Orthopedic Review | Dr Hutaif General Orthopedics Revie -...
14 Apr 2026
44 min read
111 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Review | Dr Hutaif General Orthope...
00:00
Start Quiz
Question 1High Yield
The most common complication following triple arthrodesis in the adult patient is:
Explanation
Each of the possible answers may occur following triple arthrodesis. In numerous studies, ankle arthritis is the complication most likely to occur regardless of the underlying disease process.
Question 2High Yield
Which of the following factors is most likely to contribute to pseudarthrosis in a patient who has undergone a single-level anterior decompression and fusion procedure for the treatment of cervical radiculopathy?
Explanation
Various factors affect the pseudarthrosis rate in patients who undergo anterior cervical decompression and fusion. Patient factors, including history of smoking and history of diabetes mellitus,have been shown to significantly increase pseudarthrosis rates. The literature has been mixed with regard to fusion rates for allograft versus autograft, especially for one-level fusions; in that category,there is minimal, if any, difference. Similarly, several authors have shown higher rates of fusion with uninstrumented single-level rather than instrumented anterior cervical decompressions and fusions. The level (ie, cranial or caudal) of fusion and sagittal alignment have not been correlated with fusion rates.
Question 3High Yield
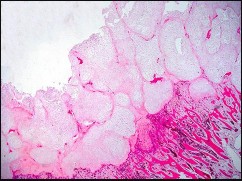
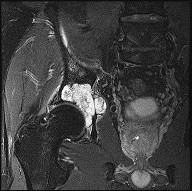
Figures 72a through 72d are the radiograph, MR images, and biopsy specimen of a 42-year-old man with an insidious onset of left hip pain. Further imaging reveals no other lesions. What is the most appropriate initial treatment?


Explanation
This patient has a localized pelvic chondrosarcoma. Treatment is wide surgical resection. There is no defined role for chemotherapy or radiotherapy in the setting of conventional chondrosarcoma. Additionally, while intralesional treatment may be used for select low-grade extremity chondrosarcomas, it is not indicated for axial lesions. Treatment involving less than a wide surgical margin correlates with local recurrence.
RECOMMENDED READINGS
43. [Pring ME, Weber KL, Unni KK, Sim FH. Chondrosarcoma of the pelvis. A review of sixty-four cases. J Bone Joint Surg Am. 2001 Nov;83-A(11):1630-42. Review. PubMed PMID: 11701784. ](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[View](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11701784)
44. [Mavrogenis AF, Angelini A, Drago G, Merlino B, Ruggieri P. Survival analysis of patients with chondrosarcomas of the pelvis. J Surg Oncol. 2013 Jul;108(1):19-27. doi: 10.1002/jso.23351. Epub 2013 May 16. PubMed PMID: 23681650.](http://www.ncbi.nlm.nih.gov/pubmed/23681650)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23681650)
RECOMMENDED READINGS
43. [Pring ME, Weber KL, Unni KK, Sim FH. Chondrosarcoma of the pelvis. A review of sixty-four cases. J Bone Joint Surg Am. 2001 Nov;83-A(11):1630-42. Review. PubMed PMID: 11701784. ](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[View](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11701784)
44. [Mavrogenis AF, Angelini A, Drago G, Merlino B, Ruggieri P. Survival analysis of patients with chondrosarcomas of the pelvis. J Surg Oncol. 2013 Jul;108(1):19-27. doi: 10.1002/jso.23351. Epub 2013 May 16. PubMed PMID: 23681650.](http://www.ncbi.nlm.nih.gov/pubmed/23681650)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23681650)
Question 4High Yield
An L3 radiculopathy is best differentiated from a femoral neuropathy by testing what muscle? ](http://www.orthobullets.com/anatomy/10065/adductor-longus)
Explanation
No detailed explanation provided for this question.
Question 5High Yield
Figures 1 through 3 show sagittal and axial MRIs and a radiograph from a 77-year-old woman with leg pain when standing and walking of 1 year duration. The pain improves when she leans forward. She has been in physical therapy, taken oral analgesics, and had epidural injections with minimal relief. What is the best next step?

Explanation
■
The patient has lumbar stenosis of L2-3 and L3-4. She has no spondylolisthesis or instability. For her condition, spinal fusion plays a minimal role. She has no evidence of instability, and her condition can be addressed through laminectomy only. No role exists for microdiskectomy, because her disease results from a combination of ligamentum flavum hypertrophy and facet hypertrophy.
The patient has lumbar stenosis of L2-3 and L3-4. She has no spondylolisthesis or instability. For her condition, spinal fusion plays a minimal role. She has no evidence of instability, and her condition can be addressed through laminectomy only. No role exists for microdiskectomy, because her disease results from a combination of ligamentum flavum hypertrophy and facet hypertrophy.
Question 6High Yield
Which of the following is true concerning Achilles tendon ruptures:
Explanation
Important points to remember about Achilles tendon ruptures: A. Most common in middle-aged men
B. Often intermittent sports activity
C . Left more than right
D. Often the tendon is abnormal (degenerative) E. Mechanism
1/. Sudden forced plantarflexion
2/. Unexpected dorsiflexion
3/. Violent dorsiflexion of the plantar flexed foot
Factors which may make the patient more prone to rupture: A. Steroids
B. Fluoroquinolones
B. Often intermittent sports activity
C . Left more than right
D. Often the tendon is abnormal (degenerative) E. Mechanism
1/. Sudden forced plantarflexion
2/. Unexpected dorsiflexion
3/. Violent dorsiflexion of the plantar flexed foot
Factors which may make the patient more prone to rupture: A. Steroids
B. Fluoroquinolones
Question 7High Yield
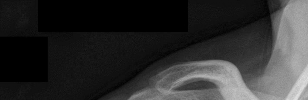
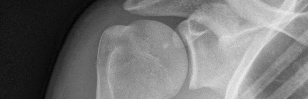
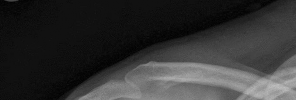
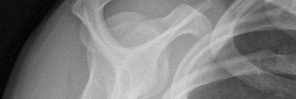
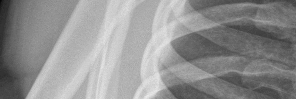
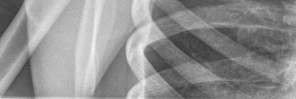
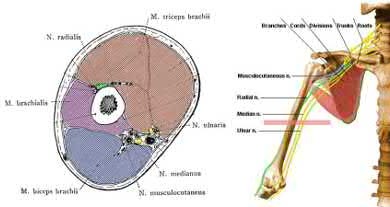
Figures 1 and 2 are the most recent radiographs of an 18-year-old high school student who sustains an anterior shoulder dislocation playing recreational football. He has a low Beighton score on physical examination. He was closed reduced and underwent a course of physical therapy but had a second dislocation playing recreational basketball. What is the most appropriate course of treatment, with the lowest complication rate, to prevent further dislocation?


Explanation
The patient has recurrent instability and is at a high rate of further dislocations due to his young age. Therefore, therapy and bracing are unlikely to decrease his dislocation rate. The radiographs are normal, and there is no Hill-Sachs lesion or bony Bankart lesion. His instability severity index score is 3, and; therefore, a bony procedure such as Latarjet is not necessary. Furthermore, the rate of complication following a Latarjet procedure, especially nerve
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
Question 8High Yield
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
In the study done by Pevny and associates, 35% of patients older than age 40 years sustained rotator cuff tears and 8% had axillary nerve palsies. All of the patients with axillary nerve palsy also had rotator cuff tears. Imaging of the rotator cuff is indicated in this age group. The incidence of recurrent instability in patients older than age 40 years is 10% to 15%.
REFERENCES: Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Hawkins RJ, Mohtadi NG: Controversy in anterior shoulder instability. Clin Orthop 1991;272:152-161.
REFERENCES: Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Hawkins RJ, Mohtadi NG: Controversy in anterior shoulder instability. Clin Orthop 1991;272:152-161.
Question 9High Yield
The fracture shown in Figure 50 is most reliably treated with what form of fixation?
Explanation
The radiograph shows a comminuted proximal ulnar fracture. The most reliable fixation is a posterior plate, acting as a tension band plate. The fracture involves the proximal shaft of the ulna; therefore, a 3.5-mm compression plate or one of similar size should be used to provide adequate stability. Kirschner wires and tension band wires do not provide axial stability of the comminution of the ulna. Compression screws alone will most likely fail and will not provide axial rotational stability to the construct. A medial plate will not resist the distraction forces across this fracture.
REFERENCES: McKee MD, Seiler JG, Jupiter JB: The application of the limited contact dynamic compression plate in the upper extremity: An analysis of 114 consecutive cases. Injury 1995;26:661-666.
McKee MD, Jupiter JB: Trauma to the adult elbow and fractures of the distal humerus, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, p 1469.
REFERENCES: McKee MD, Seiler JG, Jupiter JB: The application of the limited contact dynamic compression plate in the upper extremity: An analysis of 114 consecutive cases. Injury 1995;26:661-666.
McKee MD, Jupiter JB: Trauma to the adult elbow and fractures of the distal humerus, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, p 1469.
Question 10High Yield
The most appropriate pedorthic management of symptomatic interdigital neuroma involves
Explanation
- a metatarsal pad.
Question 11High Yield
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Initial treatment should consist of
Explanation
DISCUSSION:
This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. (Note: It may be necessary to splint the elbow in pronation if the medial collateral ligament [MCL] is intact and the lateral collateral ligament [LCL] is disrupted, or in supination if the LCL is intact but the MCL disrupted.) Surgical reconstruction of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If unstable after reconstruction,
application of a hinged external fixator may be considered.
DISCUSSION:
This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. (Note: It may be necessary to splint the elbow in pronation if the medial collateral ligament [MCL] is intact and the lateral collateral ligament [LCL] is disrupted, or in supination if the LCL is intact but the MCL disrupted.) Surgical reconstruction of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If unstable after reconstruction,
application of a hinged external fixator may be considered.
Question 12High Yield
A
B
Figures 18a and 18b are the lumbar spine radiographs of a 72-year-old man with no significant medical history who has had severe back pain for 3 weeks. He denies radiating symptoms, weakness, or numbness when he is seen in the emergency department. He is sent home with a soft corset. At his followup visit he continues to describe significant back pain with activity that is not relieved with oral narcotic mediations. A follow-up CT scan shows a nondisplaced fracture through all 3 columns of the spine. What is the most appropriate treatment?
B
Figures 18a and 18b are the lumbar spine radiographs of a 72-year-old man with no significant medical history who has had severe back pain for 3 weeks. He denies radiating symptoms, weakness, or numbness when he is seen in the emergency department. He is sent home with a soft corset. At his followup visit he continues to describe significant back pain with activity that is not relieved with oral narcotic mediations. A follow-up CT scan shows a nondisplaced fracture through all 3 columns of the spine. What is the most appropriate treatment?



Explanation
The patient has previously undiagnosed ankylosing spondylitis. Radiographs reveal nonmarginal syndesmophytes throughout the lumbar spine. The CT scan reveals a nondisplaced 3-column fracture. Many patients with missed spinal injuries present in followup with neurologic worsening or progressive deformity. Fractures can often involve all 3 columns, including the posterior elements. In patients with ankylosing spondylitis, this represents an unstable injury and a high likelihood of displacement with nonsurgical treatment. Surgical treatment in the form of a posterior spinal fusion is indicated. Because the fracture is nondisplaced and the patient is neurologically intact, decompression via an anterior approach is not indicated. Bracing either with a TLSO brace or a soft corset will not provide sufficient stability for this fracture pattern. Physical therapy and NSAIDS are not indicated in this scenario.
RECOMMENDED READINGS
Hu SS, Ananthakrishnan D. Ankylosing spondylitis. In: Herkowitz HN, Garfin SR, eds. The Spine. 5th ed. Philadelphia, PA: Elsevier; 2006:763-761.
Blam OG, Cotler JM: Fractures in the stiff and osteoporotic spine. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction,. 3rd ed. Philadelphia, PA: Elsevier; 2003.
RECOMMENDED READINGS
Hu SS, Ananthakrishnan D. Ankylosing spondylitis. In: Herkowitz HN, Garfin SR, eds. The Spine. 5th ed. Philadelphia, PA: Elsevier; 2006:763-761.
Blam OG, Cotler JM: Fractures in the stiff and osteoporotic spine. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction,. 3rd ed. Philadelphia, PA: Elsevier; 2003.
Question 13High Yield
Following surgical stabilization and fixation of the distal fibula, what is the most appropriate next step?
Explanation
- Perform a stress examination of the syndesmosis.
Question 14High Yield
1245) A 25-year-old male is a driver in a motor vehicle accident and sustains the isolated closed injury seen in Figures A and B. He is treated with an intramedullary nail, and postoperative radiographs are shown in Figures C and D. Which of the statements concerning reaming and nails is true?




Explanation
The patient in the scenario has a closed distal one-third tibia fracture. Canal reaming increases the biologic environment for fracture healing but can potentially disrupt cortical blood flow. As such, many recommend canal reaming 1-2mm greater than the canal width followed by insertion of a nail that matches the native canal width. Reamed and unreamed tibias have similar mineral apposition rates.
In 1998, Hupel et al studied the effect of loose and tight unreamed, locked nails on cortical blood flow and strength of union in a canine model. They found that loose nails allowed higher cortical reperfusion at the time of insertion and at eleven weeks.
In a later study by the same group in 2001, they studied the effect of non-reamed, limited reamed and standard reamed nails on porosity, new bone formation and mineral apposition. They found the lowest porosity in the limited reaming group but found new bone formation and mineral apposition rates similar at eleven weeks across the three groups. They concluded that limited reaming is preferred in patients with vascular compromise to the tibia.
Incorrect Answers:
1: Reamed and unreamed tibias have similar mineral apposition rates. 2: Reamed tibias have the highest amount of new bone formation.
3: The lowest porosity of bone is seen with limited reaming.
5: Nails that are tight to the cortex have less reperfusion than appropriately fitting or loose nails.
In 1998, Hupel et al studied the effect of loose and tight unreamed, locked nails on cortical blood flow and strength of union in a canine model. They found that loose nails allowed higher cortical reperfusion at the time of insertion and at eleven weeks.
In a later study by the same group in 2001, they studied the effect of non-reamed, limited reamed and standard reamed nails on porosity, new bone formation and mineral apposition. They found the lowest porosity in the limited reaming group but found new bone formation and mineral apposition rates similar at eleven weeks across the three groups. They concluded that limited reaming is preferred in patients with vascular compromise to the tibia.
Incorrect Answers:
1: Reamed and unreamed tibias have similar mineral apposition rates. 2: Reamed tibias have the highest amount of new bone formation.
3: The lowest porosity of bone is seen with limited reaming.
5: Nails that are tight to the cortex have less reperfusion than appropriately fitting or loose nails.
Question 15High Yield
Figure 63 is the radiograph of a 48-year-old woman with a long history of left forefoot pain and deformity. She says she had surgery as a teenager and that her foot has slowly gotten worse over the years. She recently reached the point at
which she cannot find comfortable shoes. What does the double density at the arrow signify?
58
which she cannot find comfortable shoes. What does the double density at the arrow signify?
58

Explanation
The radiograph shows an overlap of the base of the proximal phalanx over the second metatarsal head and no defined joint space. The base of the proximal phalanx is proximal to the distal aspect of the metatarsal head. The dislocation is chronic secondary to degeneration and disruption of the plantar plate from years of increased stress from the hallux valgus deformity and a long second metatarsal. An impaction fracture or a growth disturbance
would reveal a joint space. Chondrocalcinosis would reveal calcification of the articular cartilage and usually degenerative changes. Ossification of the plantar plate is rare and would look more like a sesamoid.
RECOMMENDED READINGS
1. Coughlin MJ. Lesser toe abnormalities. Instr Course Lect. 2003;52:421-44. Review.
[PubMed PMID: 12690869.](http://www.ncbi.nlm.nih.gov/pubmed/12690869)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690869)
2. Coughlin MJ. Lesser toe deformities. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 1. 8th ed. Philadelphia, PA: Mosby; 2007:407-443.
would reveal a joint space. Chondrocalcinosis would reveal calcification of the articular cartilage and usually degenerative changes. Ossification of the plantar plate is rare and would look more like a sesamoid.
RECOMMENDED READINGS
1. Coughlin MJ. Lesser toe abnormalities. Instr Course Lect. 2003;52:421-44. Review.
[PubMed PMID: 12690869.](http://www.ncbi.nlm.nih.gov/pubmed/12690869)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690869)
2. Coughlin MJ. Lesser toe deformities. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 1. 8th ed. Philadelphia, PA: Mosby; 2007:407-443.
Question 16High Yield
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?
Explanation
The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring.
REFERENCES: Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
REFERENCES: Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 17High Yield
What is the most proximal level of amputation that a child can undergo and still maintain a normal walking speed without significantly increasing their energy cost?
Explanation
A through-knee amputation, or knee disarticulation, is the most proximal level of amputation a child can undergo and still maintain a self-selected walking speed without significantly increasing their energy expenditure.
Jeans et al. conducted a study of 73 children. They found that children with Above-knee amputations (AKA) and hip disarticulation amputations had significantly reduced walking speed and increased oxygen consumption. They also determined that children with a Syme's amputation, transtibial
amputation, or knee disarticulation ambulated with approximately the same speed and oxygen consumption as did normal children in the same age group.
Herbert et al. performed a study of 10 children with below knee amputations (BKA's)compared to 14 children without amputations. They found that that children with BKAs did not choose speeds different from their peers without amputations, regardless of residual limb length of the BKA.
Illustration V is a video showing a through-knee amputation. Incorrect Answers:
Answer 1: Girdlestone hip resection removes the entire proximal femur and
commonly is done through a lateral approach.
Answer 2: Above-knee amputation is performed through the femur and attention is needed for adductor myodesis to prevent abduction deformity. Answer 4: Below-knee amputation is performed commonly 12-15cm inferior to the knee joint line.
Answer 5: Chopart amputation is performed through the transverse tarsal joints and leaves the talus and calcaneus intact.
Jeans et al. conducted a study of 73 children. They found that children with Above-knee amputations (AKA) and hip disarticulation amputations had significantly reduced walking speed and increased oxygen consumption. They also determined that children with a Syme's amputation, transtibial
amputation, or knee disarticulation ambulated with approximately the same speed and oxygen consumption as did normal children in the same age group.
Herbert et al. performed a study of 10 children with below knee amputations (BKA's)compared to 14 children without amputations. They found that that children with BKAs did not choose speeds different from their peers without amputations, regardless of residual limb length of the BKA.
Illustration V is a video showing a through-knee amputation. Incorrect Answers:
Answer 1: Girdlestone hip resection removes the entire proximal femur and
commonly is done through a lateral approach.
Answer 2: Above-knee amputation is performed through the femur and attention is needed for adductor myodesis to prevent abduction deformity. Answer 4: Below-knee amputation is performed commonly 12-15cm inferior to the knee joint line.
Answer 5: Chopart amputation is performed through the transverse tarsal joints and leaves the talus and calcaneus intact.
Question 18High Yield
A 6-year-old child is seen in the emergency department after falling from the monkey bars. Examination reveals tenderness of the right humerus and an inability to dorsiflex the wrist. No other injuries are identified. Radiographs show a minimally displaced and angulated (10 degrees of varus angulation) fracture of the distal one third of the humeral shaft. Initial management should consist of which of the following?
Explanation
2010 Pediatric Orthopaedic Examination
ook • 69
3. ##### Immediate exploration of the radial nerve with open reduction and plate fixation
4. ##### Monitoring of radial nerve function and application of a sling and swathe
5. ##### Monitoring of radial nerve function and external fixation PREFERRED RESPONSE: 4
DISCUSSION: Humeral shaft fractures in children rarely require open reduction. Shoulder and elbow function does not appear to be affected by up to 40 degrees of angulation in this patient population. Because of the high rate of remodeling in pediatric patients, the standard treatment is immobilization in a sling and swathe, a hanging arm cast, or a compressive dressing. Surgical fixation of humeral shaft fractures is usually only necessary in open injuries, multitrauma, or severely displaced fractures. Most radial nerve injuries associated with humerus fractures are secondary to contusion. Almost all associated radial nerve injuries in pediatric patients can be treated with observation.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 304.
Shrader MW: Proximal humerus and humeral shaft fractures in children. Hand Clin 2007;23:431-435. Caviglia H, Garrido CP, Palazzi FF, et al: Pediatric fractures of the humerus. Clin Orthop Relat Res 2005;432:49-56.
2010 Pediatric Orthopaedic Examination
ook • 69
3. ##### Immediate exploration of the radial nerve with open reduction and plate fixation
4. ##### Monitoring of radial nerve function and application of a sling and swathe
5. ##### Monitoring of radial nerve function and external fixation PREFERRED RESPONSE: 4
DISCUSSION: Humeral shaft fractures in children rarely require open reduction. Shoulder and elbow function does not appear to be affected by up to 40 degrees of angulation in this patient population. Because of the high rate of remodeling in pediatric patients, the standard treatment is immobilization in a sling and swathe, a hanging arm cast, or a compressive dressing. Surgical fixation of humeral shaft fractures is usually only necessary in open injuries, multitrauma, or severely displaced fractures. Most radial nerve injuries associated with humerus fractures are secondary to contusion. Almost all associated radial nerve injuries in pediatric patients can be treated with observation.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 304.
Shrader MW: Proximal humerus and humeral shaft fractures in children. Hand Clin 2007;23:431-435. Caviglia H, Garrido CP, Palazzi FF, et al: Pediatric fractures of the humerus. Clin Orthop Relat Res 2005;432:49-56.
Question 19High Yield
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
The patient has a pectoralis major rupture, an injury that occurs most commonly during weight lifting. Grade III injuries represent complete tears of either the musculotendinous junction or an avulsion of the tendon from the humerus, the most common injury site. Examination will most likely reveal ecchymoses and swelling in the proximal arm and axilla, and strength testing will show weakness with internal rotation and in adduction and forward flexion. Axillary webbing, caused by a more defined inferior margin of the anterior deltoid as the result of rupture of the pectoralis, can be seen as the swelling diminishes. Surgical repair is the treatment of choice for complete ruptures. Nonsurgical treatment is associated with significant losses in adduction, flexion, internal rotation, strength, and peak torque. The pectoralis major originates from the proximal clavicle and the border of the sternum, including ribs two through six. The pectoralis major inserts (rather than originates) on the humerus. The coracoid process is the insertion site for the pectoralis minor, as well as the origin for the conjoined tendon. The pectoralis major has no attachment or origin from the scapula. The anterior deltoid originates from the lateral one third of the clavicle and the anterior acromion.
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Question 20High Yield
If surgery is necessary, what is the most appropriate procedure?
Explanation
- Debridement of all infected tissue and a negative-pressure dressing for the resulting wound
Question 21High Yield
A 21-year-old man learned he had Ewing sarcoma of the right distal femur at age 13. He underwent treatment with neoadjuvant chemotherapy, surgical resection with distal femoral replacement, and adjuvant chemotherapy. He completed treatment at age 14, and subsequent surveillance imaging has shown no evidence of recurrence. He has noted increasing fatigue during the last 3 months, however, and bleeding when he brushes his teeth. An examination is unremarkable with the exception of bilateral pretibial bruising for which the patient does not recall trauma. Which tests will aid in diagnosis?
Explanation
This patient most likely has therapy-associated leukemia, which occurs in approximately 2% of patients who have Ewing sarcoma within 5 years of receiving treatment. Most cases are myelodysplasia or acute myeloid leukemia. Most patients with therapy-associated leukemia
respond poorly to conventional chemotherapies and require allogenic stem cell transplant for cure. Fatigue, gum bleeding, and bruising should raise concern for leukemia in light of his clinical history. A CBC with a peripheral smear will likely reveal an elevated leukocyte count with an abnormal percentage of myeloblasts. ESR and CRP are required to assess for infection of a prosthesis. Fatigue may be associated with chronic infection, but bleeding would be atypical. Platelet aggregation test results may be abnormal for this patient, but this testing is unlikely to reveal a specific diagnosis because drugs and genetic disorders may cause platelet aggregation dysfunction. Serum protein electrophoresis is diagnostic for multiple myeloma, but this patient is the wrong age for this condition and does not have appropriate signs and symptoms. A CBC can demonstrate early findings for leukemia with anemia and platelet suppression despite no blast presence. Of note, 25% of long-term survivors of Ewing sarcoma have findings of cardiotoxicity.
RECOMMENDED READINGS
10. [Bhatia S, Krailo MD, Chen Z, Burden L, Askin FB, Dickman PS, Grier HE, Link MP, Meyers PA, Perlman EJ, Rausen AR, Robison LL, Vietti TJ, Miser JS. Therapy-related myelodysplasia and acute myeloid leukemia after Ewing sarcoma and primitive neuroectodermal tumor of bone: A report from the Children's Oncology Group. Blood. 2007 Jan 1;109(1):46-51. Epub 2006 Sep 19. PubMed PMID: 16985182. ](http://www.ncbi.nlm.nih.gov/pubmed/16985182)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16985182)
11. [Hamilton SN, Carlson R, Hasan H, Rassekh SR, Goddard K. Long-term Outcomes and Complications in Pediatric Ewing Sarcoma. Am J Clin Oncol. 2015 Jan 16. [Epub ahead of print] PubMed PMID: 25599318. ](http://www.ncbi.nlm.nih.gov/pubmed/25599318)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25599318)
respond poorly to conventional chemotherapies and require allogenic stem cell transplant for cure. Fatigue, gum bleeding, and bruising should raise concern for leukemia in light of his clinical history. A CBC with a peripheral smear will likely reveal an elevated leukocyte count with an abnormal percentage of myeloblasts. ESR and CRP are required to assess for infection of a prosthesis. Fatigue may be associated with chronic infection, but bleeding would be atypical. Platelet aggregation test results may be abnormal for this patient, but this testing is unlikely to reveal a specific diagnosis because drugs and genetic disorders may cause platelet aggregation dysfunction. Serum protein electrophoresis is diagnostic for multiple myeloma, but this patient is the wrong age for this condition and does not have appropriate signs and symptoms. A CBC can demonstrate early findings for leukemia with anemia and platelet suppression despite no blast presence. Of note, 25% of long-term survivors of Ewing sarcoma have findings of cardiotoxicity.
RECOMMENDED READINGS
10. [Bhatia S, Krailo MD, Chen Z, Burden L, Askin FB, Dickman PS, Grier HE, Link MP, Meyers PA, Perlman EJ, Rausen AR, Robison LL, Vietti TJ, Miser JS. Therapy-related myelodysplasia and acute myeloid leukemia after Ewing sarcoma and primitive neuroectodermal tumor of bone: A report from the Children's Oncology Group. Blood. 2007 Jan 1;109(1):46-51. Epub 2006 Sep 19. PubMed PMID: 16985182. ](http://www.ncbi.nlm.nih.gov/pubmed/16985182)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16985182)
11. [Hamilton SN, Carlson R, Hasan H, Rassekh SR, Goddard K. Long-term Outcomes and Complications in Pediatric Ewing Sarcoma. Am J Clin Oncol. 2015 Jan 16. [Epub ahead of print] PubMed PMID: 25599318. ](http://www.ncbi.nlm.nih.gov/pubmed/25599318)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25599318)
Question 22High Yield
A 12-year-old boy sustains open comminuted midshaft tibial and fibular fractures while playing indoor soccer. The wound is grossly clean and measures 7 cm with some periosteal stripping. Antibiotics and tetanus toxoid are administered immediately in the emergency department. Following irrigation and debridement of the wound in the operating room, treatment should include
Explanation
Open fractures in children have similar rates of short-term complications such as compartment syndrome, vascular injury, and nerve injury when compared to adult fractures. Primary wound closure should be used for Gustillo and Anderson type 1 or uncomplicated type 2 fractures after surgical debridement. Skeletal stabilization may consist of external fixation, flexible nails, or casting with or without supplementary pin fixation. For an open comminuted midshaft fracture, external fixation is the treatment of choice. Reamed intramedullary nailing is contraindicated in children with an open physis. Plate fixation has a high complication rate in severe open fractures.
REFERENCES: Jones BG, Duncan RD: Open tibial fractures in children under 13 years of age-10 years experience. Injury 2003;34:776-780.
Bartlett CS III, Weiner LS, Yang EC: Treatment of type II and type III open tibia fractures in children. J Orthop Trauma 1997;11:357-362.
Robertson P, Karol LA, Rab GT: Open fractures of the tibia and femur in children. J Pediatr Orthop 1996;16:621-626.
Cullen MC, Roy DR, Crawford AH, et al: Open fracture of the tibia in children. J Bone Joint Surg Am 1996;78:1039-1047.
REFERENCES: Jones BG, Duncan RD: Open tibial fractures in children under 13 years of age-10 years experience. Injury 2003;34:776-780.
Bartlett CS III, Weiner LS, Yang EC: Treatment of type II and type III open tibia fractures in children. J Orthop Trauma 1997;11:357-362.
Robertson P, Karol LA, Rab GT: Open fractures of the tibia and femur in children. J Pediatr Orthop 1996;16:621-626.
Cullen MC, Roy DR, Crawford AH, et al: Open fracture of the tibia in children. J Bone Joint Surg Am 1996;78:1039-1047.
Question 23High Yield
A patient with no history of patellar instability sustains a traumatic lateral patellar dislocation. What structure most likely has been torn?
Explanation
Any of the above structures may be involved in a lateral patellar dislocation. However, biomechanic studies have found that the medial patellofemoral ligament is the major soft-tissue static restraint of lateral patellar displacement, providing at least 50% of this function.
REFERENCES: Desio SM, Burks RT, Bachus KN: Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 1998;26:59-65.
Conlan T, Garth WP Jr, Lemons JE: Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am 1993;75:682-693.
Warren LF, Marshall JL: The supporting structures and layers on the medial compartment of the knee: An anatomical analysis. J Bone Joint Surg Am 1979;61:56-62.
REFERENCES: Desio SM, Burks RT, Bachus KN: Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 1998;26:59-65.
Conlan T, Garth WP Jr, Lemons JE: Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am 1993;75:682-693.
Warren LF, Marshall JL: The supporting structures and layers on the medial compartment of the knee: An anatomical analysis. J Bone Joint Surg Am 1979;61:56-62.
Question 24High Yield
Schwannomas are differentiated from neurofibromas by all of the following except:
Explanation
Schwann cells contribute to schwannoma and neurofibroma.
Question 25High Yield
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. Knee range of motion is between 0° and 70°. What is the most appropriate treatment option?
---
---

Explanation
The MR image shows bone bruises (“kissing contusions”) consistent with an ACL tear. During the ACL subluxation event, the posterolateral tibial plateau subluxes anteriorly, making contact with the mid portion of the lateral femoral condyle and resulting in this characteristic bone bruise pattern on MRI. Randomized clinical trials comparing early accelerated versus nonaccelerated rehabilitation programs have demonstrated no significant differences in long-term results with regard to function, reinjury, and successful return to play. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 26High Yield
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
According to a study by the Scoliosis Research Society, the use of anterior decompression is most predictable for improving neurologic status. This is particularly true of bowel and bladder functional loss. Laminectomy is contraindicated because it further destabilizes the spine. Posterior instrumentation and indirect reduction through distraction and ligamentotaxis only incompletely decompress the compromised canal and are successful only if performed within 48 hours of injury. While some improvement may occur with closed management, the amount of recovery is less than that achieved with surgical decompression. A posterior approach and instrumentation may be added to the anterior decompression based on the characteristics of associated injuries to the posterior element.
REFERENCES: Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
REFERENCES: Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 27High Yield
In the diagnosis of periprosthetic infection involving a total joint arthroplasty using the 2018 Musculoskeletal Infection Society (MSIS) criteria, there are major and minor criteria. An example of a major criteria is
Explanation
82
Question 28High Yield
Which of the following activities can improve posterior capsular contractures?
Explanation
Posterior capsule stretching is performed in the cross-chest and behind the back positions. Stretching in internal rotation in the abducted shoulder will further stretch the posterior capsule. Wide grip stretch, and anterior capsule and strengthening exercises will not necessarily stretch the capsule.
REFERENCES: Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
REFERENCES: Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
Question 29High Yield
The accumulation of what metal was attributed to the 1996 episode of âbeer-drinkersâ cardiomyopathy:
Explanation
The accumulation of Co in the myocardium can induce cardiomyopathy, which was particularly evident after the 1996 episode of âbeer-drinkersâ cardiomyopathy, during which Co was used as a foam-stabilizing agent in beer
Question 30High Yield
Workup of this patient should specifically include which of the following studies?
Explanation
_
_
_
Question 31High Yield
What is the most common complication following open reduction locking plate osteosynthesis of this injury?
Explanation
- Intra-articular screw penetration_
Question 32High Yield
aOne year after undergoing a primary total knee arthroplasty, a 65-year-old man has a 1-week history of new onset anterior knee pain. He can perform a straight-leg raise with no extension lag. Radiographs reveal a transverse patella fracture with 8 mm of displacement and an intact patellar component. The best course of treatment is
Explanation
This patient has a displaced periprosthetic patella fracture with an intact extensor mechanism. Surgical treatment for this condition has been associated with relatively poor clinical results because the fracture occurs late (attributable to patella osteonecrosis). The optimal initial treatment is to treat the fracture nonsurgically with immobilization of the knee in extension either with a long-leg cast or knee immobilizer.
18
18
Question 33High Yield
A patient with a displaced and comminuted fracture of the radial head and neck also has pain and swelling about the ipsilateral distal radioulnar joint. Which treatment option may exacerbate the wrist disorder?
Explanation
This scenario describes a forearm-axial instability pattern, which must be recognized before pursuing treatment. Fracture or dislocation of the lateral elbow compartment (radial head/capitellum) associated with ipsilateral distal radioulnar joint derangement is a form of radioulnar dissociation commonly known as Essex-Lopresti fracture dislocation. Radial head excision sets off a chain of events, and delayed diagnosis can result in considerable morbidity following these injuries. Excision of the radial head allows proximal migration of the radius, causing potential problems at both the elbow and wrist. After such proximal migration has occurred, there is no reliable method of forearm reconstruction.
There are a number of treatments for this condition. Salvage of the radial head by open reduction and internal fixation is preferable if possible. However, in cases of marked comminution, radial metallic head implant arthroplasty is an acceptable substitute. The need for soft-tissue repair or pin stabilization of the distal radioulnar joint has not been defined, although some form of forearm immobilization is necessary to allow healing of the injured interosseous membrane.
RECOMMENDED READINGS
81. Trousdale RT, Amadio PC, Cooney WP, Morrey BF. Radio-ulnar dissociation. A review of twenty cases. J Bone Joint Surg Am. 1992 Dec;74(10):1486-97. PubMed PMID: 1469008.
82. Edwards GS Jr, Jupiter JB. Radial head fractures with acute distal radioulnar dislocation. Essex-Lopresti revisited. Clin Orthop Relat Res. 1988 Sep;(234):61-9. PubMed PMID: 3409602.
There are a number of treatments for this condition. Salvage of the radial head by open reduction and internal fixation is preferable if possible. However, in cases of marked comminution, radial metallic head implant arthroplasty is an acceptable substitute. The need for soft-tissue repair or pin stabilization of the distal radioulnar joint has not been defined, although some form of forearm immobilization is necessary to allow healing of the injured interosseous membrane.
RECOMMENDED READINGS
81. Trousdale RT, Amadio PC, Cooney WP, Morrey BF. Radio-ulnar dissociation. A review of twenty cases. J Bone Joint Surg Am. 1992 Dec;74(10):1486-97. PubMed PMID: 1469008.
82. Edwards GS Jr, Jupiter JB. Radial head fractures with acute distal radioulnar dislocation. Essex-Lopresti revisited. Clin Orthop Relat Res. 1988 Sep;(234):61-9. PubMed PMID: 3409602.
Question 34High Yield
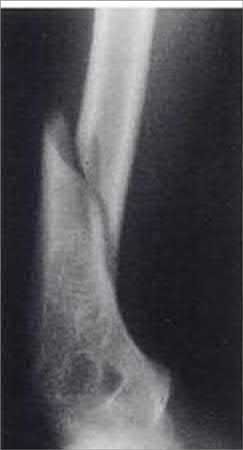
A 68-year-old male sustains the humeral shaft fracture shown in Figures A and B. Upon presentation, he is unable to extend his thumb, fingers, and wrist. After 4 months of non-operative management, the fracture has healed, but his physical exam is unchanged. What is the next most appropriate step in management?

Explanation
The clinical presentation is consistent for a residual radial nerve palsy 4 months after a humeral shaft fracture. An EMG is indicated at this time to evaluate the status of the nerve recovery.
A radial nerve injury which occurs during a humeral shaft fracture or after bracing is not an indication for immediate exploration. Most often, the nerve function returns without surgical intervention. An EMG should be performed at 3-5 months to evaluate the status of the nerve recovery. If fasciculations are present, then this represents recovery, and observation should be continued. If fibrillations are present, this represents denervation, and surgical exploration should be considered.
Pollock et al followed 24 humeral-shaft fractures with associated radial-nerve injuries, 2 of which required open exploration and all recovered. They recommend careful observation for return of nerve function and exploration at 3.5-4 months after injury if there is still no clinical or EMG evidence of recovery.
Bostman et al reviewed 59 immediate and 16 secondary radial nerve palsies and no support emerged for routine early exploration in either group.
Figures A and B show an oblique fracture at the junction of the middle and distal 1/3 of the humeral shaft.
Illustration A shows the relative close position of the radial nerve to the humerus at the midlevel of humerus, and why it is at risk with a humerus shaft fracture.
A radial nerve injury which occurs during a humeral shaft fracture or after bracing is not an indication for immediate exploration. Most often, the nerve function returns without surgical intervention. An EMG should be performed at 3-5 months to evaluate the status of the nerve recovery. If fasciculations are present, then this represents recovery, and observation should be continued. If fibrillations are present, this represents denervation, and surgical exploration should be considered.
Pollock et al followed 24 humeral-shaft fractures with associated radial-nerve injuries, 2 of which required open exploration and all recovered. They recommend careful observation for return of nerve function and exploration at 3.5-4 months after injury if there is still no clinical or EMG evidence of recovery.
Bostman et al reviewed 59 immediate and 16 secondary radial nerve palsies and no support emerged for routine early exploration in either group.
Figures A and B show an oblique fracture at the junction of the middle and distal 1/3 of the humeral shaft.
Illustration A shows the relative close position of the radial nerve to the humerus at the midlevel of humerus, and why it is at risk with a humerus shaft fracture.
Question 35High Yield
A 28-year-old obtunded man with a T12 burst fracture is treated in a thoracolumbosacral orthosis.
Explanation
- Pressure ulcers
Question 36High Yield
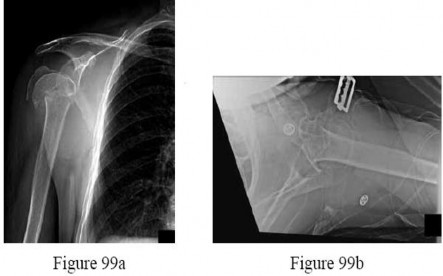
A 55-year-old woman with degenerative joint disease underwent total shoulder arthroplasty (TSA). She was doing well without complications at her 2-week visit (Figures 1 and 2). She returned at 6 weeks with increased pain, shoulder clicking, and difficulty with forward elevation and internal rotation. She recalls slipping, and to prevent a fall, moved her arm suddenly to grab a rail. New radiographs are shown in Figures 3 and
Explanation
the radiographs at her 6-week appointment show anterior subluxation of the glenohumeral joint indicative of subscapularis insufficiency. Subscapularis repair is the next best step in management, especially in this age group, with well-fixed and well-aligned components.
3
3
Question 37High Yield
Figure 35 is the radiograph of a 37-year-old woman who began having right forefoot pain about 4 weeks ago after increasing her daily running mileage. She denies any specific injury. Upon examination she has tenderness over the medial forefoot with mild swelling. In addition to her activity level, what is the primary etiology of the radiograph finding?

Explanation
Stress fractures are the result of physiological bone response to increased stress. Increased stress on bone triggers an increase in remodeling, which begins with resorption of bone at the site of stress. Ongoing stress can overwhelm bone strength, resulting in a fracture. In the foot this most commonly is seen in the second metatarsal at the junction of the middle and distal thirds. Contributing factors to increased loading of the second metatarsal include hallux valgus (decreased hallux loading transfers to the second metatarsal head), hallux rigidus (offloading of the hallux attributable to pain increases second metatarsal loading), and a long second metatarsal (increased duration of contact during push-off in the stance phase).
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
[76/. doi: 10.5435/JAAOS-20-03-167. Review. PubMed PMID: 22382289. ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22382289)
[Donahue SW, Sharkey NA. Strains in the metatarsals during the stance phase of gait: implications for stress fractures. J Bone Joint Surg Am. 1999 Sep;81(9):1236-44. PubMed PMID: 10505520. ](http://www.ncbi.nlm.nih.gov/pubmed/10505520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10505520)
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
[76/. doi: 10.5435/JAAOS-20-03-167. Review. PubMed PMID: 22382289. ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22382289)
[Donahue SW, Sharkey NA. Strains in the metatarsals during the stance phase of gait: implications for stress fractures. J Bone Joint Surg Am. 1999 Sep;81(9):1236-44. PubMed PMID: 10505520. ](http://www.ncbi.nlm.nih.gov/pubmed/10505520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10505520)
Question 38High Yield
-Clinical staging of osteomyelitis using the Cierney-Mader classification system takes into account which of the following factors?
Explanation
No detailed explanation provided for this question.
Question 39High Yield
An 18-year-old high school basketball player is being treated for Achilles tendinitis. What type of strengthening exercise has been shown to be helpful in the later phases of rehabilitation?

Explanation
DISCUSSION: Eccentric strengthening for tendinopathies has proved most helpful in the later stages of rehabilitation. Although the exact mechanism of the effect on eccentric exercises is not known, the most widely accepted theory is that the absence of concentric stretching disrupts the normal lengthing/shorten- ing cycle which may cause shearing in the tendon and injury to the collagen. Isokinetic exercise maintains a constant angular velocity of joint motion. Isotonic exercise maintains a constant force of contraction while isometric contraction develops force without changing the length of the musculotendinous unit.
All three types of these exercises have not been shown to benefit Achilles tendinitis as much as eccentric exercise.
REFERENCES: Jonsson P, Alfredson H, Sunding K, et al: New regimen for eccentric calf-muscle training in patients with chronic insertional Achilles tendinopathy: Results of a pilot study. Br J Sports Med
2008;42:746-749.
Maffulli N, Walley G, Say ana MK, et al: Eccentric calf muscle training in athletic patients with Achilles tendinopathy. Disabil Rehabil 2008;30:1677-1684.
Figure 67
DISCUSSION: Eccentric strengthening for tendinopathies has proved most helpful in the later stages of rehabilitation. Although the exact mechanism of the effect on eccentric exercises is not known, the most widely accepted theory is that the absence of concentric stretching disrupts the normal lengthing/shorten- ing cycle which may cause shearing in the tendon and injury to the collagen. Isokinetic exercise maintains a constant angular velocity of joint motion. Isotonic exercise maintains a constant force of contraction while isometric contraction develops force without changing the length of the musculotendinous unit.
All three types of these exercises have not been shown to benefit Achilles tendinitis as much as eccentric exercise.
REFERENCES: Jonsson P, Alfredson H, Sunding K, et al: New regimen for eccentric calf-muscle training in patients with chronic insertional Achilles tendinopathy: Results of a pilot study. Br J Sports Med
2008;42:746-749.
Maffulli N, Walley G, Say ana MK, et al: Eccentric calf muscle training in athletic patients with Achilles tendinopathy. Disabil Rehabil 2008;30:1677-1684.
Figure 67
Question 40High Yield
Which of the following nerves is susceptible to entrapment near the calcaneal attachment site of the plantar fascia and can mimic or co-exist with plantar fasciitis?
Explanation
The first branch of the lateral plantar nerve is susceptible to entrapment beneath the deep fascia of the adductor hallucis muscle adjacent to the calcaneal attachment of the plantar fascia. This can be a cause of chronic heel pain. Additionally, the nerve is vulnerable to injury by a blind dissection in releasing the plantar fascia. The dorsal cutaneous branch of the superficial peroneal nerve supplies sensation to the dorsum of the foot. The medial calcaneal branch of the posterior tibial nerve lies in the subcutaneous tissues and innervates the skin of the heel. It is vulnerable to injury from skin incisions on the medial side of the heel. The lateral branch of the medial plantar nerve forms the second and third common digital nerves. Entrapment of the proper medial plantar nerve can occur at the master knot of Henry. This is well distal to the calcaneal attachment of the plantar fascia, and the pain usually radiates more distally in the arch, separate from heel pain. The communicating branch of the fourth common digital nerve crosses to the third common digital nerve. Therefore, the third common digital nerve receives supply from both the lateral and medial plantar nerves. This dual supply has been implicated in the increased incidence of digital neuroma of the third common digital nerve.
REFERENCES: Bordelon RL: Heel pain, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 837-857.
Mann RA, Baxter DE: Diseases of the nerves, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 543-574.
Baxter DE: The heel in sport. Clin Sports Med 1994;13:683-693.
REFERENCES: Bordelon RL: Heel pain, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 837-857.
Mann RA, Baxter DE: Diseases of the nerves, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 543-574.
Baxter DE: The heel in sport. Clin Sports Med 1994;13:683-693.
Question 41High Yield
Increasing tibial polyethylene conformity can have what effect on fixed bearing total knee arthroplasty?
Explanation
DISCUSSION: Increasing conformity between the tibial polyethylene bearing and the femoral component has desirable and undesirable consequences. Increased conformity increases the contact area and thereby reduces contact stress within the polyethylene. This can lead to less risk of polyethylene wear, fracture, and delamination. However, increasing conformity also limits the ability of the femur to roll back during flexion, and may transfer increased shear stress to the fixation surfaces of the implants.
REFERENCES: D’Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop Relat Res 2001;392:232-238.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
REFERENCES: D’Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop Relat Res 2001;392:232-238.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 42High Yield
A 22-year-old male sustains the injury seen in Figures A and B as the result of a motor vehicle collision. He subsequently undergoes the procedure shown in Figures C and D with a 12 millimeter nail. When would full weight-bearing be allowed after surgery?




Explanation
Comminuted femoral shaft fractures treated with statically locked intramedullary nails of appropriate diameter can be treated with immediate weight-bearing, with little risk of nail/screw breakage or deformity. Immediate range of motion and weight-bearing can be extremely beneficial to short-term patient outcomes, especially in polytrauma patients.
Brumback et al.(1988) reviewed 133 dynamically locked femoral nails and report that 10.5% lost fixation and/or reduction postoperatively. They recommend reviewing high-quality radiographs to determine fracture characteristics, and note that dynamic fixation only be considered for transverse fracture patterns.
Brumback et al.(1988) performed a prospective series of 97 patients with statically locked femoral nails, and they report that 98% of these went on to successful union without additional procedures, and the 2% with nonunions were successfully treated with later conversion to dynamic interlocking. They also found that no implant failure or deformity occurred with early walking or weight-bearing.
Brumback et al.(1999) reviewed the biomechanics of immediate weightbearing after statically locked intramedullary nails are used in a segmental femur model, and they found that it would be safe. They then looked at immediate weight-bearing of these fractures after statically locked nail insertion in a series of 35 patients, and found no loss of reduction or implant failure with immediate weight-bearing.
Figures A and B show a comminuted, segmental femoral shaft fracture, while Figures C and D show the immediate postoperative radiographs of this patient after intramedullary nailing.
Incorrect Answers:
Answers 2-5: Delay in weight-bearing is not required for this injury pattern, if treated with an appropriate diameter statically locked intramedullary nail.
Brumback et al.(1988) reviewed 133 dynamically locked femoral nails and report that 10.5% lost fixation and/or reduction postoperatively. They recommend reviewing high-quality radiographs to determine fracture characteristics, and note that dynamic fixation only be considered for transverse fracture patterns.
Brumback et al.(1988) performed a prospective series of 97 patients with statically locked femoral nails, and they report that 98% of these went on to successful union without additional procedures, and the 2% with nonunions were successfully treated with later conversion to dynamic interlocking. They also found that no implant failure or deformity occurred with early walking or weight-bearing.
Brumback et al.(1999) reviewed the biomechanics of immediate weightbearing after statically locked intramedullary nails are used in a segmental femur model, and they found that it would be safe. They then looked at immediate weight-bearing of these fractures after statically locked nail insertion in a series of 35 patients, and found no loss of reduction or implant failure with immediate weight-bearing.
Figures A and B show a comminuted, segmental femoral shaft fracture, while Figures C and D show the immediate postoperative radiographs of this patient after intramedullary nailing.
Incorrect Answers:
Answers 2-5: Delay in weight-bearing is not required for this injury pattern, if treated with an appropriate diameter statically locked intramedullary nail.
Question 43High Yield
An 18-year-old man sustained a traumatic laceration of the common peroneal nerve when glass fell on the outer part of his leg 1 year ago. He has used a molded foot and ankle orthosis for the past 10 months,but would now like surgical intervention. Electromyography shows no function in the anterior or lateral compartments. He has 5/5 muscle strength of the superficial and deep posterior compartments. What is the most appropriate treatment?
Explanation
In a patient with a drop foot and with 5/5 muscle strength of the posterior tibial tendon, a split posterior tibial tendon transfer would be the most appropriate treatment option based on the options presented. The deep peroneal nerve innervates the anterior tibial tendon. This muscle has been affected by the injury; therefore, the anterior tibial tendon cannot be transferred. A subtalar fusion would help correct inversion and eversion deformities, but is not effective for plantar flexion deformities.
The foot drop is caused by a neurologic condition in this patient, not a contracture of the gastrocsoleus complex.Therefore, a recession would not be beneficial. A flexor hallucis longus tendon transfer would not take the deforming force and make it a corrective force.
The foot drop is caused by a neurologic condition in this patient, not a contracture of the gastrocsoleus complex.Therefore, a recession would not be beneficial. A flexor hallucis longus tendon transfer would not take the deforming force and make it a corrective force.
Question 44High Yield
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
Explanation
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate.
REFERENCES: Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
McCarty DJ, Halverson PB, Carrera GF, Brewer BJ, Kozin F: Milwaukee shoulder: Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I: Clinical aspects. Arthritis Rheum 1981;24:464-473.
REFERENCES: Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
McCarty DJ, Halverson PB, Carrera GF, Brewer BJ, Kozin F: Milwaukee shoulder: Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I: Clinical aspects. Arthritis Rheum 1981;24:464-473.
Question 45High Yield
What is the primary advantage of two incisions compared to one for open reduction internal fixation of a both bones forearm fracture?
Explanation
Post-osteosynthetic synostosis is a known complication in both bone forearm fractures. The risk is increased in fractures of the proximal 1/3 of the ulna and radius. Other risk factors include severity of injury, head trauma, polytrauma. Vince et al found synostosis was often associated with bone fragments or hardware in the interosseous space. Bauer et al found 1/65 cases treated utilizing the two-incision approach developed synostosis, while 5/12 cases in which the fractures were stabilized using a single incision developed synostoses. They recommended a two incision approach to both bones ORIF.
Question 46High Yield
What structure is most often injured in a volar proximal interphalangeal joint dislocation?
Explanation
Closed ruptures of the central slip of the extensor tendon may occur with volar proximal interphalangeal joint dislocation, forced flexion of the proximal interphalangeal joint, or blunt trauma to the dorsum of the proximal interphalangeal joint. The other structures are not typically injured in proximal interphalangeal joint dislocations. Treatment typically requires static splinting of the proximal interphalangeal joint. In the more common dorsal proximal interphalangeal joint dislocation, the volar plate is injured, and early range of motion may be started after reduction.
REFERENCES: Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1925.
Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
REFERENCES: Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1925.
Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Question 47High Yield
A newborn infant in the nursery must be seen because of his foot. The dorsum of the foot rests against the tibia. The heel moves up when the forefoot moves down. Power is present in all muscles. The foot has an arch and the leg lengths are equal. The diagnosis is:
Explanation
C alcaneovalgus foot has all of these findings and resolves spontaneously.
Fibular hemimelia typically has less calcaneus attitude and more valgus and shortening. Vertical talus entails loss of an arch and loss of cohesive movement of the foot as a whole. There is no evidence of muscle weakness.
There is no evidence of a neuropathic component.
Fibular hemimelia typically has less calcaneus attitude and more valgus and shortening. Vertical talus entails loss of an arch and loss of cohesive movement of the foot as a whole. There is no evidence of muscle weakness.
There is no evidence of a neuropathic component.
Question 48High Yield
-Four months after injury, the tibia is showing evidence of slow healing on radiographs. What is the optimal treatment for this potential nonunion?
Explanation
FOR QUESTIONS 108 THROUGH 110:**_
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
Question 49High Yield
Slide 1 Slide 2 Slide 3
A 65-year-old man has severe foot pain. His plain radiograph is shown in Slide 1, and a needle biopsy specimen in Slides and 3. The most likely diagnosis is:
A 65-year-old man has severe foot pain. His plain radiograph is shown in Slide 1, and a needle biopsy specimen in Slides and 3. The most likely diagnosis is:
Explanation
Gout is caused by the deposition of monosodium urate crystals in tissues, typically around joints. Common locations of gout include the great toe, heel, ankle, and knee. In approximately 50% of patients, the first affected location is the great toe. Gout commonly occurs inside a joint for two reasons - synovial fluid is a poorer solvent than plasma and lower temperatures (as in peripheral joints) favor crystallization.
Neutrophils ingest the crystals and release potent lysosomal enzymes. Punched lesions may be seen on radiographs in chroniCcases, and one can often see an overlying lip of cortex at the edge of the lesion.
Histologically, the tophi have several features: Acellular amorphous material
Macrophages
Foreign body giant cells
In this patient, the joint space is preserved on the plain radiographs. The biopsy specimen has the characteristiCfeatures of gout - acellular amorphous material, macrophages, and foreign body giant cells.
Neutrophils ingest the crystals and release potent lysosomal enzymes. Punched lesions may be seen on radiographs in chroniCcases, and one can often see an overlying lip of cortex at the edge of the lesion.
Histologically, the tophi have several features: Acellular amorphous material
Macrophages
Foreign body giant cells
In this patient, the joint space is preserved on the plain radiographs. The biopsy specimen has the characteristiCfeatures of gout - acellular amorphous material, macrophages, and foreign body giant cells.
Question 50High Yield
Which of the following noncollagenous proteins aid in regulating the maturation of bone mineral crystals:
Explanation
Bone sialoproteins are important in the initiation of mineralization of collagen. They promote apatite nucleation and growth of the crystals. Osteocalcin (bone Gla protein) is important for mineral proliferation and maturation.
Note the role of promoters and inhibitors: Apatite nucleation and growth Promoters
Type I collagen Bone sialoprotein Matrix vesicles Phosphoproteins Proteolipids Biglycan
Inhibitors
Large proteoglycans Pyrophosphate Adenosine triphosphate Citrate
Mineral proliferation
Regulators
Osteocalcin Phosphoproteins Proteoglycans
Note the role of promoters and inhibitors: Apatite nucleation and growth Promoters
Type I collagen Bone sialoprotein Matrix vesicles Phosphoproteins Proteolipids Biglycan
Inhibitors
Large proteoglycans Pyrophosphate Adenosine triphosphate Citrate
Mineral proliferation
Regulators
Osteocalcin Phosphoproteins Proteoglycans
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon