Orthopedic A Review | Dr Hutaif General Orthopedics Rev -...
14 Apr 2026
62 min read
97 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic A Review | Dr Hutaif General Ortho...
00:00
Start Quiz
Question 1High Yield
What structure is the primary restraint to inferior translation of the shoulder?
Explanation
DISCUSSION: The coracohumeral ligament has been shown to be the primary restraint to inferior translation of the shoulder. Although Bigliani and associates have demonstrated that the inferior capsule and inferior glenohumeral ligaments also play a role, none of the other choices provide primary inferior stability of the shoulder. The coracohumeral ligament is an important structure of the rotator interval of the shoulder (the rotator interval contains the long head of the biceps, the superior glenohumeral ligament, the coracohumeral ligament, and a thin layer of capsule). Harryman and associates demonstrated that an open rotator interval closure via imbrication of the coracohumeral ligament improves inferior stability of the glenohumeral joint.
REFERENCES: Harryman DTII, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53 -66.
Bigliani LU, Pollock RG, Soslowsky LJ, et al: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
REFERENCES: Harryman DTII, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53 -66.
Bigliani LU, Pollock RG, Soslowsky LJ, et al: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 2High Yield
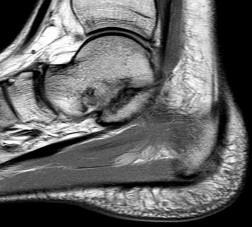
A 40-year-old man has a painful mass on his anterior ankle joint with limited range of motion. A radiograph, MRI scan, a gross specimen, and a hematoxylin/eosin biopsy specimen are shown in Figures 5a through 5d. What is the most likely diagnosis?
Explanation
Synovial chondromatosis results from chondroid metaplasia within the synovium. Male to female ratio is 2:1, with a peak incidence in early adult life. Radiographs can show speckled calcification. Multiple cartilaginous bodies are found loose in the joint and embedded in the synovium. These nodules are composed of cartilage with calcification. Treatment includes synovectomy and removal of loose bodies.
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Hocking R, Negrine J: Primary synovial chondromatosis of the subtalar joint affecting two brothers. Foot Ankle Int 2003;24:865-867.
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Hocking R, Negrine J: Primary synovial chondromatosis of the subtalar joint affecting two brothers. Foot Ankle Int 2003;24:865-867.
Question 3High Yield
A 31-year-old woman underwent a left Kidner procedure 3 months ago. She now has pain overlying the medial column of the foot. She withdraws the foot when touching of the medial foot is attempted. Examination reveals allodynia, pain, hyperalgesia, and edema of the medial foot. What is the most likely diagnosis?
Explanation
**
Patients with reflex sympathetic dystrophy (RSD) have a history of trauma, minor rather than major (eg, Colles fracture), in about 50% to 65% of cases. The condition may also follow a surgical procedure. Patients usually have symptoms and signs of RSD including: pain, described as burning, throbbing, shooting, or aching; hyperalgesia; allodynia; and hyperpathia. There are trophic changes within 10 days of onset of RSD in 30% of the extremities affected, including stiffness and edema and atrophy of hair, nails, and/or skin.
Finally there can be autonomic dysfunction, such as abnormal sweating, either
in excess or anhydrosis, heat and cold insensitivity, or redness or bluish discoloration of the extremities. Shingles, also called herpes zoster or zoster, is a painful skin rash caused by the varicella zoster virus (VZV). VZV is the same virus that causes chickenpox. After a person recovers from chickenpox, the virus stays in the body.
Usually the virus does not cause any problems; however, the virus can reappear years later, causing shingles. Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from
0.15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot's skin temperature),
erythema, joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective sensation, are often pathognomonic of acute Charcot arthropathy. Cellulitis is an infection of the skin.
Examination would reveal erythema, edema, and pain. Osteomyelitis is an infection of the bone. Examination may reveal edema, drainage, and pain.
Patients with reflex sympathetic dystrophy (RSD) have a history of trauma, minor rather than major (eg, Colles fracture), in about 50% to 65% of cases. The condition may also follow a surgical procedure. Patients usually have symptoms and signs of RSD including: pain, described as burning, throbbing, shooting, or aching; hyperalgesia; allodynia; and hyperpathia. There are trophic changes within 10 days of onset of RSD in 30% of the extremities affected, including stiffness and edema and atrophy of hair, nails, and/or skin.
Finally there can be autonomic dysfunction, such as abnormal sweating, either
in excess or anhydrosis, heat and cold insensitivity, or redness or bluish discoloration of the extremities. Shingles, also called herpes zoster or zoster, is a painful skin rash caused by the varicella zoster virus (VZV). VZV is the same virus that causes chickenpox. After a person recovers from chickenpox, the virus stays in the body.
Usually the virus does not cause any problems; however, the virus can reappear years later, causing shingles. Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from
0.15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot's skin temperature),
erythema, joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective sensation, are often pathognomonic of acute Charcot arthropathy. Cellulitis is an infection of the skin.
Examination would reveal erythema, edema, and pain. Osteomyelitis is an infection of the bone. Examination may reveal edema, drainage, and pain.
Question 4High Yield
Which of the following is considered indicative of a scaphoid-lunate ligament tear on posteroanterior radiograph:
Explanation
The VISI, DISI, and spilled tea cup signs are seen on lateral radiographs, whereas the Watson-Jones scaphoid shift test is a clinical sign. The classic pattern after scaphoid-lunate ligament injury is a DISI pattern as the lunate extends and the scaphoid flexes. The spilled tea cup sign is present in perilunate dislocations.
Question 5High Yield
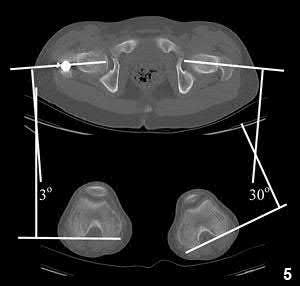
1224) A 55-year-old male is involved in a motorcycle crash and sustains a closed, right-sided, midshaft femur fracture. This is an isolated injury. He is treated with retrograde femoral nailing, and postoperatively is noted to have 30 degrees of internal rotation of the operative extremity, when compared with his nonsurgical side. Which of the following is the most likely cause of this malrotation deformity?
Explanation
Internal rotation of the distal segment of the femur relative to the proximal segment of the femur during nailing can cause a malrotation deformity.
Postsurgical internal malrotation after treatment for a diaphyseal femur fracture typically occurs either via internal rotation of the distal segment relative to the proximal or external rotation of the proximal segment relative to the distal. These clinical findings are consistent with an iatrogenic increase in femoral anteversion.
Dimitriou et al. performed a study to quantify the side-to-side anatomic variation in the proximal femur and the implications for preoperative planning and leg length discrepancy following hip arthroplasty. CT-based 3D femoral models were reconstructed for 122 paired femurs in 61 young healthy subjects with no history of hip pathology. Significant side-to-side differences were found in femoral anteversion, horizontal offset, and femoral head center location.
They concluded that relying on the anatomic landmarks of the contralateral femur during hip arthroplasty may not necessarily result in restoration of native anatomy and leg-length.
Karaman et al. conducted a study which saught to clarify the influence of a femoral rotational malalignment of ≥10° after intramedullary nailing on daily activities. They evaluated twenty-four femoral shaft fracture patients treated with closed antegrade IMN, and determined the presence of malrotation with post-operative CT scans. Ten of the 24 patients had a CT-detected true rotational malalignment of ≥10° compared with the unaffected side, and were noted to have significantly worse functional outcome scores compared with normally rotated femoral shaft patients.
Espinoza et al. present a technique using intraoperative fluoroscopy and the anteversion inherent to the IM nail for obtaining appropriate femoral rotational alignment during surgery. The authors state that their technique reliably sets the femoral anteversion within a normal physiologic range with minimal additional intraoperative steps and without preoperative measurements.
Illustration A shows a CT evaluation of femoral malrotation. The angle on the uninjured side measures 30°, while the malrotated fractured side measures only 3°, indicating a 27° external rotation deformity.
Incorrect Answers:
Answer 1: This would result in external rotation of the femur. Answer 2: This would result in external rotation of the femur. Answer 3: This would result in external rotation of the femur. Answer 4: The contralateral femur would not be affected in this case.
Postsurgical internal malrotation after treatment for a diaphyseal femur fracture typically occurs either via internal rotation of the distal segment relative to the proximal or external rotation of the proximal segment relative to the distal. These clinical findings are consistent with an iatrogenic increase in femoral anteversion.
Dimitriou et al. performed a study to quantify the side-to-side anatomic variation in the proximal femur and the implications for preoperative planning and leg length discrepancy following hip arthroplasty. CT-based 3D femoral models were reconstructed for 122 paired femurs in 61 young healthy subjects with no history of hip pathology. Significant side-to-side differences were found in femoral anteversion, horizontal offset, and femoral head center location.
They concluded that relying on the anatomic landmarks of the contralateral femur during hip arthroplasty may not necessarily result in restoration of native anatomy and leg-length.
Karaman et al. conducted a study which saught to clarify the influence of a femoral rotational malalignment of ≥10° after intramedullary nailing on daily activities. They evaluated twenty-four femoral shaft fracture patients treated with closed antegrade IMN, and determined the presence of malrotation with post-operative CT scans. Ten of the 24 patients had a CT-detected true rotational malalignment of ≥10° compared with the unaffected side, and were noted to have significantly worse functional outcome scores compared with normally rotated femoral shaft patients.
Espinoza et al. present a technique using intraoperative fluoroscopy and the anteversion inherent to the IM nail for obtaining appropriate femoral rotational alignment during surgery. The authors state that their technique reliably sets the femoral anteversion within a normal physiologic range with minimal additional intraoperative steps and without preoperative measurements.
Illustration A shows a CT evaluation of femoral malrotation. The angle on the uninjured side measures 30°, while the malrotated fractured side measures only 3°, indicating a 27° external rotation deformity.
Incorrect Answers:
Answer 1: This would result in external rotation of the femur. Answer 2: This would result in external rotation of the femur. Answer 3: This would result in external rotation of the femur. Answer 4: The contralateral femur would not be affected in this case.
Question 6High Yield
A 45-year-old woman with a history of rheumatoid arthritis has C1-C2 instability with neurologic deterioration. Her posterior atlanto-dens interval is 10 mm. Which fixation technique will be the most biomechanically sound to facilitate fusion across the atlanto-axial junction?

Explanation
C1-C2 transarticular screw fixation is 10-fold stiffer than wiring constructs, particularly in rotation; eliminates the need for postsurgical halo use; and is associated with reported fusion rates to a maximum of 100% for bilateral screws and 95% for unilateral fixation. All of the other fusion techniques mentioned are associated with a pseudarthrosis rate of at least 30%.
RECOMMENDED READINGS
[Stock GH, Vaccaro AR, Brown AK, Anderson PA. Contemporary posterior occipital fixation. J Bone Joint Surg Am. 2006 Jul;88(7):1642-9. PubMed PMID: 16841419. ](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16841419)
[Sim HB, Lee JW, Park JT, Mindea SA, Lim J, Park J. Biomechanical evaluations of various c1-c2 posterior fixation techniques. Spine (Phila Pa 1976). 2011 Mar 15;36(6):E401-7. doi: 10.1097/BRS.0b013e31820611ba. PubMed PMID: 21372651. ](http://www.ncbi.nlm.nih.gov/pubmed/21372651)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21372651)
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 43
Figure 37 is the lateral radiograph of a 71-year-old woman who has pain with ambulation that improves when she sits down. She had similar symptoms 2 years earlier when she underwent an L3-L5 posterior spinal fusion. Upon examination she has good range of hip and knee motion, 5/5 motor function, and normal sensation of her lower extremities. She has negative bilateral straight-leg raise findings and her knees slightly flex to stand upright
37
RECOMMENDED READINGS
[Stock GH, Vaccaro AR, Brown AK, Anderson PA. Contemporary posterior occipital fixation. J Bone Joint Surg Am. 2006 Jul;88(7):1642-9. PubMed PMID: 16841419. ](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16841419)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16841419)
[Sim HB, Lee JW, Park JT, Mindea SA, Lim J, Park J. Biomechanical evaluations of various c1-c2 posterior fixation techniques. Spine (Phila Pa 1976). 2011 Mar 15;36(6):E401-7. doi: 10.1097/BRS.0b013e31820611ba. PubMed PMID: 21372651. ](http://www.ncbi.nlm.nih.gov/pubmed/21372651)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21372651)
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 43
Figure 37 is the lateral radiograph of a 71-year-old woman who has pain with ambulation that improves when she sits down. She had similar symptoms 2 years earlier when she underwent an L3-L5 posterior spinal fusion. Upon examination she has good range of hip and knee motion, 5/5 motor function, and normal sensation of her lower extremities. She has negative bilateral straight-leg raise findings and her knees slightly flex to stand upright
37
Question 7High Yield
A 23-year-old man is evaluated in the emergency department after a diving accident. Radiographs reveal bilateral jumped facets at C6-7. Examination reveals no motor function below the C7 level. There is some maintained sensation in the lower extremities. What is the patient’s current grade on the ASIA (American Spinal Injury Association) impairment scale?
Explanation
The American Spinal Injury Association (ASIA) provides a standard method of measurement of spinal cord injury. The ASIA impairment scale is based on a
comprehensive motor and sensory examination. An ASIA A grade is ascribed to a patient with an injury with no motor or sensory preservation below the injury. An ASIA B grade is defined as no motor preservation below the level of injury but some sensory preservation below the injury level. An ASIA C grade is defined as a motor function grade of less than 3 below the injury level. An ASIA D grade is defined as a motor function grade of greater than 3 below the injury level. An ASIA E grade is defined as a normal neurologic examination.
comprehensive motor and sensory examination. An ASIA A grade is ascribed to a patient with an injury with no motor or sensory preservation below the injury. An ASIA B grade is defined as no motor preservation below the level of injury but some sensory preservation below the injury level. An ASIA C grade is defined as a motor function grade of less than 3 below the injury level. An ASIA D grade is defined as a motor function grade of greater than 3 below the injury level. An ASIA E grade is defined as a normal neurologic examination.
Question 8High Yield
Alumina = 340
Illustration A shows a stress vs. strain curve. Young Modulus of Elasticity is defined is defined as the slope of the line in the elastic zone
A prospective cohort study is performed looking at the relationship between blood transfusions and the risk of developing hepatitis C. In the transfused group (study group) of 595 patients, 75 patients develop hepatitis C. In the non- transfused group (control group) of 712 people, 16 people contract hepatitis C. What is the relative risk of developing hepatitis C with a transfusion.
Illustration A shows a stress vs. strain curve. Young Modulus of Elasticity is defined is defined as the slope of the line in the elastic zone
A prospective cohort study is performed looking at the relationship between blood transfusions and the risk of developing hepatitis C. In the transfused group (study group) of 595 patients, 75 patients develop hepatitis C. In the non- transfused group (control group) of 712 people, 16 people contract hepatitis C. What is the relative risk of developing hepatitis C with a transfusion.






Explanation
Vitronectin, integrin avß3, assists osteoclasts to attach to bone.
Osteoclasts attach to bone surfaces by means of integrins and then seal the space below. A ruffled border is then created and bone matrix is removed by proteolytic digestion through the lysosomal enzyme cathepsin K.
Incorrect Answers:
: RANK is a receptor on osteoclasts that when activated by RANKL stimulates osteoclasts. RANKL is found on osteoblasts.
Answer 3: Osteoprotegerin (OPG) decreases osteoclast differentiation by it’s interaction with RANKL (receptor activator of NF-kappaB ligand). OPG is made by osteoblasts and binds to RANKL (RANK Ligand) to competitively inhibit RANK binding.
Answer 4: PDGF (Platelet Derived Growth Factor) is involved in fracture healing. It is chemotactic and attracts inflammatory cells to the fracture site and is important in early fracture healing, especially the hematoma formation. Answer 5: TGF-B (transforming growth factor Beta) induces mesenchymal cells
to produce type II collagen & proteoglycans. It is important in the early stages of fracture callus formation.
Which of the following is a phenomenon whereby the symptoms of a genetic disorder become apparent at an earlier age as it is passed on to the next generation?
1) Genetic drift
2) Expansion
3) Mendelian inheritance
4) Anticipation
5) Phenotypic plasticity
Anticipation is a phenomenon whereby the symptoms of a genetic disorder become apparent at an earlier age as it is passed on to the next generation. In most cases, an increase of severity of symptoms is also noted. Anticipation is common in trinucleotide repeat disorders such as Huntington's disease, myotonic dystrophy, Friedreich ataxia, and Fragile X syndrome. Illustration A shows the genetics of the trinucleotide repeat disorders.
A 58-year-old female complains of continued pain and swelling 6 months following total knee arthroplasty. She describes a burning pain that radiates from the knee down the anterior compartment of the leg. The pain arises sporadically and is associated with swelling,
**sweating, and a purplish hue of the leg. Knee radiographs are**
provided in Figures A and B. Aspiration is negative for infection. Which of the following is the best management?
1) Lumbar spine MRI to evaluate for radiculopathy of the L3 nerve root
2) Alpha-adrenergic blockers, physical therapy, tactile discrimination training, and graded motor imagery
3) Surgical exploration of the knee
4) Surgical debridement, pulsatile irrigation, tissue sampling for culture/biopsy, and polyethylene exchange
5) Magnetic resonance arthrogram (MRA) with intra-articular contrast and diagnostic steroid injection
The clinical scenario and radiographs are consistent with a patient who is experiencing complex regional pain syndrome following total knee arthroplasty (TKA).
Complex regional pain syndrome, which was previously known as reflex sympathetic dystrophy, is characterized by intense burning pain, stiffness, swelling, and discoloration of the legs, feet, arms and hand (most common). Current treatment modalities are multi- modal and include GABA agonists, alpha-blockers, beta-blockers, physical therapy, occupational therapy, graded motor imagery, tactile discrimination treatments, sympathectomy, local anesthetics, and even spinal cord stimulators.
Mont et al. reported limited success in 27 patients who had surgical exploration of radiographically normal knees following TKA with unexplained pain. Outcomes were especially poor in patients who had achieved adequate range of motion and continued to have pain prior to surgical exploration. Patients with decreased range of motion who achieved improvement in motion postoperatively also demonstrated great relief of pain.
Figure A and B are AP and lateral radiographs of a well-fixed total knee
arthroplasty.
Incorrect Answers:
Answer 1: An MRI of the lumbar spine is not indicated in this patient as their symptoms are suggestive of complex regional pain syndrome, not an L3 radiculopathy.
Answer 3: Surgical exploration of radiographically normal knees following TKA for patients with unexplained pain has been found to have limited success. Answer 4: Surgical irrigation and debridement is not indicated in this setting as the patient is not presenting with symptoms suggestive of infection.
Answer 5: An MRA with intra-articular contrast and diagnostic steroid is not indicated in the setting of complex regional pain syndrome.
Which system of lacunar networks is used among osteocytes to communicate?
1) Volkmann canals
2) Cement lines
3) Secondary messenger systems
4) Canaliculi
5) Haversian canals
Canaliculi are a system within the lacunar network used by osteocytes to communicate with each other.
Osteocytes have numerous cell processes (filopodia) that project through the canaliculi and connect to each other via gap junctions (see Illustrations B and C). Through this network osteocytes establish contact and communication with adjacent osteocytes for exchange of nutrients and metabolic waste. They are oriented in a radial fashion around the central Haversian canal.
Knothe Tate et al described the changes occuring in different pathologies. In normal bone, osteocyte connectivity is high and processes are oriented in the direction of blood supply. In osteoporotic bone, there is decreased osteocyte connectivity and orientation and tortuous cell processes. In osteoarthritic bone, there is decreased osteocyte viability and connectivity, but preserved
orientation. In osteomalacic bone, there is preserved viability and connectivity, but tortuous and chaotic cell processes.
Illustration A shows the structure of compact and spongy bone. Illustration B shows gap junctions between cells. Illustration C shows secondary messengers crossing gap junctions.
Incorrect Answers
Vitronectin, integrin avß3, assists osteoclasts to attach to bone.
Osteoclasts attach to bone surfaces by means of integrins and then seal the space below. A ruffled border is then created and bone matrix is removed by proteolytic digestion through the lysosomal enzyme cathepsin K.
Incorrect Answers:
: RANK is a receptor on osteoclasts that when activated by RANKL stimulates osteoclasts. RANKL is found on osteoblasts.
Answer 3: Osteoprotegerin (OPG) decreases osteoclast differentiation by it’s interaction with RANKL (receptor activator of NF-kappaB ligand). OPG is made by osteoblasts and binds to RANKL (RANK Ligand) to competitively inhibit RANK binding.
Answer 4: PDGF (Platelet Derived Growth Factor) is involved in fracture healing. It is chemotactic and attracts inflammatory cells to the fracture site and is important in early fracture healing, especially the hematoma formation. Answer 5: TGF-B (transforming growth factor Beta) induces mesenchymal cells
to produce type II collagen & proteoglycans. It is important in the early stages of fracture callus formation.
Which of the following is a phenomenon whereby the symptoms of a genetic disorder become apparent at an earlier age as it is passed on to the next generation?
1) Genetic drift
2) Expansion
3) Mendelian inheritance
4) Anticipation
5) Phenotypic plasticity
Anticipation is a phenomenon whereby the symptoms of a genetic disorder become apparent at an earlier age as it is passed on to the next generation. In most cases, an increase of severity of symptoms is also noted. Anticipation is common in trinucleotide repeat disorders such as Huntington's disease, myotonic dystrophy, Friedreich ataxia, and Fragile X syndrome. Illustration A shows the genetics of the trinucleotide repeat disorders.
A 58-year-old female complains of continued pain and swelling 6 months following total knee arthroplasty. She describes a burning pain that radiates from the knee down the anterior compartment of the leg. The pain arises sporadically and is associated with swelling,
**sweating, and a purplish hue of the leg. Knee radiographs are**
provided in Figures A and B. Aspiration is negative for infection. Which of the following is the best management?
1) Lumbar spine MRI to evaluate for radiculopathy of the L3 nerve root
2) Alpha-adrenergic blockers, physical therapy, tactile discrimination training, and graded motor imagery
3) Surgical exploration of the knee
4) Surgical debridement, pulsatile irrigation, tissue sampling for culture/biopsy, and polyethylene exchange
5) Magnetic resonance arthrogram (MRA) with intra-articular contrast and diagnostic steroid injection
The clinical scenario and radiographs are consistent with a patient who is experiencing complex regional pain syndrome following total knee arthroplasty (TKA).
Complex regional pain syndrome, which was previously known as reflex sympathetic dystrophy, is characterized by intense burning pain, stiffness, swelling, and discoloration of the legs, feet, arms and hand (most common). Current treatment modalities are multi- modal and include GABA agonists, alpha-blockers, beta-blockers, physical therapy, occupational therapy, graded motor imagery, tactile discrimination treatments, sympathectomy, local anesthetics, and even spinal cord stimulators.
Mont et al. reported limited success in 27 patients who had surgical exploration of radiographically normal knees following TKA with unexplained pain. Outcomes were especially poor in patients who had achieved adequate range of motion and continued to have pain prior to surgical exploration. Patients with decreased range of motion who achieved improvement in motion postoperatively also demonstrated great relief of pain.
Figure A and B are AP and lateral radiographs of a well-fixed total knee
arthroplasty.
Incorrect Answers:
Answer 1: An MRI of the lumbar spine is not indicated in this patient as their symptoms are suggestive of complex regional pain syndrome, not an L3 radiculopathy.
Answer 3: Surgical exploration of radiographically normal knees following TKA for patients with unexplained pain has been found to have limited success. Answer 4: Surgical irrigation and debridement is not indicated in this setting as the patient is not presenting with symptoms suggestive of infection.
Answer 5: An MRA with intra-articular contrast and diagnostic steroid is not indicated in the setting of complex regional pain syndrome.
Which system of lacunar networks is used among osteocytes to communicate?
1) Volkmann canals
2) Cement lines
3) Secondary messenger systems
4) Canaliculi
5) Haversian canals
Canaliculi are a system within the lacunar network used by osteocytes to communicate with each other.
Osteocytes have numerous cell processes (filopodia) that project through the canaliculi and connect to each other via gap junctions (see Illustrations B and C). Through this network osteocytes establish contact and communication with adjacent osteocytes for exchange of nutrients and metabolic waste. They are oriented in a radial fashion around the central Haversian canal.
Knothe Tate et al described the changes occuring in different pathologies. In normal bone, osteocyte connectivity is high and processes are oriented in the direction of blood supply. In osteoporotic bone, there is decreased osteocyte connectivity and orientation and tortuous cell processes. In osteoarthritic bone, there is decreased osteocyte viability and connectivity, but preserved
orientation. In osteomalacic bone, there is preserved viability and connectivity, but tortuous and chaotic cell processes.
Illustration A shows the structure of compact and spongy bone. Illustration B shows gap junctions between cells. Illustration C shows secondary messengers crossing gap junctions.
Incorrect Answers
Question 9High Yield
Pain emanating from the sacroiliac (SI) joint is best identified by which of the following maneuvers?

Explanation
Though no gold standard exists, a reduction of concordant pain by at least 75 to 80% following an intra-articular, image-guided anesthetic injection is considered to be the most reliable method of identifying the SI joint as the cause of a patient's pain. Although provocation tests including the Gaenslen test, the compression test, thigh thrust, and Yeoman test are commonly used and can be helpful in diagnosing non-specific SI joint pain, individually they are not as reliable as the response to a diagnostic, anesthetic injection. Of note, the combination of all 4 manuevers has proven to be more useful than any one individual test. An MRI of the SI joint showing bony erosion and bone marrow edema suggests inflammatory arthritis and may not necessarily be associated with pain.
RECOMMENDED READINGS
Hancock MJ, Maher CG, Latimer J, Spindler MF, McAuley JH, Laslett M, Bogduk N. Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. Eur Spine
[J. 2007 Oct;16(10):1539-50. Epub 2007 Jun 14. PubMed PMID: 17566796. ](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17566796)
Visser LH, Nijssen PG, Tijssen CC, van Middendorp JJ, Schieving J. Sciatica-like symptoms and the sacroiliac joint: clinical features and differential diagnosis. Eur Spine J. 2013 Jul;22(7):1657-64. doi: 10.1007/s00586-013-2660-5. Epub 2013 Mar 2. PubMed PMID:
[23455949/. ](http://www.ncbi.nlm.nih.gov/pubmed/23455949)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23455949)
[Weber U, Zubler V, Pedersen SJ, Rufibach K, Lambert RG, Chan SM, Ostergaard M, Maksymowych WP. Development and validation of a magnetic resonance imaging reference criterion for defining a positive sacroiliac joint magnetic resonance imaging finding in spondyloarthritis. Arthritis Care Res (Hoboken). 2013 Jun;65(6):977-85. doi: 10.1002/acr.21893. PubMed PMID: 23203670. ](http://www.ncbi.nlm.nih.gov/pubmed/23203670)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23203670)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23203670)
CLINICAL SITUATION FOR QUESTION 72 THROUGH 75
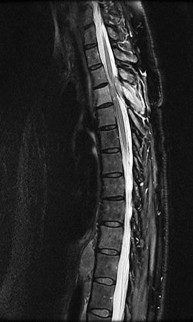
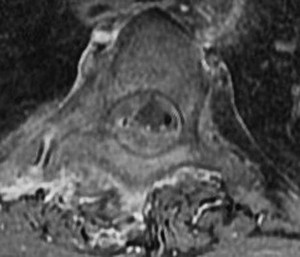
Figures 72a through 72c are the sagittal CT scan and thoracic MR images of a 52-year-old woman with a history of pancreatic neuroendocrine tumor who has severe upper thoracic back pain despite receiving aggressive oral pain treatment. She has metastases in her liver, adrenal glands, and abdominal mesentery. The thoracic disease has been treated with conventional radiation. She continues to work her part-time job without experiencing signs or symptoms of myelopathy.
A B
C
RECOMMENDED READINGS
Hancock MJ, Maher CG, Latimer J, Spindler MF, McAuley JH, Laslett M, Bogduk N. Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. Eur Spine
[J. 2007 Oct;16(10):1539-50. Epub 2007 Jun 14. PubMed PMID: 17566796. ](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17566796)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17566796)
Visser LH, Nijssen PG, Tijssen CC, van Middendorp JJ, Schieving J. Sciatica-like symptoms and the sacroiliac joint: clinical features and differential diagnosis. Eur Spine J. 2013 Jul;22(7):1657-64. doi: 10.1007/s00586-013-2660-5. Epub 2013 Mar 2. PubMed PMID:
[23455949/. ](http://www.ncbi.nlm.nih.gov/pubmed/23455949)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23455949)
[Weber U, Zubler V, Pedersen SJ, Rufibach K, Lambert RG, Chan SM, Ostergaard M, Maksymowych WP. Development and validation of a magnetic resonance imaging reference criterion for defining a positive sacroiliac joint magnetic resonance imaging finding in spondyloarthritis. Arthritis Care Res (Hoboken). 2013 Jun;65(6):977-85. doi: 10.1002/acr.21893. PubMed PMID: 23203670. ](http://www.ncbi.nlm.nih.gov/pubmed/23203670)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23203670)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23203670)
CLINICAL SITUATION FOR QUESTION 72 THROUGH 75
Figures 72a through 72c are the sagittal CT scan and thoracic MR images of a 52-year-old woman with a history of pancreatic neuroendocrine tumor who has severe upper thoracic back pain despite receiving aggressive oral pain treatment. She has metastases in her liver, adrenal glands, and abdominal mesentery. The thoracic disease has been treated with conventional radiation. She continues to work her part-time job without experiencing signs or symptoms of myelopathy.
A B
C
Question 10High Yield
A 10-year-old boy tripped as he was running down a hill, felt a painful pop in his right knee, and was unable to bear weight on the involved lower extremity. Examination reveals a tense effusion and an extensor lag of the right knee. Figures 36a and 36b show AP and lateral radiographs. Management should consist of
Explanation
DISCUSSION: The examination and radiographs are consistent with a sleeve fracture of the patella, which is an avulsion fracture of the distal pole of the patella with a disruption of the extensor mechanism. Treatment is open reduction and internal fixation of the patella, and repair of the extensor mechanism.
The distal fragment can be much larger than it appears on the radiographs because it consists largely of cartilage.
REFERENCES: Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990; 10:721 - 730. Question 37
When addressing a proximal intertrochanteric or subtrochanteric fracture in a juvenile with open growth plates, the arterial supply from what artery at the neck must be preserved?
1. ##### Lateral femoral circumflex
2. ##### Medial femoral circumflex
3. ##### Superior gluteal
4. ##### Inferior gluteal
5. ##### Obturator PREFERRED RESPONSE: 2
DISCUSSION: The medial femoral circumflex artery supplies blood to the femoral head. Its position along the
posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed.
**34 • American Academy of Orthopaedic Surgeons**
REFERENCES: Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295- 1301.
Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 419- 424.
DISCUSSION: The examination and radiographs are consistent with a sleeve fracture of the patella, which is an avulsion fracture of the distal pole of the patella with a disruption of the extensor mechanism. Treatment is open reduction and internal fixation of the patella, and repair of the extensor mechanism.
The distal fragment can be much larger than it appears on the radiographs because it consists largely of cartilage.
REFERENCES: Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990; 10:721 - 730. Question 37
When addressing a proximal intertrochanteric or subtrochanteric fracture in a juvenile with open growth plates, the arterial supply from what artery at the neck must be preserved?
1. ##### Lateral femoral circumflex
2. ##### Medial femoral circumflex
3. ##### Superior gluteal
4. ##### Inferior gluteal
5. ##### Obturator PREFERRED RESPONSE: 2
DISCUSSION: The medial femoral circumflex artery supplies blood to the femoral head. Its position along the
posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed.
**34 • American Academy of Orthopaedic Surgeons**
REFERENCES: Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295- 1301.
Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 419- 424.
Question 11High Yield
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the
Explanation
The area indicated by the arrow represents gadolinium contrast extending into a separation between the lateral labrum and its acetabular attachment. This can be a traumatic detachment, but occasionally a cleft may be present as a normal variant of the labral morphology. The capsular attachment of the iliofemoral ligament is peripheral to the labrum. The pulvinar is the common name applied to the fat and overlying synovium contained within the acetabular fossa above the ligamentum teres. The zona orbicularis is a circumferential thickening of the capsule around the femoral neck, and the retinacular vessels travel within the capsular synovium up the femoral neck to supply the femoral head.
REFERENCES: Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235.
Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Byrd JWT: Indications and contraindications, in Byrd JWT (ed): Operative Hip Arthroscopy. New York, NY, Thieme, 1998, pp 7-24.
REFERENCES: Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235.
Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Byrd JWT: Indications and contraindications, in Byrd JWT (ed): Operative Hip Arthroscopy. New York, NY, Thieme, 1998, pp 7-24.
Question 12High Yield
.Figures 12a through 12c show the radiographs of the closed fracture of a 24-year-old man who sustained an isolated injury to his left foot in a motorcycle crash. He was splinted and, on the following day, he nunderwent open reduction and internal fixation. Postoperative radiographs are shown in Figures 12d through 12f. What is the most likely complication of this injury?


Explanation
No detailed explanation provided for this question.
Question 13High Yield
Figures 7a through 7h
8
A B D …
C
E F G
8
A B D …
C
E F G





Explanation
9
Tarsal coalitions occur when primitive mesenchymal cells fail to differentiate and form the
normal articular separations between the tarsal bones of the hindfoot. Overall incidence is difficult to determine because many affected people are minimally symptomatic or asymptomatic. Symptomatic tarsal coalitions typically present in adolescents as a painful flatfoot; however, there are a number of possible presentations, and occasionally symptoms do not appear until adulthood. Most tarsal coalitions are between the calcaneus and the navicular (CN) and the talus and the calcaneus (TC). Although most TC coalitions are across the middle facet, posterior facet coalitions do occur. Plain radiographic evaluation of suspected tarsal coalition is the mainstay for diagnosis. However, coalitions can be bony or fibrous, and making the diagnosis can be difficult. The addition of CT images to distinguish bony definition and MR images to decipher soft tissue can aid in diagnostics. Bony coalitions appear as definite bony bridging between the bones, while fibrous coalitions are suspected when distortion of the bony anatomy is seen. Bony coalitions are best seen on the oblique view (CN) and Harris axial view (TC). There are a number of secondary signs such as the anteater (AE) sign (elongation of the anterior process of the calcaneus as it extends to the navicular as seen on the lateral view [CN]). talar beaking (traction spur of the talar neck thought to result from abnormal stresses as seen on the lateral view [both CN and TN]), and the “C” sign (a continuous cortical contour from the medial talus to the sustentaculum tali [ST]) as seen on the lateral view (TC). A number of newer signs are not as well known, such as a broad mediolateral dimension of the navicular on the anteroposterior (AP) view (the
navicular is wider than the talar head [CN]), nonvisualization of the middle facet on the lateral view (TC), the brick sign (a normal ST is flat, but a distorted ST is enlarged and curved [CN]), and a tapered lateral navicular bone as seen on the AP view (the medial navicular [CN] is much thicker than the lateral navicular).
Figure 1a shows talar beaking (TB), an AE, and an open middle facet (MF). Figure 1b shows a wide navicular (WN), and Figure 1c shows an abnormal articulation between the calcaneus and the navicular, all consistent with a CN coalition.
Figure 2a shows an irregularity of the anterior calcaneus. Figure 2b shows TB, AE, and MF. Figure 2c is an oblique view and shows nothing specific. Figure 2d shows an MF. Figure 2e shows an AE. Figures 2f, 2g, and 2h show edema and an abnormal connection between the calcaneus and the navicular, all consistent with a CN coalition.
Figure 3a shows a flatfoot. Figure 3b shows an MF and TB, but not a C sign. Figure 3c shows a bony irregularity between the calcaneus and the navicular and a WN. Figure 3d shows an MF. Figure 3e shows an MF, but narrowing or loss of the posterior facet. Figures 3f through 3h show medial edema and joint irregularities consistent with a posterior facet coalition.
Figures 4a through 4j do not show any signs of a coalition.
11
Figure 5a shows a WN and tapering of the lateral navicular. Figure 5b shows TB and MF, but no definite AE. Figure 5c shows an abnormal articulation between the calcaneus and the navicular with fragmentation. Figures 5d and 5e show an MF. Figure 5f shows TB and fragmentation of the articulation between the calcaneus and the navicular. Figures 5g and 5h show an MF consistent with a CN coalition.
Figure 6a shows a WN and tapering of the lateral navicular. Figure 6b shows AE and TB. Figure 6c shows an abnormal articulation between the calcaneus and the navicular. Figures 6d, 6e, 6g, 6h, and 6j show MF. Figures 6f and 6i show an abnormal articulation between the calcaneus and the navicular, all consistent with a CN coalition.
Figure 7a shows a mild flatfoot with lateral peritalar subluxation of the navicular. Figure 7b does not show an open MF and has a questionable C sign. Figure 7c shows that the opening between the calcaneus and the navicular appears normal without distortion. Figures 7d, 7e, 7g, and 7h show a lateral sloping distorted middle facet consistent with a middle facet coalition, and Figure 7f shows a normal posterior facet.
RECOMMENDED READINGS
1. [Crim JR, Kjeldsberg KM. Radiographic diagnosis of tarsal coalition. AJR Am J Roentgenol. 2004 Feb;182(2):323-8. PubMed PMID: 14736655. ](http://www.ncbi.nlm.nih.gov/pubmed/14736655)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/14736655)[ ](http://www.ncbi.nlm.nih.gov/pubmed/14736655)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14736655)
2. [Swiontkowski MF, Scranton PE, Hansen S. Tarsal coalitions: long-term results of surgical treatment. J Pediatr Orthop. 1983 Jul;3(3):287-92. PubMed PMID: 6874924. ](http://www.ncbi.nlm.nih.gov/pubmed/6874924)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6874924)
3. [Morgan RC Jr, Crawford AH. Surgical management of tarsal coalition in adolescent athletes. Foot Ankle. 1986 Dec;7(3):183-93. PubMed PMID: 3804141. ](http://www.ncbi.nlm.nih.gov/pubmed/3804141)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/3804141)[ ](http://www.ncbi.nlm.nih.gov/pubmed/3804141)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3804141)
Video 8
Tarsal coalitions occur when primitive mesenchymal cells fail to differentiate and form the
normal articular separations between the tarsal bones of the hindfoot. Overall incidence is difficult to determine because many affected people are minimally symptomatic or asymptomatic. Symptomatic tarsal coalitions typically present in adolescents as a painful flatfoot; however, there are a number of possible presentations, and occasionally symptoms do not appear until adulthood. Most tarsal coalitions are between the calcaneus and the navicular (CN) and the talus and the calcaneus (TC). Although most TC coalitions are across the middle facet, posterior facet coalitions do occur. Plain radiographic evaluation of suspected tarsal coalition is the mainstay for diagnosis. However, coalitions can be bony or fibrous, and making the diagnosis can be difficult. The addition of CT images to distinguish bony definition and MR images to decipher soft tissue can aid in diagnostics. Bony coalitions appear as definite bony bridging between the bones, while fibrous coalitions are suspected when distortion of the bony anatomy is seen. Bony coalitions are best seen on the oblique view (CN) and Harris axial view (TC). There are a number of secondary signs such as the anteater (AE) sign (elongation of the anterior process of the calcaneus as it extends to the navicular as seen on the lateral view [CN]). talar beaking (traction spur of the talar neck thought to result from abnormal stresses as seen on the lateral view [both CN and TN]), and the “C” sign (a continuous cortical contour from the medial talus to the sustentaculum tali [ST]) as seen on the lateral view (TC). A number of newer signs are not as well known, such as a broad mediolateral dimension of the navicular on the anteroposterior (AP) view (the
navicular is wider than the talar head [CN]), nonvisualization of the middle facet on the lateral view (TC), the brick sign (a normal ST is flat, but a distorted ST is enlarged and curved [CN]), and a tapered lateral navicular bone as seen on the AP view (the medial navicular [CN] is much thicker than the lateral navicular).
Figure 1a shows talar beaking (TB), an AE, and an open middle facet (MF). Figure 1b shows a wide navicular (WN), and Figure 1c shows an abnormal articulation between the calcaneus and the navicular, all consistent with a CN coalition.
Figure 2a shows an irregularity of the anterior calcaneus. Figure 2b shows TB, AE, and MF. Figure 2c is an oblique view and shows nothing specific. Figure 2d shows an MF. Figure 2e shows an AE. Figures 2f, 2g, and 2h show edema and an abnormal connection between the calcaneus and the navicular, all consistent with a CN coalition.
Figure 3a shows a flatfoot. Figure 3b shows an MF and TB, but not a C sign. Figure 3c shows a bony irregularity between the calcaneus and the navicular and a WN. Figure 3d shows an MF. Figure 3e shows an MF, but narrowing or loss of the posterior facet. Figures 3f through 3h show medial edema and joint irregularities consistent with a posterior facet coalition.
Figures 4a through 4j do not show any signs of a coalition.
11
Figure 5a shows a WN and tapering of the lateral navicular. Figure 5b shows TB and MF, but no definite AE. Figure 5c shows an abnormal articulation between the calcaneus and the navicular with fragmentation. Figures 5d and 5e show an MF. Figure 5f shows TB and fragmentation of the articulation between the calcaneus and the navicular. Figures 5g and 5h show an MF consistent with a CN coalition.
Figure 6a shows a WN and tapering of the lateral navicular. Figure 6b shows AE and TB. Figure 6c shows an abnormal articulation between the calcaneus and the navicular. Figures 6d, 6e, 6g, 6h, and 6j show MF. Figures 6f and 6i show an abnormal articulation between the calcaneus and the navicular, all consistent with a CN coalition.
Figure 7a shows a mild flatfoot with lateral peritalar subluxation of the navicular. Figure 7b does not show an open MF and has a questionable C sign. Figure 7c shows that the opening between the calcaneus and the navicular appears normal without distortion. Figures 7d, 7e, 7g, and 7h show a lateral sloping distorted middle facet consistent with a middle facet coalition, and Figure 7f shows a normal posterior facet.
RECOMMENDED READINGS
1. [Crim JR, Kjeldsberg KM. Radiographic diagnosis of tarsal coalition. AJR Am J Roentgenol. 2004 Feb;182(2):323-8. PubMed PMID: 14736655. ](http://www.ncbi.nlm.nih.gov/pubmed/14736655)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/14736655)[ ](http://www.ncbi.nlm.nih.gov/pubmed/14736655)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14736655)
2. [Swiontkowski MF, Scranton PE, Hansen S. Tarsal coalitions: long-term results of surgical treatment. J Pediatr Orthop. 1983 Jul;3(3):287-92. PubMed PMID: 6874924. ](http://www.ncbi.nlm.nih.gov/pubmed/6874924)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6874924)
3. [Morgan RC Jr, Crawford AH. Surgical management of tarsal coalition in adolescent athletes. Foot Ankle. 1986 Dec;7(3):183-93. PubMed PMID: 3804141. ](http://www.ncbi.nlm.nih.gov/pubmed/3804141)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/3804141)[ ](http://www.ncbi.nlm.nih.gov/pubmed/3804141)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3804141)
Video 8
Question 14High Yield
What is the most important predictor of functional outcome in patients with myelomeningocele?

Explanation
DISCUSSION: The functional motor level of the patient is of prime importance in determining prognosis and
outcome. Patients with thoracic and upper lumbar motor levels will need wheelchairs or hip-knee- ankle-foot orthoses to ambulate at all. Patients with midlumbar motor levels can be household or limited community walkers, whereas children with low lumbar or sacral motor levels are likely to be able to walk in the community.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 117-120.
Swank M, Dias L: Myelomeningocele: A review of the orthopaedic aspects of 206 patients treated from birth with no selection criteria. Dev Med Child Neurol 1992;34:1047-1052.
Figure 46a Figure 46b
outcome. Patients with thoracic and upper lumbar motor levels will need wheelchairs or hip-knee- ankle-foot orthoses to ambulate at all. Patients with midlumbar motor levels can be household or limited community walkers, whereas children with low lumbar or sacral motor levels are likely to be able to walk in the community.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 117-120.
Swank M, Dias L: Myelomeningocele: A review of the orthopaedic aspects of 206 patients treated from birth with no selection criteria. Dev Med Child Neurol 1992;34:1047-1052.
Figure 46a Figure 46b
Question 15High Yield
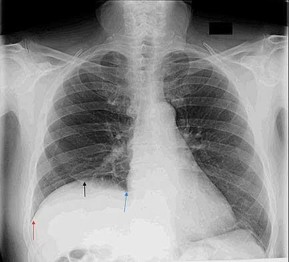
Figure 49 is the chest radiograph of a 47-year-old man who underwent right shoulder arthroscopy under general anesthesia and regional blockade (interscalene). The finding in the radiographic image likely is attributable to which mechanism?
Explanation
Positive end-pressure ventilation can cause alveolar rupture and pneumothorax, not elevation of the hemidiaphragm on the surgical side. The phrenic nerve, which controls the right hemidiaphragm, is not encountered during routine shoulder surgery because it courses medial to the scalene musculature near the midline of the neck. A traction injury is unlikely to cause injury to the phrenic nerve because it is part of the cervical plexus, which is not normally subject to traction during shoulder surgery. Hemidiaphragm paralysis via the phrenic nerve has been reported to occur as often as 100% of the time with use of interscalene regional anesthesia.
RECOMMENDED READINGS
1. [Urmey WF, Talts KH, Sharrock NE. One hundred percent incidence of hemidiaphragmatic paresis associated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg. 1991 Apr;72(4):498-503. PubMed PMID: 2006740.](http://www.ncbi.nlm.nih.gov/pubmed/2006740)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2006740)
2. [Lenters TR, Davies J, Matsen FA 3rd. The types and severity of complications associated with interscalene brachial plexus block anesthesia: local and national evidence. J Shoulder Elbow Surg. 2007 Jul-Aug;16(4):379-87. Epub 2007 Apr 19. PubMed PMID: 17448698.](http://www.ncbi.nlm.nih.gov/pubmed/17448698)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17448698)
RECOMMENDED READINGS
1. [Urmey WF, Talts KH, Sharrock NE. One hundred percent incidence of hemidiaphragmatic paresis associated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg. 1991 Apr;72(4):498-503. PubMed PMID: 2006740.](http://www.ncbi.nlm.nih.gov/pubmed/2006740)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2006740)
2. [Lenters TR, Davies J, Matsen FA 3rd. The types and severity of complications associated with interscalene brachial plexus block anesthesia: local and national evidence. J Shoulder Elbow Surg. 2007 Jul-Aug;16(4):379-87. Epub 2007 Apr 19. PubMed PMID: 17448698.](http://www.ncbi.nlm.nih.gov/pubmed/17448698)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17448698)
Question 16High Yield
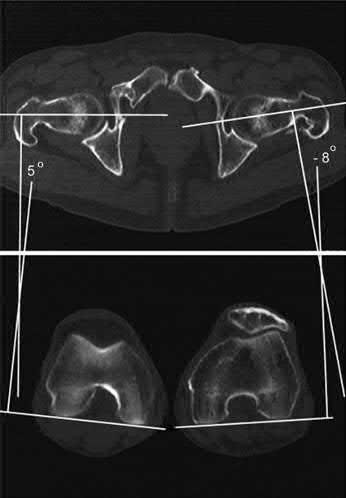
A radiologist uses CT scans to perform research on rotational malalignment of femoral shaft fractures treated with intramedullary nailing. He determines the angle between a line drawn tangential to the femoral condyles and a line drawn through the axis of the femoral neck. He does this for both the injured and uninjured sides. In Figure A, what malalignment is present for the injured left side compared with the uninjured right side?
Explanation
There is external malrotation of 13°.
Rotational malalignment arises after closed intramedullary nailing because anatomical reduction is achieved indirectly, resulting in less rotational control
compared with plate fixation. Rotational malalignment can be expressed as a difference in femoral anteversion between the injured and uninjured legs.
Jaarsma et al. reviewed rotational malalignment of femur fractures. They found that clinical assessment is inaccurate compared with CT measurement (±21°). Using CT measurement, they found the incidence of significant (=>15°) malrotation after IM nailing to be 20-30%. External malrotational leads to more symptoms than internal malrotation. Larger angles of malrotation (>15°) are more symptomatic. Complications of malrotation include degenerative arthritis of the hip and knee.
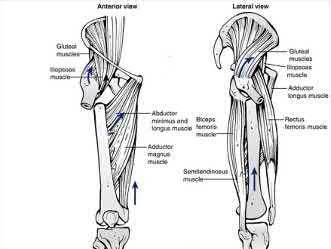
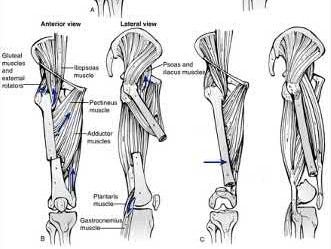
Figure A shows change in internal rotation of -8°-5°= -13°, giving 13° of external malrotation. Illustration A shows muscular attachments that contribute to rotational malalignment. In proximal fractures, the proximal fragment rotates externally (action of the glutei, iliopsoas and hip external rotators), producing internal malrotation. In distal fractures, the distal fragment rotates externally (action of the plantaris and lateral gastrocnemius), producing external malrotation.
Incorrect Answers:
Answers 1, 3, 4, 5: CT-torsion measurements show external malrotation of
13°.
Rotational malalignment arises after closed intramedullary nailing because anatomical reduction is achieved indirectly, resulting in less rotational control
compared with plate fixation. Rotational malalignment can be expressed as a difference in femoral anteversion between the injured and uninjured legs.
Jaarsma et al. reviewed rotational malalignment of femur fractures. They found that clinical assessment is inaccurate compared with CT measurement (±21°). Using CT measurement, they found the incidence of significant (=>15°) malrotation after IM nailing to be 20-30%. External malrotational leads to more symptoms than internal malrotation. Larger angles of malrotation (>15°) are more symptomatic. Complications of malrotation include degenerative arthritis of the hip and knee.
Figure A shows change in internal rotation of -8°-5°= -13°, giving 13° of external malrotation. Illustration A shows muscular attachments that contribute to rotational malalignment. In proximal fractures, the proximal fragment rotates externally (action of the glutei, iliopsoas and hip external rotators), producing internal malrotation. In distal fractures, the distal fragment rotates externally (action of the plantaris and lateral gastrocnemius), producing external malrotation.
Incorrect Answers:
Answers 1, 3, 4, 5: CT-torsion measurements show external malrotation of
13°.
Question 17High Yield
What is the most appropriate treatment?
Explanation
- Total-contact casting
Question 18High Yield
During preseason training camp, a 23-year-old football player comes to the sideline complaining of nausea, dizziness and headache after a
Explanation
The patient has exertional heat exhaustion (EHE). In cases of exertional heat illness with elevated core body temperature, it is critical to differentiate between EHE and exertional heat stroke (EHS). Patients suffering from EHE often complain of dizziness, nausea, cramping and headache. Vital signs can show mild tachycardia and normal to low blood pressure. EHS is defined by elevated core body temperature >40°C (104°F) and organ failure. Rapid cooling is critical in the setting of EHS, but not EHE. In the setting of EHE, the patient should be placed in a cool, shaded area and given fluids. Studies suggest that the presence of carbohydrate (<8%) in combination with electrolytes mildly promotes fluid retention better than drinking water alone.
Question 19High Yield
While experts disagree whether the postpolio syndrome is caused by a reactivation of the dormant virus or by an attritional aging phenomena of muscles that have been overworked over a period of time, both groups recommend which of the following guidelines for optimizing function in this population?
Explanation
Most leaders in orthopaedic surgery support Jacqueline Perry’s theory that the postpolio syndrome is an attritional degenerative process that is the result of overuse of muscles and joints that are unable to adequately tolerate overload, and have little functional reserve. For that reason, aerobic conditioning and exercise are important. Overload and exhaustion of involved muscles should be avoided.
REFERENCE: Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
REFERENCE: Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
Question 20High Yield
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
Explanation
Excision of the fracture fragment typically leads to rapid return to function. Fixation techniques are difficult to perform because of the size of the bone; hardware prominence is common. Nerve deficits are not typically noted in this injury. The motor branch of the ulnar nerve in Guyon’s canal must be protected during the surgical approach.
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
Question 21High Yield
Slide 1
A patient presents for surgical correction of a ruptured Achilles tendon. He recalls injuring his ankle 1 year previously, but did not seek any medical treatment at that time. You plan to repair the tendon, and at surgery, a gap between the tendon ends is noted (Slide). The following procedure is not consistent with an acceptable outcome:
A patient presents for surgical correction of a ruptured Achilles tendon. He recalls injuring his ankle 1 year previously, but did not seek any medical treatment at that time. You plan to repair the tendon, and at surgery, a gap between the tendon ends is noted (Slide). The following procedure is not consistent with an acceptable outcome:
Explanation
End-to-end repair of a chronic rupture of the Achilles tendon may not be considered if the gap is greater than 2 cm. Equinus positioning is never acceptable. Although each of the other alternatives above may be considered, each has its proponents and potential disadvantages.
Question 22High Yield
A 33-year-old woman reports a 3-month history of pain in both feet while running. Examination reveals bilateral point tenderness over the plantar fascia at its origin, and the pain is accentuated when the ankle is dorsiflexed. Management should consist of
Explanation
This question refers to plantar fascitis. Heel spurs are noted in approximately 50% of the cases of subcalcaneal pain syndrome. In this patient, diagnosis should rule out lumbar radiculopathy since the symptoms are bilateral.
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
Question 23High Yield
Which of the following is a risk factor for the development of a postoperative periprosthetiCfracture of the humerus:
Explanation
Osteolysis, osteopenia, and aggressive cortical reaming have been reported as potential risk factors for the development of a postoperative periprosthetiCfracture
Question 24High Yield
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
The patient has a symptomatic painful atrophic midclavicular nonunion, and the treatment of choice is rigid internal fixation with a dynamic compression plate and autogenous bone grafting. A tension band effect is desired and achieved by placing the plate superiorly. Excellent success rates of 90% to 100% have been reported using this technique. Intramedullary screw fixation without bone grafting has a decreased success rate. Partial claviculectomy is not a preferred option.
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 25High Yield
A 31-year-old woman presents for treatment of pain in the hallux. She has been experiencing the pain for 2 years. She notes limited motion of the hallux with pain in the joint, particularly when wearing high-heel shoes. She is unable to toe off with running activities. Upon examination, the motion in the hallux metatarsophalangeal (MP) joint is limited in dorsiflexion and radiographs demonstrate mild arthritis of the joint. She requests surgery to correct this disorder. The recommended treatment is:
Explanation
C heilectomy is the ideal treatment for correction of mild hallux rigidus. Although elevation of the first metatarsal rarely occurs (metatarsus primus elevatus) as the cause for hallux rigidus, osteotomy of the metatarsal should not be used as the treatment for correction of hallux rigidus with normal alignment of the first metatarsal.
Question 26High Yield
What is the most appropriate treatment at this time?




Explanation
Prompt diagnosis and treatment of patients with spinal epidural abscess is crucial to maintain and/or improve neurologic function. This clinical scenario stresses the importance of advanced imaging studies. It is also important to recognize the imaging features of spinal epidural abscess. T1-weighted gadolinium-enhanced images show ring enhancement with a central nonenhancing, low-signal area. In such a case, urgent decompression is indicated. Because of the location of the abscess, which is anterior to the spinal cord, an anterior decompression and reconstruction (ie, fusion) is probably the best treatment plan. Steroids are contraindicated in the presence of an epidural abscess. IV antibiotics alone will not adequately treat a patient with a neurological deficit. A posterior laminectomy and fusion will not safely allow access to the abscess.
RECOMMENDED READINGS
[Bluman EM, Palumbo MA, Lucas PR. Spinal epidural abscess in adults. J Am Acad Orthop Surg. 2004 May-Jun;12(3):155-63. Review. PubMed PMID: 15161168. ](http://www.ncbi.nlm.nih.gov/pubmed/15161168)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15161168) [Ghobrial GM, Beygi S, Viereck MJ, Maulucci CM, Sharan A, Heller J, Jallo J, Prasad S, Harrop JS. Timing in the surgical evacuation of spinal epidural abscesses. Neurosurg Focus. 2014 Aug;37(2):E1. doi: 10.3171/2014.6.FOCUS14120. PubMed PMID: 25081958. ](http://www.ncbi.nlm.nih.gov/pubmed/25081958)[View ](http://www.ncbi.nlm.nih.gov/pubmed/25081958)[Abstract](http://www.ncbi.nlm.nih.gov/pubmed/25081958)
[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25081958)
This is the last question of the exam.
RECOMMENDED READINGS
[Bluman EM, Palumbo MA, Lucas PR. Spinal epidural abscess in adults. J Am Acad Orthop Surg. 2004 May-Jun;12(3):155-63. Review. PubMed PMID: 15161168. ](http://www.ncbi.nlm.nih.gov/pubmed/15161168)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15161168) [Ghobrial GM, Beygi S, Viereck MJ, Maulucci CM, Sharan A, Heller J, Jallo J, Prasad S, Harrop JS. Timing in the surgical evacuation of spinal epidural abscesses. Neurosurg Focus. 2014 Aug;37(2):E1. doi: 10.3171/2014.6.FOCUS14120. PubMed PMID: 25081958. ](http://www.ncbi.nlm.nih.gov/pubmed/25081958)[View ](http://www.ncbi.nlm.nih.gov/pubmed/25081958)[Abstract](http://www.ncbi.nlm.nih.gov/pubmed/25081958)
[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25081958)
This is the last question of the exam.
Question 27High Yield
Which of the following is true concerning Achilles tendon ruptures:
Explanation
Important points to remember about Achilles tendon ruptures: A. Most common in middle-aged men
B. Often intermittent sports activity
C . Left more than right
D. Often the tendon is abnormal (degenerative) E. Mechanism
1/. Sudden forced plantarflexion
2/. Unexpected dorsiflexion
3/. Violent dorsiflexion of the plantar flexed foot
Factors which may make the patient more prone to rupture: A. Steroids
B. Fluoroquinolones
B. Often intermittent sports activity
C . Left more than right
D. Often the tendon is abnormal (degenerative) E. Mechanism
1/. Sudden forced plantarflexion
2/. Unexpected dorsiflexion
3/. Violent dorsiflexion of the plantar flexed foot
Factors which may make the patient more prone to rupture: A. Steroids
B. Fluoroquinolones
Question 28High Yield
Which of the following statements best describes what treatment is required for children with adolescent tibia vara?
Explanation
for this condition.
DISCUSSION: Spontaneous resolution of adolescent tibia vara is uncommon. Orthotic treatment has not been shown to be effective. Surgical elevation of the medial tibial plateau is a procedure that is occasionally necessary in individuals with early onset Blount’s disease but is not indicated for individuals with late onset Blount’s disease. Distal femoral varus deformity is commonly present and must be addressed.
2010 Pediatric Orthopaedic Examination Answer Book • 48
REFERENCES: Gordon JE, King DJ, Luhmann SJ, et al: Femoral deformity in tibia vara. J Bone Joint
Surg Am 2006;88:380-386.
Gordon JE, Heidenreich FP, Carpenter CJ, et al: Comprehensive treatment of late-onset tibia vara. J Bone Joint Surg Am 2005;87:1561-1570.
DISCUSSION: Spontaneous resolution of adolescent tibia vara is uncommon. Orthotic treatment has not been shown to be effective. Surgical elevation of the medial tibial plateau is a procedure that is occasionally necessary in individuals with early onset Blount’s disease but is not indicated for individuals with late onset Blount’s disease. Distal femoral varus deformity is commonly present and must be addressed.
2010 Pediatric Orthopaedic Examination Answer Book • 48
REFERENCES: Gordon JE, King DJ, Luhmann SJ, et al: Femoral deformity in tibia vara. J Bone Joint
Surg Am 2006;88:380-386.
Gordon JE, Heidenreich FP, Carpenter CJ, et al: Comprehensive treatment of late-onset tibia vara. J Bone Joint Surg Am 2005;87:1561-1570.
Question 29High Yield
Treatment of a patient with lumbar level myelomeningocele who has a vertical talus should consist of:
Explanation
Open reduction of the vertical talus will most likely prevent problems.
With observation only, the patient is likely to stand or walk and develop pressure problems. Talectomy will not produce the most usable foot.
Achilles tenotomy will not produce significant correction by itself. Triple arthrodesis will concentrate stress and lead to ulcers.
With observation only, the patient is likely to stand or walk and develop pressure problems. Talectomy will not produce the most usable foot.
Achilles tenotomy will not produce significant correction by itself. Triple arthrodesis will concentrate stress and lead to ulcers.
Question 30High Yield
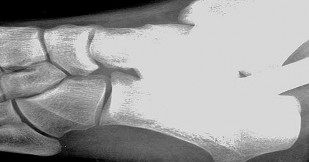
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
Explanation
The pisotriquetral joint is best seen on a lateral view in 30 degrees of supination. The carpal tunnel view provides visualization of the joint but to a lesser extent. The other views do not provide clear and accurate visualization.
REFERENCES: Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Steinmann SP, Linsheid RL: Pisotriquetral loose bodies. J Hand Surg 1997;22:918-921.
**related link****[ortho mcqs bank](https://hutaifortho.com/?sid=23)**
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
REFERENCES: Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Steinmann SP, Linsheid RL: Pisotriquetral loose bodies. J Hand Surg 1997;22:918-921.
**related link****[ortho mcqs bank](https://hutaifortho.com/?sid=23)**
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Question 31High Yield
An 11-year-old girl has had pain in the medial arch of her foot for the past 3 months. She reports that pain is present even with daily activities such as walking to class at school, and ibuprofen provides some relief. She denies any history of trauma. Examination reveals a flexible pes planus with focal tenderness over a prominent tarsal navicular tuberosity. Radiographs show a prominent accessory navicular. Management should consist of
Explanation
The patient has the classic symptoms, examination findings, and radiographs for a painful accessory navicular. Initial treatment should always be nonsurgical, specifically cast immobilization. Surgery should be reserved for those patients who fail nonsurgical management. Corticosteroids should not be injected into a posterior tibial tendon or insertion point because they can weaken the tendon and possibly cause tendon rupture. Triple arthrodesis and biopsy have no role in the management of a painful accessory navicular.
REFERENCE: Bordelon RL: Flatfoot in children and young adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 717-756.
REFERENCE: Bordelon RL: Flatfoot in children and young adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 717-756.
Question 32High Yield
A 64-year-old woman with rheumatoid arthritis cannot fully extend her fingers actively at the metacarpophalangeal (MCP) level. Full passive extension is possible, but she cannot actively maintain that extension when her fingers are released. The MCP joints do extend when her wrist is passively flexed. What is the most likely cause of this problem?
Explanation
Loss of MCP extension is common in the setting of rheumatoid arthritis, but potential causes are varied. An understanding of various etiologies is needed to address the multiple facets of inflammatory arthropathy, for which causes include extensor tendon rupture, MCP joint flexion
contracture/dislocation, subluxation of the extensor tendons at the MCP joint (sagittal band rupture), and posterior interosseous nerve (PIN) palsy. These causes are differentiated during an examination.
Extensor tendon ruptures, as seen with caput ulnae syndrome (Vaughan-Jackson syndrome) allow for passive MCP extension, not active extension or the ability to maintain extension actively, and would not involve finger extension with passive flexion tenodesis of the wrist. Flexion contractures of the MCP joints, as may be seen in dislocations, would not allow active or passive motion.
Subluxation of the extensor tendons at the MCP joints, as seen in attenuation of the sagittal bands, will usually preclude the initiation of active extension, but patients will be able to maintain extension of the MCP joints once they are placed in extension by the examiner. With a PIN palsy, no active extension or active hold is possible, but passive extension and tenodesis with wrist flexion are maintained. Synovitis of the elbow is the most likely cause of the PIN palsy. An extensor tenosynovitis or caput ulnae syndrome would not prohibit MCP extension unless the condition progressed to the point of causing other pathology.
RECOMMENDED READINGS
10. Millender LH, Nalbuff EA, Holdsworth DE. Posterior interosseous nerve syndrome secondary to rheumatoid synovitis. J Bone Joint Surg Am. 1973 Mar; 55(2):375-7. PubMed PMID: 4696167.
11. Steichen JB, Christensen AW. Posterior interosseous nerve compression syndrome. In: Gelberman RH ed. Operative Nerve Repair and Reconstruction. Philadelphia, PA: JB Lippincott; 1991:1151-1157.
contracture/dislocation, subluxation of the extensor tendons at the MCP joint (sagittal band rupture), and posterior interosseous nerve (PIN) palsy. These causes are differentiated during an examination.
Extensor tendon ruptures, as seen with caput ulnae syndrome (Vaughan-Jackson syndrome) allow for passive MCP extension, not active extension or the ability to maintain extension actively, and would not involve finger extension with passive flexion tenodesis of the wrist. Flexion contractures of the MCP joints, as may be seen in dislocations, would not allow active or passive motion.
Subluxation of the extensor tendons at the MCP joints, as seen in attenuation of the sagittal bands, will usually preclude the initiation of active extension, but patients will be able to maintain extension of the MCP joints once they are placed in extension by the examiner. With a PIN palsy, no active extension or active hold is possible, but passive extension and tenodesis with wrist flexion are maintained. Synovitis of the elbow is the most likely cause of the PIN palsy. An extensor tenosynovitis or caput ulnae syndrome would not prohibit MCP extension unless the condition progressed to the point of causing other pathology.
RECOMMENDED READINGS
10. Millender LH, Nalbuff EA, Holdsworth DE. Posterior interosseous nerve syndrome secondary to rheumatoid synovitis. J Bone Joint Surg Am. 1973 Mar; 55(2):375-7. PubMed PMID: 4696167.
11. Steichen JB, Christensen AW. Posterior interosseous nerve compression syndrome. In: Gelberman RH ed. Operative Nerve Repair and Reconstruction. Philadelphia, PA: JB Lippincott; 1991:1151-1157.
Question 33High Yield
An 80-year-old man who was involved in a fall from ground height is evaluated in the emergency department for head lacerations and mild neck pain. Examination reveals only mild tenderness of the posterior neck region with some limitation of motion. Neurologic examination is normal. Radiographs of the cervical spine are shown in
Figures 1 and
Figures 1 and

Explanation
■
The patient has radiographic findings compatible with diffuse idiopathic skeletal hyperostosis (DISH) of the cervical spine. Characteristics of DISH include flowing, non-marginal osteophytes at four or more levels. Patients with DISH develop a significant loss of flexibility of the spine. The spine acts more as a long bone with minimal force needed to create unstable fractures. Any minor trauma in patients with DISH should be worked up aggressively to rule out occult fracture. In this patient, radiographs fail to clearly rule out a fracture; therefore, CT of the cervical spine is indicated. Without a suspicion of history of a head injury, admission specifically for a possible intracranial hematoma is not warranted. The more concerning injury in a patient with DISH is occult neck fracture. Treatment with a soft or hard collar is not advised until a fracture is ruled out. Repeat radiographs are unlikely to show any occult fractures, and flexion and extension views would not be advised in a patient with a suspected vertebral fracture.
The patient has radiographic findings compatible with diffuse idiopathic skeletal hyperostosis (DISH) of the cervical spine. Characteristics of DISH include flowing, non-marginal osteophytes at four or more levels. Patients with DISH develop a significant loss of flexibility of the spine. The spine acts more as a long bone with minimal force needed to create unstable fractures. Any minor trauma in patients with DISH should be worked up aggressively to rule out occult fracture. In this patient, radiographs fail to clearly rule out a fracture; therefore, CT of the cervical spine is indicated. Without a suspicion of history of a head injury, admission specifically for a possible intracranial hematoma is not warranted. The more concerning injury in a patient with DISH is occult neck fracture. Treatment with a soft or hard collar is not advised until a fracture is ruled out. Repeat radiographs are unlikely to show any occult fractures, and flexion and extension views would not be advised in a patient with a suspected vertebral fracture.
Question 34High Yield
Figures 1 and 2 are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?

Explanation
■
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
Question 35High Yield
Slide 1
A 24-year-old man presents with a short forearm and a hand deformity. The patient is otherwise healthy with no other congenital defects. The clinical appearance of his forearm is shown (Slide). The potential complications of lengthening are discussed, and the patient is advised against it. However, the elbow flexion contracture is corrected by gradual distraction. One year postoperatively, the patient has attained a 30° correction of the flexion deformity, which remains mobile. Now, he desires that his wrist deformity be corrected. The procedure of choice is:
A 24-year-old man presents with a short forearm and a hand deformity. The patient is otherwise healthy with no other congenital defects. The clinical appearance of his forearm is shown (Slide). The potential complications of lengthening are discussed, and the patient is advised against it. However, the elbow flexion contracture is corrected by gradual distraction. One year postoperatively, the patient has attained a 30° correction of the flexion deformity, which remains mobile. Now, he desires that his wrist deformity be corrected. The procedure of choice is:
Explanation
Wrist arthrodesis is the best solution for this patient and his recurrent deformity because it provides a stable platform for grasp.
Question 36High Yield
Figures 72a through 72d are the radiograph, MR images, and biopsy specimen of a 42-year-old man with an insidious onset of left hip pain. Further imaging reveals no other lesions. What is the most appropriate initial treatment?


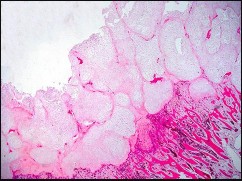
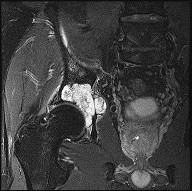
Explanation
This patient has a localized pelvic chondrosarcoma. Treatment is wide surgical resection. There is no defined role for chemotherapy or radiotherapy in the setting of conventional chondrosarcoma. Additionally, while intralesional treatment may be used for select low-grade extremity chondrosarcomas, it is not indicated for axial lesions. Treatment involving less than a wide surgical margin correlates with local recurrence.
RECOMMENDED READINGS
43. [Pring ME, Weber KL, Unni KK, Sim FH. Chondrosarcoma of the pelvis. A review of sixty-four cases. J Bone Joint Surg Am. 2001 Nov;83-A(11):1630-42. Review. PubMed PMID: 11701784. ](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[View](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11701784)
44. [Mavrogenis AF, Angelini A, Drago G, Merlino B, Ruggieri P. Survival analysis of patients with chondrosarcomas of the pelvis. J Surg Oncol. 2013 Jul;108(1):19-27. doi: 10.1002/jso.23351. Epub 2013 May 16. PubMed PMID: 23681650.](http://www.ncbi.nlm.nih.gov/pubmed/23681650)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23681650)
RECOMMENDED READINGS
43. [Pring ME, Weber KL, Unni KK, Sim FH. Chondrosarcoma of the pelvis. A review of sixty-four cases. J Bone Joint Surg Am. 2001 Nov;83-A(11):1630-42. Review. PubMed PMID: 11701784. ](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[View](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11701784)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11701784)
44. [Mavrogenis AF, Angelini A, Drago G, Merlino B, Ruggieri P. Survival analysis of patients with chondrosarcomas of the pelvis. J Surg Oncol. 2013 Jul;108(1):19-27. doi: 10.1002/jso.23351. Epub 2013 May 16. PubMed PMID: 23681650.](http://www.ncbi.nlm.nih.gov/pubmed/23681650)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23681650)
Question 37High Yield
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
The anterior border of the PCL is the most accurate and reproducible landmark for appropriate placement of the tibial tunnel for an ACL reconstruction. The central sagittal insertion point of the ACL is consistently 10 to 11 mm anterior to the anterior border of the PCL ligament. The anterior border of the tibia is not well visualized and does not serve as a reference point. While the posterior border of the anterior horn of the lateral meniscus could be used as a reference point, it has twice the variability of the PCL reference point. The posterior border of the tibia is difficult to identify and has greater variability than the PCL relative to the AP dimension of the proximal tibial surface. The anterior horn of the medial meniscus is also more variable than the PCL.
REFERENCES: Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
REFERENCES: Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 38High Yield
A 46-year-old man reports occasional squeaking of his hip 2 years after undergoing an uneventful total hip arthroplasty. History reveals no pain, physical examination cannot reproduce audible squeaking, and radiographs show appropriate implant position. What is the most appropriate management?

Explanation
DISCUSSION: In the absence of component malpositioning, hip pain, or other compelling reasons to reoperate, a squeaking ceramic bearing is not an indication for revision surgery. The patient can be reassured and observed.
Hopefully, with a better understanding of acoustic phenomena following ceramic total hip arthroplasty, this complication can be minimized.
REFERENCES: Yang CC, Kim RH, Dennis DA: The squeaking hip: A cause for concem-disagrees. Orthopedics
2007;30:739-742.
Walter WL, O’Toole GC, Walter WK, et al: Squeaking in ceramic-on-ceramic hips: The importance of acetabular component orientation. J Arthroplasty 2007;22:496-503.
Figure 80a Figure 80b
DISCUSSION: In the absence of component malpositioning, hip pain, or other compelling reasons to reoperate, a squeaking ceramic bearing is not an indication for revision surgery. The patient can be reassured and observed.
Hopefully, with a better understanding of acoustic phenomena following ceramic total hip arthroplasty, this complication can be minimized.
REFERENCES: Yang CC, Kim RH, Dennis DA: The squeaking hip: A cause for concem-disagrees. Orthopedics
2007;30:739-742.
Walter WL, O’Toole GC, Walter WK, et al: Squeaking in ceramic-on-ceramic hips: The importance of acetabular component orientation. J Arthroplasty 2007;22:496-503.
Figure 80a Figure 80b
Question 39High Yield
A 55-year-old man is about to undergo right total hip arthroplasty. A preoperative AP pelvis radiograph
is shown in Figure below. The final acetabular component and polyethylene liner are implanted. With the broach in place, the surgeon trials a standard offset neck and neutral length femoral head. The leg lengths are approximately equal, but the hip is unstable. What is the best next step?
is shown in Figure below. The final acetabular component and polyethylene liner are implanted. With the broach in place, the surgeon trials a standard offset neck and neutral length femoral head. The leg lengths are approximately equal, but the hip is unstable. What is the best next step?

Explanation
The radiograph shows that this patient has a high offset varus femoral morphology of both hips. Preoperative templating would identify this, and the surgeon should choose an implant system that has extended offset options to help match the native anatomy and biomechanics and minimize the risk of instability. Trialing a high offset neck, rather than a standard offset neck, is the next most appropriate step. Depending on the design of the implant system, this step can be accomplished by direct medialization of the femoral head, which would not affect leg length, or by lowering the neck angle, which would affect the leg length and would require a longer femoral head, because the leg lengths had previously been equal. Placement of a longer femoral head would likely improve hip stability but would also make the leg length uneven, which is a common cause of dissatisfaction after total hip arthroplasty. An offset acetabular liner also increases the leg length and does not correct the issue, which is on the femoral side. Trochanteric
advancement is sometimes used as a treatment for instability but would be inappropriate as the next step in this setting.
advancement is sometimes used as a treatment for instability but would be inappropriate as the next step in this setting.
Question 40High Yield
Figure 94 shows the lateral radiograph of an 80-year-old woman who is an independent ambulator and has a supracondylar periprosthetic fracture around the knee. What is the most appropriate management for this patient?
Explanation
DISCUSSION: A supracondylar femoral periprosthetic fracture that is a reducible or an irreducible fracture with poor distal bone stock and in the vicinity of loose or malpositioned components (type III) is very difficult to treat. One of the treatment options for patients with a loose femoral component and poor bone stock is the use of distal femoral replacement. The distal femoral replacement can be performed with relative ease, expediency, and is best suited for elderly or sedentary patients.
REFERENCES: Kassab M, Zalzal P, Azores GM, et al: Management of periprosthetic femoral fractures after total knee arthroplasty using a distal femoral allograft. J Arthroplasty 2004;19:361-368.
Kim KI, Egol KA, Hozack WJ, et al: Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res
2006;446:167-175.
REFERENCES: Kassab M, Zalzal P, Azores GM, et al: Management of periprosthetic femoral fractures after total knee arthroplasty using a distal femoral allograft. J Arthroplasty 2004;19:361-368.
Kim KI, Egol KA, Hozack WJ, et al: Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res
2006;446:167-175.
Question 41High Yield
What is the best treatment option for complex proximal humerus fractures in the
low-demand patient population?
low-demand patient population?

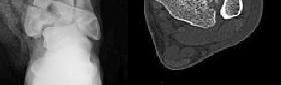
Explanation
In the recent meta-analysis by Mao and associates, there was no evidence to support the use of any of the operative modalities to treat 3- and 4-part fractures of the proximal humerus in low-demand patients. Although surgeons and patients will differ in their treatment algorithms, the recent meta-analysis showed lower complications with nonoperative treatment for these complex fractures. New treatment modalities involving fibular strut allograft, reverse total shoulder arthroplasty for elderly patients with an incompetent rotator cuff, and locked-plate fixation may prove to be superior to nonoperative treatment in select patient populations. However, not one operation has been shown to be superior to nonoperative treatment in the low-demand patient population with complex proximal humerus fractures.
**Question 15of 100**
**CLINICAL SITUATION**
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
The best delayed definitive surgical fixation plan would include
---
1. lateral plating of the fibula and a percutaneous medial column plate.
2. intramedullary fixation of the fibula and an anterolateral tibial plate.
3. open medial column plating, percutaneous screw fixation of the joint, and lateral fibular plating.
4. screw fixation of the medial column with an anterolateral tibial plate and lateral fibular plating
Answer: D
Discussion: The timely administration of antibiotics has been shown to be the best initial treatment to reduce the incidence of infection following an open fracture. Life threatening injuries must first be addressed. But in this isolated open pilon fracture, antibiotics should be initiated early along with tetanus prophylaxis. Reduction and splinting would stabilize the fracture but these interventions should follow antibiotic coverage. Emergency department irrigation is controversial. Closed reduction and splinting, external fixation, CT scan, and delayed open reduction internal fixation would be the preferred sequence of management. External fixation to provide provisional limb stabilization would be indicated in this length unstable C type injury to provide soft tissue stabilization and prevent further chondral injury. Splinting alone would not prevent shortening and would not allow soft tissue recovery. CT scans prior to limb stabilization are not warranted because the patterns make more sense after the restoration of gross length, rotation and alignment in the external fixator. Initial fibular fixation is also not recommended in this case because the location of incisions could affect the definitive surgical tactic. In this multi-fragmentary fibular injury, anatomic reduction would be challenging and malreduction could occur and influence subsequent reconstructions. Delayed open reduction internal fixation is ideal after the resolution of soft tissue swelling.
**Question 15of 100**
**CLINICAL SITUATION**
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
The best delayed definitive surgical fixation plan would include
---
1. lateral plating of the fibula and a percutaneous medial column plate.
2. intramedullary fixation of the fibula and an anterolateral tibial plate.
3. open medial column plating, percutaneous screw fixation of the joint, and lateral fibular plating.
4. screw fixation of the medial column with an anterolateral tibial plate and lateral fibular plating
Answer: D
Discussion: The timely administration of antibiotics has been shown to be the best initial treatment to reduce the incidence of infection following an open fracture. Life threatening injuries must first be addressed. But in this isolated open pilon fracture, antibiotics should be initiated early along with tetanus prophylaxis. Reduction and splinting would stabilize the fracture but these interventions should follow antibiotic coverage. Emergency department irrigation is controversial. Closed reduction and splinting, external fixation, CT scan, and delayed open reduction internal fixation would be the preferred sequence of management. External fixation to provide provisional limb stabilization would be indicated in this length unstable C type injury to provide soft tissue stabilization and prevent further chondral injury. Splinting alone would not prevent shortening and would not allow soft tissue recovery. CT scans prior to limb stabilization are not warranted because the patterns make more sense after the restoration of gross length, rotation and alignment in the external fixator. Initial fibular fixation is also not recommended in this case because the location of incisions could affect the definitive surgical tactic. In this multi-fragmentary fibular injury, anatomic reduction would be challenging and malreduction could occur and influence subsequent reconstructions. Delayed open reduction internal fixation is ideal after the resolution of soft tissue swelling.
Question 42High Yield
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?**
Explanation
Medial clavicle excision alone can be associated with postoperative instability of the clavicle. The clavicle should be stabilized to the first rib by reconstructing the costoclavicular ligament if it is torn or if the resection is lateral to its clavicular insertion. Therefore, care must be taken to resect only that part of the clavicle that is medial to the costoclavicular ligament. Adequate protection for vital structures that lie posterior to the medial end of the clavicle must be provided.
REFERENCES: Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 583-586.
REFERENCES: Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 583-586.
Question 43High Yield
The of the brachial plexus emerge between the anterior middle scalane muscles:
Explanation
After the roots emerge between the anterior scalene muscles, they merge to form trunks. The trunks branch into divisions and then merge into cords in the axilla. The cords branch into nerves.
Question 44High Yield
A 65-year-old man presents with chronic shoulder pain and weakness after failing extensive nonoperative treatment. Physical examination shows full passive range of motion, weakness with shoulder abduction, pain on palpation of the acromioclavicular (AC) joint and with cross-body adduction. Radiographs of the affected shoulder show evidence of AC joint osteoarthritis and an MRI scan reveals a full-thickness, reparable supraspinatus tear. A preoperative diagnostic lidocaine injection transiently improves the patient’s pain in the AC joint. In comparison with rotator cuff repair alone, at 2-year follow-up, distal clavicle excision for this patient’s condition has been shown to
Explanation
61
In patients with painful AC joint osteoarthritis undergoing surgery for concomitant rotator cuff tear, several well-designed studies and meta- analyses have shown that distal clavicle excision does not improve pain, function, shoulder range of motion or decrease need for revision surgery compared with rotator cuff repair alone.
In patients with painful AC joint osteoarthritis undergoing surgery for concomitant rotator cuff tear, several well-designed studies and meta- analyses have shown that distal clavicle excision does not improve pain, function, shoulder range of motion or decrease need for revision surgery compared with rotator cuff repair alone.
Question 45High Yield
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic
Explanation
The lesion is a variation of a type I superior labrum anterior and posterior lesion; therefore, appropriate treatment is simple debridement. Biceps tenodesis or release is not indicated because the biceps tendon and anchor are intact. There is no indication for labral repair or capsulorraphy.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Snyder SJ, Banas MP, Karzel RP: An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg 1995;4:243-248.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Snyder SJ, Banas MP, Karzel RP: An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg 1995;4:243-248.
Question 46High Yield
Figure 1
A 19-year-old man presents for treatment in the emergency department following a motorcycle accident. He sustained an isolated injury to his foot and ankle. The recommended treatment is:
A 19-year-old man presents for treatment in the emergency department following a motorcycle accident. He sustained an isolated injury to his foot and ankle. The recommended treatment is:
Explanation
The prognosis following fracture dislocation of the navicular is not good regardless of treatment. Although one may be tempted to perform an open reduction and immediate primary talonavicular arthrodesis, this is not necessary. Following open reduction and internal fixation, arthritis of the talonavicular joint may occur.
Question 47High Yield
Figure 29 shows the radiograph of a 25-year-old woman who has had a 3-month history of ankle pain after sustaining an inversion injury to the ankle. She reports occasional catching, but no sense of instability. Examination reveals ligament stability. Management should consist of
Explanation
Osteochondral lesions of the talar dome can have a traumatic or nontraumatic etiology. Most authors site a probable traumatic etiology for lateral lesions. Stage I and II lesions, which are composed of compressed subchondral bone or a partial detached osteochondral fragment, can be treated initially in a non-weight-bearing short leg cast for 6 weeks. Stage III medial lesions can also be treated in the same manner. If symptoms persist, the treament of choice is debridement of the fracture, curettage of the lesion, and drilling of the subchondral bone. This treatment also applies to lateral stage III and all stage IV lesions. If the fragment is at least one third of the size of the talar dome, management should consist of open reduction and internal fixation. In patients with more chronic lesions (4 to 6 months of persistent pain), the threshold to proceed with surgery is lower, even in a stage II lesion.
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Pettine KA, Morrey BF: Osteochondral fractures of the talus: A long-term follow-up. J Bone Joint Surg Br 1987;69:89-92.
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Pettine KA, Morrey BF: Osteochondral fractures of the talus: A long-term follow-up. J Bone Joint Surg Br 1987;69:89-92.
Question 48High Yield
An 11-year-old gymnast sustains a right dominant elbow dislocation. She undergoes a closed reduction in the emergency department with conscious sedation. Figures 1 and 2 are the postreduction radiographs. The best next step in treatment is

Explanation
■
The AP lateral radiographs show an incarcerated medial epicondyle. This is one of the absolute indications for surgical treatment of a displaced medial epicondyle fracture. The radiograph views show a nonconcentric reduction; therefore, immobilization without reduction will result in a painful stiff elbow. Although both MRI and CT scan will confirm the diagnosis, they are not necessary, are expensive, and a CT scan would expose the child to significant radiation.
Although controversy exists regarding surgical fixation of displaced nonincarcerated medial epicondyles, almost all surgeons agree that entrapped fragments should undergo open reduction and internal fixation. A number of fixation techniques are avaiable including divergent Kirschner wires, cannulated screws, suture anchors, and removal of the fragment with suture fixation. Screw fixation allows for shorter immobilization times and earlier motion.
■
The AP lateral radiographs show an incarcerated medial epicondyle. This is one of the absolute indications for surgical treatment of a displaced medial epicondyle fracture. The radiograph views show a nonconcentric reduction; therefore, immobilization without reduction will result in a painful stiff elbow. Although both MRI and CT scan will confirm the diagnosis, they are not necessary, are expensive, and a CT scan would expose the child to significant radiation.
Although controversy exists regarding surgical fixation of displaced nonincarcerated medial epicondyles, almost all surgeons agree that entrapped fragments should undergo open reduction and internal fixation. A number of fixation techniques are avaiable including divergent Kirschner wires, cannulated screws, suture anchors, and removal of the fragment with suture fixation. Screw fixation allows for shorter immobilization times and earlier motion.
Question 49High Yield
Figure 12 is the radiograph of a patient with type 2 diabetes, a body mass index of 42, and an Hgb A1c of 8. What is the most appropriate management for this injury?
Explanation
Several recent studies have shown that while there is an increased risk of complications following ORIF of displaced ankle fractures in diabetic patients compared with nondiabetic patients,the overall risks of treatment are less than that associated with nonsurgical treatment in diabetics. There is also the possibility that ORIF of unstable ankle fractures may forestall the development of Charcot changes in the ankle, although this is not definitively known. Extra rigid fixation may be required because of the patient’s size and poorly controlled diabetes. Nonsurgical management is associated with poorer functional outcomes (due to arthritis secondary to poor reduction of the fracture) and a higher rate of skin breakdown, due to the need for higher skin pressures from the use of highly molded casting used to maintain a closed reduction.
Question 50High Yield
Figures 1 through 4 show the radiographs, and Figures 5 through 8 show the MRIs obtained from a 32-year-old man with worsening left knee pain. A
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment.
29
Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL reconstruction alone is not indicated for this patient.
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis in the setting of reaction to metal debris?
A. Erythrocyte sedimentation rate, C-reactive protein, and white blood cell count
B. Serum cobalt and chromium ion levels
C. MRI with metal artifact reduction sequence (MARS)
D. CT of pelvis
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on-polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor-functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
Correct answer : C
30
29
Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL reconstruction alone is not indicated for this patient.
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis in the setting of reaction to metal debris?
A. Erythrocyte sedimentation rate, C-reactive protein, and white blood cell count
B. Serum cobalt and chromium ion levels
C. MRI with metal artifact reduction sequence (MARS)
D. CT of pelvis
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on-polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor-functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
Correct answer : C
30
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon