar spine
2- General reassurance, anti-inflammatory drugs, and an early home exercise program
3- Immediate radiographs of the lumbar spine and pain medications with 2 days of bed rest if the radiographs are normal
4- Office caudal epidural steroid injection with follow-up in 1 week
5- Outpatient MRI of the lumbar spine with follow-up in 1 week for test results
PREFERRED RESPONSE: 1**
**DISCUSSION: Cauda equina syndrome is a medical emergency that must be quickly diagnosed and treated to avoid long-term complications. Cauda equina syndrome typically presents with low back pain, unilateral or usually bilateral sciatica, saddle sensory disturbances, bladder and bowel dysfunction, and variable lower extremity motor and sensory loss. Although a number of pathologies can cause cauda equina syndrome, in a patient with a history of chronic back pain, disk pathology is the most common cause of acute onset cauda equina syndrome. Whereas radiographs may be useful in a traumatic onset of symptoms, MRI is the most appropriate study. Cauda equina syndrome should be evaluated on an emergent basis and admission for work-up is appropriate.**
**REFERENCES: Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.**
**Small SA, Perron AD, Brady WJ: Orthopedic pitfalls: Cauda equina syndrome. Am J Emerg Med 2005;23:159-163.**
**16****. A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time?
1- Consider fusion surgery
2- Intradiskal ozone therapy
3- Lumbar laminectomy
4- Vertebral augmentation
5- Cognitive intervention and exercise
PREFERRED RESPONSE: 5**
**DISCUSSION: The results of this patient’s lumbar diskography are equivocal at best. The two disks most likely to be her pain generators, based on their MRI appearance, produced 10/10 pain, however it was nonconcordant and did not reproduce any of her typical left-sided radicular symptoms. The only disk that produced concordant back pain was the normal disk at the L5-S1 level and it reproduced radicular symptoms on the side opposite of her typical pain. Based on these findings, it would be difficult to select a level or levels to include in a lumbar fusion. As such, continued nonsurgical management is the safest treatment option at the current time. Brox and associates reported on a randomized clinical trial comparing lumbar fusion to cognitive intervention and exercise and found similar results in both groups, with significantly less risk in the latter.**
**REFERENCES: Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.**
**Carragee EJ: Clinical practice: Persistent low back pain. N Engl J Med 2005;352:1891-1898.**
**17****. A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
1- immobilization with a halo ring and vest with reduction when medically stable.
2- closed traction reduction using Gardner-Wells tongs.
3- posterior open reduction, stabilization, and fusion.
4- cervical MRI followed by reduction.
5- anterior open reduction, stabilization, and fusion.
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a bilateral facet dislocation of C6-C7 with preservation of at least some neurologic function. Urgent reduction is necessary. However, because she is sedated and unable to follow commands, an MRI scan is necessary before any closed or open posterior reduction to look for an associated disk herniation. If a disk herniation is present, it must be removed prior to any reduction maneuver to prevent iatrogenic neurologic injury. It is very unlikely that this injury can be reduced with an open anterior procedure alone.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.**
**Kwon BK, Vaccaro AR, Grauer JN, et al: Subaxial cervical spine trauma. J Am Acad Orthop Surg 2006;14:78-89.**
**18****. A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery the neurophysiologic monitoring shows a rapid drop and then loss of amplitude in the right cortical somatosensory-evoked potential waveform. All other waveforms remained normal and unchanged, including right-sided cervical (subcortical) and peripheral (Erb’s point), and those from the left-sided upper extremity and both lower extremities. What is the most likely cause of the change?
1- Electrode placement
2- Stimulation failure
3- Anesthetic effect
4- Cord ischemia from retraction
5- Cerebral ischemia from retraction
PREFERRED RESPONSE: 5**
**DISCUSSION: The change noted is focal and confined to the cortex, sparing the opposite side, both lower extremities, and the subcortical waveforms, making all the choices unlikely with the exception of carotid compression with focal cortical ischemia. This may be associated with poor collateral flow from the opposite hemisphere due to an incomplete circle of Willis.**
**REFERENCES: Drummond JC, Englander RN, Gallo CJ: Cerebral ischemia as an apparent complication of anterior cervical discectomy in a patient with an incomplete circle of Willis. Anesth Analg 2006;102:896-899.**
**Yeh YC, Sun WZ, Lin CP, et al: Prolonged retraction on the normal common carotid artery induced lethal stroke after cervical spine surgery. Spine 2004;29:E431-E434.**
**19****. A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient’s history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
1- normal postoperative orders with frequent neurologic evaluations for the first 24 hours.
2- administration of IV steroids and placement of a soft cervical collar for 24 hours.
3- placement of both deep and superficial surgical drains prior to wound closure.
4- administration of IV mannitol and placement of a soft collar.
5- maintaining intubation for up to 24 to 48 hours.
PREFERRED RESPONSE: 5**
**DISCUSSION: Airway complications after anterior cervical surgery can be a catastrophic event necessitating emergent intubation for airway protection. Multilevel surgeries requiring long intubation and prolonged soft-tissue retraction as well as preexisting comorbidities may predispose a patient to postoperative airway complications. Sagi and associates reported that surgical times greater than 5 hours, blood loss greater than 300 mL, and multilevel surgery at or above C3-4 are risk factors for airway complications. In surgical procedures with the aforementioned factors, serious consideration should be given to elective intubation for 1 to 3 days to avoid urgent reintubation.**
**REFERENCES: Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953.**
**Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.**
**Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multi-level cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.**
**20****. A 22-year-old woman reports a 4-year history of worsening low back and left lower extremity pain following a motor vehicle accident. Management consisting of physical therapy, chiropractic manipulation, and interventional pain management, including sacroiliac joint injections and epidural steroid injections, has failed to provide relief. A sagittal T** 2**-weighted MRI scan is shown in Figure 8. No nerve root compression is seen on axial images. She is currently working and lives with her fiancé. She smokes half a pack of cigarettes per day and reports depression on her health history. She is being maintained on narcotic analgesics and is having increasing difficulty performing her activities of daily living secondary to pain. What is the most appropriate management at this time?
1- Provocative lumbar diskography
2- Laboratory studies, including a complete blood cell (CBC) count, erythrocyte sedimentation rate (ESR), and urinalysis
3- Cognitive intervention, exercise, and smoking cessation
4- Bilateral lower extremity electromyography and nerve conduction velocity studies
5- Lumbar myelogram with a postmyelography CT scan of the lumbar spine
PREFERRED RESPONSE: 3**
**DISCUSSION: The MRI scan reveals a rudimentary disk at the L5-S1 level, suggesting transitional anatomy. There is a posterior disk bulge at L3-4. At L4-5, there is disk desiccation and loss of disk height, with a posterior disk bulge and a high intensity zone in the posterior annulus, suggesting an annular tear. While these and similar radiographic findings have been associated with the severity of a patient’s pain, they are also commonly found in cross-sectional studies of asymptomatic subjects. Carragee and associates found 59% of symptomatic patients undergoing diskography have high intensity zones as compared to 25% of asymptomatic subjects of a similar patient profile. Diskographic injections provoked pain in disks with high intensity zones approximately 70% of the time whether the individual was previously symptomatic or not. This patient’s non-specific pain pattern does not require further work-up as she is not a surgical candidate.**
**REFERENCES: Carragee EJ, Paragioudakis SJ, Khurana S: 2000 Volvo Award winner in clinical studies: Lumbar high-intensity zone and discography in subjects without low back problems. Spine 2000;25:2987-2992.**
**Pneumaticos SG, Reitman CA, Lindsey RW: Diskography in the evaluation of low back pain.
J Am Acad Orthop Surg 2006;14:46-55.**
**Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.**
**Carragee EJ: Clinical practice: Persistent low back pain. N Engl J Med 2005;352:1891-1898.**
**21****. A 42-year-old man with a history of renal cell carcinoma has progressive weakness in the lower extremities for the past 3 weeks. The patient desires intervention. A sagittal T** 2**-weighted MRI scan is shown in Figure 9a, and a sagittal contrast enhanced T** 1**-weighted MRI scan is shown in Figure 9b. He currently ambulates minimal distances with a walker. His life expectancy is 8 months. Treatment of the spine lesion should consist of
1- radiation therapy.
2- posterior laminectomy.
3- anterior corpectomy and reconstruction.
4- posterior laminectomy and fusion.
5- kyphoplasty.
PREFERRED RESPONSE: 3**
**DISCUSSION: The MRI scans show a metastatic lesion in two contiguous vertebral bodies in the lower thoracic spine. Posterior laminectomy is not indicated because this does not adequately decompress the neural elements and will lead to progressive kyphosis. A posterior fusion may prevent progressive kyphosis but will not decompress the spinal cord. Renal cell carcinoma is not radiosensitive; therefore, radiation therapy would not be helpful in relieving neurologic compression. The lesion should be treated by an anterior corpectomy and reconstruction. This will allow for complete decompression as well as reconstruction of the anterior column. Kyphoplasty is not indicated in a lesion with disruption of the posterior cortex and neurologic impairment.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.**
**White AP, Kwon BK, Lindskog DM, et al: Metastatic disease of the spine. J Am Acad Orthop Surg 2006;14:587-598.**
**22****. A 40-year-old man has intractable pain following 2 years of nonsurgical management for high-grade spondylolisthesis. What is the best surgical option?
1- Posterolateral fusion
2- Posterolateral fusion with instrumentation
3- Circumferential fusion
4- Transforaminal lumbar interbody fusion
5- Anterior lumbar interbody fusion
PREFERRED RESPONSE: 3**
**DISCUSSION: Circumferential fusion is the preferred choice for patients undergoing revision surgery following failed posterolateral fusions for isthmic spondylolisthesis as well as for those patients having primary surgery for high-grade isthmic spondylolisthesis.**
**REFERENCE: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 311-317.**
**23****. An adult patient with a grade I isthmic spondylolisthesis at L5-S1 is most likely to have weakness of the
1- anterior tibialis.
2- quadriceps.
3- gastrocsoleus.
4- extensor hallucis longus.
5- iliopsoas.
PREFERRED RESPONSE: 4**
**DISCUSSION: Adult patients with isthmic spondylolisthesis most commonly have neurologic symptoms due to foraminal stenosis at the level of the spondylolisthesis. In this scenario, the patient is most likely to have weakness of the L5 myotome, which would cause weakness of the extensor hallucis longus.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 311-317.**
**Lauerman WC, Cain JE: Isthmic spondylolisthesis in the adult. J Am Acad Orthop Surg 1996;4:201-208.**
**24****. When performing a long fusion to the sacrum in an osteopenic patient in whom optimal sagittal balance is restored, which of the following is a benefit of extending the distal fixation to the pelvis, rather than the sacrum alone?
1- Decreased risk of sacral fractures
2- Decreased risk of proximal functional kyphosis
3- Easier contouring of the instrumentation
4- Reduced risk of late pubic ramus fractures
5- Improved coronal plane correction
PREFERRED RESPONSE: 1**
**DISCUSSION: In osteopenic individuals, even those with excellent obtained or maintained balance, long instrumented fusions to the sacrum impart a high degree of strain, and the sacrum may fail in a transverse fracture or fracture-dislocation pattern. The risk of proximal functional kyphosis is unrelated to distal fixation as are coronal plane correction and rod contouring. Pubic ramus fractures have been shown to be associated with both fixation to the sacrum alone as well as to the ilium.**
**REFERENCE: Hu SS, Berven SH, Bradford DS: Adult spinal deformity, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 465-477.**
**25****. Which of the following statements describing chordomas is false?
1- Treatment consisting of complete surgical resection with clean margins offers the best survival.
2- They occur in the clivus and sacrum and occur only 15% of the time in the rest of the spine.
3- They are locally aggressive and invasive tumors.
4- They are highly radiosensitive.
5- They have the ability to become malignant.
PREFERRED RESPONSE: 4**
**DISCUSSION: Casali and associates provided a recent review of the treatment options for chordomas. These tumors are not radiosensitive; however, modern intensity modulated radiosurgery techniques may be of value. The combination of surgery and radiotherapy compared to surgery alone results in the same disease-free survival time. Complete surgical resection of the chondroma with clean margins offers the best survival; however, its location may make total removal impossible. Thus subtotal resection followed by radiotherapy results in better survival despite the tumor’s lack of radiosensitivity.**
**REFERENCE: Casali PG, Stacchiotti S, Sangalli C, et al: Chordoma. Curr Opin Oncol 2007;19:367-370.**
**26****. A previously healthy 35-year-old man was involved in a rollover motor vehicle accident 2 days ago. He was placed in a semi-rigid cervical orthosis. He now reports mostly axial neck pain with attempted range of motion. Examination reveals the mechanical neck pain but no obvious neurologic deficits. AP, flexion, and extension radiographs are shown in Figures 10a through 10c, and sagittal and coronal CT scans are shown in Figures 10d and 10e. What is the most appropriate management at this time?
1- Continued immobilization in a semi-rigid cervical orthosis for 6 to 8 weeks
2- Posterior occipital-cervical fusion with iliac crest bone graft
3- Open reduction and internal fixation of the odontoid process with an anterior odontoid screw
4- Resection of the odontoid process through a transoral approach
5- Reduction with Gardner-Wells tong traction and 6 weeks of skeletal traction
PREFERRED RESPONSE: 3**
**DISCUSSION: Odontoid fractures can be classified based on the anatomic position of the fracture within the dens itself. Type I is an oblique fracture through the upper part of the odontoid process. Type II is a fracture that occurs at the base of the odontoid as it attaches to the body of C2; type III occurs when the fracture line extends through the body of the axis. Type 1 fractures typically can be treated nonsurgically with 6 to 8 weeks of immobilization with a semi-rigid cervical orthosis. Nondisplaced, deep type III fractures generally are treated with skeletal halo fixation. Deep, displaced, and angled type III fractures can be treated with closed reduction and skeletal halo fixation. Shallow type III fractures are sometimes amenable to anterior odontoid screw fixation. Type II fractures can be managed nonsurgically or surgically. Treatment options include halo immobilization, internal fixation (odontoid screw fixation), and posterior atlantoaxial arthrodesis. Management with the halo vest usually is considered if the initial dens displacement is less than 6 mm, the reduction is performed within 1 week of the injury and is able to be maintained, and the patient is younger than age 60 years. Halo vest immobilization can lead to a healing rate of more than 90%. Posterior surgical fusion techniques provide high fusion success rates but do so at the expense of cervical rotation. Up to 50% of rotation is lost with these techniques. Anterior odontoid single screw fixation is often tolerated better than skeletal halo fixation and also is noted to preserve the normal rotation at C1/C2. Studies have shown less of a malunion and nonunion rate in the treatment of type II odontoid fractures with anterior odontoid screw fixation. Osteoporosis, short neck and barrel-chested anatomy, and fractures that are more than 4 weeks old preclude anterior odontoid fixation.**
**REFERENCES: Shilpakar S, McLaughlin MR, Haid RW Jr, et al: Management of acute odontoid fractures: Operative techniques and complication avoidance. Neurosurg Focus 2000;8:e3.**
**Subach BR, Morone MA, Haid RW Jr, et al: Management of acute odontoid fractures with single-screw anterior fixation. Neurosurgery 1999;45:812-819.**
**Fountas KN, Kapsalaki EZ, Karampelas I, et al: Results of long-term follow-up in patients undergoing anterior screw fixation for type II and rostral type III odontoid fractures. Spine 2005;30:661-669.**
**27****. Which of the following palpable bony landmarks is correctly matched with its corresponding vertebral level?
1- Angle of the mandible and the C2-C3 interspace
2- Hyoid bone and C6
3- Carotid tubercle and C6
4- Superior portion of the thyroid cartilage and the C3 vertebral body
5- Cricoid cartilage and C7-T** 1
**PREFERRED RESPONSE: 3**
**DISCUSSION: The carotid tubercle is usually located at the level of C6. The angle of the mandible is at C1-C2; the hyoid is at C4; the superior portion of the thyroid cartilage is C4-C5; and the cricoid cartilage is at C6.**
**REFERENCES: Smith GW, Robinson RA: The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 1958;40:607.**
**An HS: Surgical Exposure and Fusion Techniques of the Spine: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and William, 1998, pp 31-62.**
**28****. What root is most commonly involved with a segmental root level palsy after laminoplasty?**
1- C3
2- C4
3- C5
4- C6
5- C7
**PREFERRED RESPONSE: 3**
**DISCUSSION: The postoperative incidence of C5 root palsy after laminoplasty ranges from 5% to 12%. Other roots also may be affected. The palsies tend to be motor dominant, although sensory dysfunction and radicular pain are also possible. The palsy may arise during the immediate postoperative period or up to 20 days later. C5 may be preferentially involved because it is at the apex of the cervical lordosis. Recovery usually occurs over weeks to months.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-249.**
**Uematsu Y, Tokuhashi Y, Matsuzaki H: Radiculopathy after laminoplasty of the cervical spine. Spine 1998;23:2057-2062.**
**29****. Up to what time frame are the risks minimized in anterior revision disk replacement surgery?
1- 3 days
2- 1 week
3- 10 days
4- 2 weeks
5- 6 weeks
PREFERRED RESPONSE: 4**
**DISCUSSION: Revision anterior exposure within 2 weeks of total disk replacement incurs relatively little additional morbidity because adhesion formation is minimal. Surgeons should have a low threshold for revising implants that are clearly dangerously malpositioned or show early migration within this 2-week window. Beyond this time period, a revision strategy must be individualized to the particular clinical situation. A posterior fusion with instrumentation with or without a laminectomy is currently the most effective salvage procedure.**
**REFERENCE: Tortolani JP, McAfee PC, Saiedy S: Failures of lumbar disc replacement. Sem Spine Surg 2006;18:78-86.**
**30****. Which of the following best describes the use of epidural morphine and steroid paste after laminectomy?
1- Associated with an 11% rate of postoperative surgical site complications
2- Associated with a less than 1% rate of surgical site infections
3- Associated with a decreased rate of postoperative urinary retention
4- Considered the standard for outpatient microdiskectomy
5- Should only be used in the absence of radiculopathy
PREFERRED RESPONSE: 1**
**DISCUSSION: Kramer and associates conducted a retrospective review during an “epidemic” period to identify the risk factors associated with a sudden increase in the rate of surgical site infections. They found in a multivariate analysis that the use of morphine nerve paste resulted in a 7.6-fold increase in postoperative surgical wound debridement, and an 11% rate of surgical site complications.**
**REFERENCES: Kramer MH, Mangram AJ, Pearson ML, et al: Surgical-site complications associated with a morphine nerve paste used for postoperative pain control after laminectomy. Infect Control Hosp Epidemiol 1999;20:183-186.**
**Lowell TD, Errico TJ, Eskenazi MS: Use of steroids after discectomy may predispose to infection. Spine 2000;25:516-519.**
**31****. Figures 11a and 11b show the T** 2**-weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a?
1- Ligamentum flavum
2- Lumbar synovial cyst
3- Tarlov cyst
4- Pseudomeningocele
5- Herniated nucleus pulposus
PREFERRED RESPONSE: 2**
**DISCUSSION: The arrow is pointing to a cystic-appearing structure with high signal intensity on T** 2**-weighted image sequencing. It appears to be contiguous with the hypertrophied right facet joint, which appears to also have high signal intensity. The mass significantly narrows the right lateral recess. The high signal intensity suggests that this is a fluid-filled mass. In addition, the facet joints are degenerative and there is a very mild degree of anterolisthesis on the sagittal image. These findings make a lumbar synovial cyst the most likely diagnosis. Most lumbar juxtafacet cysts are observed at the L4-5 level, extradurally and adjacent to the degenerative facet joint. They may contain synovial fluid and/or extruded synovium. Presentation is indistinguishable from that of a herniated disk. The etiology of spinal cysts remains unclear, but there appears to be a strong association between their formation and worsening spinal instability. They occasionally regress spontaneously and may respond to aspiration and injection of corticosteroids, though there is a high recurrence rate with nonsurgical management. Synovial cysts resistant to nonsurgical management should be treated surgically. If the patient’s symptoms can be attributable to radicular findings, a microsurgical decompression that limits further destabilization should suffice. However, if there is significant low back pain attributable to spinal instability, decompression and fusion remains an appropriate option.**
**REFERENCES: Banning CS, Thorell WE, Leibrock LG: Patient outcome after resection of lumbar juxtafacet cysts. Spine 2001;26:969-972.**
**Deinsberger R, Kinn E, Ungersbock K: Microsurgical treatment of juxta facet cysts of the lumbar spine. J Spinal Disord Tech 2006;19:155-160.**
**Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.**
**32****. A 38-year-old man reports a 2-week history of acute lower back pain with radiation into the left lower extremity. There is no history of trauma and no systemic signs are noted. Examination reveals a positive straight leg test at 35 degrees on the left side and a contralateral straight leg raise on the right side. Motor testing demonstrates mild weakness of the gluteus medius and weakness of the extensor hallucis longus of 3+/5. Sensory examination demonstrates decreased sensation along the lateral aspect of the calf and top of the foot. Knee and ankle reflexes are intact and symmetrical. Radiographs demonstrate no obvious abnormality. MRI scans show a posterolateral disk hernation. The diagnosis at this time is consistent with a herniated nucleus pulposus at
1- L1-2.
2- L2-3.
3- L3-4.
4- L4-5.
5- L5-S1.
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient’s history and physical examination findings are consistent with a lumbar disk herniation at the L4-5 level. Weakness of the extensor hallucis longus and gluteus medius are consistent with an L5 lumbar radiculopathy. Nerve root tension signs are also consistent with sciatica from a lumbar disk herniation. The MRI scans confirm a posterolateral disk herniation at L4-5, which typically affects the exiting L5 nerve root.**
**REFERENCES: Hoppenfeld S: Orthopedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 45-74.**
**Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 43-56.**
**33****. A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of
1- anterior diskectomy and fusion at C4-C5.
2- immobilization in a Philadelphia collar and voluntary flexion and extension radiographs when awake.
3- occipital-cervical fusion with instrumentation.
4- halo immobilization for 12 weeks.
5- left C6 superior facetectomy and posterior fusion at C6-C7 with instrumentation.
PREFERRED RESPONSE: 3**
**DISCUSSION: The CT scans reveal an occipital-cervical dissociation with subluxation of the occipitocervical joints bilaterally. Definitive management should consist of an occipital-cervical fusion with instrumentation. Immobilization in a Philadelphia collar is inadequate for this highly unstable injury, and halo immobilization, while affording adequate temporary immobilization, is not appropriate definitive management for this ligamentous injury. The patient does not have an injury at C4-C5 or C6-C7.**
**REFERENCES: Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries.
J Am Acad Orthop Surg 2002;10:271-280.**
**Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.**
**34****. A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient?
1- Bed rest for 6 weeks, followed by mobilization in a thoracolumbosacral orthosis until the fracture has healed
2- Anterior corpectomy with strut grafting and placement of an anterior plate spanning L1 to L3
3- Anterior corpectomy with strut grafting, followed by posterior spinal fusion and instrumentation
4- Posterior spinal fusion and instrumentation from T11 to L4
5- L2 laminectomy and posterior spinal fusion and instrumentation from T11 to L4
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has a burst fracture with probable unilateral entrapment of the cauda equina within the elements of the fractured lamina. A dural tear is likely in this scenario as well. It is recommended that this type of burst fracture be treated surgically with laminectomy, freeing of the entrapped nerve roots, and dural repair followed by stabilization of the fracture by either a posterior or combined approach. The degree of kyphosis and the extent of anterior canal compromise does not warrant corpectomy in this patient. Therefore, after completing the laminectomy and dural repair, posterior fusion and instrumentation should be sufficient to stabilize the fracture.**
**REFERENCES: Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.**
**Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.**
**35****. A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T** 2**-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T** 1**-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient’s symptoms?
1- Physical therapy
2- CT-guided needle biopsy and IV antibiotics
3- Revision laminotomy and diskectomy
4- L4-L5 anterior debridement and fusion
5- Open repair of the L4-L5 pseudomeningocele
PREFERRED RESPONSE: 1**
**DISCUSSION: The MRI scans show Modic changes in the L4-L5 vertebral bodies due to spondylosis. There is no increased fluid signal or enhancement in the L4-L5 disk to suggest infection or any other pathologic process. Therefore, the patient’s pain should be treated with a course of physical therapy and rehabilitation. There is no infection; therefore, IV antibiotics and debridement are not indicated. Similarly, a pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 319-329.**
**Shen FH, Samartzis D, Andersson GBJ: Nonsurgical management of acute and chronic low back pain. J Am Acad Orthop Surg 2006;14:477-487.**
**36****. What is the heaviest weight that can be safely applied to the adult cervical spine via Gardner-Wells tong traction?
1- 40 pounds
2- 50 pounds
3- 75 pounds
4- 100 pounds
5- Greater than 100 pounds
PREFERRED RESPONSE: 5**
**DISCUSSION: Cotler and associates reported on the use of awake skeletal traction to reduce facet fracture-dislocations in 24 patients. Seventeen patients required more than 50 pounds of traction (the “traditional” limit) to achieve reduction. More than 100 pounds of traction was safely used in one-third of the patients in this study. A cadaver study has supported the safe use of traction with weights in excess of 100 pounds.**
**REFERENCES: Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.**
**Anderson DG, Vacccaro AR, Gavin K: Cervical orthoses and cranioskeletal traction, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005,
pp 110-121.**
**37****. A 68-year-old man reports a 4-week history of progressive left-sided lower back and hip pain. The pain is in the posterior buttock region with radiation to the groin and to the left anterior knee region. The pain is aggravated with walking and improves with rest. There is no history of previous trauma. Radiographs are seen in Figures 14a and 14b, and MRI scans are seen in Figures 14c through 14e. What is the most appropriate treatment option at this time?
1- Epidural steroid injection at L4-5
2- Outpatient physical therapy for the lower back
3- Non-weight-bearing of the left lower extremity
4- Home exercise program, analgesics, and limited use of muscle relaxants
5- Cortisone injection of the left greater trochanter region
PREFERRED RESPONSE: 3**
**DISCUSSION: Although the imaging reveals generalized lumbar spondylosis and stenosis, in particular at L4-5, the MRI scan of the left hip clearly reveals a stress fracture of the femoral neck. Therefore, the treatment of choice is non-weight-bearing of the left lower extremity. During the evaluation of acute back pain, clinicians must include other possibilities within the differential diagnosis that may mimic mechanical axial back pain; thus, potential complications from a missed diagnosis can be avoided.**
**REFERENCES: Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2007, pp 339-361.**
**Spivak JM, Connolly PJ (ed): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 43-56.**
**38****. A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal. Examination of the lower extremities demonstrates mild early trophic changes, and her pulses distally are palpable but are diminished bilaterally. Radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
1- Decompression and posterior fusion at L4-L5
2- Epidural steroid injection at L4-5
3- Nonsteroidal medications and physical therapy for 6 weeks
4- Measurement of the ankle-brachial index
5- CT myelogram
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has symptoms that are more consistent with vascular claudication than with the pseudoclaudication anticipated from lumbar spinal stenosis. Therefore, the patient is a candidate for further vascular work-up. The radiographs reveal early spinal stenosis and spondylolisthesis at L4-5 but also show significant calcification of the iliac arteries, suggestive of peripheral vascular disease. Vascular claudication is a manifestation of peripheral vascular disease and presents with crampy leg pain that is exacerbated by physical exertion. The pain is easily relieved by standing still or sitting. Unlike pseudoclaudication, a forward-flexed posture and/or sitting does not improve the symptoms. Night pain is common in vascular claudication due to the elevation of the extremities and patients often report pain improvement by hanging their extremities in a dependent position. In evaluation of a patient with suspected vascular claudication, the five “P’s” of vascular insufficiency should be monitored, including pulselessness, paralysis, paresthesia, pallor, and pain. While pain and paresthesias can be common in both vascular claudication and pseudoclaudication, the presence of any of the remaining symptoms is suggestive of vascular disease.**
**REFERENCES: Aufderheide TP: Peripheral arteriovascular disease, in Rosen P, Barkin R (eds): Emergency Medicine: Concepts and Clinical Practice, ed 4. St Louis, MO, Mosby, 1998,
pp 1826-1844.**
**Mirkovic S, Garfin SR: Spinal stenosis: History and physical examination. Instr Course Lect 1994;43:435-440.**
**39****. Figure 16 shows the MRI scan of a 43-year-old man who has had worsening low back pain for the past 4 months. What is the most likely diagnosis?
1- Osteochondroma
2- Posttraumatic kyphosis
3- Staphylococcus aureus osteomyelitis
4- Ankylosing spondylitis
5- Tuberculosis
PREFERRED RESPONSE: 5**
**DISCUSSION: Tuberculosis of the spine is seen in 50% to 60% of skeletal disease and is most commonly found in the lower thoracic or upper lumbar spine. Typically two or more adjacent bodies are involved as seen in this MRI scan. The disk space is narrowed but still relatively preserved as opposed to pyogenic infections (black arrow). Epidural extensions often spread from vertebrae to vertebrae (white arrow); however, the posterior elements are not frequently involved (arrowhead). Tumors rarely spread to adjacent vertebrae. The anterior and posterior spread of the infectious process rules out trauma.**
**REFERENCES: Boachie-Adjei O, Squillante RG: Tuberculosis of the spine. Orthop Clin North Am 1996;27:95-103.**
**Currier BL, Eismont FJ: Infections of the spine, in Rothman RH, Simeone FA (eds): The Spine. Philadelphia, PA, WB Saunders, 1992, p 2614.**
**40****. In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if
1- a dural tear is repaired.
2- more than one level requires decompression.
3- less than one half of each facet is removed bilaterally.
4- the pars interarticularis is fractured.
5- the patient is a smoker.
PREFERRED RESPONSE: 4**
**DISCUSSION: With the notable exception of fusion for degenerative spondylolisthesis and scoliosis, there is a paucity of evidence on the indications for spinal fusion in patients undergoing laminectomy for spinal stenosis. However, it is generally recommended that if the spine is destabilized (for example by removal of one complete facet joint or by an iatrogenic pars fracture), spinal fusion should be considered. Although fusion can be considered for a very long laminectomy, a two-level laminectomy does not represent, by itself, a clear indication for the addition of a spinal fusion. The repair of a dural tear and the use of nicotine by the patient play no role in the determination of whether or not to add fusion to a laminectomy procedure.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 299-409.**
**Fischgrund JS, Mackay M, Herkowitz HN, et al: 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.**
**41****. An 18-year-old collegiate basketball player has had a 3-month history of activity-related back pain. She describes isolated low back pain without radiation that increases with training and playing basketball. Her pain resolves with rest. Physical therapy for 6 weeks has failed to provide relief. An axial CT scan is shown in Figure 17a, and Figures 17b and 17c show sagittal CT reconstructions through the right and left lumbar facets, respectively. Further management should consist of which of the following?
1- CT-guided needle biopsy followed by radiation therapy
2- L5-S1 fusion with instrumentation
3- L5-S1 hemilaminotomy and partial diskectomy
4- Activity restriction and bracing
5- L5-S1 total disk arthroplasty
PREFERRED RESPONSE: 4**
**DISCUSSION: The sagittal and axial CT scans show a bilateral spondylolysis at L5. The defect is in the pars interarticularis on the right side but at the base of the pedicle on the left. Having failed a trial of physical therapy with only a 3-month history of pain, the next most appropriate step in management should consist of activity modification and bracing in an antilordotic lumbosacral orthosis. Surgical intervention is reserved for patients who have failed to respond to a trial of bracing and activity restriction.**
**REFERENCES: Debnath UK, Freeman BJ, Grevitt MP, et al: Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 2007;32:995-1000.**
**Bono CM: Low-back pain in athletes. J Bone Joint Surg Am 2004;86:382-396.**
**42****. Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern?
1- Extending down the spine into the lumbosacral region
2- Down the inner aspect of either upper extremity
3- Cephalad up to the cervicothoracic junction
4- Around or through the chest to the anterior wall
5- Down the contralateral lower extremity
PREFERRED RESPONSE: 4**
**DISCUSSION: Although symptomatic thoracic disk herniations can affect more caudal structures, even to the point of paralysis, the pattern of radiating pain has been described as either following the dermatomal band around the chest or feeling to the patient as if the pain passes straight anteriorly to the chest wall.**
**REFERENCE: Skubic JW, Kostuik JP: Thoracic pain syndromes and thoracic disc herniation, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, pp 1443-1464.**
**43****. A 53-year-old man reports a 5-week history of worsening low back pain accompanied by bilateral knee and ankle pain and swelling. He also reports a lesser degree of neck and left elbow pain. He denies any history of trauma or provocative episodes. His medical history is significant for Reiter’s syndrome more than 25 years ago, with no subsequent exacerbations. Furthermore, he has recently returned from a vacation in Costa Rica and noted the development of infectious gastroenteritis with diarrhea within 1 week of his return. This was treated with a 10-day course of oral antibiotics and has since resolved. He denies any significant bowel or urinary symptoms at this time. His neurologic examination is essentially within normal limits, but is somewhat limited by his low back and leg pain. What further investigation is most appropriate at this time?
1- Radiographs of the lumbar spine and bilateral knees and ankles
2- MRI of the lumbar spine with and without gadolinium contrast
3- Synovial fluid analysis of the involved joints for crystals and bacteria
4- Laboratory tests including a CBC count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP)
5- Laboratory tests including CBC count, rheumatoid factor (RF), antinuclear antibodies (ANA), and human leukocyte antigen-B27 (HLA-B27)
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has pain involving the cervical and lumbar spine as well as pain and swelling in both the knees and ankles. As such, this can be classified as polyarticular arthritis. The presence of multiple joint symptoms in the lower extremities, the absence of a history of trauma, and the multiple joints involved direct attention away from the spine as the etiology of this patient’s pain. Radiographs of the involved joints are not likely to yield much useful information to assist with a diagnosis. Likewise, an MRI scan of the lumbar spine is not likely to provide much information regarding the etiology of the patient’s condition. When a rheumatologic illness is suspected, the selective use of confirmatory laboratory testing can aid in arriving at a correct diagnosis. A presumed case of gout or chondrocalcinosis can be confirmed by the presence of the appropriate crystals in a joint-fluid aspiration. Because of the patient’s recent trip to Costa Rica and the subsequent gastroenteritis, a CBC count, ESR, and CRP should be ordered to rule out infectious and inflammatory versus noninflammatory conditions. Rheumatoid factor (RF) in general should only be ordered for patients with polyarticular joint inflammation for more than 6 weeks. The presence of rheumatoid factor does not indicate rheumatoid arthritis. Antinuclear antibodies (ANA) should be ordered when a connective tissue disease such as systemic lupus erythematosus (SLE) is suspected on the basis of specific history and physical examination findings, such as inflammatory arthritis. Human leukocyte antigen-B27 (HLA-B27) should be ordered only when the patient’s history is compatible with ankylosing spondylitis or Reiter’s syndrome and this patient had a history of Reiter’s syndrome.**
**REFERENCES: Gardner GC, Kadel NJ: Ordering and interpreting rheumatologic laboratory tests. J Am Acad Orthop Surg 2003;11:60-67.**
**Shojania K: Rheumatology: 2. What laboratory tests are needed? CMAJ 2000;162:1157-1163.**
**44****. The 5-year outcome for patients with sciatica secondary to lumbar disk herniation shows which of the following results?
1- Patients have the same likelihood of receiving disability whether treated with or without surgery.
2- Sixty percent of surgically treated patients undergo at least one more operation within 5 years.
3- Only 20% of patients treated with surgery report improved symptoms of back and/or leg pain.
4- A smaller portion of surgical patients, compared to nonsurgically treated patients, report improvement.
5- Fifty percent of patients treated nonsurgically seek surgery within 5 years.
PREFERRED RESPONSE: 1**
**DISCUSSION: Atlas and associates, in the Maine Lumbar Spine Study, reported that overall, patients treated initially with surgery reported better outcomes. By 5 years, 19% of surgical patients had undergone at least one additional lumbar spine operation, and 16% of nonsurgical patients had opted for at least one lumbar spine operation. At the 5-year follow-up, 70% of patients initially treated surgically reported improvement in their predominant symptom (back or leg pain) versus 56% of those initially treated nonsurgically. They also noted that there was no difference in the proportion of patients receiving disability compensation at the 5-year follow-up.**
**REFERENCE: Atlas SJ, Keller RB, Chang Y, et al: Surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: Five-year outcomes from the Maine Lumbar Spine Study. Spine 2001;26:1179-1187.**
**45****. What is one of the principle concerns when a fracture such as the one seen in Figure 18
is encountered?
1- Fractures of the lower extremities
2- Paroxysmal hypertension
3- Infection
4- Epidural hematoma
5- Gastrointestinal bleeding
PREFERRED RESPONSE: 4**
**DISCUSSION: The injury shown is a fracture-dislocation and it is highly unstable. In addition to this concern, spinal epidural hematomas have a much higher incidence in people with ankylosing spondylitis following knee fracture. It is felt to be due to disrupted epidural veins, with hypervascular epidural soft tissue in the setting of a rigid spinal canal. Patients with ankylosing spondylitis may have other significant comorbidities, especially cardiac and pulmonary, and these should be carefully assessed.**
**REFERENCES: Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004,
pp 279-290.**
**Wu CT, Lee ST: Spinal epidural hematoma and ankylosing spondylitis: Case report and review of the literature. J Trauma 1998;44:558-561.**
**46****. Retrograde ejaculation is most commonly associated with what surgical approach?
1- Anterior retroperitoneal approach to L5-S1
2- Anterior transperitoneal approach to L5-S1
3- Anterior retroperitoneal approach to L4-5
4- Minimally invasive lateral trans-psoas approach to L4-5
5- Open lateral approach to L4-5
PREFERRED RESPONSE: 2**
**DISCUSSION: Retrograde ejaculation is the sequela of an injury to the superior hypogastric plexus. This structure needs protection, especially during anterior exposure of the lumbosacral junction. Although the superior hypogastric plexus can be injured with anterior or anterolateral spine surgery at any lumbar level, it is most at risk with anterior transperitoneal approaches to the lumbosacral junction. To avoid this complication, the use of monopolar electrocautery should be avoided during deep dissection in this region. The ideal anterior exposure starts with blunt dissection just to the medial aspect of the left common iliac vein sweeping the prevertebral tissues toward the patient’s right side.**
**REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.**
**Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983,
p 107.**
**An HS, Riley LH III: An Atlas of Surgery of the Spine. New York, NY, Lippincott Raven, 1998, p 263.**
**47****. What nerve is most likely to be injured during the anterior exposure of C2-3?
1- Facial
2- Superior laryngeal
3- Vagus
4- Hypoglossal
5- Phrenic
PREFERRED RESPONSE: 4**
**DISCUSSION: The hypoglossal nerve exits from the ansa cervicalis at approximately the C2-3 level and can be injured during retraction up to the C2 level. The superior laryngeal nerve lies at about C4-5. The facial nerve is much higher. The vagus nerve runs with the internal jugular and carotid much more laterally. The phrenic nerve exits posteriorly.**
**REFERENCES: Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-54.**
**Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.**
**48****. A 24-year-old man sustains the injury shown in Figures 19a through 19e in a paragliding accident. He is neurologically intact. He also sustained fractures of his left femur and right distal radius. Which of the following represents the best option for management of the spinal injury?
1- Bed rest for 6 weeks, followed by mobilization in a thoracolumbosacral orthosis (TLSO) until the fracture has healed
2- Immediate mobilization in a TLSO, continuing until the fracture has healed
3- Anterior corpectomy with strut grafting and placement of anterior fixation
4- Anterior corpectomy and strut grafting followed by posterior spinal fusion and instrumentation
5- Posterior spinal fusion and instrumentation
PREFERRED RESPONSE: 5**
**DISCUSSION: The injury pattern is that of a burst fracture at L1 contiguous with a compression fracture at T12. There is associated kyphosis and slight spondylolisthesis of T12 on L1. Treatment of this type of burst fracture in neurologically intact patients is somewhat controversial, with at least one study demonstrating equal long-term results comparing nonsurgical treatment to surgical treatment. In this study, however, body casts were used initially in the nonsurgical group. Moreover, because this patient has multiple fractures, spinal fracture stabilization should be considered to facilitate early mobilization. Surgical stabilization and fusion via a posterior approach is the best treatment option in this patient. Anterior decompression is not necessary since the patient is neurologically intact.**
**REFERENCES: McLain RF, Benson DR: Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine 1999;24:1646-1654.**
**Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study.
J Bone Joint Surg Am 2003;85:773-781.**
**Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.**
**49****. An 82-year-old man is seen in consultation after being admitted for a fall from ground level. There was no loss of consciousness and the patient recalls striking his head and sustaining a hyperextension-type injury to the cervical spine. Examination reveals an
8-cm head laceration with only mild axial neck tenderness. He has generalized weakness throughout the upper extremities and maintained motor function of the lower extremities. There are no obvious sensory deficits, and the bulbocavernous reflex and deep tendon reflexes are maintained. What is the most appropriate diagnosis at this time?
1- Anterior cord syndrome
2- Central cord syndrome
3- Posterior cord syndrome
4- Brown-Séquard syndrome
5- Spinal shock
PREFERRED RESPONSE: 2**
**DISCUSSION: Incomplete cord syndromes have variable neurologic findings with partial loss of sensory and/or motor function below the level of injury. Incomplete cord syndromes include the anterior cord syndrome, the Brown-Séquard syndrome, central cord syndrome, and posterior cord syndrome. Central cord syndrome is characterized with greater motor weakness in the upper extremities than in the lower extremities. The pattern of motor weakness shows greater distal involvement in the affected extremity than proximal muscle weakness. Anterior cord syndrome involves a variable loss of motor function and pain and/or temperature sensation, with preservation of proprioception. The Brown-Séquard syndrome involves a relatively greater ipsilateral loss of proprioception and motor function, with contralateral loss of pain and temperature sensation. Posterior cord syndrome is a rare injury and is characterized by preservation of motor function, sense of pain, and light touch, with loss of proprioception and temperature sensation below the level of the lesion. Spinal shock is the period of time, usually 24 hours, after a spinal injury that is characterized by absent reflexes, flaccidity, and loss of sensation below the level of the injury.**
**REFERENCES: Penrod LE, Hegde SK, Ditunno JF: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.**
**Harrop JS, Sharan A, Ratliff J: Central cord injury: Pathophysiology, management, and outcomes. Spine J 2006;6:198S-206S.**
**50****. Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to
1- progressive increase in lumbar lordosis.
2- load transfer to the superior adjacent vertebra.
3- normalization of load transfer with working kyphosis.
4- reduced strain at the occipito-cervical junction.
5- reduced strain at the apex of the deformity.
PREFERRED RESPONSE: 2**
**DISCUSSION: Kayanja and associates, in a number of biomechanical studies, showed that in a kyphotic spine the strain is located at the apex of the deformity, the force is transmitted to the superior adjacent vertebrae, and that realignment and cement augmentation effectively normalize the load transfer.**
**REFERENCES: Kayanja MM, Ferrara LA, Lieberman IH: Distribution of anterior cortical shear strain after a thoracic wedge compression fracture. Spine J 2004;4:76-87.**
**Kayanja MM, Togawa D, Lieberman IH: Biomechanical changes after the augmentation of experimental osteoporotic vertebral compression fractures in the cadaveric thoracic spine. Spine J 2005;5:55-63.**
**Kayanja MM, Schlenk R, Togawa D, et al: The biomechanics of 1, 2, and 3 levels of vertebral augmentation with polymethylmethacrylate in multilevel spinal segments. Spine 2006;31:769-774.**
**Kayanja M, Evans K, Milks R, et al: The mechanics of polymethylmethacrylate augmentation. Clin Orthop Relat Res 2006;443:124-130.**
**51****. A 58-year-old woman with rheumatoid arthritis has progressive neck pain, upper extremity and lower extremity weakness, and difficulty with fine motor movements. Examination reveals hyperreflexia with mild to moderate objective weakness but the patient has no difficulty with ambulation for short distances. What is the most important preoperative imaging finding that predicts full neurologic recovery with surgical stabilization?
1- Basilar invagination of less than 1 cm
2- Anterior atlanto-dens interval of 4 mm
3- Posterior atlanto-dens interval of greater than 14 mm
4- Rotatory subluxation of less than 10 degrees
5- Subaxial subluxation of less than 3.5 mm
PREFERRED RESPONSE: 3**
**DISCUSSION: Boden and associates’ article presents compelling evidence that patients with rheumatoid arthritis and neurologic deterioration in C1-2 instability are more likely to achieve some improvement if the posterior atlanto-dens interval is greater than 10 mm on preoperative studies. All the patients in their series who had neurologic deterioration and a preoperative posterior atlanto-dens interval of greater than 14 mm achieved complete motor recovery.**
**REFERENCES: Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.**
**Boden SD, Clark CR: Rheumatoid arthritis of the cervical spine, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.**
**Monsey RD: Rheumatoid arthritis of the cervical spine. J Am Acad Orthop Surg 1997;5:240-248.**
**52****. Figures 20a through 20d show the radiographs and MRI scans of a 59-year-old woman who has had symptoms consistent with progressive neurogenic claudication and back pain for the past 9 months. In the last 6 months, nonsurgical management consisting of nonsteroidal anti-inflammatory drugs, physical therapy, and a series of epidural steroid injections have been used; however the injections, while beneficial, have provided only temporary relief of her symptoms. What is the most appropriate management at this time?
1- Repeat trial of epidural steroid injections
2- Pain management referral for narcotic management of symptoms
3- Lumbar laminectomies at L4-5
4- Lumbar laminectomies and fusion at L4-5
5- Bilateral lumbar laminotomies at L3-4 and L4-5
PREFERRED RESPONSE: 4**
**DISCUSSION: Patients with a degenerative spondylolisthesis and severe stenosis who have failed appropriate nonsurgical management are candidates for surgical intervention. Most studies show good to excellent results in more than 85% of patients after lumbar decompression for stenosis. Atlas and associates found that at 8- to 10-year follow-up, leg pain relief and back-related functional status were greater in those patients opting for surgical treatment of the stenosis. Similarly, the decision to fuse a spondylolisthetic segment has been supported in the literature. Herkowitz and Kurz compared decompressive laminectomy alone and decompressive laminectomy with intertransverse arthrodesis in 50 patients with single-level spinal stenosis and degenerative spondylolisthesis. They demonstrated good to excellent results in 90% of the fused group compared to 44% in the nonfusion group. The decision to include instrumentation during the fusion is more controversial. Whereas the use of instrumentation has shown to improve fusion rates, it has not been conclusively shown to improve the overall clinical outcomes of patients.**
**REFERENCES: Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine lumbar spine study. Spine 2005;30:936-943.**
**Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intratransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.**
**Fischgrund JS, Mackay M, Herkowitz HN, et al: 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.**
**53****. A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?
1- Discontinue use of the soft collar and encourage range of motion
2- Semi-rigid collar immobilization for 6 to 8 weeks
3- Surgical stabilization
4- Halo skeletal fixation
5- Outpatient physical therapy with isometric neck exercises
PREFERRED RESPONSE: 3**
**DISCUSSION: Dickman and associates classified injuries of the transverse atlantal ligament into two categories. Type I injuries are disruptions through the substance of the ligament itself. Type II injuries render the transverse ligament physiologically incompetent through fractures and avulsions involving the tubercle of insertion of the transverse ligament on the C1 lateral mass. Type I injuries are incapable of healing without supplemental internal fixation. Type II injuries can be treated with a rigid cervical orthosis with a success rate of 74%. Surgery may be required for type II injures that fail to heal with 3 to 4 months of nonsurgical management.**
**REFERENCES: Findlay JM: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;39:210.**
**Dickman CA, Mamourian A, Sonntag VK, et al: Magnetic resonance imaging of the transverse atlantal ligament for the evaluation of atlantoaxial instability. J Neurosurgery 1991;75:221-227.**
**54****. Figure 22 reveals what anatomic variant of the lumbar spine?
1- Spina bifida occulta
2- Unilateral sacralization
3- An aplastic or hypoplastic pedicle
4- Lumbarization
5- Facet tropism
PREFERRED RESPONSE: 2**
**DISCUSSION: Unilateral sacralization of the fifth lumbar vertebra was first described by Bertolotti in 1917. Bertolotti’s syndrome is present in 12% to 21% of the population. The altered biomechanics have been postulated to cause low back pain by placing increased stress on the adjacent cephalad disk, thus contributing to accelerated degenerative disk disease at this level. It has also been found that the neoarticulation between the enlarged transverse process and the sacrum and/or ilium may be a source of neural impingement on the exited L5 nerve root and results in radicular pain syndrome. Brault and associates reported on a case treated surgically at the Mayo Clinic, in which the pain generator was found to be the contralateral facet joint.**
**REFERENCES: Brault JS, Smith J, Currier BL: Partial lumbosacral transitional vertebra resection for contralateral facetogenic pain. Spine 2001;26:226-229.**
**Quinlan JF, Duke D, Eustace S: Bertolotti’s syndrome: A cause of back pain in young people.
J Bone Joint Surg Br 2006;88:1183-1186.**
**Whelan MA, Feldman F: The variant lumbar pedicle. Neuroradiology 1982;22:235-242.**
**55****. Posterior lumbar spine arthrodesis may be associated with adjacent segment degeneration cephalad or caudad to the fusion segment. Which of the following is the predicted rate of symptomatic degeneration at an adjacent segment warranting either decompression and/or arthrodesis at mid-range follow-up (5-10 years) after lumbar fusion?
1- 2%
2- 10%
3- 25%
4- 50%
5- 80%
PREFERRED RESPONSE: 3**
**DISCUSSION: The rate of symptomatic degeneration at an adjacent segment warranting either decompression or arthrodesis was predicted to be 16.5% at 5 years and 36.1% at 10 years based on a Kaplan-Meier analysis.**
**REFERENCE: Ghiselli G, Wang J, Bhatia NN, et al: Adjacent segment degeneration in the lumbar spine. J Bone Joint Surg Am 2004;86:1497-1503.**
**56****. A 24-year-old man who was involved in a high speed motor vehicle accident is transferred for definitive care after having been diagnosed with an acute spinal cord injury from a fracture-dislocation at C6-7. He has a complete C6 neurologic level and it is now approximately 10 hours from his injury. What is the most appropriate pharmacologic treatment at this time?
1- No pharmacologic intervention is recommended at this time
2- Administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours
3- Administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 48 hours
4- Administration of naloxone with an initial bolus of 30 mg/kg followed by
5.4 mg/kg for 24 hours
5- Administration of naloxone with an initial bolus of 30 mg/kg followed by
5.4 mg/kg for 48 hours
PREFERRED RESPONSE: 1**
**DISCUSSION: The standard practice in the pharmacologic treatment of a spinal cord injury in the United States has been the administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours, in accordance with the findings of the second and third National Acute Spinal Cord Injury Studies (NASCIS). Although the studies have subsequently drawn criticism for their methodology and outcomes, it has been generally accepted that beneficial neurologic outcomes were anticipated in patients who were able to start the protocol within 8 hours of their initial injury. Further improvement was noted in patients receiving the methylprednisolone within 3 hours of their injury and continuing an infusion for
48 hours. In this patient, who is outside the 8-hour treatment window, no studies have supported starting the methylprednisolone protocol at this time.**
**REFERENCES: Braken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.**
**Kwon BK, Tetzlaff W, Grauer JN, et al: Pathophysiology and pharmacologic treatment of acute spinal cord injury. Spine J 2004;4:451-464.**
**57****. Figures 23a and 23b show the MRI scans of a 50-year-old woman who has increasing gait disturbance. She reports three falls in the past week. Examination reveals hyperreflexia, motor weakness in the biceps and triceps, and a positive Hoffman’s sign. What is the most appropriate treatment plan?
1- Observation
2- Physical therapy
3- Epidural steroid injections
4- Cervical laminectomy
5- Anterior cervical diskectomy and fusion
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has obvious signs of progressive myelopathy. Based on her significant physical examination findings, nonsurgical management will not significantly impact her outcome. Cervical decompression alone is contraindicated in patients with cervical kyphosis such as seen here. Anterior cervical fusion is the best option.**
**REFERENCES: Emery SE, Bohlman HH, Bolesta MJ, et al: Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy: Two to seventeen-year follow-up. J Bone Joint Surg Am 1998;80:941-951.**
**Ferguson RJ, Caplan LR: Cervical spondylotic myelopathy. Neurol Clin 1985;3:373-382.**
**Herkowitz HN: A comparison of anterior cervical fusion, cervical laminectomy, and cervical laminoplasty for the surgical management of multiple level spondylotic radiculopathy. Spine 1988;13:774-780.**
**58****. What structure (arrow) is shown in Figure 24?
1- Ilioinguinal nerve
2- Sympathetic chain
3- Ureter
4- Iliac vein
5- L5 nerve
PREFERRED RESPONSE: 2**
**DISCUSSION: The structure illustrated is the sympathetic chain viewed from an anterolateral view of the lower lumbar spine. It descends along the anterolateral aspect of the spine into the pelvis closely adherent to the vertebral column. The spinal nerves, including L5, can be seen exiting from the foramen. The ureters descend from the kidneys and cross anterior to the iliac vessels to the bladder.**
**REFERENCES: Onibokun A, Khoo LT, Holly L: Anterior retroperitoneal approach to the lumbar spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 101-105.**
**Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.**
**59****. The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following?
1- Extent of bowel and bladder dysfunction
2- Extent of the motor deficit
3- Extent of the perianal saddle anesthesia
4- Timing of surgery
5- Location of the herniation
PREFERRED RESPONSE: 4**
**DISCUSSION: The most predictable positive outcome from spinal surgery due to a cauda equina syndrome is early surgical intervention before any significant neurologic deficit develops. Meta-analysis studies demonstrate that surgical intervention more than 48 hours after the onset of cauda equina syndrome show an increased risk for poor outcomes.**
**REFERENCES: Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.**
**Kohles SS, Kohles JD, Karp AP, et al: Time-dependent surgical outcomes following cauda equina syndrome diagnosis: Comments on meta-analysis. Spine 2004;29:1281-1287.**
**60****. A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and
C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?
1- Admit for observation and reassurance
2- Surgical exploration and removal of the anterior instrumentation
3- Esophageal swallowing study
4- Soft cervical collar and early range-of-motion exercises
5- CT of the cervical spine
PREFERRED RESPONSE: 1**
**DISCUSSION: The radiograph shows significant prevertebral soft-tissue swelling following a two-level anterior cervical diskectomy and fusion. The incidence of dysphagia 2 years after anterior cervical spine surgery is 13.6%. Risk factors for long-term dysphagia after anterior cervical spine surgery include gender, revision surgeries, and multilevel surgeries. The use of instrumentation, higher levels, or corpectomy versus diskectomy did not significantly increase the prevalence of dysphagia. Lee and associates demonstrated that while dysphagia after anterior cervical spine surgery is a common early finding, it generally decreases significantly by
6 months with nonsurgical management. A minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels have been identified as risk factors for the development of postoperative dysphagia.**
**REFERENCES: Lee MJ, Bazaz R, Furey CG, et al: Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J 2007;7:141-147.**
**Bazaz R, Lee MJ, Yoo JU: Incidence of dysphagia after anterior cervical spine surgery:
A prospective study. Spine 2002;27:2453-2458.**
**61****. Steroids are thought to prevent neurologic deterioration after traumatic spinal cord injury by which of the following mechanisms?
1- Maintains calcium influx into damaged cells
2- Destabilizes lysosomal membranes in the zone of injury
3- Reduces TNF-alpha expression
4- Increases NF-kB binding capacity
5- Maintains free radical oxidation
PREFERRED RESPONSE: 3**
**DISCUSSION: The proposed mechanisms by which steroids such as methylprednisolone are thought to prevent neurologic deterioration by limiting secondary insult, include: decreasing the area of ischemia in the cord, reducing TNF-alpha expression and NF-kB binding activity, decreasing free radical oxidation and thus stabilizing cell and lysosomal membranes, and checking the influx of calcium into the injured cells, thus reducing cord edema.**
**REFERENCES: Slucky AV: Pathomechanics of spinal cord injury. Spine: State Art Rev 1999;13:409-417.**
**Torg JS, Thibault L, Sennett B, et al: The Nicolas Andry Award. The pathomechanics and pathophysiology of cervical spinal cord injury. Clin Orthop Relat Res 1995;321:259-269.**
**62****. Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
1- Diminished revascularization of cancellous bone graft
2- Increased activity of osteoblasts
3- Increased activity of osteocytes
4- Antibody-induced necrosis
5- Inhibition of prostaglandins
PREFERRED RESPONSE: 1**
**DISCUSSION: Cigarette smoking has been directly linked to pseudarthrosis in spinal fusions. The direct mechanism of action is diminished revascularization of cancellous bone graft. Additionally, a smaller area of revascularization is seen in these grafts, as well as an increased area of necrosis. Increased activity of osteoblasts would result in more bone production. Increased activity of osteocytes would not affect the fusion because osteocytes are mature bone cells.**
**REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.**
**64****. A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
1- Radiographs, including anterior, lateral, and oblique views
2- MRI of the lumbar spine and follow-up at the clinic in 1 week
3- Caudal epidural steroid injection
4- Reassurance, limited analgesics, and early range of motion as tolerated
5- Immediate MRI of the lumbar spine and possible urgent surgical decompression
PREFERRED RESPONSE: 4**
**DISCUSSION: In general, a previously healthy patient with an acute onset of nontraumatic lower back pain does not need diagnostic imaging before proceeding with therapeutic treatment. In the absence of any “red flags” during the history and physical examination, such as trauma or constitutional symptoms (ie, fevers, chills, weight loss), the appropriate treatment for acute onset lower back pain is purely symptomatic treatment including limited analgesics and early range of motion. Diagnostic imaging is not necessary unless the initial treatment is unsuccessful and symptoms are prolonged. Miller and associates suggested that the use of radiographs can lead to better patient satisfaction but not necessarily better outcomes.**
**REFERENCES: Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.**
**Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins 2007, pp 298-338.**
**65****. Sacral fractures are most likely to be associated with neurologic deficits when they involve what portion of the sacrum?
1- Zone 1 (the ala)
2- Zone 2 (the foramina)
3- Zone 3 (the central canal)
4- Zones 1 and 2
5- The sacral laminae
PREFERRED RESPONSE: 3**
**DISCUSSION: Denis divided the sacrum into three zones: zone 1 represents the lateral ala, zone 2 represents the foramina, and zone 3 represents the central canal. A fracture is classified according to its most medial extension. Those in zone 3 are typically bursting-type fractures or fracture-dislocations and are most prone to neurologic sequelae.**
**REFERENCES: Denis F, Davis S, Comfort T: Sacral fractures: An important problem.
A retrospective analysis of 236 cases. Clin Orthop Relat Res 1988;227:67-81.**
**Wood KB, Denis F: Fractures of the sacrum and coccyx, in Vacarro AR (ed): Fractures of the Cervical, Thoracic and Lumbar Spine. New York, NY, Marcel Dekker, 2003, pp 473-488.**
**66****. Which of the following is associated with the use of bisphosphonates in the setting of metastatic breast cancer to the spine?
1- Reduction in skeletal-related events by 30% to 40%
2- Jaw osteonecrosis in 15% of patients
3- Pain improvement in only 30% of patients
4- Improvement in serum hypocalcemia in 40% of patients
5- Accelerated bone destruction in 10% of patients
PREFERRED RESPONSE: 1**
**DISCUSSION: The indications of bisphosphonate therapy in breast cancer patients range from the correction of hypercalcemia to the prevention of cancer treatment-induced bone loss. Bisphosphonates reduce metastatic bone pain in at least 50% of patients and can reduce the frequency of skeletal-related events by 30% to 40%. Osteonecrosis of the jaw could occur in up to 2.5% of breast cancer patients during long-term bisphosphonate therapy.**
**REFERENCE: Body JJ: Breast cancer: Bisphosphonate therapy for metastatic bone disease. Clin Cancer Res 2006;12:6258s-6263s.**
**67****. A 67-year-old retired steelworker was involved in a motor vehicle accident and sustained a midcervical spinal cord injury. Radiographs and MRI scans reveal severe cervical stenosis and spondylosis without fractures or dislocations. Neurologic examination reveals an ASIA C spinal cord impairment with greater motor involvement of the upper extremities than the lower extremities. What is the probability that the patient eventually will become ambulatory?
1- 2% to 5%
2- 15% to 20%
3- 35% to 45%
4- 60% to 70%
5- Greater than 90%
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient sustained an incomplete spinal cord injury known as central cord syndrome. Central cord syndrome characteristically has disproportionate involvement of the upper extremities with the lower extremities being relatively spared. It is most commonly seen after cervical injuries in elderly patients with spondylosis and spinal stenosis, often without fracture. Penrod and associates noted that 23 of 59 patients with central cord syndrome
(ASIA C and D) ultimately walked. The poorest prognosis, however, was in ASIA C patients older than age 50, in which only 40% walked. **
**REFERENCES: Penrod LE, Hegde SK, Ditunno JF Jr: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.**
**Northrup BE: Acute injuries to the spine and spinal cord: Evaluation and early treatment, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, p 735.**
**68****. A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals
a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning
and has no other obvious traumatic injuries. What is the most appropriate treatment at this time?
1- Further imaging studies, including MRI
2- An awake closed reduction with Gardner-Wells traction with neurologic examination
3- Immobilization in a halo skeletal fixation for definitive treatment
4- Closed reduction under general anesthesia
5- Immediate open reduction and internal fixation in the surgical suite
PREFERRED RESPONSE: 2**
**DISCUSSION: In the patient who is neurologically intact or has an incomplete injury from a cervical facet dislocation, a closed reduction with weighted tong traction is appropriate when the patient is awake, alert, and cooperative. Although there is a risk that a cervical facet dislocation could occur with an underlying cervical disk herniation, Vaccaro and associates have shown that closed reduction can be safely carried out in the awake, responsive patient. Closed reduction can be performed in the emergency department with traction with skull tongs or a halo ring. A slow stepwise application of weight is added until a reduction is achieved. Any worsening of the neurologic status of the patient requires immediate termination of the closed reduction and further diagnostic imaging before proceeding with further treatment.**
**REFERENCES: Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217.**
**Hart RA: Cervical facet dislocation: When is magnetic resonance imaging indicated? Spine 2002;27:116-117.**
**Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.**
**69****. A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
1- MRI of chest
2- Laboratory studies, including a complete blood cell (CBC) count, erythrocyte sedimentation rate (ESR), and urinalysis, PSA, CEA
3- Activity alterations to avoid undue back irritation
4- Comfort measures, including medications
5- Spinal manipulative therapy within the first 6 weeks
PREFERRED RESPONSE: 2**
**DISCUSSION: In the initial assessment of acute low back pain in adults, no diagnostic testing is indicated during the first 4 weeks in the absence of “red flags” for a serious underlying condition. The purpose of the initial assessment of acute low back pain in adults is to rule out serious underlying conditions presenting as low back pain. The Agency for Healthcare Policy and Research, in its 1994 clinical practice guideline, identified four serious conditions that may present with low back pain, including fracture, tumor, infection, and cauda equina syndrome. This patient has five “red flags” for a spinal tumor as a possible etiology of his low back pain, including age of older than 50 years, constitutional symptoms (recent weight loss), pain worse when supine, severe nighttime pain, and a history of cancer. Of these, his history of cancer is most significant, as greater than 90% of spinal tumors are metastatic. In order of frequency, breast, prostate, lung, and kidney make up approximately 80% of all secondary spread to the spine. In the presence of “red flags” for tumor or infection, it is recommended that the clinician obtain a CBC count, ESR, and a urinalysis. If these are within normal limits and suspicions still remain, consider consultation or seek further evidence with a bone scan, radiographs, or additional laboratory studies. Negative radiographs alone are insufficient to rule out disease. If radiographs are positive, the anatomy can be better defined with MRI.**
**REFERENCES: Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.**
**Gertzbein SD: Metastatic spine tumors, in Herkowitz HN, Dvorak J, Bell G, et al (eds): The Lumbar Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 792-802.**
**70****. Which of the following increases radiation exposure to patients and personnel during surgery?
1- Orienting the beam in the opposite direction of the working team and keeping the team outside a 6-foot radius of the fluoroscopy machine
2- Orienting the cathode ray tube beneath the patient with the image intensifier receptor as close to the patient as possible
3- Limiting the beam on time to only what is clinically important
4- The use of continuous fluoroscopy whenever possible to ensure proper placement of implants
5- The use of lead glasses, a thyroid shield, and a lead apron with an equivalent lead thickness of 0.25 mm
PREFERRED RESPONSE: 4**
**DISCUSSION: Continuous fluoroscopy and cine radiography expose the patient and personnel to markedly increased levels of direct and scatter radiation exposure. Continuous fluoroscopy should be limited to only what is absolutely needed for safe completion of the procedure. By orienting the cathode ray tube beneath the patient and placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.**
**REFERENCE: Wagner L, Archer B: Minimizing Risks from Fluoroscopic X-rays: A Credentialing Program for Anesthesiologists, Cardiologists, Surgeons, Radiologists, and Urologists, ed 3. The Woodlands, TX, Partners in Radiation Management, 2000.**
**71****. A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?
1- Continued serial neurologic examinations
2- CT with a myelogram of the lumbar spine
3- Immediate surgical exploration and hematoma drainage
4- Electromyography of bilateral lower extremities
5- IV antibiotics for 24 hours, followed by surgical exploration if symptoms persist
PREFERRED RESPONSE: 3**
**DISCUSSION: The MRI scans reveal a large postoperative hematoma causing significant thecal compression. An epidural hematoma with neurologic deficit is a surgical emergency requiring immediate evacuation of the hematoma. Although the incidence of postoperative epidural hematomas is rare, the consequences of a missed diagnosis can be catastrophic. Early recognition and evacuation are essential in preserving or restoring neurologic function. Uribe and associates attributed delayed postoperative hematomas to previous multiple lumbar surgeries as a possible contributing factor.**
**REFERENCES: Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.**
**Uribe J, Moza K, Jimenez O, et al: Delayed postoperative spinal epidural hematomas. Spine J 2003;3:125-129.**
**72****. Figures 27a through 27c show the radiographs and CT scan of a 27-year-old man who sustained a low-velocity gunshot wound to the neck. He is quadriplegic (ASIA A), hemodynamically stable, and does not have drainage from his wound. After initial resuscitation and stabilization, the cervical spine and spinal cord injuries are best managed by
1- wound debridement, anterior corpectomy, spinal cord decompression, dural repair, and anterior fusion with strut graft and anterior plating.
2- wound debridement, anterior corpectomy, spinal cord decompression, dural repair, anterior fusion with strut graft and anterior plating followed by posterior laminectomy, and spinal cord decompression and dural repair with excision of the bullet fragment.
3- wound debridement, anterior corpectomy, spinal cord decompression, dural repair, anterior fusion with strut graft and anterior plating followed by laminectomy and posterior fusion, and spinal cord decompression and dural repair with excision of the bullet fragment.
4- laminectomy and posterior fusion, and spinal cord decompression and dural repair with excision of the bullet fragment.
5- surgical treatment based on extraspinal pathology with orthotic treatment of the spinal fractures.
PREFERRED RESPONSE: 5**
**DISCUSSION: Although the spinal canal has been penetrated, the lateral masses are intact bilaterally with only partial destruction of the vertebral body and penetration of the lamina on one side, thus the cervical spine is not unstable and surgical stabilization is not indicated. Dural repair is not indicated since there is no external cerebrospinal fluid leakage. Surgical treatment should be based on the need to treat extraspinal pathology only.**
**REFERENCES: Bono CM, Heary RF: Gunshot wounds to the spine. Spine J 2004;4:230-240.**
**Punjabi MM, Jue JJ, Dvorak J, et al: Cervical spine kinematics and clinical instability, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005,
pp 55-87.**
**73****. Which of the following is a true statement regarding thoracic disk herniations?
1- Are most commonly discovered during the fifth to seventh decades of life
2- Occur with similar frequency as cervical disk herniations
3- Occur most commonly in the midthoracic or apical region of the spine
4- Can be found in 40% of asymptomatic individuals
5- Are best treated surgically with posterior laminectomy and excision
PREFERRED RESPONSE: 4**
**DISCUSSION: Symptomatic herniations of the thoracic spine are much less common than those of the cervical or lumbar region. They tend to occur most commonly during the third to fifth decades of life and although they can be found at all levels, they are most common in the lower third near the thoracolumbar region. Posterior laminectomy and disk excision has the highest rate of neurologic deterioration and is not recommended. Multiple studies have shown that herniated thoracic disks can be found at one or more levels in 40% of asymptomatic individuals.**
**REFERENCES: Shah RP, Grauer JN: Thoracoscopic excision of thoracic herniated disc, in Vaccaro AR, Bono CM (eds): Minimally Invasive Spine Surgery. New York, NY, Informa Healthcare, 2007, pp 73-80.**
**Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:1038-1047.**
**74****. A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
1- Surgery on the wrong patient
2- Surgery on the wrong side
3- Incorrect procedure performed
4- Intraoperative death
5- Surgery on the wrong level
PREFERRED RESPONSE: 5**
**DISCUSSION: Patient safety and prevention of medical errors is a major focus of recent national advocacy groups. Analysis has shown that the most common sentinel event in spine surgery is surgery on the wrong level. Therefore, it is recommended that every patient have the surgical site signed, the level of surgery marked intraoperatively, and a radiograph taken. Surgery on the wrong level is most likely to occur in single-level decompressive procedures.**
**REFERENCES: Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.**
**Wong DA: Spinal surgery and patient safety: A systems approach. J Am Acad Orthop Surg 2006;14:226-232.**
**75****. What structure is most at risk with anterior penetration of C1 lateral mass screws?
1- Vertebral artery
2- External carotid artery
3- Internal carotid artery
4- Pharynx
5- Glossopharyngeal nerve
PREFERRED RESPONSE: 3**
**DISCUSSION: Posterior screw fixation of the upper cervical spine has gained a great deal of popularity due to its stable fixation, obviating the use of halo vest immobilization, and its high fusion rates. The use of screws in this location, however, has introduced a whole new set of potential complications. Vertebral artery injury is one of the most feared complications associated with screws in the C1/C2 region. This structure, however, is lateral and posterior at the C2 level and then penetrates the foramen transversarium of C1 to lie cephalad to the arch of C1 before entering the foramen magnum. It is the internal carotid artery that lies immediately anterior to the arch of C1 that is particularly at risk by anterior penetration of C1 lateral mass or C1-C2 transarticular screws as demonstrated by Currier and associates. The internal carotid artery lies posterior to the pharynx. The external carotid artery and the glossopharyngeal nerve are not at risk with this method of fixation.**
**REFERENCES: Currier BL, Todd LT, Maus TP, et al: Anatomic relationship of the internal carotid artery to the C1 vertebra: A case report of cervical reconstruction for chordoma and pilot study to assess the risk of screw fixation of the atlas. Spine 2003;28:E461-E467.**
**Grant JC: Grant’s Atlas of Anatomy, ed 6. Baltimore, MD, Williams & Wilkins, 1972.**
**Harms J, Melcher RP: Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine 2001;26:2467-2471.**
**76****. During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital
rim and
1- lateral placement, directly within the temporalis muscle.
2- lateral to the medial third of the orbit.
3- lateral to the lateral aspect of the orbit.
4- above the medial third of the orbit.
5- lateral between the temporalis muscle and zygomatic temporal nerve.
PREFERRED RESPONSE: 2**
**DISCUSSION: Halo fixation is the most rigid form of cervical orthosis, but complications can arise from improper placement of the initial halo ring. A relatively safe zone for anterior pin placement is located 1 cm above the orbital rim and superior to the lateral two thirds of the orbit. This position avoids the supraorbital and supratrochlear nerves and arteries over the medial one third of the orbit. The more lateral positions in the temporal fossa have very thin bone and can interfere with the muscles of mastication. Posterior pin site locations are less critical; positioning on the posterolateral aspect of the skull, diagonal to the contralateral anterior pins, is generally desirable.**
**REFERENCES: Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.**
**Garfin SR, Botte MJ, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1987;69:954.**
**77****. Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?
1- He can expect complete resolution of his symptoms during the first month.
2- All patients experience relief within 3 months and continue to improve over the next 4 years.
3- Most patients experience some pain relief within the first 3 months.
4- He may experience some improvement but if he requires surgery at a later date he will have a poorer result because of the delay.
5- The patient requires immediate surgery to avoid permanent nerve damage.
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has lumbar spinal stenosis and the MRI scans reveal the pathology at L4-5, which is secondary to posterior disk bulging and hypertrophy and infolding of the ligamentum flavum, as well as degenerative facet arthrosis. The degree of spinal stenosis is moderate and his symptoms are positional in nature. Tadokoro and associates reported on a prospective study of 89 patients older than 70 years of age who underwent nonsurgical management for lumbar spinal stenosis. They found the prognosis to be relatively good with patients scoring at “excellent” or “good” for activities of daily living at final follow-up. However, they did note that patients with a complete block on myelography did not respond favorably to nonsurgical management. Amundsen and associates reported on a 10-year prospective study comparing surgical care to nonsurgical management. They concluded that, while the long-term results largely favored surgical treatment, more than half of the nonsurgically managed patients had a satisfactory outcome. They also concluded that a delay of surgery for some months did not worsen the prognosis. Therefore, their recommendation was for an initial primarily nonsurgical approach.**
**REFERENCES: Amundsen T, Weber H, Nordal HJ, et al: Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000;25:1424-1435.**
**Hilibrand AS, Rand N: Degenerative lumbar stenosis: Diagnosis and management. J Am Acad Orthop Surg 1999;7:239-249.**
**Tadokoro K, Miyamoto H, Sumi M, et al: The prognosis of conservative treatments for lumbar spinal stenosis: Analysis of patients over 70 years of age. Spine 2005;30:2458-2463.**
**78****. Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?**
1- T10
2- T11
3- T12
4- L1
5- L2
**PREFERRED RESPONSE: 4**
**DISCUSSION: The smallest pedicle isthmic width is at L1, whereas T12 has the largest pedicle width in the upper lumbar and lower thoracic spine. Although smaller in diameter than T12, both T10 and T11 have larger pedicle widths than L1.**
**REFERENCE: Ofiram E, Polly DW, Gilbert TJ Jr, et al: Is it safe to place pedicle screws in the lower thoracic spine than in the upper lumbar spine? Spine 2007;32:49-54.**
**79****. Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis?
1- Grade I degenerative spondylolisthesis
2- Inability to walk at least 100 feet
3- Cauda equina syndrome
4- Fixed sensory deficit
5- Intermittent foot drop
PREFERRED RESPONSE: 3**
**DISCUSSION: Kondrashov and associates noted stable good outcomes at 4 years in 14 of 18 patients treated with X-STOP interspinous process decompression as defined as an improvement over preoperative Oswestry scores of 15 points or more. Similar results were seen after 1 year in a European study by Siddiqui and associates. Exclusion and inclusion criteria for these studies varied somewhat, but cauda equina syndrome was the only exclusion criteria listed in both studies. All of the other choices did not represent exclusion criteria in either study.**
**REFERENCES: Kondrashov DG, Hannibal M, Hsu KY, et al: Interspinous process decompression with the X-STOP device for lumbar spinal stenosis: A 4-year follow-up study.
J Spinal Disord Tech 2006;19:323-327.**
**Siddiqui M, Smith FW, Wardlaw D: One-year results of X Stop interspinous implant for the treatment of lumbar spinal stenosis. Spine 2007;32:1345-1348.**
**80****. Which of the following statements about hoarseness due to vocal cord paralysis after anterior cervical diskectomy and fusion is most accurate?
1- Vocal cord paralysis is three times as likely with a right-sided approach as compared to a left-sided approach.
2- Vocal cord paralysis is twice as likely with a right-sided approach as compared to a left-sided approach.
3- Vocal cord paralysis is equally likely with either a right-sided or a left-sided approach.
4- Vocal cord paralysis is three times as likely with a left-sided approach as compared to a right-sided approach.
5- Vocal cord paralysis is twice as likely with a left-sided approach as compared to a right-sided approach.
PREFERRED RESPONSE: 3**
**DISCUSSION: It has been traditionally taught that a left-sided approach to the anterior cervical spine is associated with a lower incidence of injury compared to the right-sided approach. This is due in part to the anatomic differences in the path the recurrent laryngeal nerve (RLN) takes on the right as compared to the left. Both nerves ascend in the tracheoesophageal groove after branching off the vagus nerve in the upper thorax. The left-sided RLN loops around the aortic arch and stays relatively medial as compared to the right-sided RLN which loops around the right subclavian artery and is somewhat more lateral at this point, and therefore is theoretically more vulnerable as it ascends toward the larynx before becoming protected in the tracheoesophageal groove. Furthermore, the variant of a nonrecurrent inferior laryngeal nerve branching directly off the vagus nerve at the level of the midcervical spine is much more common on the right than the left. Despite this reasoning, there has been no clinical evidence to suggest that laterality of approach for anterior cervical surgery makes any difference in the incidence of vocal cord paralysis. Furthermore, two recent studies have shown that the incidence of RLN injury and vocal cord paralysis is equal with either side of approach.**
**REFERENCES: Beutler WJ, Sweeney CA, Connolly PJ: Recurrent laryngeal nerve injury with anterior cervical spine surgery risk with laterality of surgical approach. Spine 2001;26:1337-1342.**
**Kilburg C, Sullivan HG, Mathiason MA: Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 2006;4:273-277.**
**81****. A 23-year-old man is involved in a motor vehicle accident. An AP radiograph is shown in Figure 29a, and axial and sagittal CT scans are shown in Figures 29b and 29c. Neurologic examination shows 1/5 strength of his quadriceps and iliopsoas on the right, with 1/5 quadriceps function on the left. Definitive treatment of his injury should
consist of
1- anterior corpectomy with interbody strut.
2- posterior fusion with instrumentation and posterolateral decompression.
3- closed reduction and a thoracolumbosacral orthosis (TLSO).
4- anterior reduction and instrumentation.
5- supine bed rest for 6 weeks, followed by immobilization in a TLSO.
PREFERRED RESPONSE: 2**
**DISCUSSION: The imaging studies show a fracture-dislocation. Surgical treatment of this injury consists of a decompression reduction, stabilization, and fusion. A posterolateral decompression can also be performed as necessary. An isolated anterior procedure in this type of injury is contraindicated. The anterior longitudinal ligament is most likely intact; therefore, an anterior procedure further destabilizes the spine. Reduction by an anterior approach would also be difficult. Nonsurgical management of the neurologic injury in this patient is not indicated.**
**REFERENCES: Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.**
**Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.**
**82****. Surgical treatment for symptomatic disk herniations is associated with which of the following?
1- Substantial rate of nerve root injury
2- Early relief of pain sustained out to 2 years
3- Recurrent herniation rate of 35%
4- Outcomes that are substantially worse than nonsurgical management
5- 10% rate of infectious diskitis
PREFERRED RESPONSE: 2**
**DISCUSSION: The recently published SPORT trial verifies that surgical treatment of symptomatic disk herniations is associated with early and sustained pain relief. The trial also verifies that nonsurgical management is associated with improved symptoms as well. Nerve root injury, recurrent herniation, and diskitis are known complications of surgery, but all are less common than described above.**
**REFERENCE: Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.**
**83****. A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time?
1- Lateral radiographs with passive flexion/extension views
2- Helical CT scan of the cervical-thoracic region
3- Careful manual palpation of the cervical spine for subtle defects or step-offs
4- MRI of the cervical spine
5- Continued use of the cervical collar until the patient becomes responsive for examination
PREFERRED RESPONSE: 2**
**DISCUSSION: Clearance of the cervical spine can be difficult in the obtunded or unresponsive patient. Various trauma series have been reported to detect up to 95% of cervical fractures but only when ideal imaging views have been obtained, which is not often possible in the unresponsive or uncooperative patient. Passively performed cervical flexion-extension under live fluoroscopy has been suggested but is not without inherent risk in the potentially unstable cervical spine. CT of the cervical spine has gained acceptance for the evaluation of these patients given the excellent evaluation of the osseous anatomy and for the common availability in most emergency departments. Sanchez and associates, using a protocol to evaluate for cervical spine injuries after blunt trauma, were able to detect 99% of cervical fractures with 100% specificity.**
**REFERENCES: Chiu WC, Haan JM, Cushing BM, et al: Ligamentous injuries of the cervical spine in unreliable blunt trauma patients: Incidence, evaluation, and outcome. J Trauma 2001;50:457-463.**
**Sanchez B, Waxman K, Jones T, et al: Cervical spine clearance in blunt trauma: Evaluation of a computed tomography-based protocol. J Trauma 2005;59:179-183.**
**Nunez D Jr: Value of complete cervical helical computed tomographic scanning in identifying cervical spine injury in the unevaluable blunt trauma patient with multiple injuries:
A prospective study. J Trauma 2000;48:988-989.**
**84****. A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
1- Revision surgery caudad to C6
2- Persistent left cervical radiculopathy
3- History of a left-sided Horner’s syndrome
4- Transient dysphagia following the initial anterior cervical procedure
5- Nonfunctional left vocal cord
PREFERRED RESPONSE: 5**
**DISCUSSION: When attempting a revision anterior cervical approach from the side opposite the original approach, it is important to evaluate the function of the vocal cords. If this evaluation reveals dysfunction of the vocal cord on the side of the original approach, then an approach on the contralateral side should not be attempted. Injury to the stellate ganglion, which causes a Horner’s syndrome, should not preclude an approach on the contralateral side. While the side of the symptomatology can influence the surgeon’s choice as to the side of an anterior approach, it does not preclude a certain approach. When approaching the lower cervical spine from the right side, the recurrent laryngeal nerve can cross the surgical field and should be preserved. Excessive intraoperative pressure on the esophagus can increase the incidence of dysphagia, but its incidence is no different with either approach.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.**
**Edwards CC II, Riew KD, Anderson PA, et al: Cervical myelopathy: Current diagnostic and treatment strategies. Spine J 2003;3:68-81.**
**85****. A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?
1- Flexion distraction
2- Vertical shear
3- Extension distraction
4- Flexion compression
5- Axial load
PREFERRED RESPONSE: 5**
**DISCUSSION: The CT scans show a burst fracture that results from an axial load injury. The radiographic hallmark of a burst fracture is compression of the posterior cortex of the vertebral body with retropulsion of bone into the spinal canal. AP radiographs often show widening of the interpedicular distance with a fracture of the lamina.**
**REFERENCES: Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.**
**Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.**
**86****. In providing culturally competent care to a Muslim woman with a cervical spine injury, which of the following most accurately describes the steps a male orthopaedist should take to respect her religious beliefs during his examination?
1- No one should be in the exam room except the patient and the physician.
2- Another woman should be in the exam room and only the affected body part should be exposed.
3- A chaperone of either gender should be in the exam room and no skin should be exposed.
4- No particular steps need to be taken in this case.
5- The patient’s closest male relative should be in the exam room but a standard hospital gown may be used.
PREFERRED RESPONSE: 2**
**DISCUSSION: In examining a traditional Muslim woman, a male physician should have another woman present, and the patient’s husband, if possible. Only the affected limb or area needing examination should be exposed.**
**REFERENCE: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.**
**87****. Figure 31 shows the radiograph of a 64-year-old woman who is seen in the emergency department following a motor vehicle accident. She has no voluntary motor function in her distal upper extremities or lower extremities. She does not have a bulbocavernosus reflex. She has a blood pressure of 80/50 mm Hg with a pulse of 50/min. Her hypotension does not improve with initial fluid resuscitation. Further treatment of her hypotension should consist of
1- continued rapid fluid infusion.
2- administration of broad-spectrum antibiotics.
3- administration of 30/mg/kg methylprednisolone over 1 hour.
4- administration of pressors.
5- cardioversion and implantation of a pacemaker.
PREFERRED RESPONSE: 4**
**DISCUSSION: The hallmark of neurogenic shock is hypotension without tachycardia. It is associated most commonly with high cervical spinal cord injuries and results from loss of function of the sympathetic nervous system. Because the peripheral vasculature is dilated due to loss of its sympathetic tone, continued rapid administration of fluid corrects the hypotension and can quickly lead to fluid overload and congestive heart failure. Therefore, neurogenic shock is best treated by the use of pressors. Cardioversion or administration of antibiotics or systemic steroids is not appropriate treatment for this patient’s hypotension.**
**REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.**
**Nockels RP: Nonoperative management of acute spinal cord injury. Spine 2001;26:S31-S37.**
**88****. What is the typical axial plane transverse angulation of the thoracic pedicles?**
**1- 5 degrees medial at T** 1**and T** 2**; 10 degrees from T3 to T10**
**2- 5 degrees lateral at T** 1**; neutral at T** 2**; 5 degrees medial from T3 to T12
3- 10 degrees medial from T1 to T10; 15 degrees medial at T11 and T12
4- 10 degrees medial from T** 1**to T12**
**5- 25 degrees medial at T** 1**; 15 degrees at T** 2**; and 10 degrees medial from T3 to T10**
**PREFERRED RESPONSE: 5**
**DISCUSSION: Thoracic pedicles typically are angled 25 degrees medially at T** 1**so the
starting point is more lateral. T**2**angles about 15 degrees, and then the pedicles average about
5 to 7 degrees down to T10. At T11 and 12, the angulation is minimal.**
**REFERENCES: Weinstein L: Pediatric Spine Principles and Practice. New York, NY, Raven Press, 1994, pp 1659-1681.**
**Lenke LG, Orchowski J: Segmental posterior spinal instrumentation: Thoracic spine to sacrum, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 537-552.**
**89****. What muscle is most often encountered during surgical approaches to C5-6?
1- Omohyoid
2- Cricohyoid
3- Splenius capitus
4- Thyrohyoid
5- Posterior digastric
PREFERRED RESPONSE: 1**
**DISCUSSION: The omohyoid muscle crosses the surgical field from inferior lateral to anterior superior traveling from the scapula to the hyoid bone and may need to be transected. The posterior digastric crosses the field as well but higher near C3-4. The other muscles run longitudinally.**
**REFERENCES: Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-56.**
**Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.**
**90****. Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
1- Nucleus pulposus
2- Cartilaginous end plate
3- Anterior longitudinal ligament
4- Annulus fibrosis
5- Cellular matrix
PREFERRED RESPONSE: 4**
**DISCUSSION: The annulus fibrosis has a multilayer lamellar architecture mode of type I collagen fibers. Each successive layer is oriented at 30 degrees to the horizontal in the opposite direction, leading to a “criss-cross” type pattern. This composition allows the annulus, which has the highest tensile modulus, to resist torsional, axial, and tensile loads.**
**REFERENCE: Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.**
**91****. When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in
1- fracture kyphosis.
2- reduction of retropulsed bone.
3- pain reduction.
4- incidence of complications.
5- return to work.
PREFERRED RESPONSE: 4**
**DISCUSSION: When patients are compared at 5 years follow-up, there are no statistically significant differences between the two groups with respect to kyphosis, the degree of retropulsed bone resorption, pain and function levels, or the ability to return to work. Nonsurgical management of stable neurologically intact burst fractures has a very low incidence of complications.**
**REFERENCES: Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.**
**Shen WJ, Liu TJ, Shen YS: Nonoperative treatment versus posterior fixation for thoracolumbar junction burst fractures without neurologic deficit. Spine 2001;26:1038-1045.**
**92****. A 42-year-old woman who has had an 18-month history of severe low back pain is referred to your office for surgical evaluation. She reports that the pain initially began with right lower extremity pain and management consisted of oral analgesics, nonsteroidal anti-inflammatory drugs, and muscle relaxants. She has seen a chiropractor as well as a pain management specialist and she is status-post epidural steroid injections. She has also completed exhaustive physical therapy, as she is a certified athletic trainer and runs a health fitness program at a community hospital. Currently, she denies lower extremity pain and her pain is isolated to her low back and is subjectively graded as 8/10, with 10 being the worst pain she has ever experienced. The pain is interfering with her activities of daily living and she is seeking definitive treatment. Figures 32a through 32c show current MRI scans. Based on the current available medical literature, what is the most appropriate treatment?
1- Continued nonsurgical management to include long-acting narcotic analgesics
2- Referral for vertebral axial decompression
3- Referral to interventional pain management for a spinal cord stimulator
4- Intradiskal electrothermal therapy (IDET) at L5-S1
5- Lumbar spinal fusion at L5-S1
PREFERRED RESPONSE: 5**
**DISCUSSION: The MRI scans reveal advanced degenerative disk disease at L5-S1. Nonsurgical management has failed to provide relief and the patient is quite debilitated as a result of her back pain. Fritzell and associates demonstrated that in a well-informed and selected group of patients with severe low back pain, lumbar fusion can diminish pain and decrease disability more efficiently than commonly used nonsurgical treatments. In a recent updated Cochrane Review of surgery for degenerative lumbar spondylosis, it was noted that while Fritzell and associates appeared to provide strong evidence in favor of fusion, a more recent trial by Brox and associates demonstrated no difference between those patients undergoing lumbar fusion compared to those receiving cognitive intervention and exercise. The Cochrane Review suggests that this may reflect a difference between the control groups. Fritzell and associates compared lumbar fusion to standard 1990s “usual care,” whereas Brox and associates compared lumbar fusion to a “modern rehabilitation program.” Bear in mind that this patient is a certified athletic trainer and runs a hospital health fitness department; therefore, at least for purposes of this question, it can be assumed that she has participated in a “modern rehabilitation program.” The Cochrane Review goes on to state that preliminary results of three small trials of intradiskal electrotherapy suggest that it is ineffective and that preliminary data from three trials of disk arthroplasty do not permit firm conclusions.**
**REFERENCES: Gibson JN, Waddell G: Surgery for degenerative lumbar spondylosis: Updated Cochrane Review. Spine 2005;30:2312-2320.**
**Fritzell P, Hagg O, Wessberg P, et al: 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 2001;26:2521-2532.**
**Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.**
**93****. Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?
1- L4 nerve root radiculopathy
2- L5 nerve root radiculopathy
3- Associated bowel and bladder dysfunction
4- Symptoms associated with arachnoiditis
5- Wide-based gait, left-sided Hoffman’s sign
PREFERRED RESPONSE: 1**
**DISCUSSION: The MRI scan reveals a L4-L5 foraminal disk herniation originating from the L4-5 disk space that has migrated up into the foramen, compressing the left L4 nerve root. There is normal distribution of the roots in the cerebrospinal fluid, excluding arachnoiditis as a diagnosis, and disk herniation in this location would not result in cauda equina syndrome or myelopathy.**
**REFERENCE: McCullouch JA, Transfeldt EE: Macnab’s Backache, ed 3. Philadelphia, PA, Williams and Wilkins, 1997, pp 569-608.**
**94****. Intradiskal electrothermal therapy (IDET) uses an intradiskal catheter to deliver controlled thermal energy to the inner periphery of the annulus fibrosis of a chronically painful intervertebral disk. Lumbar diskography is used diagnostically to identify the presumed pain generator to be targeted with IDET. Based on the medical literature, what can be said about the current status of IDET?
1- IDET has been proven to seal annular tears in the annulus fibrosis.
2- IDET restores segmental stability by shrinking collagen fibrils in the disk.
3- IDET has demonstrated no significant benefit over placebo in controlled trials.
4- IDET is an unsafe procedure with significant risk of permanent complications.
5- IDET has demonstrated poor clinical results in all reported series to date.
PREFERRED RESPONSE: 3**
**DISCUSSION: Intradiskal electrothermal therapy (IDET) initial clinical results were reported in 2000. The early case series were quite encouraging with reported therapeutic success rates of 60% to 80%. Early enthusiasm was high as IDET provided a nonsurgical treatment option for an otherwise complex and difficult clinical entity, chronic diskogenic low back pain. The actual mechanism of action was not well understood, and while the theoretic explanation made good sense, it did not hold up under laboratory testing. Soon clinical results from the field did not meet the high expectations set by the developers of the technique. Since those early case studies, a few level I evidence studies have been conducted, one by Freeman and associates and one by Pauza and associates. These randomized, placebo-controlled trials demonstrated no significant benefit of IDET over the placebo.**
**REFERENCES: Freeman BJ, Fraser RD, Cain CM, et al: A randomized, double-blind, controlled trial: Intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine 2005;30:2369-2377.**
**Pauza KJ, Howell S, Dreyfuss P, et al: A randomized, placebo-controlled trial of intradiscal electrothermal therapy for the treatment of discogenic low back pain. Spine J 2004;4:27-35.**
**Wetzel FT, McNally TA: Treatment of chronic discogenic low back pain with intradiskal electrothermal therapy. J Am Acad Orthop Surg 2003;11:6-11.**
**95****. A 56-year-old mechanic has had pain in the hypothenar region of his dominant right hand for the past 6 months. He reports weakness in his grip and pain is worse with activity. Which of the following examination findings is most suggestive of a cervical etiology?
1- Relief of symptoms with shoulder abduction (placing hand over the head)
2- Hypothenar atrophy
3- Reproduction of pain with hyperflexion and contralateral rotation of the head
4- Positive Tinel’s sign at the levator scapulae
5- Subluxable ulnar nerve at the cubital tunnel
PREFERRED RESPONSE: 1**
**DISCUSSION: Hypothenar atrophy is a nonspecific sign that can be seen in ulnar neuropathy, C8 radiculopathy, or even cervical myelopathy; however, the atrophy usually is not unilateral and includes other muscle groups. The Spurling test is an excellent method of eliciting cervical radicular pain but involves hyperextension and ipsilateral rotation of the cervical spine, resulting in nerve root compression by reducing the cross-sectional area of the ipsilateral neuroforamen. Tinel’s sign at the levator scapulae, if present, is indicative of an upper cervical (C3 or C4) radiculopathy. A subluxable ulnar nerve at the cubital tunnel, while often asymptomatic, points toward cubital tunnel syndrome as an etiology for this patient’s pain. The shoulder abduction relief (SAR) sign (relief of upper extremity pain with shoulder abduction) is virtually pathognomic of cervical radiculopathy because this maneuver results in relaxation of a compressed and/or inflamed cervical nerve root. The SAR sign is the converse analog of the straight leg raising sign in the lumbar examination for lumbar radiculopathy, as it relieves tension in the nerve root, thereby relieving symptoms.**
**REFERENCES: Ducker TB, Zeidman SM: Neurologic and functional evaluation, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 143-161.**
**An HS: Clinical presentation of discogenic neck pain, radiculopathy, and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.**
**Hoppenfeld S: Physical examination of the cervical spine and temporomandibular joint, in Physical Examination of the Spine and Extremities. New York, NY, Appleton-Century-Crofts, 1976, pp 105-132.**
**96****. A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?**
1- C3-4
2- C4-5
3- C5-6
4- C6-7
**5- C7-T** 1
**PREFERRED RESPONSE: 4**
**DISCUSSION: The patient’s neurologic examination is consistent with a C7 radiculopathy on the right side. In a patient with this symptom complex in the absence of trauma, a cervical disk herniation is the most common etiology for a C7 radiculopathy. There are eight cervical nerve roots and the C7 nerve exits at the C6-7 disk space and is most frequently impinged by a disk herniation at this level.**
**REFERENCES: Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.**
**Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-43.**
**97****. What is the most common nonanesthetic-related reversible cause of changes in intraoperative neurophysiologic monitoring data?
1- Pedicle screw misplacement
2- Patient positioning
3- Spinal cord ischemia
4- Retractor placement
5- Hypotension
PREFERRED RESPONSE: 2**
**DISCUSSION: Patient positioning that results in local nerve compression, plexus traction, or improper neck alignment is the most common nonanesthetic-related cause of changes in intraoperative neurophysiologic monitoring data during spinal surgery.**
**REFERENCES: Jones SC, Fernau R, Woeltjen BL: Use of somatosensory evoked potentials to detect peripheral ischemia and potential injury resulting from positioning of the surgical patient: Case reports and discussion. Spine J 2004;4:360-362.**
**Schwartz DM, Sestokas AK, Hilibrand AS, et al: Neurophysiological identification of position-induced neurologic injury during anterior cervical spine surgery. J Clin Monit Comput 2006;20:437-444.**
**98****. During a left-sided transforaminal lumbar interbody fusion at the L4-5 level, the surgeon notes a significant amount of bleeding that cannot be controlled while using a pituitary rongeur. What anatomic structure has been injured?
1- Aorta
2- Common iliac artery
3- Common iliac vein
4- External iliac artery
5- External iliac vein
PREFERRED RESPONSE: 2**
**DISCUSSION: The surgeon perforated the anterior longitudinal ligament and injured the common iliac artery. Bingol and associates described injuries to the vascular structures during lumbar disk surgery. The common iliac artery was most commonly affected and constituted 76.9% of injuries.**
**REFERENCE: Bingol H, Cingoz F, Yilmaz AT, et al: Vascular complications related to lumbar disc surgery: J Neurosurg 2004;100:249-253.**
**99****. Six weeks after onset, what is the most clearly accepted indication for surgical management for lumbar disk herniation?
1- Stable sensory loss
2- Stable motor weakness
3- Refractory radicular pain
4- Size of the herniation
5- Lost time at work
PREFERRED RESPONSE: 3**
**DISCUSSION: In the absence of a cauda equina syndrome or progressive weakness, the best indication for surgical management is refractory radicular pain. Surgical decision-making should not be based on the size of the herniation. Large extruded herniations tend to resolve more predictably than smaller herniations. Stable motor weakness and numbness resolve similarly in both surgical and nonsurgical management, although surgery hastens the process. When intractable radicular pain is the strict indication for surgery, surgical intervention provides substantial and more rapid pain relief than nonsurgical care.**
**REFERENCES: Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.**
**Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the Maine lumbar spine study. Spine 2005;30:927-935.**
**100****. A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient’s pulmonary function postoperatively?
1- Unaffected
2- Transiently reduced postoperatively but ultimately improves to greater than preoperative function
3- Transiently reduced immediately postoperatively but then quickly returns to preoperative levels
4- Improves postoperatively due to correction of the scoliosis and is maintained long term
5- Reduced postoperatively and often remains reduced long term
PREFERRED RESPONSE: 5**
**DISCUSSION: A thoracotomy in an adult with idiopathic scoliosis causes a reduction in pulmonary function that often does not return to preoperative levels. What pulmonary function that does recover, recovers over many months. Long-term improvement in pulmonary function, compared to preoperative function, is rarely seen. This should be considered in planning surgical intervention in adults with scoliosis.**
**REFERENCES: Graham EJ, Lenke LG, Lowe TG, et al: Prospective pulmonary function evaluation following open thoracotomy for anterior spinal fusion in adolescent idiopathic scoliosis. Spine 2000;25:2319-2325.**
**Kishan S, Bastrom T, Betz RR, et al: Thoracoscopic scoliosis surgery affects pulmonary function less than thoracotomy at 2 years postsurgery. Spine 2007;32:453-458.**
Question 6High Yield
What is the most common complication following surgical treatment of a displaced talar neck fracture?
Explanation
The most frequent complication is posttraumatic arthritis. With talar neck fractures,osteonecrosis is relatively common, occurring in up to 50% of patients. Fracture nonunion occurs in 10%to 12% of patients. Varus malunion can occur with medial comminution. Wound dehiscence and deep infection are much less frequently encountered.
Question 7High Yield
..A 42-year-old woman has a posterior elbow dislocation. Closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Further treatment should consist of
Explanation
- early mobilization only.
RESPONSES FOR QUESTIONS 12 THROUGH 16
RESPONSES FOR QUESTIONS 12 THROUGH 16
Question 8High Yield
After normal menses has begun and in the absence of pregnancy, secondary amenorrhea is defined as which of the following?
Explanation
DISCUSSION: Secondary amenorrhea is defined as the absence of menstrual bleeding for 6 months or the absence of three to six consecutive menstrual cycles after normal menses has begun. The prevalence of amenorrhea among female athletes is estimated at 10% to 20% in women who exercise vigorously and as high as 40% to 66% in elite runners and professional ballet dancers.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 345-346.
Feingold D, Hame SL: Female athlete triad and stress fractures. Orthop Clin North Am 2006;37:575-583.
DISCUSSION: Secondary amenorrhea is defined as the absence of menstrual bleeding for 6 months or the absence of three to six consecutive menstrual cycles after normal menses has begun. The prevalence of amenorrhea among female athletes is estimated at 10% to 20% in women who exercise vigorously and as high as 40% to 66% in elite runners and professional ballet dancers.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 345-346.
Feingold D, Hame SL: Female athlete triad and stress fractures. Orthop Clin North Am 2006;37:575-583.
Question 9High Yield
Figure 1 is the clinical photograph of a 64-year-old man who crashed while riding his motorcycle. An examination reveals his long-finger metacarpophalangeal (MP) joint is stuck in extension. He cannot passively or actively flex at the MP joint. A hand radiograph is seen in Figure



Explanation
This patient has a dorsally dislocated MP joint. In these cases, the volar plate can be displaced dorsal to the metacarpal head, preventing reduction. Although early publications described a “noose effect” of the lumbrical and flexor tendons, the primary block to reduction is the volar plate. Simple MP dislocations can be reduced closed by flexing the wrist and then gently sliding the base of the proximal phalanx over the end of the metacarpal. Longitudinal traction on the finger will only incarcerate the volar plate further and should be avoided. Patients with complex dislocations that fail closed reduction require open
reduction.
reduction.
Question 10High Yield
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. Further workup confirms an anterosuperior tear of the acetabular labrum and prominence of the acetabulum. What is the most likely location of a chondral injury associated with these findings?
---
---
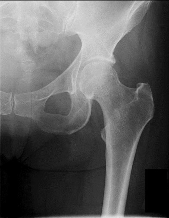
Explanation
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown. The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. Ultrasonography may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasonography is not commonly used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has _important functions for hip stability and maintenance of the suction seal of the joint._
Question 11High Yield
A 65-year-old right–hand-dominant woman has been experiencing thenar and wrist pain for 18 months. She has no history of trauma. The pain worsens during the opening of jars, grasping, writing, and repetitive thumb use. Examination reveals tenderness to palpation over the volar thenar eminence, just distal to the scaphoid tubercle, and along the flexor carpi radialis sheath. A Watson scaphoid shift test produces pain but no instability or clunk. Radiographs reveal isolated scaphotrapeziotrapezoidal (STT) arthritis with mild dorsal intercalated segment instability (DISI) deformity. She has worn a splint on and off for the past year, has had multiple cortisone injections, and has modified her activity, all of which helped initially. She wants to move forward with surgical intervention. STT arthrodesis is chosen over distal pole scaphoid excision. What factor in her evaluation indicates that arthrodesis would be preferred over distal pole excision?
Explanation
Isolated STT arthritis is common and can cause substantial patient disability and pain. After nonsurgical treatment has failed, surgical intervention is warranted. Surgical options include distal pole scaphoid excision, STT arthrodesis, or carpometacarpal (CMC) arthroplasty, if concomitant thumb CMC degenerative changes are present. Distal pole scaphoid excision is less commonly employed for the treatment of STT arthritis, because of the potential development of intercalated segmental instability. However, distal pole scaphoid excision is less technically demanding, engenders fewer surgical complications, and promotes a faster return to previous activity levels. In any patient with preoperative carpal malalignment, removing the distal pole of the scaphoid would exacerbate that deformity and could lead to symptoms from the DISI deformity. Thus, in this patient with mild DISI deformity seen on _preoperative radiographs, STT arthrodesis is the most appropriate treatment option._
Question 12High Yield
A 19-year-old college cross-country runner is amenorrheic and has recurrent stress fractures. Long-term management should consist of
Explanation
The triad of menstrual dysfunction, disordered eating, and stress fracture is well recognized in women who participate in endurance sports. The best treatment remains to be determined, but at present, the combination of oral contraceptives to regulate menses, an increased intake of calcium and vitamin D, as well as nutritional counseling, is the recommended treatment for decreased bone mass related to exercise-induced amenorrhea.
REFERENCES: Nattiv A, Armsey TD Jr: Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
Drinkwater BL: Exercise and bones: Lessons learned from female athletes. Am J Sports Med 1996;24:S33-S35.
REFERENCES: Nattiv A, Armsey TD Jr: Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
Drinkwater BL: Exercise and bones: Lessons learned from female athletes. Am J Sports Med 1996;24:S33-S35.
Question 13High Yield
A 36-year-old woman presents with a grade 3 open midshaft femoral shaft fracture as the result of a high-speed motor vehicle collision. Concomitant injuries include a high-grade splenic laceration requiring splenectomy as well as a subdural hematoma that requires monitoring and maintenance of cerebral perfusion pressure. After irrigation and debridement of the open fracture, which of the following is the most appropriate management of the femoral shaft fracture at this time?
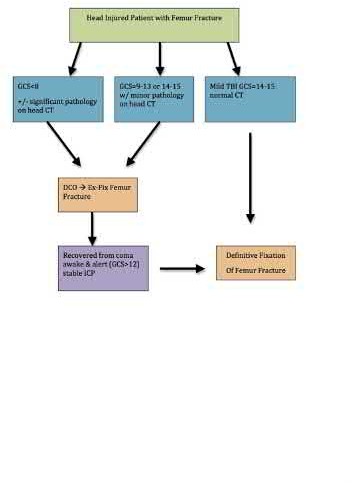
Explanation
The clinical scenario is consistent with a femoral shaft fracture in a patient that is not stable from a neurosurgical perspective. Therefore, the most appropriate treatment at this time is placement of an external fixator.
When evaluating polytrauma patients with long bone fractures, timing of surgery must be approached considering all clinical conditions. One factor most likely to adversely affect long term outcome in polytrauma patients with severe brain injury is intra-operative hypotension; therefore, whenever a patient has a subdural hematoma that requires close observation, definitive surgery of long bone fractures should be delayed.
Flierl et al. review the immunopathophysiology of traumatic brain injury and the role of the orthopaedic surgeon in avoiding a "second hit" injury to the brain by appropriately timing the fixation of femoral shaft fractures. They recommend a multidisciplinary approach, taking individual patient-specific factors into consideration and in general, DCO principles for severe head-injured patients (GCS 3-13) and "early total care" principles for patients with mild head injury (GCS 14-15).
Illustration A is a visual representation of the treatment algorithm recommended in the article.
Incorrect Answers:
Answer choice 1 is incorrect because it does not appropriately address the fracture and there is no indication for bead placement.
Answer choices 2 and 3 are incorrect as this patient is not stable for prolonged surgery.
Answer 4 is incorrect as this patient is already under general anesthesia and external fixation is a better option than traction for stabilization of the fracture.
When evaluating polytrauma patients with long bone fractures, timing of surgery must be approached considering all clinical conditions. One factor most likely to adversely affect long term outcome in polytrauma patients with severe brain injury is intra-operative hypotension; therefore, whenever a patient has a subdural hematoma that requires close observation, definitive surgery of long bone fractures should be delayed.
Flierl et al. review the immunopathophysiology of traumatic brain injury and the role of the orthopaedic surgeon in avoiding a "second hit" injury to the brain by appropriately timing the fixation of femoral shaft fractures. They recommend a multidisciplinary approach, taking individual patient-specific factors into consideration and in general, DCO principles for severe head-injured patients (GCS 3-13) and "early total care" principles for patients with mild head injury (GCS 14-15).
Illustration A is a visual representation of the treatment algorithm recommended in the article.
Incorrect Answers:
Answer choice 1 is incorrect because it does not appropriately address the fracture and there is no indication for bead placement.
Answer choices 2 and 3 are incorrect as this patient is not stable for prolonged surgery.
Answer 4 is incorrect as this patient is already under general anesthesia and external fixation is a better option than traction for stabilization of the fracture.
Question 14High Yield
-Which of the following imaging studies must be obtained for this patient?
Explanation
No detailed explanation provided for this question.
Question 15High Yield
A 7-year-old boy presents with bilateral high arches. His parents report that they are having difficulty finding shoes that comfortably fit him. The patient denies any foot pain. The father had similar problems with his feet and was diagnosed with a âmildâ neurologic condition. On exam, the child has bilateral pes cavus with a supple hindfoot. Treatment of the feet at this time should consist of:
Explanation
The child has a supple deformity secondary to C harcot-Marie-Tooth disease that will progress if untreated. Soft tissue procedures, which may consist of claw toe correction, plantar release, and possibly tendon transfer, are recommended for children younger than 8 years old who have a supple hindfoot.
The calcaneal osteotomy is reserved for patients with a rigid hindfoot.
Triple arthrodesis is a salvage procedure reserved for a fixed, painful foot in older children.
Bracing and observation are not preferred options due to the progressive nature of the disease, and the lack of ability to apply corrective forces to the foot in cavus.
The calcaneal osteotomy is reserved for patients with a rigid hindfoot.
Triple arthrodesis is a salvage procedure reserved for a fixed, painful foot in older children.
Bracing and observation are not preferred options due to the progressive nature of the disease, and the lack of ability to apply corrective forces to the foot in cavus.
Question 16High Yield
The nerve most likely to be at risk during surgical exposure when performing a triple arthrodesis is the:
Explanation
The sural nerve has a variable path in the distal leg, but lies immediately adjacent to the peroneal tendons on the lateral side of the foot. The lateral incision used to expose the subtalar and calcaneocuboid joints is adjacent to this nerve.
Question 17High Yield
A healthy 2-year-old boy falls from a swing and sustains a displaced midshaft femoral fracture with 1 cm of shortening. What is the most appropriate treatment?

Explanation
**28 • American Academy of Orthopaedic Surgeons**
DISCUSSION: For children between the ages of 1 and 6 years, closed reduction and early spica casting is recommended. In some instances, associated injuries or body habitus may preclude cast treatment. Pavlik harness treatment of femoral fractures is for infants younger than 1 year of age. Rarely is there an indication for traction. Internal fixation is reserved in general for children older than age 6 years or with confounding factors.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 271-280.
Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347- 359.
Figure 29a Figure 29b
**28 • American Academy of Orthopaedic Surgeons**
DISCUSSION: For children between the ages of 1 and 6 years, closed reduction and early spica casting is recommended. In some instances, associated injuries or body habitus may preclude cast treatment. Pavlik harness treatment of femoral fractures is for infants younger than 1 year of age. Rarely is there an indication for traction. Internal fixation is reserved in general for children older than age 6 years or with confounding factors.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 271-280.
Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347- 359.
Figure 29a Figure 29b
Question 18High Yield
A 34-year-old female is involved in a high-speed motor vehicle collision and sustains a traumatic proximal forearm amputation. She successfully undergoes debridement and closure, and six weeks later, is fitted with her temporary prosthesis. In order to optimize her
outcomes upon returning to work as a secretary, which of the following is recommended?
outcomes upon returning to work as a secretary, which of the following is recommended?

Explanation
Upper extremity trauma has serious, acute psychological effects that can linger long after the physical injury. These effects may negatively affect patient-reported outcomes, and may also be associated with worsening pain complaints. Coping and stress management techniques can be reviewed with formal psychological counseling, and should be offered to all patients who have underwent an amputation.
Richards et al surveyed 34 patients who had emergency upper extremity surgery and found high levels of psychological distress in patients, including 29% with high levels of both depression and post-traumatic stress disorder (PTSD). They also found that disability was strongly related to pain, depression, and PTSD symptoms.
Mallette et al assessed the attitudes of hand surgery patients and hand surgeons regarding psychologic influences on illness and compared their attitudes with those of the general population. They found that surgeons underestimated the openness of patients to discuss psychological issues and that patients believed in the strong effect of psychologic factors on healing and pain.
Illustration A shows a myoelectric prosthesis in a military veteran. Incorrect Answers:
Answer 1: Formal function capacity testing is not typically necessary unless
Workers' Compensation is involved or formal disability proceedings occur. Answer 2: Final prosthetic fitting is not necessary for full release.
Answer 3: Prosthetic use will vary according to needs and patient factors such as pain.
Answer 4: Return to work does not have to wait for full return of elbow range of motion.
Richards et al surveyed 34 patients who had emergency upper extremity surgery and found high levels of psychological distress in patients, including 29% with high levels of both depression and post-traumatic stress disorder (PTSD). They also found that disability was strongly related to pain, depression, and PTSD symptoms.
Mallette et al assessed the attitudes of hand surgery patients and hand surgeons regarding psychologic influences on illness and compared their attitudes with those of the general population. They found that surgeons underestimated the openness of patients to discuss psychological issues and that patients believed in the strong effect of psychologic factors on healing and pain.
Illustration A shows a myoelectric prosthesis in a military veteran. Incorrect Answers:
Answer 1: Formal function capacity testing is not typically necessary unless
Workers' Compensation is involved or formal disability proceedings occur. Answer 2: Final prosthetic fitting is not necessary for full release.
Answer 3: Prosthetic use will vary according to needs and patient factors such as pain.
Answer 4: Return to work does not have to wait for full return of elbow range of motion.
Question 19High Yield
A 6-year-old girl is wearing a seatbelt but no shoulder harness when the car she is occupying strikes another car. She suffers an abdominal contusion as well as a spine injury. The facets of L1 and L2 are spread apart as is the disk between them. The angle between the two vertebrae is 35°. The neurologic exam is within normal limits. Recommended treatment includes:
Explanation
Open reduction and 2-level fusion is the simplest way of handling this injury.
Immobilization in a hyperextension cast is likely to exacerbate the abdominal injury. An orthosis is not likely to reduce the deformity.
Traction would not be a good mechanism to reduce the deformity. In situ fusion would be insufficient without instrumentation.
Immobilization in a hyperextension cast is likely to exacerbate the abdominal injury. An orthosis is not likely to reduce the deformity.
Traction would not be a good mechanism to reduce the deformity. In situ fusion would be insufficient without instrumentation.
Question 20High Yield
An 83-year-old woman with a long history of her foot slowly and progressively “turning out” now reports significant ankle pain. History reveals that she has significant cardiac disease and exercise-induced angina. Examination reveals a deficiency in the posterior tibial tendon; however, the hindfoot remains moderately supple. Radiographs reveal a valgus tilt of the tibiotalar joint and early arthrosis. What is the most appropriate orthotic management?
Explanation
The patient will continue to have pain secondary to the ankle arthrosis with both the UCBL and the molded articulated ankle-foot orthosis. The total contact orthotic does not provide enough hindfoot control to support the progressive collapse of the ankle into valgus positioning. A molded leather gauntlet will not only control tibiotalar motion but also control hindfoot motion and allow support of the longitudinal arch.
REFERENCE: Augustin JF, Lin SS, Berberian WS, et al: Nonoperative treatment of adult acquired flat foot with the Arizona brace. Foot Ankle Clin 2003;8:491-502.
REFERENCE: Augustin JF, Lin SS, Berberian WS, et al: Nonoperative treatment of adult acquired flat foot with the Arizona brace. Foot Ankle Clin 2003;8:491-502.
Question 21High Yield
A 42-year-old woman reports neck stiffness, upper extremity pain, clumsiness, weakness, and instability of gait. Examination reveals 4+ of 5 strength in the upper extremities and 3+ biceps, brachioradialis, and patellar reflexes with a positive Hoffman sign bilaterally. MRI and CT scans are shown in Figures 10a and 10b. Based on the history and imaging findings, what is the most likely diagnosis?
Explanation
The sagittal T2-weighted MRI scan shows moderate-severe multilevel cervical stenosis.The cord compression is noted to be not only
at the disk levels but also at the midvertebral body levels,and the posterior longitudinal ligament appears to be thickened. The CT scan confirms that the posterior longitudinal ligament is indeed thickened and ossified, compatible with a diagnosis of ossification of the posterior longitudinal ligament. This diagnosis is most common in individuals of
Japanese descent and has a genetic linkage. The anterior osteophytes are smaller than those seen in diffuse idiopathic skeletal hyperostosis and are not syndesmotic. Patients with ankylosing spondylitis typically have non-marginal syndesmophytes. Patients with rheumatoid arthritis may have evidence of instability at C1-C2 on flexionextension radiographs and subaxial subluxations.
at the disk levels but also at the midvertebral body levels,and the posterior longitudinal ligament appears to be thickened. The CT scan confirms that the posterior longitudinal ligament is indeed thickened and ossified, compatible with a diagnosis of ossification of the posterior longitudinal ligament. This diagnosis is most common in individuals of
Japanese descent and has a genetic linkage. The anterior osteophytes are smaller than those seen in diffuse idiopathic skeletal hyperostosis and are not syndesmotic. Patients with ankylosing spondylitis typically have non-marginal syndesmophytes. Patients with rheumatoid arthritis may have evidence of instability at C1-C2 on flexionextension radiographs and subaxial subluxations.
Question 22High Yield
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
The pectoralis major tendon inserts lateral to the biceps tendon, which runs in the bicipital groove. The primary vascular supply of the articular surface of the humeral head is derived from the anterior circumflex humeral artery, which continues into the arcuate artery once it enters the bone. The entry point is on the anterolateral aspect of the humerus just medial to the greater tuberosity within the bicipital groove. To avoid compromising circulation, the blade plate should be placed lateral to the bicipital groove and pectoralis major tendon insertion.
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 23High Yield
Figures 1 and 2 are the radiographs of a 21-year-old man who has a long history of thoracic back pain. His lumbar spine is asymptomatic. He has failed prolonged nonsurgical treatment. Surgical correction should consist of

Explanation
■
When planning surgical intervention for Scheuermann kyphosis, it is imperative that the instrumentation and fusion extend across the entirety of the deformity. Distally, this means extending across the first lordotic disk space. In this scenario, this disk is the L1-L2 disk, which means the fusion needs to extend to L2. Shorter and longer fusions are not necessary or appropriate.
When planning surgical intervention for Scheuermann kyphosis, it is imperative that the instrumentation and fusion extend across the entirety of the deformity. Distally, this means extending across the first lordotic disk space. In this scenario, this disk is the L1-L2 disk, which means the fusion needs to extend to L2. Shorter and longer fusions are not necessary or appropriate.
Question 24High Yield
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. Radiographs of the player’s right ankle confirm there are no fractures. With a lateral talar tilt test result of 19°, which additional structure is most likely damaged?
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. Radiographs of the player’s right ankle confirm there are no fractures. With a lateral talar tilt test result of 19°, which additional structure is most likely damaged?
Explanation
The anterior drawer test is performed with the ankle in 10° of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician uses one hand to stabilize the distal leg and with the other hand applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The
anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization _and a guided rehabilitation program that emphasizes proprioceptive stability._
anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization _and a guided rehabilitation program that emphasizes proprioceptive stability._
Question 25High Yield
1222) Which of the following fluoroscopic views is used to assess
intra-articular screw penetration during volar fixation of a distal radius fracture?
intra-articular screw penetration during volar fixation of a distal radius fracture?


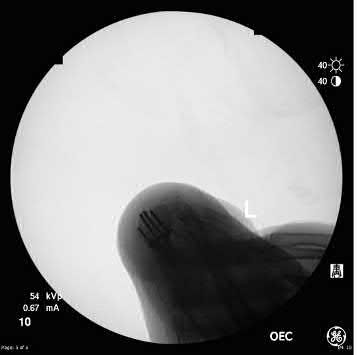
Explanation
Due to radial inclination, a true lateral view of the wrist will not show whether screws from a volar plate are intra-articular; a 23° elevated lateral view is needed to adequately assess this.
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
Answer 1: The dorsal skyline view shows dorsal screw length and is useful to
check for long distal screws.
Answers 2 and 3: The AP and PA wrist views do not show intra-articular screw penetration due to the volar tilt and concavity of the joint.
Answer 5: A 45° oblique lateral view does not visualize the joint as this angle does not match the radial inclination.
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
Answer 1: The dorsal skyline view shows dorsal screw length and is useful to
check for long distal screws.
Answers 2 and 3: The AP and PA wrist views do not show intra-articular screw penetration due to the volar tilt and concavity of the joint.
Answer 5: A 45° oblique lateral view does not visualize the joint as this angle does not match the radial inclination.
Question 26High Yield
A 10-month-old infant has no flexion at the elbows, mild flexion contractures at the wrist, a rigid clubfoot deformity on the left foot, and a rigid rocker bottom deformity on the right foot. Examination of the patient’s hips reveals limited abduction with 80 degrees of hip flexion/extension and full range of motion of the knees. A radiograph of the pelvis is seen in Figure 35. What is the most appropriate treatment for the patient’s hip problem?

Explanation
DISCUSSION: The patient has arthrogryposis. Szoke and associates performed open reduction through a medial approach on 40 hip dislocations in 26 patients with this condition and reported good results in 80% and fair results in 12%. Due to the stiffness associated with this disorder, closed reduction with or without skin or skeletal traction is not feasible. Open reduction through an anterior approach is reserved for older children.
REFERENCES: Szoke G, Staheli LT, Jaffe K., et al: Medial-approach open reduction of hip dislocations in amyoplasia-type arthrogryposis. J Pediat Orthop 1996;16:127-130.
Staheli LT, Chew DE, Elliott JS, et al: Management of hip dislocations in children with arthrogryposis. J Pediatr
Orthop 1987;7:681-685.
**2010 Pediatric Orthopaedic Examination Answer Book • 33**
Figure 36a Figure 36b
REFERENCES: Szoke G, Staheli LT, Jaffe K., et al: Medial-approach open reduction of hip dislocations in amyoplasia-type arthrogryposis. J Pediat Orthop 1996;16:127-130.
Staheli LT, Chew DE, Elliott JS, et al: Management of hip dislocations in children with arthrogryposis. J Pediatr
Orthop 1987;7:681-685.
**2010 Pediatric Orthopaedic Examination Answer Book • 33**
Figure 36a Figure 36b
Question 27High Yield
Figures 1 and 2 show CT images from a 24-year-old man who was the unrestrained driver in a single motor vehicle collision. By report, he was ejected from the vehicle and initially was found unresponsive. The patient was intubated in the field and then brought by ambulance to the emergency department, where he was resuscitated aggressively with crystalloid and blood transfusions. Radiographs were taken and showed an intracranial hemorrhage, which required emergent burr hole evacuation by Neurosurgery. In the intensive care unit, his blood pressure is 80/48, and his pulse is 48. He is breathing spontaneously on the ventilator at 16 breaths per minute. He can follow commands. Physical examination reveals absent motor function in the legs, no sensation below the nipple level, and a positive bulbocavernosus reflex. His skin is warm and dry. What best describes his condition?

Explanation
■
This patient has classic neurogenic shock, which usually occurs when a cervical or high thoracic cord injury disrupts the autonomic pathways and causes a loss of sympathetic tone. Characteristic hypotension and bradycardia are present due to an unopposed vagal tone. Low cardiac output also is present, along with venous and arterial dilatation. The treatment for neurogenic shock is administration of agents called pressors (phenylephrine, dopamine, dobutamine, and norepinephrine) to improve cardiac contractility and increase peripheral vascular resistance. Atropine is given to increase the heart rate. Pressors are titrated to keep the mean arterial pressure above 80 and maintain spinal cord perfusion.
This patient has classic neurogenic shock, which usually occurs when a cervical or high thoracic cord injury disrupts the autonomic pathways and causes a loss of sympathetic tone. Characteristic hypotension and bradycardia are present due to an unopposed vagal tone. Low cardiac output also is present, along with venous and arterial dilatation. The treatment for neurogenic shock is administration of agents called pressors (phenylephrine, dopamine, dobutamine, and norepinephrine) to improve cardiac contractility and increase peripheral vascular resistance. Atropine is given to increase the heart rate. Pressors are titrated to keep the mean arterial pressure above 80 and maintain spinal cord perfusion.
Question 28High Yield
A
B
C
Figures 62a through 62c are the MR images and CT scan of a 65-year-old man with a history of diabetes mellitus, hypertension, and smoking. He has a 6-week history of increasing midback pain, lower extremity pain, and weakness. What is the most likely diagnosis, and how should this diagnosis be confirmed?
B
C
Figures 62a through 62c are the MR images and CT scan of a 65-year-old man with a history of diabetes mellitus, hypertension, and smoking. He has a 6-week history of increasing midback pain, lower extremity pain, and weakness. What is the most likely diagnosis, and how should this diagnosis be confirmed?
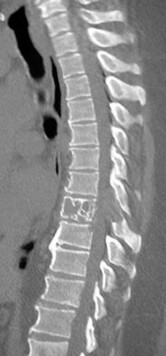

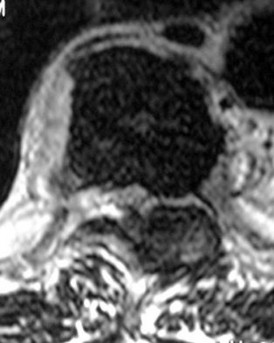
Explanation
The sagittal T2-weighted and axial T2-weighted images show a lesion within the T8 vertebral body that involves the posterior elements. There is an associated epidural component that results in compression of the spinal cord. The sagittal reconstructed CT image shows a lytic lesion within the T8 vertebral body. This pattern of vertebral body involvement with preservation
of the adjacent disks and endplates in a 65-year-old patient is most compatible with a diagnosis of a tumor. The most likely tumor is a metastatic lesion. A CT-guided biopsy will confirm this diagnosis. Although thoracic tuberculosis does not typically cross the disk space, the lack of an anterior soft-tissue component decreases the likelihood of this diagnosis.
RECOMMENDED READINGS
[Khanna AJ, Shindle MK, Wasserman BA, Gokaslan ZL, Gonzales RA, Buchowski JM, Riley LH 3rd. Use of magnetic resonance imaging in differentiating compartmental location of spinal tumors. Am J Orthop (Belle Mead NJ). 2005 Oct;34(10):472-6. Review. PubMed PMID: 16304794. ](http://www.ncbi.nlm.nih.gov/pubmed/16304794)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16304794)
[White AP, Kwon BK, Lindskog DM, Friedlaender GE, Grauer JN. Metastatic disease of the spine. J Am Acad Orthop Surg. 2006 Oct;14(11):587-98. Review. PubMed PMID: 17030592. ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[View](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17030592)
of the adjacent disks and endplates in a 65-year-old patient is most compatible with a diagnosis of a tumor. The most likely tumor is a metastatic lesion. A CT-guided biopsy will confirm this diagnosis. Although thoracic tuberculosis does not typically cross the disk space, the lack of an anterior soft-tissue component decreases the likelihood of this diagnosis.
RECOMMENDED READINGS
[Khanna AJ, Shindle MK, Wasserman BA, Gokaslan ZL, Gonzales RA, Buchowski JM, Riley LH 3rd. Use of magnetic resonance imaging in differentiating compartmental location of spinal tumors. Am J Orthop (Belle Mead NJ). 2005 Oct;34(10):472-6. Review. PubMed PMID: 16304794. ](http://www.ncbi.nlm.nih.gov/pubmed/16304794)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16304794)
[White AP, Kwon BK, Lindskog DM, Friedlaender GE, Grauer JN. Metastatic disease of the spine. J Am Acad Orthop Surg. 2006 Oct;14(11):587-98. Review. PubMed PMID: 17030592. ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[View](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17030592)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17030592)
Question 29High Yield
Figures 16a through 16c are the radiograph, MR image, and biopsy specimen of a 12-year-old boy who injured his leg during a soccer game. Assuming other staging study findings are negative, what is the Musculoskeletal Tumor Society (MSTS) stage of this lesion?

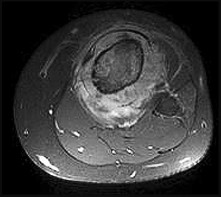
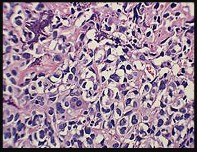
Explanation
The MSTS staging system assigns progressively higher degrees of risk to neoplasms based on their surgical grade, anatomic location, and presence or absence of metastases. Lesions that are low grade are assigned a score of I, while high-grade lesions are assigned a score of II. Lesions contained in the bone or those that are intracompartmental are designated as A, and extracompartmental lesions are designated as B. Metastases elevates the score to III. The radiograph and biopsy specimen reveal a high-grade bone sarcoma with a soft-tissue component with no evidence of metastatic disease. Therefore, this is a stage IIB lesion.
RECOMMENDED READINGS
28. [Wolf RE, Enneking WF. The staging and surgery of musculoskeletal neoplasms. Orthop Clin North Am. 1996 Jul;27(3):473-81. Review. PubMed PMID: 8649730.](http://www.ncbi.nlm.nih.gov/pubmed/8649730)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8649730)
29. [Wafa H, Grimer RJ. Surgical options and outcomes in bone sarcoma. Expert Rev Anticancer Ther. 2006 Feb;6(2):239-48. Review. PubMed PMID: 16445376. ](http://www.ncbi.nlm.nih.gov/pubmed/16445376)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16445376)
RECOMMENDED READINGS
28. [Wolf RE, Enneking WF. The staging and surgery of musculoskeletal neoplasms. Orthop Clin North Am. 1996 Jul;27(3):473-81. Review. PubMed PMID: 8649730.](http://www.ncbi.nlm.nih.gov/pubmed/8649730)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8649730)
29. [Wafa H, Grimer RJ. Surgical options and outcomes in bone sarcoma. Expert Rev Anticancer Ther. 2006 Feb;6(2):239-48. Review. PubMed PMID: 16445376. ](http://www.ncbi.nlm.nih.gov/pubmed/16445376)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16445376)
Question 30High Yield
Figures 1 and 2 are the radiographs after attempted reduction of an injury in a 9-year-old girl. Which anatomic structure is most likely to be interposed?

Explanation
■
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.
■
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.
Question 31High Yield
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality
and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?

Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 32High Yield
Based on this patient's history and examination, what is the best next step?
Explanation
- Obtain blood cultures
Question 33High Yield
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?
Explanation
The stretched peroneus brevis muscle and tendon follow anterior to the fibula and are most likely incarcerated with reduction. The anterior talofibular ligament is too small to prevent reduction of the ankle joint itself. The extensor digitorum brevis originates from the talus; therefore, it is not involved in the tibiotalar joint. The posterior tibial tendon lies medially and would not be interposed into the ankle joint. Similarly, the anterior tibialis tendon also would not be involved.
REFERENCES: Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Rivera F, Bertone C, De Martino M, et al: Pure dislocation of the ankle: Three case reports and literature review. Clin Orthop 2001;382:179-184.
REFERENCES: Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Rivera F, Bertone C, De Martino M, et al: Pure dislocation of the ankle: Three case reports and literature review. Clin Orthop 2001;382:179-184.
Question 34High Yield
Injury to the structure noted with an arrow in the MRI in Figure 1 would lead to what clinical condition?
Explanation
The image depicts the medial ulnar collateral ligament of the elbow. This ligament is the primary restraint to valgus forces at the elbow. It is commonly injured in baseball pitchers. Pain with resisted wrist flexion would suggest medial epicondylitis. Pain with resisted wrist extension would suggest lateral epicondylitis. Lateral elbow pain and varus instability would suggest posterolateral rotatory instability.
Question 35High Yield
A 16-year-old football player reports the acute onset of pain in his left foot. An AP radiograph is shown in Figure
8/. What treatment is most likely to result in successful healing for this injury?
8/. What treatment is most likely to result in successful healing for this injury?
Explanation
Fractures in this region of the fifth metatarsal have been shown to be prone to delayed union and
nonunion and therefore are most reliably managed with internal fixation. Bone grafting is generally not required.
REFERENCES: Herrera-Soto JA, Scherb M, Duffy MF, et al: Fractures of the fifth metatarsal in children and adolescents. J Pediatr Orthop 2007;27:427-431.
Fetzer GB, Wright RW: Metatarsal shaft fractures and fractures of the proximal fifth metatarsal. Clin Sports Med 2006;25:139-150.
nonunion and therefore are most reliably managed with internal fixation. Bone grafting is generally not required.
REFERENCES: Herrera-Soto JA, Scherb M, Duffy MF, et al: Fractures of the fifth metatarsal in children and adolescents. J Pediatr Orthop 2007;27:427-431.
Fetzer GB, Wright RW: Metatarsal shaft fractures and fractures of the proximal fifth metatarsal. Clin Sports Med 2006;25:139-150.
Question 36High Yield
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
Explanation
Bracing for spina bifida paraplegia provides both support and improved function of the movable limb. An orthosis has value in controlling unstable joints. The three-point pressure effect applies a force above and below the joint to prevent it from buckling. A four-point pressure effect is only required for a two-joint system (this patient has problems only at the ankle). A longer lever arm brace and a brace with a greater area of support provide better stability. Finally, a straighter limb, without contracture, applies less pressure to the brace and lessens overload to the skin.
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
Question 37High Yield
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. The injured structure is composed of an
---
---

Explanation
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used.
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
Question 38High Yield
Which of the following activities predisposes a patient to an anterior tibial cortex stress fracture:
Explanation
Repetitive stresses from jumping or leaping is a risk factor for anterior tibial cortex stress fractures. C orrect Answer: Repetitive jumping or leaping
Question 39High Yield
What is the main function of collagen found within articular cartilage?
Explanation
The main function of collagen in articular cartilage is to provide the tissue’s tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint.
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
Question 40High Yield
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?
Explanation
The dual plate fixation construct is significantly stronger than single plate or “Y” plate fixation. Two-plate constructs at right angles, the ulnar plate medially and the lateral plate posteriorly, would appear to be biomechanically optimal. This approach usually is feasible at the time of surgery. Clinically, dual 3.5-mm reconstruction or dynamic compression plates are superior to one third tubular plate fixation. Supplementary external fixation is not considered a better treatment option. Failure of fixation and nonunion are often the result of inadequate fixation and osteoporosis.
REFERENCES: Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Sodergard J, Sandelin J, Bostman O: Mechanical failures of internal fixation in T and Y fractures of the distal humerus. J Trauma 1992;33:687-690.
REFERENCES: Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Sodergard J, Sandelin J, Bostman O: Mechanical failures of internal fixation in T and Y fractures of the distal humerus. J Trauma 1992;33:687-690.
Question 41High Yield
The lateral arm flap is based on what arterial supply?
Explanation
The lateral arm flap is based on the posterior radial collateral artery, a branch of the profunda brachial artery.
REFERENCES: Katsaros J, Tan E, Zoltie N: The use of the lateral arm flap in upper limb surgery. J Hand Surg 1991;16:598-604.
Katsaros J, Schusterman M, Beppu M, et al: The lateral upper arm flap: Anatomy and clinical applications. Ann Plast Surg 1984;12:489-499.
REFERENCES: Katsaros J, Tan E, Zoltie N: The use of the lateral arm flap in upper limb surgery. J Hand Surg 1991;16:598-604.
Katsaros J, Schusterman M, Beppu M, et al: The lateral upper arm flap: Anatomy and clinical applications. Ann Plast Surg 1984;12:489-499.
Question 42High Yield
If the patient had an isolated spine injury without neurologic deficit, the most appropriate next step would be
Explanation
The treatment of thoracolumbar burst fractures has evolved over the years. In the absence of a neurologic deficit or a posterior ligamentous complex injury, nonsurgical treatment is as effective as surgery. The degree of spinal canal compromise is not a risk factor for neurologic symptoms. Similarly, although kyphosis may be a marker of more significant injury, the degree of kyphosis does not correlate with chronic pain. In the setting of a burst fracture, MRI can be used to evaluate the integrity of the posterior ligamentous complex. Polytrauma may be considered a relative indication for surgical intervention in the setting of a stable burst fracture.
RECOMMENDED READINGS
[Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. ](http://www.ncbi.nlm.nih.gov/pubmed/16685232)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16685232)
[Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. ](http://www.ncbi.nlm.nih.gov/pubmed/10065527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10065527)
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.](http://www.ncbi.nlm.nih.gov/pubmed/24332321)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24332321)
RECOMMENDED READINGS
[Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. ](http://www.ncbi.nlm.nih.gov/pubmed/16685232)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16685232)
[Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. ](http://www.ncbi.nlm.nih.gov/pubmed/10065527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10065527)
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.](http://www.ncbi.nlm.nih.gov/pubmed/24332321)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24332321)
Question 43High Yield
Slide 1
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
Explanation
The extensor hallucis longus or the extensor hallucis brevis (rarely the abductor hallucis) may be used as a tendon transfer for correction. Arthrodesis of the hallux interphalangeal joint may be performed for correction of a fixed claw deformity of the interphalangeal joint, usually in conjunction with a tendon transfer. Arthrodesis of the metatarsophalangeal joint is a reasonable alternative provided there is no fixed deformity of the interphalangeal joint present and when arthritis or fixed deformity of the metatarsophalangeal joint is present.
Question 44High Yield
A 16-year-old female gymnast reports a 2-month history of back pain since falling off the parallel bars, and she has been unable to return to gymnastics. She has no numbness or tingling. Examination reveals lower back tenderness, some paravertebral muscle spasm, range of motion of the lumbosacral spine is 20 degrees of flexion and 20 degrees of extension, and an equivocal straight leg raise. Lumbosacral spine radiographs demonstrate Schomorl’s nodes but no evidence of spondylolisthesis. What is the next best step in management?
Explanation
DISCUSSION: Injuries to the anterior and middle column in gymnasts occur but are far less common than posterior column injuries such as spondylolysis and spondylolisthesis. The data on injuries to the anterior and middle columns are more limited. Long-term gymnastics exercise is associated with disk degeneration and other anterior and middle column abnormalities as reported by Katz and Scerpella. They identified a series of anterior and middle column abnormalities, including vertebral compression fractures, Schmorl’s nodes, disk degeneration, and disk herniation in young competitive female gymnasts with back pain. Therefore, the differential diagnosis of back pain in these athletes should include abnormalities of the anterior and middle column. Although diagnostic imaging should begin with radiographs, MRI is the best way to diagnosis these abnormalities. A bone scan is more useful for imaging bony abnormalities of the posterior elements. Flexion-extension radiographs are not indicated in this patient. Treatment such as physical therapy or a lumbosacral corset should not be initiated prior to a complete work-up.
REFERENCES: Katz DA, Scerpella TA: Anterior and middle column thoracolumbar spine injuries in young female gymnasts: Report of seven cases and review of the literature. Am J Sports Med 2003;31:611-616.
Tertti M, Paajanen H, Kujala UM, et al: Disc degeneration in young gymnasts: A magnetic resonance imaging study. Am J Sports Med 1990;18:206-208.
REFERENCES: Katz DA, Scerpella TA: Anterior and middle column thoracolumbar spine injuries in young female gymnasts: Report of seven cases and review of the literature. Am J Sports Med 2003;31:611-616.
Tertti M, Paajanen H, Kujala UM, et al: Disc degeneration in young gymnasts: A magnetic resonance imaging study. Am J Sports Med 1990;18:206-208.
Question 45High Yield
-A 45-year-old man sustained bilateral femur fractures in a motorcycle accident. On admission to the emergency department, the patient is unconscious with a heart rate of 120 bpm and a systolic blood pressure of 80 mm Hg. A chest radiograph reveals bilateral pulmonary contusions. After resuscitation with 2 L of crystalloid, the patient’s heart rate is 115 bpm, the systolic blood pressure is 90 mm Hg, and the patient’s delta base is -10 mmol/L. What is the most appropriate treatment for the femoral fractures at this point?
Explanation
No detailed explanation provided for this question.
Question 46High Yield
A patient presents with hand weakness. On examination, she has no sensory deficient, decreased strength with pronation, and her elbow is at 90º of flexion and pulp-to-pulp contact on key pinch. The most likely diagnosis is:
Explanation
Anterior interosseous nerve syndrome is due to compression of the anterior interosseous nerve (AIN) in the forearm by lacterus fibrosis, flexor digitorum superficialis, or pronator teres. The AIN innervates the pronator quadratus, flexor digitorum profundus (FDP) to the index finger and the flexor pollicis longus (FPL). Anatomy variation exists where the AIN may innervate part of the flexor digitorum superficialis. In this patient, she has decreased pronation at 90º flexion, which relaxes the humeral attachment of the pronator from the pronator quadrus weakness. She also has pulp-to-pulp contract due to weakness of the FPL and FDP to the index finger.
Question 47High Yield
A 72-year-old female presents to the office 5 weeks after distal radius fracture surgery with the findings seen in Figure A. She performed daily cleansing with soap and water and dry dressings.
Which of the following has been shown to decrease the risk of developing this complication?
Which of the following has been shown to decrease the risk of developing this complication?

Explanation
There is no difference between daily showers with soap, water and dry dressings, and solutions comprising (1) saline and chlorhexidine, or (2) saline and hydrogen peroxide.
The risks of external fixation include cellulitis, pin-track drainage, osteomyelitis and pin loosening. The rate of complications is about 20%. Chlorhexidine gluconate has broad spectrum activity against gram-positive and negative bacteria by disrupting cell membranes. It is not affected by blood and has low skin irritancy. Studies show that simple pin-site care (showers, dry dressings) maintains a low infection rate.
Egol et al. performed a randomized trial examining external fixation pin tracts about the wrist. They compared (1) weekly dry dressings, (2) daily pin care with half normal saline (NS) and hydrogen peroxide (H2O2) and (3) chlorhexidine discs with weekly changes. They found pin-site complications in 19%, with no difference between the 3 groups. They do not recommend additional wound care beyond sterile dressings.
Stinner et al. performed a survey on the use of half-pins by the limb lengthening and reconstruction society. They found that most respondents preferred hydroxyapatite coating (81%) because of improved fixation and decreased loosening (less radiographic pin-tract rarefaction and greater extraction torque, which may lead to lower infection rates). Most encouraged
shower (60%) and washing solution (67%)(soap and water, peroxide or saline) for pin site care.
Figure A shows an external fixator around the wrist with cellulitis around the proximal half-pins.
Incorrect Answers
Answers 1-4: Hydrogen peroxide and chlorhexidine based solutions have not been conclusively shown to decrease the rate of pin site complications.
The risks of external fixation include cellulitis, pin-track drainage, osteomyelitis and pin loosening. The rate of complications is about 20%. Chlorhexidine gluconate has broad spectrum activity against gram-positive and negative bacteria by disrupting cell membranes. It is not affected by blood and has low skin irritancy. Studies show that simple pin-site care (showers, dry dressings) maintains a low infection rate.
Egol et al. performed a randomized trial examining external fixation pin tracts about the wrist. They compared (1) weekly dry dressings, (2) daily pin care with half normal saline (NS) and hydrogen peroxide (H2O2) and (3) chlorhexidine discs with weekly changes. They found pin-site complications in 19%, with no difference between the 3 groups. They do not recommend additional wound care beyond sterile dressings.
Stinner et al. performed a survey on the use of half-pins by the limb lengthening and reconstruction society. They found that most respondents preferred hydroxyapatite coating (81%) because of improved fixation and decreased loosening (less radiographic pin-tract rarefaction and greater extraction torque, which may lead to lower infection rates). Most encouraged
shower (60%) and washing solution (67%)(soap and water, peroxide or saline) for pin site care.
Figure A shows an external fixator around the wrist with cellulitis around the proximal half-pins.
Incorrect Answers
Answers 1-4: Hydrogen peroxide and chlorhexidine based solutions have not been conclusively shown to decrease the rate of pin site complications.
Question 48High Yield
Based on imaging alone, what does this bone lesion most closely resemble?
Explanation
- Enchondroma_
Question 49High Yield
Figure 35

Explanation
- Walking boot and weight bearing as tolerated until pain subsides_
Question 50High Yield
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
Explanation
The patient has the classic signs of Little Leaguer’s shoulder, with findings that include pain localized to the proximal humerus during the act of throwing and radiographic evidence of widening of the proximal humeral physis. Examination usually reveals tenderness to palpation over the proximal humerus, but the presence of any swelling, weakness, atrophy, or loss of motion is unlikely. The treatment of choice is rest from throwing for at least 3 months, followed by a gradual return to pitching once the shoulder is asymptomatic.
REFERENCES: Carson WG Jr, Gasser SI: Little Leaguer’s shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
REFERENCES: Carson WG Jr, Gasser SI: Little Leaguer’s shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon